
A Scoping Review and Meta-Analysis of Anti-CGRP Monoclonal Antibodies: Predicting Response
 , , and
, , and
Abstract
1. Introduction
2. Results
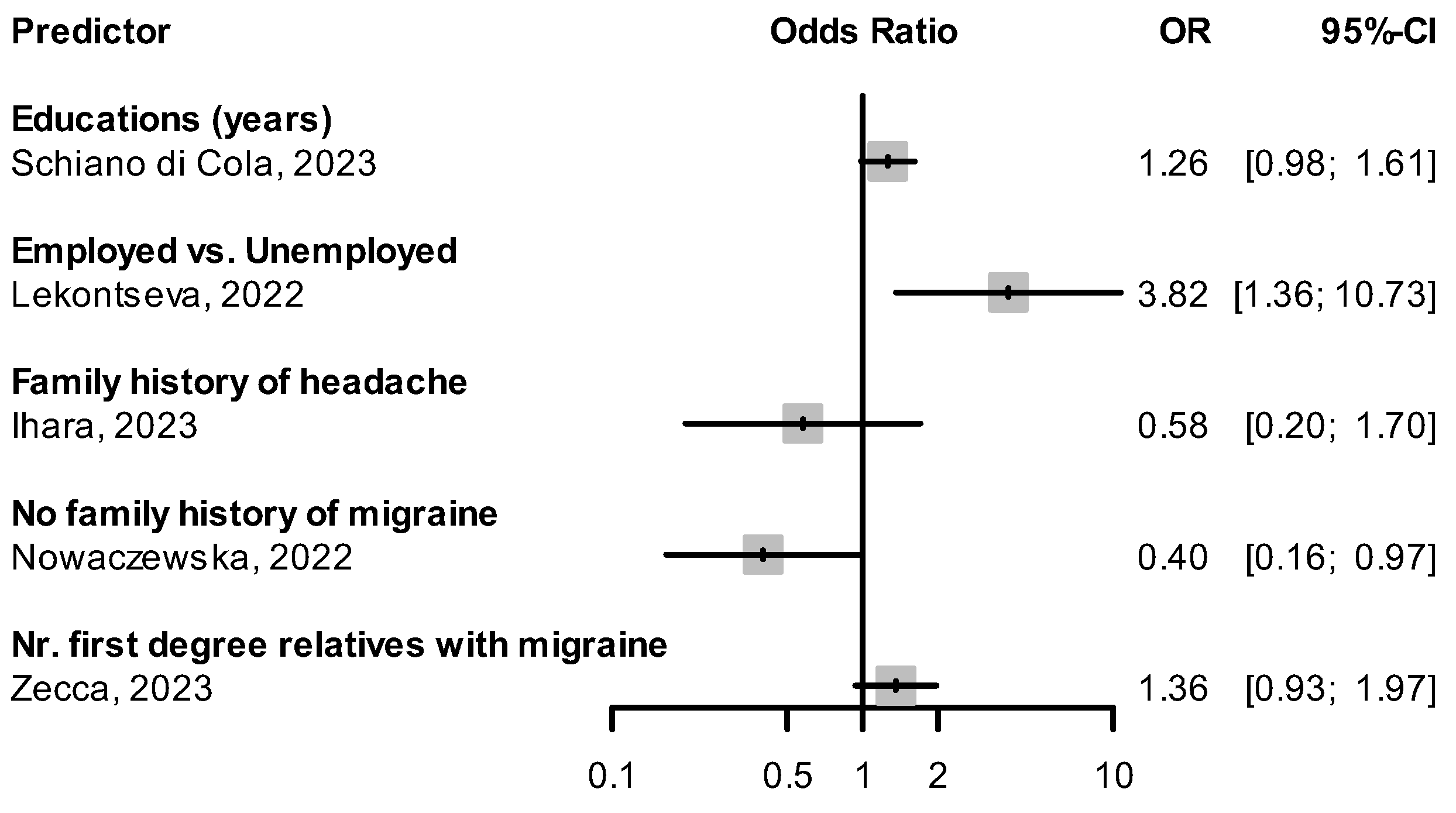
2.1. Demographic Characteristics
Weight
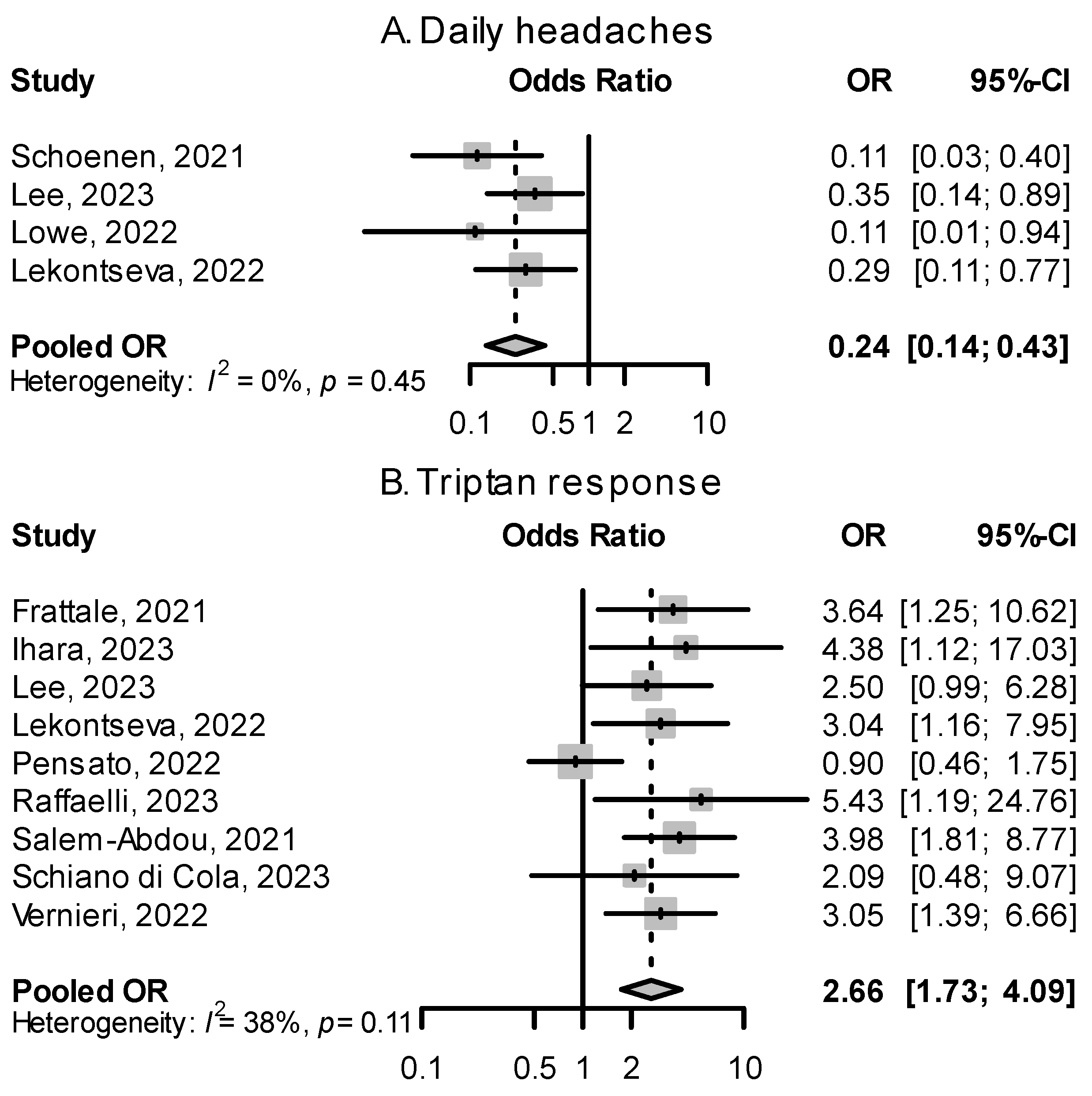
2.2. Migraine Attack Features
2.2.1. Unilateral Pain
2.2.2. Presence of Accompanying Symptoms
2.2.3. Sensitization
2.3. Migraine History
2.3.1. Continuous Chronic Migraine and Monthly Headache Days at Baseline
2.3.2. Migraine Burden at Baseline
2.3.3. Response to Triptans
2.3.4. Medication Overuse
2.3.5. Previous Preventive Treatments
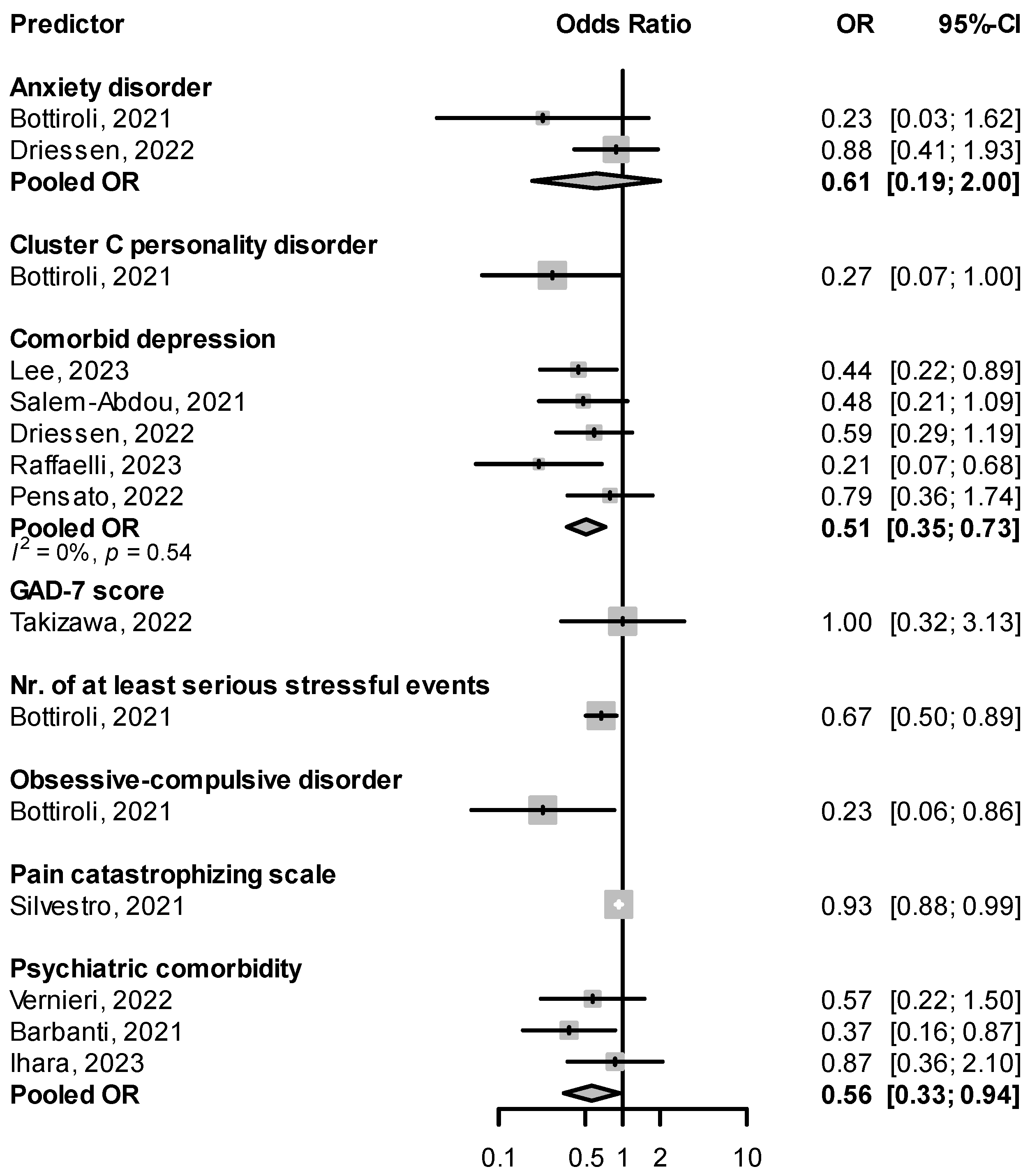
2.4. Comorbidities
2.4.1. Psychiatric Comorbidities
2.4.2. Other Comorbidities
2.5. Other Predictors
3. Discussion
4. Materials and Methods
4.1. Literature Search
4.2. Data Extraction and Synthesis
4.3. Categories of Predictive Factors
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferrari, M.D.; Goadsby, P.J.; Burstein, R.; Kurth, T.; Ayata, C.; Charles, A.; Ashina, M.; van den Maagdenberg, A.M.J.M.; Dodick, D.W. Migraine. Nat. Rev. Dis. Prim. 2022, 8, 2. [Google Scholar] [CrossRef]
- Burch, R.C.; Buse, D.C.; Lipton, R.B. Migraine. Neurol. Clin. 2019, 37, 631–649. [Google Scholar] [CrossRef] [PubMed]
- Evers, S.; Áfra, J.; Frese, A.; Goadsby, P.J.; Linde, M.; May, A.; Sándor, P.S. EFNS Guideline on the Drug Treatment of Migraine—Revised Report of an EFNS Task Force. Eur. J. Neurol. 2009, 16, 968–981. [Google Scholar] [CrossRef]
- Hepp, Z.; Bloudek, L.M.; Varon, S.F. Systematic Review of Migraine Prophylaxis Adherence and Persistence. J. Manag. Care Pharm. 2014, 20, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Goadsby, P.J.; Edvinsson, L.; Ekman, R. Vasoactive Peptide Release in the Extracerebral Circulation of Humans during Migraine Headache. Ann. Neurol. 1990, 28, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Ho, T.W.; Edvinsson, L.; Goadsby, P.J. CGRP and Its Receptors Provide New Insights into Migraine Pathophysiology. Nat. Rev. Neurol. 2010, 6, 573–582. [Google Scholar] [CrossRef]
- Edvinsson, L.; Haanes, K.A.; Warfvinge, K.; Krause, D.N. CGRP as the Target of New Migraine Therapies—Successful Translation from Bench to Clinic. Nat. Rev. Neurol. 2018, 14, 338–350. [Google Scholar] [CrossRef] [PubMed]
- Reuter, U.; Goadsby, P.J.; Lanteri-Minet, M.; Wen, S.; Hours-Zesiger, P.; Ferrari, M.D.; Klatt, J. Efficacy and Tolerability of Erenumab in Patients with Episodic Migraine in Whom Two-to-Four Previous Preventive Treatments Were Unsuccessful: A Randomised, Double-Blind, Placebo-Controlled, Phase 3b Study. Lancet 2018, 392, 2280–2287. [Google Scholar] [CrossRef]
- Mulleners, W.M.; Kim, B.-K.; Láinez, M.J.A.; Lanteri-Minet, M.; Pozo-Rosich, P.; Wang, S.; Tockhorn-Heidenreich, A.; Aurora, S.K.; Nichols, R.M.; Yunes-Medina, L.; et al. Safety and Efficacy of Galcanezumab in Patients for Whom Previous Migraine Preventive Medication from Two to Four Categories Had Failed (CONQUER): A Multicentre, Randomised, Double-Blind, Placebo-Controlled, Phase 3b Trial. Lancet Neurol. 2020, 19, 814–825. [Google Scholar] [CrossRef]
- Ferrari, M.D.; Diener, H.C.; Ning, X.; Galic, M.; Cohen, J.M.; Yang, R.; Mueller, M.; Ahn, A.H.; Schwartz, Y.C.; Grozinski-Wolff, M.; et al. Fremanezumab versus Placebo for Migraine Prevention in Patients with Documented Failure to up to Four Migraine Preventive Medication Classes (FOCUS): A Randomised, Double-Blind, Placebo-Controlled, Phase 3b Trial. Lancet 2019, 394, 1030–1040. [Google Scholar] [CrossRef]
- Dux, M.; Vogler, B.; Kuhn, A.; Mackenzie, K.D.; Stratton, J.; Messlinger, K. The Anti-CGRP Antibody Fremanezumab Lowers CGRP Release from Rat Dura Mater and Meningeal Blood Flow. Cells 2022, 11, 1768. [Google Scholar] [CrossRef]
