Abstract
Acute exacerbations of chronic obstructive pulmonary disease (COPD) with severe hyperglycemia may require insulin to lower glucose levels in people with coexisting type 2 diabetes (T2D) and COPD. We conducted this study to examine the risk of hospitalization for COPD, pneumonia, ventilator use, lung cancer, hypoglycemia, and mortality with and without insulin use in people with T2D and COPD. We adopted propensity-score-matching to identify 2370 paired insulin users and non-users from Taiwan’s National Health Insurance Research Database between 1 January 2000 and 31 December 2018. Cox proportional hazards models and the Kaplan–Meier method were utilized to compare the risk of outcomes between study and control groups. The mean follow-up for insulin users and non-users was 6.65 and 6.37 years. Compared with no insulin use, insulin use was associated with a significantly increased risk of hospitalization for COPD (aHR 1.7), bacterial pneumonia (aHR 2.42), non-invasive positive pressure ventilation (aHR 5.05), invasive mechanical ventilation (aHR 2.72), and severe hypoglycemia (aHR 4.71), but with no significant difference in the risk of death. This nationwide cohort study showed that patients with T2D and COPD requiring insulin therapy may have an increased risk of acute COPD exacerbations, pneumonia, ventilator use, and severe hypoglycemia without a significant increase in the risk of death.
1. Introduction
Genetic factors, early-life events, infections, smoking, and environmental pollutants are the risk factors for developing chronic obstructive pulmonary disease (COPD) [1,2,3]. These factors can lead to lung damage or remodeling of the airways, pulmonary parenchyma, and vasculature, resulting in progressive airway limitation, dyspnea, exercise intolerance, restricted daily activity, and premature mortality [1,2]. Unstable COPD or infections can lead to episodic acute exacerbations. Each exacerbation contributes to pulmonary function deterioration and patient suffering [1,4,5]. The number of people with COPD worldwide has increased from 142 million to 212 million (33%) between 1999 and 2019 [6]. COPD is also the third leading cause of death worldwide [1,2]. COPD is usually associated with cardiovascular diseases and type 2 diabetes (T2D), possibly due to shared risk factors (aging, physical inactivity, and smoking) [1,2,5,7]. The frequent use of corticosteroids and low-grade systemic inflammation in people with COPD also predispose them to T2D. People with COPD have elevated levels of plasma CRP and nuclear factor-κB (NF-κB) activation, which can attenuate the suppression of hepatic glucose production by insulin and can induce insulin resistance in peripheral tissues. Pulmonary inflammation can spill over into systemic inflammation and adversely influence systemic glucose homeostasis by reducing the recruitment of skeletal muscle capillaries that deliver glucose and insulin to muscle cells, to increase blood glucose levels [1,7,8,9]. Approximately 16% of patients with COPD have T2D, and T2D can worsen the prognosis of COPD [1,7,8,10]. However, there is little research and progress on treating comorbid T2D and COPD [1,2,7].
Insulin was discovered in 1921 and has been in use to treat and save many people with type 1 diabetes (T1D), with little or no insulin production [11]. It also is the most powerful glucose-lowering medicine in adult persons with T2D [12]. Insulin is indicated for patients with severe hyperglycemia (random glucose >300 mg/dL), symptomatic diabetes, ketoacidosis, acute medical events, concomitant diseases, admission, and inability to take oral antidiabetic drugs [12]. Randomized prospective studies have shown that insulin effectively lowers blood glucose and reduces microvascular complications [13,14]. One report indicates that insulin has potential anti-inflammatory, anti-oxidant, and anti-apoptotic effects [15]. Patients with cystic fibrosis have less insulin secretion and are more likely to have diabetes and require insulin therapy. They often have poorer nutrition, greater catabolism and a higher risk of infection. This can have a negative impact on the function of their lungs and their chances of survival [16]. COPD often coexists with other comorbidities and can lead to acute exacerbations requiring urgent care [4,5]. Currently, there are no guidelines for managing diabetes mellitus in persons with T2D and COPD. The recommendation for antidiabetic treatment in these patients is in accordance with the guidelines for the management of diabetes mellitus [7,17]. Patients with acute exacerbations of COPD can be treated with oral antidiabetic agents or glucagon-like peptide-1 agonist if their blood glucose levels are not very high. However, if they have severe hyperglycemia, acute symptoms or require hospitalization, they may need insulin or follow inpatient diabetes management guidelines [18]. They can, therefore, be treated initially with long-acting insulin analogues because they are more stable, have a longer lasting effect and have a lower risk of glucose fluctuations and hypoglycemia than neutral protamine Hagedorn insulin and premixed insulin [17]. Rapid-acting insulin analogues can then be added as needed, as they can rapidly lower blood glucose levels with less risk of postprandial hypoglycemia than regular short-acting insulin [17]. Combined with tight titration of insulin doses and blood glucose monitoring, insulin treatment can be a safe and effective antidiabetic management strategy in persons with COPD and high blood glucose levels [7,18]. Both T2D and COPD are metabolic disorders. Insulin is a drug candidate for treating severe hyperglycemia in people with T2D and COPD. However, no research has studied the long-term results of using insulin in these patients [7,8,9]. Therefore, we conducted this cohort study to compare the outcomes of all-cause mortality, hospitalization for COPD, bacterial pneumonia, ventilator use, lung cancer, and severe hypoglycemia in people with coexisting T2D and COPD with or without receiving insulin therapy.
