
Potential Anti-Inflammatory and Anti-Fatigue Effects of an Oral Food Supplement in Long COVID Patients

 , , , ,
, , , , 
Abstract
1. Introduction
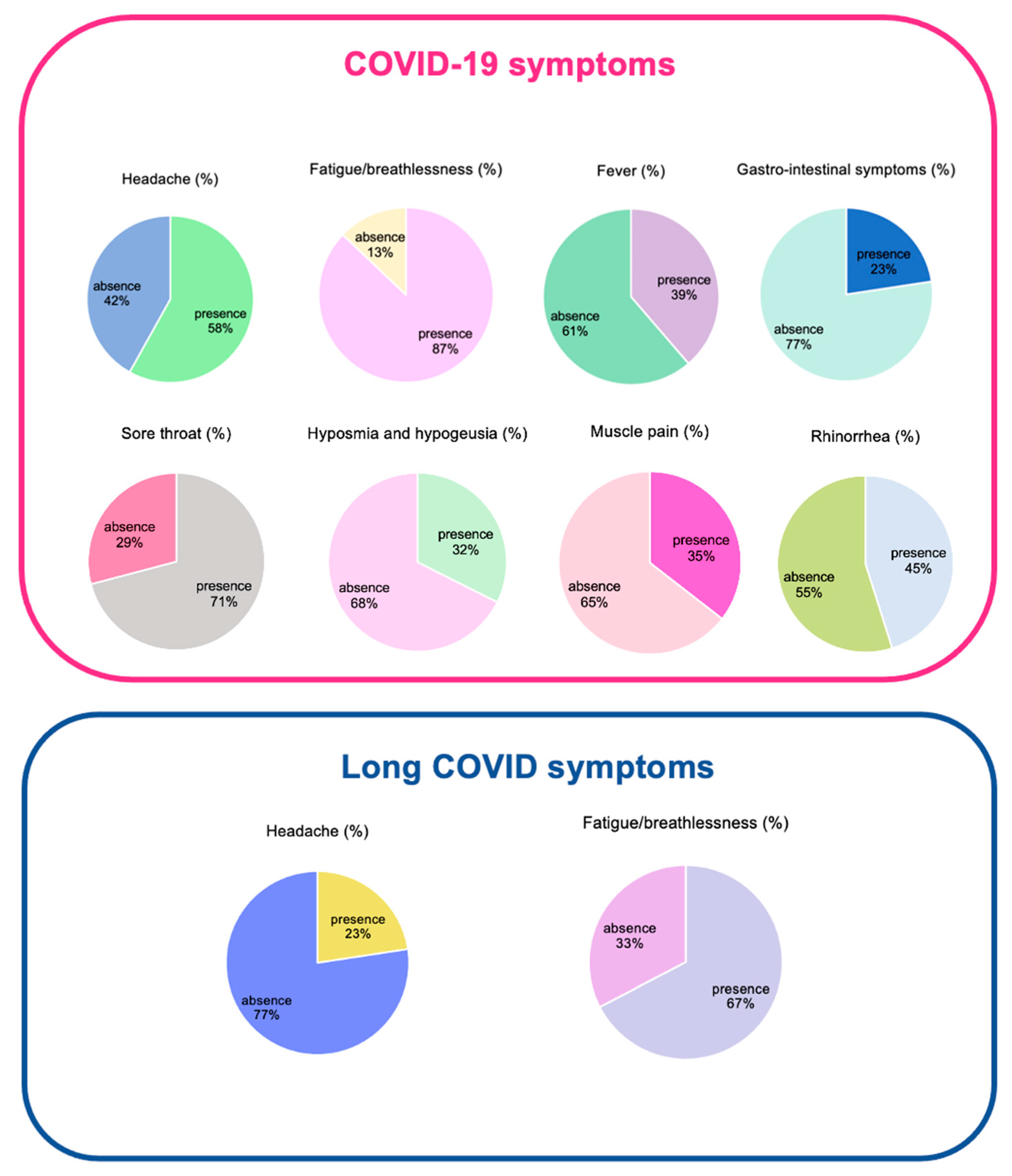
2. Results
3. Discussion
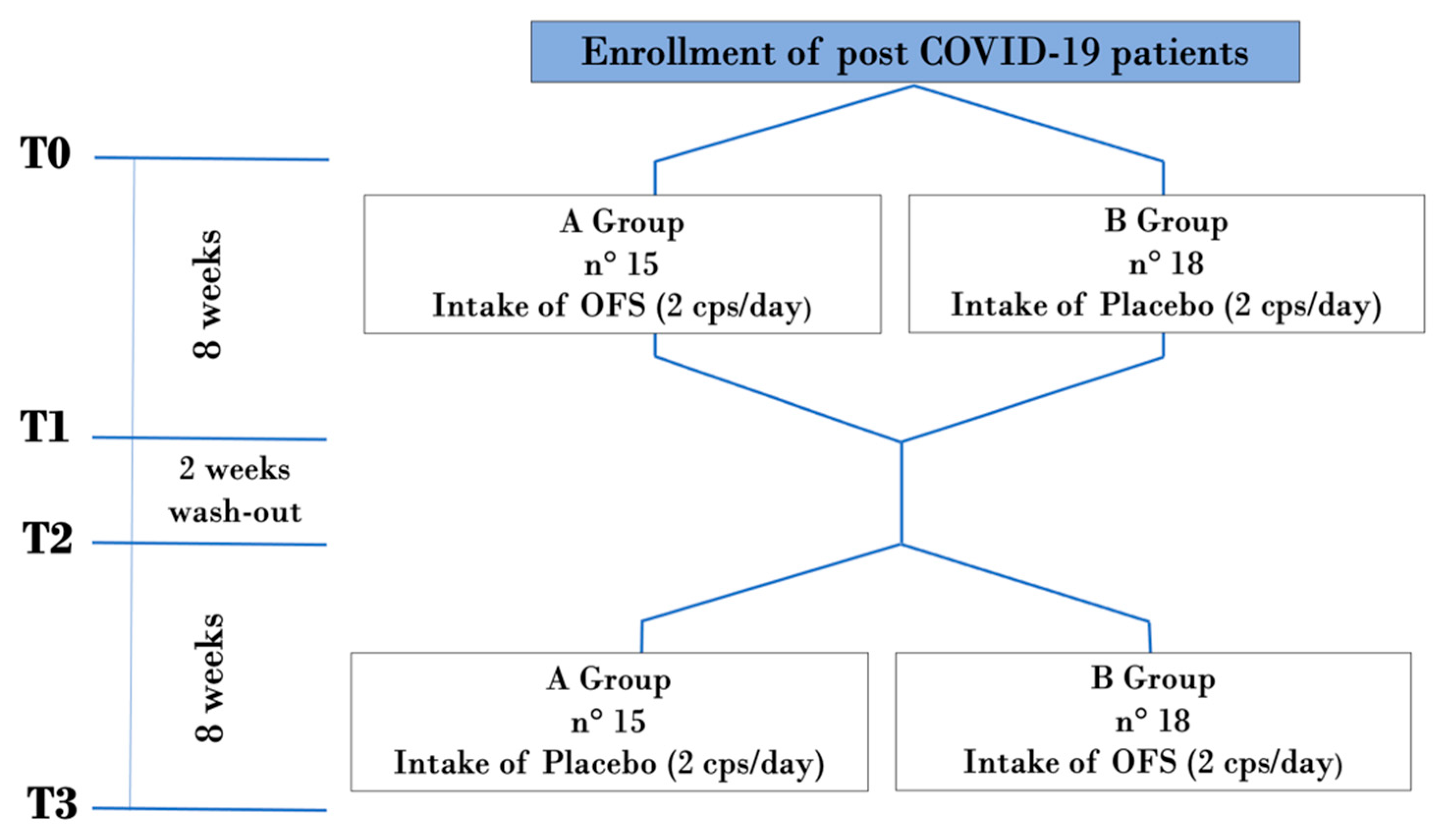
4. Materials and Methods
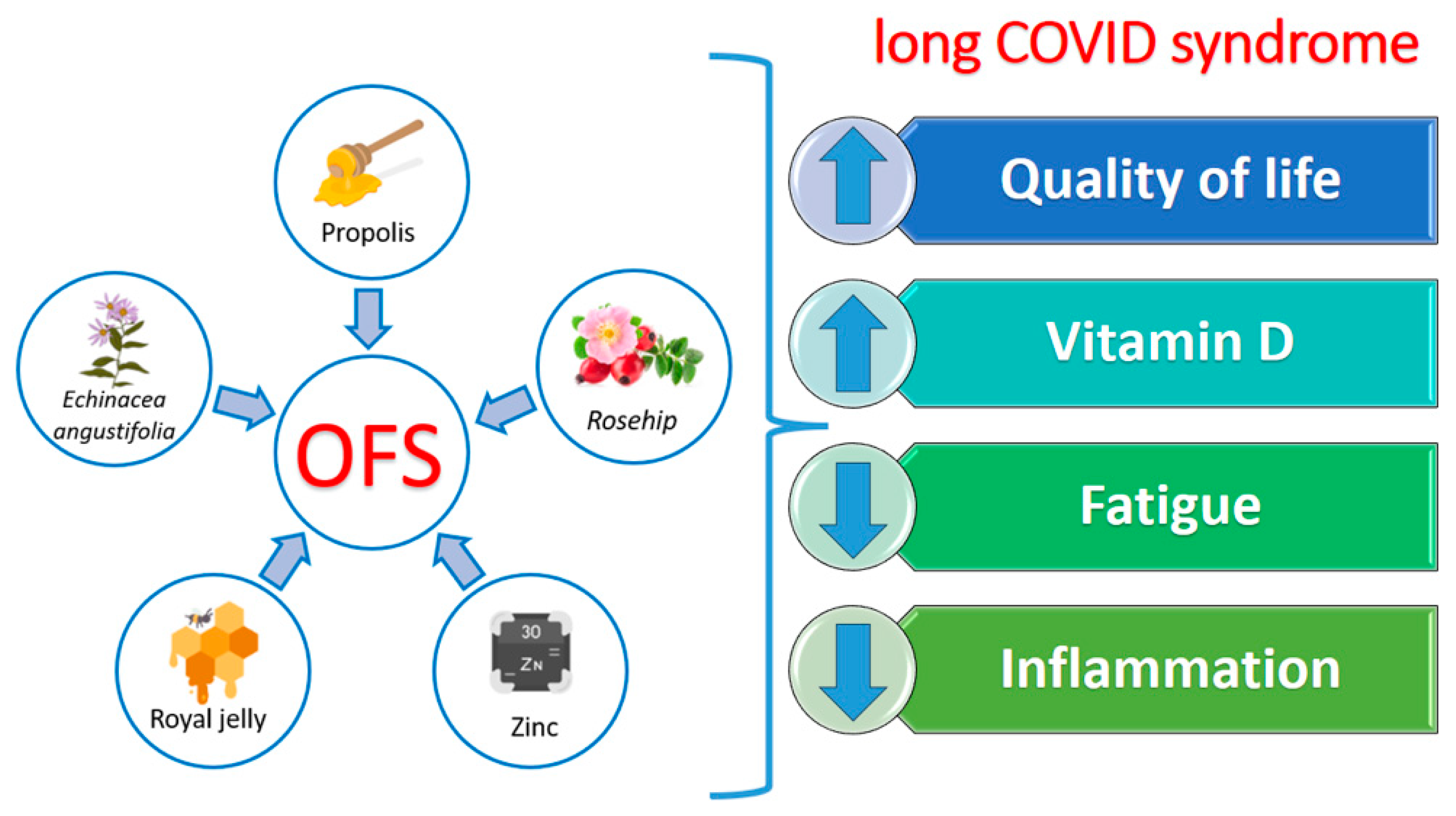
4.1. Analytical Characterization of OFS
4.1.1. Determination of the Quantity of Total Polyphenols: Folin–Ciocalteu Method
4.1.2. Determination of Anti-Radical Activity: DPPH Test
4.1.3. HPLC/UV Chromatographic Analyses
4.2. Enrolled Patients
- Both sexes;
- Age between 18 and 75 years;
- Body mass index (BMI) between 18.5 and 25 kg/m2;
- Patients with previous COVID-19 infection (ascertained by double-positive nose-pharyngeal molecular swab) in remission from 1 to 6 months (as confirmed by the negativity of the molecular nose-pharyngeal swab for SARS-CoV-2).
- Medications;
- Pregnancy and lactation;
- Both solid and hematological active phase neoplasms;
- HIV, HbsAg and HCV-positive patients;
- Not accepting informed consent;
- Any chronic pathological condition;
- Possible allergies to OFS components;
- Assumption of other OFSs with anti-inflammatory and antioxidant properties in the previous two months.
4.3. Laboratory Parameters
4.4. Blood Pressure Monitoring
4.5. Body Composition Analysis
4.6. Questionnaires
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rothan, H.A.; Byrareddy, S.N. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J. Autoimmun. 2020, 109, 102433. [Google Scholar] [CrossRef] [PubMed]
- Patterson, B.K.; Guevara-Coto, J.; Yogendra, R.; Francisco, E.B.; Long, E.; Pise, A.; Rodrigues, H.; Parikh, P.; Mora, J.; Mora-Rodriguez, R.A. Immune-Based Prediction of COVID-19 Severity and Chronicity Decoded Using Machine Learning. Front. Immunol. 2021, 12, 700782. [Google Scholar] [CrossRef]
- Turner, S.; Khan, M.A.; Putrino, D.; Woodcock, A.; Kell, D.B.; Pretorius, E. Long COVID: Pathophysiological factors and abnormalities of coagulation. Trends Endocrinol. Metab. 2023, 34, 321–344. [Google Scholar] [CrossRef] [PubMed]
- Borczuk, A.C.; Yantiss, R.K. The pathogenesis of coronavirus-19 disease. J. Biomed. Sci. 2022, 29, 87. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post-Coronavirus Disease 2019 (COVID-19) Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022, 226, 1593–1607. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.; Park, S.; Kim, E.Y.; Koyanagi, A.; Jacob, L.; Yon, D.K.; Lee, S.W.; Kim, M.S.; Radua, J.; Elena, D.; et al. Immunogenicity of COVID-19 vaccines in patients with diverse health conditions: A comprehensive systematic review. J. Med. Virol. 2022, 94, 4144–4155. [Google Scholar] [CrossRef]
