
Prolactin Relationship with Fertility and In Vitro Fertilization Outcomes—A Review of the Literature


Abstract
1. Introduction
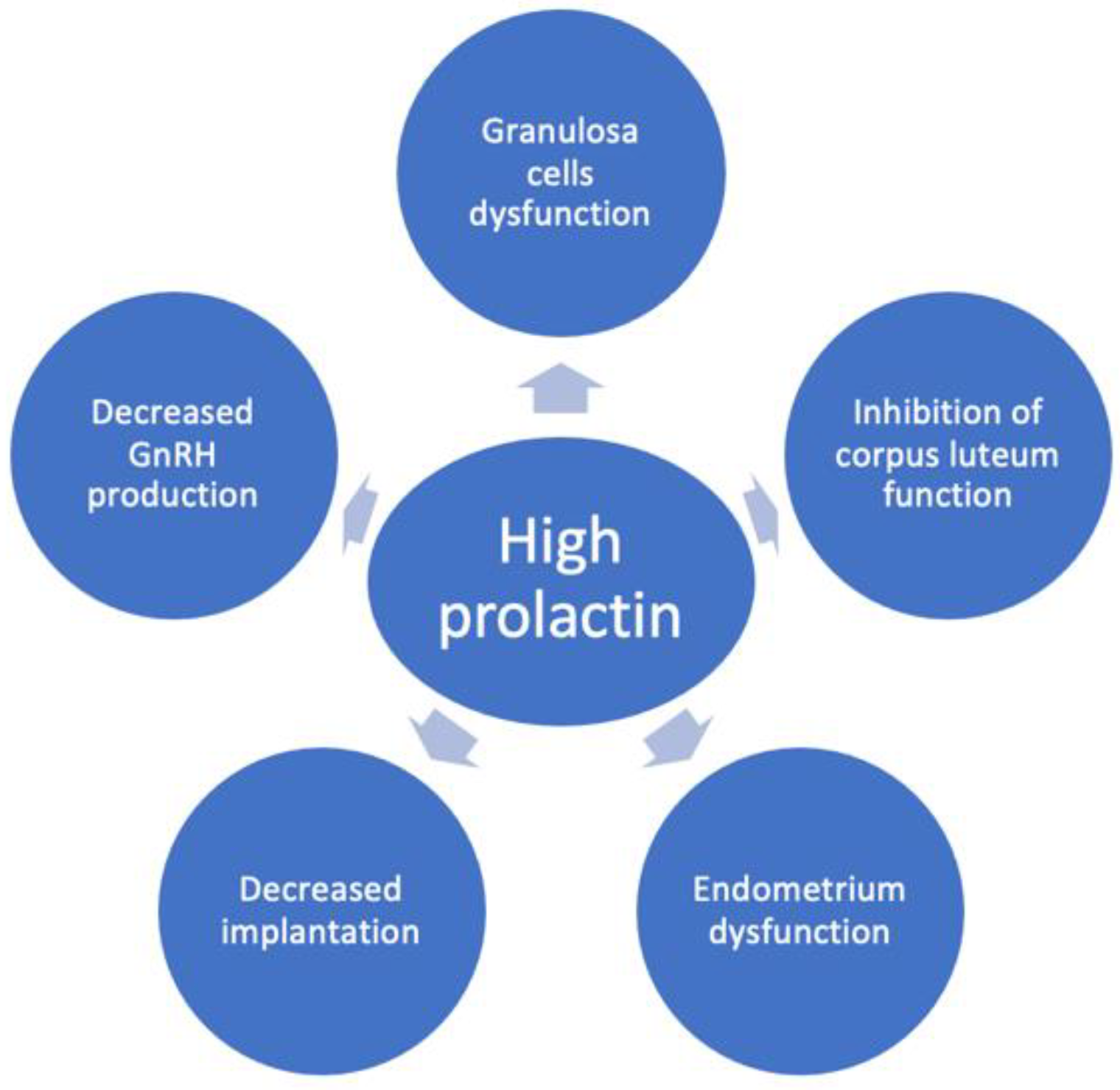
2. The Mechanisms behind Reduced Fertility in Hyperprolactinemic Patients
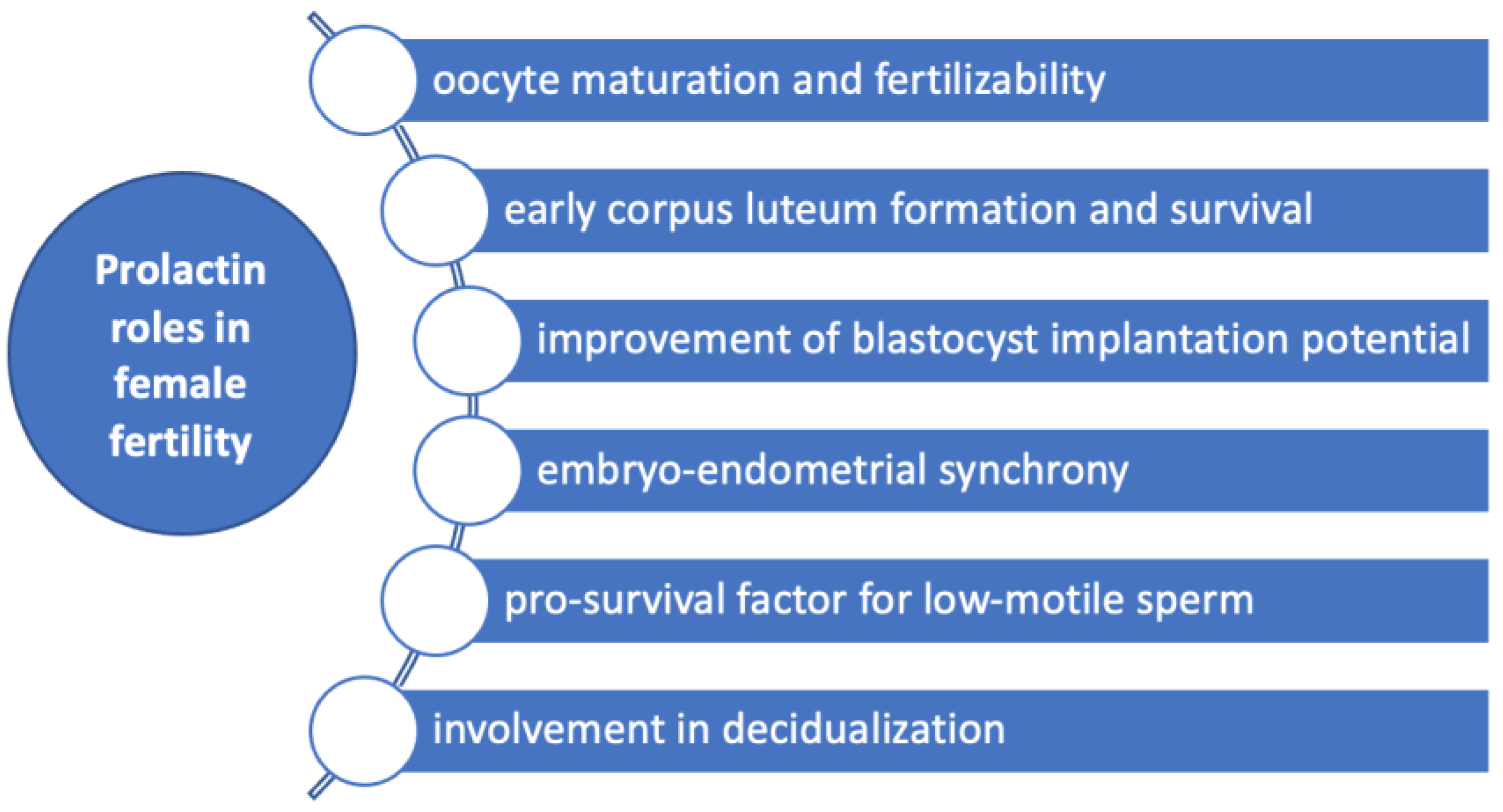
3. Prolactin Roles in Fertility
4. The Relationship between Prolactin Levels and ART Outcomes
Prolactin Relation with Hyper-Response to COS and Ovarian Hyperstimulation Syndrome
5. The Role of Dopamine Agonist Administration in IVF Treatment

{kind=link}
{kind=link}
{kind=link}
| Study | No of Patients | Type of the Study | Study Population | Type of HPRL | IVF Outcome | Prolactin Levels before Dopamine Agonist Treatment |
|---|---|---|---|---|---|---|
| Duan et al. (2019) [14] | 535 pts | Retrospective | 123 pts with treated HPRL and 369 matched controls | Preexistent to COS | CLBR similar in the two groups (69.1% versus s 66.4%, p = 0.58) | Median prolactin 80 ng/mL (study group) vs. 15.17 ng/mL (controls) |
| Doldi et al. (2000) [82] | 135 pts | Prospective | 59 pts with HPRL treated with BRC and 76 pts with HPRL without treatment | Preexistent to COS, mild HPRL in a cycle before COS | In the group with untreated HPRL a higher number of mature oocytes (87.9% versus 80.4%; p < 0.05), increased fertilization rate (70.8 +/− 28.0 versus 60.8 +/− 28.5; p < 0.03) and higher numbers of embryos transferred (3.6 +/− 1.6 versus 3.2 +/− 1.5; p < 0.05) | Mean 24.74 ± 3.17 ng/mL |
| Reinthaller et al. (1988) [72] | 50 cycles, 40 pts | Prospective | 18 pts with PRL ≤ 25 ng/mL (group 1), 15 pts with PRL > 25 ng/mL (group 2), 17 pts treated with BRC 3.75 mg/day (group 3) | Transient during COS | Higher fertilization rate (81.5%) in group 3 in comparison with group 2 (40.9%), but similar fertilization rates to group 1 (65.9%) | |
| Sopelak et al. (1989) [56] | 32 pts | Prospective | 19 controls and 13 pts treated with BRC 2.5 mg at 1 h (7 pts) and 12 h (6 pts) before anaesthesia | Transient, during anaesthesia for oocyte retrieval laparoscopy | 95% cleaving embryo in treated pts vs. 63% in controls, p < 0.001, similar fertilization and pregnancy rates | 22.4 ± 5.2 ng/mL in controls, 7 ± 1.7 ng/mL (1 h), 3.1 ± 0.3 ng/mL (12 h) |
| Taylor et al. (1986) [57] | 20 pts | Prospective | 10 pts treated with BRC, 10 pts without treatment | Transient, during anaesthesia for oocyte retrieval laparoscopy | No relationship between change in PRL and occurence of pregnancy | |
| Seppälä et al. (1989) [85] | 35 pts | Double-blind placebo-controlled study | 17 pts treated with BRC 1.25 mg/day from day 2 till HCG administration 18 pts treated with placebo | Normal PRL levels | Number of oocytes, embryo quality and pregnancies were similar between groups | |
| Parsanezhad et al. (2004) [86] | 100 pts | Prospective, double-blind, placebo-controlled study | CC-resistant normoprolactinemic PCOS women 47 pts treated with CC 200 mg × 5 days plus BRC 7.5 mg/day and 53 pts with placebo | Normal PRL levels | Similar ovulation rate in treated vs. placebo | |
| Jinno et al. (1997) [87] | 162 cycles | Prospective randomized study | Ovulatory women with previous IVF failure (82 cycles treated with BRC rebound method and 80 cycles with long protocol) | Normal PRL levels | Clinical pregnancy and live birth rates were higher (38% and 33%) in BRC rebound group versus long protocol (21% and 19%) | |