2. Results
2.1. Participants
From the 1 January 2000 until the 31 December 2018, we identified 28,399 insulin users and 25,592 nonusers among persons with coexisting T2D and COPD. After excluding unsuitable patients, there were 3490 insulin users and 5667 nonusers. Finally, we identified 2370 insulin users and 2370 nonusers through 1:1 matching of the propensity scores (Figure 1).
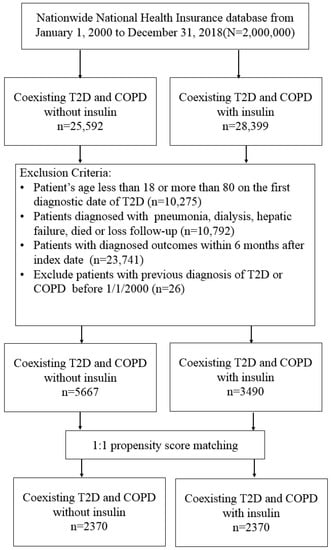
Figure 1.
Patient selection flowchart.
The basic characteristics, comorbidities, and medication were well matched between the study group and the control group with SMD values <0.1 (Table 1). In the comparison cohorts of the insulin users and nonusers, the male proportion was 62.45% and 62.28%, respectively; the mean (SD) age was 61.02 (11.11) and 60.73 (11.21) years, respectively; the mean follow-up time was 6.65 (4.34) and 6.37 (4.29) years in each case.

Table 1.
Comparison of variables in patients with coexisting T2D and COPD with and without insulin use.
2.2. Main Outcomes
In the cohorts that were matched, 357 (15.06%) insulin users and 326 (13.76%) insulin non-users died during the follow-up period (incidence rate: 22.28 versus 21.45 per 1000 person-years). Multivariable analysis showed that the adjusted HR (aHR) for insulin users vs. non-users was 1.08 (95% CI = 0.93–1.26, p = 0.3076; Table 2). However, compared with nonusers, insulin users had a significantly higher risk of hospitalization for COPD (aHR 1.7, 95% CI 1.24–2.32), bacterial pneumonia (aHR 2.42, 95% CI 1.95–3), NIPPV (aHR 5.05, 95% CI 2.76–9.22), IMV (aHR 2.72, 95% CI 1.99–3.72), and severe hypoglycemia (aHR 4.71, 95% CI 2.5–8.89).
Table 2.
Hazard ratio (HR) and 95% confidence interval (CI) for the disease outcome in patients with T2D and COPD.
The cumulative incidence of hospitalization for COPD (Log-rank test p-value < 0.001), bacterial pneumonia (Log-rank test p-value < 0.001), and IMV (Log-rank test p-value < 0.001) were significantly higher in insulin users than in non-users (Figure 2).
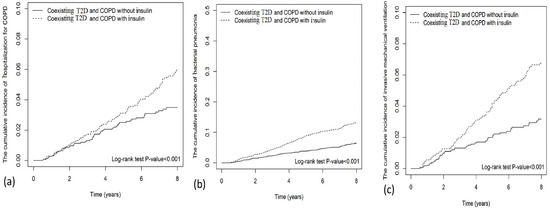
Figure 2.
Cumulative incidence of (a) hospitalization for COPD, (b) bacterial pneumonia, and (c) invasive mechanical ventilation (IMV) between insulin use and no-use.
2.3. Dose-Response Analysis
The cumulative duration (<90, 90–179, >179 days) of insulin use had significantly increased risks of hospitalization for COPD, bacterial pneumonia, and IMV than insulin no-use, and longer cumulative insulin use appeared to increase the risk of these outcomes (Table 3).
Table 3.
The risk of outcomes in patients with a cumulative duration of insulin use or with no insulin use.
3. Discussion
This nationwide cohort study demonstrated that patients with coexisting T2D and COPD requiring insulin therapy might increase the risk of hospitalization for COPD, bacterial pneumonia, ventilation use, and severe hypoglycemia; however, it did not increase the risk of death. Longer cumulative insulin use had association with increased risk of hospitalization for COPD, bacterial pneumonia, and invasive mechanical ventilation than insulin no-use.