- Ryan, F.J.; Hope, C.M.; Masavuli, M.G.; Lynn, M.A.; Mekonnen, Z.A.; Yeow, A.E.L.; Garcia-Valtanen, P.; Al-Delfi, Z.; Gummow, J.; Ferguson, C.; et al. Long-term perturbation of the peripheral immune system months after SARS-CoV-2 infection. BMC Med. 2022, 20, 26. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, J.Y.; Lee, S.; Lee, S.; Stubbs, B.; Koyanagi, A.; Dragioti, E.; Jacob, L.; Carvalho, A.F.; Radua, J.; et al. Environmental risk factors, protective factors, and biomarkers for postpartum depressive symptoms: An umbrella review. Neurosci. Biobehav. Rev. 2022, 140, 104761. [Google Scholar] [CrossRef]
- Joli, J.; Buck, P.; Zipfel, S.; Stengel, A. Post-COVID-19 fatigue: A systematic review. Front. Psychiatry 2022, 13, 947973. [Google Scholar] [CrossRef]
- Rosenthal, T.C.; Majeroni, B.A.; Pretorius, R.; Malik, K. Fatigue: An overview. Am. Fam. Physician 2008, 78, 1173–1179. [Google Scholar]
- Giuliano, M.; Tiple, D.; Agostoni, P.; Armocida, B.; Biardi, L.; Bonfigli, A.R.; Campana, A.; Ciardi, M.; Di Marco, F.; Floridia, M.; et al. Italian good practice recommendations on management of persons with Long-COVID. Front. Public. Health 2023, 11, 1122141. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Raveendran, A.V.; Jayadevan, R.; Sashidharan, S. Long COVID: An overview. Diabetes Metab. Syndr. 2021, 15, 869–875. [Google Scholar] [CrossRef]
- Noce, A.; Albanese, M.; Marrone, G.; Di Lauro, M.; Pietroboni Zaitseva, A.; Palazzetti, D.; Guerriero, C.; Paolino, A.; Pizzenti, G.; Di Daniele, F.; et al. Ultramicronized Palmitoylethanolamide (um-PEA): A New Possible Adjuvant Treatment in COVID-19 patients. Pharmaceuticals 2021, 14, 336. [Google Scholar] [CrossRef] [PubMed]
- Albanese, M.; Marrone, G.; Paolino, A.; Di Lauro, M.; Di Daniele, F.; Chiaramonte, C.; D’Agostini, C.; Romani, A.; Cavaliere, A.; Guerriero, C.; et al. Effects of Ultramicronized Palmitoylethanolamide (um-PEA) in COVID-19 Early Stages: A Case-Control Study. Pharmaceuticals 2022, 15, 253. [Google Scholar] [CrossRef]
