
Cardioprotective Effect of Flibanserin against Isoproterenol-Induced Myocardial Infarction in Female Rats: Role of Cardiac 5-HT2A Receptor Gene/5-HT/Ca2+ Pathway

 , , ,
, , ,  ,
,  and
and
Abstract
1. Introduction
2. Results
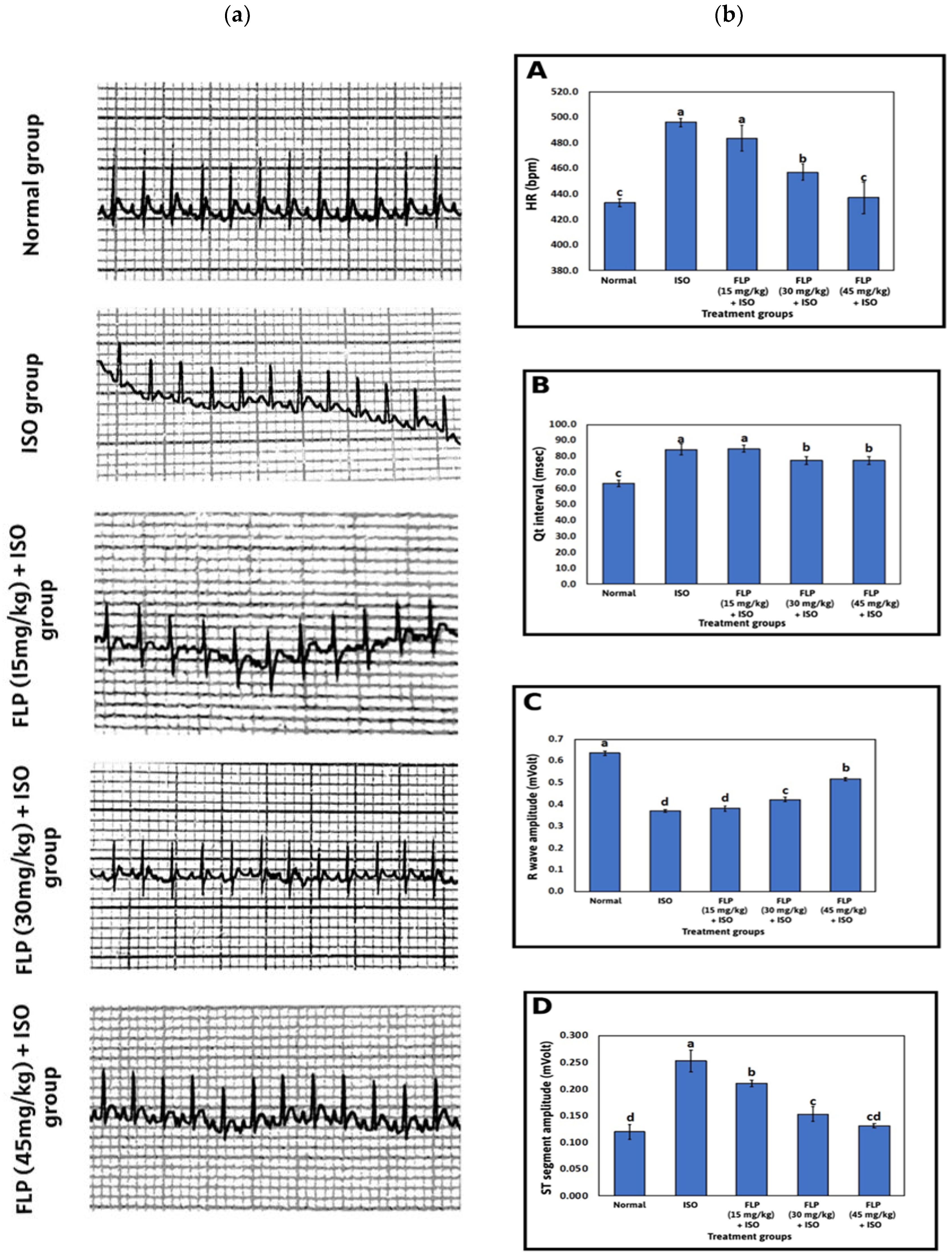
2.1. Effect of FLP Pretreatment on Heart Rate (HR), R Wave Amplitude, ST Segment Amplitude, and Qt Interval
2.2. Effect of FLP Pretreatment on Histopathology
2.3. Effect of FLP Pretreatment on Serum Troponin I (TnI), Lactate Dehydrogenase (LDH), Creatinine Kinase-MB (CK-MB), and Creatine Kinase (CK)
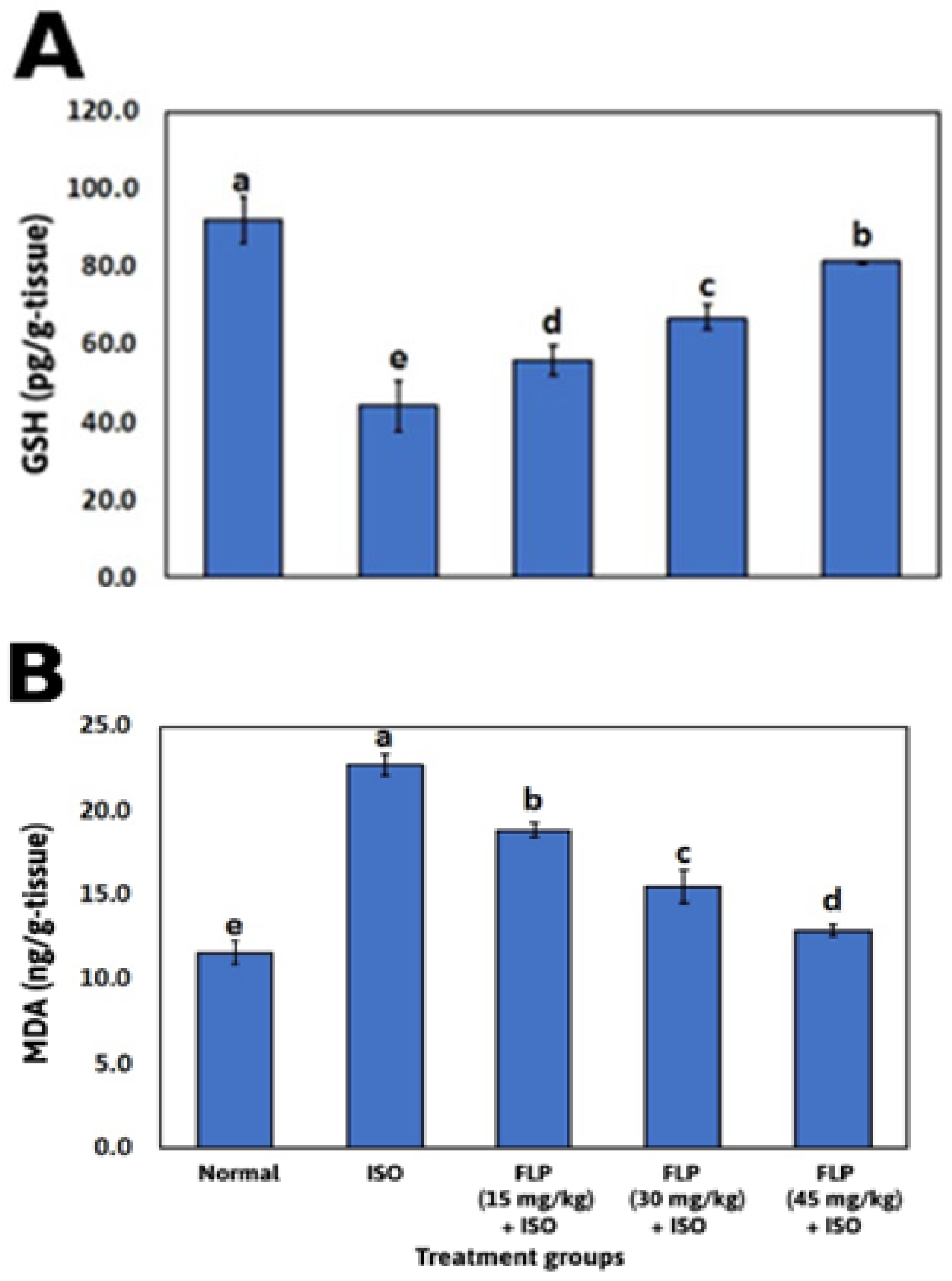
2.4. Effect of FLP Pretreatment on Cardiac Oxidative Stress Markers
2.5. Effect of FLP Pretreatment on Serum 5-HT, Cardiac 5-HT, and Cardiac Total Calcium (Ca2+)
2.6. Effect of FLP Pretreatment on Cardiac 5-HT2A Gene Expression
3. Discussion
4. Materials and Methods
4.1. Experimental Animals
4.2. Drugs and Chemicals
4.3. Experimental Design
4.3.1. Sample Size Calculations
4.3.2. Experiment
- Normal group: Rats received two s.c. Injections of normal saline (vehicle of ISO) in a volume of 1.5 mL/kg, one injection per day on days 27 and 28.
