
Stable Gastric Pentadecapeptide BPC 157 Therapy: Effect on Reperfusion Following Maintained Intra-Abdominal Hypertension (Grade III and IV) in Rats

 ,
,  , , , ,
, , , ,  , , add
Show full author list
, , add
Show full author list
Abstract
:1. Introduction
2. Results
2.1. A Perilous Syndrome Occurred Peripherally and Centrally
2.1.1. Blood Pressure Disturbances
2.1.2. Thrombosis
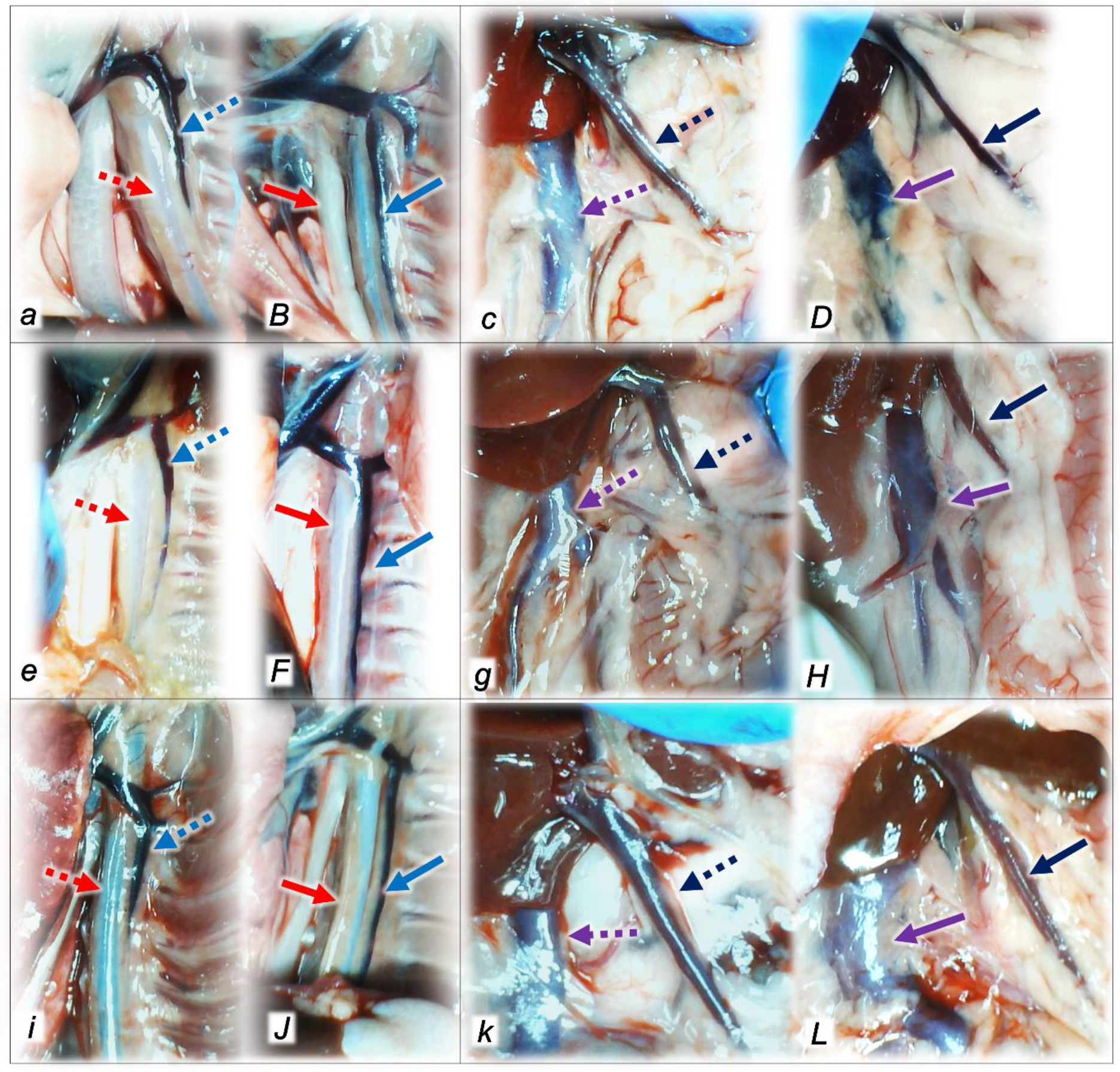
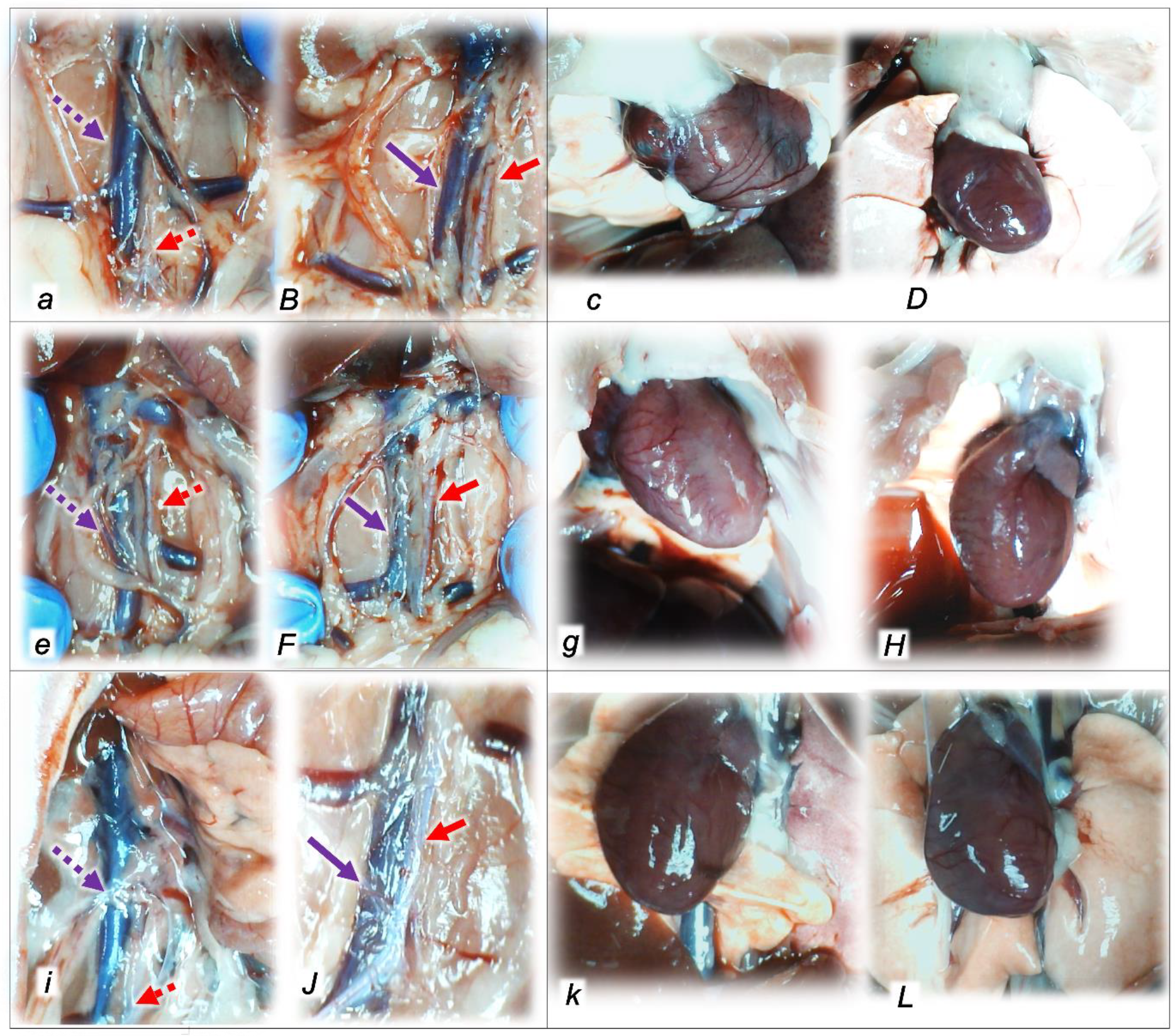
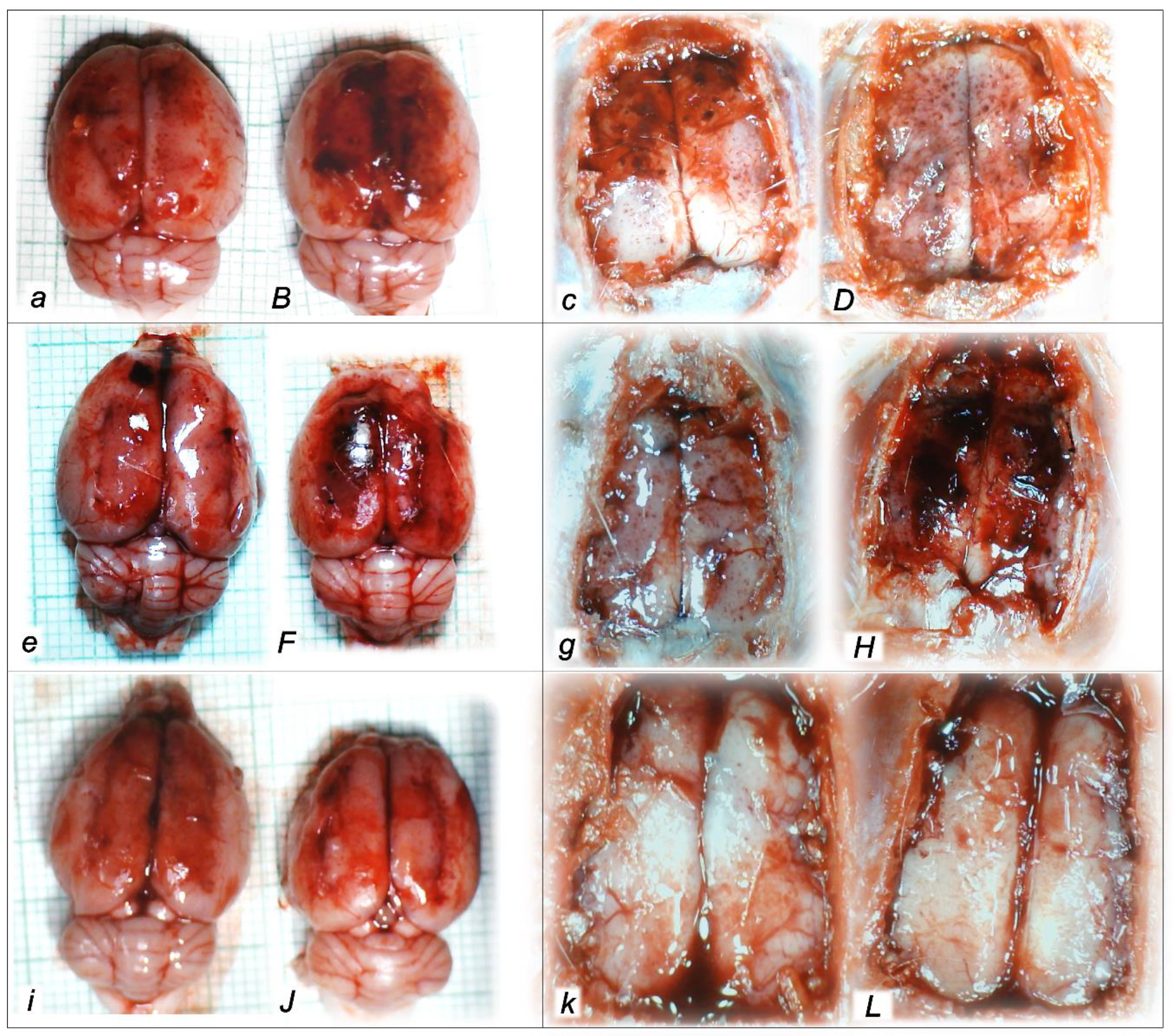
2.1.3. Collateral Pathways, Blood Vessels, and Brain Gross Presentation
2.1.4. Heart and ECG Disturbances
2.1.5. Oxidative Stress
2.2. A Perilous Syndrome Occurred Peripherally
2.2.1. Gastrointestinal, Lung, Liver, Kidney, and Heart Lesions
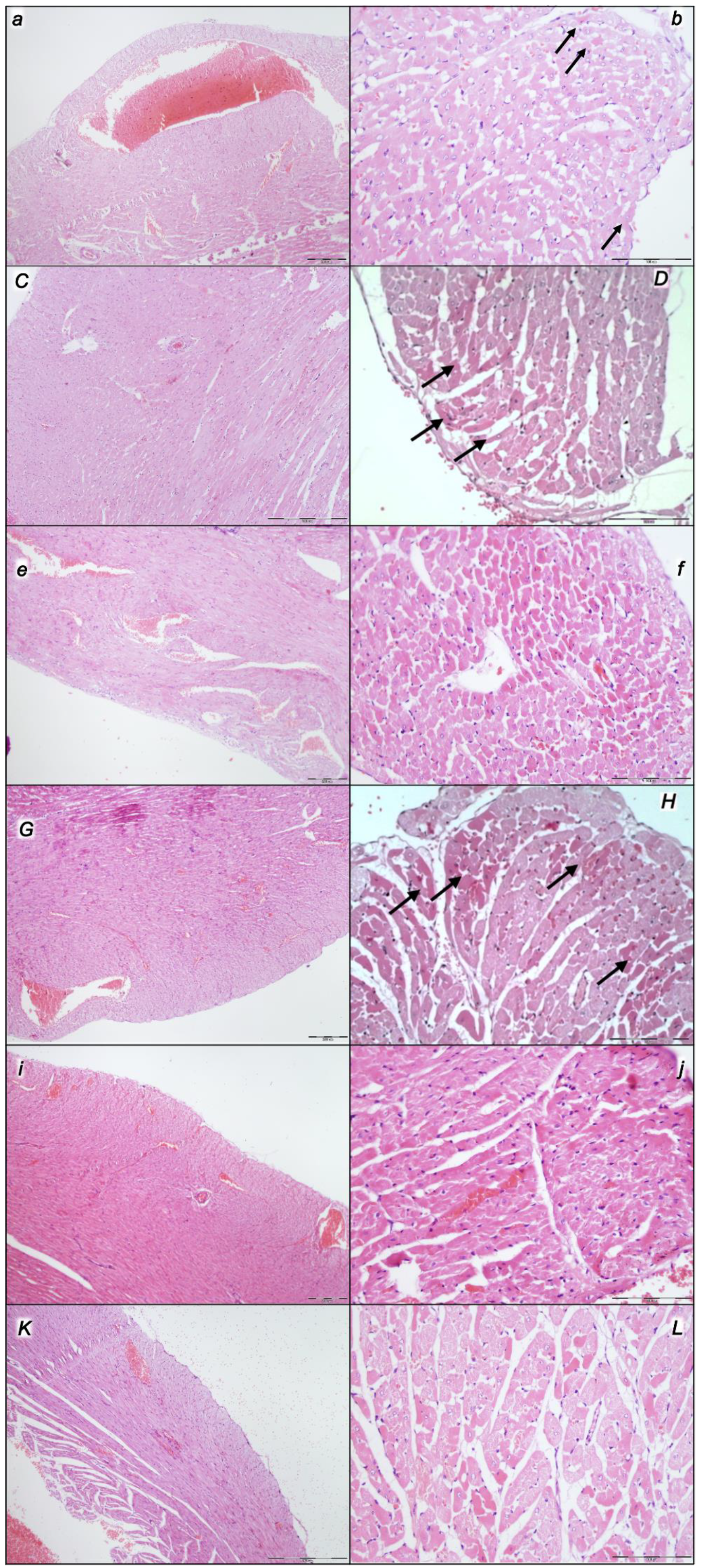
2.2.2. Heart
2.2.3. Lung
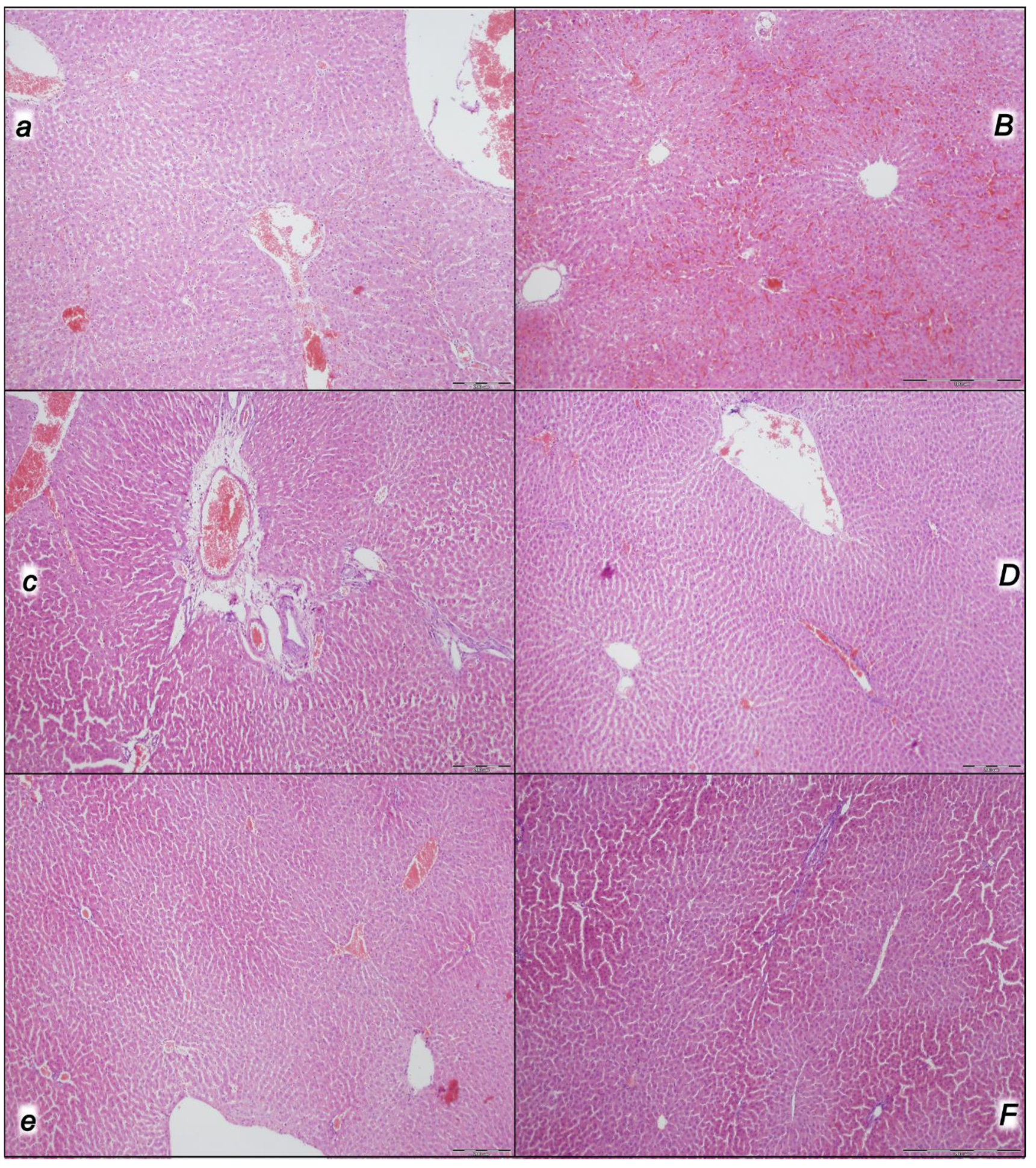
2.2.4. Liver
2.2.5. Kidney
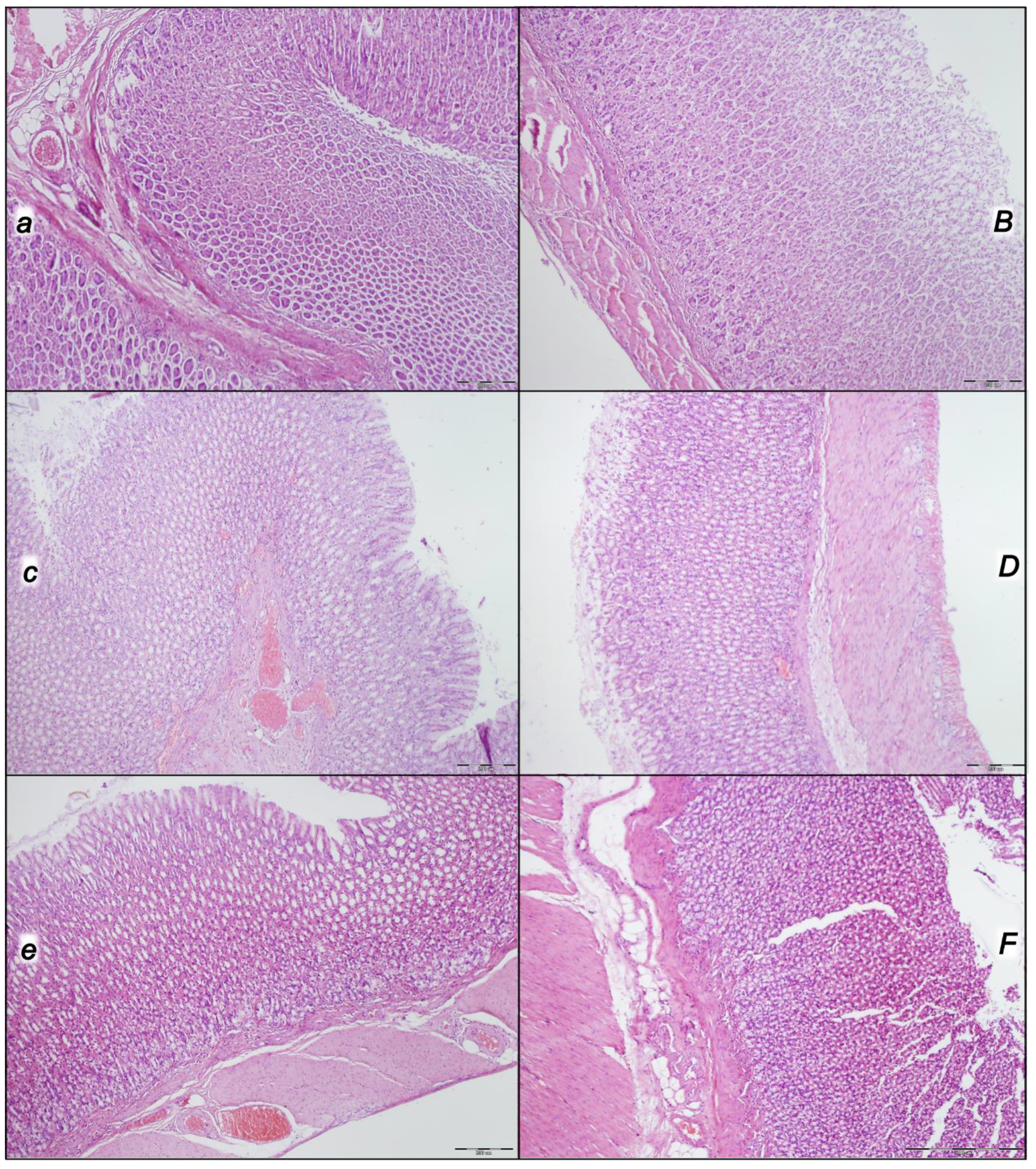
2.2.6. Gastrointestinal Lesion
2.3. A Perilous Syndrome Occurred Centrally
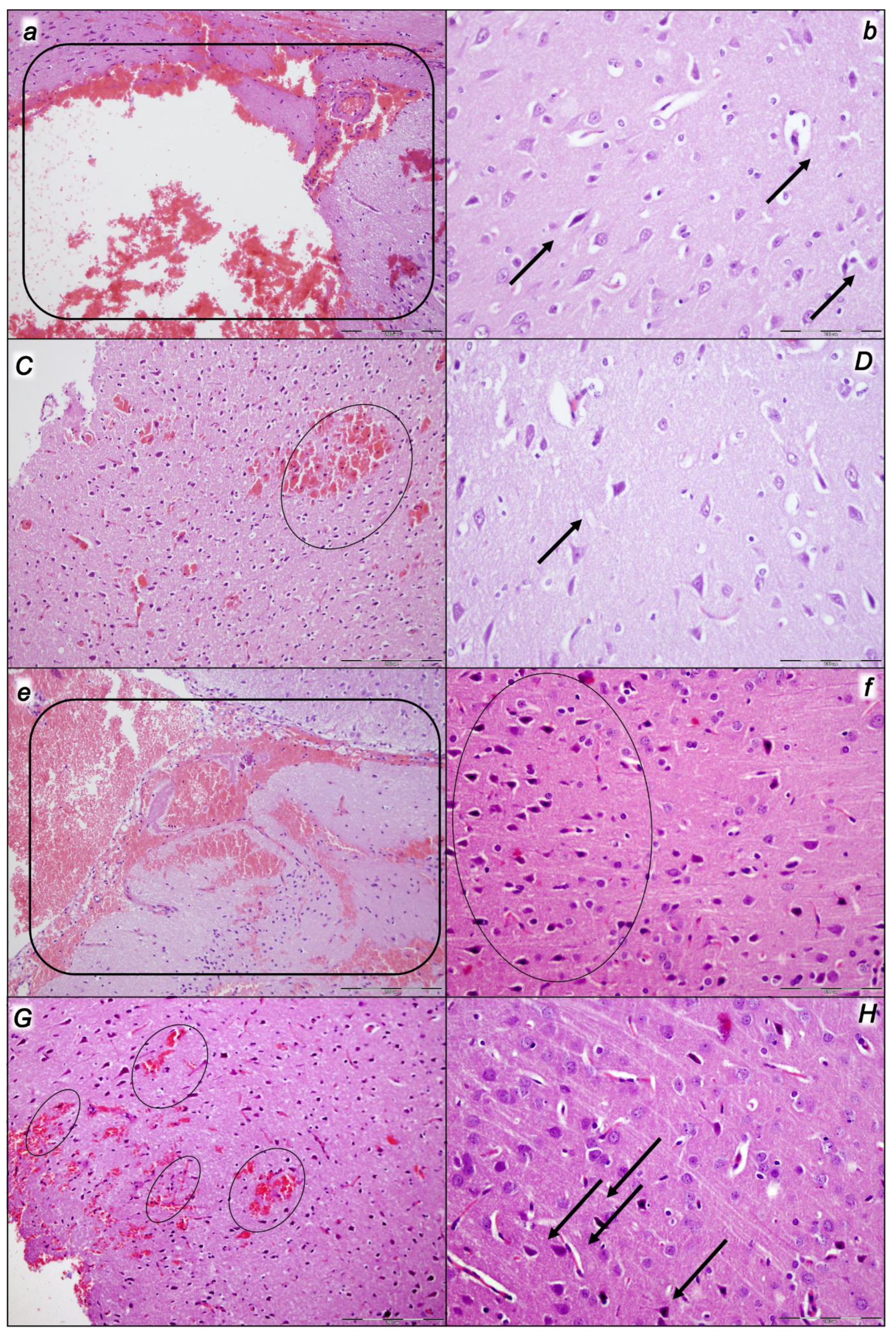
2.3.1. Brain Lesions, Cerebral and Cerebellar Cortex, Hypothalamus/Thalamus, and Hippocampus
2.3.2. Cerebrum
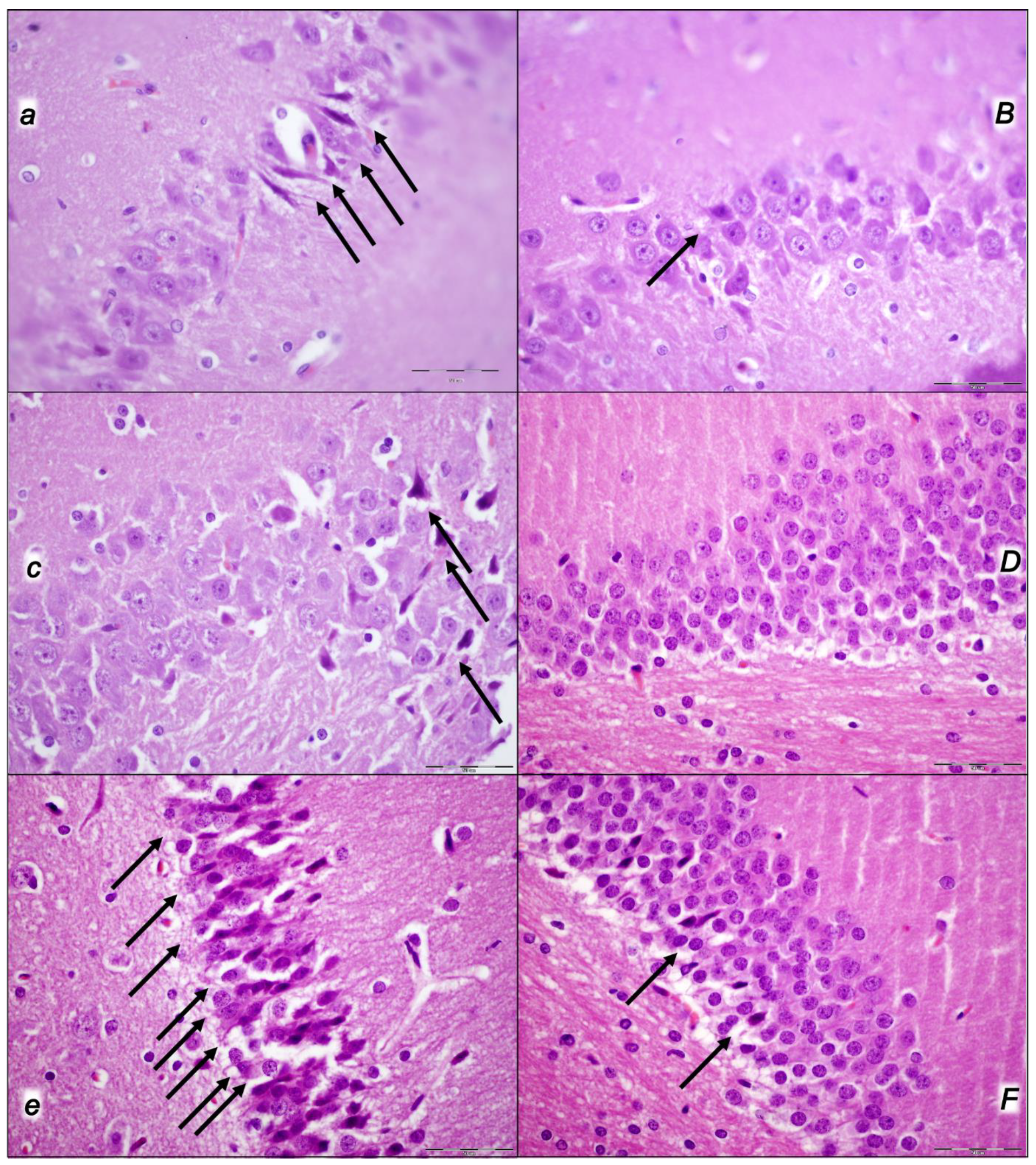
2.3.3. Cerebellum
2.3.4. Hippocampus
2.3.5. Hypothalamus
3. Discussion
4. Materials and Methods
4.1. Animals
4.2. Drugs
4.3. Experimental Protocol
4.4. Superior Sagittal Sinus, Portal, Superior Mesenteric and Caval Vein and Abdominal Aorta: Pressure Recording
4.5. ECG Recording
4.6. Thrombus Assessment
4.7. Brain Volume, Heart Volume, and Vessel Volume Presentation
4.8. Gross Assessment of Gastrointestinal Lesions
4.9. Microscopy
4.9.1. Brain Histology
4.9.2. Lung Histology
4.9.3. Gastrointestinal Histology
4.10. Oxidative Stress
4.11. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Sikiric, P.; Skrtic, A.; Gojkovic, S.; Krezic, I.; Zizek, H.; Lovric, E.; Sikiric, S.; Knezevic, M.; Strbe, S.; Milavic, M.; et al. Cytoprotective gastric pentadecapeptide BPC 157 resolves major vessel occlusion disturbances, ischemia-reperfusion injury following Pringle maneuver, and Budd-Chiari syndrome. World J. Gastroenterol. 2022, 28, 23–46. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Hahm, K.B.; Blagaic, A.B.; Tvrdeic, A.; Pavlov, K.H.; Petrovic, A.; Kokot, A.; Gojkovic, S.; Krezic, I.; Drmic, D.; et al. Stable gastric pentadecapeptide BPC 157, Robert’s stomach cytoprotection/adaptive cytoprotection/organoprotection, and Selye’s stress coping response: Progress, achievements, and the future. Gut Liver 2020, 14, 153–167. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Rucman, R.; Turkovic, B.; Sever, M.; Klicek, R.; Radic, B.; Drmic, D.; Stupnisek, M.; Misic, M.; Vuletic, L.B.; et al. Novel cytoprotective mediator, stable gastric pentadecapeptide BPC 157. Vascular recruitment and gastrointestinal tract healing. Curr. Pharm. Des. 2018, 24, 1990–2001. [Google Scholar] [CrossRef] [PubMed]
- Vukojevic, J.; Milavic, M.; Perovic, D.; Ilic, S.; Zemba Cilic, A.; Duran, N.; Strbe, S.; Zoricic, Z.; Filipcic, I.; Brecic, P.; et al. Pentadecapeptide BPC 157 and the central nervous system. Neural Regen. Res. 2022, 17, 482–487. [Google Scholar] [CrossRef]
- Seiwerth, S.; Milavic, M.; Vukojevic, J.; Gojkovic, S.; Krezic, I.; Vuletic, L.B.; Pavlov, K.H.; Petrovic, A.; Sikiric, S.; Vranes, H.; et al. Stable gastric pentadecapeptide BPC 157 and wound healing. Front. Pharmacol. 2021, 12, 627533. [Google Scholar] [CrossRef] [PubMed]
- Park, J.M.; Lee, H.J.; Sikiric, P.; Hahm, K.B. BPC 157 rescued NSAID-cytotoxicity via stabilizing intestinal permeability and enhancing cytoprotection. Curr. Pharm. Des. 2020, 26, 2971–2981. [Google Scholar] [CrossRef]
- Deek, S.A. BPC 157 as potential treatment for COVID-19. Med. Hypotheses 2021, 158, 110736. [Google Scholar] [CrossRef]
- Tepes, M.; Gojkovic, S.; Krezic, I.; Zizek, H.; Madzar, Z.; Santak, G.; Batelja, L.; Milavic, M.; Sikiric, S.; Kocman, I.; et al. Stable gastric pentadecapeptide BPC 157 therapy for primary abdominal compartment syndrome in rats. Front. Pharmacol. 2021, 12, 718147. [Google Scholar] [CrossRef]
- Vukojevic, J.; Siroglavic, M.; Kasnik, K.; Kralj, T.; Stancic, D.; Kokot, A.; Kolaric, D.; Drmic, D.; Sever, A.Z.; Barisic, I.; et al. Rat inferior caval vein (ICV) ligature and particular new insights with the stable gastric pentadecapeptide BPC 157. Vascul. Pharmacol. 2018, 106, 54–66. [Google Scholar] [CrossRef]
- Kolovrat, M.; Gojkovic, S.; Krezic, I.; Malekinusic, D.; Vrdoljak, B.; Kasnik Kovac, K.; Kralj, T.; Drmic, D.; Barisic, I.; Horvat Pavlov, K.; et al. Pentadecapeptide BPC 157 resolves Pringle maneuver in rats, both ischemia and reperfusion. World J. Hepatol. 2020, 12, 184–206. [Google Scholar] [CrossRef]
- Gojkovic, S.; Krezic, I.; Vrdoljak, B.; Malekinusic, D.; Barisic, I.; Petrovic, A.; Horvat Pavlov, K.; Kolovrat, M.; Duzel, A.; Knezevic, M.; et al. Pentadecapeptide BPC 157 resolves suprahepatic occlusion of the inferior caval vein, Budd-Chiari syndrome model in rats. World J. Gastrointest. Pathophysiol. 2020, 11, 1–19. [Google Scholar] [CrossRef]
- Knezevic, M.; Gojkovic, S.; Krezic, I.; Zizek, H.; Vranes, H.; Malekinusic, D.; Vrdoljak, B.; Knezevic, T.; Pavlov, K.H.; Drmic, D.; et al. Complex syndrome of the complete occlusion of the end of the superior mesenteric vein, opposed with the stable gastric pentadecapeptide BPC 157 in rats. Biomedicines 2021, 9, 1029. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, M.; Gojkovic, S.; Krezic, I.; Zizek, H.; Malekinusic, D.; Vrdoljak, B.; Knezevic, T.; Vranes, H.; Drmic, D.; Staroveski, M.; et al. Occluded superior mesenteric artery and vein. Therapy with the stable gastric pentadecapeptide BPC 157. Biomedicines 2021, 9, 792. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, M.; Gojkovic, S.; Krezic, I.; Zizek, H.; Malekinusic, D.; Vrdoljak, B.; Vranes, H.; Knezevic, T.; Barisic, I.; Horvat Pavlov, K.; et al. Occlusion of the superior mesenteric artery in rats reversed by collateral pathways activation: Gastric pentadecapeptide BPC 157 therapy counteracts multiple organ dysfunction syndrome; intracranial, portal and caval hypertension; and aortal hypotension. Biomedicines 2021, 9, 609. [Google Scholar] [CrossRef] [PubMed]
