


Simultaneous Quantification of Seven Antifungal Agents in Human Serum Using Liquid Chromatography-Tandem Mass Spectrometry

Abstract
:
1. Introduction
2. Results and Discussion
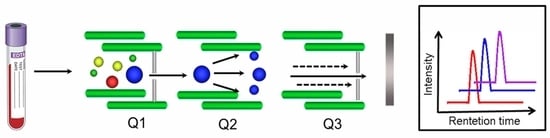
2.1. Method Establishment
2.2. Method Validation
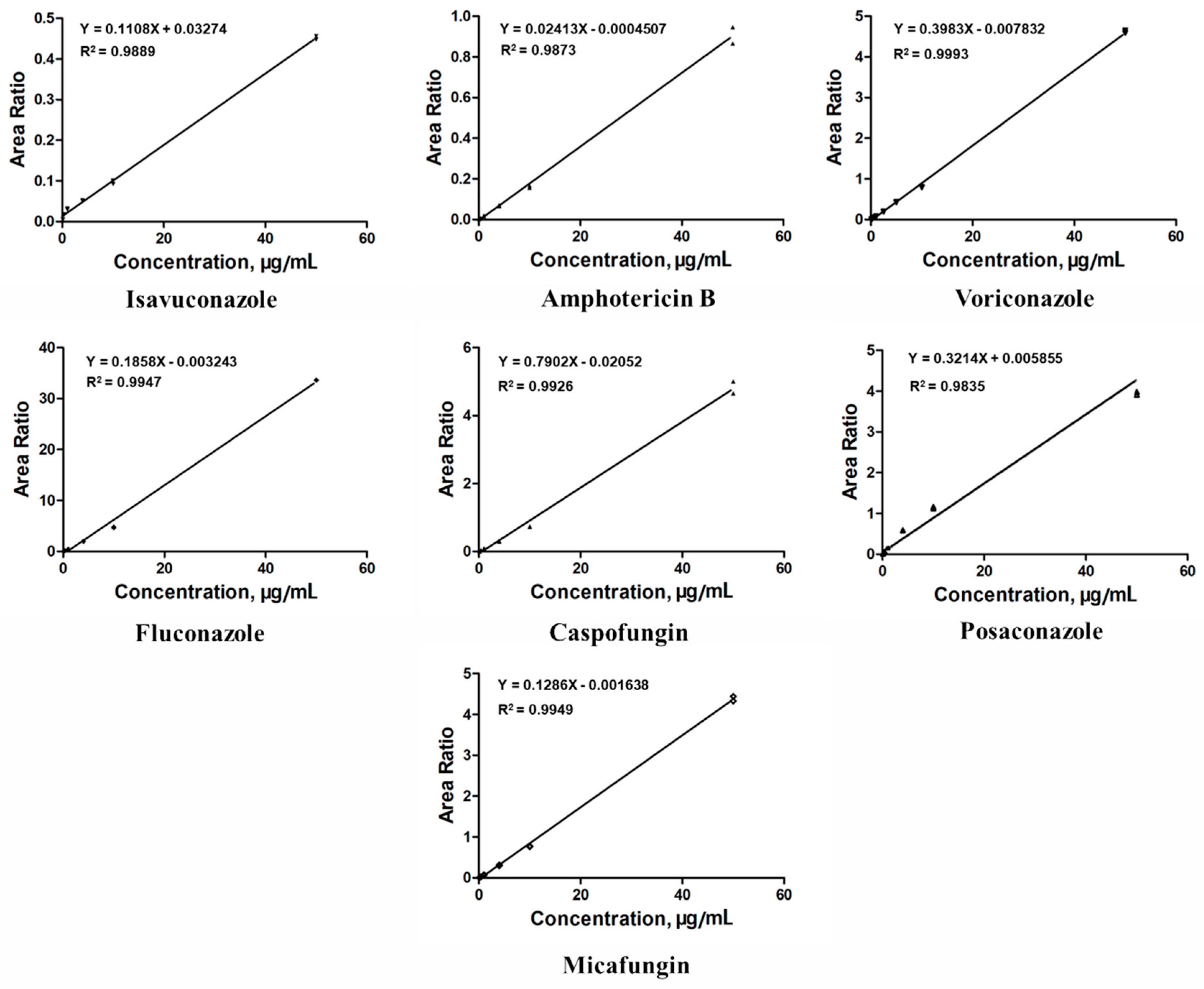
2.2.1. Linearity, Precision, and Accuracy
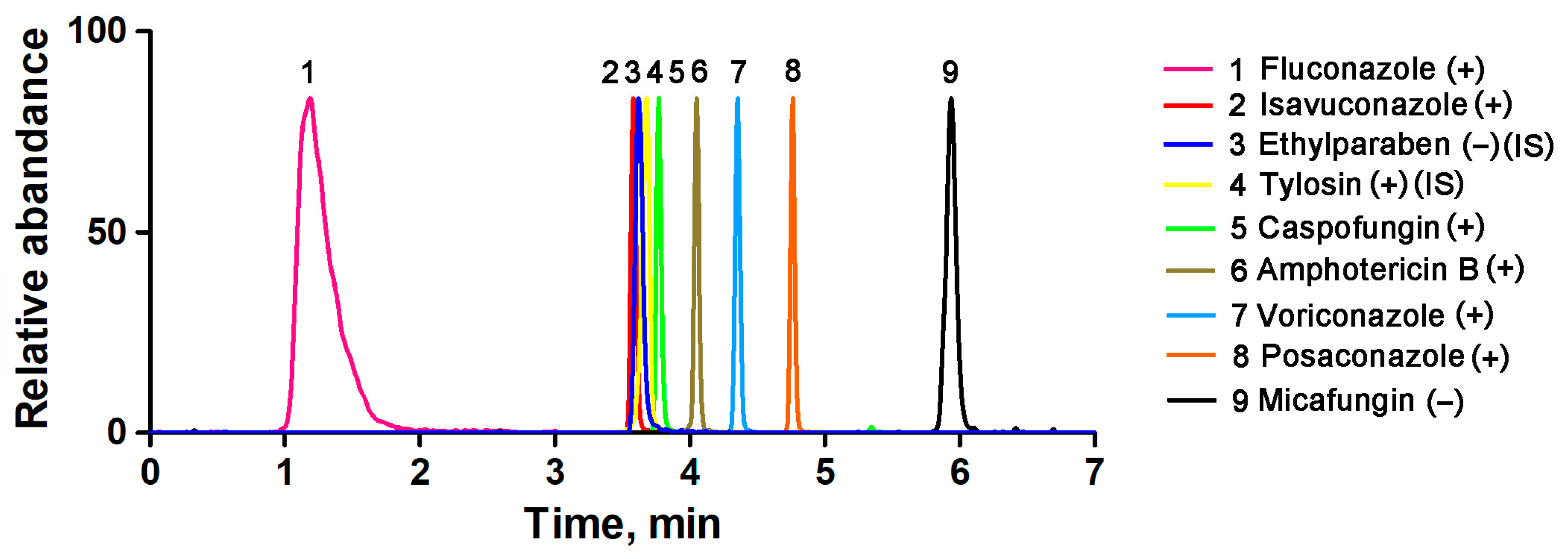
2.2.2. Specificity and Selectivity
2.2.3. Extraction Recovery and Matrix Effect
2.2.4. Stability
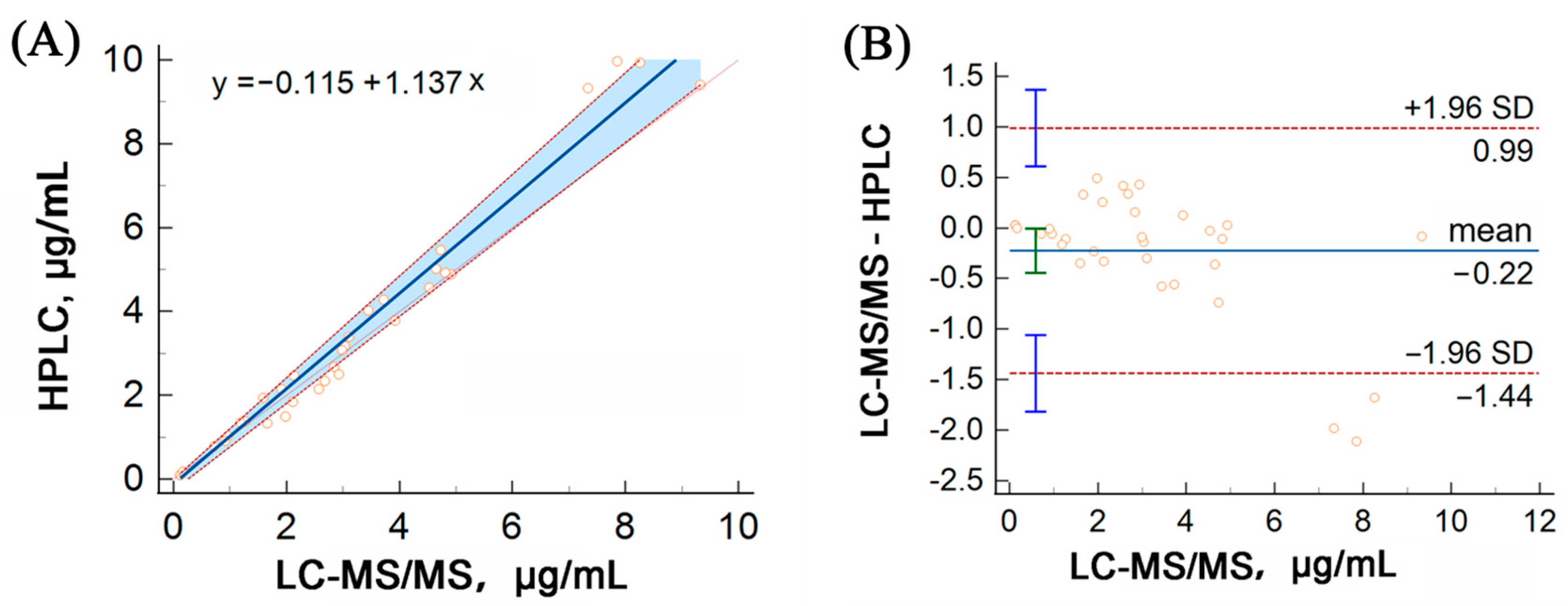
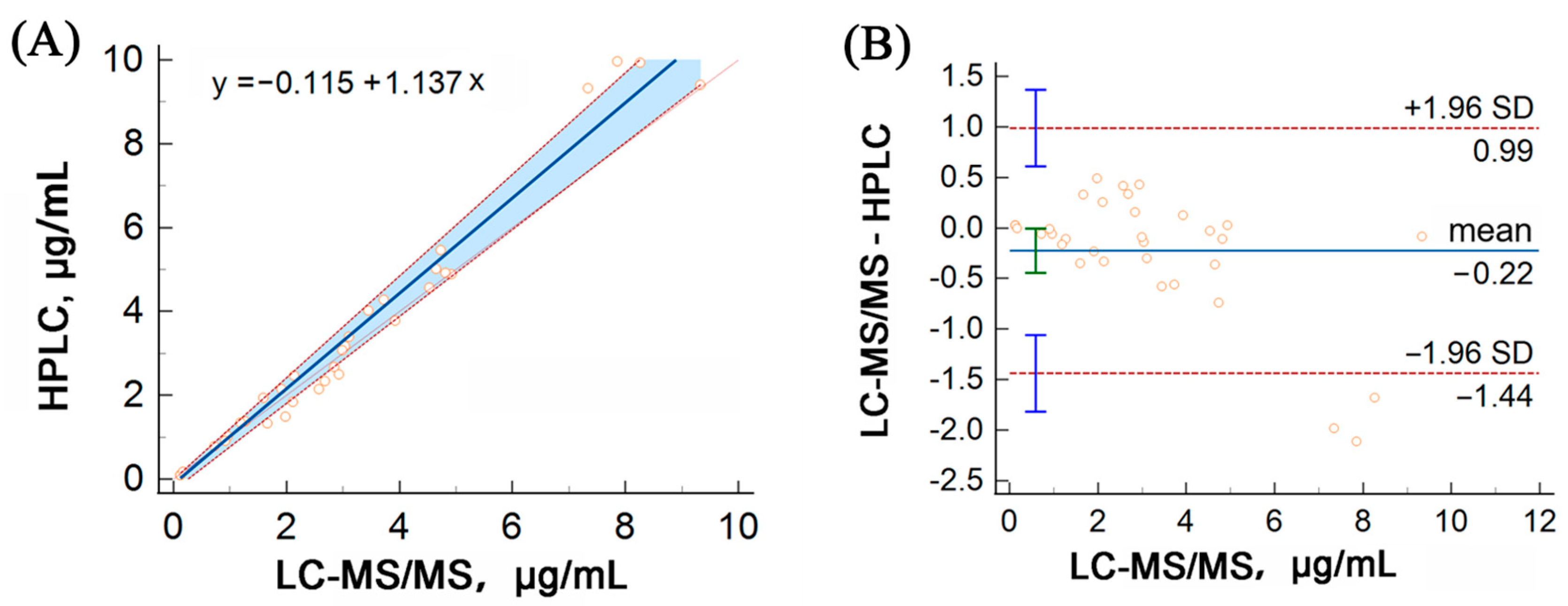
2.3. HPLC Validation
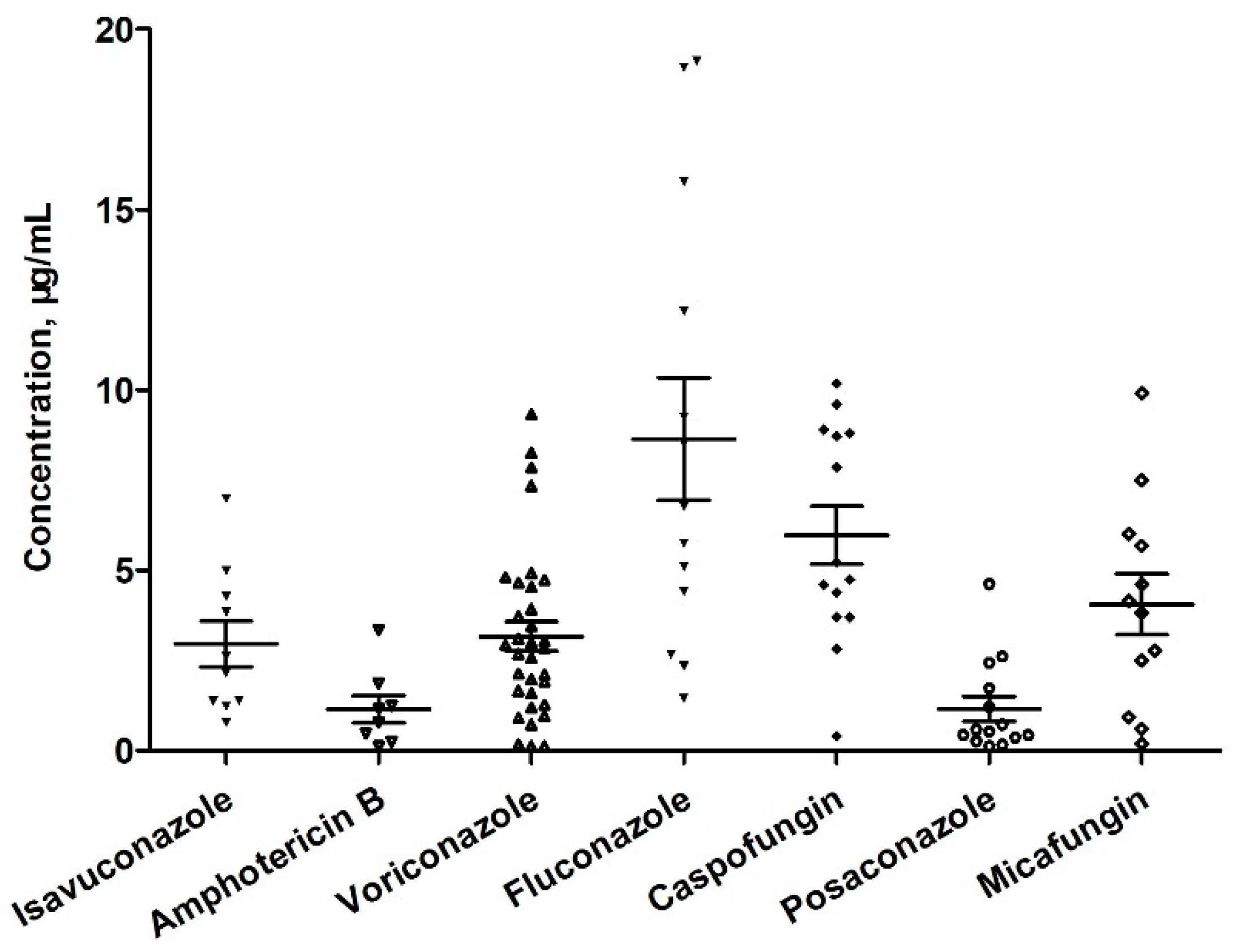
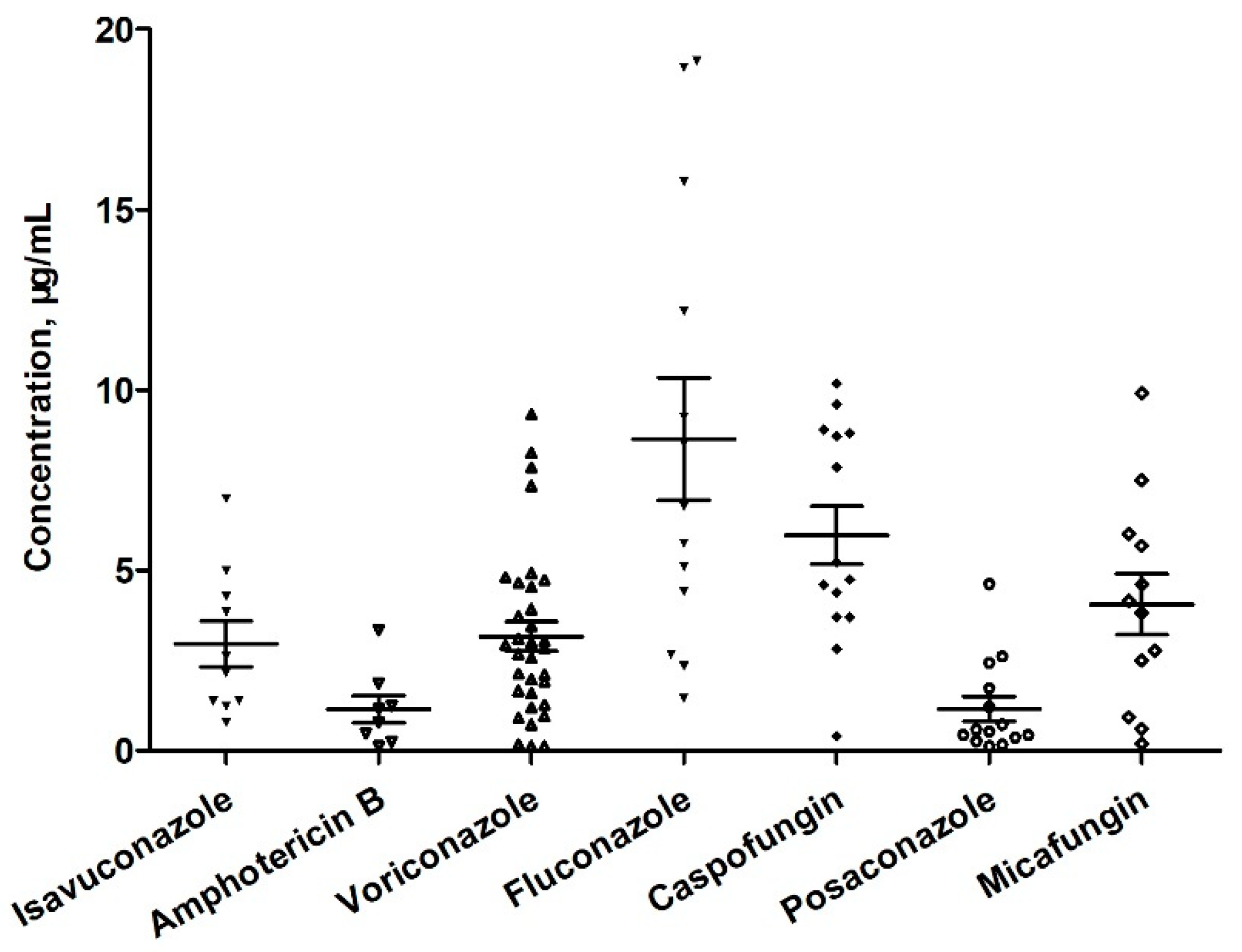
2.4. Application
2.5. Comparison with Reported Methods
3. Materials and Methods
3.1. Chemicals and Reagents
3.2. Serum Sample Collection
3.3. Sample Preparation
3.4. Chromatographic and Mass Spectrometric Conditions
3.5. Preparation of Stock Solutions, Calibrations, and Quality Controls
3.6. Method Validation
3.6.1. Linearity
3.6.2. Accuracy and Precision
3.6.3. Selectivity
3.6.4. Matrix Effect and Extraction Recovery
3.6.5. Stability
3.7. Statistical Analysis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef]
- Bassetti, M.; Azoulay, E.; Kullberg, B.-J.; Ruhnke, M.; Shoham, S.; Vazquez, J.; Giacobbe, D.R.; Calandra, T. EORTC/MSGERC Definitions of Invasive Fungal Diseases: Summary of Activities of the Intensive Care Unit Working Group. Clin. Infect. Dis. 2021, 72, S121–S127. [Google Scholar] [CrossRef] [PubMed]
- Neoh, C.F.; Jeong, W.; Kong, D.C.; Slavin, M.A. The Antifungal Pipeline for Invasive Fungal Diseases: What Does the Future Hold? Expert. Rev. Anti Infect. Ther. 2023, 21, 577–594. [Google Scholar] [CrossRef] [PubMed]
- Azoulay, E.; Russell, L.; Van de Louw, A.; Metaxa, V.; Bauer, P.; Povoa, P.; Montero, J.G.; Loeches, I.M.; Mehta, S.; Puxty, K.; et al. Diagnosis of Severe Respiratory Infections in Immunocompromised Patients. Intensive Care Med. 2020, 46, 298–314. [Google Scholar] [CrossRef]
