
Bacteriophages and Their Host Range in Multidrug-Resistant Bacterial Disease Treatment
Abstract
:1. Introduction
2. Survey Methodology
3. Brief Overview of Bacteriophages and Their Interactions with Bacterial Hosts
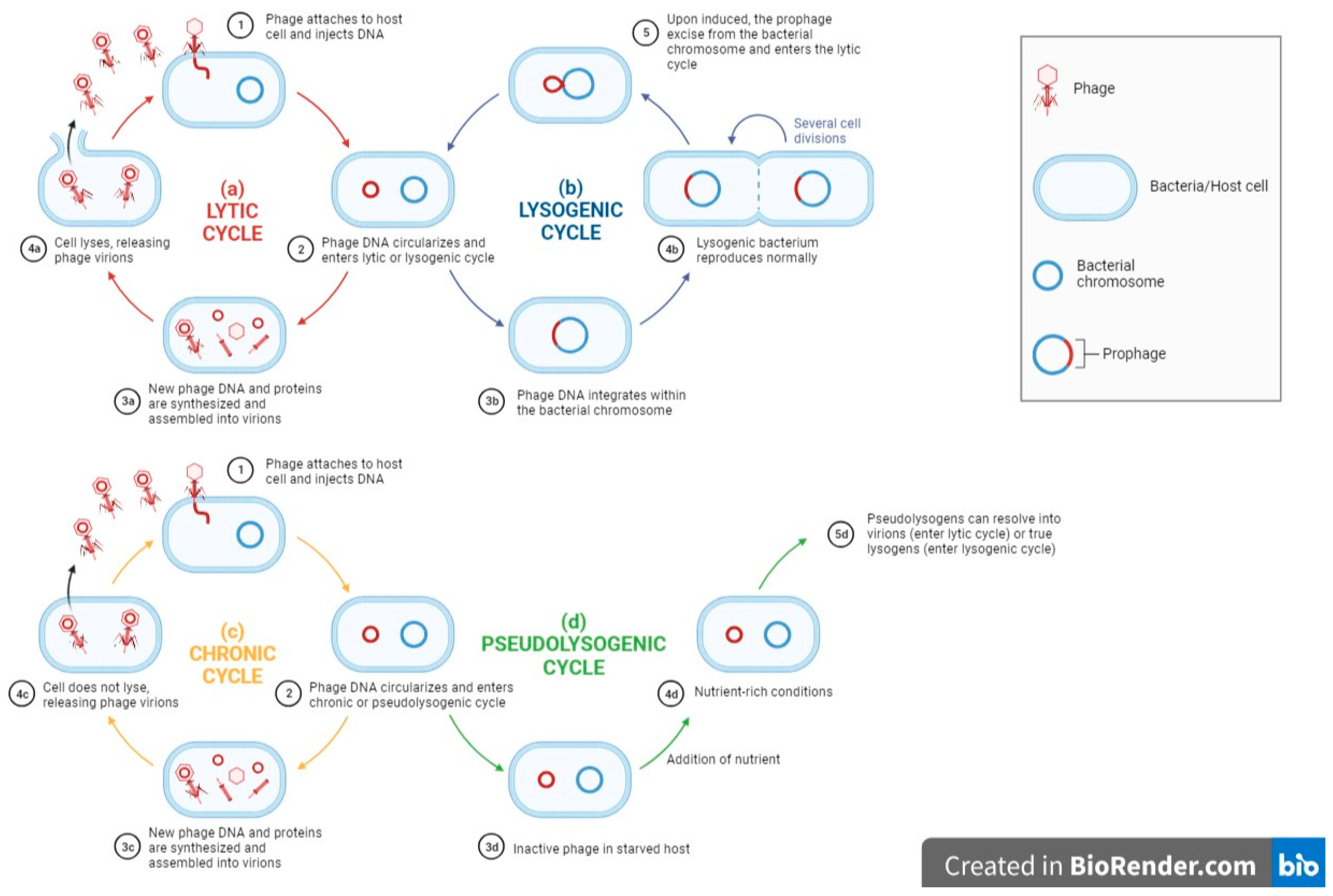
3.1. Phage Life Cycle and Its Relations to Phage Host Range
3.2. Bacteriophage Adsorption and Receptors Present in MDR Bacteria
3.3. Phage–Host Interaction
4. Broad-Host Range and Narrow-Host Range Phages
Advantages and Limitations of the Different Phage Host Ranges in the Treatment of MDR Bacteria
5. Importance of Phage Applications in the Following
5.1. Clinical MDR Bacterial Treatment
5.2. Combating MDR Bacteria in the Agriculture and Food Sectors
6. Current Studies of Broad-Host Range Phages against MDR Bacteria
7. Future Directions
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tommasi, R.; Brown, D.G.; Walkup, G.K.; Manchester, J.I.; Miller, A.A. ESKAPEing the labyrinth of antibacterial discovery. Nat. Rev. Drug Discov. 2015, 14, 529–542. [Google Scholar] [CrossRef] [PubMed]
- Reygaert, W.C. An overview of the antimicrobial resistance mechanisms of bacteria. AIMS Microbiol. 2018, 4, 482–501. [Google Scholar] [CrossRef] [PubMed]
- Tanwar, J.; Das, S.; Fatima, Z.; Hameed, S. Multidrug Resistance: An Emerging Crisis. Interdiscip. Perspect. Infect. Dis. 2014, 2014, 541340. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Antimicrobial Resistance. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance#:~:text=The%20main%20drivers%20of%20antimicrobial,access%20to%20quality%2C%20affordable%20medicines%2C (accessed on 6 May 2023).
