

Association between Use of Spironolactone and Risk of Stroke in Hypertensive Patients: A Cohort Study


Abstract
1. Introduction
2. Results
2.1. Study Population
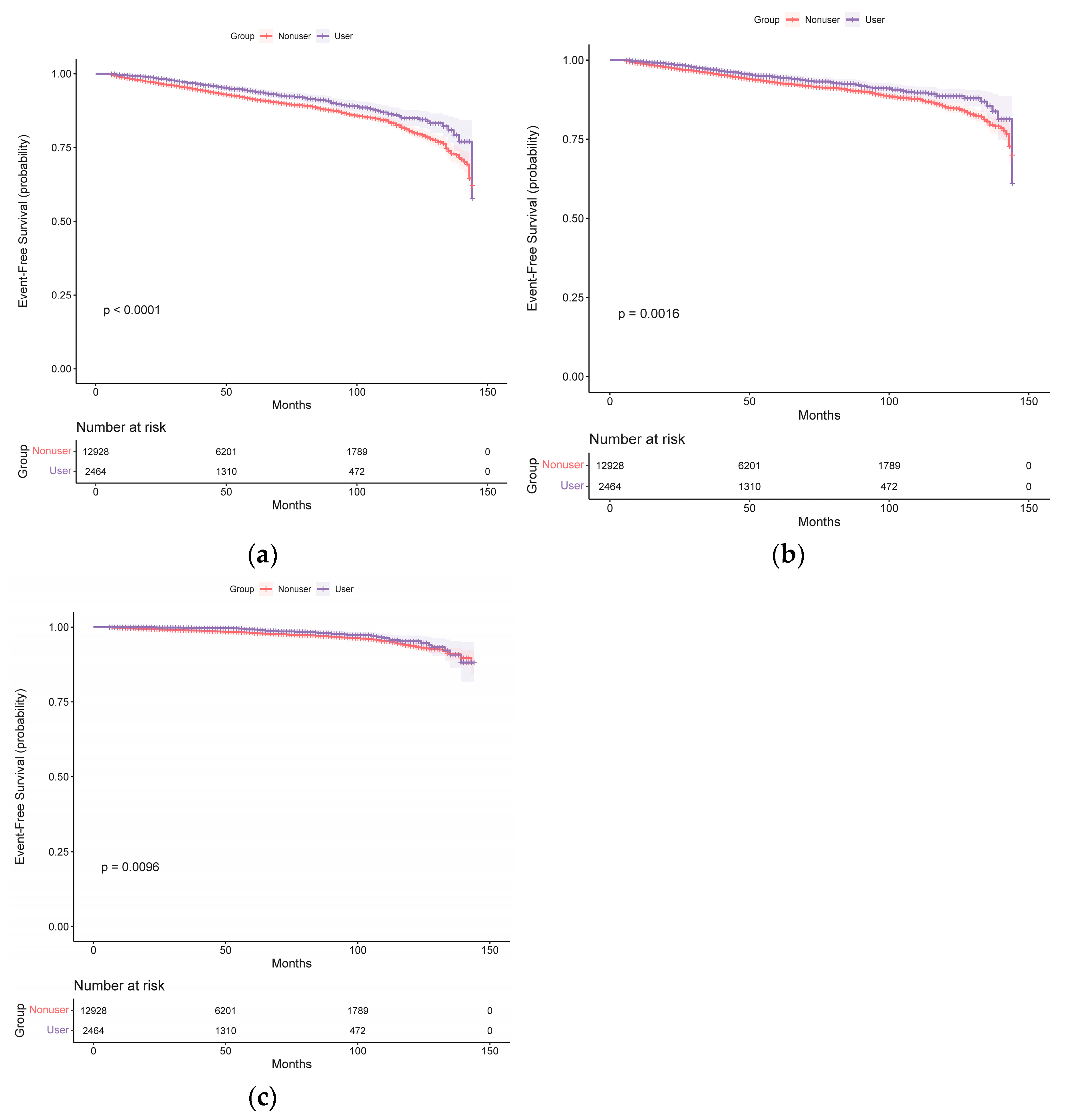
2.2. Spironolactone Use and Stroke Risk in the Unmatched Original Cohort
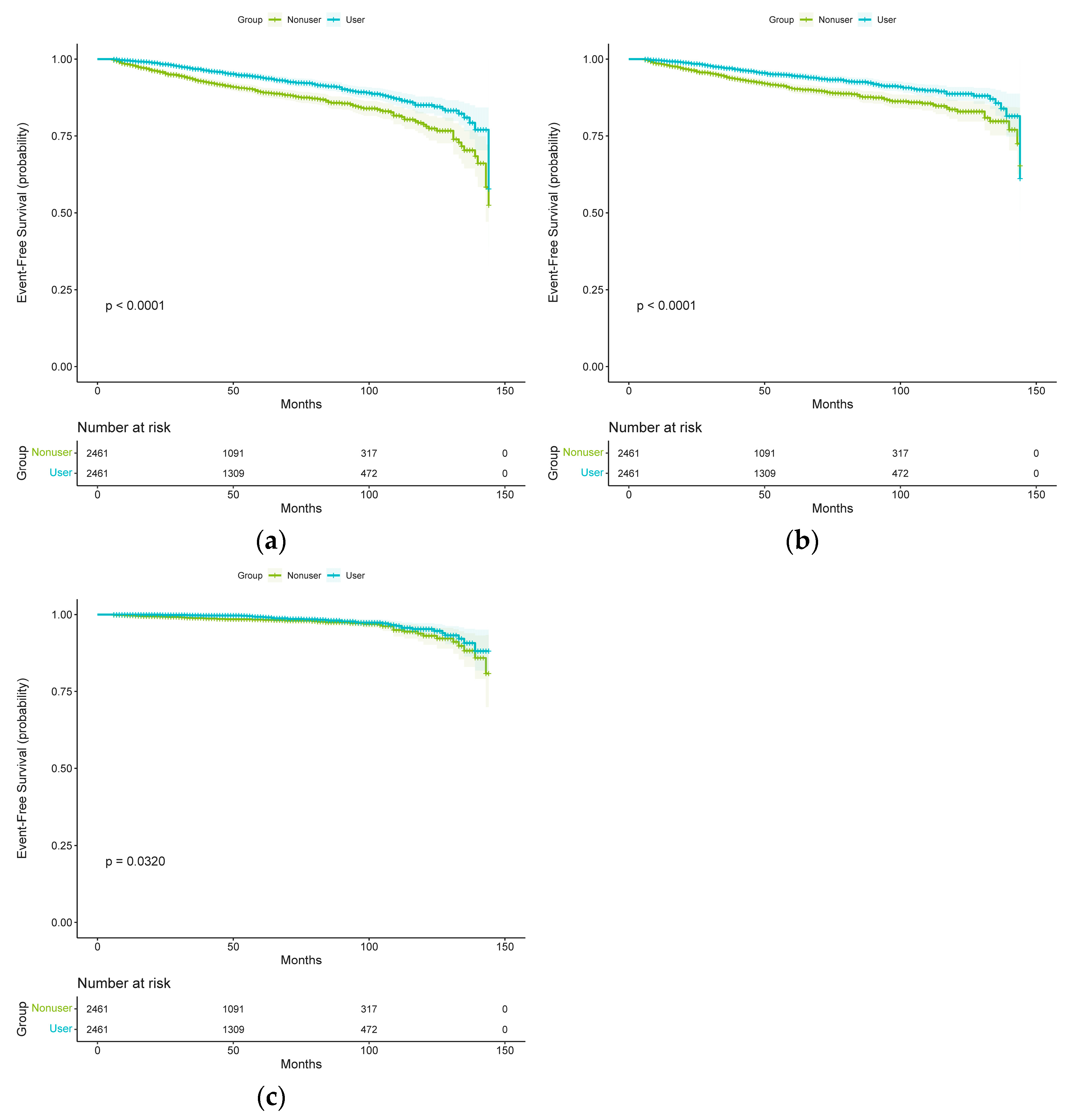
2.3. Spironolactone Use and Stroke Risk in Propensity-Score-Matched Cohort
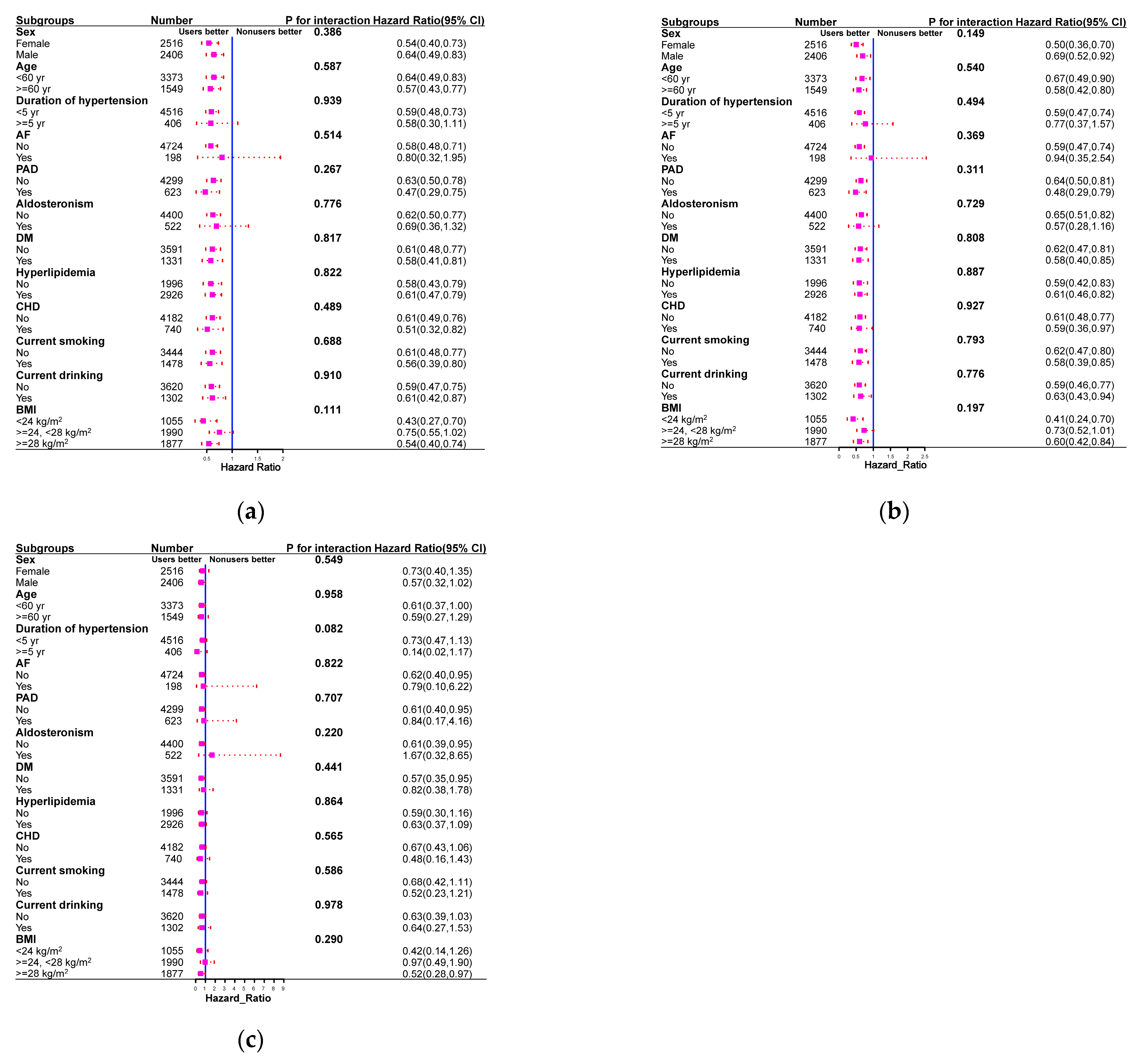
2.4. Subgroups and Sensitivity Analyses
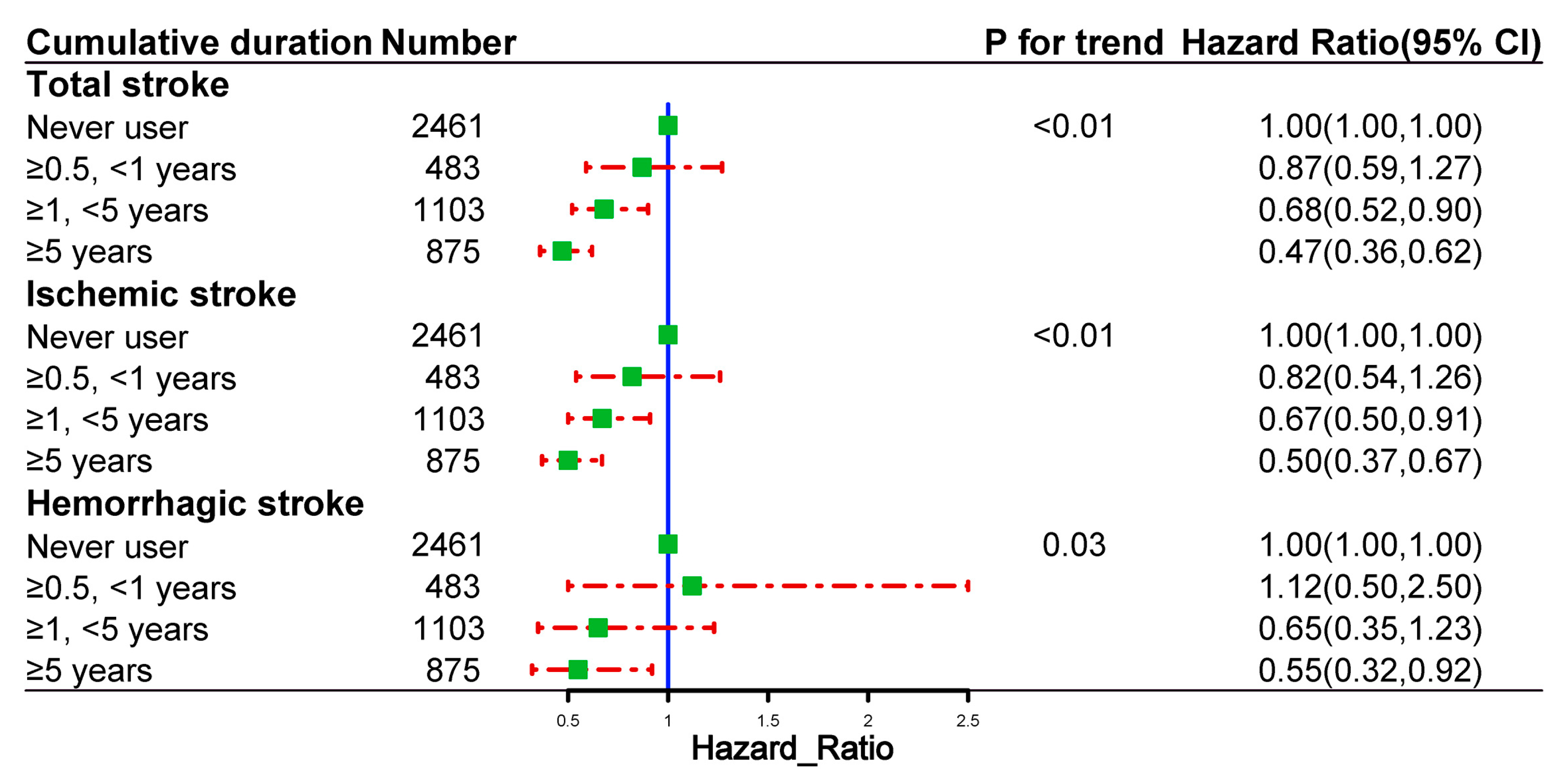
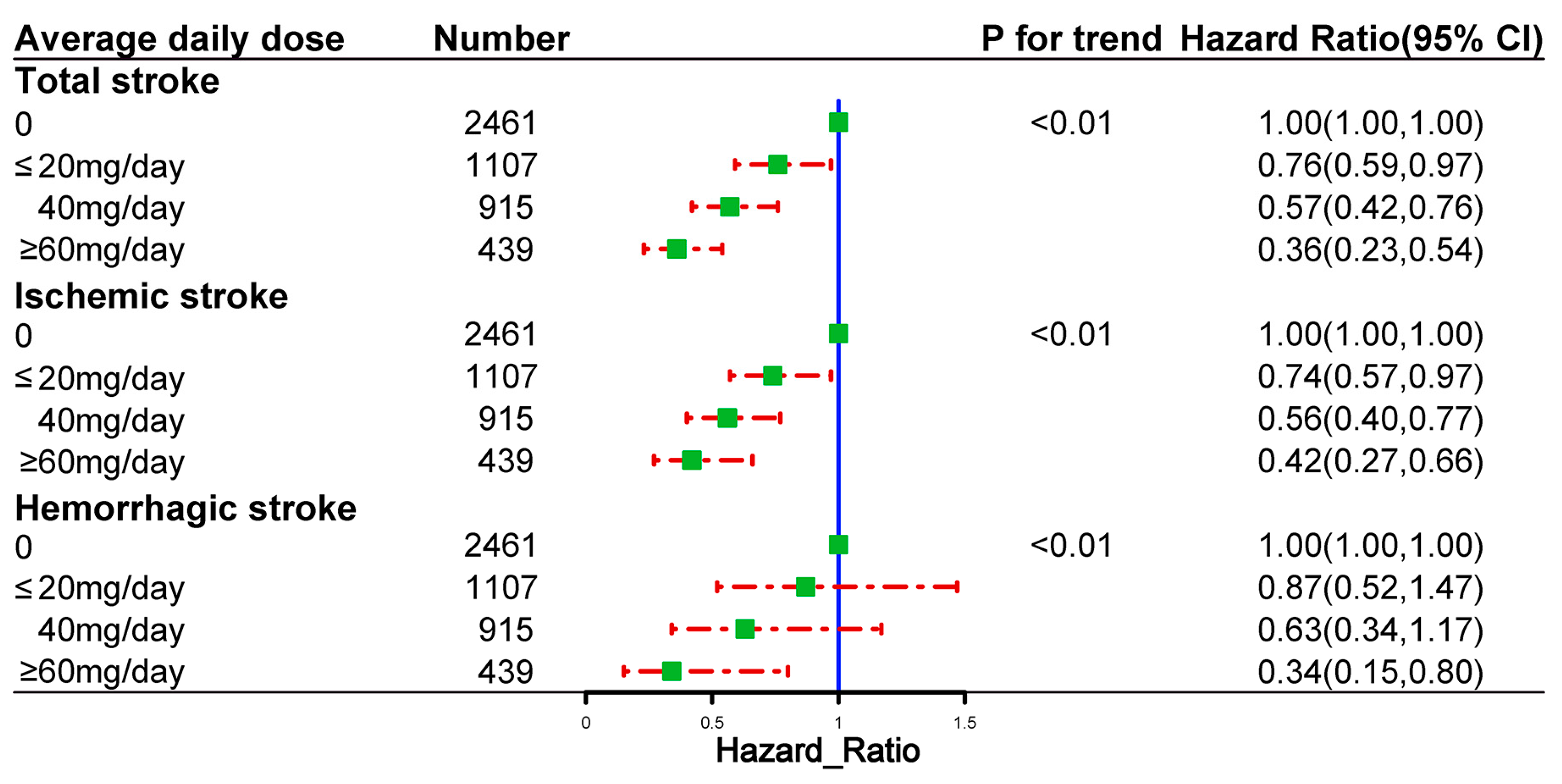
2.5. Dose and Cumulative Duration of Spironolactone Use and the Risk of Outcome Events
2.6. Safety Outcome
3. Discussion
4. Materials and Methods
4.1. Study Design and Participants
4.2. Variables
4.3. Follow-Up and Outcomes
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Wu, B.; Liu, M.; Chen, Z.; Wang, W.; Anderson, C.S.; Sandercock, P.; Wang, Y.; Huang, Y.; Cui, L.; et al. Stroke in China: Advances and challenges in epidemiology, prevention, and management. Lancet Neurol. 2019, 18, 394–405. [Google Scholar] [CrossRef] [PubMed]
- Ma, Q.; Li, R.; Wang, L.; Yin, P.; Wang, Y.; Yan, C.; Ren, Y.; Qian, Z.; Vaughn, M.G.; McMillin, S.E.; et al. Temporal trend and attributable risk factors of stroke burden in China, 1990-2019: An analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2021, 6, e897–e906. [Google Scholar] [CrossRef]
- Lioutas, V.A.; Ivan, C.S.; Himali, J.J.; Aparicio, H.J.; Leveille, T.; Romero, J.R.; Beiser, A.S.; Seshadri, S. Incidence of Transient Ischemic Attack and Association With Long-term Risk of Stroke. JAMA 2021, 325, 373–381. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.J.; Chin, S.L.; Rangarajan, S.; Xavier, D.; Liu, L.; Zhang, H.; Rao-Melacini, P.; Zhang, X.; Pais, P.; Agapay, S.; et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): A case-control study. Lancet 2016, 388, 761–775. [Google Scholar] [CrossRef]
- Owolabi, M.O.; Thrift, A.G.; Mahal, A.; Ishida, M.; Martins, S.; Johnson, W.D.; Pandian, J.; Abd-Allah, F.; Yaria, J.; Phan, H.T.; et al. Primary stroke prevention worldwide: Translating evidence into action. Lancet Public Health 2022, 7, e74–e85. [Google Scholar] [CrossRef]