- Edvinsson, L.; Warfvinge, K. Recognizing the Role of CGRP and CGRP Receptors in Migraine and Its Treatment. Cephalalgia 2019, 39, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Wattiez, A.-S.; Sowers, L.P.; Russo, A.F. Calcitonin Gene-Related Peptide (CGRP): Role in Migraine Pathophysiology and Therapeutic Targeting. Expert Opin. Ther. Targets 2020, 24, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Szkutnik-Fiedler, D. Pharmacokinetics, Pharmacodynamics and Drug–Drug Interactions of New Anti-Migraine Drugs—Lasmiditan, Gepants, and Calcitonin-Gene-Related Peptide (CGRP) Receptor Monoclonal Antibodies. Pharmaceutics 2020, 12, 1180. [Google Scholar] [CrossRef]
- Vandervorst, F.; Van Deun, L.; Van Dycke, A.; Paemeleire, K.; Reuter, U.; Schoenen, J.; Versijpt, J. CGRP Monoclonal Antibodies in Migraine: An Efficacy and Tolerability Comparison with Standard Prophylactic Drugs. J. Headache Pain 2021, 22, 128. [Google Scholar] [CrossRef] [PubMed]
- Mascarella, D.; Matteo, E.; Favoni, V.; Cevoli, S. The Ultimate Guide to the Anti-CGRP Monoclonal Antibodies Galaxy. Neurol. Sci. 2022, 43, 5673–5685. [Google Scholar] [CrossRef]
- Takeshima, T.; Sakai, F.; Hirata, K.; Imai, N.; Matsumori, Y.; Yoshida, R.; Peng, C.; Cheng, S.; Mikol, D.D. Erenumab Treatment for Migraine Prevention in Japanese Patients: Efficacy and Safety Results from a Phase 3, Randomized, Double-blind, Placebo-controlled Study. Headache J. Head Face Pain 2021, 61, 927–935. [Google Scholar] [CrossRef]
- Dodick, D.W.; Ashina, M.; Brandes, J.L.; Kudrow, D.; Lanteri-Minet, M.; Osipova, V.; Palmer, K.; Picard, H.; Mikol, D.D.; Lenz, R.A. ARISE: A Phase 3 Randomized Trial of Erenumab for Episodic Migraine. Cephalalgia 2018, 38, 1026–1037. [Google Scholar] [CrossRef]
- Goadsby, P.J.; Reuter, U.; Hallström, Y.; Broessner, G.; Bonner, J.H.; Zhang, F.; Sapra, S.; Picard, H.; Mikol, D.D.; Lenz, R.A. A Controlled Trial of Erenumab for Episodic Migraine. N. Engl. J. Med. 2017, 377, 2123–2132. [Google Scholar] [CrossRef]
- Tepper, S.; Ashina, M.; Reuter, U.; Brandes, J.L.; Doležil, D.; Silberstein, S.; Winner, P.; Leonardi, D.; Mikol, D.; Lenz, R. Safety and Efficacy of Erenumab for Preventive Treatment of Chronic Migraine: A Randomised, Double-Blind, Placebo-Controlled Phase 2 Trial. Lancet Neurol. 2017, 16, 425–434. [Google Scholar] [CrossRef]
- Ashina, M.; Saper, J.; Cady, R.; Schaeffler, B.A.; Biondi, D.M.; Hirman, J.; Pederson, S.; Allan, B.; Smith, J. Eptinezumab in Episodic Migraine: A Randomized, Double-Blind, Placebo-Controlled Study (PROMISE-1). Cephalalgia 2020, 40, 241–254. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B.; Goadsby, P.J.; Smith, J.; Schaeffler, B.A.; Biondi, D.M.; Hirman, J.; Pederson, S.; Allan, B.; Cady, R. Efficacy and Safety of Eptinezumab in Patients with Chronic Migraine: PROMISE-2. Neurology 2020, 94, e1365–e1377. [Google Scholar] [CrossRef]
- Stauffer, V.L.; Dodick, D.W.; Zhang, Q.; Carter, J.N.; Ailani, J.; Conley, R.R. Evaluation of Galcanezumab for the Prevention of Episodic Migraine: The EVOLVE-1 Randomized Clinical Trial. JAMA Neurol. 2018, 75, 1080. [Google Scholar] [CrossRef]
- Skljarevski, V.; Matharu, M.; Millen, B.A.; Ossipov, M.H.; Kim, B.-K.; Yang, J.Y. Efficacy and Safety of Galcanezumab for the Prevention of Episodic Migraine: Results of the EVOLVE-2 Phase 3 Randomized Controlled Clinical Trial. Cephalalgia 2018, 38, 1442–1454. [Google Scholar] [CrossRef]
- Silberstein, S.D.; Dodick, D.W.; Bigal, M.E.; Yeung, P.P.; Goadsby, P.J.; Blankenbiller, T.; Grozinski-Wolff, M.; Yang, R.; Ma, Y.; Aycardi, E. Fremanezumab for the Preventive Treatment of Chronic Migraine. N. Engl. J. Med. 2017, 377, 2113–2122. [Google Scholar] [CrossRef]