Acute attacks of COPD often require hospitalization and can lead to respiratory failure or death [1,2,19]. The goal of COPD treatment is to reduce acute exacerbations of COPD [1,4,5]. One report showed that insulin sensitizers such as metformin may reduce the risk of severe COPD exacerbations [20]. Hyperglycemia tends to impair pulmonary function and increase the risk of acute COPD attacks [7,8,10]. Although insulin is the most effective glucose-lowering drug, our study showed that it might increase the risk of hospitalization for COPD. Insulin treatment has a direct effect on the lungs by inducing prostaglandin-mediated contraction of airway smooth muscle [21]. Insulin-like growth factor-1 (IGF-1) appears to play an important role in lung disease, but circulating IGF-1 has been reported to be associated with a lower risk of airway hyperresponsiveness [22]. Using insulin is likely to cause hypoglycemia and weight gain [8,23]. Prolonged use of insulin can lead to hyperinsulinemia, downregulation of insulin signaling and insulin resistance, which can increase glucose levels and oxidative stress. The downregulated insulin signaling leads to an imbalance in the anabolic activity of insulin, favoring protein synthesis and suppressing autophagy. The latter promotes cell senescence by inhibiting autophagic protein and lipid degradation and turnover [24]. All these factors can worsen lung function and exacerbate COPD.
Patients with COPD may exhibit alteration of the airway microbiome and impaired airway immune response, thus increasing susceptibility to bacterial infections [1,3,19]. Hyperglycemia tends to increase the permeability and spread of bacteria through the airways [8,25]. Diabetes mellitus is associated with a higher risk of bacterial pneumonia due to impaired cellular immunity [7,10]. We have previously shown that thiazolidinediones may increase the risk of developing bacterial pneumonia in people with COPD [26]. This study also found that insulin may increase the risk of bacterial pneumonia in people with T2D and COPD. The reason for this result is unclear. However, previous research has shown that hyperinsulinemia or insulin resistance can increase proinflammatory cytokines, predispose patients to inflammation, and impair immune function, thus increasing infection risk [23].
Hypoxia or respiratory failure can be a medical emergency in patients receiving COPD treatment [1] and often requires noninvasive ventilation to improve the patient’s condition [2,4,19]. Intubation with invasive mechanical ventilation can be a life-saving procedure in patients with persistent hypercapnia [4]. This study showed that the use of insulin was associated with a higher risk of both NIPPV and IMV in people with COPD, and longer cumulative insulin use was associated with further increased risk of these outcomes. The use of insulin in patients with coexisting COPD and T2D may require attention to the possibility of respiratory failure.
Smoking is the main cause of lung cancer [1,27,28,29]. Both COPD and T2D are risk factors for lung cancer [1,8,19]. A meta-analysis has shown that metformin may reduce the risk of lung cancer development [30]. Insulin can promote cell proliferation and mediate a mitogenic effect as binding to the insulin receptor. Insulin receptors can also bind to the insulin-like growth factor with potential oncogenic effects [31]. However, this finding has not been proved in large, long-term randomized controlled insulin trials [32]. Our study showed that insulin was associated with a non-significantly increased risk of lung cancer (aHR 2.11, 95%CI 0.99–4.49) in people with T2D and COPD. Insulin therapy in patients with COPD may need close monitoring for the occurrence of lung cancers.
Almost all studies on insulin therapy demonstrate the side effect of hypoglycemia [12,13,14]. Previous study has shown that about 37% of patients receiving insulin therapy developed hypoglycemia, and about 2.3% of patients with T2D had severe hypoglycemia annually [14]. Hypoglycemia can cause symptoms of cold sweating, palpitation, dyspnea, and general weakness. Kasirye et al. showed that hypoglycemia resulted in more severe acute exacerbation in patients with COPD [33]. Our research revealed that insulin use in patients with coexisting T2D and COPD could increase the risk of severe hypoglycemia. Dyspnea, weakness, acute exacerbation of COPD, and ventilation use could be attributed to severe hypoglycemia in patients on insulin therapy in this study. Elliot P Joslin stated, “Insulin is a remedy primarily for the wise and not for the foolish, be they patients or doctors… to use insulin successfully requires more brains” in 1928 [34]. Insulin therapy requires effective doctor-patient communication and careful monitoring for hypoglycemia.