- FLP (15 mg/kg) + ISO group: Rats were treated with FLP at a dose of (15 mg/kg/day, p.o.) for 28 days, followed by two injections of ISO (85 mg/kg/day, s.c.), one injection per day at day 27 and 28.
- FLP (30 mg/kg) + ISO group: Rats were treated with FLP at a dose of (30 mg/kg/day, p.o.) for 28 days, followed by two injections of ISO (85 mg/kg/day, s.c.), one injection per day at day 27 and 28.
- FLP (45 mg/kg) + ISO group: Rats were treated with FLP at a dose of (45 mg/kg/day, p.o.) for 28 days, followed by two injections of ISO (85 mg/kg/day, s.c.), one injection per day on days 27 and 28.
4.4. Induction of MI
4.5. Electrocardiogram Monitoring
4.6. Collection of Blood and Tissue Samples
4.7. Histopathological Examination of the Heart Tissue
4.8. Determination of Serum Cardiac Markers
4.9. Determination of the Cardiac Oxidative Stress Markers
4.10. Determination of the Serum, Cardiac 5-HT, and the Cardiac Total Ca2+
4.11. Determination of the Cardiac 5-HT2A Receptors Regulation
4.12. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anderson, J.L.; Morrow, D.A. Acute Myocardial Infarction. Available online: https://www.nejm.org/doi/pdf/10.1056/NEJMra1606915 (accessed on 5 February 2023).