- Dodick, D.W.; Silberstein, S.D.; Bigal, M.E.; Yeung, P.P.; Goadsby, P.J.; Blankenbiller, T.; Grozinski-Wolff, M.; Yang, R.; Ma, Y.; Aycardi, E. Effect of Fremanezumab Compared with Placebo for Prevention of Episodic Migraine: A Randomized Clinical Trial. JAMA 2018, 319, 1999. [Google Scholar] [CrossRef] [PubMed]
- Raffaelli, B.; De Icco, R.; Corrado, M.; Terhart, M.; Ailani, J. Open-Label Trials for CGRP-Targeted Drugs in Migraine Prevention: A Narrative Review. Cephalalgia 2023, 43, 033310242211370. [Google Scholar] [CrossRef]
- Ashina, M.; Goadsby, P.J.; Reuter, U.; Silberstein, S.; Dodick, D.; Rippon, G.A.; Klatt, J.; Xue, F.; Chia, V.; Zhang, F.; et al. Long-Term Safety and Tolerability of Erenumab: Three-plus Year Results from a Five-Year Open-Label Extension Study in Episodic Migraine. Cephalalgia 2019, 39, 1455–1464. [Google Scholar] [CrossRef] [PubMed]
- Reuter, U.; Lucas, C.; Dolezil, D.; Hand, A.L.; Port, M.D.; Nichols, R.M.; Stroud, C.; Tockhorn-Heidenreich, A.; Detke, H.C. Galcanezumab in Patients with Multiple Previous Migraine Preventive Medication Category Failures: Results from the Open-Label Period of the CONQUER Trial. Adv. Ther. 2021, 38, 5465–5483. [Google Scholar] [CrossRef]
- Pozo-Rosich, P.; Detke, H.C.; Wang, S.; Doležil, D.; Li, L.Q.; Aurora, S.K.; Reuter, U. Long-Term Treatment with Galcanezumab in Patients with Chronic Migraine: Results from the Open-Label Extension of the REGAIN Study. Curr. Med. Res. Opin. 2022, 38, 731–742. [Google Scholar] [CrossRef]
- Hirata, K.; Takeshima, T.; Imai, N.; Igarashi, H.; Shiosakai, M.; Inage, M.; Sakurai, F.; Ning, X.; Nakai, M.; Koga, N. A Multicenter, Open-Label, Phase 3 Study to Evaluate the Safety of Fremanezumab for Migraine, Subcutaneously Self-Administered with an Auto-Injection Device at Institutional Sites and at Home. Expert Opin. Drug Saf. 2022, 1–8, Advance online publication. [Google Scholar] [CrossRef] [PubMed]
- Sakai, F.; Suzuki, N.; Ning, X.; Ishida, M.; Usuki, C.; Iba, K.; Isogai, Y.; Koga, N. Long-Term Safety and Tolerability of Fremanezumab for Migraine Preventive Treatment in Japanese Outpatients: A Multicenter, Randomized, Open-Label Study. Drug Saf. 2021, 44, 1355–1364. [Google Scholar] [CrossRef] [PubMed]
- Murray, A.M.; Stern, J.I.; Robertson, C.E.; Chiang, C.-C. Real-World Patient Experience of CGRP-Targeting Therapy for Migraine: A Narrative Review. Curr. Pain Headache Rep. 2022, 26, 783–794. [Google Scholar] [CrossRef]
- Pavlovic, J.M.; Paemeleire, K.; Göbel, H.; Bonner, J.; Rapoport, A.; Kagan, R.; Zhang, F.; Picard, H.; Mikol, D.D. Efficacy and Safety of Erenumab in Women with a History of Menstrual Migraine. J. Headache Pain 2020, 21, 95. [Google Scholar] [CrossRef] [PubMed]
- Silvestro, M.; Orologio, I.; Bonavita, S.; Scotto Di Clemente, F.; Fasano, C.; Tessitore, A.; Tedeschi, G.; Russo, A. Effectiveness and Safety of CGRP-MAbs in Menstrual-Related Migraine: A Real-World Experience. Pain Ther. 2021, 10, 1203–1214. [Google Scholar] [CrossRef]
- Ornello, R.; Frattale, I.; Caponnetto, V.; De Matteis, E.; Pistoia, F.; Sacco, S. Menstrual Headache in Women with Chronic Migraine Treated with Erenumab: An Observational Case Series. Brain Sci. 2021, 11, 370. [Google Scholar] [CrossRef]
- Cullum, C.K.; Do, T.P.; Ashina, M.; Bendtsen, L.; Hugger, S.S.; Iljazi, A.; Gusatovic, J.; Snellman, J.; Lopez-Lopez, C.; Ashina, H.; et al. Real-World Long-Term Efficacy and Safety of Erenumab in Adults with Chronic Migraine: A 52-Week, Single-Center, Prospective, Observational Study. J. Headache Pain 2022, 23, 61. [Google Scholar] [CrossRef]