- Santos, D.; Dhamoon, M.S. Trends in Antihypertensive Medication Use Among Individuals With a History of Stroke and Hypertension, 2005 to 2016. JAMA Neurol. 2020, 77, 1382–1389. [Google Scholar] [CrossRef]
- McCarthy, J.; Yang, J.; Clissold, B.; Young, M.J.; Fuller, P.J.; Phan, T. Hypertension Management in Stroke Prevention: Time to Consider Primary Aldosteronism. Stroke 2021, 52, e626–e634. [Google Scholar] [CrossRef]
- Chang, Y.H.; Chung, S.D.; Wu, C.H.; Chueh, J.S.; Chen, L.; Lin, P.C.; Lin, Y.H.; Huang, K.H.; Wu, V.C.; Chu, T.S. Surgery decreases the long-term incident stroke risk in patients with primary aldosteronism. Surgery 2020, 167, 367–377. [Google Scholar] [CrossRef]
- Lin, X.; Ullah, M.; Wu, X.; Xu, F.; Shan, S.K.; Lei, L.M.; Yuan, L.Q.; Liu, J. Cerebro-Cardiovascular Risk, Target Organ Damage, and Treatment Outcomes in Primary Aldosteronism. Front. Cardiovasc. Med. 2021, 8, 798364. [Google Scholar] [CrossRef]
- Monticone, S.; D’Ascenzo, F.; Moretti, C.; Williams, T.A.; Veglio, F.; Gaita, F.; Mulatero, P. Cardiovascular events and target organ damage in primary aldosteronism compared with essential hypertension: A systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2018, 6, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Takeda, R.; Matsubara, T.; Miyamori, I.; Hatakeyama, H.; Morise, T. Vascular complications in patients with aldosterone producing adenoma in Japan: Comparative study with essential hypertension. The Research Committee of Disorders of Adrenal Hormones in Japan. J. Endocrinol. Investig. 1995, 18, 370–373. [Google Scholar] [CrossRef]
- Satoh, M.; Kikuya, M.; Ohkubo, T.; Mori, T.; Metoki, H.; Hara, A.; Utsugi, M.T.; Hashimoto, T.; Hirose, T.; Obara, T.; et al. Aldosterone-to-renin ratio as a predictor of stroke under conditions of high sodium intake: The Ohasama study. Am. J. Hypertens. 2012, 25, 777–783. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chrissobolis, S.; Drummond, G.R.; Faraci, F.M.; Sobey, C.G. Chronic aldosterone administration causes Nox2-mediated increases in reactive oxygen species production and endothelial dysfunction in the cerebral circulation. J. Hypertens. 2014, 32, 1815–1821. [Google Scholar] [CrossRef] [PubMed]
