The Role of Non-Steroidal Anti-Inflammatory Drugs in Renal Colic

Abstract
:1. Introduction
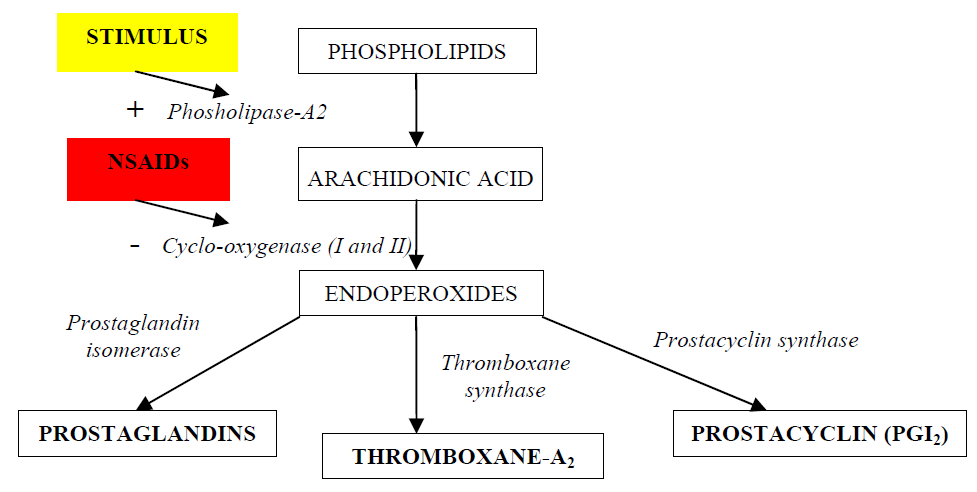
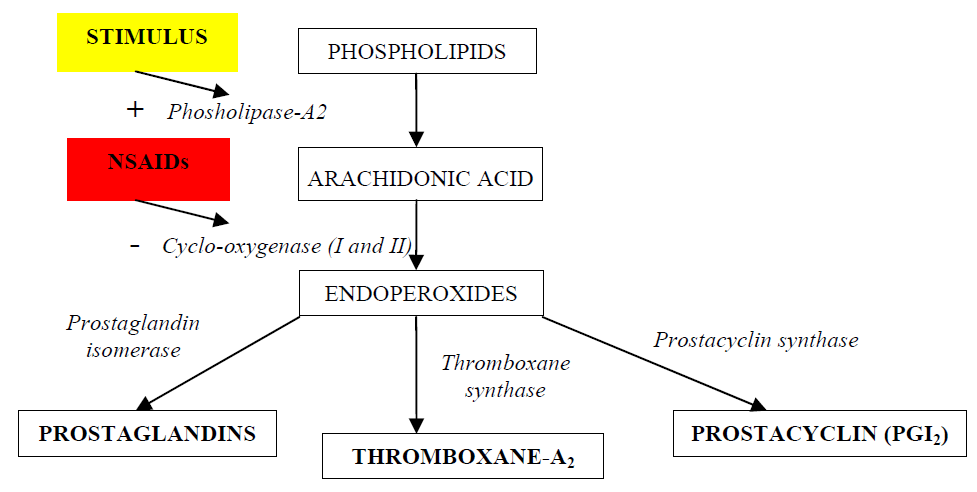
2. NSAIDs and Their Mechanism of Action
3. The Role of NSAIDs in Providing Analgesia in Renal Colic

{kind=link}
| Mean Pain Score % | |||
| Intravenous Indomethacin | Rectal Indomethacin | ||
| Time from Administration (min) | 10 | 54 | 73 |
| Side effects % | 55 | 37 | |
| Laerum 1995 [20] | Grenabo 1984 [21] | Kapoor 1985 [22] | ||||
| Diclofenac 50 mg PO tds | Placebo tds | Indomethacin 25mg PO bd + 100 mg PR nocte | Placebo bd + nocte | Indomethacin 50 mg PR tds | Placebo tds | |
| n | 41 | 39 | 37 | 41 | 13 | 13 |
| Mean stone size | 78% <6 mm | 97% <6 mm | 2.9 mm | 2.8 mm | 3.4 mm | 3.1 mm |
| Readmission Rate | 10% | 67% | 11% | 39% | 0% | 38% |
| Mean stone passage rate | 68% at 3 weeks | 74% at 3 weeks | 59% at 1 week | 61% at 1 week | 11/13 | 10/13 |
| Mean interval to passage | 3 days | 3.8 days | N/A | N/A | 3.4 days | 3.7 days |
4. The Role of NSAIDs in the Promotion of Stone Passage
5. Conclusions
References
- Coll, D.M.; Varanelli, M.J.; Smith, R.C. Relationship of spontaneous stone passage of ureteral calculi to stone size and location as revealed by unenhanced helical CT. Am. J. Roentgenol. 2002, 178, 101–103. [Google Scholar]
- Miller, O.F.; Kane, C.J. Time to stone passage for observed ureteral calculi: A guide for patient education. J. Urol. 1999, 162, 688–691. [Google Scholar]
- Painter, D.J.; Keeley, F.X., Jr. New concepts in the treatment of ureteral calculi. Curr. Opin. Urol. 2001, 11, 373–378. [Google Scholar]
- Crowley, A.R.; Byrne, J.C.; Darracott Vaughan, E.; Marion, D.N. The effect of acute obstruction on ureteral function. J. Urol. 1990, 143, 596–599. [Google Scholar]
- Perlmutter, A.; Miller, L.; Trimble, L.A.; Marion, D.N.; Vaughan, E.D., Jr.; Felson, D. Toradel, an NSAID used for renal colic, decreases renal perfusion and ureteral pressure in a canine model of unilateral ureteral obstruction. J. Urol. 1993, 149, 926–930. [Google Scholar] [PubMed]
- Cole, R.S.; Fry, C.H.; Shuttleworth, K.E.D. The action of the prostaglandins on isolated human ureteric smooth muscle. Br. J. Urol. 1988, 61, 19–26. [Google Scholar]
- Lennon, G.M.; Bourke, J.; Ryan, P.C.; Fitzpatrick, J.M. Pharmacological options for the treatment of acute ureteric colic. Br. J. Urol. 1993, 71, 401–407. [Google Scholar]
- Sivrikaya, A.; Celik, O.F.; Sivrikaya, N.; Ozgur, G.K. The effect of diclofenac sodium and papaverine on isolated human ureteric smooth muscle. Int. Urol. Neph. 2003, 35, 479–483. [Google Scholar]