- Adembri, C.; Villa, G.; Rosi, E.; Tofani, L.; Fallani, S.; De Gaudio, A.R.; Novelli, A. Caspofungin PK in Critically Ill Patients after the First and Fourth Doses: Suggestions for Therapeutic Drug Monitoring? J. Chemother. 2020, 32, 124–131. [Google Scholar] [CrossRef]
- Bellmann, R.; Smuszkiewicz, P. Pharmacokinetics of Antifungal Drugs: Practical Implications for Optimized Treatment of Patients. Infection 2017, 45, 737–779. [Google Scholar] [CrossRef]
- Payne, K.D.; Hall, R.G. Dosing of Antifungal Agents in Obese People. Expert Rev. Anti-Infect. Ther. 2016, 14, 257–267. [Google Scholar] [CrossRef]
- Asín-Prieto, E.; Rodríguez-Gascón, A.; Isla, A. Applications of the Pharmacokinetic/Pharmacodynamic (PK/PD) Analysis of Antimicrobial Agents. J. Infect. Chemother. 2015, 21, 319–329. [Google Scholar] [CrossRef]
- Gómez-López, A. Antifungal Therapeutic Drug Monitoring: Focus on Drugs without a Clear Recommendation. Clin. Microbiol. Infect. 2020, 26, 1481–1487. [Google Scholar] [CrossRef]
- Ceesay, M.M.; Couchman, L.; Smith, M.; Wade, J.; Flanagan, R.J.; Pagliuca, A. Triazole Antifungals Used for Prophylaxis and Treatment of Invasive Fungal Disease in Adult Haematology Patients: Trough Serum Concentrations in Relation to Outcome. Med. Mycol. 2016, 54, 691–698. [Google Scholar] [CrossRef]
- Sanz-Codina, M.; Bozkir, H.Ö.; Jorda, A.; Zeitlinger, M. Individualized Antimicrobial Dose Optimization: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Clin. Microbiol. Infect. 2023, 29, 845–857. [Google Scholar] [CrossRef] [PubMed]
- Marr, K.A.; Schlamm, H.T.; Herbrecht, R.; Rottinghaus, S.T.; Bow, E.J.; Cornely, O.A.; Heinz, W.J.; Jagannatha, S.; Koh, L.P.; Kontoyiannis, D.P.; et al. Combination Antifungal Therapy for Invasive Aspergillosis: A Randomized Trial. Ann. Intern. Med. 2015, 162, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Baddley, J.W.; Pappas, P.G. Antifungal Combination Therapy: Clinical Potential. Drugs 2005, 65, 1461–1480. [Google Scholar] [CrossRef] [PubMed]
- Molloy, S.F.; Kanyama, C.; Heyderman, R.S.; Loyse, A.; Kouanfack, C.; Chanda, D.; Mfinanga, S.; Temfack, E.; Lakhi, S.; Lesikari, S.; et al. Antifungal Combinations for Treatment of Cryptococcal Meningitis in Africa. N. Engl. J. Med. 2018, 378, 1004–1017. [Google Scholar] [CrossRef]