- Ornello, R.; Baraldi, C.; Guerzoni, S.; Lambru, G.; Andreou, A.P.; Raffaelli, B.; Gendolla, A.; Barbanti, P.; Aurilia, C.; Egeo, G.; et al. Comparing the Relative and Absolute Effect of Erenumab: Is a 50% Response Enough? Results from the ESTEEMen Study. J. Headache Pain 2022, 23, 38. [Google Scholar] [CrossRef]
- Overeem, L.H.; Lange, K.S.; Fitzek, M.P.; Siebert, A.; Steinicke, M.; Triller, P.; Hong, J.B.; Reuter, U.; Raffaelli, B. Effect of Switching to Erenumab in Non-Responders to a CGRP Ligand Antibody Treatment in Migraine: A Real-World Cohort Study. Front. Neurol. 2023, 14, 1154420. [Google Scholar] [CrossRef]
- Briceño-Casado, M.D.P.; Gil-Sierra, M.D.; De-La-Calle-Riaguas, B. Switching of Monoclonal Antibodies against Calcitonin Gene-Related Peptide in Chronic Migraine in Clinical Practice: A Case Series. Eur. J. Hosp. Pharm. 2023, 30, e19. [Google Scholar] [CrossRef]
- Alpuente, A.; Gallardo, V.J.; Asskour, L.; Caronna, E.; Torres-Ferrus, M.; Pozo-Rosich, P. Salivary CGRP and Erenumab Treatment Response: Towards Precision Medicine in Migraine. Ann. Neurol. 2022, 92, 846–859. [Google Scholar] [CrossRef] [PubMed]
- Nowaczewska, M.; Straburzyński, M.; Waliszewska-Prosół, M.; Meder, G.; Janiak-Kiszka, J.; Kaźmierczak, W. Cerebral Blood Flow and Other Predictors of Responsiveness to Erenumab and Fremanezumab in Migraine—A Real-Life Study. Front. Neurol. 2022, 13, 895476. [Google Scholar] [CrossRef] [PubMed]
- Ashina, S.; Melo-Carrillo, A.; Szabo, E.; Borsook, D.; Burstein, R. Pre-Treatment Non-Ictal Cephalic Allodynia Identifies Responders to Prophylactic Treatment of Chronic and Episodic Migraine Patients with Galcanezumab: A Prospective Quantitative Sensory Testing Study (NCT04271202). Cephalalgia 2023, 43, 033310242211478. [Google Scholar] [CrossRef] [PubMed]
- Peng, K.-P.; Basedau, H.; Oppermann, T.; May, A. Trigeminal Sensory Modulatory Effects of Galcanezumab and Clinical Response Prediction. Pain 2022, 163, 2194–2199. [Google Scholar] [CrossRef]
- Bottiroli, S.; De Icco, R.; Vaghi, G.; Pazzi, S.; Guaschino, E.; Allena, M.; Ghiotto, N.; Martinelli, D.; Tassorelli, C.; Sances, G. Psychological Predictors of Negative Treatment Outcome with Erenumab in Chronic Migraine: Data from an Open Label Long-Term Prospective Study. J. Headache Pain 2021, 22, 114. [Google Scholar] [CrossRef] [PubMed]
- Lovati, C.; Bernasconi, G.; Capogrosso, C.; Molteni, L.; Giorgetti, F.; Dell’Osso, B.; Pantoni, L. Personality Traits and Efficacy of Anti-CGRP Monoclonal Antibodies in Migraine Prevention. Neurol. Sci. 2022, 43, 5765–5767. [Google Scholar] [CrossRef] [PubMed]
- Driessen, M.T.; Cohen, J.M.; Patterson-Lomba, O.; Thompson, S.F.; Seminerio, M.; Carr, K.; Totev, T.I.; Sun, R.; Yim, E.; Mu, F.; et al. Real-World Effectiveness of Fremanezumab in Migraine Patients Initiating Treatment in the United States: Results from a Retrospective Chart Study. J. Headache Pain 2022, 23, 47. [Google Scholar] [CrossRef]
- Vernieri, F.; Altamura, C.; Brunelli, N.; Costa, C.M.; Aurilia, C.; Egeo, G.; Fofi, L.; Favoni, V.; Lovati, C.; Bertuzzo, D.; et al. Rapid Response to Galcanezumab and Predictive Factors in Chronic Migraine Patients: A 3-month Observational, Longitudinal, Cohort, Multicenter, Italian Real-life Study. Eur. J. Neurol. 2022, 29, 1198–1208. [Google Scholar] [CrossRef]
- Russo, A.; Silvestro, M.; Scotto di Clemente, F.; Trojsi, F.; Bisecco, A.; Bonavita, S.; Tessitore, A.; Tedeschi, G. Multidimensional Assessment of the Effects of Erenumab in Chronic Migraine Patients with Previous Unsuccessful Preventive Treatments: A Comprehensive Real-World Experience. J. Headache Pain 2020, 21, 69. [Google Scholar] [CrossRef]