- Cho, K.; Park, S.; Koyanagi, A.; Jacob, L.; Yon, D.K.; Lee, S.W.; Kim, M.S.; Kim, S.U.; Kim, B.K.; Shin, J.I.; et al. The effect of pharmacological treatment and lifestyle modification in patients with nonalcoholic fatty liver disease: An umbrella review of meta-analyses of randomized controlled trials. Obes. Rev. 2022, 23, e13464. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, R.; Botelho, F.D.; Pinto, A.M.V.; La Torre, A.M.A.; Almeida, J.; LaPlante, S.R.; Franca, T.C.C.; Veiga-Junior, V.F.; Dos Santos, M.C. Molecular modeling study of natural products as potential bioactive compounds against SARS-CoV-2. J. Mol. Model. 2023, 29, 183. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Romano, L.; Marrone, G.; Noce, A.; Pujia, A.; Perrone, M.A.; Aiello, V.; Colica, C.; De Lorenzo, A. Role of Personalized Nutrition in Chronic-Degenerative Diseases. Nutrients 2019, 11, 1707. [Google Scholar] [CrossRef]
- Ahbap, E.; Sakaci, T.; Kara, E.; Sahutoglu, T.; Koc, Y.; Basturk, T.; Sevinc, M.; Akgol, C.; Kayalar, A.O.; Ucar, Z.A.; et al. Neutrophil-to-lymphocyte ratio and platelet-tolymphocyte ratio in evaluation of inflammation in end-stage renal disease. Clin. Nephrol. 2016, 85, 199–208. [Google Scholar] [CrossRef]
- Bharadwaj, S.; El-Kafrawy, S.A.; Alandijany, T.A.; Bajrai, L.H.; Shah, A.A.; Dubey, A.; Sahoo, A.K.; Yadava, U.; Kamal, M.A.; Azhar, E.I.; et al. Structure-Based Identification of Natural Products as SARS-CoV-2 M(pro) Antagonist from Echinacea angustifolia Using Computational Approaches. Viruses 2021, 13, 305. [Google Scholar] [CrossRef]
- Melchart, D.; Linde, K.; Fischer, P.; Kaesmayr, J. Echinacea for preventing and treating the common cold. Cochrane Database Syst. Rev. 2000, 2, CD000530. [Google Scholar] [CrossRef]
- Giles, J.T.; Palat, C.T., 3rd; Chien, S.H.; Chang, Z.G.; Kennedy, D.T. Evaluation of echinacea for treatment of the common cold. Pharmacotherapy 2000, 20, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.A.; Weber, W.; Standish, L.; Quinn, H.; Goesling, J.; McGann, M.; Calabrese, C. Efficacy and safety of echinacea in treating upper respiratory tract infections in children: A randomized controlled trial. JAMA 2003, 290, 2824–2830. [Google Scholar] [CrossRef] [PubMed]
- Riemma, G.; Schettino, M.T.; Munno, G.M.; Fasulo, D.D.; Sandullo, L.; Amabile, E.; La Verde, M.; Torella, M. Echinacea angustifolia and Echinacea purpurea Supplementation Combined with Vaginal Hyaluronic Acid to Boost the Remission of Cervical Low-Grade Squamous Intraepithelial Lesions (L-SILs): A Randomized Controlled Trial. Medicina 2022, 58, 646. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, N.; Giampaolino, P.; Lavitola, G.; Morra, I.; Formisano, C.; Nappi, C.; Bifulco, G. Effect of Immunomodulatory Supplements Based on Echinacea Angustifolia and Echinacea Purpurea on the Posttreatment Relapse Incidence of Genital Condylomatosis: A Prospective Randomized Study. Biomed. Res. Int. 2019, 2019, 3548396. [Google Scholar] [CrossRef]