- Ngan, N.T.T.; Thanh Hoang Le, N.; Vi Vi, N.N.; Van, N.T.T.; Mai, N.T.H.; Van Anh, D.; Trieu, P.H.; Lan, N.P.H.; Phu, N.H.; Chau, N.V.V.; et al. An Open Label Randomized Controlled Trial of Tamoxifen Combined with Amphotericin B and Fluconazole for Cryptococcal Meningitis. eLife 2021, 10, e68929. [Google Scholar] [CrossRef]
- Peña-Lorenzo, D.; Rebollo, N.; Sánchez-Hernández, J.G.; Zarzuelo-Castañeda, A. Comparison of Ultra-Performance Liquid Chromatography and ARK Immunoassay for Therapeutic Drug Monitoring of Voriconazole. Ann. Clin. Biochem. 2021, 58, 657–660. [Google Scholar] [CrossRef]
- Li, X.; Li, W.; Li, M.; Zhang, Z.; Liu, S.; Chen, Z. Correlation between Enzyme Multiplied Immunoassay Technique and High-performance Liquid Chromatography in the Quantification of Voriconazole in a Paediatric Population. Scand. J. Clin. Lab. Investig. 2021, 81, 121–126. [Google Scholar] [CrossRef]
- Barco, S.; Mesini, A.; Barbagallo, L.; Maffia, A.; Tripodi, G.; Pea, F.; Saffioti, C.; Castagnola, E.; Cangemi, G. A Liquid Chromatography-Tandem Mass Spectrometry Platform for the Routine Therapeutic Drug Monitoring of 14 Antibiotics: Application to Critically Ill Pediatric Patients. J. Pharm. Biomed. Anal. 2020, 186, 113273. [Google Scholar] [CrossRef]
- Ferrari, D.; Ripa, M.; Premaschi, S.; Banfi, G.; Castagna, A.; Locatelli, M. LC-MS/MS Method for Simultaneous Determination of Linezolid, Meropenem, Piperacillin and Teicoplanin in Human Plasma Samples. J. Pharm. Biomed. Anal. 2019, 169, 11–18. [Google Scholar] [CrossRef]
- Cendejas-Bueno, E.; Forastiero, A.; Rodriguez-Tudela, J.L.; Cuenca-Estrella, M.; Gomez-Lopez, A. HPLC/UV or Bioassay: Two Valid Methods for Posaconazole Quantification in Human Serum Samples. Clin. Microbiol. Infect. 2012, 18, 1229–1235. [Google Scholar] [CrossRef]
- Nannetti, G.; Pagni, S.; Palù, G.; Loregian, A. A Sensitive and Validated HPLC-UV Method for the Quantitative Determination of the New Antifungal Drug Isavuconazole in Human Plasma. Biomed. Chromatogr. 2018, 32, e4333. [Google Scholar] [CrossRef] [PubMed]