- Kralj, T.; Kokot, A.; Zlatar, M.; Masnec, S.; Kasnik Kovac, K.; Milkovic Perisa, M.; Batelja Vuletic, L.; Giljanovic, A.; Strbe, S.; Sikiric, S.; et al. Stable gastric pentadecapeptide BPC 157 therapy of rat glaucoma. Biomedicines 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Gojkovic, S.; Krezic, I.; Vranes, H.; Zizek, H.; Drmic, D.; Pavlov, K.H.; Petrovic, A.; Batelja, L.; Milavic, M.; Sikiric, S.; et al. BPC 157 therapy and the permanent occlusion of the superior sagittal sinus in rat. Vascular recruitment. Biomedicines 2021, 9, 744. [Google Scholar] [CrossRef]
- Vukojevic, J.; Vrdoljak, B.; Malekinusic, D.; Siroglavic, M.; Milavic, M.; Kolenc, D.; Boban Blagaic, A.; Bateljam, L.; Drmic, D.; Seiwerth, S.; et al. The effect of pentadecapeptide BPC 157 on hippocampal ischemia/reperfusion injuries in rats. Brain Behav. 2020, 10, e01726. [Google Scholar] [CrossRef]
- Gojkovic, S.; Krezic, I.; Vranes, H.; Zizek, H.; Drmic, D.; Batelja Vuletic, L.; Milavic, M.; Sikiric, S.; Stilinovic, I.; Simeon, P.; et al. Robert’s intragastric alcohol-induced gastric lesion model as an escalated general peripheral and central syndrome, counteracted by the stable gastric pentadecapeptide BPC 157. Biomedicines 2021, 9, 1300. [Google Scholar] [CrossRef]
- Strbe, S.; Gojkovic, S.; Krezic, I.; Zizek, H.; Vranes, H.; Barisic, I.; Strinic, D.; Orct, T.; Vukojevic, J.; Ilic, S.; et al. Over-dose lithium toxicity as an occlusive-like syndrome in rats and gastric pentadecapeptide BPC 157. Biomedicines 2021, 9, 1506. [Google Scholar] [CrossRef]
- Barisic, I.; Balenovic, D.; Udovicic, M.; Bardak, D.; Strinic, D.; Vlainic, J.; Vranes, H.; Smoday, I.M.; Krezic, I.; Milavic, M.; et al. Stable gastric pentadecapeptide BPC 157 may counteract myocardial infarction induced by isoprenaline in rats. Biomedicines 2022, 10, 265. [Google Scholar] [CrossRef]
- Smoday, I.M.; Petrovic, I.; Kalogjera, L.; Vranes, H.; Zizek, H.; Krezic, I.; Gojkovic, S.; Skorak, I.; Hriberski, K.; Brizic, I.; et al. Therapy effect of the stable gastric pentadecapeptide BPC 157 on acute pancreatitis as vascular failure-induced severe peripheral and central syndrome in rats. Biomedicines 2022, 10, 1299. [Google Scholar] [CrossRef]
- Kalogjera, L.; Krezic, I.; Smoday, I.M.; Vranes, H.; Zizek, H.; Yago, H.; Oroz, K.; Vukovic, V.; Kavelj, I.; Novosel, L.; et al. Stomach perforation-induced general occlusion/occlusion-like syndrome and stable gastric pentadecapeptide BPC 157 therapy effect. World J. Gastroenterol. 2023, 29, 4289–4316. [Google Scholar] [CrossRef]
- Premuzic Mestrovic, I.; Smoday, I.M.; Kalogjera, L.; Krezic, I.; Zizek, H.; Vranes, H.; Vukovic, V.; Oroz, K.; Skorak, I.; Brizic, I.; et al. Antiarrhythmic sotalol, occlusion/oOcclusion-like syndrome in rats, and stable gastric pentadecapeptide BPC 157 therapy. Pharmaceuticals 2023, 16, 977. [Google Scholar] [CrossRef] [PubMed]
- Strbe, S.; Smoday, I.M.; Krezic, I.; Kalogjera, L.; Vukovic, V.; Zizek, H.; Gojkovic, S.; Vranes, H.; Barisic, I.; Sikiric, S.; et al. Innate vascular failure by application of neuroleptics, amphetamine, and domperidone rapidly induced severe occlusion/occlusion-like syndromes in rats and stable gastric pentadecapeptide BPC 157 as therapy. Pharmaceuticals 2023, 16, 788. [Google Scholar] [CrossRef]
- Smoday, I.M.; Krezic, I.; Kalogjera, L.; Vukovic, V.; Zizek, H.; Skoro, M.; Kasnik Kovac, K.; Vranes, H.; Barisic, I.; Sikiric, S.; et al. Pentadecapeptide BPC 157 as therapy for inferior caval vein embolization: Recovery of sodium laurate-post-embolization syndrome in rats. Pharmaceuticals 2023, 16, 1507. [Google Scholar] [CrossRef] [PubMed]
- Rajasurya, V.; Surani, S. Abdominal compartment syndrome: Often overlooked conditions in medical intensive care units. World J. Gastroenterol. 2020, 26, 266–278. [Google Scholar] [CrossRef] [PubMed]
- De Laet, I.E.; Malbrain, M.L.N.G.; De Waele, J.J. A clinician’s guide to management of intra-abdominal hypertension and abdominal compartment syndrome in critically ill patients. Crit. Care 2020, 24, 97. [Google Scholar] [CrossRef]
- Malbrain, M.L.; De Laet, I.E.; De Waele, J.J.; Kirkpatrick, A.W. Intra-abdominal hypertension: Definitions, monitoring, interpretation and management. Best Pract. Res. Clin. Anaesthesiol. 2013, 27, 249–270. [Google Scholar] [CrossRef]
- Malbrain, M.L.; De Laet, I.E. Intra-abdominal hypertension: Evolving concepts. Crit. Care Nurs. Clin. N. Am. 2012, 24, 275–309. [Google Scholar] [CrossRef]
- Sikiric, P.; Gojkovic, S.; Krezic, I.; Smoday, I.M.; Kalogjera, L.; Zizek, H.; Oroz, K.; Vranes, H.; Vukovic, V.; Labidi, M.; et al. Stable gastric pentadecapeptide BPC 157 may recover brain–gut axis and gut–brain axis function. Pharmaceuticals 2023, 16, 676. [Google Scholar] [CrossRef]
- Sikiric, P.; Udovicic, M.; Barisic, I.; Balenovic, D.; Zivanovic Posilovic, G.; Strinic, D.; Uzun, S.; Sikiric, S.; Krezic, I.; Zizek, H.; et al. Stable gastric pentadecapeptide BPC 157 as useful cytoprotective peptide therapy in the hearth disturbances, myocardial infarction, heart failure, pulmonary hypertension, arrhythmias, and thrombosis presentation. Biomedicines 2022, 10, 2696. [Google Scholar] [CrossRef] [PubMed]
- Staresinic, M.; Japjec, M.; Vranes, H.; Prtoric, A.; Zizek, H.; Krezic, I.; Gojkovic, S.; Smoday, I.M.; Oroz, K.; Staresinic, E.; et al. Stable gastric pentadecapeptide BPC 157 and striated, smooth, and heart muscle. Biomedicines 2022, 10, 3221. [Google Scholar] [CrossRef]
- Sikiric, P.; Kokot, A.; Kralj, T.; Zlatar, M.; Masnec, S.; Lazic, R.; Loncaric, K.; Oroz, K.; Sablic, M.; Boljesic, M.; et al. Stable gastric pentadecapeptide BPC 157—Possible novel therapy of glaucoma and other ocular conditions. Pharmaceuticals 2023, 16, 1052. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Gojkovic, S.; Knezevic, M.; Tepes, M.; Strbe, S.; Vukojevic, J.; Duzel, A.; Kralj, T.; Krezic, I.; Zizek, H.; et al. Stable gastric pentadecapeptide BPC 157: Prompt particular activation of the collateral pathways. Curr. Med. Chem. 2023, 30, 1568–1573. [Google Scholar] [CrossRef] [PubMed]
- Robert, A. Cytoprotection by prostaglandins. Gastroenterology 1979, 77, 761–767. [Google Scholar] [CrossRef]
