
Stability Study of Parenteral N-Acetylcysteine, and Chemical Inhibition of Its Dimerization

 ,
,  , , and
, , and 
Abstract
1. Introduction
2. Results
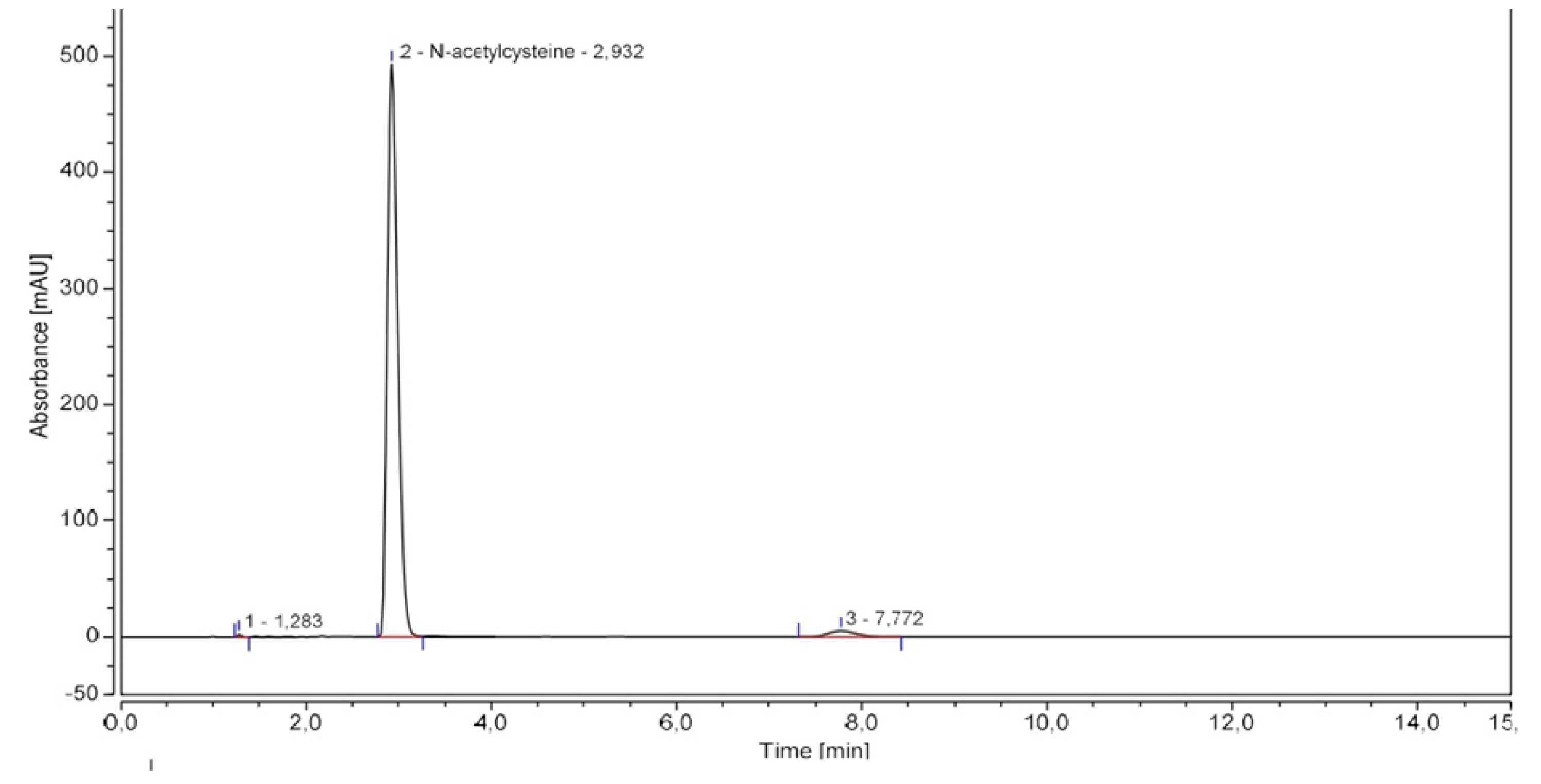
2.1. N-acetylcysteine Dosing Method Validation
2.2. Forced Degradation Studies
2.3. Stability Study
3. Discussion
4. Materials and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Downs, J.W.; Cumpston, K.L.; Kershner, E.K.; Troendle, M.M.; Rose, S.R.; Wills, B.K. Clinical outcome of massive acetaminophen overdose treated with standard-dose N-acetylcysteine. Clin. Toxicol. 2021, 59, 932–936. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.S.; Lee, N.; Chan, P.K.; Beigel, J.H. The role of adjuvant immunomodulatory agents for treatment of severe influenza. Antivir. Res. 2018, 150, 202–216. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.-J.; Huang, C.-H. The Clinical Efficacy of N-Acetylcysteine in the Treatment of ST Segment Elevation Myocardial Infarction. Int. Heart J. 2021, 62, 142–147. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. RENACTIF: Reduction of the Thrombotic Phenotype in Renal Insufficiency With N-AcetylCysteine. Identifier: NCT03636932. Available online: https://clinicaltrials.gov/ct2/show/NCT03636932 (accessed on 20 November 2022).
- Dribben, W.H.; Porto, S.M.; Jeffords, B.K. Stability and microbiology of inhalant n-acetylcysteine used as an intravenous solution for the treatment of acetaminophen poisoning. Ann. Emerg. Med. 2003, 42, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Friciu, M.M.; Monfort, A.; Dubé, P.-A.; Leclair, G. Stability of N-Acetylcysteine 60 mg/mL in Extemporaneously Compounded Injectable Solutions. Can. J. Hosp. Pharm. 2021, 74, 344. [Google Scholar] [CrossRef] [PubMed]