| Moride et al. (2018) [88] | 121 pts | Retrospective | Pts with repeated unsuccessful ART (22 women treated with BRC rebound method and 99 pts with long protocol) | Normal PRL levels | superior results were obtained with the BR method in terms of higher number of fertilized oocytes, cleaved embryos, transplanted embryos and clinical pregnancy rates (27.2% vs. 10.1%) in BRC rebound group | 5.9 ± 3.3 ng/mL (BRC rebound) vs. 7.5 ± 8.3 ng/mL (long agonist) |
6. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Bernard, V.; Young, J.; Chanson, P.; Binart, N. New insights in prolactin: Pathological implications. Nat. Rev. Endocrinol. 2015, 11, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Ben-Rafael, Z.; Meloni, F.; Mastroianni, L.; Flickinger, G.L. Relationship of human oocyte maturity, fertilization, and cleavage to follicular fluid prolactin and steroids. J. In Vitro Fertil. Embryo Transf. 1987, 4, 168–172. [Google Scholar] [CrossRef]
- Reinthaller, A.; Deutinger, J.; Riss, P.; Müller-Tyl, E.; Fischl, F.; Bieglmayer, C.; Janisch, H. Relationship between the steroid and prolactin concentration in follicular fluid and the maturation and fertilization of human oocytes. J. In Vitro Fertil. Embryo Transf. 1987, 4, 228–231. [Google Scholar] [CrossRef] [PubMed]
- Lindner, C.; Lichtenberg, V.; Westhof, G.; Braendle, W.; Bettendorf, G. Endocrine Parameters of Human Follicular Fluid and Fertilization Capacity of Oocytes. Horm. Metab. Res. 1988, 20, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Wyse, B.A.; Fuchs, W.N.; Defer, M.; Montbriand, J.; Szaraz, P.; Librach, C. The follicular fluid adipocytokine milieu could serve as a prediction tool for fertility treatment outcomes. Reprod. Biomed. Online 2021, 43, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Perks, C.M.; Newcomb, P.V.; Grohmann, M.; Wright, R.J.; Mason, H.D.; Holly, J.M. Prolactin acts as a potent survival factor against C2-ceramide-induced apoptosis in human granulosa cells. Hum. Reprod. 2003, 18, 2672–2677. [Google Scholar] [CrossRef]
- Takeuchi, M.; Seki, M.; Furukawa, E.; Takahashi, A.; Saito, K.; Kobayashi, M.; Ezoe, K.; Fukui, E.; Yoshizawa, M.; Matsumoto, H. Improvement of implantation potential in mouse blastocysts derived from IVF by combined treatment with prolactin, epidermal growth factor and 4-hydroxyestradiol. Mol. Hum. Reprod. 2017, 23, 557–570. [Google Scholar] [CrossRef]
- Zhong, Y.-P.; Shen, X.-T.; Ying, Y.; Wu, H.-T.; Li, J.; Qi, Q.; Zhou, C.-Q.; Zhuang, G.-L. Impact of Transitory Hyperprolactinemia on Clinical Outcome of In Vitro Fertilization and Embryo Transfer. J. Med Biochem. 2011, 31, 27–33. [Google Scholar] [CrossRef]
- McNeilly, A.S.; Glasier, A.; Jonassen, J.; Howie, P.W. Evidence for direct inhibition of ovarian function by prolactin. Reproduction 1982, 65, 559–569. [Google Scholar] [CrossRef]
- Borba, V.V.; Zandman-Goddard, G.; Shoenfeld, Y. Prolactin and autoimmunity. Front. Immunol 2018, 9, 73. [Google Scholar] [CrossRef]
- Healy, D.L.; Burger, H.G. Serum Follicle-Stimulating Hormone, Luteinizing Hormone, and Prolactin during the Induction of Ovulation with Exogenous Gonadotropin. J. Clin. Endocrinol. Metab. 1983, 56, 474–478. [Google Scholar] [CrossRef] [PubMed]
- Crosignani, P.G.; Maini, M.C.; Negri, E.; Ragni, G. Human prolactin release induced by follicle stimulating hormone, luteinizing hormone and human chorionic gonadotrophin. Hum. Reprod. 1991, 6, 1070–1073. [Google Scholar] [CrossRef] [PubMed]
