
Benzydamine—An Affordable Over-the-Counter Drug with Psychoactive Properties—From Chemical Structure to Possible Pharmacological Properties


 and
and
Abstract
1. Introduction
1.1. The Therapeutic Effects of Benzydamine
1.2. The Side Effects of Benzydamine
2. Benzydamine-Proven and Potential Pharmacological Effects
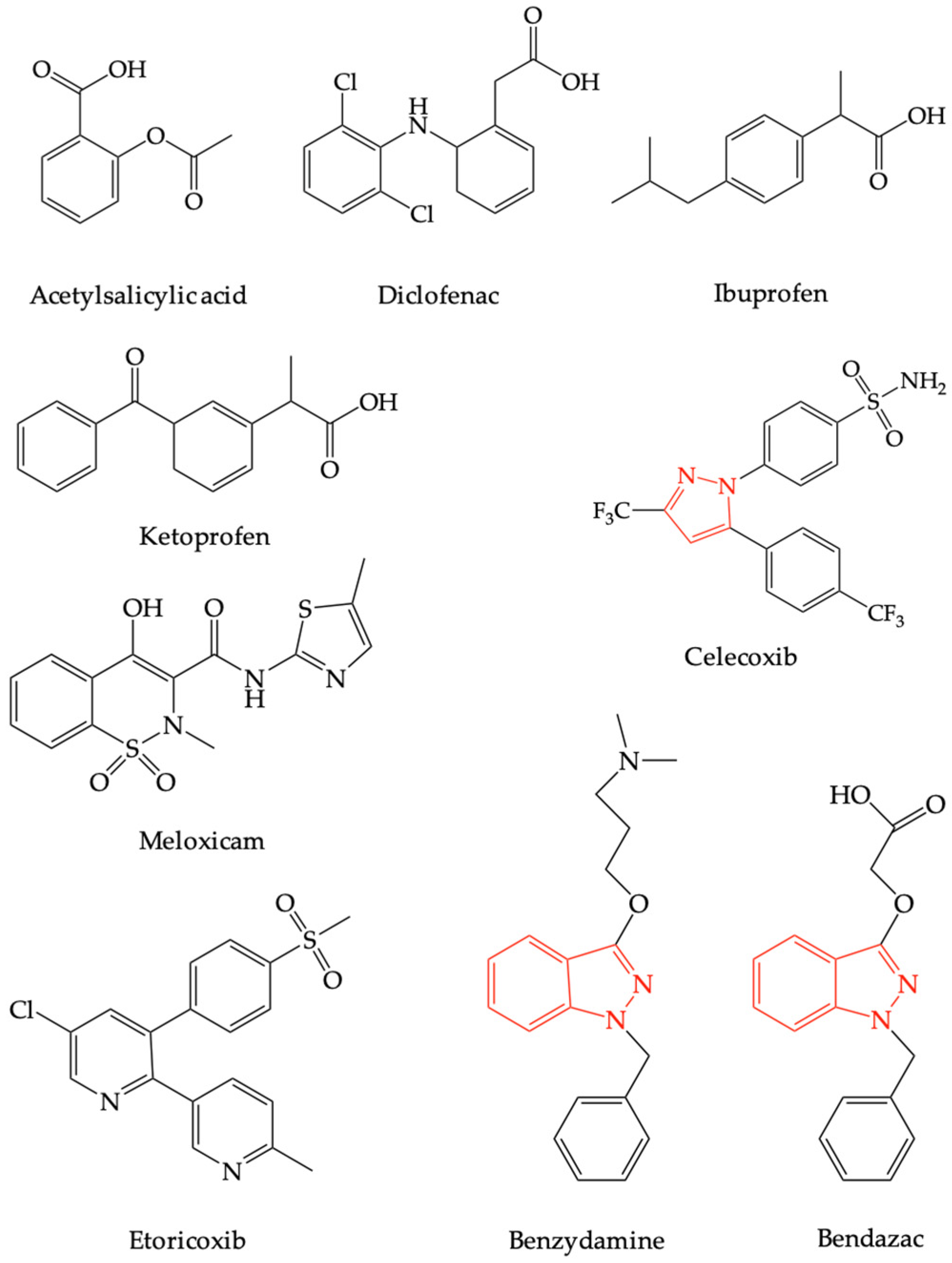
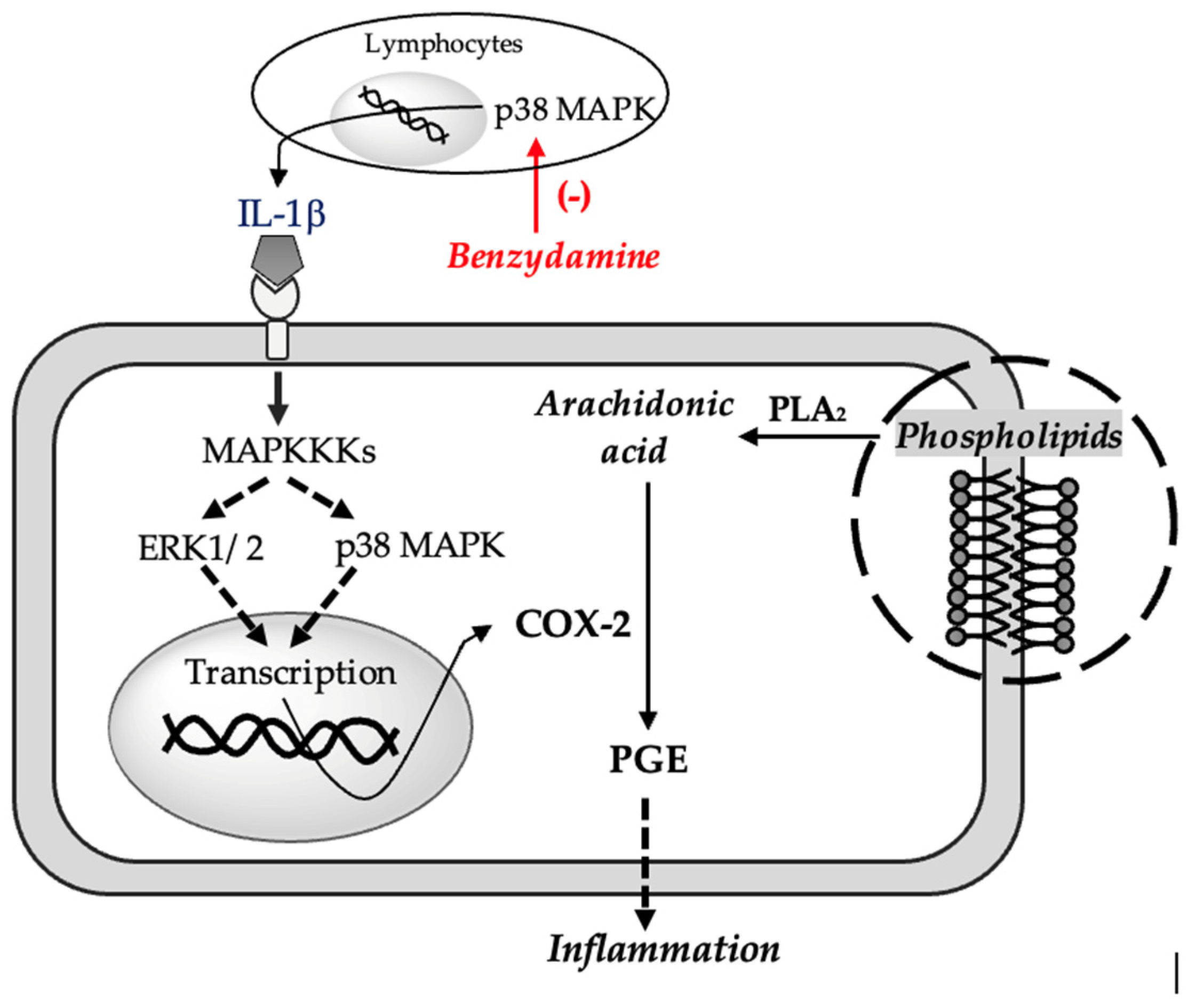
2.1. Benzydamine as a Non-Steroidal Anti-Inflammatory Drug
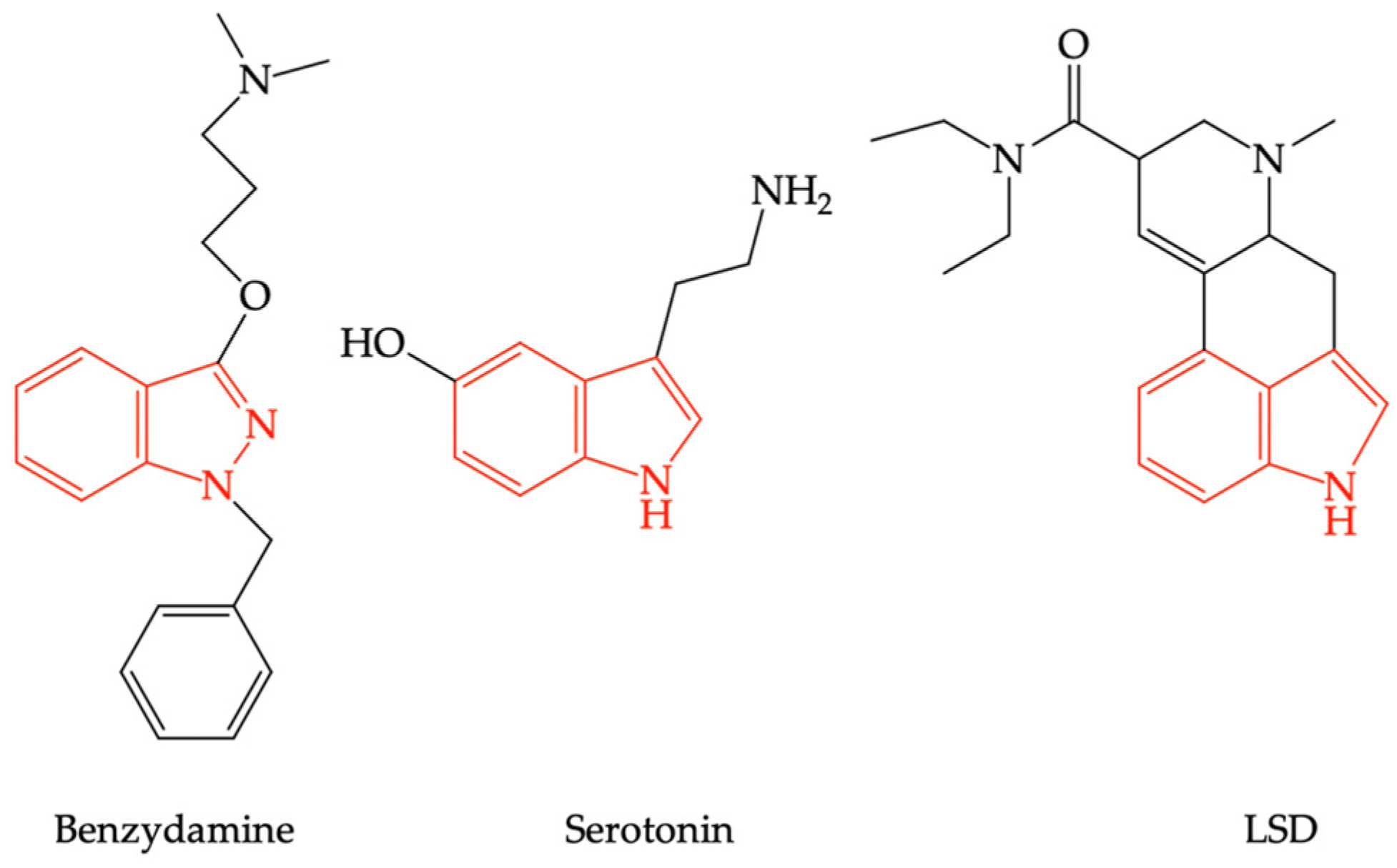
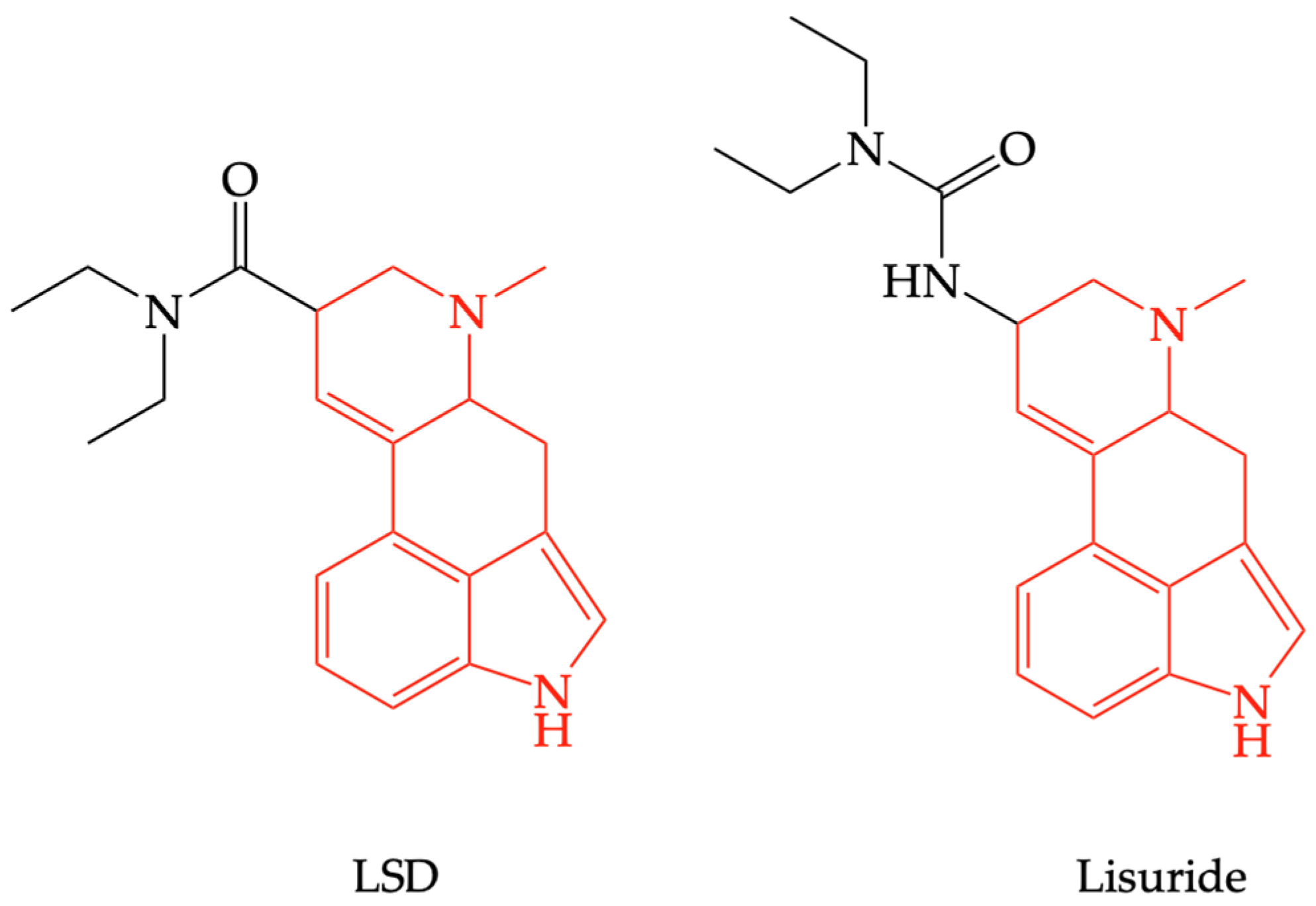
2.2. Benzydamine as Serotonin Receptor Modulator
2.3. Benzydamine as a Cannabinoid (CB1) Receptor Modulator
2.3.1. The Psychotropic Properties of Benzydamine Linked to Cannabinoid Receptor Type 1 (CB1R)
2.3.2. Analgesic Properties of Benzydamine Linked to Cannabinoid Receptor Type 2 (CB2R)
2.4. Benzydamine as Local Anesthetic
3. Conclusions
- The analgesic and/or anti-inflammatory effect could be the consequence of agonist action at the level of CB2R, decreased synthesis of pro-inflammatory cytokines (TNFα, IL-1) as a result of inhibition of p38 MAPK pathway, blockade of Nav1.7 of dorsal root ganglia, modulation of the opening of acid-sensing ion channels (ASICs), and/or decreased release of neuropeptides in the periphery as a result of the inflow of the opening state of TRP channels;
- The local anesthetic effect would be due to blocking voltage-gated sodium channels (Navs) in peripheral nerves;
- The psychotropic and hallucinogenic effect occurs as a result of increased dopamine release in the nucleus accumbens, or as a result of 5-HT2AR stimulation due to the action on CB1R receptors following the suppression of GABA-inhibitory control over the release of dopamine.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Medicines Agency. List of Nationally Authorised Medicinal Products. Active Substance(s): Benzydamine. Available online: https://www.ema.europa.eu/en/documents/psusa/benzydamine-list-nationally-authorised-medicinal-products-psusa/00000375/202110_en (accessed on 2 April 2023).