- Iannone, L.F.; Fattori, D.; Benemei, S.; Chiarugi, A.; Geppetti, P.; De Cesaris, F. Long-Term Effectiveness of Three Anti-CGRP Monoclonal Antibodies in Resistant Chronic Migraine Patients Based on the MIDAS Score. CNS Drugs 2022, 36, 191–202. [Google Scholar] [CrossRef]
- Barbanti, P.; Egeo, G.; Aurilia, C.; Altamura, C.; d’Onofrio, F.; Finocchi, C.; Albanese, M.; Aguggia, M.; Rao, R.; Zucco, M.; et al. Predictors of Response to Anti-CGRP Monoclonal Antibodies: A 24-Week, Multicenter, Prospective Study on 864 Migraine Patients. J. Headache Pain 2022, 23, 138. [Google Scholar] [CrossRef] [PubMed]
- Frattale, I.; Caponnetto, V.; Casalena, A.; Assetta, M.; Maddestra, M.; Marzoli, F.; Affaitati, G.; Giamberardino, M.A.; Viola, S.; Gabriele, A.; et al. Association between Response to Triptans and Response to Erenumab: Real-Life Data. J. Headache Pain 2021, 22, 1. [Google Scholar] [CrossRef] [PubMed]
- Schoenen, J.; Timmermans, G.; Nonis, R.; Manise, M.; Fumal, A.; Gérard, P. Erenumab for Migraine Prevention in a 1-Year Compassionate Use Program: Efficacy, Tolerability, and Differences Between Clinical Phenotypes. Front. Neurol. 2021, 12, 805334. [Google Scholar] [CrossRef] [PubMed]
- Caronna, E.; Gallardo, V.J.; Alpuente, A.; Torres-Ferrus, M.; Pozo-Rosich, P. Anti-CGRP Monoclonal Antibodies in Chronic Migraine with Medication Overuse: Real-Life Effectiveness and Predictors of Response at 6 Months. J. Headache Pain 2021, 22, 120. [Google Scholar] [CrossRef]
- Raffaelli, B.; Fitzek, M.; Overeem, L.H.; Storch, E.; Terhart, M.; Reuter, U. Clinical Evaluation of Super-Responders vs. Non-Responders to CGRP(-Receptor) Monoclonal Antibodies: A Real-World Experience. J. Headache Pain 2023, 24, 16. [Google Scholar] [CrossRef]
- Ihara, K.; Ohtani, S.; Watanabe, N.; Takahashi, N.; Miyazaki, N.; Ishizuchi, K.; Hori, S.; Takemura, R.; Nakahara, J.; Takizawa, T. Predicting Response to CGRP-Monoclonal Antibodies in Patients with Migraine in Japan: A Single-Centre Retrospective Observational Study. J. Headache Pain 2023, 24, 23. [Google Scholar] [CrossRef]
- Zecca, C.; Cargnin, S.; Schankin, C.; Giannantoni, N.M.; Viana, M.; Maraffi, I.; Riccitelli, G.C.; Sihabdeen, S.; Terrazzino, S.; Gobbi, C. Clinic and Genetic Predictors in Response to Erenumab. Eur. J. Neurol. 2022, 29, 1209–1217. [Google Scholar] [CrossRef]
- Silvestro, M.; Tessitore, A.; Scotto di Clemente, F.; Battista, G.; Tedeschi, G.; Russo, A. Refractory Migraine Profile in CGRP-monoclonal Antibodies Scenario. Acta Neurol. Scand. 2021, 144, 325–333. [Google Scholar] [CrossRef]
- Schiano di Cola, F.; Bolchini, M.; Ceccardi, G.; Caratozzolo, S.; Liberini, P.; Rao, R.; Padovani, A. An Observational Study on Monoclonal Antibodies against Calcitonin-gene-related Peptide and Its Receptor. Eur. J. Neurol. 2023, 30, 1764–1773. [Google Scholar] [CrossRef]
- Lee, H.C.; Cho, S.; Kim, B.-K. Predictors of Response to Galcanezumab in Patients with Chronic Migraine: A Real-World Prospective Observational Study. Neurol. Sci. 2023, 44, 2455–2463. [Google Scholar] [CrossRef]
- Lowe, M.; Murray, L.; Tyagi, A.; Gorrie, G.; Miller, S.; Dani, K. The NHS Greater Glasgow and Clyde Headache Service Efficacy of Erenumab and Factors Predicting Response after 3 Months in Treatment Resistant Chronic Migraine: A Clinical Service Evaluation. J. Headache Pain 2022, 23, 86. [Google Scholar] [CrossRef] [PubMed]
- Lekontseva, O.; Wang, M.; Amoozegar, F. Predictors of Clinical Response to Erenumab in Patients with Migraine. Cephalalgia Rep. 2022, 5, 251581632211281. [Google Scholar] [CrossRef]
- Kwon, S.; Gil, Y.-E.; Lee, M.J. Real-World Efficacy of Galcanezumab for the Treatment of Migraine in Korean Patients. Cephalalgia 2022, 42, 705–714. [Google Scholar] [CrossRef] [PubMed]