- Szabo, S.; Trier, J.S.; Brown, A.; Schnoor, J. Early vascular injury and increased vascular permeability in gastric mucosal injury caused by ethanol in the rat. Gastroenterology 1985, 88, 228–236. [Google Scholar] [CrossRef]
- Perovic, D.; Kolenc, D.; Bilic, V.; Somun, N.; Drmic, D.; Elabjer, E.; Buljat, G.; Seiwerth, S.; Sikiric, P. Stable gastric pentadecapeptide BPC 157 can improve the healing course of spinal cord injury and lead to functional recovery in rats. J. Orthop. Surg. Res. 2019, 14, 199. [Google Scholar] [CrossRef] [PubMed]
- Perovic, D.; Milavic, M.; Dokuzovic, S.; Krezic, I.; Gojkovic, S.; Vranes, H.; Bebek, I.; Bilic, V.; Somun, N.; Brizic, I.; et al. Novel therapeutic effects in rat spinal cord injuries: Recovery of the definitive and early spinal cord injury by the administration of pentadecapeptide BPC 157 therapy. Curr. Issues Mol. Biol. 2022, 44, 1901–1927. [Google Scholar] [CrossRef]
- Duzel, A.; Vlainic, J.; Antunovic, M.; Malekinusic, D.; Vrdoljak, B.; Samara, M.; Gojkovic, S.; Krezic, I.; Vidovic, T.; Bilic, Z.; et al. Stable gastric pentadecapeptide BPC 157 in the treatment of colitis and ischemia and reperfusion in rats: New insights. World J. Gastroenterol. 2017, 23, 8465–8488. [Google Scholar] [CrossRef]
- Sikiric, P.; Seiwerth, S.; Rucman, R.; Turkovic, B.; Rokotov, D.S.; Brcic, L.; Sever, M.; Klicek, R.; Radic, B.; Drmic, D.; et al. Toxicity by NSAIDs: Counteraction by stable gastric pentadecapeptide BPC 157. Curr. Pharm. Des. 2013, 19, 76–83. [Google Scholar]
- Sikiric, P.; Drmic, D.; Boban Blagaic, A.; Tvrdeic, A.; Krezic, I.; Gojkovic, S.; Zizek, H.; Sikiric, S.; Strbe, S.; Smoday, I.M.; et al. Stable gastric pentadecapeptide BPC 157 and NO-system. In Nitric Oxide: From Research to Therapeutics; Ray, A., Gulati, K., Eds.; Advances in Biochemistry in Health and Disease 22; Springer Nature Switzerland AG: Cham, Switzerland, 2023; pp. 349–376. [Google Scholar] [CrossRef]
- Sikiric, P.; Seiwerth, S.; Rucman, R.; Turkovic, B.; Rokotov, D.S.; Brcic, L.; Sever, M.; Klicek, R.; Radic, B.; Drmic, D.; et al. Stable gastric pentadecapeptide BPC 157-NO-system relation. Curr. Pharm. Des. 2014, 20, 1126–1135. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Seiwerth, S.; Grabarevic, Z.; Rucman, R.; Petek, M.; Jagic, V.; Turkovic, B.; Rotkvic, I.; Mise, S.; Zoricic, I.; et al. The influence of a novel pentadecapeptide, BPC 157, on N(G)-nitro-L-arginine methylester and L-arginine effects on stomach mucosa integrity and blood pressure. Eur. J. Pharmacol. 1997, 332, 23–33. [Google Scholar] [CrossRef]
- Turkovic, B.; Sikiric, P.; Seiwerth, S.; Mise, S.; Anic, T.; Petek, M. Stable gastric pentadecapeptide BPC 157 studied for inflammatory bowel disease (PLD-116, PL14736, Pliva) induces nitric oxide synthesis. Gastroenterology 2004, 126, 287. [Google Scholar]
- Stupnisek, M.; Kokot, A.; Drmic, D.; Hrelec Patrlj, M.; Zenko Sever, A.; Kolenc, D.; Radic, B.; Suran, J.; Bojic, D.; Vcev, A.; et al. Pentadecapeptide BPC 157 reduces bleeding and thrombocytopenia after amputation in rats treated with heparin, warfarin, L-NAME and L-arginine. PLoS ONE 2015, 10, e0123454. [Google Scholar] [CrossRef] [PubMed]
- Stupnisek, M.; Franjic, S.; Drmic, D.; Hrelec, M.; Kolenc, D.; Radic, B.; Bojic, D.; Vcev, A.; Seiwerth, S.; Sikiric, P. Pentadecapeptide BPC 157 reduces bleeding time and thrombocytopenia after amputation in rats treated with heparin, warfarin or aspirin. Thromb. Res. 2012, 129, 652–659. [Google Scholar] [CrossRef]
- Konosic, S.; Petricevic, M.; Ivancan, V.; Konosic, L.; Goluza, E.; Krtalic, B.; Drmic, D.; Stupnisek, M.; Seiwerth, S.; Sikiric, P. Intragastric application of aspirin, clopidogrel, cilostazol, and BPC 157 in rats: Platelet aggregation and blood clot. Oxid. Med. Cell Longev. 2019, 2019, 9084643. [Google Scholar] [CrossRef]
- Hsieh, M.J.; Liu, H.T.; Wang, C.N.; Huang, H.Y.; Lin, Y.; Ko, Y.S.; Wang, J.S.; Chang, V.H.; Pang, J.S. Therapeutic potential of pro-angiogenic BPC157 is associated with VEGFR2 activation and up-regulation. J. Mol. Med. 2017, 95, 323–333. [Google Scholar] [CrossRef]
- Hsieh, M.J.; Lee, C.H.; Chueh, H.Y.; Chang, G.J.; Huang, H.Y.; Lin, Y.; Pang, J.S. Modulatory effects of BPC 157 on vasomotor tone and the activation of Src-Caveolin-1-endothelial nitric oxide synthase pathway. Sci. Rep. 2020, 10, 17078. [Google Scholar] [CrossRef]
- Huang, T.; Zhang, K.; Sun, L.; Xue, X.; Zhang, C.; Shu, Z.; Mu, N.; Gu, J.; Zhang, W.; Wang, Y.; et al. Body protective compound-157 enhances alkali-burn wound healing in vivo and promotes proliferation, migration, and angiogenesis in vitro. Drug Des. Dev. Ther. 2015, 9, 2485–2499. [Google Scholar] [CrossRef]
- Huang, B.S.; Huang, S.C.; Chen, F.H.; Chang, Y.; Mei, H.F.; Huang, H.Y.; Chen, W.Y.; Pang, J.S. Pentadecapeptide BPC 157 efficiently reduces radiation-induced liver injury and lipid accumulation through Kruppel-like factor 4 upregulation both in vivo and in vitro. Life Sci. 2022, 310, 121072. [Google Scholar] [CrossRef]
- Chang, C.H.; Tsai, W.C.; Lin, M.S.; Hsu, Y.H.; Pang, J.H.S. The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration. J. Appl. Physiol. 2011, 110, 774–780. [Google Scholar] [CrossRef]
- Chang, C.H.; Tsai, W.C.; Hsu, Y.H.; Pang, J.H.S. Pentadecapeptide BPC 157 enhances the growth hormone receptor expression in tendon fibroblasts. Molecules 2014, 19, 19066–19077. [Google Scholar] [CrossRef]
- Wang, X.Y.; Qu, M.; Duan, R.; Shi, D.; Jin, L.; Gao, J.; Wood, J.D.; Li, J.; Wang, G.D. Cytoprotective mechanism of the novel gastric peptide BPC157 in gastrointestinal tract and cultured enteric neurons and glial cells. Neurosci. Bull. 2019, 35, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Tkalcevic, V.I.; Cuzic, S.; Brajsa, K.; Mildner, B.; Bokulic, A.; Situm, K.; Perovic, D.; Glojnaric, I.; Parnham, M.J. Enhancement by PL 14736 of granulation and collagen organization in healing wounds and the potential role of egr-1 expression. Eur. J. Pharmacol. 2007, 570, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Kang, E.A.; Han, Y.M.; An, J.M.; Park, Y.J.; Sikiric, P.; Kim, D.H.; Kwon, K.A.; Kim, Y.J.; Yang, D.; Tchah, H.; et al. BPC157 as potential agent rescuing from cancer cachexia. Curr. Pharm. Des. 2018, 24, 1947–1956. [Google Scholar] [CrossRef] [PubMed]