- Singh, A.K.; Jat, R.K. Myocardial Infarction. Himal. J. Health Sci. 2021, 6, 16–32. [Google Scholar] [CrossRef]
- Pamukçu, B. Myocardial Infarction; BoD—Books on Demand: Norderstedt, Germany, 2019; ISBN 978-1-78984-868-7. [Google Scholar]
- Ferri, F.F. Ferri’s Clinical Advisor 1030-1040.e1 2022; Elsevier-Health Science: Philadelphia, PA, USA, 2022. [Google Scholar]
- Madigan, M.; Atoui, R. Therapeutic Use of Stem Cells for Myocardial Infarction. Bioengineering 2018, 5, 28. [Google Scholar] [CrossRef] [PubMed]
- Fishbein, G.A. Chapter 10. Myocardial Ischemia and Its Complications. In Cardiovascular Pathology; Academic Press: London, UK, 2022; p. 39. [Google Scholar]
- Ziaee, M.; Khorrami, A.; Ebrahimi, M.; Nourafcan, H.; Amiraslanzadeh, M.; Rameshrad, M.; Garjani, M.; Garjani, A. Cardioprotective Effects of Essential Oil of Lavandula Angustifolia on Isoproterenol-Induced Acute Myocardial Infarction in Rat. Iran. J. Pharm. Res. 2015, 14, 279–289. [Google Scholar] [PubMed]
- Elshourbagy, N. The effect of carvedilol and Q10 on isoprenaline-induced cardiotoxicity: Electrocardiographic, biochemical and histopathological evaluation in rats. Al-Azhar J. Pharm. Sci. 2016, 54, 148–158. [Google Scholar] [CrossRef]
- Khalifa, A.A.; El Sokkary, N.H.; Elblehi, S.S.; Diab, M.A.; Ali, M.A. Potential Cardioprotective Effect of Octreotide via NOXs Mitigation, Mitochondrial Biogenesis and MAPK/Erk1/2/STAT3/NF-Kβ Pathway Attenuation in Isoproterenol-Induced Myocardial Infarction in Rats. Eur. J. Pharmacol. 2022, 925, 174978. [Google Scholar] [CrossRef]
- Shimizu, Y.; Minatoguchi, S.; Hashimoto, K.; Uno, Y.; Arai, M.; Wang, N.; Chen, X.; Lu, C.; Takemura, G.; Shimomura, M.; et al. The Role of Serotonin in Ischemic Cellular Damage and the Infarct Size-Reducing Effect of Sarpogrelate, a 5-Hydroxytryptamine-2 Receptor Blocker, in Rabbit Hearts. J. Am. Coll. Cardiol. 2002, 40, 1347–1355. [Google Scholar] [CrossRef]
- Horibe, E.; Nishigaki, K.; Minatoguchi, S.; Fujiwara, H. Sarpogrelate, a 5-HT2 Receptor Blocker, May Have a Preconditioning-Like Effect in Patients With Coronary Artery Disease. Circ. J. 2004, 68, 68–72. [Google Scholar] [CrossRef]
- Mauler, M.; Herr, N.; Schoenichen, C.; Witsch, T.; Marchini, T.; Härdtner, C.; Koentges, C.; Kienle, K.; Ollivier, V.; Schell, M.; et al. Platelet Serotonin Aggravates Myocardial Ischemia/Reperfusion Injury via Neutrophil Degranulation. Circulation 2019, 139, 918–931. [Google Scholar] [CrossRef]
- Sonobe, T.; Akiyama, T.; Du, C.-K.; Zhan, D.-Y.; Shirai, M. Contribution of Serotonin Uptake and Degradation to Myocardial Interstitial Serotonin Levels during Ischaemia-Reperfusion in Rabbits. Acta Physiol. 2013, 207, 260–268. [Google Scholar] [CrossRef]
- Du, C.-K.; Zhan, D.-Y.; Akiyama, T.; Inagaki, T.; Shishido, T.; Shirai, M.; Pearson, J.T. Myocardial Interstitial Levels of Serotonin and Its Major Metabolite 5-Hydroxyindole Acetic Acid during Ischemia-Reperfusion. Am. J. Physiol.-Heart Circ. Physiol. 2017, 312, H60–H67. [Google Scholar] [CrossRef]
- Ayme-Dietrich, E.; Aubertin-Kirch, G.; Maroteaux, L.; Monassier, L. Cardiovascular Remodeling and the Peripheral Serotonergic System. Arch. Cardiovasc. Dis. 2017, 110, 51–59. [Google Scholar] [CrossRef]
- Brasil, D.; Temsah, R.M.; Kumar, K.; Kumamoto, H.; Takeda, N.; Dhalla, N.S. Blockade of 5-HT2A Receptors by Sarpogrelate Protects the Heart Against Myocardial Infarction in Rats. J. Cardiovasc. Pharmacol. Ther. 2002, 7, 53–59. [Google Scholar] [CrossRef]
- Rajesh, K.G.; Suzuki, R.; Maeda, H.; Murio, Y.; Sasaguri, S. 5-HT2 Receptor Blocker Sarpogrelate Prevents Downregulation of Antiapoptotic Protein Bcl-2 and Protects the Heart against Ischemia–Reperfusion Injury. Life Sci. 2006, 79, 1749–1755. [Google Scholar] [CrossRef]
- Grover, G.J.; Sargent, C.A.; Dzwonczyk, S.; Normandin, D.E.; Antonaccio, M.J. Protective Effect of Serotonin (5-HT2) Receptor Antagonists in Ischemic Rat Hearts. J. Cardiovasc. Pharmacol. 1993, 22, 664–672. [Google Scholar] [CrossRef]
- Baid, R.; Agarwal, R. Flibanserin: A Controversial Drug for Female Hypoactive Sexual Desire Disorder. Ind. Psychiatry J. 2018, 27, 154–157. [Google Scholar] [CrossRef]
- Thangaraju, P.; Velmurugan, H.; Ty, S.S. Drug Flibanserin–in Hypoactive Sexual Desire Disorder. Gynecol. Obstet. Clin. Med. 2022, 2, 91–95. [Google Scholar] [CrossRef]
- Stahl, S.M. Mechanism of Action of Flibanserin, a Multifunctional Serotonin Agonist and Antagonist (MSAA), in Hypoactive Sexual Desire Disorder. CNS Spectr. 2015, 20, 455–459. [Google Scholar] [CrossRef]
- Thorp, J.; Simon, J.; Dattani, D.; Taylor, L.; Kimura, T.; Garcia, M.G., Jr.; Lesko, L.; Pyke, R. Treatment of Hypoactive Sexual Desire Disorder in Premenopausal Women: Efficacy of Flibanserin in the DAISY Study. J. Sex. Med. 2012, 9, 793–804. [Google Scholar] [CrossRef]