- Kamel, A.; Halim, A.A.; Shehata, M.; Alfarra, S.; El-Faissal, Y.; Ramadan, W.; Hussein, A.M. Changes in serum prolactin level during intracytoplasmic sperm injection, and effect on clinical pregnancy rate: A prospective observational study. BMC Pregnancy Childbirth 2018, 18, 141. [Google Scholar] [CrossRef] [PubMed]
- Duan, Y.; Liu, X.; Hou, W.; Deng, M.; Gao, J.; Zhou, C.; Xu, Y. No impact of treated hyperprolactinemia on cumulative live birth rate and perinatal outcomes in in vitro fertilization-embryo transfer. J. Obstet. Gynaecol. Res. 2019, 45, 1236–1244. [Google Scholar] [CrossRef] [PubMed]
- Lecomte, P.; Lecomte, C.; Lansac, J.; Gallier, J.; Sonier, C.B.; Simonetta, C. Pregnancy after intravenous pulsatile gonadotropin-releasing hormone in a hyperprolactinemic woman resistant to treatment with dopamine agonist. Eur. J. Obstet. Gynecol. 1997, 74, 219–221. [Google Scholar] [CrossRef]
- Souter, I.; Baltagi, L.M.; Toth, T.L.; Petrozza, J.C. “âPrevalence of hyperprolactinemia and abnormal magnetic resonance imaging findings in a population with infertility. Fertil Steril 2010, 94, 1159–1162. [Google Scholar] [CrossRef]
- Laufer, M.R.; Floor, A.E.; Parsons, K.E.; Kuntz, K.M.; Barbieri, R.L.; Friedman, A.J. Evaluation of hormonal testing in the screening for in vitro fertilization (IVF) of women with tubal factor infertility. J. Assist. Reprod. Genet. 1995, 12, 93–96. [Google Scholar] [CrossRef]
- Hsueh, A.J.W.; Adashi, E.Y.; Jones, P.B.C.; Welsh, J.T.H. Hormonal Regulation of the Differentiation of Cultured Ovarian Granulosa Cells*. Endocr. Rev. 1984, 5, 76–127. [Google Scholar] [CrossRef]
- Tsai-Morris, C.-H.; Ghosh, M.; Hirshfield, A.N.; Wise, P.M.; Brodie, A.M.H. Inhibition of Ovarian Aromatase by Prolactin In Vivo. Biol. Reprod. 1983, 29, 342–346. [Google Scholar] [CrossRef]
- Fortune, J.E.; Wissler, R.N.; Vincent, S.E. Prolactin Modulates Steroidogenesis by Rat Granulosa Cells: II. Effects on Estradiol. Biol. Reprod. 1986, 35, 92–99. [Google Scholar] [CrossRef]
- Jonassen, J.A.; Baker, S.P.; McNeilly, A.S. Long-term hyperprolactinaemia reduces basal but not androgen-stimulated oestradiol production in small antral follicles of the rat ovary. J. Endocrinol. 1991, 129, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Veldhuis, J.D.; Klase, P.; Hammond, J.M. Divergent Effects of Prolactin upon Steroidogenesis by Porcine Granulosa Cells in Vitro: Influence of Cytodifferentiation. Endocrinology 1980, 107, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.B.C.; Valk, C.A.; Hsueh, A.J.W. Regulation of Progestin Biosynthetic Enzymes in Cultured Rat Granulosa Cells: Effects of Prolactin, β 2-Adrenergic Agonist, Human Chorionic Gonadotropin and Gonadotropin Releasing Hormone 1. Biol. Reprod. 1983, 29, 572–585. [Google Scholar] [CrossRef] [PubMed]
- Russell, D.L.; Richards, J.S. Differentiation-dependent prolactin responsiveness and stat (signal transducers and activators of transcription) signaling in rat ovarian cells. Mol. Endocrinol. 1999, 13, 2049–2064. [Google Scholar] [CrossRef] [PubMed]
- Dorrington, J.H.; Gore-Langton, R.E. Antigonadal Action of Prolactin: Further Studies on the Mechanism of Inhibition of Follicle-Stimulating Hormone-Induced Aromatase Activity in Rat Granulosa Cell Cultures. Endocrinology 1982, 110, 1701–1707. [Google Scholar] [CrossRef]