- Paul, V.D.; Sundarrajan, S.; Rajagopalan, S.S.; Hariharan, S.; Kempashanaiah, N.; Padmanabhan, S.; Sriram, B.; Ramachandran, J. Lysis-deficient phages as novel therapeutic agents for controlling bacterial infection. BMC Microbiol. 2011, 11, 195. [Google Scholar] [CrossRef]
- Nagel, T.; Musila, L.; Muthoni, M.; Nikolich, M.; Nakavuma, J.L.; Clokie, M.R. Phage banks as potential tools to rapidly and cost-effectively manage antimicrobial resistance in the developing world. Curr. Opin. Virol. 2022, 53, 101208. [Google Scholar] [CrossRef]
- Hitchcock, N.M.; Nunes, D.D.G.; Shiach, J.; Hodel, K.V.S.; Barbosa, J.D.V.; Rodrigues, L.A.P.; Coler, B.S.; Soares, M.B.P.; Badaró, R. Current Clinical Landscape and Global Potential of Bacteriophage Therapy. Viruses 2023, 15, 1020. [Google Scholar] [CrossRef]
- Kulpakko, J.; Juusti, V.; Rannikko, A.; Hänninen, P.E. Detecting disease associated biomarkers by luminescence modulating phages. Sci. Rep. 2022, 12, 2433. [Google Scholar] [CrossRef]
- Sundell, K.; Landor, L.; Castillo, D.; Middelboe, M.; Wiklund, T. Bacteriophages as Biocontrol Agents for Flavobacterium psychrophilum Biofilms and Rainbow Trout Infections. Phage 2020, 1, 198–204. [Google Scholar] [CrossRef]
- Kim, S.H.; Adeyemi, D.E.; Park, M.K. Characterization of a new and efficient polyvalent phage infecting E. coli o157:H7, salmonella spp., and shigella sonnei. Microorganisms 2021, 9, 2105. [Google Scholar] [CrossRef]
- Martins, W.M.B.S.; Li, M.; Sands, K.; Lenzi, M.H.; Portal, E.; Mathias, J.; Dantas, P.P.; Migliavacca, R.; Hunter, J.R.; Medeiros, E.A.; et al. Effective phage cocktail to combat the rising incidence of extensively drug-resistant Klebsiella pneumoniae sequence type 16. Emerg. Microbes Infect. 2022, 11, 1015–1023. [Google Scholar] [CrossRef]
- Mapes, A.C.; Trautner, B.W.; Liao, K.S.; Ramig, R.F. Development of expanded host range phage active on biofilms of multi-drug resistant Pseudomonas aeruginosa. Bacteriophage 2016, 6, e1096995. [Google Scholar] [CrossRef] [PubMed]
- Singla, S.; Harjai, K.; Katare, O.P.; Chhibber, S. Encapsulation of Bacteriophage in Liposome Accentuates Its Entry in to Macrophage and Shields It from Neutralizing Antibodies. PLoS ONE 2016, 11, e0153777. [Google Scholar] [CrossRef] [PubMed]
- Hankin, M.E. The bactericidal action of the waters of the Jamuna and Ganges rivers on Cholera microbes. Ann. Inst. Pasteur 10:511–523 (1896). Bacteriophage 2011, 1, 117–126. [Google Scholar] [CrossRef]
- Schullian, D.M.; Rogers, F.B. Notes and Events. J. Hist. Med. Allied Sci. 1979, XXXIV, 460–462. [Google Scholar] [CrossRef]
- Twort, F. An investigation on the nature of ultra-microscopic viruses. Lancet 1915, 186, 1241–1243. [Google Scholar] [CrossRef]
- Service, P. On an invisible microbe antagonistic toward dysenteric bacilli: Brief note by Mr. F. D’Herelle, presented by Mr. Roux. Res. Microbiol. 2007, 158, 553–554. [Google Scholar] [CrossRef] [PubMed]
- Moineau, S. Bacteriophage; Elsevier EBooks: Amsterdam, The Netherlands, 2013; pp. 280–283. [Google Scholar]
- Zrelovs, N.; Dislers, A.; Kazaks, A. Motley Crew: Overview of the Currently Available Phage Diversity. Front. Microbiol. 2020, 11, 579452. [Google Scholar] [CrossRef]
- E Bradley, D. Ultrastructure of bacteriophage and bacteriocins. Bacteriol. Rev. 1967, 31, 230–314. [Google Scholar] [CrossRef]
- Ackermann, H. Tailed Bacteriophages: The Order Caudovirales. Adv. Virus Res. 1998, 51, 135–201. [Google Scholar] [CrossRef]
- Ackermann, H.W. Classification of bacteriophages. Bacteriophages 2006, 2, 8–16. [Google Scholar]
- Ackermann, H.-W. Bacteriophage observations and evolution. Res. Microbiol. 2003, 154, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Sieiro, C.; Areal-Hermida, L.; Pichardo-Gallardo, Á.; Almuiña-González, R.; De Miguel, T.; Sánchez, S.; Sánchez-Pérez, Á.; Villa, T.G. A Hundred Years of Bacteriophages: Can Phages Replace Antibiotics in Agriculture and Aquaculture? Antibiotics 2020, 9, 493. [Google Scholar] [CrossRef] [PubMed]
- Le, S.; He, X.; Tan, Y.; Huang, G.; Zhang, L.; Lux, R.; Shi, W.; Hu, F. Mapping the Tail Fiber as the Receptor Binding Protein Responsible for Differential Host Specificity of Pseudomonas aeruginosa Bacteriophages PaP1 and JG004. PLoS ONE 2013, 8, e68562. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Roznowski, A.P.; Tokuda, J.M.; Klose, T.; Mauney, A.; Pollack, L.; Fane, B.A.; Rossmann, M.G. Structural changes of tailless bacteriophage ΦX174 during penetration of bacterial cell walls. Proc. Natl. Acad. Sci. USA 2017, 114, 13708–13713. [Google Scholar] [CrossRef]
- Storms, Z.J.; Sauvageau, D. Modeling tailed bacteriophage adsorption: Insight into mechanisms. Virology 2015, 485, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Bertozzi Silva, J.; Storms, Z.; Sauvageau, D. Host receptors for bacteriophage adsorption. FEMS Microbiol. Lett. 2016, 363, fnw002. [Google Scholar] [CrossRef] [PubMed]