- Nakada, S.Y.; Jerde, T.J.; Bjorling, D.E.; Saban, R. Selective cyclooxygenase-2 inhibitors reduce ureteral contraction in vitro: A better alternative for renal colic? J. Urol. 2000, 163, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, E.L.; Patrignani, P.; Tacconelli, S.; Rodriquez, L.A. Variability of risk of upper gastrointestinal bleeding among nonsteroidal anti-inflammatory drugs. Arthritis Rheum. 2010. Epub ahead of print. Available online: http://www3.interscience.wiley.com/journal/123299889/abstract.
- Riedemann, P.J.; Bersinic, S.; Cuddy, L.J.; Torrance, G.W.; Tugwell, P.X. A study to determine the efficacy and safety of tenoxicam versus piroxicam, diclofenac and indomethacin in patients with osteoarthritis: a meta-analysis. J. Rheumatol. 1993, 20, 2095–2103. [Google Scholar]
- Cohen, E.; Hafner, R.; Rotenberg, Z.; Fadilla, M.; Garty, M. Comparison of ketorolac and diclofenac in the treatment of renal colic. Eur. J. Clin. Pharmacol. 1998, 54, 455–458. [Google Scholar]
- Lafrance, J.P.; Miller, D.R. Selective and non-selective non-steroidal anti-inflammatory drugs and the risk of acute kidney injury. Pharmacoepidemiol. Drug. Saf. 2009, 18, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Bleumink, G.S.; Feenstra, J.; Sturkenboom, M.C.; Stricker, B.H. Non-steroidal anti-inflammatory drugs and heart failure. Drugs 2003, 63, 525–534. [Google Scholar]
- Dzau, V.J.; Packer, M.; Lilly, L.S.; Swartz, S.L.; Hollenberg, N.K.; Williams, G.H. Prostaglandins in severe congestive heart failure. N. Engl. J. Med. 1984, 310, 347–352. [Google Scholar]
- Kearney, P.M.; Baigent, C.; Godwin, J,; Halls, H.; Emberson, J.R.; Patrono, C. Do selective cyclo-oxygenase-2 inhibitors and traditional non-steroidal anti-inflammatory drugs increase the risk of atherothrombosis? Meta-analysis of randomised trials. BMJ. 2006, 332, 1302–1308. [Google Scholar] [PubMed]
- Cordell, W.H.; Larson, T.A.; Lingeman, J.E.; Nelson, D.R.; Woods, J.R.; Burns, L.B.; Klee, L.W. Indomethacin suppositories versus intravenous titrated morphine for the treatment of ureteral colic. Ann. Emerg. Med. 1994, 23, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Nissen, I.; Birke, H.; Olson, J.B.; Würtz, E.; Lorentzen, K.; Salomon, H.; Lynge, P.; Fly, P.; Jørgensen, T.H.; Svane, S.; et al. Treatment of ureteric colic: intravenous versus rectal administration of indomethacin. Br. J. Urol. 1990, 65, 576–579. [Google Scholar] [CrossRef] [PubMed]