COPD has been the third leading cause of death worldwide for years [1,4]. Diabetes mellitus can increase the severity of COPD and the risk of death [1,7,10]. Therefore, people with coexisting T2D and COPD are at high risk of death. Previous study has shown that metformin may have an effect on the risk of death in these patients [35]. Empagliflozin has been shown to have consistent benefits on cardiopulmonary and mortality outcomes in patients with T2D and COPD [36]. Our study showed that although insulin use might increase the risk of severe hypoglycemia, bacterial pneumonia, and ventilation use, it might not increase the risk of death in patients with T2D and COPD. Insulin studies tend to recruit patients with a longer duration of diabetes or more severe cases with a higher mortality rate. However, it is possible that this condition is not prominent in this study.
This study had several advantages. First, this was a nationwide population-based study. As 99% of Taiwan’s 23 million people are covered by National Health Insurance, the patients enrolled in the study had less selection bias. Second, the study had a large sample size and an observational period of 18 years, which allowed for subgroup analysis and assessment of outcomes that took years to develop. Third, although this was only an observational study, no known randomized insulin studies have been conducted in patients with COPD recently, and the possibility of other randomized studies on insulin use in patients with COPD is low in the future [1,7,8,9]. Therefore, this real-world data may fill some knowledge gaps in the clinical care of patients with T2D and COPD.
Our study had a number of limitations. First, national health administrative data lacked complete information on family history, individual lifestyle, smoking, and alcohol consumption, which could have influenced the findings of our study. In any case, we had well-matched baseline characteristics (all SMD values <0.1) and tried to reduce the difference between the study and control groups. Second, this administrative database lacked results of hemoglobin A1C levels, biochemical tests, pulmonary function tests, and imaging methods, which precluded accurate evaluation of T2D and COPD severity. However, we utilized DCSI scores, antidiabetics, and cardiovascular medications as representative factors to assess T2D status and the clinical records of moderate and severe COPD exacerbations to assess COPD severity. Third, patients on insulin therapy often exhibit a long duration of T2D, suboptimal glycemic control, and more comorbidities. Although we considered these factors, unknown residual confounders could bias the results. Fourth, the participants in this study were mainly of Taiwanese descent; therefore, the results may not be applicable to other racial groups. Finally, in a retrospective cohort study, there are always unobserved confounders. Therefore, there is a need for randomized control trials to confirm our findings.
4. Materials and Methods
4.1. Data Source and Population of the Study
We identified patients from the Taiwan’s National Health Insurance Research Database (NHIRD), which was described in our previous study [25]. About 450 hospitals and over 10,000 clinics across Taiwan participate in the National Health Insurance program. The Health Insurance Authority conducts random inspections of all medical institutions annually to ensure the diagnostic accuracy and quality of care. The NHIRD has a link to the National Death Registry to confirm the diagnosis of death. The Declaration of Helsinki was followed for all methods used in this study. The China Medical University and Hospital Research Ethics Committee (CMUH104-REC2-115-CR4) approved this study. To prevent data leakage, detailed patient and provider information was encrypted and de-identified before release. The research ethics committee granted a waiver of informed consent.
4.2. Study Design
We identified persons with coexisting T2D and COPD from the NHIRD between 1 January 2000 and 31 December 2018, and followed them until 31 December 2019 (Figure 1). T2D and COPD were diagnosed with the ICD-9/10-CM codes for at least two outpatient visits or one admission in 1 year (Supplementary Table S1). Previous studies validated the ICD coding algorithms to define T2D and COPD with acceptable accuracy [37,38]. A moderate exacerbation of COPD was determined by the use of medication (systemic corticosteroids or antibiotics) and treatment in the outpatient claims; severe COPD exacerbations were defined as an acute attack treated at the emergency room (ER) or hospitalization [39]. Exclusion criteria were (1) age <18 or >80 years; (2) missing data of age or sex; (3) diagnosis of T1D, bacterial pneumonia, liver failure, or on dialysis; (4) hospitalization for COPD, bacterial pneumonia, ventilation use, or lung cancer, or death within 180 days of the index date to exclude latent morbidity; and (5) diagnosis of T2D or COPD prior to 1 January 2000 for the exclusion of prevalent disease.
4.3. Procedures
We defined the day of simultaneous diagnosis of T2D and COPD as the comorbid date (Figure 3). In our database, there are 49,837 people from the diagnosis of T2D to T2D and COPD, 51,596 people from the diagnosis of COPD to COPD and T2D. Patients who received insulin treatment after the comorbid date were defined as insulin users, whereas those who never received insulin treatment during the study period were defined as insulin non-users. The index date was defined as the first date of insulin use after the comorbid date. The index date of insulin non-user was considered to be the same period of time from the comorbid date to the index date of the insulin user. We assessed and matched the following variates that could interfere with the results: sex, age, obesity (the diagnoses of obesity, overweight, or severe obesity), smoking, comorbidities (hypertension, coronary artery disease, dyslipidemia, chronic kidney disease, atrial fibrillation, liver cirrhosis, and peripheral artery disease diagnosed one year before the index date), and medications (respiratory drugs, oral antidiabetics, antihypertensives, statins, and aspirin). Charlson Comorbidity Index (CCI) was assessed as a proxy for disease burden [40]. The Diabetes Complication Severity Index (DCSI) score [41] was used to assess complications of T2D; the occurrence of moderate or severe COPD exacerbations was used to assess COPD severity.