- Stefania, C.; Andrea, M.; Alessio, M.; Mauro, P.; Amira, G.; Martin, C.J.; Giovanni, M.; Massimo, D.G.; Fabrizio, S. The Benzydamine Experience: A Systematic Review of Benzydamine Abuse. Curr. Neuropharmacol. 2021, 19, 1728–1737. [Google Scholar] [CrossRef]
- Zaprutko, T.; Koligat, D.; Michalak, M.; Wieczorek, M.; Józiak, M.; Ratajczak, M.; Szydłowska, K.; Miazek, J.; Kus, K.; Nowakowska, E. Misuse of OTC Drugs in Poland. Health Policy 2016, 120, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Opaleye, E.S.; Noto, A.R.; van der Sanchez, Z.M.; de Moura, Y.G.; Galduróz, J.C.F.; Carlini, E.A. Recreational Use of Benzydamine as a Hallucinogen among Street Youth in Brazil. Braz. J. Psychiatry 2009, 31, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Gürü, M.; Şafak, Y.; Cengiz, G.F.; Kuru, E.; Örsel, S. Chronic Psychosis Related to Benzydamine Hydrochloride Abuse. Neurocase 2019, 25, 156–158. [Google Scholar] [CrossRef] [PubMed]
- Can, B.; Oz, I.; Ozer, H.; Simsek, T. Hallucinations after Ingesting a High Dose of Benzydamine Hydrochloride. Clin. Psychopharmacol. Neurosci. 2016, 14, 407–408. [Google Scholar] [CrossRef]
- Acar, Y.A.; Kalkan, M.; Çetin, R.; Çevik, E.; Çınar, O. Acute Psychotic Symptoms Due to Benzydamine Hydrochloride Abuse with Alcohol. Case Rep. Psychiatry 2014, 2014, 290365. [Google Scholar] [CrossRef]
- Settimi, L.; Davanzo, F.; Lauria, L.; Casini, M.L.; Ferrazin, F. Oral Ingestion of a Topical Benzydamine Hydrochloride-Containing Gynaecological Preparation in Association with Television Advertising in Italy: Analysis of Cases Managed by a National Poison Control Centre. BMJ Open 2012, 2, e000204. [Google Scholar] [CrossRef]
- Baldock, G.A.; Brodie, R.R.; Chasseaud, L.F.; Taylor, T.; Walmsley, L.M.; Catanese, B. Pharmacokinetics of Benzydamine after Intravenous, Oral, and Topical Doses to Human Subjects. Biopharm. Drug Dispos. 1991, 12, 481–492. [Google Scholar] [CrossRef]
- Alaiye, A.; Kaya, E.; Pınarbaşlı, M.Ö.; Harmancı, N.; Yıldırım, C.; Dönmez, D.B.; Cingi, C. An Experimental Comparison of the Analgesic and Anti-Inflammatory Effects of Safflower Oil, Benzydamine HCl, and Naproxen Sodium. J. Med. Food 2020, 23, 862–869. [Google Scholar] [CrossRef]