- The United States Pharmacopeia; USP 42 NF 37; N acetylcysteine; The United States Pharmacopeial Convention: Rockville, MD, USA, 2019; Volume 2.
- ICH Q1A (R2) Stability Testing of New Drug Substances and Drug Products—Scientific Guideline. Available online: https://www.ema.europa.eu/en/ich-q1a-r2-stability-testing-new-drug-substances-drug-products-scientific-guideline (accessed on 6 December 2022).
- ICH Q2(R2) Validation of Analytical Procedures—Scientific Guideline. Available online: https://www.ema.europa.eu/en/ich-q2r2-validation-analytical-procedures-scientific-guideline (accessed on 6 December 2022).
- FDA. Guidance for Industry: Stability Testing of Drug Substances and Drug Products (Draft guidance); Food and Drug Administration: Rockville, MD, USA, 1998.
- Barrieu, M.; Chennell, P.; Yessaad, M.; Bouattour, Y.; Wasiak, M.; Jouannet, M.; Le Basle, Y.; Sautou, V. Physicochemical Stability of a Novel Tacrolimus Ophthalmic Formulation for the Treatment of Ophthalmic Inflammatory Diseases. Pharmaceutics 2022, 14, 118. [Google Scholar] [CrossRef] [PubMed]
- D’Huart, E.; Vigneron, J.; Blaise, F.; Charmillon, A.; Demoré, B. Physicochemical Stability of Cefotaxime Sodium in Polypropylene Syringes at High Concentrations for Intensive Care Units. Pharm. Technol. Hosp. Pharm. 2019, 4, 59–67. [Google Scholar] [CrossRef]
- Curti, C.; Lamy, E.; Primas, N.; Fersing, C.; Jean, C.; Bertault-Peres, P.; Vanelle, P. Stability studies of five anti-infectious eye drops under exhaustive storage conditions. Die Pharm.-Int. J. Pharm. Sci. 2017, 72, 741–746. [Google Scholar] [CrossRef]
- Council of Europe. European Pharmacopoeia (10.0); Acetylcysteine monograph; European Directorate for the Quality of Medicines & HealthCare: Strasbourg, France, 2022.