- Namara, K.M.; Alzubaidi, H.; Jackson, J.K. Cardiovascular Disease as a Leading Cause of Death: How Are Pharmacists Getting Involved? IPRP 2019, 8, 1–11. [Google Scholar] [CrossRef]
- Kumar, M.; Kasala, E.R.; Bodduluru, L.N.; Kumar, V.; Lahkar, M. Molecular and Biochemical Evidence on the Protective Effects of Quercetin in Isoproterenol-Induced Acute Myocardial Injury in Rats. J. Biochem. Mol. Toxicol. 2017, 31, e21832. [Google Scholar] [CrossRef] [PubMed]
- Panda, S.; Kar, A.; Biswas, S. Preventive Effect of Agnucastoside C against Isoproterenol-Induced Myocardial Injury. Sci. Rep. 2017, 7, 16146. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.Y.; Lee, J.; Park, J.; Lee, Y.; Ahn, S.; Lee, J.H.; Koh, D.; Lee, Y.H.; Lim, Y. Design, Synthesis, and Biological Activities of 1-Aryl-(3-(2-Styryl)Phenyl)Prop-2-En-1-Ones. Bioorganic Chem. 2019, 83, 438–449. [Google Scholar] [CrossRef] [PubMed]
- Nagatomo, T.; Rashid, M.; Abul Muntasir, H.; Komiyama, T. Functions of 5-HT2A Receptor and Its Antagonists in the Cardiovascular System. Pharmacol. Ther. 2004, 104, 59–81. [Google Scholar] [CrossRef]
- Bampalis, V. Role of the Serotonin Transporter and the 5-HT2A and 5-HT4 Receptors for Platelet Function in Blood. Ph.D. Thesis, Ludwig-Maximilians-Universität München, Munich, Germany, 2016. [Google Scholar]
- Saadat, S.; Panahi, Y.; Hosseinialhashemi, M.; Kabir, A.; Rahmani, K.; Sahebkar, A. Systematic Review and Meta-Analysis of Flibanserin’s Effects and Adverse Events in Women with Hypoactive Sexual Desire Disorder. CDM 2017, 18, 78–85. [Google Scholar] [CrossRef]
- Clayton, A.H.; Brown, L.; Kim, N.N. Evaluation of Safety for Flibanserin. Expert Opin. Drug Saf. 2020, 19, 1–8. [Google Scholar] [CrossRef]
- Khalifa, A.A.; Rashad, R.M.; El-Hadidy, W.F. Thymoquinone Protects against Cardiac Mitochondrial DNA Loss, Oxidative Stress, Inflammation and Apoptosis in Isoproterenol-Induced Myocardial Infarction in Rats. Heliyon 2021, 7, e07561. [Google Scholar] [CrossRef]
- Priscilla, D.H.; Prince, P.S.M. Cardioprotective Effect of Gallic Acid on Cardiac Troponin-T, Cardiac Marker Enzymes, Lipid Peroxidation Products and Antioxidants in Experimentally Induced Myocardial Infarction in Wistar Rats. Chem. Biol. Interact. 2009, 179, 118–124. [Google Scholar] [CrossRef]
- Pullaiah, C.P.; Narasimha Kumar, G.V.; Jyothsna, K.; Thyagaraju, K.; Nelson, V.K.; Dayanand Reddy, G. Rosa damascena Mill. L. Attenuates Myocardial Lysosomal Membrane Destabilization in Isoproterenol Induced Oxidative Stress. Orient. Pharm. Exp. Med. 2017, 17, 373–380. [Google Scholar] [CrossRef]
- Rajadurai, M.; Stanely Mainzen Prince, P. Preventive Effect of Naringin on Lipid Peroxides and Antioxidants in Isoproterenol-Induced Cardiotoxicity in Wistar Rats: Biochemical and Histopathological Evidences. Toxicology 2006, 228, 259–268. [Google Scholar] [CrossRef]
- Zhou, B.; Wu, L.-J.; Li, L.-H.; Tashiro, S.; Onodera, S.; Uchiumi, F.; Ikejima, T. Silibinin Protects against Isoproterenol-Induced Rat Cardiac Myocyte Injury through Mitochondrial Pathway after up-Regulation of SIRT1. J. Pharmacol. Sci. 2006, 102, 387–395. [Google Scholar] [CrossRef]
- Dhalla, N.S.; Adameova, A.; Kaur, M. Role of Catecholamine Oxidation in Sudden Cardiac Death. Fundam. Clin. Pharmacol. 2010, 24, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Zhang, J.; Ren, T.; Dong, Z. Targeted Metabolomic Profiling of Cardioprotective Effect of Ginkgo biloba L. Extract on Myocardial Ischemia in Rats. Phytomedicine 2016, 23, 621–631. [Google Scholar] [CrossRef]
- Shaikh, S.; Bhatt, L.K.; Barve, K. Attenuation of Isoproterenol-Induced Cardiotoxicity in Rats by Narirutin Rich Fraction from Grape Fruit. Phytomedicine 2019, 55, 222–228. [Google Scholar] [CrossRef]
- Sharmila, S.T.; Rajadurai, M. Preventive Effect of Bio-Aq on Cardiac Markers, Lipids, and Membrane Bound Enzymes in Isoproterenol—Induced Myocardial Infarction in Rats. Asian J. Pharm. Clin. Res. 2012, 5, 8. [Google Scholar]
- Goyal, S.; Arora, S.; Bhatt, T.K.; Das, P.; Sharma, A.; Kumari, S.; Arya, D.S. Modulation of PPAR-Gamma by Telmisartan Protects the Heart against Myocardial Infarction in Experimental Diabetes. Chem. Biol. Interact. 2010, 185, 271–280. [Google Scholar] [CrossRef]
- Ojha, S.; Azimullah, S.; Mohanraj, R.; Sharma, C.; Yasin, J.; Arya, D.S.; Adem, A. Thymoquinone Protects against Myocardial Ischemic Injury by Mitigating Oxidative Stress and Inflammation. Evid. Based Complement. Alternat. Med. 2015, 2015, 143629. [Google Scholar] [CrossRef]
- Panda, V.; Bhandare, N.; Mistry, K.; Sudhamani, S.; Dande, P. Cardioprotective Potential of Spinacia oleracea (Spinach) against Isoproterenol-Induced Myocardial Infarction in Rats. Arch. Physiol. Biochem. 2022, 128, 101–110. [Google Scholar] [CrossRef]