- Roman, I.; Stanila, A.; Stanila, S. Bioactive compounds and antioxidant activity of Rosa canina L. biotypes from spontaneous flora of Transylvania. Chem. Cent. J. 2013, 7, 73. [Google Scholar] [CrossRef] [PubMed]
- Deliorman Orhan, D.; Hartevioglu, A.; Kupeli, E.; Yesilada, E. In vivo anti-inflammatory and antinociceptive activity of the crude extract and fractions from Rosa canina L. fruits. J. Ethnopharmacol. 2007, 112, 394–400. [Google Scholar] [CrossRef]
- Jager, A.K.; Eldeen, I.M.; van Staden, J. COX-1 and -2 activity of rose hip. Phytother. Res. 2007, 21, 1251–1252. [Google Scholar] [CrossRef]
- Winther, K.; Apel, K.; Thamsborg, G. A powder made from seeds and shells of a rose-hip subspecies (Rosa canina) reduces symptoms of knee and hip osteoarthritis: A randomized, double-blind, placebo-controlled clinical trial. Scand. J. Rheumatol. 2005, 34, 302–308. [Google Scholar] [CrossRef]
- Winther, K.; Rein, E.; Kharazmi, A. The anti-inflammatory properties of rose-hip. Inflammopharmacology 1999, 7, 63–68. [Google Scholar] [CrossRef]
- Kharazmi, A.; Winther, K. Rose hip inhibits chemotaxis and chemiluminescence of human peripheral blood neutrophils in vitro and reduces certain inflammatory parameters in vivo. Inflammopharmacology 1999, 7, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Cornara, L.; Biagi, M.; Xiao, J.; Burlando, B. Therapeutic Properties of Bioactive Compounds from Different Honeybee Products. Front. Pharmacol. 2017, 8, 412. [Google Scholar] [CrossRef] [PubMed]
- Bueno-Silva, B.; Kawamoto, D.; Ando-Suguimoto, E.S.; Casarin, R.C.V.; Alencar, S.M.; Rosalen, P.L.; Mayer, M.P.A. Brazilian red propolis effects on peritoneal macrophage activity: Nitric oxide, cell viability, pro-inflammatory cytokines and gene expression. J. Ethnopharmacol. 2017, 207, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Botezan, S.; Baci, G.M.; Bagameri, L.; Pasca, C.; Dezmirean, D.S. Current Status of the Bioactive Properties of Royal Jelly: A Comprehensive Review with a Focus on Its Anticancer, Anti-Inflammatory, and Antioxidant Effects. Molecules 2023, 28, 1510. [Google Scholar] [CrossRef]
- Honda, Y.; Araki, Y.; Hata, T.; Ichihara, K.; Ito, M.; Tanaka, M.; Honda, S. 10-Hydroxy-2-decenoic Acid, the Major Lipid Component of Royal Jelly, Extends the Lifespan of Caenorhabditis elegans through Dietary Restriction and Target of Rapamycin Signaling. J. Aging Res. 2015, 2015, 425261. [Google Scholar] [CrossRef] [PubMed]