- Anggraeni, D.; Kamaluddin, K.; Theodorus, T. Effectiveness of Garlic Water Extract Gel (Allium sativum L.) Against Necrotic Factor Alfa (TNF-α) Tumors and Mouth Ulcer Diameter in Rats. Biomed. J. Indones. 2020, 6, 27–34. [Google Scholar] [CrossRef]
- Mahattanadul, S.; Mustafa, M.W.; Kuadkaew, S.; Pattharachayakul, S.; Ungphaiboon, S.; Sawanyawisuth, K. Oral Ulcer Healing and Anti-Candida Efficacy of an Alcohol-Free Chitosan-Curcumin Mouthwash. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 7020–7023. [Google Scholar] [CrossRef]
- Chitapanarux, I.; Tungkasamit, T.; Petsuksiri, J.; Kannarunimit, D.; Katanyoo, K.; Chakkabat, C.; Setakornnukul, J.; Wongs-rita, S.; Jirawatwarakul, N.; Lertbusayanukul, C.; et al. Randomized Control Trial of Benzydamine HCl versus Sodium Bicar-bonate for Prophylaxis of Concurrent Chemoradiation-Induced Oral Mucositis. Support Care Cancer 2018, 26, 879–886. [Google Scholar] [CrossRef]
- Alalwani, A.; Buhara, O.; Tüzüm, M.Ş. Oral Health-Related Quality of Life and the Use of Oral and Topical Nonsteroidal Anti-Inflammatory Drugs for Pericoronitis. Med. Sci. Monit. 2019, 25, 9200–9206. [Google Scholar] [CrossRef]
- Golac-Guzina, N.; Novaković, Z.; Sarajlić, Z.; Šukalo, A.; Džananović, J.; Glamočlija, U.; Kapo, B.; Čordalija, V.; Mehić, M. Comparative Study of the Efficacy of the Lysozyme, Benzydamine and Chlorhexidine Oral Spray in the Treatment of Acute Ton-sillopharyngitis-Results of a Pilot Study. Acta Med. Acad. 2019, 48, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Khabazian, A.; Tavakoli, A.; Soltani, S.; Karami, E.; Mohaghegh, N. Comparison of Benzydamine Hydrochloride Mouth-Wash 0.15% and Ibuprofen in Reducing Postoperative Pain during 24 Hours after Crown Lengthening: A Randomized Clinical Trial. Open Dent. J. 2020, 14, 66–70. [Google Scholar] [CrossRef]
- Elmarssafy, L.H.; Sadek, H.S.; Hussein, F.F.; Alqahtani, M.; Elkwatehy, W. Clinical Evaluation of Using Benzydamine Hy-drochloride Oral Gel with Intralesional Corticosteroid Injection for Pain Control in Symptomatic Oral Lichen Planus. Egypt. Dent. J. 2020, 66, 969–979. [Google Scholar] [CrossRef]