- Vernieri, F.; Brunelli, N.; Marcosano, M.; Aurilia, C.; Egeo, G.; Lovati, C.; Favoni, V.; Perrotta, A.; Maestrini, I.; Rao, R.; et al. Maintenance of Response and Predictive Factors of 1-year GalcanezumAb Treatment in Real-life Migraine Patients in Italy: The Multicenter Prospective Cohort GARLIT Study. Eur. J. Neurol. 2023, 30, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Baraldi, C.; Castro, F.L.; Cainazzo, M.M.; Pani, L.; Guerzoni, S. Predictors of Response to Erenumab after 12 Months of Treatment. Brain Behav. 2021, 11, e22600. [Google Scholar] [CrossRef] [PubMed]
- Salem-Abdou, H.; Simonyan, D.; Puymirat, J. Identification of Predictors of Response to Erenumab in a Cohort of Patients with Migraine. Cephalalgia Rep. 2021, 4, 251581632110266. [Google Scholar] [CrossRef]
- Torres-Ferrús, M.; Gallardo, V.J.; Alpuente, A.; Caronna, E.; Gine-Cipres, E.; Pozo-Rosich, P. The Impact of Anti-CGRP Monoclonal Antibodies in Resistant Migraine Patients: A Real-World Evidence Observational Study. J. Neurol. 2021, 268, 3789–3798. [Google Scholar] [CrossRef]
- Pensato, U.; Baraldi, C.; Favoni, V.; Cainazzo, M.M.; Torelli, P.; Querzani, P.; Pascazio, A.; Mascarella, D.; Matteo, E.; Quintana, S.; et al. Real-Life Assessment of Erenumab in Refractory Chronic Migraine with Medication Overuse Headache. Neurol. Sci. 2022, 43, 1273–1280. [Google Scholar] [CrossRef] [PubMed]
- Argyriou, A.A.; Dermitzakis, E.V.; Xiromerisiou, G.; Rallis, D.; Soldatos, P.; Litsardopoulos, P.; Vikelis, M. Efficacy and Safety of Fremanezumab for Migraine Prophylaxis in Patients with at Least Three Previous Preventive Failures: Prospective, Multicenter, Real-world Data from a Greek Registry. Eur. J. Neurol. 2023, 30, 1435–1442. [Google Scholar] [CrossRef] [PubMed]
- Ornello, R.; Baraldi, C.; Guerzoni, S.; Lambru, G.; Fuccaro, M.; Raffaelli, B.; Gendolla, A.; Barbanti, P.; Aurilia, C.; Cevoli, S.; et al. Gender Differences in 3-Month Outcomes of Erenumab Treatment—Study on Efficacy and Safety of Treatment with Erenumab in Men. Front. Neurol. 2021, 12, 774341. [Google Scholar] [CrossRef] [PubMed]
- Cetta, I.; Messina, R.; Zanandrea, L.; Colombo, B.; Filippi, M. Comparison of Efficacy and Safety of Erenumab between over and under 65-Year-Old Refractory Migraine Patients: A Pivotal Study. Neurol. Sci. 2022, 43, 5769–5771. [Google Scholar] [CrossRef]
- Guerzoni, S.; Baraldi, C.; Brovia, D.; Cainazzo, M.M.; Lo Castro, F.; Pani, L. Monoclonal Anti-CGRP Antibodies in Post-Menopausal Women: A Real-Life Study. Acta Neurol. Belg. 2023, 123, 1039–1047. [Google Scholar] [CrossRef]
- Cheng, S.; Jenkins, B.; Limberg, N.; Hutton, E. Erenumab in Chronic Migraine: An Australian Experience. Headache J. Head Face Pain 2020, 60, 2555–2562. [Google Scholar] [CrossRef] [PubMed]
- Barbanti, P.; Aurilia, C.; Cevoli, S.; Egeo, G.; Fofi, L.; Messina, R.; Salerno, A.; Torelli, P.; Albanese, M.; Carnevale, A.; et al. Long-term (48 Weeks) Effectiveness, Safety, and Tolerability of Erenumab in the Prevention of High-frequency Episodic and Chronic Migraine in a Real World: Results of the EARLY 2 Study. Headache J. Head Face Pain 2021, 61, 1351–1363. [Google Scholar] [CrossRef]
- Ornello, R.; Casalena, A.; Frattale, I.; Gabriele, A.; Affaitati, G.; Giamberardino, M.A.; Assetta, M.; Maddestra, M.; Marzoli, F.; Viola, S.; et al. Real-Life Data on the Efficacy and Safety of Erenumab in the Abruzzo Region, Central Italy. J. Headache Pain 2020, 21, 32. [Google Scholar] [CrossRef] [PubMed]
- De Matteis, E.; Caponnetto, V.; Casalena, A.; Frattale, I.; Gabriele, A.; Affaitati, G.; Giamberardino, M.A.; Maddestra, M.; Viola, S.; Pistoia, F.; et al. Cranial Autonomic Symptoms and Response to Monoclonal Antibodies Targeting the Calcitonin Gene-Related Peptide Pathway: A Real-World Study. Front. Neurol. 2022, 13, 973226. [Google Scholar] [CrossRef] [PubMed]