- Saravanan, G.; Ponmurugan, P.; Sathiyavathi, M.; Vadivukkarasi, S.; Sengottuvelu, S. Cardioprotective Activity of Amaranthus Viridis Linn: Effect on Serum Marker Enzymes, Cardiac Troponin and Antioxidant System in Experimental Myocardial Infarcted Rats. Int. J. Cardiol. 2013, 165, 494–498. [Google Scholar] [CrossRef]
- Mythili, S.; Malathi, N. Diagnostic Markers of Acute Myocardial Infarction (Review). Biomed. Rep. 2015, 3, 743–748. [Google Scholar] [CrossRef]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation: The Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Aydin, S.; Ugur, K.; Aydin, S.; Sahin, İ.; Yardim, M. Biomarkers in Acute Myocardial Infarction: Current Perspectives. Vasc. Health Risk Manag. 2019, 15, 1–10. [Google Scholar] [CrossRef]
- Chen, Y.; Peng, L.; Shi, S.; Guo, G.; Wen, H. Boeravinone B Alleviates Gut Dysbiosis during Myocardial Infarction-Induced Cardiotoxicity in Rats. J. Cell. Mol. Med. 2021, 25, 6403–6416. [Google Scholar] [CrossRef] [PubMed]
- Maleki Dizaji, N.; Garjani, A.; Mousavi, S.; Mohammadi, M.; Vaez, H. Time-Dependent Influence of Infliximab on Hemodynamic Responses and Cardiac Injuries of Isoproterenol-Induced Myocardial Infarction in Rats. Eur. J. Pharmacol. 2021, 903, 174122. [Google Scholar] [CrossRef]
- Danese, E.; Montagnana, M. An Historical Approach to the Diagnostic Biomarkers of Acute Coronary Syndrome. Ann. Transl. Med. 2016, 4, 194. [Google Scholar] [CrossRef]
- Saqib, F.; Ali, A.; Ahmedah, H.T.; Irimie, C.A.; Toma, S.I.; Popovici, B.E.; Moga, M.; Irimie, M. Cardioprotective, Hypotensive and Toxicological Studies of Populus ciliata (Wall. Ex Royle). Biomed. Pharmacother. 2021, 142, 112065. [Google Scholar] [CrossRef]
- Cinar, I.; Yayla, M.; Tavaci, T.; Toktay, E.; Ugan, R.A.; Bayram, P.; Halici, H. In Vivo and In Vitro Cardioprotective Effect of Gossypin Against Isoproterenol-Induced Myocardial Infarction Injury. Cardiovasc. Toxicol. 2022, 22, 52–62. [Google Scholar] [CrossRef]
- Frampton, J.; Devries, J.T.; Welch, T.D.; Gersh, B.J. Modern Management of ST-Segment Elevation Myocardial Infarction. Curr. Probl. Cardiol. 2020, 45, 100393. [Google Scholar] [CrossRef]
- Omar, E.M.; Omar, R.S.; Shoela, M.S.; Sayed, N.S.E. A Study of the Cardioprotective Effect of Spermidine: A Novel Inducer of Autophagy. Chin. J. Physiol. 2021, 64, 281. [Google Scholar] [CrossRef]
- Thippeswam, B.S.; Thakker, S.P.; Tubachi, S.; Kalyani, G.A.; Netra, M.K.; Patil, U.; Desai, S.; Gavimath, C.; Veerapur, V. Cardioprotective Effect of Cucumis Trigonus Roxb on Isoproterenol-Induced Myocardial Infarction in Rat. Am. J. Pharmacol. Toxicol. 2009, 4, 29–37. [Google Scholar] [CrossRef]
- Metias, E.; Omar, N.; Hussein, A.; Abdallah, E.; Abdel-Aziz, A. Modulation of ECG, Myocardial Oxidative Stress Markers and Connexion 43 Expression by Ascorbic Acid and Ferulic Acid in Isoproterenol-Induced Myocardial Infarction in Rats. Biochem. Physiol. 2016, 5, 210. [Google Scholar] [CrossRef]
- Patel, V.; Upaganlawar, A.; Zalawadia, R.; Balaraman, R. Cardioprotective Effect of Melatonin against Isoproterenol Induced Myocardial Infarction in Rats: A Biochemical, Electrocardiographic and Histoarchitectural Evaluation. Eur. J. Pharmacol. 2010, 644, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Khdhiri, E.; Mnafgui, K.; Ncir, M.; Feriani, A.; Ghazouani, L.; Hajji, R.; Jallouli, D.; Abid, M.; Jamoussi, K.; Allouche, N.; et al. Cardiopreventive Capacity of a Novel (E)-N′-(1-(7-Methoxy-2-Oxo-2H-Chromen-3-Yl) Ethylidene)-4-Methylbenzenesulfonohydrazide against Isoproterenol-Induced Myocardial Infarction by Moderating Biochemical, Oxidative Stress, and Histological Parameters. J. Biochem. Mol. Toxicol. 2021, 35, e22747. [Google Scholar] [CrossRef]
- Medhet, M.; El-Bakly, W.M.; Badr, A.M.; Awad, A.; El-Demerdash, E. Thymoquinone Attenuates Isoproterenol-Induced Myocardial Infarction by Inhibiting Cytochrome C and Matrix Metalloproteinase-9 Expression. Clin. Exp. Pharmacol. Physiol. 2022, 49, 391–405. [Google Scholar] [CrossRef]
- Abbas, A.M. Cardioprotective Effect of Resveratrol Analogue Isorhapontigenin versus Omega-3 Fatty Acids in Isoproterenol-Induced Myocardial Infarction in Rats. J. Physiol. Biochem. 2016, 72, 469–484. [Google Scholar] [CrossRef]
- Qudus, A.A. Effect of Ethanolic Extract of Parquetina Nigrescens (Bullock) Leaves on Some Indices of Myocardial Infarction in Isoproterenol Administered Rats. Ph.D. Thesis, Kwara State University, Kwara, Nigeria, 2021; p. 145. [Google Scholar]
- Upaganlawar, A.; Gandhi, C.; Balaraman, R. Effect of Green Tea and Vitamin E Combination in Isoproterenol Induced Myocardial Infarction in Rats. Plant Foods Hum. Nutr. 2009, 64, 75–80. [Google Scholar] [CrossRef]