- Japjec, M.; Horvat Pavlov, K.; Petrovic, A.; Staresinic, M.; Sebecic, B.; Buljan, M.; Vranes, H.; Giljanovic, A.; Drmic, D.; Japjec, M.; et al. Stable gastric pentadecapeptide BPC 157 as a therapy for the disable myotendinous junctions in rats. Biomedicines 2021, 9, 1547. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Wei, M.; Li, N.; Lu, Q.; Shrestha, S.M.; Tan, J.; Zhang, Z.; Wu, G.; Shi, R. Clopidogrel-induced gastric injury in rats is attenuated by stable gastric pentadecapeptide BPC 157. Drug Des. Dev. Ther. 2020, 14, 5599–5610. [Google Scholar] [CrossRef]
- Gamulin, O.; Oroz, K.; Coric, L.; Krajacic, M.; Skrabic, M.; Dretar, V.; Strbe, S.; Talapko, J.; Juzbasic, M.; Krezic, I.; et al. Fourier transform infrared spectroscopy reveals molecular changes in blood vessels of rats treated with pentadecapeptide BPC 157. Biomedicines 2022, 10, 3130. [Google Scholar] [CrossRef]
- Belosic Halle, Z.; Vlainic, J.; Drmic, D.; Strinic, D.; Luetic, K.; Sucic, M.; Medvidovic-Grubisic, M.; Pavelic Turudic, T.; Petrovic, I.; Seiwerth, S.; et al. Class side effects: Decreased pressure in the lower oesophageal and the pyloric sphincters after the administration of dopamine antagonists, neuroleptics, anti-emetics, L-NAME, pentadecapeptide BPC 157 and L-arginine. Inflammopharmacology 2017, 25, 511–522. [Google Scholar] [CrossRef]
- Luetic, K.; Sucic, M.; Vlainic, J.; Halle, Z.B.; Strinic, D.; Vidovic, T.; Luetic, F.; Marusic, M.; Gulic, S.; Pavelic, T.T.; et al. Cyclophosphamide induced stomach and duodenal lesions as a NO-system disturbance in rats: L-NAME, L-arginine, stable gastric pentadecapeptide BPC 157. Inflammopharmacology 2017, 25, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Sucic, M.; Luetic, K.; Jandric, I.; Drmic, D.; Sever, A.Z.; Vuletic, L.B.; Halle, Z.B.; Strinic, D.; Kokot, A.; Seiwerth, R.S.; et al. Therapy of the rat hemorrhagic cystitis induced by cyclophosphamide. Stable gastric pentadecapeptide BPC 157, L-arginine, L-NAME. Eur. J. Pharmacol. 2019, 861, 172593. [Google Scholar] [CrossRef] [PubMed]
- Sever, A.Z.; Sever, M.; Vidovic, T.; Lojo, N.; Kolenc, D.; Vuletic, L.B.; Drmic, D.; Kokot, A.; Zoricic, I.; Coric, M.; et al. Stable gastric pentadecapeptide BPC 157 in the therapy of the rats with bile duct ligation. Eur. J. Pharmacol. 2019, 847, 130–142. [Google Scholar] [CrossRef] [PubMed]
- Staresinic, M.; Sebecic, B.; Patrlj, L.; Jadrijevic, S.; Suknaic, S.; Perovic, D.; Aralica, G.; Zarkovic, N.; Borovic, S.; Srdjak, M.; et al. Gastric pentadecapeptide BPC 157 accelerates healing of transected rat Achilles tendon and in vitro stimulates tendocytes growth. J. Orthop. Res. 2003, 21, 976–983. [Google Scholar] [CrossRef] [PubMed]
- Eom, B.H.; Lim, H.K.; Tae, N.; Shinn, H.K. Abdominal compartment syndrome caused by gastric distension in bulimia nervosa and fatal injury following surgical decompression—A case report. Anesth. Pain Med. 2020, 15, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Muresan, M.; Muresan, S.; Brinzaniuc, K.; Voidazan, S.; Sala, D.; Jimborean, O.; Hussam, A.H.; Bara, T.; Popescu, G.; Borz, C.; et al. How much does decompressive laparotomy reduce the mortality rate in primary abdominal compartment syndrome? A single-center prospective study on 66 patients. Medicine 2017, 96, e6006. [Google Scholar] [CrossRef] [PubMed]
- De Waele, J.J.; Hoste, E.A.; Malbrain, M.L. Decompressive laparotomy for abdominal compartment syndrome-a critical analysis. Critical Care 2006, 10, R51. [Google Scholar] [CrossRef]
- Rollins, M.D.; Deamorim-Filho, J.; Scaife, E.R.; Hubbard, A.; Barnhart, D.C. Decompressive laparotomy for abdominal compartment syndrome in children on ECMO: Effect on support and survival. J. Pediatr. Surg. 2013, 48, 1509–1513. [Google Scholar] [CrossRef]
- Rmalho, D.; Freitas, J. Drug-induced life-threatening arrhythmias and sudden cardiac death: A clinical perspective of long QT, short QT and Brugada syndromes. Rev. Port. Cardiol. 2018, 37, 435–446. [Google Scholar] [CrossRef]
- Brugada, J.; Gussak, I.; Brugada, P. Short QT syndrome: A predictable story. Cardiology 2014, 128, 231–233. [Google Scholar] [CrossRef]
- Gussak, I.; Brugada, P.; Brugada, J.; Wright, R.S.; Kopecky, S.L.; Chaitman, B.R.; Bjerregaard, P. Idiopathic short QT interval: A new clinical syndrome? Cardiology 2000, 94, 99–102. [Google Scholar] [CrossRef]
- Ramakrishna, H.; O’Hare, M.; Mookadam, F.; Gutsche, J.T.; Shah, R.; Augoustides, J.G. Sudden cardiac death and disorders of the QT interval: Anesthetic implications and focus on perioperative management. J. Cardiothorac. Vasc. Anesth. 2015, 29, 1723–1733. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.R. Drug-induced QT interval shortening: Potential harbinger of proarrhythmia and regulatory perspectives. Br. J. Pharmacol. 2010, 159, 58–69. [Google Scholar] [CrossRef] [PubMed]
- Schimpf, R.; Veltmann, C.; Papavassiliu, T.; Rudic, B.; Göksu, T.; Kuschyk, J.; Wolpert, C.; Antzelevitch, C.; Ebner, A.; Borggrefe, M.; et al. Drug-induced QT interval shortening following antiepileptic treatment with oral rufinamide. Heart Rhythm. 2012, 9, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Drmic, D.; Kolenc, D.; Ilic, S.; Bauk, L.; Sever, M.; Zenko Sever, A.; Luetic, K.; Suran, J.; Seiwerth, S.; Sikiric, P. Celecoxib-induced gastrointestinal, liver and brain lesions in rats, counteraction by BPC 157 or L-arginine, aggravation by L-NAME. World J. Gastroenterol. 2017, 23, 5304–5312. [Google Scholar] [CrossRef]
- Ilic, S.; Drmic, D.; Zarkovic, K.; Kolenc, D.; Coric, M.; Brcic, L.; Klicek, R.; Radic, B.; Sever, M.; Djuzel, V.; et al. High hepatotoxic dose of paracetamol produces generalized convulsions and brain damage in rats. A counteraction with the stable gastric pentadecapeptide BPC 157 (PL 14736). J. Physiol. Pharmacol. 2010, 61, 241–250. [Google Scholar] [PubMed]