- Kamboj, K.; Dhull, A.K.; Atri, R.A.; Kaushal, V.; Nongkynrih, A. Comparative Study Evaluating the Role of Benzydamine versus Povidone Iodine in Oral Mucositis during Concomitant Chemoradiation in Locally Advanced Head and Neck Cancer. Cancer Prev. Curr. Res. 2018, 9, 00319. [Google Scholar] [CrossRef]
- Mohamed, N.H.; Kamel, A.M.; Edress, M.F.; Mahmoud, A.S.S.; Gaafar, A.I.A.E.-H. Low Level Laser Therapy versus Ben-zydamin in Prevention and Treatment of Oral Mucositis Induced by Anticancer Treatments (Clinical and Biochemical Study). Braz. Dent. Sci. 2022, 25, e3406. [Google Scholar] [CrossRef]
- Altiparmak, B.; Turan, M. Benzydamine Gargle versus Ketamine Gargle for Postoperative Sore Throat. Med. Sci. 2018, 7, 802–804. [Google Scholar] [CrossRef]
- Hanani, T.; Gadban, H.; Jahshan, F.; Ronen, O. Tantum Verde Mouthwash for Tonsillectomy: A Prospective, Double-Blind, Randomized Control Trial. Int. J. Pediatr. Otorhinolaryngol. 2019, 121, 173–178. [Google Scholar] [CrossRef]
- Tymofieiev, O.; Ushko, N.; Maksymcha, S.; Yarifa, M.; Ripa, V.; Myroshnyk, A.; Savytskyi, O.; Dubichenko, S.; Blinova, V.; Uharska, O.; et al. Prevention of Inflammatory Complications in Fractures of Alveolar Processes of the Jaw. J. Diagn. Treat. Oral Maxillofac. Pathol. 2021, 5, 20–31. [Google Scholar] [CrossRef]
- Ariyawardana, A.; Cheng, K.K.F.; Kandwal, A.; Tilly, V.; Al-Azri, A.R.; Galiti, D.; Chiang, K.; Vaddi, A.; Ranna, V.; Nicola-tou-Galitis, O.; et al. Systematic Review of Anti-Inflammatory Agents for the Management of Oral Mucositis in Cancer Patients and Clinical Practice Guidelines. Support Care Cancer 2019, 27, 3985–3995. [Google Scholar] [CrossRef] [PubMed]
- Thornton, C.P.; Li, M.; Budhathoki, C.; Yeh, C.H.; Ruble, K. Anti-Inflammatory Mouthwashes for the Prevention of Oral Mu-cositis in Cancer Therapy: An Integrative Review and Meta-Analysis. Support Care Cancer 2022, 30, 7205–7218. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, E.; Visintini, S. Benzydamine for the Treatment of Oropharyngeal Mucositis from Radiation Therapy: A Review of Clinical Effectiveness and Guidelines; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2018.