- Oyaert, M.; Peersman, N.; Kieffer, D.; Deiteren, K.; Smits, A.; Allegaert, K.; Spriet, I.; Van Eldere, J.; Verhaegen, J.; Vermeersch, P.; et al. Novel LC-MS/MS Method for Plasma Vancomycin: Comparison with Immunoassays and Clinical Impact. Clin. Chim. Acta 2015, 441, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Pan, M.; Ke, H.; Liang, J.; Liang, W.; Yu, P.; Zhang, P.; Wang, Q. An LC-MS/MS Method for the Simultaneous Determination of 18 Antibacterial Drugs in Human Plasma and Its Application in Therapeutic Drug Monitoring. Front. Pharmacol. 2022, 13, 1044234. [Google Scholar] [CrossRef] [PubMed]
- Lamoth, F.; Lewis, R.E.; Kontoyiannis, D.P. Investigational Antifungal Agents for Invasive Mycoses: A Clinical Perspective. Clin. Infect. Dis. 2022, 75, 534–544. [Google Scholar] [CrossRef]
- Liu, L.; Zhang, L.; Zheng, X.; Liu, X.; Liu, W.; Wu, J. LC-MS/MS-Based Multiplex Antibacterial Platform for Therapeutic Drug Monitoring in Intensive Care Unit Patients. Front. Pharmacol. 2023, 14, 1116071. [Google Scholar] [CrossRef]
- King, R.; Bonfiglio, R.; Fernandez-Metzler, C.; Miller-Stein, C.; Olah, T. Mechanistic investigation of ionization suppression in electrospray ionization. J. Am. Soc. Mass. Spectrom. 2000, 11, 942–950. [Google Scholar] [CrossRef]
- Gu, H.; Liu, G.; Wang, J.; Aubry, A.-F.; Arnold, M.E. Selecting the Correct Weighting Factors for Linear and Quadratic Calibration Curves with Least-Squares Regression Algorithm in Bioanalytical LC-MS/MS Assays and Impacts of Using Incorrect Weighting Factors on Curve Stability, Data Quality, and Assay Performance. Anal. Chem. 2014, 86, 8959–8966. [Google Scholar] [CrossRef]
- Yan, M.; Wu, Z.-F.; Tang, D.; Wang, F.; Xiao, Y.-W.; Xu, P.; Zhang, B.-K.; Liu, Y.-P.; Xiang, D.-X.; Banh, H.L. The Impact of Proton Pump Inhibitors on the Pharmacokinetics of Voriconazole In Vitro and In Vivo. Biomed. Pharmacother. 2018, 108, 60–64. [Google Scholar] [CrossRef]
- Patterson, T.F.; Thompson, G.R.; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef]