- Rakhuba, D.V.; Kolomiets, E.I.; Dey, E.S.; Novik, G.I. Bacteriophage Receptors, Mechanisms of Phage Adsorption and Penetration into Host Cell. Pol. J. Microbiol. 2010, 59, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.; Hanawa, T.; Azam, A.H.; LeBlanc, C.; Ung, P.; Matsuda, T.; Onishi, H.; Miyanaga, K.; Tanji, Y. Silviavirus phage ΦMR003 displays a broad host range against methicillin-resistant Staphylococcus aureus of human origin. Appl. Microbiol. Biotechnol. 2019, 103, 7751–7765. [Google Scholar] [CrossRef]
- Azam, A.H.; Hoshiga, F.; Takeuchi, I.; Miyanaga, K.; Tanji, Y. Analysis of phage resistance in Staphylococcus aureus SA003 reveals different binding mechanisms for the closely related Twort-like phages ΦSA012 and ΦSA039. Appl. Microbiol. Biotechnol. 2018, 102, 8963–8977. [Google Scholar] [CrossRef]
- Chatterjee, A.; Johnson, C.N.; Luong, P.; Hullahalli, K.; McBride, S.W.; Schubert, A.M.; Palmer, K.L.; Carlson, P.E., Jr.; Duerkop, B.A. Bacteriophage Resistance Alters Antibiotic-Mediated Intestinal Expansion of Enterococci. Infect. Immun. 2019, 87, e00085-19. [Google Scholar] [CrossRef]
- Ahamed, S.T.; Roy, B.; Basu, U.; Dutta, S.; Ghosh, A.N.; Bandyopadhyay, B.; Giri, N. Genomic and Proteomic Characterizations of Sfin-1, a Novel Lytic Phage Infecting Multidrug-Resistant Shigella spp. and Escherichia coli C. Front. Microbiol. 2019, 10, 1876. [Google Scholar] [CrossRef] [PubMed]
- Altamirano, F.G.; Forsyth, J.H.; Patwa, R.; Kostoulias, X.; Trim, M.; Subedi, V.O.R.I.P.; Archer, S.; Morris, V.O.R.I.P.C.; Oliveira, C.; Kielty, L.; et al. Bacteriophages targeting Acinetobacter baumannii capsule induce antimicrobial resensitization. bioRxiv 2020, 1–28. [Google Scholar] [CrossRef]
- Chan, B.; Stanley, G.L.; Kortright, K.E.; Modak, M.; Ott, I.M.; Sun, Y.; Würstle, S.; Grun, C.; Kazmierczak, B.; Rajagopalan, G.; et al. Personalized Inhaled Bacteriophage Therapy Decreases Multidrug-Resistant Pseudomonas aeruginosa. medRxiv 2023. [Google Scholar] [CrossRef]
- Hesse, S.; Rajaure, M.; Wall, E.; Johnson, J.; Bliskovsky, V.; Gottesman, S.; Adhya, S. Phage Resistance in Multidrug-Resistant Klebsiella pneumoniae ST258 Evolves via Diverse Mutations That Culminate in Impaired Adsorption. mBio 2020, 11, e02530-19. [Google Scholar] [CrossRef]
- Abedon, S.; Thomas-Abedon, C. Phage Therapy Pharmacology. Curr. Pharm. Biotechnol. 2010, 11, 28–47. [Google Scholar] [CrossRef] [PubMed]
- Kutter, E.; Raya, R.; Carlson, K. Molecular Mechanisms of Phage Infection. In Bacteriophages: Biology and Application; CRC Press-Taylor & Francis Group: Boca Raton, FL, USA, 2005; pp. 165–222. [Google Scholar]
- Little, J.W. Lysogeny, Prophage Induction, and Lysogenic Conversion. Phages 2014, 37–54. [Google Scholar] [CrossRef]
- Skorb, E.V.; Andreeva, D.V.; Raiski, A.P.; Belyasova, N.A.; Möhwald, H.; Sviridov, D.V. Titanium dioxide-assisted photocatalytic induction of prophages to lytic cycle. Photochem. Photobiol. Sci. 2011, 10, 1974–1978. [Google Scholar] [CrossRef] [PubMed]
- Moons, P.; Faster, D.; Aertsen, A. Lysogenic Conversion and Phage Resistance Development in Phage Exposed Escherichia coli Biofilms. Viruses 2013, 5, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Edgar, R.; Friedman, N.; Molshanski-Mor, S.; Qimron, U. Reversing Bacterial Resistance to Antibiotics by Phage-Mediated Delivery of Dominant Sensitive Genes. Appl. Environ. Microbiol. 2012, 78, 744–751. [Google Scholar] [CrossRef]
- Park, J.Y.; Moon, B.Y.; Park, J.W.; Thornton, J.A.; Park, Y.H.; Seo, K.S. Genetic engineering of a temperate phage-based delivery system for CRISPR/Cas9 antimicrobials against Staphylococcus aureus. Sci. Rep. 2017, 7, srep44929. [Google Scholar] [CrossRef]
- Yu, P.; Mathieu, J.; Li, M.; Dai, Z.; Alvarez, P.J.J. Isolation of Polyvalent Bacteriophages by Sequential Multiple-Host Approaches. Appl. Environ. Microbiol. 2016, 82, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Duc, H.M.; Son, H.M.; Yi, H.P.S.; Sato, J.; Ngan, P.H.; Masuda, Y.; Honjoh, K.-I.; Miyamoto, T. Isolation, characterization and application of a polyvalent phage capable of controlling Salmonella and Escherichia coli O157:H7 in different food matrices. Food Res. Int. 2020, 131, 108977. [Google Scholar] [CrossRef] [PubMed]
- Sui, B.; Han, L.; Ren, H.; Liu, W.; Zhang, C. A Novel Polyvalent Bacteriophage vB_EcoM_swi3 Infects Pathogenic Escherichia coli and Salmonella enteritidis. Front. Microbiol. 2021, 12, 649673. [Google Scholar] [CrossRef] [PubMed]