- Ilic, S.; Drmic, D.; Franjic, S.; Kolenc, D.; Coric, M.; Brcic, L.; Klicek, R.; Radic, B.; Sever, M.; Djuzel, V.; et al. Pentadecapeptide BPC 157 and its effects on a NSAID toxicity model: Diclofenac-induced gastrointestinal, liver, and encephalopathy lesions. Life Sci. 2011, 88, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Ilic, S.; Drmic, D.; Zarkovic, K.; Kolenc, D.; Brcic, L.; Radic, B.; Djuzel, V.; Blagaic, A.B.; Romic, Z.; Dzidic, S.; et al. Ibuprofen hepatic encephalopathy, hepatomegaly, gastric lesion and gastric pentadecapeptide BPC 157 in rats. Eur. J. Pharmacol. 2011, 667, 322–329. [Google Scholar] [CrossRef]
- Lojo, N.; Rasic, Z.; Sever, A.Z.; Kolenc, D.; Vukusic, D.; Drmic, D.; Zoricic, I.; Sever, M.; Seiwerth, S.; Sikiric, P. Effects of diclofenac, L-NAME, L-arginine, and pentadecapeptide BPC157 on gastrointestinal, liver, and brain lesions, failed anastomosis, and intestinal adaptation deterioration in 24 h-short-bowel rats. PLoS ONE 2016, 11, e0162590. [Google Scholar] [CrossRef]
- Guo, A.W. The search for a magic bullet to fight multiple organ failure secondary to ischemia/reperfusion injury and abdominal compartment syndrome. J. Surg. Res. 2013, 184, 792–793. [Google Scholar] [CrossRef]
- Marinis, A.; Argyra, E.; Lykoudis, P.; Brestas, P.; Theodoraki, K.; Polymeneas, G.; Boviatsis, E.; Voros, D. Ischemia as a possible effect of increased intra-abdominal pressure on central nervous system cytokines, lactate and perfusion pressures. Crit. Care 2010, 14, R31. [Google Scholar] [CrossRef]
- Hamidian Jahromi, A.; Freeland, K.; Youssef, A.M. Intra-abdominal hypertension causes disruption of the blood–brain barrier in mice, which is increased with added severe head trauma. J. Trauma Acute Care Surg. 2012, 73, 1175–1179. [Google Scholar] [CrossRef] [PubMed]
- Youssef, A.M.; Hamidian Jahromi, A.; Vijay, C.G.; Granger, D.N.; Alexander, J.S. Intra-abdominal hypertension causes reversible blood–brain barrier disruption. J. Trauma Acute Care Surg. 2012, 72, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Deigendesch, N.; Wittig, H.; Scheurer, E.; Lenz, C. Tissue sample analysis for post mortem determination of brain edema. Forensic Sci. Int. 2021, 323, 110808. [Google Scholar] [CrossRef] [PubMed]
- Chui, C.J.; McArdle, A.H.; Brown, R.; Scott, H.; Gurd, F. Intestinal mucosal lesion in low-flow states. Arch. Surg. 1970, 101, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Lane, J.S.; Todd, K.E.; Lewis, M.P.; Gloor, B.; Ashley, S.W.; Reber, H.A.; McFadden, D.W.; Chandler, C.F. Interleukin-10 reduces the systemic inflammatory response in a murine model of intestinal ischemia/reperfusion. Surgery 1997, 122, 288–294. [Google Scholar] [CrossRef]
- Balenovic, D.; Bencic, M.L.; Udovicic, M.; Simonji, K.; Hanzevacki, J.S.; Barisic, I.; Kranjcevic, S.; Prkacin, I.; Coric, V.; Brcic, L.; et al. Inhibition of methyldigoxin-induced arrhythmias by pentadecapeptide BPC 157: A relation with NO-system. Regul. Pept. 2009, 156, 83–89. [Google Scholar] [CrossRef]
- Barisic, I.; Balenovic, D.; Klicek, R.; Radic, B.; Nikitovic, B.; Drmic, D.; Udovicic, M.; Strinic, D.; Bardak, D.; Berkopic, L.; et al. Mortal hyperkalemia disturbances in rats are NO-system related. The life saving effect of pentadecapeptide BPC 157. Regul. Pept. 2013, 181, 50–66. [Google Scholar] [CrossRef]
- Stambolija, V.; Stambolija, T.P.; Holjevac, J.K.; Murselovic, T.; Radonic, J.; Duzel, V.; Duplancic, B.; Uzun, S.; Zivanovic-Posilovic, G.; Kolenc, D.; et al. BPC 157: The counteraction of succinylcholine, hyperkalemia, and arrhythmias. Eur. J. Pharmacol. 2016, 781, 83–91. [Google Scholar] [CrossRef]
- Balenovic, D.; Barisic, I.; Prkacin, I.; Horvat, I.; Udovicic, M.; Uzun, S.; Strinic, D.; Pevec, D.; Drmic, D.; Radic, B.; et al. Mortal furosemide-hypokalemia-disturbances in rats NO-system related shorten survival by L-NAME. Therapy benefit with BPC 157 peptide more than with L-arginine. J. Clin. Exp. Cardiolog. 2012, 3, 7. [Google Scholar] [CrossRef]
- Zivanovic-Posilovic, G.; Balenovic, D.; Barisic, I.; Strinic, D.; Stambolija, V.; Udovicic, M.; Uzun, S.; Drmic, D.; Vlainic, J.; Bencic, M.L.; et al. Stable gastric pentadecapeptide BPC 157 and bupivacaine. Eur. J. Pharmacol. 2016, 793, 56–65. [Google Scholar] [CrossRef]
- Lozic, M.; Stambolija, V.; Krezic, I.; Dugandzic, A.; Zivanovic-Posilovic, G.; Gojkovic, S.; Kovacevic, J.; Vrdoljak, L.; Mirkovic, I.; Kokot, A.; et al. In relation to NO-system, stable pentadecapeptide BPC 157 counteracts lidocaine-Induced adverse effects in rats and depolarisation in vitro. Emerg. Med. Int. 2020, 2020, 6805354. [Google Scholar] [CrossRef] [PubMed]
- Lovric-Bencic, M.; Sikiric, P.; Hanzevacki, J.S.; Seiwerth, S.; Rogic, D.; Kusec, V.; Aralica, G.; Konjevoda, P.; Batelja, L.; Blagaic, A.B. Doxorubicine-congestive heart failure-increased big endothelin-1 plasma concentration: Reversal by amlodipine, losartan, and gastric pentadecapeptide BPC157 in rat and mouse. J. Pharmacol. Sci. 2004, 95, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Udovicic, M.; Sever, M.; Kavur, L.; Loncaric, K.; Barisic, I.; Balenovic, D.; Zivanovic Posilovic, G.; Strinic, D.; Uzun, S.; Batelja Vuletic, L.; et al. Stable gastric pentadecapeptide BPC 157 therapy for monocrotaline-induced pulmonary hypertension in rats leads to prevention and reversal. Biomedicines 2021, 9, 822. [Google Scholar] [CrossRef] [PubMed]
- Stancic-Rokotov, D.; Slobodnjak, Z.; Aralica, J.; Aralica, G.; Perovic, D.; Staresinic, M.; Gjurasin, M.; Anic, T.; Zoricic, I.; Buljat, G.; et al. Lung lesions and anti-ulcer agents beneficial effect: Anti-ulcer agents pentadecapeptide BPC 157, ranitidine, omeprazole and atropine ameliorate lung lesion in rats. J. Physiol. Paris 2001, 95, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Grabarevic, Z.; Tisljar, M.; Artukovic, B.; Bratulic, M.; Dzaja, P.; Seiwerth, S.; Sikiric, P.; Peric, J.; Geres, D.; Kos, J. The influence of BPC 157 on nitric oxide agonist and antagonist induced lesions in broiler chicken. J. Physiol. Paris 1997, 91, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Stancic-Rokotov, D.; Sikiric, P.; Seiwerth, S.; Slobodnjak, Z.; Aralica, J.; Aralica, G.; Perovic, D.; Anic, T.; Zoricic, I.; Buljat, G.; et al. Ethanol gastric lesion aggravated by lung injury in rat. Therapy effect of antiulcer agents. J. Physiol. Paris. 2001, 95, 289–293. [Google Scholar] [CrossRef]