- Terada, Y.; Narukawa, M.; Watanabe, T. Specific hydroxy fatty acids in royal jelly activate TRPA1. J. Agric. Food Chem. 2011, 59, 2627–2635. [Google Scholar] [CrossRef]
- Yoshida, M.; Hayashi, K.; Watadani, R.; Okano, Y.; Tanimura, K.; Kotoh, J.; Sasaki, D.; Matsumoto, K.; Maeda, A. Royal jelly improves hyperglycemia in obese/diabetic KK-Ay mice. J. Vet. Med. Sci. 2017, 79, 299–307. [Google Scholar] [CrossRef]
- Vajdi, M.; Musazadeh, V.; Khajeh, M.; Safaei, E.; Darzi, M.; Noshadi, N.; Bazyar, H.; Askari, G. The effects of royal jelly supplementation on anthropometric indices: A GRADE-assessed systematic review and dose-response meta-analysis of randomized controlled trials. Front. Nutr. 2023, 10, 1196258. [Google Scholar] [CrossRef] [PubMed]
- Mariani, E.; Cattini, L.; Neri, S.; Malavolta, M.; Mocchegiani, E.; Ravaglia, G.; Facchini, A. Simultaneous evaluation of circulating chemokine and cytokine profiles in elderly subjects by multiplex technology: Relationship with zinc status. Biogerontology 2006, 7, 449–459. [Google Scholar] [CrossRef]
- Prasad, A.S. Zinc in human health: Effect of zinc on immune cells. Mol. Med. 2008, 14, 353–357. [Google Scholar] [CrossRef]
- Yoon, S.Y.; Park, H.W.; Kim, H.J.; Kronbichler, A.; Koyanagi, A.; Smith, L.; Shin, J.I.; Rhee, S.Y.; Lee, S.W.; Kim, J.S.; et al. National trends in the prevalence of chronic kidney disease among Korean adults, 2007–2020. Sci. Rep. 2023, 13, 5831. [Google Scholar] [CrossRef] [PubMed]
- Cobo, G.; Lindholm, B.; Stenvinkel, P. Chronic inflammation in end-stage renal disease and dialysis. Nephrol. Dial. Transpl. 2018, 33, iii35–iii40. [Google Scholar] [CrossRef] [PubMed]
- Younis, H.A.; Nafady, M.A.; Mahmoud, M. Value of carotid intimal–medial thickness as independent predictor of endothelial dysfunction in uremic patients. Egypt. Heart J. 2011, 63, 73–78. [Google Scholar] [CrossRef][Green Version]
- Jacobs, J.J.L. Persistent SARS-2 infections contribute to long COVID-19. Med. Hypotheses 2021, 149, 110538. [Google Scholar] [CrossRef] [PubMed]
- Ninfali, P.; Mea, G.; Giorgini, S.; Rocchi, M.; Bacchiocca, M. Antioxidant capacity of vegetables, spices and dressings relevant to nutrition. Br. J. Nutr. 2005, 93, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Società Italiana di Nutrizione Umana (SINU). MINERALI—Livello Massimo Tollerabile di Assunzione (UL) e Obiettivo Nutrizionale per la Popolazione (SDT). Available online: https://sinu.it/2019/07/09/minerali-livello-massimo-tollerabile-di-assunzione-ul-e-obiettivo-nutrizionale-per-la-popolazione-sdt/ (accessed on 8 March 2024).