- Lairez, O.; Cognet, T.; Schaak, S.; Calise, D.; Guilbeau-Frugier, C.; Parini, A.; Mialet-Perez, J. Role of Serotonin 5-HT2A Receptors in the Development of Cardiac Hypertrophy in Response to Aortic Constriction in Mice. J. Neural Transm. 2013, 120, 927–935. [Google Scholar] [CrossRef]
- Chernorudskiy, A.L.; Zito, E. Regulation of Calcium Homeostasis by ER Redox: A Close-Up of the ER/Mitochondria Connection. J. Mol. Biol. 2017, 429, 620–632. [Google Scholar] [CrossRef]
- Paulino, E.T.; Rodrigues, A.K.B.F.; Machado, M.L.D.P.; de Oliveira, K.R.V.; Bernardino, A.C.; Quintans-Júnior, L.J.; Oliveira, A.P.; Ribeiro, Ê.A.N. Alpha-Terpineol Prevents Myocardial Damage against Isoproterenol-MI Induced in Wistar-Kyoto Rats: New Possible to Promote Cardiovascular Integrity. Life Sci. 2022, 290, 120087. [Google Scholar] [CrossRef]
- Hassan, M.Q.; Akhtar, M.S.; Akhtar, M.; Ali, J.; Haque, S.E.; Najmi, A.K. Edaravone, a Potent Free Radical Scavenger and a Calcium Channel Blocker Attenuate Isoproterenol Induced Myocardial Infarction by Suppressing Oxidative Stress, Apoptotic Signaling and Ultrastructural Damage. Ther. Adv. Cardiovasc. Dis. 2016, 10, 214–223. [Google Scholar] [CrossRef]
- Prince, P.S.M.; Dey, P.; Roy, S.J. Sinapic Acid Safeguards Cardiac Mitochondria from Damage in Isoproterenol-Induced Myocardial Infarcted Rats. J. Biochem. Mol. Toxicol. 2020, 34, e22556. [Google Scholar] [CrossRef]
- Dorn, G.W.; Maack, C. SR and Mitochondria: Calcium Cross-Talk between Kissing Cousins. J. Mol. Cell. Cardiol. 2013, 55, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Hemalatha, K.L.; Prince, P.S.M. Preventive Effects of Zingerone on Cardiac Mitochondrial Oxidative Stress, Calcium Ion Overload and Adenosine Triphosphate Depletion in Isoproterenol Induced Myocardial Infarcted Rats. RSC Adv. 2016, 6, 112332–112339. [Google Scholar] [CrossRef]
- Hausenloy, D.J.; Yellon, D.M. Ischaemic Conditioning and Reperfusion Injury. Nat. Rev. Cardiol. 2016, 13, 193–209. [Google Scholar] [CrossRef]
- Chouchani, E.T.; Pell, V.R.; Gaude, E.; Aksentijević, D.; Sundier, S.Y.; Robb, E.L.; Logan, A.; Nadtochiy, S.M.; Ord, E.N.J.; Smith, A.C.; et al. Ischaemic Accumulation of Succinate Controls Reperfusion Injury through Mitochondrial ROS. Nature 2014, 515, 431–435. [Google Scholar] [CrossRef]
- Lesnefsky, E.J.; Chen, Q.; Tandler, B.; Hoppel, C.L. Mitochondrial Dysfunction and Myocardial Ischemia-Reperfusion: Implications for Novel Therapies. Annu. Rev. Pharmacol. Toxicol. 2017, 57, 535–565. [Google Scholar] [CrossRef]
- Waller, D.; Sampson, A.P. Medical Pharmacology & Therapeutics; Elsevier: London, UK, 2018; ISBN 978-0-7020-7193-5. [Google Scholar]
- James, M.R.; Flower, R.J.; Henderson, G.; Loke, Y.K.; MacEwan, D.J.; Rang, H.P. Rang and Dale’s Pharmacology; Elsevier: Edinburgh, UK, 2020; ISBN 978-0-7020-7446-2. [Google Scholar]
- Clemetson, K.J.; Clemetson, J.M. Platelet Receptors. In Platelets; Elsevier: Amsterdam, The Netherlands, 2019; pp. 169–192. ISBN 978-0-12-813456-6. [Google Scholar]
- Vanhoutte, P.M. Serotonin: A Forgotten Signal from the Blood. In Handbook of Behavioral Neuroscience; Elsevier: London, UK, 2020; Volume 31, pp. 393–409. ISBN 978-0-444-64125-0. [Google Scholar]
- Monassier, L.; Maroteaux, L. Serotonin and Cardiovascular Diseases. In Serotonin; Elsevier: London, UK, 2019; pp. 203–238. ISBN 978-0-12-800050-2. [Google Scholar]
- Kaur, G.; Krishan, P. Understanding Serotonin 5-HT2A Receptors-Regulated Cellular and Molecular Mechanisms of Chronic Kidney Diseases. Ren. Replace. Ther. 2020, 6, 25. [Google Scholar] [CrossRef]
- Liu, G.; Ma, C.; Yang, H.; Zhang, P.-Y. Transforming Growth Factor β and Its Role in Heart Disease. Exp. Ther. Med. 2017, 13, 2123–2128. [Google Scholar] [CrossRef]
- Kaludercic, N.; Carpi, A.; Menabò, R.; Lisa, F.D.; Paolocci, N. Monoamine Oxidases (MAO) in the Pathogenesis of Heart Failure and Ischemia/Reperfusion Injury. Biochim. Biophys. Acta 2011, 1813, 1323–1332. [Google Scholar] [CrossRef]
- Sonobe, T.; Akiyama, T.; Du, C.; Pearson, J.T. Serotonin Uptake via Plasma Membrane Monoamine Transporter during Myocardial Ischemia-reperfusion in the Rat Heart in Vivo. Physiol. Rep. 2019, 7, e14297. [Google Scholar] [CrossRef]
- Ardehali, H. Role of the Mitochondrial ATP-Sensitive K+ Channels in Cardioprotection. Acta Biochim. Pol. 2004, 51, 379–390. [Google Scholar] [CrossRef]
- O’Rourke, B. Evidence for Mitochondrial K+ Channels and Their Role in Cardioprotection. Circ. Res. 2004, 94, 420–432. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M. Mitochondrial ATP-Sensitive K+ Channels, Protectors of the Heart. J. Physiol. 2010, 588, 283–286. [Google Scholar] [CrossRef]
- Isoproterenol (Hydrochloride) (CAS 51-30-9). Available online: https://www.caymanchem.com/product/15592 (accessed on 25 February 2023).