- De Vries Lentsch, S.; Garrelds, I.M.; Danser, A.H.J.; Terwindt, G.M.; MaassenVanDenBrink, A. Serum CGRP in Migraine Patients Using Erenumab as Preventive Treatment. J. Headache Pain 2022, 23, 120. [Google Scholar] [CrossRef] [PubMed]
- Takizawa, T.; Ohtani, S.; Watanabe, N.; Miyazaki, N.; Ishizuchi, K.; Sekiguchi, K.; Iba, C.; Shibata, M.; Takemura, R.; Hori, S.; et al. Real-World Evidence of Galcanezumab for Migraine Treatment in Japan: A Retrospective Analysis. BMC Neurol. 2022, 22, 512. [Google Scholar] [CrossRef]
- Sarchielli, P.; Pini, L.; Zanchin, G.; Alberti, A.; Maggioni, F.; Rossi, C.; Floridi, A.; Calabresi, P. Clinical-Biochemical Correlates of Migraine Attacks in Rizatriptan Responders and Non-Responders. Cephalalgia 2006, 26, 257–265. [Google Scholar] [CrossRef]
- Buse, D.C.; Silberstein, S.D.; Manack, A.N.; Papapetropoulos, S.; Lipton, R.B. Psychiatric Comorbidities of Episodic and Chronic Migraine. J. Neurol. 2013, 260, 1960–1969. [Google Scholar] [CrossRef]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. SCID-5-CV: Structured Clinical Interview for DSM-5 Disorders: Clinician Version; American Psychiatric Association Publishing: Arlington, VA, USA, 2016; ISBN 978-1-58562-461-4. [Google Scholar]
- Iani, L.; Lauriola, M.; Costantini, M. A Confirmatory Bifactor Analysis of the Hospital Anxiety and Depression Scale in an Italian Community Sample. Health Qual. Life Outcomes 2014, 12, 84. [Google Scholar] [CrossRef]
- Bottiroli, S.; Galli, F.; Viana, M.; Sances, G.; Tassorelli, C. Traumatic Experiences, Stressful Events, and Alexithymia in Chronic Migraine with Medication Overuse. Front. Psychol. 2018, 9, 704. [Google Scholar] [CrossRef]
- Seo, J.-G.; Park, S.-P. Validation of the Patient Health Questionnaire-9 (PHQ-9) and PHQ-2 in Patients with Migraine. J. Headache Pain 2015, 16, 65. [Google Scholar] [CrossRef]
- Seo, J.-G.; Park, S.-P. Validation of the Generalized Anxiety Disorder-7 (GAD-7) and GAD-2 in Patients with Migraine. J. Headache Pain 2015, 16, 97. [Google Scholar] [CrossRef]
- Krueger, R.F.; Derringer, J.; Markon, K.E.; Watson, D.; Skodol, A.E. Personality Inventory for DSM-5 (PID-5). APA PsycTests 2012. [Google Scholar] [CrossRef]
- Arnold, M. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd Edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Ailani, J.; Kaiser, E.A.; Mathew, P.G.; McAllister, P.; Russo, A.F.; Vélez, C.; Ramajo, A.P.; Abdrabboh, A.; Xu, C.; Rasmussen, S.; et al. Role of Calcitonin Gene-Related Peptide on the Gastrointestinal Symptoms of Migraine—Clinical Considerations: A Narrative Review. Neurology 2022, 99, 841–853. [Google Scholar] [CrossRef] [PubMed]
- Mason, B.N.; Wattiez, A.-S.; Balcziak, L.K.; Kuburas, A.; Kutschke, W.J.; Russo, A.F. Vascular Actions of Peripheral CGRP in Migraine-like Photophobia in Mice. Cephalalgia 2020, 40, 1585–1604. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Jakubowski, M.; Rauch, S.D. The Science of Migraine. J. Vestib. Res. 2011, 21, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Dodick, D.; Silberstein, S. Central Sensitization Theory of Migraine: Clinical Implications. Headache J. Head Face Pain 2006, 46, S182–S191. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Collins, B.; Jakubowski, M. Defeating Migraine Pain with Triptans: A Race against the Development of Cutaneous Allodynia. Ann. Neurol. 2004, 55, 19–26. [Google Scholar] [CrossRef]