- Xiao, Y.; Xu, Y.-K.; Pattengale, P.; O’Gorman, M.R.; Fu, X. A Rapid High-Performance LC-MS/MS Method for Therapeutic Drug Monitoring of Voriconazole, Posaconazole, Fluconazole, and Itraconazole in Human Serum. J. Appl. Lab. Med. 2017, 1, 626–636. [Google Scholar] [CrossRef]
- Smith, A.; Dowis, J.; French, D. Quantification of Serum Voriconazole, Isavuconazole, and Posaconazole by Liquid Chromatography Tandem Mass Spectrometry (LC-MS/MS). Curr. Protoc. Toxicol. 2018, 76, e47. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.J.; Lee, K.; Oh, J.; Woo, H.I.; Lee, S.-Y. Experience with Therapeutic Drug Monitoring of Three Antifungal Agents Using an LC-MS/MS Method in Routine Clinical Practice. Clin. Biochem. 2019, 70, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Müller, C.; Gehlen, D.; Blaich, C.; Prozeller, D.; Liss, B.; Streichert, T.; Wiesen, M.H.J. Reliable and Easy-To-Use Liquid Chromatography-Tandem Mass Spectrometry Method for Simultaneous Analysis of Fluconazole, Isavuconazole, Itraconazole, Hydroxy-Itraconazole, Posaconazole, and Voriconazole in Human Plasma and Serum. Ther. Drug Monit. 2017, 39, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Matuszewski, B.K.; Constanzer, M.L.; Chavez-Eng, C.M. Strategies for the Assessment of Matrix Effect in Quantitative Bioanalytical Methods Based on HPLC-MS/MS. Anal. Chem. 2003, 75, 3019–3030. [Google Scholar] [CrossRef]
- FDA. Bioanalytical Method Validation Guidance for Industry; FDA: Silver Spring, MD, USA, 2018.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compound | Retention Time (min) | Molecular Weight | Precursor Ion (m/z) | Product Ion (m/z) | Collision Energy (eV) | Dwell Time (msec) | Linear Range (μg/mL) | IS |
|---|---|---|---|---|---|---|---|---|
| Isavuconazole | 3.60 | 716.74 | 717.20 | 236.15 | −10 | 20 | 0.1–50 | VOR-IS |
| 165.10 | −10 | 20 | ||||||
| Amphotericin B | 4.05 | 924.08 | 906.50 | 743.50 | −10 | 20 | 0.1–50 | VOR-IS |
| 725.40 | −10 | 20 | ||||||
| Voriconazole | 4.37 | 349.31 | 350.20 | 281.20 | −5 | 20 | 0.1–50 | VOR-IS |
| 127.20 | −5 | 20 | ||||||
| Fluconazole | 1.29 | 306.27 | 307.10 | 220.10 | −19 | 20 | 0.1–50 | Tylosin |
| 238.10 | −5 | 20 | ||||||
| Caspofungin | 3.78 | 1093.31 | 547.40 | 137.10 | −30 | 20 | 0.1–50 | Tylosin |