- El-Behairy, M.F.; Ahmed, R.M.; Fayed, M.A.A.; Mowafy, S.; Abdallah, I.A. Insights into Flibanserin Oxidative Stress Degradation Pathway: In Silico—In Vitro Toxicity Assessment of Its Degradates. New J. Chem. 2021, 45, 2620–2630. [Google Scholar] [CrossRef]
- Ferger, B.; Shimasaki, M.; Ceci, A.; Ittrich, C.; Allers, K.A.; Sommer, B. Flibanserin, a Drug Intended for Treatment of Hypoactive Sexual Desire Disorder in Pre-Menopausal Women, Affects Spontaneous Motor Activity and Brain Neurochemistry in Female Rats. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2010, 381, 573–579. [Google Scholar] [CrossRef]
- Allers, K.A.; Dremencov, E.; Ceci, A.; Flik, G.; Ferger, B.; Cremers, T.I.F.H.; Ittrich, C.; Sommer, B. ORIGINAL RESEARCH—BASIC SCIENCE: Acute and Repeated Flibanserin Administration in Female Rats Modulates Monoamines Differentially Across Brain Areas: A Microdialysis Study. J. Sex. Med. 2010, 7, 1757–1767. [Google Scholar] [CrossRef]
- Gelez, H.; Clement, P.; Compagnie, S.; Gorny, D.; Laurin, M.; Allers, K.; Sommer, B.; Giuliano, F. Brain Neuronal Activation Induced by Flibanserin Treatment in Female Rats. Psychopharmacology 2013, 230, 639–652. [Google Scholar] [CrossRef]
- El-Deeb, N.K.; El-Tanbouly, D.M.; Khattab, M.A.; EL-Yamany, M.F.; Mohamed, A.F. Crosstalk between PI3K/AKT/KLF4 Signaling and Microglia M1/M2 Polarization as a Novel Mechanistic Approach towards Flibanserin Repositioning in Parkinson’s Disease. Int. Immunopharmacol. 2022, 112, 109191. [Google Scholar] [CrossRef]
- Yang, Q.; Huang, D.D.; Li, D.G.; Chen, B.; Zhang, L.M.; Yuan, C.L.; Huang, H.H. Tetramethylpyrazine Exerts a Protective Effect against Injury from Acute Myocardial Ischemia by Regulating the PI3K/Akt/GSK-3β Signaling Pathway. Cell. Mol. Biol. Lett. 2019, 24, 17. [Google Scholar] [CrossRef]
- Ghasi, S.I.; Umana, I.K.; Ogbonna, A.O.; Nwokike, M.O.; Ufelle, S. Cardioprotective Effects of Animal Grade Piperazine Citrate on Isoproterenol Induced Myocardial Infarction in Wistar Rats: Biochemical and Histopathological Evaluation. Afr. J. Pharm. Pharmacol. 2020, 14, 285–293. [Google Scholar] [CrossRef]
- Meeran, M.F.N.; Azimullah, S.; Adeghate, E.; Ojha, S. Nootkatone Attenuates Myocardial Oxidative Damage, Inflammation, and Apoptosis in Isoproterenol-Induced Myocardial Infarction in Rats. Phytomedicine 2021, 84, 153405. [Google Scholar] [CrossRef] [PubMed]
- Khodeer, D.M.; Zaitone, S.A.; Farag, N.E.; Moustafa, Y.M. Cardioprotective Effect of Pioglitazone in Diabetic and Non-Diabetic Rats Subjected to Acute Myocardial Infarction Involves Suppression of AGE-RAGE Axis and Inhibition of Apoptosis. Can. J. Physiol. Pharmacol. 2016, 94, 463–476. [Google Scholar] [CrossRef] [PubMed]
- Khodeer, D.M.; Bilasy, S.E.; Farag, N.E.; Mehana, A.E.; Elbaz, A.A. Sitagliptin Protects Diabetic Rats with Acute Myocardial Infarction through Induction of Angiogenesis: Role of IGF-1 and VEGF. Can. J. Physiol. Pharmacol. 2019, 97, 1053–1063. [Google Scholar] [CrossRef]
- Elkazzaz, S.K.; Khodeer, D.M.; El Fayoumi, H.M.; Moustafa, Y.M. Role of Sodium Glucose Cotransporter Type 2 Inhibitors Dapagliflozin on Diabetic Nephropathy in Rats; Inflammation, Angiogenesis and Apoptosis. Life Sci. 2021, 280, 119018. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Initial Body Weight (g) | Final Body Weight (g) | Heart Weight (g) | Left Ventricular Weight (g) | Myocardial Weight Index | Left Ventricle Weight Index | |
|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||
| Normal | 123.13 ± 15.76 c | 133.21 ± 17.55 b | 0.51 ± 0.09 b | 0.18 ± 0.03 c | 0.38 ± 0.01 c | 35.13 ± 0.62 b | |