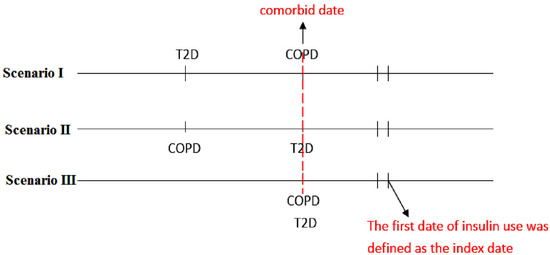
Figure 3.
The scenarios of comorbid type 2 diabetes and COPD.
4.4. The Outcomes of Interest
The outcomes of interest in this study were all-cause mortality (the diagnosis of mortality was confirmed with the linkage to the National Death Registry), hospitalization for COPD, bacterial pneumonia, invasive mechanical ventilation (IMV), noninvasive positive pressure ventilation (NIPPV), lung cancers, and severe hypoglycemia (hypoglycemia requiring an emergency room visit or hospitalization). To calculate the outcomes, we followed patients until the date of death, respective outcomes, or at the end of follow-up on 31 December 2019, whichever came first.
4.5. Statistical Analyses
We used the Kelsey method and adopted the two-sided significance level of 95%, power of 80%, ratio of sample size between unexposed/exposed of 1, percentage of unexposed with outcome of 5%, and odds ratio of 1.5 to estimate the required exposed and unexposed sample size of 1690 and 1690, respectively [42]. Propensity score matching has been used for adjustment and comparability between insulin users and non-users [43]. We selected 32 clinically related variables as independent variates (including age, gender, comorbidities, DCSI and CCI scores, COPD exacerbation, and medications; Table 1) and insulin use as a dependent variable to estimate each patient’s propensity score using non-parsimonious multivariable logistic regression. The nearest neighbor algorithm has been used for the construction of matched pairs, and a standardized mean difference (SMD) <0.1 was considered a negligible difference between the study group and the control groups. Using the propensity score matching method, a total of 2370 pairs of insulin users and non-users were identified.
Chi-squared tests were used to determine statistical differences in categorical variables, and Student’s t-tests were used to determine statistical differences in continuous variables and between the study and control groups. To examine outcomes between insulin users and non-users, Cox proportional hazards models with multivariable adjustment were used. Results are presented as hazard ratios (HRs) and 95% confidence intervals (CIs). The Kaplan–Meier method and the log-rank test were used to compare the cumulative incidence of hospitalization for COPD, bacterial pneumonia, and invasive mechanical ventilation between insulin use and non-use. We have also compared the cumulative duration (<90, 90–179, >179 days) of insulin use and the risks of hospitalization for COPD, bacterial pneumonia, and invasive mechanical ventilation with insulin non-use. The cumulative duration of insulin was calculated by adding up from the index day to the end day of insulin use during the follow-up time.
Statistical significance was defined as a two-sided p-value of less than 0.05. Analyses of this study were performed using SAS (version 9.4; SAS Institute, Cary, NC, USA).
5. Conclusions
Patients with coexisting T2D and COPD require integrated, patient-centered, and multidisciplinary care. Pitifully, research on treatment strategies is scarce. Insulin may be indicated in diabetic patients with acute exacerbation of COPD to lower blood glucose. Our study has shown that patients with coexisting T2D and COPD requiring insulin therapy was associated with a higher risk of hypoglycemia, hospitalization for COPD, bacterial pneumonia, and ventilator use. However, we should be aware that this could be the result of the patients’ intrinsic severe metabolic decompensation, which led to the previous administration of insulin. Insulin administration requires effective doctor–patient communication for careful monitoring of hypoglycemia, pneumonia, acute exacerbation of COPD, and respiratory failure with immediate and appropriate disposal.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ph16050643/s1, Table S1: Diseases and related ICD-9-CM, ICD-10-CM codes.