- Bonaventura, P.; Benedetti, G.; Albarede, F.; Miossec, P. Zinc and its role in immunity and inflammation. Autoimmun. Rev. 2015, 14, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Jarosz, M.; Olbert, M.; Wyszogrodzka, G.; Mlyniec, K.; Librowski, T. Antioxidant and anti-inflammatory effects of zinc. Zinc-dependent NF-kappaB signaling. Inflammopharmacology 2017, 25, 11–24. [Google Scholar] [CrossRef]
- Noce, A.; Bocedi, A.; Campo, M.; Marrone, G.; Di Lauro, M.; Cattani, G.; Di Daniele, N.; Romani, A. A Pilot Study of a Natural Food Supplement as New Possible Therapeutic Approach in Chronic Kidney Disease Patients. Pharmaceuticals 2020, 13, 148. [Google Scholar] [CrossRef]
- Cannell, J.J.; Grant, W.B.; Holick, M.F. Vitamin D and inflammation. Dermatoendocrinol 2014, 6, e983401. [Google Scholar] [CrossRef]
- Yin, K.; Agrawal, D.K. Vitamin D and inflammatory diseases. J. Inflamm. Res. 2014, 7, 69–87. [Google Scholar] [CrossRef]
- Roy, S.; Sherman, A.; Monari-Sparks, M.J.; Schweiker, O.; Hunter, K. Correction of Low Vitamin D Improves Fatigue: Effect of Correction of Low Vitamin D in Fatigue Study (EViDiF Study). N. Am. J. Med. Sci. 2014, 6, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Nowak, A.; Boesch, L.; Andres, E.; Battegay, E.; Hornemann, T.; Schmid, C.; Bischoff-Ferrari, H.A.; Suter, P.M.; Krayenbuehl, P.A. Effect of vitamin D3 on self-perceived fatigue: A double-blind randomized placebo-controlled trial. Medicine 2016, 95, e5353. [Google Scholar] [CrossRef] [PubMed]
- Singleton, V.L.; Orthofer, R.; Lamuela-Raventós, R.M. Analysis of total phenols and other oxidation substrates and antioxidants by means of folin-ciocalteu reagent. In Methods in Enzymology; Academic Press: London, UK, 1999; Volume 299, pp. 152–178. [Google Scholar]
- Gulcin, İ.; Alwasel, S.H. DPPH Radical Scavenging Assay. Processes 2023, 11, 2248. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hypertens. 2018, 36, 1953–2041. [Google Scholar] [CrossRef] [PubMed]
- Lohman, T.G.; Roche, F.A.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Bellizzi, V.; Scalfi, L.; Terracciano, V.; De Nicola, L.; Minutolo, R.; Marra, M.; Guida, B.; Cianciaruso, B.; Conte, G.; Di Iorio, B.R. Early changes in bioelectrical estimates of body composition in chronic kidney disease. J. Am. Soc. Nephrol. 2006, 17, 1481–1487. [Google Scholar] [CrossRef] [PubMed]
- Burholt, V.; Nash, P. Short Form 36 (SF-36) Health Survey Questionnaire: Normative data for Wales. J. Public. Health 2011, 33, 587–603. [Google Scholar] [CrossRef] [PubMed]
- Naik, H.; Shao, S.; Tran, K.C.; Wong, A.W.; Russell, J.A.; Khor, E.; Nacul, L.; McKay, R.J.; Carlsten, C.; Ryerson, C.J.; et al. Evaluating fatigue in patients recovering from COVID-19: Validation of the fatigue severity scale and single item screening questions. Health Qual. Life Outcomes 2022, 20, 170. [Google Scholar] [CrossRef] [PubMed]
- Walker, N.A.; Sunderram, J.; Zhang, P.; Lu, S.E.; Scharf, M.T. Clinical utility of the Epworth sleepiness scale. Sleep. Breath. 2020, 24, 1759–1765. [Google Scholar] [CrossRef]