- Born-Frontsberg, E.; Reincke, M.; Rump, L.C.; Hahner, S.; Diederich, S.; Lorenz, R.; Allolio, B.; Seufert, J.; Schirpenbach, C.; Beuschlein, F.; et al. Cardiovascular and cerebrovascular comorbidities of hypokalemic and normokalemic primary aldosteronism: Results of the German Conn’s Registry. J. Clin. Endocrinol. Metab. 2009, 94, 1125–1130. [Google Scholar] [CrossRef] [PubMed]
- Petramala, L.; Pignatelli, P.; Carnevale, R.; Zinnamosca, L.; Marinelli, C.; Settevendemmie, A.; Concistrè, A.; Tonnarini, G.; De Toma, G.; Violi, F.; et al. Oxidative stress in patients affected by primary aldosteronism. J. Hypertens. 2014, 32, 2022–2029; discussion 2029. [Google Scholar] [CrossRef] [PubMed]
- Barrera-Chimal, J.; Bonnard, B.; Jaisser, F. Roles of Mineralocorticoid Receptors in Cardiovascular and Cardiorenal Diseases. Annu. Rev. Physiol. 2022, 84, 585–610. [Google Scholar] [CrossRef]
- Bauersachs, J.; Jaisser, F.; Toto, R. Mineralocorticoid receptor activation and mineralocorticoid receptor antagonist treatment in cardiac and renal diseases. Hypertension 2015, 65, 257–263. [Google Scholar] [CrossRef]
- Barrera-Chimal, J.; Lima-Posada, I.; Bakris, G.L.; Jaisser, F. Mineralocorticoid receptor antagonists in diabetic kidney disease—Mechanistic and therapeutic effects. Nat. Rev. Nephrol. 2022, 18, 56–70. [Google Scholar] [CrossRef]
- Beldhuis, I.E.; Myhre, P.L.; Bristow, M.; Claggett, B.; Damman, K.; Fang, J.C.; Fleg, J.L.; McKinlay, S.; Lewis, E.F.; O’Meara, E.; et al. Spironolactone in Patients With Heart Failure, Preserved Ejection Fraction, and Worsening Renal Function. J. Am. Coll. Cardiol. 2021, 77, 1211–1221. [Google Scholar] [CrossRef]
- Solomon, S.D.; Claggett, B.; Lewis, E.F.; Desai, A.; Anand, I.; Sweitzer, N.K.; O’Meara, E.; Shah, S.J.; McKinlay, S.; Fleg, J.L.; et al. Influence of ejection fraction on outcomes and efficacy of spironolactone in patients with heart failure with preserved ejection fraction. Eur. Heart J. 2016, 37, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, Y.; Mori, Y.; Kageyama, S.; Arihara, K.; Sugiyama, T.; Ohmura, H.; Yakushigawa, T.; Sugiyama, H.; Shimada, Y.; Nojima, Y.; et al. Spironolactone reduces cardiovascular and cerebrovascular morbidity and mortality in hemodialysis patients. J. Am. Coll. Cardiol. 2014, 63, 528–536. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Norrving, B.; George, M.G.; Foltz, J.L.; Roth, G.A.; Mensah, G.A. Prevention of stroke: A strategic global imperative. Nat. Rev. Neurol. 2016, 12, 501–512. [Google Scholar] [CrossRef]