- Blakaj, A.; Bonomi, M.; Gamez, M.E.; Blakaj, D.M. Oral Mucositis in Head and Neck Cancer: Evidence-Based Management and Review of Clinical Trial Data. Oral Oncol. 2019, 95, 29–34. [Google Scholar] [CrossRef]
- Colella, G.; Boschetti, C.E.; Vitagliano, R.; Colella, C.; Jiao, L.; King-Smith, N.; Li, C.; Nuoh Lau, Y.; Lai, Z.; Mohammed, A.I.; et al. Interventions for the Prevention of Oral Mucositis in Patients Receiving Cancer Treatment: Evidence from Randomised Controlled Trials. Curr. Oncol. 2023, 30, 967–980. [Google Scholar] [CrossRef]
- Kuriyama, A.; Aga, M.; Maeda, H. Topical Benzydamine Hydrochloride for Prevention of Postoperative Sore Throat in Adults Undergoing Tracheal Intubation for Elective Surgery: A Systematic Review and Meta-Analysis. Anaesthesia 2018, 73, 889–900. [Google Scholar] [CrossRef]
- Schalch, T.O.; Martimbianco, A.L.C.; Gonçalves, M.L.L.; Motta, L.J.; Santos, E.M.; Cecatto, R.B.; Bussadori, S.K.; Horliana, A.C.R.T. Interventions for Early-Stage Pericoronitis: Systematic Review of Randomized Clinical Trials. Antibiotics 2022, 11, 71. [Google Scholar] [CrossRef]
- Khoshkhoonejad, A.; Khorsand, A.; Rastgar, F. A Comparative Study on Benzydamine HCL 0.5% and Acetaminophen Codeine in Pain Reduction Following Periodontal Surgery. J. Dent. Med. 2004, 17, 39–44. [Google Scholar]
- Patrignani, P.; Patrono, C. Cyclooxygenase Inhibitors: From Pharmacology to Clinical Read-Outs. Biochim. Biophys. Acta BBA Mol. Cell Biol. Lipids 2015, 1851, 422–432. [Google Scholar] [CrossRef]
- Abdelkader, H.; Alany, R.G.; Pierscionek, B. Age-Related Cataract and Drug Therapy: Opportunities and Challenges for Topical Antioxidant Delivery to the Lens. J. Pharm. Pharmacol. 2015, 67, 537–550. [Google Scholar] [CrossRef]
- Sironi, M.; Massimiliano, L.; Transidico, P.; Pinza, M.; Sozzani, S.; Mantovani, A.; Vecchi, A. Differential Effect of Benzydamine on Pro- versus Anti-Inflammatory Cytokine Production: Lack of Inhibition of Interleukin-10 and Interleukin-1 Receptor Antagonist. Int. J. Clin. Lab. Res. 2000, 30, 17–19. [Google Scholar] [CrossRef]
- Sironi, M.; Pozzi, P.; Polentarutti, N.; Benigni, F.; Coletta, I.; Guglielmotti, A.; Milanese, C.; Ghezzi, P.; Vecchi, A.; Pinza, M.; et al. Inhibition of Inflammatory Cytokine Production and Protection against Endotoxin Toxicity by Benzydamine. Cytokine 1996, 8, 710–716. [Google Scholar] [CrossRef]
- Molina-Holgado, E.; Ortiz, S.; Molina-Holgado, F.; Guaza, C. Induction of COX-2 and PGE2 Biosynthesis by IL-1β Is Mediated by PKC and Mitogen-Activated Protein Kinases in Murine Astrocytes. Br. J. Pharmacol. 2000, 131, 152–159. [Google Scholar] [CrossRef]
- Cho, W.; Choe, J. Prostaglandin E2 Stimulates COX-2 Expression via Mitogen-Activated Protein Kinase P38 but Not ERK in Human Follicular Dendritic Cell-like Cells. BMC Immunol. 2020, 21, 20. [Google Scholar] [CrossRef] [PubMed]
- Riboldi, E.; Frascaroli, G.; Transidico, P.; Luini, W.; Bernasconi, S.; Mancini, F.; Guglielmotti, A.; Milanese, C.; Pinza, M.; Sozzani, S.; et al. Benzydamine Inhibits Monocyte Migration and MAPK Activation Induced by Chemotactic Agonists. Br. J. Pharmacol. 2003, 140, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Quane, P.A.; Graham, G.G.; Ziegler, J.B. Pharmacology of Benzydamine. Inflammopharmacology 1998, 6, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Balaban, O.D.; Atagun, M.I.; Yilmaz, H.; Yazar, M.S.; Alpkan, L.R. Benzydamine Abuse as a Hallucinogen: A Case Report. Bull. Clin. Psychopharmacol. 2013, 23, 276–279. [Google Scholar] [CrossRef][Green Version]
- Howell, L.L.; Cunningham, K.A. Serotonin 5-HT2 Receptor Interactions with Dopamine Function: Implications for Therapeutics in Cocaine Use Disorder. Pharmacol. Rev. 2015, 67, 176–197. [Google Scholar] [CrossRef]
- López-Giménez, J.F.; González-Maeso, J. Hallucinogens and Serotonin 5-HT2A Receptor-Mediated Signaling Pathways. Curr. Top. Behav. Neurosci. 2018, 36, 45–73. [Google Scholar] [CrossRef] [PubMed]
- Glennon, R.A.; Titeler, M.; McKenney, J.D. Evidence for 5-HT2 Involvement in the Mechanism of Action of Hallucinogenic Agents. Life Sci. 1984, 35, 2505–2511. [Google Scholar] [CrossRef] [PubMed]
- González-Maeso, J.; Yuen, T.; Ebersole, B.J.; Wurmbach, E.; Lira, A.; Zhou, M.; Weisstaub, N.; Hen, R.; Gingrich, J.A.; Sealfon, S.C. Transcriptome Fingerprints Distinguish Hallucinogenic and Nonhallucinogenic 5-Hydroxytryptamine 2A Receptor Agonist Effects in Mouse Somatosensory Cortex. J. Neurosci. 2003, 23, 8836–8843. [Google Scholar] [CrossRef]
- Halberstadt, A.L.; Geyer, M.A. LSD but Not Lisuride Disrupts Prepulse Inhibition in Rats by Activating the 5-HT2A Receptor. Psychopharmacology 2009, 208, 179. [Google Scholar] [CrossRef]
- Hannon, J.; Hoyer, D. Molecular Biology of 5-HT Receptors. Behav. Brain Res. 2008, 195, 198–213. [Google Scholar] [CrossRef]
- Bittencourt, J.; Velasques, B.; Teixeira, S.; Aprígio, D.; Gongora, M.; Cagy, M.; Fernandes, T.; Ribeiro, P.; Marinho, V. Schizophrenia: A Disorder of Timing and Sensorimotor Integration During Decision-Making. In Multidisciplinarity and Interdisciplinarity in Health; Integrated Science; Rezaei, N., Ed.; Springer International Publishing: Cham, Switzerland, 2022; pp. 123–141. ISBN 978-3-030-96814-4. [Google Scholar]