- Uilenbroek, J.; van der Schoot, P.; Besten, D.D.; Lankhorst, R.R. A Possible Direct Effect of Prolactin on Follicular Activity. Biol. Reprod. 1982, 27, 1119–1125. [Google Scholar] [CrossRef]
- Nakamura, E.; Otsuka, F.; Inagaki, K.; Miyoshi, T.; Yamanaka, R.; Tsukamoto, N.; Suzuki, J.; Ogura, T.; Makino, H. A Novel Antagonistic Effect of the Bone Morphogenetic Protein System on Prolactin Actions in Regulating Steroidogenesis by Granulosa Cells. Endocrinology 2010, 151, 5506–5518. [Google Scholar] [CrossRef]
- Vlahos, N.P.; Bugg, E.M.; Shamblott, M.J.; Phelps, J.Y.; Gearhart, J.D.; Zacur, H.A. Prolactin receptor gene expression and immunolocalization of the prolactin receptor in human luteinized granulosa cells. Mol. Hum. Reprod. 2001, 7, 1033–1038. [Google Scholar] [CrossRef]
- Seppälä, M.; Ranta, T.; Hirvonen, E. Hyperprolactinaemia and luteal insufficiency. Lancet 1976, 307, 229–230. [Google Scholar] [CrossRef]
- Nawroth, F. Hyperprolactinaemia and the regular menstrual cycle in asymptomatic women: Should it be treated during therapy for infertility? Reprod. Biomed Online 2005, 11, 581–588. [Google Scholar] [CrossRef]
- Shimatsu, A.; Hattori, N. Macroprolactinemia: Diagnostic, Clinical, and Pathogenic Significance. Clin. Dev. Immunol. 2012, 2012, 167132. [Google Scholar] [CrossRef] [PubMed]
- Panzan, M.Q.; Junior, J.M.S.; Da Motta, E.L.A. Metoclopramide-induced hyperprolactinemia caused marked decline in pinopodes and pregnancy rates in mice. Hum. Reprod. 2006, 21, 2514–2520. [Google Scholar] [CrossRef] [PubMed]
- Gomes, R.C.; Maioral, G.C.; Verna, C. Hyperprolactinemia changes the sulfated gycosaminoglycan amount on the murine uterus during estrous cycle. Fertil Steril 2013, 100, 1419–1427. [Google Scholar] [CrossRef]
- Shelly, S.; Boaz, M.; Orbach, H. Prolactin and autoimmunity. Autoimmun. Rev. 2012, 1, A465–A470. [Google Scholar] [CrossRef] [PubMed]
- Ohwaki, M.; Suganuma, N.; Seo, H.; Nawa, A.; Kikkawa, F.; Narita, O.; Matsui, N.; Tomoda, Y. Source of Prolactin in Human Follicular Fluid. Endocrinol. JPN 1992, 39, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Romão, G.S.; Ferriani, R.A.; Moura, M.D.; Martins, A.R. Screening for prolactin isoforms in the follicular fluid of patients undergoing in vitro fertilization. Gynecol. Obstet. Investig. 2002, 54, 46–49. [Google Scholar] [CrossRef]
- Subramanian, M.G.; Sacco, A.G.; Moghissi, K.S.; Magyar, D.M.; Hayes, M.F.; Lawson, D.M.; Gala, R.R. Human follicular fluid: Prolactin is biologically active and ovum fertilization correlates with estradiol concentration. J. In Vitro Fertil. Embryo Transf. 1988, 5, 129–133. [Google Scholar] [CrossRef]
- Laufer, N.; Botero-Ruiz, W.; DeCherney, A.H.; Haseltine, F.; Polan, M.L.; Behrman, H.R. Gonadotropin and Prolactin Levels in Follicular Fluid of Human Ova Successfully Fertilized in Vitro. J. Clin. Endocrinol. Metab. 1984, 58, 430–434. [Google Scholar] [CrossRef]
- Mendoza, C.; Cremades, N.; Ruiz-Requena, E.; Martinez, F.; Ortega, E.; Bernabeu, S.; Tesarik, J. Relationship between fertilization results after intracytoplasmic sperm injection, and intrafollicular steroid, pituitary hormone and cytokine concentrations. Hum. Reprod. 1999, 14, 628–635. [Google Scholar] [CrossRef]