- Huo, Y.; Li, J.; Qin, X.; Huang, Y.; Wang, X.; Gottesman, R.F.; Tang, G.; Wang, B.; Chen, D.; He, M.; et al. Efficacy of folic acid therapy in primary prevention of stroke among adults with hypertension in China: The CSPPT randomized clinical trial. JAMA 2015, 313, 1325–1335. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Rigsby, C.S.; Cannady, W.E.; Dorrance, A.M. Aldosterone: Good guy or bad guy in cerebrovascular disease. Trends Endocrinol. Metab. 2005, 16, 401–406. [Google Scholar] [CrossRef]
- Stier, C.T., Jr.; Rocha, R.; Chander, P.N. Effect of aldosterone and MR blockade on the brain and the kidney. Heart Fail. Rev. 2005, 10, 53–62. [Google Scholar] [CrossRef]
- Catena, C.; Colussi, G.; Nait, F.; Martinis, F.; Pezzutto, F.; Sechi, L.A. Aldosterone and the heart: Still an unresolved issue. Front. Endocrinol. 2014, 5, 168. [Google Scholar] [CrossRef]
- Jaisser, F.; Farman, N. Emerging Roles of the Mineralocorticoid Receptor in Pathology: Toward New Paradigms in Clinical Pharmacology. Pharmacol. Rev. 2016, 68, 49–75. [Google Scholar] [CrossRef]
- Parviz, Y.; Iqbal, J.; Pitt, B.; Adlam, D.; Al-Mohammad, A.; Zannad, F. Emerging cardiovascular indications of mineralocorticoid receptor antagonists. Trends Endocrinol. Metab. 2015, 26, 201–211. [Google Scholar] [CrossRef]
- Dorrance, A.M.; Rupp, N.C.; Nogueira, E.F. Mineralocorticoid receptor activation causes cerebral vessel remodeling and exacerbates the damage caused by cerebral ischemia. Hypertension 2006, 47, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Rocha, R.; Chander, P.N.; Khanna, K.; Zuckerman, A.; Stier, C.T., Jr. Mineralocorticoid blockade reduces vascular injury in stroke-prone hypertensive rats. Hypertension 1998, 31, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Dorrance, A.M.; Osborn, H.L.; Grekin, R.; Webb, R.C. Spironolactone reduces cerebral infarct size and EGF-receptor mRNA in stroke-prone rats. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2001, 281, R944–R950. [Google Scholar] [CrossRef] [PubMed]