- Tao, C.; Yi, Z.; Zhang, Y.; Wang, Y.; Zhu, H.; Afayibo, D.J.A.; Li, T.; Tian, M.; Qi, J.; Ding, C.; et al. Characterization of a Broad-Host-Range Lytic Phage SHWT1 against Multidrug-Resistant Salmonella and Evaluation of Its Therapeutic Efficacy in vitro and in vivo. Front. Vet. Sci. 2021, 8, 683853. [Google Scholar] [CrossRef]
- Xu, J.; Chen, M.; He, L.; Zhang, S.; Ding, T.; Yao, H.; Lu, C.; Zhang, W. Isolation and characterization of a T4-like phage with a relatively wide host range within Escherichia coli. J. Basic Microbiol. 2016, 56, 405–421. [Google Scholar] [CrossRef]
- De Melo, A.C.C.; da Mata Gomes, A.; Melo, F.L.; Ardisson-Araújo, D.M.P.; De Vargas, A.P.C.; Ely, V.L.; Kitajima, E.W.; Ribeiro, B.M.; Wolff, J.L.C. Characterization of a bacteriophage with broad host range against strains of Pseudomonas aeruginosa isolated from domestic animals. BMC Microbiol. 2019, 19, 134. [Google Scholar] [CrossRef]
- Ackermann, H.W.; DuBow, M.S. Viruses of Prokaryotes: General Properties of Bacteriophages; CRC Press Inc.: Boca Raton, FL, USA, 1987; Volume 1, pp. 49–85. [Google Scholar]
- Hamdi, S.; Rousseau, G.M.; Labrie, S.J.; Tremblay, D.M.; Kourda, R.S.; Slama, K.B.; Moineau, S. Characterization of two polyvalent phages infecting Enterobacteriaceae. Sci. Rep. 2017, 7, 40349. [Google Scholar] [CrossRef]
- Gupta, R.; Prasad, Y. Efficacy of polyvalent bacteriophage P-27/HP to control multidrug resistant staphylococcus aureus associated with human infections. Curr. Microbiol. 2011, 62, 255–260. [Google Scholar] [CrossRef]
- Hyman, P. Phages for Phage Therapy: Isolation, Characterization, and Host Range Breadth. Pharmaceuticals 2019, 12, 35. [Google Scholar] [CrossRef]
- Auad, L.; Holgado, A.D.R.; Forsman, P.; Alatossava, T.; Raya, R. Isolation and Characterization of a New Lactobacillus delbrueckii ssp. bulgaricus Temperate Bacteriophage. J. Dairy Sci. 1997, 80, 2706–2712. [Google Scholar] [CrossRef]
- Lu, Z.; Breidt, F.; Fleming, H.; Altermann, E.; Klaenhammer, T. Isolation and characterization of a Lactobacillus plantarum bacteriophage, ΦJL-1, from a cucumber fermentation. Int. J. Food Microbiol. 2003, 84, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Han, J.; Ji, X.; Hong, W.; Huang, L.; Wei, Y. Isolation and characterization of a new bacteriophage MMP17 from Meiothermus. Extremophiles 2011, 15, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-K.; Liu, C.-P.; Leung, C.-H.; Sun, F.-J. Clinical and microbiological analysis of adult perianal abscess. J. Microbiol. Immunol. Infect. 2011, 44, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Kong, H.; Yu, F.; Zhang, W.; Li, X. Clinical and microbiological characteristics of pyogenic liver abscess in a tertiary hospital in East China. Medicine 2017, 96, e8050. [Google Scholar] [CrossRef]
- Lin, Y.-T.; Cheng, Y.-H.; Chuang, C.; Chou, S.-H.; Liu, W.-H.; Yang, T.-C.; Kreiswirth, B.N.; Chen, L. Molecular and Clinical Characterization of Multidrug-Resistant and Hypervirulent Klebsiella pneumoniae Strains from Liver Abscess in Taiwan. Antimicrob. Agents Chemother. 2020, 64, e00174-20. [Google Scholar] [CrossRef]
- Law, N.; Logan, C.; Yung, G.; Furr, C.-L.L.; Lehman, S.M.; Morales, S.; Rosas, F.; Gaidamaka, A.; Bilinsky, I.; Grint, P.; et al. Successful adjunctive use of bacteriophage therapy for treatment of multidrug-resistant Pseudomonas aeruginosa infection in a cystic fibrosis patient. Infection 2019, 47, 665–668. [Google Scholar] [CrossRef] [PubMed]
- Ngiam, L.; Schembri, M.A.; Weynberg, K.; Guo, J. Bacteriophage isolated from non-target bacteria demonstrates broad host range infectivity against multidrug-resistant bacteria. Environ. Microbiol. 2021, 23, 5569–5586. [Google Scholar] [CrossRef]
- Feng, T.; Leptihn, S.; Dong, K.; Loh, B.; Zhang, Y.; Stefan, M.I.; Li, M.; Guo, X.; Cui, Z. JD419, a Staphylococcus aureus Phage with a Unique Morphology and Broad Host Range. Front. Microbiol. 2021, 12, 602902. [Google Scholar] [CrossRef]
- Morello, E.; Saussereau, E.; Maura, D.; Huerre, M.; Touqui, L.; Debarbieux, L. Pulmonary Bacteriophage Therapy on Pseudomonas aeruginosa Cystic Fibrosis Strains: First Steps towards Treatment and Prevention. PLoS ONE 2011, 6, e16963. [Google Scholar] [CrossRef]
- Khorshidtalab, M.; Durukan, I.; Tufekci, E.F.; Nas, S.S.; Abdurrahman, M.A.; Kilic, A.O. Isolation and Characterization of Lytic Bacteriophages from Wastewater with Phage Therapy Potentials against Gram-Negative Bacteria. Eurasian J. Med. 2022, 54, 157–164. [Google Scholar] [CrossRef]
- Bhetwal, A.; Maharjan, A.; Shakya, S.; Satyal, D.; Ghimire, S.; Khanal, P.R.; Parajuli, N.P. Isolation of Potential Phages against Multidrug-Resistant Bacterial Isolates: Promising Agents in the Rivers of Kathmandu, Nepal. BioMed Res. Int. 2017, 2017, 3723254. [Google Scholar] [CrossRef]
- Summers, W.C. Felix d’Herelle and the Origins of Molecular Biology; Yale University Press: New Haven, CT, USA, 1999. [Google Scholar]