- Lebedeva, I.Y.; Singina, G.N.; Lopukhov, A.V.; Shedova, E.N.; Zinovieva, N.A. Prolactin and growth hormone affect metaphase-II chromosomes in aging oocytes via cumulus cells using similar signaling pathways. Front. Genet. 2015, 6, 274. [Google Scholar] [CrossRef]
- Lebedeva, I.Y.; Singina, G.N.; Volkova, N.A.; Vejlsted, M.; Zinovieva, N.A.; Schmidt, M. Prolactin affects bovine oocytes through direct and cumulus-mediated pathways. Theriogenology 2014, 82, 1154–1164. [Google Scholar] [CrossRef] [PubMed]
- Starowicz, A.; Galas, J.; Duda, M.; Tabarowski, Z.; Szołtys, M. Effects of testosterone and prolactin on steroidogenesis in post-ovulatory cumuli oophori and on in vitro oocyte fertilisation in the rat. Reprod. Fertil. Dev. 2017, 29, 406. [Google Scholar] [CrossRef]
- Evans, J.; Hannan, N.J.; Hincks, C.; Rombauts, L.J.F.; Salamonsen, L.A. Defective Soil for a Fertile Seed? Altered Endometrial Development Is Detrimental to Pregnancy Success. PLoS ONE 2012, 7, e53098. [Google Scholar] [CrossRef] [PubMed]
- Kauma, S.; Shapiro, S.S. Immunoperoxidase localization of prolactin in endometrium during normal menstrual, luteal phase defect, and corrected luteal phase defect cycles. Fertil. Steril. 1986, 46, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Garzia, E.; Borgato, S.; Cozzi, V. Lack of expression of endometrial prolactin in early implantation failure: A pilot study. Hum. Reprod. 2004, 19, 1911–1916. [Google Scholar] [CrossRef]
- Altmäe, S.; Koel, M.; Võsa, U.; Adler, P.; Suhorutšenko, M.; Laisk-Podar, T.; Kukushkina, V.; Saare, M.; Velthut-Meikas, A.; Krjutškov, K.; et al. Meta-signature of human endometrial receptivity: A meta-analysis and validation study of transcriptomic biomarkers. Sci. Rep. 2017, 7, 10077. [Google Scholar] [CrossRef]
- Critchley, H.O.; Robertson, K.A.; Forster, T.; Henderson, T.A.; Williams, A.R.; Ghazal, P. Gene expression profiling of mid to late secretory phase endometrial biopsies from women with menstrual complaint. Am. J. Obstet. Gynecol. 2006, 195, 406–416. [Google Scholar] [CrossRef]
- Wu, W.-X.; Brooks, J.; Glasier, A.F.; McNeilly, A.S. The relationship between decidualization and prolactin mRNA and production at different stages of human pregnancy. J. Mol. Endocrinol. 1995, 14, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Gellersen, B.; Brosens, J. Cyclic Decidualization of the Human Endometrium in Reproductive Health and Failure. Endocr. Rev. 2014, 35, 851–905. [Google Scholar] [CrossRef]
- Berkhout, R.P.; Lambalk, C.B.; Repping, S.; Hamer, G.; Mastenbroek, S. Premature expression of the decidualization marker prolactin is associated with repeated implantation failure. Gynecol. Endocrinol. 2020, 36, 360–364. [Google Scholar] [CrossRef]
- Fu, Y.-X.; Yang, H.-M.; OuYang, X.-E.; Hu, R.; Hu, T.; Wang, F.-M. Assessment of Anti-Mullerian Hormone and Anti-Mullerian Hormone Type II Receptor Variants in Women with Repeated Implantation Failures. Reprod. Sci. 2021, 28, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Keyser, S.; van der Horst, G.; Maree, L. Progesterone, Myo-Inositol, Dopamine and Prolactin Present in Follicular Fluid Have Differential Effects on Sperm Motility Subpopulations. Life 2021, 11, 1250. [Google Scholar] [CrossRef] [PubMed]