- Rigsby, C.S.; Burch, A.E.; Ogbi, S.; Pollock, D.M.; Dorrance, A.M. Intact female stroke-prone hypertensive rats lack responsiveness to mineralocorticoid receptor antagonists. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2007, 293, R1754–R1763. [Google Scholar] [CrossRef]
- Rigsby, C.S.; Pollock, D.M.; Dorrance, A.M. Spironolactone improves structure and increases tone in the cerebral vasculature of male spontaneously hypertensive stroke-prone rats. Microvasc. Res. 2007, 73, 198–205. [Google Scholar] [CrossRef] [PubMed]
- McClain, J.L.; Dorrance, A.M. Temporary mineralocorticoid receptor antagonism during the development of hypertension improves cerebral artery dilation. Exp. Biol. Med. (Maywood) 2014, 239, 619–627. [Google Scholar] [CrossRef]
- McGraw, A.P.; Bagley, J.; Chen, W.S.; Galayda, C.; Nickerson, H.; Armani, A.; Caprio, M.; Carmeliet, P.; Jaffe, I.Z. Aldosterone increases early atherosclerosis and promotes plaque inflammation through a placental growth factor-dependent mechanism. J. Am. Heart Assoc. 2013, 2, e000018. [Google Scholar] [CrossRef]
- Guo, C.; Ricchiuti, V.; Lian, B.Q.; Yao, T.M.; Coutinho, P.; Romero, J.R.; Li, J.; Williams, G.H.; Adler, G.K. Mineralocorticoid receptor blockade reverses obesity-related changes in expression of adiponectin, peroxisome proliferator-activated receptor-gamma, and proinflammatory adipokines. Circulation 2008, 117, 2253–2261. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unmatched Original Cohort | Propensity-Score-Matched Cohort | |||||
|---|---|---|---|---|---|---|
| Characteristic | Non-User Group | User Group | ASD | Non-User Group | User Group | ASD |
| No. of participants | 12928 | 2464 | 2461 | 2461 | ||
| Age, year | 51.55 ± 12.22 | 53.22 ± 11.64 | 0.14 | 53.20 ± 12.30 | 53.23 ± 11.63 | 0.00 |
| Male, % | 7005 (54.18%) | 1202 (48.78%) | 0.11 | 1206 (49.00%) | 1200 (48.76%) | 0.00 |
| Current smoker, % | 3824 (29.58%) | 734 (29.79%) | 0.00 | 746 (30.31%) | 732 (29.74%) | 0.01 |
| Current drinker, % | 3449 (26.68%) | 665 (26.99%) | 0.01 | 639 (25.97%) | 663 (26.94%) | 0.02 |