- Sikiric, P.; Seiwerth, S.; Grabarevic, Z.; Rucman, R.; Petek, M.; Rotkvic, I.; Turkovic, B.; Jagic, V.; Mildner, B.; Duvnjak, M.; et al. Hepatoprotective effect of BPC 157, a 15-amino acid peptide, on liver lesions induced by either restraint stress or bile duct and hepatic artery ligation or CCl4 administration. A comparative study with dopamine agonists and somatostatin. Life Sci. 1993, 53, PL291–PL296. [Google Scholar] [CrossRef] [PubMed]
- Prkacin, I.; Separovic, J.; Aralica, G.; Perovic, D.; Gjurasin, M.; Lovric-Bencic, M.; Stancic-Rokotov, D.; Staresinic, M.; Anic, T.; Mikus, D.; et al. Portal hypertension and liver lesions in chronically alcohol drinking rats prevented and reversed by stable gastric pentadecapeptide BPC 157 (PL-10, PLD-116), and propranolol, but not ranitidine. J. Physiol. Paris 2001, 95, 315–324. [Google Scholar] [CrossRef]
- Vranes, H.; Krezic, I.; Gojkovic, S.; Zizek, H.; Durasin, T.; Petrovic, A.; Horvat Pavlov, K.; Batelja, L.; Blagaic Boban, A.; Seiwerth, S.; et al. In hydronephrosis-rats, BPC 157 exerts a strong anti-ulcer effect in both stomach and duodenum along with marked kidney recovery. FASEB J. 2020, 34, 1. [Google Scholar] [CrossRef]
- Drmic, D.; Sucic, M.; Zenko Sever, A.; Kolenc, D.; Suran, J.; Seiwerth, S.; Sikiric, P. BPC 157 counteracts gastric lesions after bilateral nephrectomy and attenuates deleterious course in rats. FASEB J. 2015, 29, 628.10. [Google Scholar] [CrossRef]
- Drmic, D.; Sucic, M.; Zenko Sever, A.; Kolenc, D.; Andrijasevic, V.; Suran, J.; Seiwerth, S.; Sikiric, P. Attenuation of the deleterious cause and gastric lesions after bilateral nephrectomy in rats, NO-system relation. BPC 157, L-arginine, L-NAME. FASEB J. 2016, 30, 720.2. [Google Scholar]
- Seiwerth, S.; Rucman, R.; Turkovic, B.; Sever, M.; Klicek, R.; Radic, B.; Drmic, D.; Stupnisek, M.; Misic, M.; Vuletic, L.B.; et al. BPC 157 and standard angiogenic growth factors. Gastrointestinal tract healing, lessons from tendon, ligament, muscle and bone healing. Curr. Pharm. Des. 2018, 24, 1972–1989. [Google Scholar] [CrossRef]
- Tlak Gajger, I.; Ribaric, J.; Smodis Skerl, M.; Vlainic, J.; Sikiric, P. Stable gastric pentadecapeptide BPC 157 in honeybee (Apis mellifera) therapy, to control Nosema ceranae invasions in apiary conditions. J. Vet. Pharmacol. Ther. 2018, 41, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Tlak Gajger, I.; Smodis Skerl, M.I.; Sostaric, P.; Suran, J.; Sikiric, P.; Vlainic, J. Physiological and immunological status of Adult honeybees (Apis mellifera) fed sugar syrup supplemented with pentadecapeptide BPC 157. Biology 2021, 10, 891. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Sun, L.; Ren, F.; Huang, P.; Tian, Z.; Cui, J.; Zhang, W.; Wang, S.; Zhang, K.; He, L.; et al. Preclinical safety evaluation of body protective compound-157, a potential drug for treating various wounds. Regul. Toxicol. Pharmacol. 2020, 114, 104665. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Blood Pressures and Thrombosis in Rats at 60 min, 30 min, and 25 min Following Decompression after Compression with Intra-abdominal Hypertension (25 mmHg/60 min; 30 mmHg/30 min; 40 mmHg/25 min) | |||
|---|---|---|---|
| 60 min (25 mmHg) | 30 min (30 mmHg) | 30 min (40 mmHg) | |
| Superior sagittal sinus pressure, mm Hg, means ± SD | |||
| Control | 7 ± 1 | 8 ± 1 | 7 ± 1 |
| BPC 157 10 μg/kg | −2 ± 1 * | −1 ± 1 * | −1 ± 1 * |
| BPC 157 10 ng/kg | −1 ± 1 * | −1 ± 1 * | −2 ± 1 * |
| Portal pressure, mm Hg, means ± SD | |||
| Control | 17 ± 1 | 17 ± 2 | 18 ± 3 |
| BPC 157 10 μg/kg | 6 ± 1 * | 5 ± 1 * | 6 ± 1 * |
| BPC 157 10 ng/kg | 6 ± 1 * | 5 ± 1 * | 6 ± 1 * |
| Caval pressure, mm Hg, means ± SD | |||
| Control | 10 ± 2 | 11 ± 1 | 12 ± 2 |
| BPC 157 10 μg/kg | 5 ± 1 * | 5 ± 1 * | 5 ± 1 * |
| BPC 157 10 ng/kg | 5 ± 1 * | 5 ± 1 * | 6 ± 1 * |
| Abdominal aorta pressure, mm Hg, means ± SD | |||
| Control | 70 ± 5 | 65 ± 5 | 70 ± 5 |
| BPC 157 10 μg/kg | 100 ± 5 * | 105 ± 7 * | 98 ± 6 * |
| BPC 157 10 ng/kg | 102 ± 7 * | 98 ± 8 * | 100 ± 7 * |
| Superior sagittal sinus, thrombus mass, g, means ± SD | |||
| Control | 0.0019 ± 0.0004 | 0.0021 ± 0.0006 | 0.0042 ± 0.0008 |
| BPC 157 10 μg/kg | 0.0002 ± 0.0001 * | 0.0006 ± 0.0002 * | 0.0003 ± 0.0001 * |
| BPC 157 10 ng/kg | 0.0001 ± 0.0001 * | 0.0007 ± 0.0001 * | 0.0005 ± 0.0002 * |
| Portal vein, thrombus mass, g, means ± SD | |||
| Control | 0.0022 ± 0.0004 | 0.0035 ± 0.0006 | 0.0058 ± 0.0007 |
| BPC 157 10 μg/kg | 0.0005 ± 0.0001 * | 0.0013 ± 0.0003 * | 0.0002 ± 0.0001 * |
| BPC 157 10 ng/kg | 0.0004 ± 0.0001 * | 0.0010 ± 0.0002 * | 0.0004 ± 0.0001 * |
| Inferior caval vein, thrombus mass, g, means ± SD | |||
| Control | 0.0031 ± 0.0004 | 0.0082 ± 0.0004 | 0.0223 ± 0.0014 |
| BPC 157 10 μg/kg | 0.0008 ± 0.0004 * | 0.0015 ± 0.0003 * | 0.0029 ± 0.0005 * |
| BPC 157 10 ng/kg | 0.0006 ± 0.0002 * | 0.0010 ± 0.0004 * | 0.0010 ± 0.0004 * |
| Abdominal aorta, thrombus mass, g, means ± SD | |||
| Control | 0.0019 ± 0.0004 | 0.0022 ± 0.0005 | 0.0061 ± 0.0010 |
| BPC 157 10 μg/kg | 0.0005 ± 0.0001 * | 0.0012 ± 0.0003 * | 0.0011 ± 0.0004 * |
| BPC 157 10 ng/kg | 0.0004 ± 0.0001 * | 0.0010 ± 0.0004 * | 0.0009 ± 0.0002 * |
| The Relative Volume of the Brain, Peripheral Blood Vessels, and Heart in Rats at 60 min, 30 min, and 30 min Following Decompression after Compression with Intra-Abdominal Hypertension (25 mmHg/60 min; 30 mmHg/30 min; 40 mmHg/30 min) | |||
|---|---|---|---|
| 60 min (25 mmHg) | 30 min (30 mmHg) | 30 min (40 mmHg) | |
| Relative volume (control/treated) (%) of the brain, means ± SD | |||
| BPC 157 10 μg/kg | 110 ± 2 * | 129 ± 5 * | 120 ± 2 * |
| BPC 157 10 ng/kg | 111 ± 2 * | 125 ± 2 * | 118 ± 2 * |
| Relative volume (control/treated) (%) of the heart, means ± SD | |||
| BPC 157 10 μg/kg | 112 ± 3 * | 141 ± 9 * | 119 ± 6 * |
| BPC 157 10 ng/kg | 116 ± 3 * | 149 ± 9 * | 122 ± 7 * |
| Relative volume (control/treated) (%) of the azygos vein, means ± SD | |||
| BPC 157 10 μg/kg | 48 ± 5 * | 48 ± 4 * | 58 ± 5 * |
| BPC 157 10 ng/kg | 46 ± 5 * | 50 ± 6 * | 54 ± 5 * |
| Relative volume (control/treated) (%) of the inferior caval vein, means ± SD | |||
| BPC 157 10 μg/kg | 126 ± 5 * | 158 ± 8 * | 124 ± 5 * |
| BPC 157 10 ng/kg | 124 ± 5 * | 152 ± 9 * | 128 ± 8 * |
| Relative volume (control/treated) (%) of the superior mesenteric vein, means ± SD | |||