| 131.10 | −26 | 20 | ||||||
| Posaconazole | 4.76 | 700.78 | 701.30 | 614.30 | −36 | 20 | 0.1–50 | VOR-IS |
| 344.20 | −47 | 20 | ||||||
| Micafungin | 6.02 | 1270.27 | 1268.70 | 246.95 | 50 | 20 | 0.1–50 | Ethylparaben |
| 319.91 | 65 | 20 | ||||||
| VOR-IS | 4.37 | 354.31 | 355.3 | 284.10 | −5 | 20 | ||
| 128.20 | −5 | 20 | ||||||
| Tylosin | 3.74 | 916.10 | 916.75 | 772.50 | −35 | 20 | ||
| 174.20 | −30 | 20 | ||||||
| Ethylparaben | 3.67 | 166.18 | 165.15 | 92.05 | 35 | 20 | ||
| 136.70 | 20 | 20 |
| Compound | LLOQ | LQC | ||||||||
| Concentraion (μg/mL) | Mean (μg/mL) | %Bias | Intra-Day Precision (%CV) | Inter-Day Precision (%CV) | Concentraion (μg/mL) | Mean (μg/mL) | %Bias | Intra-Day Precision (%CV) | Inter-Day Precision (%CV) | |
| Isavuconazole | 0.10 | 0.116 | 16.1 | 9.4 | 12.8 | 0.30 | 0.341 | 13.6 | 6.2 | 10.2 |
| Amphotericin B | 0.10 | 0.109 | 9.2 | 7.9 | 11.3 | 0.30 | 0.312 | 4.2 | 7.3 | 9.4 |
| Voriconazole | 0.10 | 0.105 | 4.6 | 4.8 | 8.4 | 0.30 | 0.332 | 10.7 | 4.1 | 9.3 |
| Fluconazole | 0.10 | 0.103 | 2.8 | 4.4 | 4.1 | 0.30 | 0.302 | 0.8 | 2.3 | 5.4 |
| Caspofungin | 0.10 | 0.104 | 4.3 | 8.9 | 12.7 | 0.30 | 0.332 | 10.8 | 9.2 | 11.4 |
| Posaconazole | 0.10 | 0.109 | 8.9 | 11.9 | 13.2 | 0.30 | 0.316 | 5.3 | 6.6 | 6.7 |
| Micafungin | 0.10 | 0.112 | 11.9 | 8.3 | 10.4 | 0.30 | 0.322 | 7.3 | 8.2 | 7.9 |
| Compound | MQC | HQC | ||||||||
| Concentraion (μg/mL) | Mean (μg/mL) | %Bias | Intra-day Precision (%CV) | Inter-day Precision (%CV) | Concentraion (μg/mL) | Mean (μg/mL) | %Bias | Intra-day Precision (%CV) | Inter-day Precision (%CV) | |
| Isavuconazole | 5.00 | 5.360 | 7.2 | 6.3 | 8.9 | 40.00 | 35.63 | −10.9 | 8.2 | 13.2 |
| Amphotericin B | 5.00 | 5.212 | 4.2 | 3.9 | 8.6 | 40.00 | 43.34 | 8.4 | 7.5 | 6.9 |
| Voriconazole | 5.00 | 5.423 | 8.5 | 3.2 | 5.7 | 40.00 | 39.60 | 1.0 | 3.5 | 3.1 |
| Fluconazole | 5.00 | 5.072 | 1.4 | 1.2 | 3.2 | 40.00 | 44.34 | 10.9 | 2.1 | 2.4 |
| Caspofungin | 5.00 | 5.136 | 2.7 | 6.7 | 8.3 | 40.00 | 39.45 | −1.4 | 11.2 | 9.3 |
| Posaconazole | 5.00 | 5.446 | 8.9 | 5.6 | 4.2 | 40.00 | 37.45 | −6.4 | 10.3 | 12.5 |