| Duration of hypertension, % | 0.04 | 0.04 | ||||
| <5 year | 11918 (92.19%) | 2246 (91.15%) | 2273 (92.36%) | 2243 (91.14%) | ||
| ≥5 year | 1010 (7.81%) | 218 (8.85%) | 188 (7.64%) | 218 (8.86%) | ||
| Hemodynamics | ||||||
| Heart rate, bpm | 80.78 ± 10.37 | 80.85 ± 10.41 | 0.01 | 80.84 ± 10.56 | 80.85 ± 10.41 | 0.00 |
| Diastolic blood pressure, mmHg | 89.25 ± 14.58 | 89.04 ± 14.57 | 0.01 | 88.94 ± 14.36 | 89.04 ± 14.58 | 0.01 |
| Systolic blood pressure, mmHg | 144.54 ± 21.29 | 144.06 ± 20.74 | 0.02 | 143.80 ± 20.95 | 144.07 ± 20.75 | 0.01 |
| Body mass index, kg/m2 | 27.10 ± 3.86 | 27.05 ± 3.91 | 0.01 | 27.07 ± 3.82 | 27.05 ± 3.91 | 0.01 |
| Laboratory data | ||||||
| Alanine aminotransferase, U/L | 24.00 (15.00–35.36) | 24.30 (15.27–35.89) | 0.03 | 24.00 (15.00–34.34) | 24.29 (15.28–35.90) | 0.05 |
| Aspartate aminotransferase, U/L | 21.16 (16.19–28.00) | 21.00 (16.40–28.13) | 0.01 | 21.00 (16.00–27.96) | 21.00 (16.41–28.15) | 0.01 |
| Gamma-glutamyl transferase, U/L | 28.13 (17.71–42.00) | 29.04 (18.47–43.12) | 0.07 | 28.71 (17.79–42.00) | 29.00 (18.47–43.14) | 0.06 |
| Estimated glomerular filtration rate, mL/(min*1.73 m2) | 96.96 ± 18.49 | 96.24 ± 19.91 | 0.04 | 96.32 ± 19.37 | 95.49 ± 20.14 | 0.04 |
| Total cholesterol, mmol/L | 4.52 ± 1.01 | 4.49 ± 1.00 | 0.04 | 4.51 ± 1.01 | 4.49 ± 1.00 | 0.03 |
| Triglyceride, mmol/L | 1.60 (1.10–2.38) | 1.63 (1.12–2.45) | 0.05 | 1.92 ± 1.36 | 2.00 ± 1.57 | 0.06 |
| High-density lipoprotein cholesterol, mmol/L | 1.08 ± 0.29 | 1.07 ± 0.28 | 0.02 | 1.08 ± 0.29 | 1.07 ± 0.28 | 0.04 |
| Low-density lipoprotein cholesterol, mmol/L | 2.79 ± 0.84 | 2.72 ± 0.82 | 0.08 | 2.72 ± 0.86 | 2.72 ± 0.82 | 0.01 |
| Hemoglobin A1c, % | 6.12 ± 1.24 | 6.14 ± 1.29 | 0.01 | 6.17 ± 1.24 | 6.14 ± 1.29 | 0.03 |
| Fasting plasma glucose, mmol/L | 5.37 ± 1.82 | 5.41 ± 1.87 | 0.02 | 5.34 ± 1.91 | 5.41 ± 1.87 | 0.04 |
| Plasma aldosterone concentration, ng/dL | 16.51 ± 7.05 | 16.38 ± 7.04 | 0.02 | 16.48 ± 6.87 | 16.38 ± 7.04 | 0.01 |
| High-sensitivity C-reactive protein, mg/L | 2.68 (0.99–6.55) | 2.64 (1.01–6.97) | 0.02 | 2.86 (1.56–6.36) | 2.90 (1.20-7.34) | 0.02 |
| Comorbidity | ||||||
| Chronic kidney disease, % | 412 (3.19%) | 143 (5.80%) | 0.13 | 122 (4.96%) | 143 (5.81%) | 0.04 |