- Huyser, C.; Fourie, F.R.; Moolman, H. The influence of sera, follicular fluids and seminal plasma on human sperm-zona pellucida binding. Hum. Reprod. 1997, 12, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Molina, R.; Castilla, J.A.; Vergara, F.; Pérez, M.; Garrido, F.; Herruzo, A.J. Luteal cytoplasmic estradiol and progesterone receptors in human endometrium: In vitro fertilization and normal cycles. Fertil. Steril. 1989, 51, 976–979. [Google Scholar] [CrossRef]
- Pattinson, H.A.; Taylor, P.J.; Fleetham, J.A.; Servis, S.A. Transient hyperprolactinemia has no effect on endocrine response and outcome in in vitro fertilization (IVF). J. In Vitro Fertil. Embryo Transf. 1990, 7, 89–93. [Google Scholar] [CrossRef]
- Sopelak, V.M.; Whitworth, N.S.; Norman, P.F.; Cowan, B.D. Bromocriptine inhibition of anesthesia-induced hyperprolactinemia: Effect on serum and follicular fluid hormones, oocyte fertilization, and embryo cleavage rates during in vitro fertilization. Fertil. Steril. 1989, 52, 627–632. [Google Scholar] [CrossRef]
- Taylor, P.J.; Trounson, A.; Besanko, M.; Burger, H.G.; Stockdale, J. Plasma progesterone and prolactin changes in superovulated women before, during, and immediately after laparoscopy for in vitro fertilization and their relation to pregnancy. Fertil. Steril. 1986, 45, 680–686. [Google Scholar] [CrossRef]
- Boyers, S.P.; Lavy, G.; Russell, J.B.; Polan, M.L.; DeCherney, A.H. Serum prolactin response to embryo transfer during human in vitro fertilization and embryo transfer. J. In Vitro Fertil. Embryo Transf. 1987, 4, 269–272. [Google Scholar] [CrossRef]
- Harlow, C.; Fahy, U.; Talbot, W.; Wardle, P.; Hull, M. Stress and stress-related hormones during in-vitro fertilization treatment. Hum. Reprod. 1996, 11, 274–279. [Google Scholar] [CrossRef]
- Csemiczky, G.; Landgren, B.M.; Collins, A. The influence of stress and state anxiety on the outcome of IVF-treatment: Psychological and endocrinological assessment of Swedish women entering IVF-treatment. Acta Obstet. Gynecol. Scand. 2000, 79, 113–118. [Google Scholar] [CrossRef]
- Milad, M.; Klock, S.C.; Moses, S.; Chatterton, R. Stress and anxiety do not result in pregnancy wastage. Hum. Reprod. 1998, 13, 2296–2300. [Google Scholar] [CrossRef]
- Trikoilis, Ν.; Mavromatidis, G.; Tzafetas, M.; Deligeoroglou, Ε.; Tzafetta, M.; Loufopoulos, A.; Dafoulis, V.; Tziomalos, K.; Goulis, D.G. The association of in vitro fertilization/intracytoplasmic sperm injection results with anxiety levels and stress biomarkers: An observational, case-control study. J. Gynecol. Obstet. Hum. Reprod. 2022, 51, 102254. [Google Scholar] [CrossRef]
- Shin, M.T.; Chu, T.Y.; Hsu, C.H.; Yu, M.H.; Chang, J.S.; Sun, D.; Lao, Z.H.; Wu, K.T.; Lee, C.K.; Yang, C.L. FSH, LH, PRL and E2 levels in follicular fluid and serum of patients undergoing follicle stimulation with different protocols for IVF. Asia Ocean. J. Obs. Gynaecol. 1988, 14, 227–232. [Google Scholar] [CrossRef]
- Meldrum, D.R.; Cedars, M.I.; Hamilton, F.; Huynh, D.; Wisot, A.; Marr, B. Leuprolide acetate elevates prolactin during ovarian stimulation with gonadotropins. J. Assist. Reprod. Genet. 1992, 9, 251–253. [Google Scholar] [CrossRef]