| BPC 157 10 μg/kg | 256 ± 9 * | 269 ± 9 * | 249 ± 9 * |
| BPC 157 10 ng/kg | 266 ± 7 * | 275 ± 8 * | 255 ± 9 * |
| Relative volume (control/treated) (%) of the brain, ex vivo means ± SD | |||
| BPC 157 10 μg/kg | 115 ± 3 * | 119 ± 2 * | 115 ± 4 * |
| BPC 157 10 ng/kg | 117 ± 3 * | 120 ± 2 * | 117 ± 2 * |
| ECG Changes in Rats after Acute Abdominal Compartment, Course during Reperfusion and after Therapy Application | ||||||
|---|---|---|---|---|---|---|
| Reperfusion assessment time (min) | 0–15 min | |||||
| Time (min) after medication application | 2 min | 5 min | ||||
| 25 mmHg | 30 mmHg | 40 mmHg | 25 mmHg | 30 mmHg | 40 mmHg | |
| Heart frequency, beats/min, means ± SD | ||||||
| Control | 300 ± 10 | 290 ± 10 | 280 ± 10 | 290 ± 10 | 280 ± 10 | 270 ± 10 |
| BPC 157 10 μg/kg | 370 ± 10 * | 380 ± 9 * | 375 ± 9 * | 376 ± 10 * | 378 ± 10 * | 388 ± 8 * |
| BPC 157 10 ng/kg | 378 ± 10 * | 383 ± 8 * | 376 ± 10 * | 386 ± 9 * | 375 ± 9 * | 380 ± 10 * |
| QTc intervals, ms, means ± SD | ||||||
| Control | 170 ± 10 | 165 ± 5 | 165 ± 5 | 170 ± 10 | 165 ± 5 | 165 ± 5 |
| BPC 157 10 μg/kg | 200 ± 10 * | 195 ± 5 * | 199 ± 5 * | 200 ± 10 * | 195 ± 5 * | 199 ± 5 * |
| BPC 157 10 ng/kg | 200 ± 10 * | 197 ± 5 * | 196 ± 5 * | 200 ± 10 * | 197 ± 5 * | 196 ± 5 * |
| ST elevation, mV, means ± SD | ||||||
| Control | 0.2 ± 0.1 | 0.2 ± 0.1 | 0.2 ± 0.1 | 0.2 ± 0.1 | 0.2 ± 0.1 | 0.2 ± 0.1 |
| BPC 157 10 μg/kg | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * |
| BPC 157 10 ng/kg | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * |
| Reperfusion assessment time (min) | 15–30 min | |||||
| Time (min) after medication application | 15 min | 25 min | ||||
| 25 mmHg | 30 mmHg | 40 mmHg | 25 mmHg | 30 mmHg | 40 mmHg | |
| Heart frequency, beats/min, means ± SD | ||||||
| Control | 300 ± 10 | 260 ± 10 | 250 ± 10 | 290 ± 10 | 100 ± 10 | 90 ± 10 |
| BPC 157 10 μg/kg | 376 ± 10 * | 370 ± 10 * | 375 ± 9 * | 386 ± 10 * | 378 ± 10 * | 375 ± 9 * |
| BPC 157 10 ng/kg | 378 ± 10 * | 373 ± 8 * | 380 ± 9 * | 380 ± 9 * | 387 ± 8 * | 380 ± 10 * |
| QTc intervals, ms, means ± SD | ||||||
| Control | 160 ± 10 | 163 ± 5 | 162 ± 5 | 160 ± 10 | 155 ± 5 | 159 ± 5 |
| BPC 157 10 μg/kg | 195 ± 5 * | 200 ± 10 * | 197 ± 5 * | 198 ± 5 * | 195 ± 5 * | 200 ± 10 * |
| BPC 157 10 ng/kg | 200 ± 8 * | 198 ± 5 * | 196 ± 5 * | 199 ± 5 * | 200 ± 10 * | 196 ± 5 * |
| ST elevation, mV, means ± SD | ||||||
| Control | 0.2 ± 0.1 | 0.2 ± 0.1 | 0.2 ± 0.1 | 0.2 ± 0.1 | 0.2 ± 0.1 | 0.2 ± 0.1 |
| BPC 157 10 μg/kg | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * |
| BPC 157 10 ng/kg | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * |
| Reperfusion assessment time (min) | 30–60 min | |||||
| Time (min) after medication application | 40 min | 55 min | ||||
| 25 mmHg | 30 mmHg | 40 mmHg | 25 mmHg | 30 mmHg | 40 mmHg | |
| Heart frequency, beats/min, means ± SD | ||||||
| Control | 250 ± 10 | / | / | 100 ± 10 | / | / |
| BPC 157 10 μg/kg | 386 ± 11 * | / | / | 376 ± 10 * | / | / |
| BPC 157 10 ng/kg | 388 ± 10 * | / | / | 383 ± 9 * | / | / |
| QTc intervals, ms, means ± SD | ||||||
| Control | 160 ± 10 | / | / | 160 ± 10 | / | / |
| BPC 157 10 μg/kg | 200 ± 5 * | / | / | 198 ± 5 * | / | / |
| BPC 157 10 ng/kg | 196 ± 5 * | / | / | 200 ± 5 * | / | / |
| ST elevation, mV, means ± SD | ||||||
| Control | 0.2 ± 0.1 | / | / | 0.2 ± 0.1 | / | / |
| BPC 157 10 μg/kg | 0 ± 0 * | / | / | 0 ± 0 * | / | / |
| BPC 157 10 ng/kg | 0 ± 0 * | / | / | 0 ± 0 * | / | / |
| MDA (Brain, Heart, Lung, Liver, Kidney, Blood, Stomach, Small and Large Intestine) or Macroscopic (Stomach) Values in Rats at 60 min, 30 min, and 30 min Following Decompression after Compression with Intra-Abdominal Hypertension (25 mmHg/60 min; 30 mmHg/30 min; 40 mmHg/25 min) | |||
|---|---|---|---|
| 60 min (25 mmHg) | 30 min (30 mmHg) | 30 min (40 mmHg) | |
| Brain nmol/mg protein, means ± SD | |||
| Control | 8.7 ± 0.5 | 9 ± 0.5 | 10 ± 1.5 |
| BPC 157 10 μg/kg | 6.0 ± 0.3 * | 6.4 ± 0.3 * | 6.5 ± 0.5 * |
| BPC 157 10 ng/kg | 5.5 ± 0.5 * | 6.5 ± 0.5 * | 7.5 ± 0.5 * |
| Heart nmol/mg protein, means ± SD | |||
| Control | 52 ± 5 | 62 ± 5 | 66 ± 8 |
| BPC 157 10 μg/kg | 25 ± 7 * | 28 ± 8 * | 24 ± 5 * |
| BPC 157 10 ng/kg | 22 ± 6 * | 26 ± 6 * | 29 ± 5 * |
| Lung nmol/mg protein, means ± SD | |||
| Control | 62 ± 8 | 66 ± 7 | 60 ± 8 |
| BPC 157 10 μg/kg | 35 ± 8 * | 38 ± 8 * | 29 ± 5 * |
| BPC 157 10 ng/kg | 34 ± 7 * | 31 ± 6 * | 35 ± 5 * |
| Liver, nmol/mg protein, means ± SD | |||
| Control | 42 ± 5 | 45 ± 5 | 46 ± 3 |
| BPC 157 10 μg/kg | 30 ± 3 * | 31 ± 3 * | 30 ± 5 * |
| BPC 157 10 ng/kg | 32 ± 3 * | 32 ± 3 * | 33 ± 5 * |
| Kidney nmol/mg protein, means ± SD | |||
| Control | 25 ± 5 | 28 ± 5 | 46 ± 3 |
| BPC 157 10 μg/kg | 15 ± 3 * | 17 ± 4 * | 30 ± 5 * |
| BPC 157 10 ng/kg | 17 ± 3 * | 14 ± 3 * | 33 ± 5 * |
| Blood (nmol/mg protein Means ± SD) | |||
| Control | 55 ± 5 | 58 ± 8 | 60 ± 7 |
| BPC 157 10 μg/kg | 20 ± 3 * | 18 ± 4 * | 22 ± 5 * |
| BPC 157 10 ng/kg | 16 ± 3 * | 21 ± 5 * | 25 ± 5 * |
| Stomach (nmol/mg protein Means ± SD) | |||
| Control | 2.5 ± 0.5 | 3.5 ± 0.5 | 3.3 ± 0.5 |
| BPC 157 10 μg/kg | 1.0 ± 0.3 * | 1.3 ± 0.3 * | 1.5 ± 0.5 * |
| BPC 157 10 ng/kg | 1.5 ± 0.2 * | 1.4 ± 0.4 * | 1.7 ± 0.5 * |
| Small intestine (nmol/mg protein Means ± SD) | |||
| Control | 3.5 ± 0.5 | 3.3 ± 0.5 | 3.6 ± 0.7 |
| BPC 157 10 μg/kg | 1.0 ± 0.4 * | 1.1 ± 0.3 * | 1.2 ± 0.3 * |
| BPC 157 10 ng/kg | 1.3 ± 0.2 * | 1.5 ± 0.4 * | 1.3 ± 0.4 * |
| Large intestine (nmol/mg protein Means ± SD) | |||
| Control | 2.8 ± 0.5 | 3.1 ± 0.5 | 3.3 ± 0.7 |
| BPC 157 10 μg/kg | 1.0 ± 0.4 * | 1.3 ± 0.3 * | 1.4 ± 0.3 * |
| BPC 157 10 ng/kg | 1.1 ± 0.2 * | 1.2 ± 0.4 * | 1.5 ± 0.4 * |
| Lesions, Scored Microscopically (Heart, Lung, Liver, Kidney, Stomach, Small and Large Intestine), or Macroscopically (Stomach), in Rats at 60 min, 30 min, and 30 min Following Decompression after Compression with Intra-Abdominal Hypertension (25 mmHg/60 min; 30 mmHg/30 min; 40 mmHg/30 min) | |||
|---|---|---|---|
| 60 min (25 mmHg) | 30 min (30 mmHg) | 30 min (40 mmHg) | |
| Heart (scored 0–3, Min/Med/Max) | |||
| Control | 3/3/3 | 3/3/3 | 3/3/3 |
| BPC 157 10 μg/kg | 0/0/0 * | 0/0/0 * | 0/0/0 * |