Author Contributions
Conceptualization, F.-S.Y., C.-M.H., S.-H.C. and J.C.-C.W.; methodology, F.-S.Y. and Y.-H.S.; software, S.-H.C. and Y.-H.S.; validation, S.-H.C., C.-M.H. and Y.-H.S.; formal analysis, Y.-H.S.; investigation, F.-S.Y., J.C.-C.W. and Y.-H.S.; resources, Y.-H.S., S.-H.C. and J.C.-C.W.; data curation, C.-M.H.; writing—original draft preparation, F.-S.Y., S.-H.C. and C.-M.H.; writing—review and editing, F.-S.Y., J.C.-C.W. and Y.-H.S.; visualization, S.-H.C. and Y.-H.S.; supervision, C.-M.H.; project administration, Y.-H.S., J.C.-C.W. and C.-M.H.; funding acquisition, J.C.-C.W. and C.-M.H. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported in part by the Ministry of Health and Welfare Clinical Trial Center, Taiwan (MOHW109-TDU-B-212-114004), MOST Clinical Trial Consortium for Stroke, Taiwan (MOST 108-2321-B-039-003-), and Tseng-Lien Lin Foundation, Taichung, Taiwan. These funding agencies did not influence the study design, data collection, and analysis; decision to publish; or preparation of the manuscript. The writing or preparation of this paper was not funded by any organization; the data analyses were not undertaken by individuals who are employees of funders, or any author who received funding from funders; and no writing support was provided by the funders. The corresponding authors had complete access to all data in the study and were responsible for the decision to submit this manuscript for publication.
Institutional Review Board Statement
All methods of this study were performed in accordance with the Declaration of Helsinki. This research was approved by the Research Ethics Committee of China Medical University and Hospital (CMUH104-REC2-115-CR4).
Informed Consent Statement
The detailed information of patients and health care providers was scrambled and de-identified before release to prevent data leaks. Informed consent was waived by the Research Ethics Committee.
Data Availability Statement
Data of this study are available from the National Health Insurance Research Database (NHIRD) published by Taiwan National Health Insurance (NHI) Administration. The data utilized in this study cannot be made available in the paper, the Supplemental Files, or in a public repository due to the “Personal Information Protection Act” executed by Taiwan government starting from 2012. Requests for data can be sent as a formal proposal to the NHIRD Office (https://dep.mohw.gov.tw/DOS/cp-2516-3591-113.html, accessed on 24 October 2022) or by email to stsung@mohw.gov.tw.
Acknowledgments
We thank the Health Data Science Center of China Medical University Hospital for providing funding, administrative, and technical support.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
COPD: Chronic obstructive pulmonary disease; T2D: type 2 diabetes mellitus; CAD: coronary artery disease; NIPPV: noninvasive positive pressure ventilation; IMV: invasive mechanical ventilation.
References
- Stolz, D.; Mkorombindo, T.; Schumann, D.M.; Agusti, A.; Ash, S.Y.; Bafadhel, M.; Bai, C.; Chalmers, J.D.; Criner, G.J.; Dharmage, S.C.; et al. Towards the elimination of chronic obstructive pulmonary disease: A Lancet commission. Lancet 2022, 400, 921–972. [Google Scholar] [CrossRef] [PubMed]
- Christenson, S.A.; Smith, B.M.; Bafadhel, M.; Putcha, N. Chronic obstructive pulmonary disease. Lancet 2022, 399, 2227–2242. [Google Scholar] [CrossRef] [PubMed]
- Agustí, A.; Hogg, J.C. Update on the pathogenesis of chronic obstructive pulmonary disease. N. Engl. J. Med. 2019, 381, 1248–1256. [Google Scholar] [CrossRef] [PubMed]
- Celli, B.R.; Wedzicha, J.A. Update on clinical aspects of chronic obstructive pulmonary disease. N. Engl. J. Med. 2019, 381, 1257–1266. [Google Scholar] [CrossRef]
- Wedzicha, J.A.; Seemungal, T.A. COPD exacerbations: Defining their cause and prevention. Lancet 2007, 370, 786–796. [Google Scholar] [CrossRef]
- GBD. Institute for Health Metrics and Evaluation, Global Health Data Exchange, Global Burden of Disease Study 2019 (GBD 2019) Data Resources, GBD Results Tool, Terms and Conditions (2019). Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 9 September 2022).