- Gobert, A.; Millan, M.J. Serotonin (5-HT)2A Receptor Activation Enhances Dialysate Levels of Dopamine and Noradrenaline, but Not 5-HT, in the Frontal Cortex of Freely-Moving Rats. Neuropharmacology 1999, 38, 315–317. [Google Scholar] [CrossRef]
- Yan, Q.; Reith, M.E.; Yan, S. Enhanced Accumbal Dopamine Release Following 5-HT(2A) Receptor Stimulation in Rats Pretreated with Intermittent Cocaine. Brain Res. 2000, 863, 254–258. [Google Scholar] [CrossRef]
- Haber, S.N. Neuroanatomy of Reward: A View from the Ventral Striatum. In Neurobiology of Sensation and Reward; Gottfried, J.A., Ed.; Frontiers in Neuroscience; CRC Press: Boca Raton, FL, USA; Taylor & Francis: Oxfordshire, UK, 2011; ISBN 978-1-4200-6726-2. [Google Scholar]
- Fantegrossi, W.E.; Murnane, K.S.; Reissig, C.J. The Behavioral Pharmacology of Hallucinogens. Biochem. Pharmacol. 2008, 75, 17–33. [Google Scholar] [CrossRef]
- Kurrasch-Orbaugh, D.M.; Parrish, J.C.; Watts, V.J.; Nichols, D.E. A Complex Signaling Cascade Links the Serotonin2A Receptor to Phospholipase A2 Activation: The Involvement of MAP Kinases. J. Neurochem. 2003, 86, 980–991. [Google Scholar] [CrossRef] [PubMed]
- Šaki, M.; Crnkovi, D.I. Increased calcium-independent lipoprotein phospholipase A2 but not protein S100 in patients with schizophrenia. Psychiatr. Danub. 2016, 28, 45–50. [Google Scholar]
- Chrast, R.; Saher, G.; Nave, K.-A.; Verheijen, M.H.G. Lipid Metabolism in Myelinating Glial Cells: Lessons from Human Inherited Disorders and Mouse Models. J. Lipid Res. 2011, 52, 419–434. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Li, M.; Jiang, J.; Hu, X.; Qing, Y.; Sun, L.; Yang, T.; Wang, D.; Cui, G.; Gao, Y.; et al. Dysregulation of Phospholipase and Cyclooxygenase Expression Is Involved in Schizophrenia. E Bio Med. 2021, 64, 103239. [Google Scholar] [CrossRef]
- Bar-Sagi, D.; Hall, A. Ras and Rho GTPases: A Family Reunion. Cell 2000, 103, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, A.; Hall, A. Rho GTPases: Biochemistry and Biology. Annu. Rev. Cell Dev. Biol. 2005, 21, 247–269. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.; Lalli, G. Rho and Ras GTPases in Axon Growth, Guidance, and Branching. Cold Spring Harb. Perspect. Biol. 2010, 2, a001818. [Google Scholar] [CrossRef] [PubMed]
- Cherfils, J.; Zeghouf, M. Regulation of Small GTPases by GEFs, GAPs, and GDIs. Physiol. Rev. 2013, 93, 269–309. [Google Scholar] [CrossRef]
- Hsieh, G.C.; Pai, M.; Chandran, P.; Hooker, B.A.; Zhu, C.Z.; Salyers, A.K.; Wensink, E.J.; Zhan, C.; Carroll, W.A.; Dart, M.J.; et al. Central and Peripheral Sites of Action for CB2 Receptor Mediated Analgesic Activity in Chronic Inflammatory and Neuropathic Pain Models in Rats. Br. J. Pharmacol. 2011, 162, 428–440. [Google Scholar] [CrossRef] [PubMed]
- Herkenham, M.; Lynn, A.B.; Little, M.D.; Johnson, M.R.; Melvin, L.S.; de Costa, B.R.; Rice, K.C. Cannabinoid Receptor Localization in Brain. Proc. Natl. Acad. Sci. USA 1990, 87, 1932–1936. [Google Scholar] [CrossRef]
- Avvisati, R.; Meringolo, M.; Stendardo, E.; Malavasi, E.; Marinelli, S.; Badiani, A. Intravenous Self-Administration of Benzydamine, a Non-Steroidal Anti-Inflammatory Drug with a Central Cannabinoidergic Mechanism of Action. Addict. Biol. 2018, 23, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Mackie, K. Understanding Cannabinoid Psychoactivity with Mouse Genetic Models. PLoS Biol. 2007, 5, e280. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, D.C.; Perry, E.; MacDougall, L.; Ammerman, Y.; Cooper, T.; Wu, Y.; Braley, G.; Gueorguieva, R.; Krystal, J.H. The Psychotomimetic Effects of Intravenous Delta-9-Tetrahydrocannabinol in Healthy Individuals: Implications for Psychosis. Neuropsychopharmacology 2004, 29, 1558–1572. [Google Scholar] [CrossRef]
- Howlett, A.C.; Thomas, B.F.; Huffman, J.W. The Spicy Story of Cannabimimetic Indoles. Molecules 2021, 26, 6190. [Google Scholar] [CrossRef]
- Trexler, K.R.; Vanegas, S.O.; Poklis, J.L.; Kinsey, S.G. The Short-Acting Synthetic Cannabinoid AB-FUBINACA Induces Physical Dependence in Mice. Drug Alcohol Depend. 2020, 214, 108179. [Google Scholar] [CrossRef]
- Ameri, A. The Effects of Cannabinoids on the Brain. Prog. Neurobiol. 1999, 58, 315–348. [Google Scholar] [CrossRef] [PubMed]
- Derkinderen, P.; Ledent, C.; Parmentier, M.; Girault, J.A. Cannabinoids Activate P38 Mitogen-Activated Protein Kinases through CB1 Receptors in Hippocampus. J. Neurochem. 2001, 77, 957–960. [Google Scholar] [CrossRef] [PubMed]
- Piomelli, D. The Molecular Logic of Endocannabinoid Signalling. Nat. Rev. Neurosci. 2003, 4, 873–884. [Google Scholar] [CrossRef]
- Bloomfield, M.A.P.; Ashok, A.H.; Volkow, N.D.; Howes, O.D. The Effects of Δ9-Tetrahydrocannabinol on the Dopamine System. Nature 2016, 539, 369–377. [Google Scholar] [CrossRef]