- González-González, O.; Ramirez, I.O.; Ramirez, B.I.; O’Connell, P.; Ballesteros, M.P.; Torrado, J.J.; Serrano, D.R. Drug Stability: ICH versus Accelerated Predictive Stability Studies. Pharmaceutics 2022, 14, 2324. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, N.B.; Lissner, L.A.; Klimaczewski, C.V.; Colpo, E.; Rocha, J.B. Ascorbic acid oxidation of thiol groups from dithiotreitol is mediated by its conversion to dehydroascorbic acid. EXCLI J. 2012, 11, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Nagy, P. Kinetics and Mechanisms of Thiol–Disulfide Exchange Covering Direct Substitution and Thiol Oxidation-Mediated Pathways. Antioxidants Redox Signal. 2013, 18, 1623–1641. [Google Scholar] [CrossRef] [PubMed]
- Crowley, P.J. Excipients as stabilizers. Pharm. Sci. Technol. Today 1999, 2, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Flora, S.J.S. Structural, Chemical and Biological Aspects of Antioxidants for Strategies Against Metal and Metalloid Exposure. Oxidative Med. Cell. Longev. 2009, 2, 191–206. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Samples | Repeatability (% RSD within-Day) | Intermediate Precision (% RSD between-Day) | Accuracy (Bias in %) |
|---|---|---|---|
| NAC 450 µg·mL−1 | 0.640% | 2.458% | −1.827% |
| NAC 500 µg·mL−1 | 0.287% | 1.909% | −1.656% |
| NAC 550 µg·mL−1 | 0.319% | 0.910% | −2.081% |
| Conditions | %RSD 1 | |
|---|---|---|
| pH of mobile phase | 2.7 | 0.887 |
| 3.0 | 0.347 | |
| 3.3 | 2.757 | |
| Composition of mobile phase | 98:2 | 0.501 |
| 97:3 | 0.347 | |
| 96:4 | 0.281 | |
| Flow | 1.8 mL·min−1 | 0.216 |
| 2.0 mL·min−1 | 0.347 | |
| 2.2 mL·min−1 | 0.244 | |
| Column | C18 Kromasil®, 4.6 × 250 mm, 5 µm | 0.089 |
| C18 XTerra®, 4.6 × 250 mm, 5 µm | 0.347 | |
| C18 Lichrospher®, 4.6 × 250 mm, 5 µm | 4.404 | |
| Wavelength | 198 nm | 1.502 |
| 200 nm | 0.347 | |
| 202 nm | 0.588 | |
| Experimental Conditions | API Degradation | Degradation Products’ Retention Times |
|---|---|---|
| Heat (80 °C, 3 h) | 24% | 1.3 min, 1.5 min, 1.8 min, 2.2 min, 5.3 min, 7.2–7.7 min |
| Light (sunlamp, 28 days) | 3% | 7.2–7.7 min |
| Oxidation (H2O2 0.3%, 3 h) | 6% | 1.6 min, 2.0 min, 7.2–7.7 min |
| Acid (HCl 0.5 M, 1 min) | 15% | 1.5 min, 1.7 min, 7.2–7.7 min |
| Alkaline (NaOH 0.1 M, 10 min) | 23% | 1.9 min, 2.0 min, 7.2–7.7 min |
| T0 | 6 h | 1 Day | 2 Days | 3 Days | 4 Days | 7 Days | 8 Days | R 2,4 | p Value 5 | |