| ISO | 137.12 ± 4.32 bc | 149.78 ± 4.29 ab | 0.70 ± 0.02 a | 0.29 ± 0.02 a | 0.47 ± 0.03 a | 42.09 ± 0.94 a | |
| FLP (15 mg/kg) + ISO | 151.30 ± 5.14 ab | 162.93 ± 5.55 a | 0.71 ± 0.04 a | 0.29 ± 0.03 a | 0.44 ± 0.02 ab | 40.58 ± 2.23 a | |
| FLP (30 mg/kg) + ISO | 162.41 ± 17.94 a | 173.48 ± 19.04 a | 0.71 ± 0.09 a | 0.26 ± 0.04 ab | 0.41 ± 0.01 bc | 37.19 ± 0.98 b | |
| FLP (45 mg/kg) + ISO | 154.13 ± 4.26 ab | 163.44 ± 4.76 a | 0.64 ± 0.01 a | 0.23 ± 0.01 b | 0.39 ± 0.01 c | 35.92 ± 1.00 b | |
| ANOVA | F | 5.708 | 4.877 | 6.491 | 9.965 | 11.89 | 16.715 |
| p | 0.012 * | 0.019 * | 0.008 ** | 0.002 ** | 0.001 *** | <0.001 *** | |
| Group | 5-HT (ng/mL-Serum) | 5-HT (ng/g-Tissue) | Total Ca2+ (mg/dL-Tissue) | |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | ||
| Normal | 87.90 ± 9.02 a | 39.70 ± 1.55 a | 1.7 ± 0.03 c | |
| ISO | 33.00 ± 2.26 e | 15.40 ± 1.10 e | 2.0 ± 0.05 a | |
| FLP (15 mg/kg) + ISO | 43.60 ± 6.70 d | 23.80 ± 0.70 d | 1.8 ± 0.04 b | |
| FLP (30 mg/kg) + ISO | 66.90 ± 4.02 c | 28.70 ± 0.80 c | 1.8 ± 0.03 b | |
| FLP (45 mg/kg) + ISO | 77.50 ± 2.25 b | 33.40 ± 0.04 b | 1.8 ± 0.06 c | |
| ANOVA | F-ratio | 52.024 | 269.747 | 18.74 |
| p-value | <0.001 *** | <0.001 *** | <0.001 *** | |
| Group | 5-HT2A Receptors CT | 5-HT2A Receptors ΔCt | 5-HT2A Receptors ΔΔCT | 5-HT2A Receptors Normalized Fold Change | |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||
| Normal | 28.53 ± 0.55 a | 4.62 ± 0.05 a | 0.00 ± 0.00 a | 0.80 ± 0.40 d | |
| ISO | 23.23 ± 0.55 d | 2.98 ± 0.06 e | −1.64 ± 0.04 e | 2.92 ± 0.40 a | |
| FLP (15 mg/kg) + ISO | 24.70 ± 0.55 c | 3.38 ± 0.06 d | −1.24 ± 0.04 d | 2.16 ± 0.40 b | |
| FLP (30 mg/kg) + ISO | 25.46 ± 0.55 bc | 3.68 ± 0.06 c | −0.94 ± 0.04 c | 1.72 ± 0.40 bc | |
| FLP (45 mg/kg) + ISO | 26.07 ± 0.55 b | 4.00 ± 0.05 b | −0.62 ± 0.02 b | 1.34 ± 0.40 cd | |
| ANOVA | F-ratio | 37.816 | 383.855 | 1119.577 | 12.026 |
| p-value | <0.001 *** | <0.001 *** | <0.001 *** | <0.001 *** | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, M.I.; Abdelrazek, H.M.A.; Moustafa, Y.M.; Alshawwa, S.Z.; Mobasher, M.A.; Abdel-Wahab, B.A.; Abdelgawad, F.E.; Khodeer, D.M. Cardioprotective Effect of Flibanserin against Isoproterenol-Induced Myocardial Infarction in Female Rats: Role of Cardiac 5-HT2A Receptor Gene/5-HT/Ca2+ Pathway. Pharmaceuticals 2023, 16, 502. https://doi.org/10.3390/ph16040502
Ahmed MI, Abdelrazek HMA, Moustafa YM, Alshawwa SZ, Mobasher MA, Abdel-Wahab BA, Abdelgawad FE, Khodeer DM. Cardioprotective Effect of Flibanserin against Isoproterenol-Induced Myocardial Infarction in Female Rats: Role of Cardiac 5-HT2A Receptor Gene/5-HT/Ca2+ Pathway. Pharmaceuticals. 2023; 16(4):502. https://doi.org/10.3390/ph16040502
Chicago/Turabian StyleAhmed, Mohamed I., Heba M. A. Abdelrazek, Yasser M. Moustafa, Samar Z. Alshawwa, Maysa A. Mobasher, Basel A. Abdel-Wahab, Fathy Elsayed Abdelgawad, and Dina M. Khodeer. 2023. "Cardioprotective Effect of Flibanserin against Isoproterenol-Induced Myocardial Infarction in Female Rats: Role of Cardiac 5-HT2A Receptor Gene/5-HT/Ca2+ Pathway" Pharmaceuticals 16, no. 4: 502. https://doi.org/10.3390/ph16040502
APA StyleAhmed, M. I., Abdelrazek, H. M. A., Moustafa, Y. M., Alshawwa, S. Z., Mobasher, M. A., Abdel-Wahab, B. A., Abdelgawad, F. E., & Khodeer, D. M. (2023). Cardioprotective Effect of Flibanserin against Isoproterenol-Induced Myocardial Infarction in Female Rats: Role of Cardiac 5-HT2A Receptor Gene/5-HT/Ca2+ Pathway. Pharmaceuticals, 16(4), 502. https://doi.org/10.3390/ph16040502