| Micafungin | 5.00 | 5.352 | 7.0 | 8.2 | 7.6 | 40.00 | 42.52 | 6.3 | 9.3 | 13.2 |
| Compound | Recovery % | Matrix Effect | ||||||
|---|---|---|---|---|---|---|---|---|
| LQC | RSD | HQC | RSD | LQC | RSD | HQC | RSD | |
| Isavuconazole | 91.23 | 7.3 | 87.23 | 9.2 | 1.68 | 6.0 | 2.17 | 10.3 |
| Amphotericin B | 95.22 | 5.3 | 104.34 | 8.5 | 2.31 | 8.3 | 2.21 | 3.6 |
| Voriconazole | 94.33 | 4.7 | 105.24 | 4.1 | 1.68 | 6.2 | 1.81 | 5.8 |
| Fluconazole | 92.11 | 9.5 | 87.35 | 4.3 | 1.39 | 10.9 | 1.47 | 6.2 |
| Caspofungin | 94.23 | 8.7 | 90.27 | 11.7 | 2.14 | 12.5 | 1.94 | 7.2 |
| Posaconazole | 92.65 | 3.6 | 82.27 | 2.2 | 1.17 | 8.4 | 1.42 | 3.1 |
| Micafungin | 85.34 | 5.8 | 82.45 | 6.7 | 1.29 | 10.4 | 1.41 | 3.5 |
| Compound | Concentration (μg/mL) | Freshly Prepared QC (μg/mL) | 4 °C for 48 h (μg/mL) | Four Freeze-Thraw Cycles (μg/mL) | −80 °C for 3 Months (μg/mL) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| LQC | HQC | LQC | HQC | LQC | HQC | LQC | HQC | LQC | HQC | |
| Isavuconazole | 0.30 | 40.00 | 0.332 (106.7) | 36.89 (92.2) | 0.322 (107.3) | 36.24 (90.6) | 0.293 (97.7) | 35.45 (88.63) | 0.314 (104.7) | 40.83 (102.1) |
| Amphotericin B | 0.30 | 40.00 | 0.313 (104.3) | 42.12 (105.3) | 0.304 (101.3) | 42.13 (105.8) | 0.286 (95.3) | 41.21 (103.0) | 0.313 (104.3) | 42.22 (105.6) |
| Voriconazole | 0.30 | 40.00 | 0.327 (109.1) | 40.23 (100.6) | 0.314 (104.7) | 41.23 (103.1) | 0.307 (102.3) | 40.27 (100.7) | 0.318 (106.0) | 40.31 (100.7) |
| Fluconazole | 0.30 | 40.00 | 0.296 (98.7) | 43.21 (108.0) | 0.283 (94.3) | 42.12 (105.3) | 0.288 (96.0) | 41.29 (103.2) | 0.297 (99.0) | 42.97 (107.4) |
| Caspofungin | 0.30 | 40.00 | 0.331 (110.3) | 39.23 (98.1) | 0.333 (111.0) | 40.23 (100.6) | 0.314 (104.7) | 39.56 (98.9) | 0.323 (107.7) | 39.49 (98.7) |
| Posaconazole | 0.30 | 40.00 | 0.314 (104.6) | 38.22 (95.6) | 0.311 (103.7) | 38.11 (95.28) | 0.302 (106.7) | 37.11 (92.8) | 0.315 (105.0) | 38.33 (95.83) |
| Micafungin | 0.30 | 40.00 | 0.318 (106.2) | 41.21 (103.0) | 0.312 (104.0) | 40.38 (101.0) | 0.307 (102.3) | 39.29 (98.2) | 0.312 (104.0) | 40.86 (102.2) |