- Martinez-Gonzalez, M.A.; Garcia-Arellano, A.; Toledo, E.; Salas-Salvado, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schroder, H.; Aros, F.; Gomez-Gracia, E.; et al. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | OFS | PLACEBO | p | ||
|---|---|---|---|---|---|
| T0 | T1 | T0 | T1 | ||
| Red blood cells (millions/μL) | 4.60 ± 0.41 | 4.73 ± 0.53 | 4.72 ± 0.53 | 4.61 ± 0.41 | n.s. |
| Hemoglobin (g/dL) | 13.94 ± 1.50 | 14.06 ± 1.50 | 14.03 ± 1.53 | 14.07 ± 1.51 | n.s. |
| White blood cells (thousands/μL) | 6.43 ± 1.54 | 6.50 ± 1.38 | 6.17 ± 1.52 | 6.29 ± 1.51 | n.s. |
| Platelets (thousands/μL) | 230.81 ± 56.56 | 231.19 ± 53.34 | 236.13 ± 47.58 | 234.29 ± 48.46 | n.s. |
| Neutrophils (thousands/μL) | 3.74 ± 1.29 | 3.74 ± 1.14 | 3.54 ± 1.19 | 3.50 ± 0.98 | n.s. |
| Lymphocytes (thousands/µL) | 2.06 ± 0.61 | 2.12 ± 0.72 | 2.02 ± 0.56 | 2.19 ± 0.06 | n.s. |
| Monocytes (thousands/μL) | 0.50 ± 0.18 | 0.48 ± 0.18 | 0.47 ± 0.14 | 0.45 ± 0.13 | n.s. |
| Eosinophils(thousands/μL) | 0.12 ± 0.10 | 0.13 ± 0.13 | 0.11 ± 0.10 | 0.12 ± 0.11 | n.s. |
| Creatininemia (mg/L) | 0.73 ± 0.16 | 0.76 ± 0.17 | 0.76 ± 0.18 | 0.76 ± 0.17 | n.s. |
| eGFR (mL/min/1.73 m2) | 103.49 ± 13.55 | 100.48 ± 15.27 | 100.61 ± 14.94 | 100.92 ± 15.81 | n.s. |
| Azotemia (mg/dL) | 32.71 ± 7.84 | 33.19 ± 9.17 | 32.68 ± 8.43 | 33.48 ± 10.43 | n.s. |
| Vitamin D (mg/dL) | 27.96 ± 10.25 | 34.54 ± 12.53 | 31.20 ± 10.65 | 33.98 ± 13.40 | 0.0005 |
| D-dimer (ng/mL) | 350.4 ± 80 | 335.9 ± 49 | 360.7 ± 70 | 350.1 ± 75 | n.s. |
| Ferritin (ng/mL) | 200.7 ± 80.3 | 190.3 ± 70.9 | 193.2 ± 90.1 | 210.1 ± 60.8 | n.s. |
| Serum anti-SARS-CoV-2 antibody (U/mL) | 10,304.73 ± 10,795.05 | 12,837.32 ± 15,230.70 | 10,466 ± 10,653.86 | 9762.73 ± 10,771.67 | n.s. |
| Albuminuria on urine sample morning (mg/dL) | 20.01 ± 51.53 | 25.96 ± 47.84 | 23.14 ± 43.11 | 21.27 ± 52.97 | n.s. |
| Parameters | OFS | PLACEBO | p | ||
|---|---|---|---|---|---|
| T0 | T1 | T0 | T1 | ||
| CRP (mg/L) | 2.77 ± 2.5 | 1.44 ± 1.70 | 2.15 ± 2.40 | 1.90 ± 2.52 | 0.0145 |
| ESR (mm/h) | 14.25 ± 13.16 | 11.35 ± 10.93 | 11.39 ± 9.61 | 15.55 ± 12.81 | n.s. |
| NLR | 2.08 ± 0.81 | 1.77 ± 1.03 | 1.85 ± 0.66 | 1.70 ± 0.61 | 0.0455 |
| PLR | 119.75 ± 40.27 | 121.56 ± 49.86 | 121.91 ± 21.5 | 116.31 ± 39.21 | n.s. |
| MLR | 0.26 ± 0.14 | 0.13 ± 0.05 | 0.25 ± 0.08 | 0.21 ± 0.06 | 0.0005 |
| LMR | 4.54 ± 1.43 | 4.63 ± 1.39 | 4.42 ± 1.30 | 5.01 ± 1.20 | n.s. |
| Parameters | OFS | PLACEBO | p | ||
|---|---|---|---|---|---|
| T0 | T1 | T0 | T1 | ||
| Weight (kg) | 68.25 ± 10.77 | 67.52 ± 10.70 | 67.29 ± 10.85 | 67.80 ± 11.10 | n.s. |
| Height (m) | 1.67 ± 0.09 | 1.67 ± 0.09 | 1.67 ± 0.09 | 1.67 ± 0.09 | n.s. |
| BMI (kg/m2) | 24.41 ± 3.28 | 24.15 ± 3.21 | 24.19 ± 3.43 | 30.68 ± 35.91 | n.s. |
| RZ (Ohm) | 52.94 ± 10.76 | 53.16 ± 9.81 | 53.64 ± 9.31 | 54.3 ± 9.89 | n.s. |
| RX (Ohm) | 541.03 ± 109.59 | 535.74 ± 93.10 | 545.10 ± 92.18 | 511 ± 123 | n.s. |
| PA (°) | 5.67 ± 1.00 | 5.76 ± 0.89 | 6.1 ± 2.63 | 6.02 ± 0.81 | n.s. |