| Heart failure, % | 209 (1.62%) | 118 (4.79%) | 0.18 | 98 (3.98%) | 118 (4.79%) | 0.04 |
| Atrial fibrillation, % | 285 (2.20%) | 87 (3.53%) | 0.08 | 112 (4.55%) | 86 (3.49%) | 0.05 |
| Peripheral artery disease, % | 1318 (10.19%) | 292 (11.85%) | 0.05 | 332 (13.49%) | 291 (11.82%) | 0.05 |
| Aldosteronism, % | 476 (3.68%) | 264 (10.71%) | 0.27 | 261 (10.61%) | 261 (10.61%) | 0.00 |
| Diabetes mellitus, % | 3165 (24.48%) | 671 (27.23%) | 0.06 | 661 (26.86%) | 670 (27.22%) | 0.01 |
| Hyperlipidemia, % | 7489 (57.93%) | 1472 (59.74%) | 0.04 | 1456 (59.16%) | 1470 (59.73%) | 0.01 |
| Coronary heart disease, % | 1736 (13.43%) | 365 (14.81%) | 0.04 | 376 (15.28%) | 364 (14.79%) | 0.01 |
| Co-medications | ||||||
| Statins, % | 5612 (43.41%) | 1158 (47.00%) | 0.07 | 1134 (46.08%) | 1156 (46.97%) | 0.02 |
| Aspirin, % | 8307 (64.26%) | 1653 (67.09%) | 0.06 | 1641 (66.68%) | 1652 (67.13%) | 0.01 |
| Calcium channel blockers, % | 9997 (77.33%) | 1972 (80.03%) | 0.07 | 2018 (82.00%) | 1970 (80.05%) | 0.05 |
| ACEI/ARB, % | 9616 (74.38%) | 1768 (71.75%) | 0.06 | 1717 (69.77%) | 1766 (71.76%) | 0.04 |
| Beta blockers, % | 4880 (37.75%) | 969 (39.33%) | 0.03 | 957 (38.89%) | 967 (39.29%) | 0.01 |
| Other diuretics, % | 1411 (10.91%) | 325 (13.19%) | 0.07 | 307 (12.47%) | 325 (13.21%) | 0.02 |
| Insulin, % | 1116 (8.63%) | 227 (9.21%) | 0.02 | 220 (8.94%) | 227 (9.22%) | 0.01 |
| Oral antidiabetic agents, % | 2117 (16.38%) | 439 (17.82%) | 0.04 | 388 (15.77%) | 438 (17.80%) | 0.05 |
| Unmatched Original Cohort | Propensity-Score-Matched Cohort | |||||
|---|---|---|---|---|---|---|
| Non-User Group | User Group | E Value | Non-User Group | User Group | E Value | |
| Total stroke | ||||||
| No. of events (%) | 1110 (8.6%) | 169 (6.9%) | 244 (9.9%) | 168 (6.8%) | ||
| IR per 1000 person-years (95% CI) | 18.96 (17.86, 20.11) | 13.80 (11.80, 16.05) | 23.09 (20.28, 26.18) | 13.73 (11.73, 15.97) | ||
| Unadjusted HR (95% CI) | 1.00 (reference) | 0.71 (0.61, 0.84) | 2.17 | 1.00 (reference) | 0.59 (0.48, 0.72) | 2.78 |
| Multivariable-adjusted HR (95% CI) | 1.00 (reference) | 0.69 (0.59, 0.81) | 2.26 | 1.00 (reference) | 0.60 (0.49, 0.73) | 2.72 |