- May, A.; Schulte, L.H. Chronic Migraine: Risk Factors, Mechanisms and Treatment. Nat. Rev. Neurol. 2016, 12, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Ashina, S.; Serrano, D.; Lipton, R.B.; Maizels, M.; Manack, A.N.; Turkel, C.C.; Reed, M.L.; Buse, D.C. Depression and Risk of Transformation of Episodic to Chronic Migraine. J. Headache Pain 2012, 13, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B.; Fanning, K.M.; Serrano, D.; Reed, M.L.; Cady, R.; Buse, D.C. Ineffective Acute Treatment of Episodic Migraine Is Associated with New-Onset Chronic Migraine. Neurology 2015, 84, 688–695. [Google Scholar] [CrossRef]
- Recober, A.; Goadsby, P.J. Calcitonin Gene-Related Peptide: A Molecular Link between Obesity and Migraine? Drug News Perspect. 2010, 23, 112. [Google Scholar] [CrossRef] [PubMed]
- Bigal, M.E.; Lipton, R.B.; Holland, P.R.; Goadsby, P.J. Obesity, Migraine, and Chronic Migraine: Possible Mechanisms of Interaction. Neurology 2007, 68, 1851–1861. [Google Scholar] [CrossRef]
- Martin, V.; Nagy, A.J.; Janelidze, M.; Giorgadze, G.; Hirman, J.; Cady, R.; Mehta, L.; Buse, D.C. Impact of Baseline Characteristics on the Efficacy and Safety of Eptinezumab in Patients with Migraine: Subgroup Analyses of PROMISE-1 and PROMISE-2. Clin. Ther. 2022, 44, 389–402. [Google Scholar] [CrossRef]
- Förderreuther, S.; Zhang, Q.; Stauffer, V.L.; Aurora, S.K.; Láinez, M.J.A. Preventive Effects of Galcanezumab in Adult Patients with Episodic or Chronic Migraine Are Persistent: Data from the Phase 3, Randomized, Double-Blind, Placebo-Controlled EVOLVE-1, EVOLVE-2, and REGAIN Studies. J. Headache Pain 2018, 19, 121. [Google Scholar] [CrossRef]
- Spierings, E.L.H.; Kärppä, M.; Ning, X.; Cohen, J.M.; Campos, V.R.; Yang, R.; Reuter, U. Efficacy and Safety of Fremanezumab in Patients with Migraine and Inadequate Response to Prior Preventive Treatment: Subgroup Analyses by Country of a Randomized, Placebo-Controlled Trial. J. Headache Pain 2021, 22, 26. [Google Scholar] [CrossRef]
- Nundy, S.; Kakar, A.; Bhutta, Z.A. Systematic, Scoping and Narrative Reviews. In How to Practice Academic Medicine and Publish from Developing Countries? Springer Nature Singapore: Singapore, 2022; pp. 277–281. ISBN 9789811652479. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- R Core Team R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023.
- Posit team RStudio: Integrated Development Environment for R; Posit Software, PBC: Boston, MA, USA, 2022.
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to Perform a Meta-Analysis with R: A Practical Tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Harrer, M.; Cuijpers, P.; Furukawa, T.; Ebert, D.D. Dmetar: Companion R Package for The Guide “Doing Meta-Analysis in R”; 2019. R package version 0.1.0. Available online: http://dmetar.protectlab.org/ (accessed on 22 June 2023).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, J.B.; Lange, K.S.; Overeem, L.H.; Triller, P.; Raffaelli, B.; Reuter, U. A Scoping Review and Meta-Analysis of Anti-CGRP Monoclonal Antibodies: Predicting Response. Pharmaceuticals 2023, 16, 934. https://doi.org/10.3390/ph16070934
Hong JB, Lange KS, Overeem LH, Triller P, Raffaelli B, Reuter U. A Scoping Review and Meta-Analysis of Anti-CGRP Monoclonal Antibodies: Predicting Response. Pharmaceuticals. 2023; 16(7):934. https://doi.org/10.3390/ph16070934
Chicago/Turabian StyleHong, Ja Bin, Kristin Sophie Lange, Lucas Hendrik Overeem, Paul Triller, Bianca Raffaelli, and Uwe Reuter. 2023. "A Scoping Review and Meta-Analysis of Anti-CGRP Monoclonal Antibodies: Predicting Response" Pharmaceuticals 16, no. 7: 934. https://doi.org/10.3390/ph16070934
APA StyleHong, J. B., Lange, K. S., Overeem, L. H., Triller, P., Raffaelli, B., & Reuter, U. (2023). A Scoping Review and Meta-Analysis of Anti-CGRP Monoclonal Antibodies: Predicting Response. Pharmaceuticals, 16(7), 934. https://doi.org/10.3390/ph16070934