- Schultz, E.W. The Bacteriophage as a Therapeutic Agent. Calif. West. Med. 1929, 31, 5–10. [Google Scholar]
- Ligon, B. Penicillin: Its discovery and early development. Semin. Pediatr. Infect. Dis. 2004, 15, 52–57. [Google Scholar] [CrossRef]
- Girija, A.S.; Priyadharsini, J.V. CLSI based antibiogram profile and the detection of MDR and XDR strains of Acinetobacter baumannii isolated from urine samples. Med. J. Islam. Repub. Iran MJIRI 2019, 33, 3. [Google Scholar] [CrossRef]
- Shahkarami, F.; Rashki, A.; Ghalehnoo, Z.R. Microbial Susceptibility and Plasmid Profiles of Methicillin-Resistant Staphylococcus aureus and Methicillin-Susceptible S. aureus. Jundishapur J. Microbiol. 2014, 7, e16984. [Google Scholar] [CrossRef]
- Gastmeier, P.; Schröder, C.; Behnke, M.; Meyer, E.; Geffers, C. Dramatic increase in vancomycin-resistant enterococci in Germany. J. Antimicrob. Chemother. 2014, 69, 1660–1664. [Google Scholar] [CrossRef]
- Kutter, E.M.; Kuhl, S.J.; Abedon, S.T. Re-establishing a place for phage therapy in western medicine. Future Microbiol. 2015, 10, 685–688. [Google Scholar] [CrossRef]
- Oduor, J.M.O.; Onkoba, N.; Maloba, F.; Nyachieo, A. Experimental phage therapy against haematogenous multi-drug resistant Staphylococcus aureus pneumonia in mice. Afr. J. Lab. Med. 2016, 5, 435. [Google Scholar] [CrossRef] [PubMed]
- Abedon, S.T.; Kuhl, S.J.; Blasdel, B.G.; Kutter, E.M. Phage treatment of human infections. Bacteriophage 2011, 1, 66–85. [Google Scholar] [CrossRef]
- Borysowski, J.; Gorski, A. Is phage therapy acceptable in the immunocompromised host? Int. J. Infect. Dis. 2008, 12, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Van Belleghem, J.D.; de Vries, C.R.; Burgener, E.; Chen, Q.; Manasherob, R.; Aronson, J.R.; Amanatullah, D.F.; Tamma, P.D.; Suh, G.A. The Safety and Toxicity of Phage Therapy: A Review of Animal and Clinical Studies. Viruses 2021, 13, 1268. [Google Scholar] [CrossRef]
- Jault, P.; Leclerc, T.; Jennes, S.; Pirnay, J.P.; Que, Y.-A.A.; Resch, G.; Rousseau, A.F.; Ravat, F.; Carsin, H.; Le Floch, R.; et al. Efficacy and tolerability of a cocktail of bacteriophages to treat burn wounds infected by Pseudomonas aeruginosa (PhagoBurn): A randomised, controlled, double-blind phase 1/2 trial. Lancet Infect. Dis. 2019, 19, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Dedrick, R.M.; Guerrero-Bustamante, C.A.; Garlena, R.A.; Russell, D.A.; Ford, K.; Harris, K.; Gilmour, K.C.; Soothill, J.; Jacobs-Sera, D.; Schooley, R.T.; et al. Engineered bacteriophages for treatment of a patient with a disseminated drug-resistant Mycobacterium abscessus. Nat. Med. 2019, 25, 730–733. [Google Scholar] [CrossRef] [PubMed]
- Rhoads, D.D.; Wolcott, R.D.; Kuskowski, M.A.; Wolcott, B.M.; Ward, L.S.; Sulakvelidze, A. Bacteriophage therapy of venous leg ulcers in humans: Results of a phase I safety trial. J. Wound Care 2009, 18, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.; Hawkins, C.H.; Änggård, E.E.; Harper, D.R. A controlled clinical trial of a therapeutic bacteriophage preparation in chronic otitis due to antibiotic-resistant Pseudomonas aeruginosa; a preliminary report of efficacy. Clin. Otolaryngol. Allied Sci. 2009, 34, 349–357. [Google Scholar] [CrossRef]
- Leitner, L.; Sybesma, W.; Chanishvili, N.; Goderdzishvili, M.; Chkhotua, A.; Ujmajuridze, A.; Schneider, M.P.; Sartori, A.; Mehnert, U.; Bachmann, L.M.; et al. Bacteriophages for treating urinary tract infections in patients undergoing transurethral resection of the prostate: A randomized, placebo-controlled, double-blind clinical trial. BMC Urol. 2017, 17, 90. [Google Scholar] [CrossRef]
- Alam Sarker, S.; Berger, B.; Deng, Y.; Kieser, S.; Foata, F.; Moine, D.; Descombes, P.; Sultana, S.; Huq, S.; Bardhan, P.K.; et al. Oral application of Escherichia coli bacteriophage: Safety tests in healthy and diarrheal children from Bangladesh. Environ. Microbiol. 2017, 19, 237–250. [Google Scholar] [CrossRef]
- Jiang, L.; Tan, J.; Hao, Y.; Wang, Q.; Yan, X.; Wang, D.; Tuo, L.; Wei, Z.; Huang, G. Isolation and Characterization of a Novel Myophage Abp9 against Pandrug Resistant Acinetobacater baumannii. Front. Microbiol. 2020, 11, 506068. [Google Scholar] [CrossRef]
- Fish, R.; Kutter, E.; Wheat, G.; Blasdel, B.; Kutateladze, M.; Kuhl, S. Bacteriophage treatment of intransigent diabetic toe ulcers: A case series. J. Wound Care 2016, 25, S27–S33. [Google Scholar] [CrossRef]
- Khan, F.M.; Gondil, V.S.; Li, C.; Jiang, M.; Li, J.; Yu, J.; Wei, H.; Yang, H. A Novel Acinetobacter baumannii Bacteriophage Endolysin LysAB54 with High Antibacterial Activity against Multiple Gram-Negative Microbes. Front. Cell. Infect. Microbiol. 2021, 11, 637313. [Google Scholar] [CrossRef]