| TBW% | 55.60 ± 6.00 | 55.91 ± 5.78 | 55.5 ± 5.15 | 57.3 ± 6.19 | n.s. |
| ICW% | 52.25 ± 5.20 | 52.75 ± 4.73 | 52.41 ± 3.88 | 54.24 ± 3.66 | n.s. |
| ECW% | 47.75 ± 5.20 | 47.25 ± 4.73 | 47.59 ± 3.87 | 45.76 ± 3.66 | n.s. |
| FM% | 24.69 ± 7.83 | 23.69 ± 8.14 | 24.41 ± 7.09 | 22.03 ± 8.29 | n.s. |
| FFM% | 75.30 ± 7.84 | 76.31 ± 8.14 | 75.59 ± 7.09 | 77.97 ± 8.29 | n.s. |
| BCM% | 51.61 ± 5.57 | 52.12 ± 5.07 | 51.51 ± 4.02 | 53.62 ± 4.10 | n.s. |
| BCMI (kg/m2) | 9.54 ± 2.28 | 9.63 ± 2.02 | 9.45 ± 1.74 | 10.12 ± 1.90 | n.s. |
| Parameters | OFS | PLACEBO | p | ||
|---|---|---|---|---|---|
| T0 | T1 | T0 | T1 | ||
| Systolic blood pressure (mmHg) | 120.26 ± 14.01 | 114.97 ± 12.45 | 119 ± 15.67 | 116.19 ± 13.32 | n.s. |
| Diastolic blood pressure (mmHg) | 73.16 ± 8.07 | 71.52 ± 7.96 | 73.87 ± 9.13 | 73.19 ± 9.02 | n.s. |
| Heart rate (bpm) | 67.90 ± 9.96 | 68.32 ± 9.14 | 69.29 ± 11.61 | 66.74 ± 10.30 | n.s. |
| Components | For Daily Dose (2 cp) | %VNR/2 cp |
|---|---|---|
| Zinc | 9 mg | 90% |
| Echinacea angustifolia e.s. tit. min. 4% echinacoside | 30 mg | - |
| Rosehip e.s. tit. min. 10% Vitamin C | 20 mg 14 mg | 17.5% |
| 90%—Propolis powder cryo macinate tit. min. 12.15% in galangin total flavonoids | 5.56 mg | - |
| Lyophilized royal jelly | 40 mg | - |
| Sample | Total Polyphenols for Capsule, Expressed as Gallic Acid (mg) |
|---|---|
| OFS | 43.98 |
| Sample Dilution | Anti-Radical Activity% |
|---|---|
| 1:10 | 92.15 |
| Total patients (n) | 33 |
| Sex (male/female) | 14/19 |
| Mean age (years) | 47.6 ± 16.05 |
| Time since infection (days) | 73.7 ± 35.9 |
| Duration of SARS-CoV-2 infection (days) | 12.3 ± 5.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noce, A.; Marrone, G.; Di Lauro, M.; Vita, C.; Montalto, G.; Giorgino, G.; Chiaramonte, C.; D’Agostini, C.; Bernardini, S.; Pieri, M. Potential Anti-Inflammatory and Anti-Fatigue Effects of an Oral Food Supplement in Long COVID Patients. Pharmaceuticals 2024, 17, 463. https://doi.org/10.3390/ph17040463
Noce A, Marrone G, Di Lauro M, Vita C, Montalto G, Giorgino G, Chiaramonte C, D’Agostini C, Bernardini S, Pieri M. Potential Anti-Inflammatory and Anti-Fatigue Effects of an Oral Food Supplement in Long COVID Patients. Pharmaceuticals. 2024; 17(4):463. https://doi.org/10.3390/ph17040463
Chicago/Turabian StyleNoce, Annalisa, Giulia Marrone, Manuela Di Lauro, Chiara Vita, Giulia Montalto, Gloria Giorgino, Carlo Chiaramonte, Cartesio D’Agostini, Sergio Bernardini, and Massimo Pieri. 2024. "Potential Anti-Inflammatory and Anti-Fatigue Effects of an Oral Food Supplement in Long COVID Patients" Pharmaceuticals 17, no. 4: 463. https://doi.org/10.3390/ph17040463
APA StyleNoce, A., Marrone, G., Di Lauro, M., Vita, C., Montalto, G., Giorgino, G., Chiaramonte, C., D’Agostini, C., Bernardini, S., & Pieri, M. (2024). Potential Anti-Inflammatory and Anti-Fatigue Effects of an Oral Food Supplement in Long COVID Patients. Pharmaceuticals, 17(4), 463. https://doi.org/10.3390/ph17040463