| Compound | LLOQ (μg/mL) | Linear Range (μg/mL) | Sample Volume (μL) | Run Time (min) | Reference |
|---|---|---|---|---|---|
| Voriconazole | 0.01 | 0.01–20 | 100 | 3.0 | 30 |
| Posaconazole | 0.02 | 0.02–40 | |||
| Fluconazole | 0.2 | 0.2–200 | |||
| Itraconazole | 0.02 | 0.02–20 | |||
| Hydroxy-itraconazole | 0.01 | 0.01–10 | |||
| Voriconazole | 0.5–10 | 50 | 6.0 | 31 | |
| Isavuconazole | 0.1 | 0.5–10 | |||
| Posaconazole | 0.17–8 | ||||
| Voriconazole | 0.1 | 0.1–30 | 10 | 3.8 | 32 |
| Itraconazole | 0.05 | 0.05–10 | |||
| 4OH-itraconazole | 0.05 | 0.05–10 | |||
| Posaconazole | 0.05 | 0.05–10 | |||
| Fuconazole | 0.0283 | 0.5–40 | 50 | 3.0 | 33 |
| Isavuconazole | 0.001 | 0.1–9 | |||
| Itraconazole | 0.0017 | 0.1–4 | |||
| OH-ITZ | 0.0262 | 0.05–4 | |||
| Posaconazole | 0.103 | 0.05–8 | |||
| Voriconazole | 0.006 | 0.1–6 | |||
| Isavuconazole | 0.1 | 0.1–50 | 50 | 10.0 | our assay |
| Amphotericin B | |||||
| Voriconazole | |||||
| Fluconazole | |||||
| Caspofungin | |||||
| Posaconazole | |||||
| Micafungin |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, W.; Li, Y.; Cai, J.; Wang, Y.; Liu, Y.; Hu, H.; Liu, L. Simultaneous Quantification of Seven Antifungal Agents in Human Serum Using Liquid Chromatography-Tandem Mass Spectrometry. Pharmaceuticals 2023, 16, 1537. https://doi.org/10.3390/ph16111537
Li W, Li Y, Cai J, Wang Y, Liu Y, Hu H, Liu L. Simultaneous Quantification of Seven Antifungal Agents in Human Serum Using Liquid Chromatography-Tandem Mass Spectrometry. Pharmaceuticals. 2023; 16(11):1537. https://doi.org/10.3390/ph16111537
Chicago/Turabian StyleLi, Wenjing, Yang Li, Junlong Cai, Yue Wang, Yanan Liu, Hankun Hu, and Liang Liu. 2023. "Simultaneous Quantification of Seven Antifungal Agents in Human Serum Using Liquid Chromatography-Tandem Mass Spectrometry" Pharmaceuticals 16, no. 11: 1537. https://doi.org/10.3390/ph16111537
APA StyleLi, W., Li, Y., Cai, J., Wang, Y., Liu, Y., Hu, H., & Liu, L. (2023). Simultaneous Quantification of Seven Antifungal Agents in Human Serum Using Liquid Chromatography-Tandem Mass Spectrometry. Pharmaceuticals, 16(11), 1537. https://doi.org/10.3390/ph16111537