- Ahn, K.; McKinney, M.K.; Cravatt, B.F. Enzymatic Pathways That Regulate Endocannabinoid Signaling in the Nervous System. Chem. Rev. 2008, 108, 1687–1707. [Google Scholar] [CrossRef] [PubMed]
- El Rawas, R.; Amaral, I.M.; Hofer, A. Is P38 MAPK Associated to Drugs of Abuse-Induced Abnormal Behaviors? Int. J. Mol. Sci. 2020, 21, 4833. [Google Scholar] [CrossRef] [PubMed]
- Prieto, G.A.; Cotman, C.W. Cytokines and Cytokine Networks Target Neurons to Modulate Long-Term Potentiation. Cytokine Growth Factor Rev. 2017, 34, 27–33. [Google Scholar] [CrossRef]
- Aso, E.; Juvés, S.; Maldonado, R.; Ferrer, I. CB2 Cannabinoid Receptor Agonist Ameliorates Alzheimer-like Phenotype in AβPP/PS1 Mice. J. Alzheimers Dis. 2013, 35, 847–858. [Google Scholar] [CrossRef]
- Petzke, F.; Tölle, T.; Fitzcharles, M.-A.; Häuser, W. Cannabis-Based Medicines and Medical Cannabis for Chronic Neuropathic Pain. CNS Drugs 2022, 36, 31–44. [Google Scholar] [CrossRef]
- Hess, C.; Schoeder, C.T.; Pillaiyar, T.; Madea, B.; Müller, C.E. Pharmacological Evaluation of Synthetic Cannabinoids Identified as Constituents of Spice. Forensic Toxicol. 2016, 34, 329–343. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.M.; Porreca, F.; Lai, J.; Albrecht, P.J.; Rice, F.L.; Khodorova, A.; Davar, G.; Makriyannis, A.; Vanderah, T.W.; Mata, H.P.; et al. CB2 Cannabinoid Receptor Activation Produces Antinociception by Stimulating Peripheral Release of Endogenous Opioids. Proc. Natl. Acad. Sci. USA 2005, 102, 3093–3098. [Google Scholar] [CrossRef]
- Starnowska-Sokół, J.; Przewłocka, B. Multifunctional Opioid-Derived Hybrids in Neuropathic Pain: Preclinical Evidence, Ideas and Challenges. Molecules 2020, 25, 5520. [Google Scholar] [CrossRef] [PubMed]
- Körner, J.; Albani, S.; Sudha Bhagavath Eswaran, V.; Roehl, A.B.; Rossetti, G.; Lampert, A. Sodium Channels and Local Anesthetics—Old Friends with New Perspectives. Front. Pharmacol. 2022, 13, 837088. [Google Scholar] [CrossRef]
- Tian, J.-J.; Tan, C.-Y.; Chen, Q.-Y.; Zhou, Y.; Qu, Z.-W.; Zhang, M.; Ma, K.-T.; Shi, W.-Y.; Li, L.; Si, J.-Q. Upregulation of Nav1.7 by Endogenous Hydrogen Sulfide Contributes to Maintenance of Neuropathic Pain. Int. J. Mol. Med. 2020, 46, 782–794. [Google Scholar] [CrossRef] [PubMed]
- Luo, G.; Chen, L.; Easton, A.; Newton, A.; Bourin, C.; Shields, E.; Mosure, K.; Soars, M.G.; Knox, R.J.; Matchett, M.; et al. Discovery of Indole- and Indazole-Acylsulfonamides as Potent and Selective NaV1.7 Inhibitors for the Treatment of Pain. J. Med. Chem. 2019, 62, 831–856. [Google Scholar] [CrossRef]
- Mekhemar, N.A.; El-agwany, A.S.; Radi, W.K.; El-Hady, S.M. Comparative Study between Benzydamine Hydrochloride Gel, Lidocaine 5% Gel and Lidocaine 10% Spray on Endotracheal Tube Cuff as Regards Postoperative Sore Throat. Braz. J. Anesthesiol. 2016, 66, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Chari, V.R.; Paul, A. Comparative Study to Analyze the Incidence of Sore Throat, Cough, and Hoarseness of Voice after General Anesthesia with the Use of Topical Benzydamine Hydrochloride and 2% Lignocaine Gel with Placebo. Med. J. Dr. D.Y. Patil Univ. 2016, 9, 61. [Google Scholar] [CrossRef]
- Huang, Y.-S.; Hung, N.-K.; Lee, M.-S.; Kuo, C.-P.; Yu, J.-C.; Huang, G.-S.; Cherng, C.-H.; Wong, C.-S.; Chu, C.-H.; Wu, C.-T. The Effectiveness of Benzydamine Hydrochloride Spraying on the Endotracheal Tube Cuff or Oral Mucosa for Postoperative Sore Throat. Anesth. Analg. 2010, 111, 887–891. [Google Scholar] [CrossRef]
- Ferrer-Montiel, A.V.; Nikolaeva-Koleva, M.; Vergassola, M.; Mangano, G.; Polenzani, L.; Espinosa, A.; Ragni, L.; Devesa, I. Benzydamine Inhibits Neuronal Excitability Induced by Inflammatory Mediators to Relieve Pain. Biophys. J. 2022, 121, 504a–505a. [Google Scholar] [CrossRef]
- Gu, Q.; Lee, L.-Y. Acid-Sensing Ion Channels and Pain. Pharmaceuticals 2010, 3, 1411–1425. [Google Scholar] [CrossRef] [PubMed]
- Sluka, K.A.; Winter, O.C.; Wemmie, J.A. Acid-Sensing Ion Channels: A New Target for Pain and CNS Diseases. Curr. Opin. Drug Discov. Devel. 2009, 12, 693–704. [Google Scholar] [PubMed]
- Lee, J.Y.P.; Saez, N.J.; Cristofori-Armstrong, B.; Anangi, R.; King, G.F.; Smith, M.T.; Rash, L.D. Inhibition of Acid-Sensing Ion Channels by Diminazene and APETx2 Evoke Partial and Highly Variable Antihyperalgesia in a Rat Model of Inflammatory Pain. Br. J. Pharmacol. 2018, 175, 2204–2218. [Google Scholar] [CrossRef] [PubMed]
- Verkest, C.; Salinas, M.; Diochot, S.; Deval, E.; Lingueglia, E.; Baron, A. Mechanisms of Action of the Peptide Toxins Targeting Human and Rodent Acid-Sensing Ion Channels and Relevance to Their In Vivo Analgesic Effects. Toxins 2022, 14, 709. [Google Scholar] [CrossRef]
- Mourier, G.; Salinas, M.; Kessler, P.; Stura, E.A.; Leblanc, M.; Tepshi, L.; Besson, T.; Diochot, S.; Baron, A.; Douguet, D.; et al. Mambalgin-1 Pain-Relieving Peptide, Stepwise Solid-Phase Synthesis, Crystal Structure, and Functional Domain for Acid-Sensing Ion Channel 1a Inhibition. J. Biol. Chem. 2016, 291, 2616–2629. [Google Scholar] [CrossRef]