| Propensity-score-adjusted HR (95% CI) | 1.00 (reference) | 0.68 (0.58, 0.80) | 2.30 | 1.00 (reference) | 0.59 (0.49, 0.72) | 2.78 |
| Types of stroke | ||||||
| Ischemic stroke | ||||||
| No. of events (%) | 877 (6.8%) | 139 (5.6%) | 200 (8.1%) | 138 (5.6%) | ||
| IR per 1000 person-years (95% CI) | 14.98 (14.00, 16.00) | 11.35 (9.54, 13.40) | 18.92 (16.39, 21.73) | 11.28 (9.48, 13.33) | ||
| Unadjusted HR (95% CI) | 1.00 (reference) | 0.75 (0.63, 0.90) | 2.00 | 1.00 (reference) | 0.60 (0.48, 0.74) | 2.72 |
| Multivariable-adjusted HR (95% CI) | 1.00 (reference) | 0.71 (0.60, 0.85) | 2.17 | 1.00 (reference) | 0.61 (0.49, 0.76) | 2.66 |
| Propensity-score-adjusted HR (95% CI) | 1.00 (reference) | 0.71 (0.59, 0.85) | 2.17 | 1.00 (reference) | 0.60 (0.49, 0.75) | 2.72 |
| Hemorrhagic stroke | ||||||
| No. of events (%) | 275 (2.1%) | 39 (1.6%) | 50 (2.0%) | 39 (1.5%) | ||
| IR per 1000 person-years (95% CI) | 4.70 (4.16, 5.29) | 3.19 (2.27, 4.35) | 4.73 (3.51, 6.24) | 3.19 (2.27, 4.36) | ||
| Unadjusted HR (95% CI) | 1.00 (reference) | 0.64 (0.46, 0.90) | 2.50 | 1.00 (reference) | 0.63 (0.42, 0.96) | 2.55 |
| Multivariable-adjusted HR (95% CI) | 1.00 (reference) | 0.66 (0.47, 0.92) | 2.40 | 1.00 (reference) | 0.63 (0.42, 0.96) | 2.55 |
| Propensity-score-adjusted HR (95% CI) | 1.00 (reference) | 0.63 (0.45, 0.88) | 2.55 | 1.00 (reference) | 0.64 (0.42, 0.97) | 2.50 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, X.; Li, N. Association between Use of Spironolactone and Risk of Stroke in Hypertensive Patients: A Cohort Study. Pharmaceuticals 2023, 16, 57. https://doi.org/10.3390/ph16010057
Cai X, Li N. Association between Use of Spironolactone and Risk of Stroke in Hypertensive Patients: A Cohort Study. Pharmaceuticals. 2023; 16(1):57. https://doi.org/10.3390/ph16010057
Chicago/Turabian StyleCai, Xintian, and Nanfang Li. 2023. "Association between Use of Spironolactone and Risk of Stroke in Hypertensive Patients: A Cohort Study" Pharmaceuticals 16, no. 1: 57. https://doi.org/10.3390/ph16010057
APA StyleCai, X., & Li, N. (2023). Association between Use of Spironolactone and Risk of Stroke in Hypertensive Patients: A Cohort Study. Pharmaceuticals, 16(1), 57. https://doi.org/10.3390/ph16010057