- Wu, M.; Hu, K.; Xie, Y.; Liu, Y.; Mu, D.; Guo, H.; Zhang, Z.; Zhang, Y.; Chang, D.; Shi, Y. A Novel Phage PD-6A3, and Its Endolysin Ply6A3, with Extended Lytic Activity against Acinetobacter baumannii. Front. Microbiol. 2019, 9, 3302. [Google Scholar] [CrossRef] [PubMed]
- Pallavali, R.R.; Degati, V.L.; Narala, V.R.; Velpula, K.K.; Yenugu, S.; Durbaka, V.R.P. Lytic Bacteriophages against Bacterial Biofilms Formed by Multidrug-Resistant Pseudomonas aeruginosa, Escherichia coli, Klebsiella pneumoniae, and Staphylococcus aureus Isolated from Burn Wounds. Ther. Appl. Res. 2021, 2, 120–130. [Google Scholar] [CrossRef] [PubMed]
- Drulis-Kawa, Z.; Weber-Dabrowska, B.; Łusiak-Szelachowska, M.; Doroszkiewicz, W. Potential possibilities of using phage typing in elimination of multidrug resistant staphylococci. Pol. J. Microbiol. 2005, 54, 63–67. [Google Scholar] [PubMed]
- Mohammed, M. Phage typing or CRISPR typing for epidemiological surveillance of Salmonella Typhimurium? BMC Res. Notes 2017, 10, 578. [Google Scholar] [CrossRef] [PubMed]
- Velayudham, A.; Manavalan, J.; Vadivel, S.; Kaliyamoorthy, B.; Kuthalaramalingam, S. Bacteriophage Typing of Methicillin Resistant Staphylococcus aureus and Changing Trend in their Antibiotic Profile. Ann. Int. Med. Dent. Res. 2016, 3, 1–5. [Google Scholar] [CrossRef]
- Venturini, C.; Bowring, B.; Partridge, S.R.; Ben Zakour, N.L.; Fajardo-Lubian, A.; Ayala, A.L.; Qin, J.; Totsika, M.; van Galen, G.; Norris, J.; et al. Co-Occurrence of Multidrug Resistant Klebsiella pneumoniae Pathogenic Clones of Human Relevance in an Equine Pneumonia Case. Microbiol. Spectr. 2022, 10, e0215821. [Google Scholar] [CrossRef]
- Perera, M.N.; Abuladze, T.; Li, M.; Woolston, J.; Sulakvelidze, A. Bacteriophage cocktail significantly reduces or eliminates Listeria monocytogenes contamination on lettuce, apples, cheese, smoked salmon and frozen foods. Food Microbiol. 2015, 52, 42–48. [Google Scholar] [CrossRef]
- Kazi, M.; Annapure, U.S. Bacteriophage biocontrol of foodborne pathogens. J. Food Sci. Technol. 2016, 53, 1355–1362. [Google Scholar] [CrossRef]
- Amarillas, L.; Rubí-Rangel, L.; Chaidez, C.; González-Robles, A.; Lightbourn-Rojas, L.; León-Félix, J. Isolation and Characterization of phiLLS, a Novel Phage with Potential Biocontrol Agent against Multidrug-Resistant Escherichia coli. Front. Microbiol. 2017, 8, 1355. [Google Scholar] [CrossRef]
- Tian, L.; He, L.; Jackson, K.; Saif, A.; Khan, S.; Wan, Z.; Didar, T.F.; Hosseinidoust, Z. Self-assembling nanofibrous bacteriophage microgels as sprayable antimicrobials targeting multidrug-resistant bacteria. Nat. Commun. 2022, 13, 7158. [Google Scholar] [CrossRef]
- Le, T.S.; Southgate, P.C.; O’connor, W.; Poole, S.; Kurtböke, D.I. Bacteriophages as Biological Control Agents of Enteric Bacteria Contaminating Edible Oysters. Curr. Microbiol. 2018, 75, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Bao, J.; Wu, N.; Zeng, Y.; Chen, L.; Li, L.; Yang, L.; Zhang, Y.; Guo, M.; Li, L.; Li, J.; et al. Non-active antibiotic and bacteriophage synergism to successfully treat recurrent urinary tract infection caused by extensively drug-resistant Klebsiella pneumoniae. Emerg. Microbes Infect. 2020, 9, 771–774. [Google Scholar] [CrossRef] [PubMed]
- Arumugam, S.N.; Rudraradhya, A.C.; Sadagopan, S.; Sukumaran, S.; Sambasivam, G.; Ramesh, N. Analysis of Susceptibility Patterns of Pseudomonas aeruginosa and Isolation, Characterization of Lytic Bacteriophages Targeting Multi Drug Resistant Pseudomonas aeruginosa. Biomed. Pharmacol. J. 2018, 11, 1105–1117. [Google Scholar] [CrossRef]
- Popova, A.V.; Zhilenkov, E.L.; Myakinina, V.P.; Krasilnikova, V.M.; Volozhantsev, N.V. Isolation and characterization of wide host range lytic bacteriophage AP22 infecting Acinetobacter baumannii. FEMS Microbiol. Lett. 2012, 332, 40–46. [Google Scholar] [CrossRef]
- Nyachieo, A.; Alafi, S.; Mutai, I.J.; Ngolobe, B.; Nabunje, R.; Nakavuma, J.L. Isolation and Characterization of Novel Lytic Phages to Combat Multidrug-Resistant E. coli and Salmonella spp. J. Microbiol. Infect. Dis. 2021, 11, 183–190. [Google Scholar] [CrossRef]
- Arumugam, S.N.; Manohar, P.; Sukumaran, S.; Sadagopan, S.; Loh, B.; Leptihn, S.; Nachimuthu, R. Antibacterial efficacy of lytic phages against multidrug-resistant Pseudomonas aeruginosa infections in bacteraemia mice models. BMC Microbiol. 2022, 22, 187. [Google Scholar] [CrossRef]
- Dhungana, G.; Nepal, R.; Regmi, M.; Malla, R. Pharmacokinetics and Pharmacodynamics of a Novel Virulent Klebsiella Phage Kp_Pokalde_002 in a Mouse Model. Front. Cell. Infect. Microbiol. 2021, 11, 684704. [Google Scholar] [CrossRef]
- Tang, S.-S.; Biswas, S.K.; Tan, W.S.; Saha, A.K.; Leo, B.-F. Efficacy and potential of phage therapy against multidrug resistant Shigella spp. PeerJ 2019, 7, e6225. [Google Scholar] [CrossRef]