- Chang, C.-T.; Fong, S.W.; Lee, C.-H.; Chuang, Y.-C.; Lin, S.-H.; Chen, C.-C. Involvement of Acid-Sensing Ion Channel 1b in the Development of Acid-Induced Chronic Muscle Pain. Front. Neurosci. 2019, 13, 1247. [Google Scholar] [CrossRef]
- Silverman, H.A.; Chen, A.; Kravatz, N.L.; Chavan, S.S.; Chang, E.H. Involvement of Neural Transient Receptor Potential Channels in Peripheral Inflammation. Front. Immunol. 2020, 11, 590261. [Google Scholar] [CrossRef]
- Molyva, D. Neuropeptides and Pain. Ann. Gen. Psychiatry 2010, 9, S3. [Google Scholar] [CrossRef][Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Medicinal Product | Concentration/Dose | Route of Administration | Member State Where Product Is Authorized * |
|---|---|---|---|
| Solution (spray) | 0.30% | Oral mucosa | BG, HU, PL, GR, FI, SE, NO, SK, HR, CZ, RO, BE, DE, AT, XI |
| Solution (spray) | 0.15% | Oral mucosa | BG, IT, DE, SK, RO, ES, UK, IE, SI, CZ, SK, PL, SE, NO, DK, LT, HR, MT, IS, HU, BE, AT, XI |
| Solution (mouthwash) | 0.30% | Oral mucosa | IT, PL |
| Solution (mouthwash) | 0.15% | Oral mucosa | IT, PL, SK, SI, RO, HR, CZ, IE, MT, XI |
| Solution (vaginal irrigation) | 1% | Vaginal mucosa | DE, IT |
| Solution (vaginal irrigation) | 0.1% | Vaginal mucosa | IT, FR |
| Solution (vaginal irrigation) | 140 mg | Vaginal mucosa | SK, CZ, ES |
| Cream | 0.5% | Vaginal mucosa | IT |
| Tablets | 3 mg | Oral mucosa | BG, IT, PL, RO, CZ, LT, HU, SI, GR, LT, AT, SK, AT, DE |
| Gel | 5% | Skin | BG, IT, RO, ES |
| Cream | 5% | Skin | BG, IT, PL |
| Cream | 3% | Skin | NL, IE |
| Ointment | 3% | Skin | ES |
| Granules for vaginal solution | 500 mg | Vaginal mucosa | SK, IT, ES, LT, RO |
| Powder for vaginal solution | 53.2 mg/g | Vaginal mucosa | PL |
| Toothpaste | 0.5% | - | IT |
| Study Design | Animal Species | Dose/Route | Evidence of Efficacy | References |
|---|---|---|---|---|
| Experimental inflammation (2% formaldehyde) | Rats | 100 mg/kg/injection (rat paw) | Inhibition of paw edema | [10] |
| Experimental oral ulcers (50% acetic acid) | Rats | Not mentioned | Oral ulcers diameter reduction; reduction of TNF-alpha levels | [11] |
| Experimental buccal mucosal ulcer (99.7% acetic acid) | Hamsters | 0.15% benzydamine mouthwash | Oral ulcers healing | [12] |
| Study Design | No. of Participants | Dose/Route | Evidence of Efficacy | References |
|---|---|---|---|---|
| Multicenter, randomized | 60 | 0.15% benzydamine hydrochloride (mouthwash) | Reducing the severity of oral mucositis (after platinum-based chemotherapy) | [13] |
| Randomized, placebo-controlled | 60 | 0.045 g, 30 mL oral spray | Reduction of the severity of pericoronitis (after surgery) | [14] |
| Prospective, two-arm pilot study | 32 | Not declared | Reduction of throat inflammation (patients with acute tonsillopharyngitis) | [15] |
| Randomized | 36 | 0.15% benzydamine hydrochloride (mouthwash) | Reduction of postoperative pain after periodontal surgery | [16] |
| Randomized | 20 | 10 g mouth gel, each g contains: benzydamine hydrochloride 10 mg, cetylpyridinium chloride 1 mg | Reduction in the severity of symptoms in patients with oral lichen planus | [17] |
| Randomized | 60 | 0.15% benzydamine hydrochloride (mouthwash) | Reduction of oral mucositis severity (after chemoradiotherapy) | [18] |
| Randomized | 80 | 0.15% benzydamine hydrochloride (mouthwash) | Reduction of oral mucositis severity after neck and head radiotherapy | [19] |
| Restrospctive | 153 | 0.15% benzydamine hydrochloride (mouthwash gargle) | Alleviating postoperative pain in the neck | [20] |
| Randomized, double-blind, placebo-controlled | 39 | 0.15% benzydamine hydrochloride (mouthwash gargle) | Reduction in post-tonsillectomy pain and bleeding | [21] |
| Randomized | 129 | 0.15% benzydamine hydrochloride (mouthwash) | Reduction in the number of inflammatory complications (patients with fractures of the alveolar processes of the jaws) | [22] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ősz, B.-E.; Jîtcă, G.; Sălcudean, A.; Rusz, C.M.; Vari, C.-E. Benzydamine—An Affordable Over-the-Counter Drug with Psychoactive Properties—From Chemical Structure to Possible Pharmacological Properties. Pharmaceuticals 2023, 16, 566. https://doi.org/10.3390/ph16040566
Ősz B-E, Jîtcă G, Sălcudean A, Rusz CM, Vari C-E. Benzydamine—An Affordable Over-the-Counter Drug with Psychoactive Properties—From Chemical Structure to Possible Pharmacological Properties. Pharmaceuticals. 2023; 16(4):566. https://doi.org/10.3390/ph16040566
Chicago/Turabian StyleŐsz, Bianca-Eugenia, George Jîtcă, Andreea Sălcudean, Carmen Maria Rusz, and Camil-Eugen Vari. 2023. "Benzydamine—An Affordable Over-the-Counter Drug with Psychoactive Properties—From Chemical Structure to Possible Pharmacological Properties" Pharmaceuticals 16, no. 4: 566. https://doi.org/10.3390/ph16040566
APA StyleŐsz, B.-E., Jîtcă, G., Sălcudean, A., Rusz, C. M., & Vari, C.-E. (2023). Benzydamine—An Affordable Over-the-Counter Drug with Psychoactive Properties—From Chemical Structure to Possible Pharmacological Properties. Pharmaceuticals, 16(4), 566. https://doi.org/10.3390/ph16040566