| BPC 157 10 ng/kg | 0/0/0 * | 0/1/1 * | 0/1/1 * |
| Lung (scored 0–3, Min/Med/Max) | |||
| Control | 3/3/3 | 3/3/3 | 3/3/3 |
| BPC 157 10 μg/kg | 0/0/0 * | 0/0/0 * | 0/0/0 * |
| BPC 157 10 ng/kg | 0/0/0 * | 0/0/0 * | 0/0/0 * |
| Liver (scored 0–3, Min/Med/Max) | |||
| Control | 3/3/3 | 3/3/3 | 3/3/3 |
| BPC 157 10 μg/kg | 0/0/0 * | 0/1/1 * | 0/1/1 * |
| BPC 157 10 ng/kg | 0/0/0 * | 0/1/1 * | 0/1/1 * |
| Kidney (scored 0–3, Min/Med/Max) | |||
| Control | 3/3/3 | 3/3/3 | 3/3/3 |
| BPC 157 10 μg/kg | 0/0/0 * | 0/1/1 * | 0/1/1 * |
| BPC 157 10 ng/kg | 0/0/0 * | 0/1/1 * | 0/1/1 * |
| Stomach (sum of longest diameters, mm, means ± SD) | |||
| Control | 3/3/3 | 3/3/3 | 3/3/3 |
| BPC 157 10 μg/kg | 0/0/0 * | 0/0/0 * | 0/0/0 * |
| BPC 157 10 ng/kg | 0/0/0 * | 0/0/0 * | 0/0/0 * |
| Stomach (scored 0–15, Min/Med/Max) | |||
| Control | 3/3/3 | 3/3/3 | 3/3/3 |
| BPC 157 10 μg/kg | 0/0/0 * | 0/0/0 * | 0/0/0 * |
| BPC 157 10 ng/kg | 0/0/0 * | 0/0/0 * | 0/0/0 * |
| Small intestine (scored 0–15, Min/Med/Max) | |||
| Control | 3/3/3 | 3/3/3 | 3/3/3 |
| BPC 157 10 μg/kg | 0/0/0 * | 0/0/0 * | 0/0/0 * |
| BPC 157 10 ng/kg | 0/0/0 * | 0/0/0 * | 0/0/0 * |
| Lesions, Scored Microscopically Cerebrum, Cerebellum, Hypothalamus, and Hippocampus in Rats at 60 min (i), or 30 min (ii, iii) Following Decompression after Compression with Intra-Abdominal Hypertension (25 mmHg/60min (i); 30 mmHg/30min (ii); 40 mmHg/30min (iii) | |||
|---|---|---|---|
| 60 min (25 mmHg) | 30 min (30 mmHg) | 30 min (40 mmHg) | |
| Cerebrum (scored 0–8, Min/Med/Max) # | |||
| Control | 2/3/3 | 3/3/3 | 3/3/3 |
| BPC 157 10 μg/kg | 0/1/1 * | 0/1/1 * | 0/1/1 * |
| BPC 157 10 ng/kg | 0/1/1 * | 0/1/1 * | 0/1/1 * |
| Neuronal damage in the karyopyknotic areas, %, means ± SD (10 HPF, 400×) | |||
| Control | 56 ± 5 | 64 ± 5 | 69 ± 5 |
| BPC 157 10 μg/kg | 14 ± 1 * | 18 ± 1 * | 15 ± 1 * |
| BPC 157 10 ng/kg | 16 ± 1 * | 14 ± 1 * | 17 ± 1 * |
| Hemorrhage (% of total area) | |||
| Control | 20 ± 3 | 30 ± 3 | 35 ± 3 |
| BPC 157 10 μg/kg | 2 ± 1 * | 5 ± 2 * | 5 ± 1 * |
| BPC 157 10 ng/kg | 2 ± 1 * | 6 ± 2 * | 7 ± 1 * |
| Edema (scored 0–3, Min/Med/Max) | |||
| Control | 2/3/3 | 3/3/3 | 3/3/3 |
| BPC 157 10 μg/kg | 0/1/1 * | 0/1/1 * | 0/1/1 * |
| BPC 157 10 ng/kg | 0/1/1 * | 0/1/1 * | 0/1/1 * |
| Cerebellum (scored 0–8, Min/Med/Max) | |||
| Control | 2/2/2 | 2/2/2 | 3/3/3 |
| BPC 157 10 μg/kg | 0/1/1 * | 0/1/1 * | 0/1/1 * |
| BPC 157 10 ng/kg | 0/1/1 * | 0/1/1 * | 0/1/1 * |
| Neuronal damage in the karyopyknotic areas, %, means ± SD (10 HPF, 400×) | |||
| Control | 55 ± 5 | 61 ± 4 | 73 ± 5 |
| BPC 157 10 μg/kg | 12 ± 3 * | 16 ± 2 * | 24 ± 3 * |
| BPC 157 10 ng/kg | 15 ± 3 * | 14 ± 2 * | 22 ± 4 * |
| Hemorrhage (% of total area) | |||
| Control | 0 ± 0 | 0 ± 0 | 0 ± 0 |
| BPC 157 10 μg/kg | 0 ± 0 | 0 ± 0 | 0 ± 0 |
| BPC 157 10 ng/kg | 0 ± 0 | 0 ± 0 | 0 ± 0 |
| Edema (scored 0–3, Min/Med/Max) | |||
| Control | 2/3/3 | 2/3/3 | 3/3/3 |
| BPC 157 10 μg/kg | 0/1/1 * | 0/1/1 * | 0/1/1 * |
| BPC 157 10 ng/kg | 0/1/1 * | 0/1/1 * | 0/1/1 * |
| Hippocampus (scored 0–8, Min/Med/Max) | |||
| Control | 2/3/3 | 2/3/3 | 2/3/3 |
| BPC 157 10 μg/kg | 0/1/1 * | 0/1/1 * | 0/1/1 * |
| BPC 157 10 ng/kg | 0/1/1 * | 0/1/1 * | 0/1/1 * |
| Neuronal damage in the karyopyknotic areas, %, means ± SD (10 HPF, 400×) | |||
| Control | 24 ± 3 | 25 ± 3 | 43 ± 5 |
| BPC 157 10 μg/kg | 2 ± 1 * | 4 ± 1 * | 12 ± 2 * |
| BPC 157 10 ng/kg | 3 ± 1 * | 3 ± 1 * | 14 ± 2 * |
| Hemorrhage (% of total area) | |||
| Control | 0 ± 0 | 0 ± 0 | 0 ± 0 |
| BPC 157 10 μg/kg | 0 ± 0 | 0 ± 0 | 0 ± 0 |
| BPC 157 10 ng/kg | 0 ± 0 | 0 ± 0 | 0 ± 0 |
| Edema (scored 0–3, Min/Med/Max) | |||
| Control | 2/2/3 | 2/2/3 | 2/3/3 |
| BPC 157 10 μg/kg | 0/0/0 * | 0/0/0 * | 0/0/0 * |
| BPC 157 10 ng/kg | 0/0/0 * | 0/0/0 * | 0/0/0 * |
| Hypothalamus (scored 0–8, Min/Med/Max) | |||
| Control | 3/3/3 | 3/3/3 | 3/3/3 |
| BPC 157 10 μg/kg | 0/1/1 * | 0/1/1 * | 0/1/1 * |
| BPC 157 10 ng/kg | 0/1/1 * | 0/1/1 * | 0/1/1 * |
| Neuronal damage in the karyopyknotic areas, %, means ± SD (10 HPF, 400×) | |||
| Control | 83 ± 4 | 96 ± 4 | 94 ± 6 |
| BPC 157 10 μg/kg | 21 ± 2 * | 32 ± 2 * | 43 ± 3 * |
| BPC 157 10 ng/kg | 24 ± 2 * | 35 ± 2 * | 40 ± 3 * |
| Hemorrhage (% of total area) | |||
| Control | 20 ± 2 | 25 ± 5 | 25 ± 2 |
| BPC 157 10 μg/kg | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * |
| BPC 157 10 ng/kg | 0 ± 0 * | 0 ± 0 * | 0 ± 0 * |
| Edema (scored 0–3, Min/Med/Max) | |||
| Control | 2/3/3 | 3/3/3 | 3/3/3 |
| BPC 157 10 μg/kg | 0/1/1 * | 0/1/1 * | 0/1/1 * |
| BPC 157 10 ng/kg | 0/1/1 * | 0/1/1 * | 0/1/1 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tepes, M.; Krezic, I.; Vranes, H.; Smoday, I.M.; Kalogjera, L.; Zizek, H.; Vukovic, V.; Oroz, K.; Kovac, K.K.; Madzar, Z.; et al. Stable Gastric Pentadecapeptide BPC 157 Therapy: Effect on Reperfusion Following Maintained Intra-Abdominal Hypertension (Grade III and IV) in Rats. Pharmaceuticals 2023, 16, 1554. https://doi.org/10.3390/ph16111554
Tepes M, Krezic I, Vranes H, Smoday IM, Kalogjera L, Zizek H, Vukovic V, Oroz K, Kovac KK, Madzar Z, et al. Stable Gastric Pentadecapeptide BPC 157 Therapy: Effect on Reperfusion Following Maintained Intra-Abdominal Hypertension (Grade III and IV) in Rats. Pharmaceuticals. 2023; 16(11):1554. https://doi.org/10.3390/ph16111554
Chicago/Turabian StyleTepes, Marijan, Ivan Krezic, Hrvoje Vranes, Ivan Maria Smoday, Luka Kalogjera, Helena Zizek, Vlasta Vukovic, Katarina Oroz, Katarina Kasnik Kovac, Zrinko Madzar, and et al. 2023. "Stable Gastric Pentadecapeptide BPC 157 Therapy: Effect on Reperfusion Following Maintained Intra-Abdominal Hypertension (Grade III and IV) in Rats" Pharmaceuticals 16, no. 11: 1554. https://doi.org/10.3390/ph16111554
APA StyleTepes, M., Krezic, I., Vranes, H., Smoday, I. M., Kalogjera, L., Zizek, H., Vukovic, V., Oroz, K., Kovac, K. K., Madzar, Z., Rakic, M., Miskic, B., Sikiric, S., Barisic, I., Strbe, S., Antunovic, M., Novosel, L., Kavelj, I., Vlainic, J., ... Sikiric, P. (2023). Stable Gastric Pentadecapeptide BPC 157 Therapy: Effect on Reperfusion Following Maintained Intra-Abdominal Hypertension (Grade III and IV) in Rats. Pharmaceuticals, 16(11), 1554. https://doi.org/10.3390/ph16111554