- Gläser, S.; Krüger, S.; Merkel, M.; Bramlage, P.; Herth, F.J. Chronic obstructive pulmonary disease and diabetes mellitus: A systematic review of the literature. Respiration 2015, 89, 253–264. [Google Scholar] [CrossRef]
- Mirrakhimov, A.E. Chronic obstructive pulmonary disease and glucose metabolism: A bitter sweet symphony. Cardiovasc. Diabetol. 2012, 11, 132. [Google Scholar] [CrossRef]
- Park, S.S.; Perez Perez, J.L.; Perez Gandara, B.; Agudelo, C.W.; Rodriguez Ortega, R.; Ahmed, H.; Garcia-Arcos, I.; McCarthy, C.; Geraghty, P. Mechanisms Linking COPD to Type 1 and 2 Diabetes Mellitus: Is There a Relationship between Diabetes and COPD? Medicina 2022, 58, 1030. [Google Scholar] [CrossRef]
- Gunasekaran, K.; Murthi, S.; Elango, K.; Rahi, M.S.; Thilagar, B.; Ramalingam, S.; Voruganti, D.; Paramasivam, V.K.; Kolandaivel, K.P.; Arora, A.; et al. The Impact of Diabetes Mellitus in Patients with Chronic Obstructive Pulmonary Disease (COPD) Hospitalization. J. Clin. Med. 2021, 10, 235. [Google Scholar] [CrossRef]
- Hegele, R.A.; Maltman, G.M. Insulin’s centenary: The birth of an idea. Lancet Diabetes Endocrinol. 2020, 8, 971–977. [Google Scholar] [CrossRef]
- Cahn, A.; Miccoli, R.; Dardano, A.; Del Prato, S. New forms of insulin and insulin therapies for the treatment of type 2 diabetes. Lancet Diabetes Endocrinol. 2015, 3, 638–652. [Google Scholar] [CrossRef] [PubMed]
- Ohkubo, Y.; Kishikawa, H.; Araki, E.; Miyata, T.; Isami, S.; Motoyoshi, S.; Kojima, Y.; Furuyoshi, N.; Shichiri, M. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: A randomized prospective 6-year study. Diabetes Res. Clin. Pract. 1995, 28, 103–117. [Google Scholar] [CrossRef] [PubMed]
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998, 352, 837–853, Erratum in Lancet 1999, 354, 602. [Google Scholar] [CrossRef]
- Dandona, P.; Chaudhuri, A.; Mohanty, P.; Ghanim, H. Anti-inflammatory effects of insulin. Curr. Opin. Clin. Nutr. Metab. Care 2007, 10, 511–517, Erratum in Curr. Opin. Clin. Nutr. Metab. Care 2007, 10, 660. [Google Scholar] [CrossRef]
- Moran, A.; Brunzell, C.; Cohen, R.C.; Katz, M.; Marshall, B.C.; Onady, G.; Robinson, K.A.; Sabadosa, K.A.; Stecenko, A.; Slovis, B.; et al. Clinical care guidelines for cystic fibrosis-related diabetes: A position statement of the American Diabetes Association and a clinical practice guideline of the Cystic Fibrosis Foundation, endorsed by the Pediatric Endocrine Society. Diabetes Care 2010, 33, 2697–2708. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S125–S143. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 16. Diabetes Care in the Hospital: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S244–S253. [Google Scholar] [CrossRef]
- Rabe, K.F.; Watz, H. Chronic obstructive pulmonary disease. Lancet 2017, 389, 1931–1940. [Google Scholar] [CrossRef]
- Wang, M.T.; Lai, J.H.; Huang, Y.L.; Kuo, F.C.; Wang, Y.H.; Tsai, C.L.; Tu, M.Y. Use of antidiabetic medications and risk of chronic obstructive pulmonary disease exacerbation requiring hospitalization: A disease risk score-matched nested case-control study. Respir. Res. 2020, 21, 319. [Google Scholar] [CrossRef]
- Dandona, P.; Mohanty, P.; Chaudhuri, A.; Garg, R.; Aljada, A. Insulin infusion in acute illness. J. Clin. Investig. 2005, 115, 2069–2072. [Google Scholar] [CrossRef]
- Jiang, S.; Xu, Z.; Shi, Y.; Liang, S.; Jiang, X.; Xiao, M.; Wang, K.; Ding, L. Circulating insulin-like growth factor-1 and risk of lung diseases: A Mendelian randomization analysis. Front. Endocrinol. 2023, 14, 1126397. [Google Scholar] [CrossRef] [PubMed]
- Herman, M.E.; O’Keefe, J.H.; Bell, D.S.H.; Schwartz, S.S. Insulin therapy increases cardiovascular risk in Type 2 diabetes. Prog. Cardiovasc. Dis. 2017, 60, 422–434. [Google Scholar] [CrossRef]
- Kolb, H.; Kempf, K.; Röhling, M.; Martin, S. Insulin: Too much of a good thing is bad. BMC Med. 2020, 18, 224. [Google Scholar] [CrossRef]
- Yen, F.S.; Wei, J.C.; Yang, Y.C.; Hsu, C.C.; Hwu, C.M. Thiazolidinedione use in individuals with Type 2 diabetes and chronic obstructive pulmonary disease. Front. Med. 2021, 8, 729518. [Google Scholar] [CrossRef]