|---|---|---|---|---|---|---|---|---|---|---|
| NAC content ± S.D. 1 | 22.82 ± 1.99 | 22.28 ± 0.18 | 22.09 ± 0.04 | 22.41 ± 0.41 | 22.22 ± 0.35 | 21.56 ± 0.23 | 21.88 ± 0.21 | 21.42 ± 0.50 | 0.65 | <0.02 |
| % NAC dimer ± S.D. 2 | 0.20 ± 0.03 | 0.29 ± 0.01 | 0.32 ± 0.01 | 0.34 ± 0.02 | 0.37 ± 0.01 | 0.42 ± 0.01 | 0.53 ± 0.02 | 0.54 ± 0.04 | 0.94 | <0.001 |
| Osmolality 3 | 511 | 500 | 510 | 508 | 524 | 510 | 515 | 512 | 0.15 | NS 6 |
| pH | 6.26 | 6.24 | 6.24 | 6.21 | 6.24 | 6.15 | 6.10 | 6.12 | 0.87 | <0.001 |
| Visible particles | none | none | none | none | none | none | none | none |
| T0 | 6 h | 1 Day | 2 Days | 3 Days | 4 Days | 7 Days | 8 Days | R 2,4 | p Value 5 | |
|---|---|---|---|---|---|---|---|---|---|---|
| NAC content ± S.D. 1 | 22.82 ± 1.99 | 22.15 ± 0.17 | 21.78 ± 0.26 | 22.03 ± 0.43 | 21.52 ± 0.29 | 21.95 ± 0.25 | 21.61 ± 0.42 | 21.27 ± 0.20 | 0.58 | <0.05 |
| % NAC dimer ± S.D. 2 | 0.20 ± 0.03 | 0.29 ± 0.01 | 0.39 ± 0.02 | 0.52 ± 0.01 | 0.61 ± 0.01 | 0.71 ± 0.02 | 1.09 ± 0.10 | 1.13 ± 0.18 | 0.99 | <0.001 |
| Osmolality 3 | 511 | 508 | 507 | 507 | 505 | 521 | 515 | 520 | 0.48 | NS 6 |
| pH | 6.26 | 6.13 | 6.11 | 6.04 | 6.05 | 6.04 | 6.04 | 5.95 | 0.65 | <0.02 |
| Visible particles | none | none | none | none | none | none | none | none |
| T0 | 4 Days | 8 Days | ||
|---|---|---|---|---|
| Control | % NAC dimer | 0.20 | 0.42 | 0.54 |
| variation from baseline | ×2.1 | ×2.7 | ||
| ascorbic acid 12.5 mg·mL−1 | % NAC dimer | 0.27 | 2.08 | 3.68 |
| variation from baseline | ×7.7 | ×13.6 | ||
| Sodium edetate 2 mg·mL−1 | % NAC dimer | 0.39 | 0.50 | 0.64 |
| variation from baseline | ×1.3 | ×1.6 | ||
| Zinc gluconate 12.5 µg·mL−1 | % NAC dimer | 0.36 | 0.48 | 0.58 |
| variation from baseline | ×1.3 | ×1.6 | ||
| Zinc gluconate 62.5 µg·mL−1 | % NAC dimer | 0.28 | 0.33 | 0.36 |
| variation from baseline | ×1.2 | ×1.3 | ||
| Zinc gluconate 125 µg·mL−1 | % NAC dimer | 0.31 | 0.29 | 0.25 |
| variation from baseline | ×0.9 | ×0.8 | ||
| Tocopherol 1.25 mg·mL−1 | % NAC dimer | 0.28 | 0.46 | 0.63 |
| variation from baseline | ×1.6 | ×2.3 |
| T0 | 1 Day | 2 Days | 3 Days | 4 Days | 7 Days | 8 Days | R 2,4 | p Value 5 | |
|---|---|---|---|---|---|---|---|---|---|
| NAC content ± S.D. 1 | 21.78 ± 0.20 | 21.97 ± 0.43 | 22.33 ± 0.60 | 22.42 ± 0.61 | 22.17 ± 0.10 | 22.57 ± 0.13 | 23.25 ± 0.05 | 0.80 | <0.01 |