- Gu, J.; Liu, X.; Li, Y.; Han, W.; Lei, L.; Yang, Y.; Zhao, H.; Gao, Y.; Song, J.; Lu, R.; et al. A Method for Generation Phage Cocktail with Great Therapeutic Potential. PLoS ONE 2012, 7, e31698. [Google Scholar] [CrossRef]
- Shahin, K.; Bouzari, M.; Komijani, M.; Wang, R. A New Phage Cocktail against Multidrug, ESBL-Producer Isolates of Shigella sonnei and Shigella flexneri with Highly Efficient Bacteriolytic Activity. Microb. Drug Resist. 2020, 26, 831–841. [Google Scholar] [CrossRef]
- Pereira, S.; Santos, L.; Klumpp, J.; Almeida, A. Potential of phage cocktails in the inactivation of Enterobacter cloacae—An in vitro study in a buffer solution and in urine samples. Virus Res. 2016, 211, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Haines, M.E.K.; Hodges, F.E.; Nale, J.Y.; Mahony, J.; van Sinderen, D.; Kaczorowska, J.; Alrashid, B.; Akter, M.; Brown, N.; Sauvageau, D.; et al. Analysis of Selection Methods to Develop Novel Phage Therapy Cocktails against Antimicrobial Resistant Clinical Isolates of Bacteria. Front. Microbiol. 2021, 12, 564. [Google Scholar] [CrossRef]
- Lin, T.-Y.; Lo, Y.-H.; Tseng, P.-W.; Chang, S.-F.; Lin, Y.-T.; Chen, T.-S. A T3 and T7 Recombinant Phage Acquires Efficient Adsorption and a Broader Host Range. PLoS ONE 2012, 7, e30954. [Google Scholar] [CrossRef] [PubMed]
- Yehl, K.; Lemire, S.; Yang, A.C.; Ando, H.; Mimee, M.; Torres, M.D.T.; de la Fuente-Nunez, C.; Lu, T.K. Engineering Phage Host-Range and Suppressing Bacterial Resistance through Phage Tail Fiber Mutagenesis. Cell 2019, 179, 459–469.e9. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Pan, P.; Zheng, D.W.; Bao, P.; Zeng, X.; Zhang, X.Z. Bioinorganic hybrid bacteriophage for modulation of intestinal microbiota to remodel tumor-immune microenvironment against colorectal cancer. Sci. Adv. 2020, 6, eaba1590. [Google Scholar] [CrossRef]
- He, X.; Yang, Y.; Guo, Y.; Lu, S.; Du, Y.; Li, J.-J.; Zhang, X.; Leung, N.L.C.; Zhao, Z.; Niu, G.; et al. Phage-Guided Targeting, Discriminative Imaging, and Synergistic Killing of Bacteria by AIE Bioconjugates. J. Am. Chem. Soc. 2020, 142, 3959–3969. [Google Scholar] [CrossRef]
- Dong, S.; Shi, H.; Zhang, X.; Chen, X.; Cao, D.; Mao, C.; Gao, X.; Wang, L. Difunctional bacteriophage conjugated with photosensitizers for Candida albicans-targeting photodynamic inactivation. Int. J. Nanomed. 2018, 13, 2199–2216. [Google Scholar] [CrossRef]
- Anany, H.; Chen, W.; Pelton, R.; Griffiths, M.W. Biocontrol of Listeria monocytogenes and Escherichia coli O157:H7 in Meat by Using Phages Immobilized on Modified Cellulose Membranes. Appl. Environ. Microbiol. 2011, 77, 6379–6387. [Google Scholar] [CrossRef]
- Abdelsattar, A.S.; Nofal, R.; Makky, S.; Safwat, A.; Taha, A.; El-Shibiny, A. The Synergistic Effect of Biosynthesized Silver Nanoparticles and Phage ZCSE2 as a Novel Approach to Combat Multidrug-Resistant Salmonella enterica. Antibiotics 2021, 10, 678. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.; Pereira, C.; Almeida, A. Sequential Combined Effect of Phages and Antibiotics on the Inactivation of Escherichia coli. Microorganisms 2018, 6, 125. [Google Scholar] [CrossRef]
- Mai, V.; Ukhanova, M.; Reinhard, M.K.; Li, M.; Sulakvelidze, A. Bacteriophage administration significantly reduces Shigella colonization and shedding by Shigella-challenged mice without deleterious side effects and distortions in the gut microbiota. Bacteriophage 2015, 5, e1088124. [Google Scholar] [CrossRef] [PubMed]
- Llanos-Chea, A.; Citorik, R.J.; Nickerson, K.P.; Ingano, L.; Serena, G.; Senger, S.; Lu, T.K.; Fasano, A.; Faherty, C.S. Bacteriophage Therapy Testing against Shigella flexneri in a Novel Human Intestinal Organoid-Derived Infection Model. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 509–516. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| No. | Phage(s)/Phage Cocktail Name | Effective Against | Application | Reference |
|---|---|---|---|---|
| 1. | Abp9 | MDR A. baumannii strain ABZY9 | Therapeutic agent | [83] |
| 2. | Sb-1 | MDR S. aureus | Therapeutic agent | [84] |
| 3. | p54 | MDR A. baumannii, P. aeruginosa, K. pneumoniae, and E. coli | Therapeutic agent | [85] |
| 4. | PD6A3 | MDR A. baumannii, E. coli, E. faecium and P. aeruginosa | Therapeutic agent | [86] |
| 5. | DT104 phage types | MDR S. Typhimurium | Phenotyping tool | [89] |
| 6. | 5 phage groups consisting of 23 phages | Methicillin Resistant S. aureus | Phenotyping tool | [90] |
| 7. | JIPh_Kp 192– 199, and JIPh_Kp 202 | MDR K. pneumoniae | Phenotyping tool | [91] |
| 8. | phiLLS | MDR E. coli | Biocontrol agent | [94] |
| 9. | M13 | MDR E. coli O157:H7 | Biocontrol agent | [95] |
| 10. | Phage cocktail consisting of ΦEco1, ΦEco2, ΦEco3, ΦEco5, ΦEco6 and ΦS1 | MDR enteric bacteria such as E. coli and S. enterica | Biocontrol agent | [96] |