- Holdgate, A.; Pollock, T. Systematic review of the relative efficacy of non-steroidal anti-inflammatory drugs and opioids in the treatment of acute renal colic. BMJ. 2004, 328, 1401–1408. [Google Scholar]
- Laerum, E.; Omundsen, O.E.; Gronseth, J.E.; Christianson, A.; Fagertun, H.E. Oral diclofenac in the prophylactic treatment of recurrent renal colic: A double blind comparison with placebo. Eur. Urol. 1995, 28, 108–111. [Google Scholar]
- Grenabo, L.; Holmlund, D. Indomethacin as prophylaxis against recurrent ureteral colic. Scand. J. Urol. Nephrol. 1984, 18, 325–327. [Google Scholar]
- Kapoor, D.; Weitzel, S.; Mowad, J.; Melanson, S.; Gillen, J. Use of indomethacin suppositories in the prophylaxis of recurrent ureteral colic. J. Urol. 1989, 142, 1428–1430. [Google Scholar]
- Cole, R.S.; Palfrey, E.L.H.; Smith, S.E.; Shuttleworth, K.E.D. Indomethacin as prophylaxis against ureteral colic following extracorporeal shock wave lithotripsy. J. Urol. 1989, 141, 9–12. [Google Scholar]
- Labanaris, A.P.; Kuhn, R.; Schott, G.E.; Zugor, V. Perirenal haematomas induced by extracorporeal shock wave lithotripsy (ESWL). Therapeutic management. Sci. World J. 2007, 7, 1563–1566. [Google Scholar]
- Rose, J.G.; Gillenwater, J.Y. Pathophysiology of ureteral obstruction. Am. J. Physiol. 1973, 225, 830–837. [Google Scholar]
- Davenport, K.; Timoney, A.G.; Keeley, F.X. A comparative in vitro study to determine the beneficial effect of calcium-channel and alpha (1)-adrenoceptor antagonism on human ureteric activity. BJU. Int. 2006, 98, 651–655. [Google Scholar] [CrossRef] [PubMed]
- Davenport, K.; Timoney, A.G.; Keeley, F.X., Jr. Effect of smooth muscle relaxant drugs on proximal human ureteric activity in vivo: a pilot study. Urol. Res. 2007, 35, 207–213. [Google Scholar] [CrossRef] [PubMed]
© 2010 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Davenport, K.; Waine, E. The Role of Non-Steroidal Anti-Inflammatory Drugs in Renal Colic. Pharmaceuticals 2010, 3, 1304-1310. https://doi.org/10.3390/ph3051304
Davenport K, Waine E. The Role of Non-Steroidal Anti-Inflammatory Drugs in Renal Colic. Pharmaceuticals. 2010; 3(5):1304-1310. https://doi.org/10.3390/ph3051304
Chicago/Turabian StyleDavenport, Kim, and Elizabeth Waine. 2010. "The Role of Non-Steroidal Anti-Inflammatory Drugs in Renal Colic" Pharmaceuticals 3, no. 5: 1304-1310. https://doi.org/10.3390/ph3051304
APA StyleDavenport, K., & Waine, E. (2010). The Role of Non-Steroidal Anti-Inflammatory Drugs in Renal Colic. Pharmaceuticals, 3(5), 1304-1310. https://doi.org/10.3390/ph3051304