- Kamel, M.A.; Zabel, G.; Bernart, W.; Neulen, J.; Breckwoldt, M. Comparison between prolactin, gonadotrophins and steroid hormones in serum and follicular fluid after stimulation with gonadotrophin-releasing hormone agonists and human menopausal gonadotrophin for an in-vitro fertilization programme. Hum. Reprod. 1994, 9, 1803–1806. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, G.E.; Denis, A.L.; Scott, R.T.; Muasher, S.J. The incidence of transient hyperprolactinemia in gonadotropin-stimulated cycles for in vitro fertilization and its effect on pregnancy outcome. Fertil Steril 1989, 4, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Forman, R.; Fishel, S.; Edwards, S.; Walters, E. The Influence of Transient Hyperprolactinemia on in Vitro Fertilization in Humans. J. Clin. Endocrinol. Metab. 1985, 60, 517–522. [Google Scholar] [CrossRef]
- Hummel, W.P.; Clark, M.R.; Talbert, L.M. Transient hyperprolactinemia during cycle stimulation and its influence on oocyte retrieval and fertilization rates. Fertil. Steril. 1990, 53, 677–681. [Google Scholar] [CrossRef] [PubMed]
- Balasch, J.; Creus, M.; Fábregues, F.; Carmona, F.; Casamitjana, R.; Peñarrubia, J.; Rivera, F.; Vanrell, J.A. Hormonal profiles in successful and unsuccessful implantation in IVF–ET after combined GnRH agonist/gonadotropin treatment for superovulation and hCG luteal support. Gynecol. Endocrinol. 1995, 9, 51–58. [Google Scholar] [CrossRef]
- Oda, T.; Yoshimura, Y.; Takehara, Y.; Kohriyama, S.; Sano, Y.; Tanabe, K.; Kobayashi, T.; Nakamura, Y.; Ohno, T.; Nozawa, S. Effects of prolactin on fertilization and cleavage of human oocytes. Horm. Res. 1991, 35, 33–38. [Google Scholar] [CrossRef]
- Gonen, Y.; Casper, R.F. The influence of transient hyperprolactinemia on hormonal parameters, oocyte recovery, and fertilization rates in in vitro fertilization. J. In Vitro Fertil. Embryo Transf. 1989, 6, 155–159. [Google Scholar] [CrossRef]
- Reinthaller, A.; Bieglmayer, C.; Deutinger, J.; Csaicsich, P. Transient hyperprolactinemia during cycle stimulation: Influence on the endocrine response and fertilization rate of human oocytes and effects of bromocriptine treatment. Fertil Steril 1988, 3, 432–436. [Google Scholar] [CrossRef] [PubMed]
- Tarín, J.J.; Pascual, E.; García-Pérez, M.A.; Gómez, R.; Hidalgo-Mora, J.J.; Cano, A. A predictive model for women’s assisted fecundity before starting the first IVF/ICSI treatment cycle. J. Assist. Reprod. Genet. 2020, 37, 171–180. [Google Scholar] [CrossRef]
- Zhang, D.; Yuan, X.; Zhen, J.; Sun, Z.; Deng, C.; Yu, Q. Mildly Higher Serum Prolactin Levels Are Directly Proportional to Cumulative Pregnancy Outcomes in in-vitro Fertilization/Intracytoplasmic Sperm Injection Cycles. Front. Endocrinol. 2020, 11, 584. [Google Scholar] [CrossRef] [PubMed]
- Mendes, M.C.; Ferriani, R.A.; Sala, M.M.; Moura, M.D.; Carrara, H.H.; de Sá, M.F. Effect of transitory hyperprolactinemia on in vitro fertilization of human oocytes (abstract). J. Reprod. Med. 2001, 45, 444–450. [Google Scholar]
- Ozaki, T.; Takahashi, K.; Kurioka, H.; Miyazaki, K. Clinical Assisted Reproduction: Influence of Midluteal Serum Prolactin on Outcome of Pregnancy After IVF-ET: A Preliminary Study. J. Assist. Reprod. Genet. 2001, 18, 387–390. [Google Scholar] [CrossRef] [PubMed]
- Pérez, P.A.S.; Ceschin, Á.P.; Moraes, D.M.P.; Oliveira, L.K.S.N.; Ceschin, N.I.; Ichikawa, N. Early serum progesterone and prolactin analysis at day 9 of oocyte retrieval as a predictor of success in fresh ICSI cycles. JBRA Assist. Reprod. 2018, 2, 95–98. [Google Scholar] [CrossRef]
- Gonen, Y.; Casper, R.F. Does transient hyperprolactinemia during ovarian hyperstimulation interfere with conception or pregnancy outcome? Fertil. Steril. 1989, 6, 1007–1010. [Google Scholar] [CrossRef]