| No. | Phage/s | Host Strain | Against | Effectiveness | Description/ Remarks | Reference |
|---|---|---|---|---|---|---|
| In vitro | ||||||
| 1. | vB_EcoM_LNA1 (A1) | E. coli K12 MG1655 w/RP4 plasmid | E. coli K12 MG1655 w/RP4 plasmid, E. coli K12 MG1655 w/pMS6198A plasmid, uropathogenic E. coli (UPEC) S79EC, UPEC S129EC | Phage exhibited broad host range recognition and strong infectivity against UPEC strains as demonstrated by a large burst size and extended bacterial growth suppression. | [A] | [61] |
| 2. | SHWT1 | Salmonella pullorum | MDR Salmonella (S. Pullorum, Salmonella Gallinarum, S. Enteritidis, S. Typhimurium, Salmonella Derby, Salmonella London, Salmonella Typhi, Salmonella Heidelberg, Salmonella Paratyphi B) | Phage had a short latent period (5 min) and an average burst size of 146.6 ± 10.8 PFUs/cell. It retained lytic activity for at least 60 min at temperatures ranging between 4 and 65 °C and remained stable at pH 3 to 12. | [A] | [47] |
| 3. | JD419 | S. aureus | MDR clinical S. aureus strains | A temperate phage that is stable at pH 6 to 8 and below 50 °C. Rapid replication and lysis of host strains were observed. No virulence or antibiotic resistance genes. | [A] | [62] |
| 4. | AP025 and AP006 | P. aeruginosa PAO1/ P. aeruginosa ATCC9027 /clinical isolate | MDR P. aeruginosa | AP025 and AP006 phages exhibited a good infectivity rate (host range infectivity) of 39% and 30%, respectively, against MDR strains. | [A] | [98] |
| 5. | AP22 | A. baumannii | Genotype-varying MDR clinical A. baumannii strains | Phage exhibits rapid adsorption (>99% adsorbed in 5 min), a large burst size (240 PFU per cell), and stability in a wide range of pH. Infect and lyse 68% of MDR A. baumannii. | [A] | [99] |
| 6. | C11S1A | E. coli | MDR E. coli in East Africa | Phage killed all 23 E. coli strains. Highly efficacious at 37 °C and pH 7.4. | [A] | [100] |
| 7. | ΦSER1 | Serratia | E. coli, Enterobacter spp., Klebsiella spp., Serratia spp., Pseudomonas spp., Citrobacter spp., MDR Pseudomonas | 85% effectiveness in terms of host range when compared with other phages. | [B] | [65] |
| In vivo | ||||||
| 8. | SHWT1 | S. pullorum | MDR S. enteritidis and S. typhimurium | Reduced mice mortality when phage treatment was introduced. Survival rate of S. Enteritidis infection: 40% Survival rate of S. Typhimurium infection: 80%. | [A] | [47] |
| 9. | AP025 and AP006 | P. aeruginosa PAO1/P. aeruginosa ATCC9027 /clinical isolate | MDR P. aeruginosa | A single dose of phages at higher concentrations, bacteria:phages at 1:10 and 1:100 were effective in eliminating bloodstream infection and achieving 100% mice survival. | [A] | [101] |
| 10. | PAK-P3 and P3-CHA | P. aeruginosa | MDR P. aeruginosa cystic fibrosis strains | A curative treatment (one single dose) administered 2 h after the onset of the infection allowed over 95% survival. A four-day preventive treatment (one single dose) resulted in 100% survival. | [A] | [63] |
| 11. | øKp_Pokalde_002 | K. pneumoniae | Carbapenem-resistant K. pneumoniae (Kp56) | Bacterial count significantly decreased in blood and other organs after 24 h of phage administration. Phage exhibited rapid clearance and did not stimulate proinflammatory cytokines. There is also a significant reduction in proinflammatory cytokines caused by bacterial infection, reducing tissue inflammation. | [A] | [102] |
| Case reports | ||||||
| 12. | Cocktail III (Kp152, Kp154, Kp155, Kp164, Kp6377, and HD001) | K. pneumonia | Extensively drug-resistant K. pneumonia (ERKp) in UTI | Phage-resistant mutants emerged when Cocktails I and II were used. After phage therapy (Cocktail III) combined with non-active antibiotics treatment, the patient’s pathogenic ERKp was completely eliminated and there are no recurrent UTI symptoms. No signs of recurrence for 6 months of follow-up. | [A] | [97] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, K.M.; Liau, X.L.; Tang, S.S. Bacteriophages and Their Host Range in Multidrug-Resistant Bacterial Disease Treatment. Pharmaceuticals 2023, 16, 1467. https://doi.org/10.3390/ph16101467
Chung KM, Liau XL, Tang SS. Bacteriophages and Their Host Range in Multidrug-Resistant Bacterial Disease Treatment. Pharmaceuticals. 2023; 16(10):1467. https://doi.org/10.3390/ph16101467
Chicago/Turabian StyleChung, Ka Mun, Xiew Leng Liau, and Swee Seong Tang. 2023. "Bacteriophages and Their Host Range in Multidrug-Resistant Bacterial Disease Treatment" Pharmaceuticals 16, no. 10: 1467. https://doi.org/10.3390/ph16101467
APA StyleChung, K. M., Liau, X. L., & Tang, S. S. (2023). Bacteriophages and Their Host Range in Multidrug-Resistant Bacterial Disease Treatment. Pharmaceuticals, 16(10), 1467. https://doi.org/10.3390/ph16101467