- Hecht, S.S. Tobacco smoke carcinogens and lung cancer. J. Natl. Cancer Inst. 1999, 91, 1194–1210. [Google Scholar] [CrossRef] [PubMed]
- Sasco, A.J.; Secretan, M.B.; Straif, K. Tobacco smoking and cancer: A brief review of recent epidemiological evidence. Lung Cancer 2004, 45, S3–S9. [Google Scholar] [CrossRef]
- Aredo, J.V.; Luo, S.J.; Gardner, R.M.; Sanyal, N.; Choi, E.; Hickey, T.P.; Riley, T.L.; Huang, W.Y.; Kurian, A.W.; Leung, A.N.; et al. Tobacco Smoking and Risk of Second Primary Lung Cancer. J. Thorac. Oncol. 2021, 16, 968–979. [Google Scholar] [CrossRef] [PubMed]
- Philips, B.J.; Meguer, J.X.; Redman, J.; Baker, E.H. Factors determining the appearance of glucose in upper and lower respiratory tract secretions. Intensive Care Med. 2003, 29, 2204–2210. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, Y.; Gong, Y.I.; He, J.; Chen, X. Metformin and lung cancer risk of patients with type 2 diabetes mellitus: A meta-analysis. Biomed. Rep. 2015, 3, 235–241. [Google Scholar] [CrossRef]
- Bowker, S.L.; Majumdar, S.R.; Veugelers, P.; Johnson, J.A. Increased cancer-related mortality for patients with type 2 diabetes who use sulfonylureas or insulin. Diabetes Care 2006, 29, 254–258. [Google Scholar] [CrossRef]
- ORIGIN Trial Investigators; Gerstein, H.C.; Bosch, J.; Dagenais, G.R.; Díaz, R.; Jung, H.; Maggioni, A.P.; Pogue, J.; Probstfield, J.; Ramachandran, A.; et al. Basal insulin and cardiovascular and other outcomes in dysglycemia. N. Engl. J. Med. 2012, 367, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Kasirye, Y.; Simpson, M.; Mamillapalli, C.K.; Epperla, N.; Liang, H.; Yale, S.H. Association between blood glucose level and outcomes in patients hospitalized for acute exacerbation of chronic obstructive pulmonary disease. WMJ 2013, 112, 244–249, quiz 250. [Google Scholar] [PubMed]
- Joslin, E.P. The Treatment of Diabetes Mellitus, 4th ed.; Lea & Febiger: Philadelphia, PA, USA, 1928. [Google Scholar]
- Yen, F.S.; Chen, W.; Wei, J.C.; Hsu, C.C.; Hwu, C.M. Effects of metformin use on total mortality in patients with type 2 diabetes and chronic obstructive pulmonary disease: A matched-subject design. PLoS ONE 2018, 13, e0204859. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Sander, L.E.; Fitchett, D.H.; Zinman, B.; Pernille, O.A.; Wanner, C.; Vedin, O.; Lauer, S.; Verma, S.; Yaggi, H.K.; et al. Empagliflozin in patients with type 2 diabetes mellitus and chronic obstructive pulmonary disease. Diabetes Res. Clin. Pract. 2022, 186, 109837. [Google Scholar] [CrossRef]
- Lin, C.C.; Lai, M.S.; Syu, C.Y.; Chang, S.C.; Tseng, F.Y. Accuracy of diabetes diagnosis in health insurance claims data in Taiwan. J. Formos. Med. Assoc. 2005, 104, 157–163. [Google Scholar] [PubMed]
- Ho, T.W.; Ruan, S.Y.; Huang, C.T.; Tsai, Y.J.; Lai, F.; Yu, C.J. Validity of ICD9-CM codes to diagnose chronic obstructive pulmonary disease from National Health Insurance claim data in Taiwan. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 3055–3063. [Google Scholar] [CrossRef]
- Rodriguez-Roisin, R. Towards a consensus definition for COPD exacerbations. Chest 2000, 117, 398S–401S. [Google Scholar] [CrossRef]
- Meduru, P.; Helmer, D.; Rajan, M.; Tseng, C.L.; Pogach, L.; Sambamoorthi, U. Chronic illness with complexity: Implications for performance measurement of optimal glycemic control. J. Gen. Intern. Med. 2007, 22, 408–418. [Google Scholar] [CrossRef]
- Young, B.A.; Lin, E.; Von Korff, M.; Simon, G.; Ciechanowski, P.; Ludman, E.J.; Everson-Stewart, S.; Kinder, L.; Oliver, M.; Boyko, E.J.; et al. Diabetes complications severity index and risk of mortality, hospitalization, and health care utilization. Am. J. Manag. Care 2008, 14, 15–23. [Google Scholar]
- Kelsey, J.L.; Whittemore, A.S.; Evans, A.S.; Thompson, W.D. Methods in Observational Epidemiology, 2nd ed.; Tables 12–15; Oxford University Press: Oxford, UK, 1996. [Google Scholar]
- D’Agostino, R.B., Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).