- Cottrell, H.N.; Deepak, V.; Spencer, J.B.; Sidell, N.; Rajakumar, A. Effects of Supraphysiologic Levels of Estradiol on Endometrial Decidualization, sFlt1, and HOXA10 Expression. Reprod. Sci. 2019, 12, 1626–1632. [Google Scholar] [CrossRef]
- Pakhomov, S.P.; Orlova, V.S.; Verzilina, I.N.; Sukhih, N.V.; Nagorniy, A.V.; Matrosova, A.V. Risk Factors and Methods for Predicting Ovarian Hyperstimulation Syndrome (OHSS) in the in vitro Fertilization. Arch. Razi Inst. 2020, 5, 1461–1468. [Google Scholar]
- Berinder, K.; Hulting, A.-L.; Granath, F.; Hirschberg, A.L.; Akre, O. Parity, pregnancy and neonatal outcomes in women treated for hyperprolactinaemia compared with a control group. Clin. Endocrinol. 2007, 67, 393–397. [Google Scholar] [CrossRef]
- Doldi, N.; Papaleo, E.; De Santis, L.; Ferrari, A. Treatment versus no treatment of transient hyperprolactinemia in patients undergoing intracytoplasmic sperm injection programs. Gynecol. Endocrinol. 2000, 6, 437–441. [Google Scholar] [CrossRef]
- Del Pozo, E. Management of Borderline Hyperprolactinemia. Horm. Res. 1985, 22, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Ben-David, M.; Schenker, J. Transient hyperprolactinemia: A correctable cause of idiopathic female infertility. J. Clin. Endocrinol. Metab. 1983, 57, 442–444. [Google Scholar] [CrossRef] [PubMed]
- Seppälä, M.; Martikainen, H.; Rönnberg, L.; Riittinen, L.; Kauppila, A. Suppression of prolactin secretion during ovarian hyperstimulation is followed by elevated serum levels of endometrial protein PP14 in the late luteal phase. Hum. Reprod. 1989, 4, 389–391. [Google Scholar] [CrossRef] [PubMed]
- Parsanezhad, M.E.; Alborzi, S.; Jahromi, B.N. A prospective, double-blind, randomized, placebo-controlled clinical trial of bromocriptin in clomiphene-resistant patients with polycystic ovary syndrome and normal prolactin level. Arch. Gynecol. Obstet. 2004, 269, 125–129. [Google Scholar] [CrossRef]
- Jinno, M.; Katsumata, Y.; Hoshiai, T.; Nakamura, Y.; Matsumoto, K.; Yoshimura, Y. A therapeutic role of prolactin supplementation in ovarian stimulation for in vitro fertilization: The bromocriptine-rebound method. J. Clin. Endocrinol. Metab. 1997, 11, 3603–3611. [Google Scholar] [CrossRef]
- Moride, N.; Kuwahara, A.; Yamashita, M.; Tanaka, Y.; Matsuzaki, T.; Yasui, T.; Irahara, M. Does the bromocriptine-rebound method improve embryo quality? J. Med. Investig. 2018, 1–2, 63–66. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iancu, M.E.; Albu, A.I.; Albu, D.N. Prolactin Relationship with Fertility and In Vitro Fertilization Outcomes—A Review of the Literature. Pharmaceuticals 2023, 16, 122. https://doi.org/10.3390/ph16010122
Iancu ME, Albu AI, Albu DN. Prolactin Relationship with Fertility and In Vitro Fertilization Outcomes—A Review of the Literature. Pharmaceuticals. 2023; 16(1):122. https://doi.org/10.3390/ph16010122
Chicago/Turabian StyleIancu, Mirela E., Alice I. Albu, and Dragoș N. Albu. 2023. "Prolactin Relationship with Fertility and In Vitro Fertilization Outcomes—A Review of the Literature" Pharmaceuticals 16, no. 1: 122. https://doi.org/10.3390/ph16010122
APA StyleIancu, M. E., Albu, A. I., & Albu, D. N. (2023). Prolactin Relationship with Fertility and In Vitro Fertilization Outcomes—A Review of the Literature. Pharmaceuticals, 16(1), 122. https://doi.org/10.3390/ph16010122