| % NAC dimer ± S.D. 2 | 0.28 ± 0.03 | 0.28 ± 0.03 | 0.30 ± 0.04 | 0.32 ± 0.03 | 0.34 ± 0.01 | 0.36 ± 0.01 | 0.36 ± 0.01 | 0.92 | <0.001 |
| Osmolality 3 | 499 | 512 | 505 | 502 | 526 | 522 | 484 | 0.01 | NS 6 |
| pH | 5.22 | 5.14 | 5.19 | 5.19 | 5.21 | 5.14 | 5.20 | 0.03 | NS 6 |
| Sterility | Sterile | ND | ND | ND | Sterile | ND | Sterile | ||
| Endotoxins 4 | 0.1< | ND | ND | ND | 0.1< | ND | 0.1< | ||
| Visible particles | none | none | none | none | none | none | none |
| T0 | 1 Day | 2 Days | 3 Days | 4 Days | 7 Days | 8 Days | R 2,4 | p Value 5 | |
|---|---|---|---|---|---|---|---|---|---|
| NAC content ± S.D. 1 | 22.10 ± 0.20 | 21.93 ± 0.18 | 21.40 ± 0.15 | 21.58 ± 0.08 | 21.65 ± 0.10 | 21.17 ± 0.08 | 21.23 ± 0.18 | 0.75 | <0.02 |
| % NAC dimer ± S.D. 2 | 0.27 ± 0.03 | 0.29 ± 0.03 | 0.34 ± 0.03 | 0.38 ± 0.04 | 0.42 ± 0.05 | 0.50 ± 0.04 | 0.53 ± 0.04 | 0.99 | <0.001 |
| Osmolality 3 | 541 | 540 | 580 | 584 | 569 | 540 | 538 | 0.06 | NS 6 |
| pH | 5.29 | 5.29 | 5.31 | 5.32 | 5.33 | 5.41 | 5.43 | 0.96 | <0.001 |
| Sterility | Sterile | ND | ND | ND | Sterile | ND | Sterile | ||
| Endotoxins 4 | 0.1< | ND | ND | ND | 0.1< | ND | 0.1< | ||
| Visible particles | none | none | none | none | none | none | none |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Primas, N.; Lano, G.; Brun, D.; Curti, C.; Sallée, M.; Sampol-Manos, E.; Lamy, E.; Bornet, C.; Burtey, S.; Vanelle, P. Stability Study of Parenteral N-Acetylcysteine, and Chemical Inhibition of Its Dimerization. Pharmaceuticals 2023, 16, 72. https://doi.org/10.3390/ph16010072
Primas N, Lano G, Brun D, Curti C, Sallée M, Sampol-Manos E, Lamy E, Bornet C, Burtey S, Vanelle P. Stability Study of Parenteral N-Acetylcysteine, and Chemical Inhibition of Its Dimerization. Pharmaceuticals. 2023; 16(1):72. https://doi.org/10.3390/ph16010072
Chicago/Turabian StylePrimas, Nicolas, Guillaume Lano, Damien Brun, Christophe Curti, Marion Sallée, Emmanuelle Sampol-Manos, Edouard Lamy, Charleric Bornet, Stéphane Burtey, and Patrice Vanelle. 2023. "Stability Study of Parenteral N-Acetylcysteine, and Chemical Inhibition of Its Dimerization" Pharmaceuticals 16, no. 1: 72. https://doi.org/10.3390/ph16010072
APA StylePrimas, N., Lano, G., Brun, D., Curti, C., Sallée, M., Sampol-Manos, E., Lamy, E., Bornet, C., Burtey, S., & Vanelle, P. (2023). Stability Study of Parenteral N-Acetylcysteine, and Chemical Inhibition of Its Dimerization. Pharmaceuticals, 16(1), 72. https://doi.org/10.3390/ph16010072