
Current and Potential Pharmacologic Therapies for Traumatic Brain Injury


Abstract
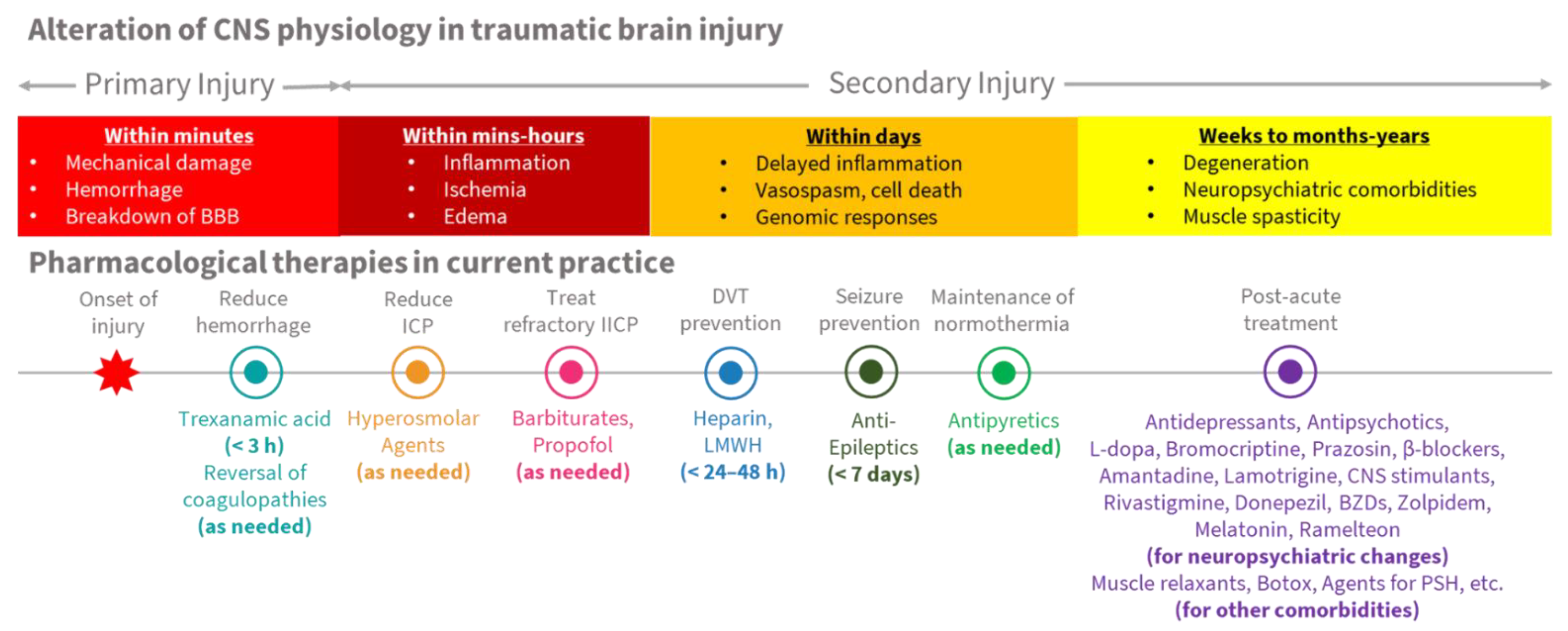
:1. Introduction
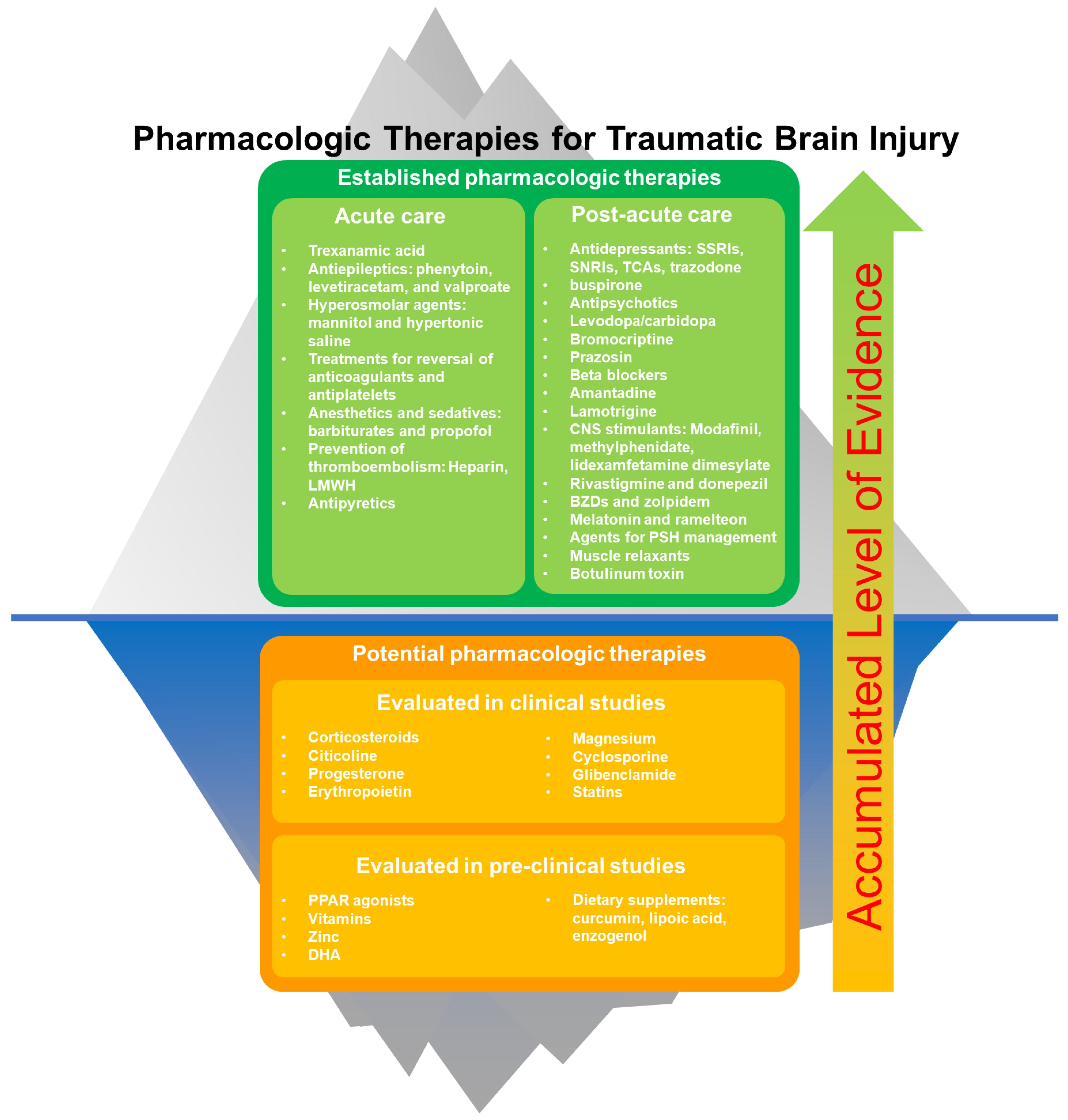
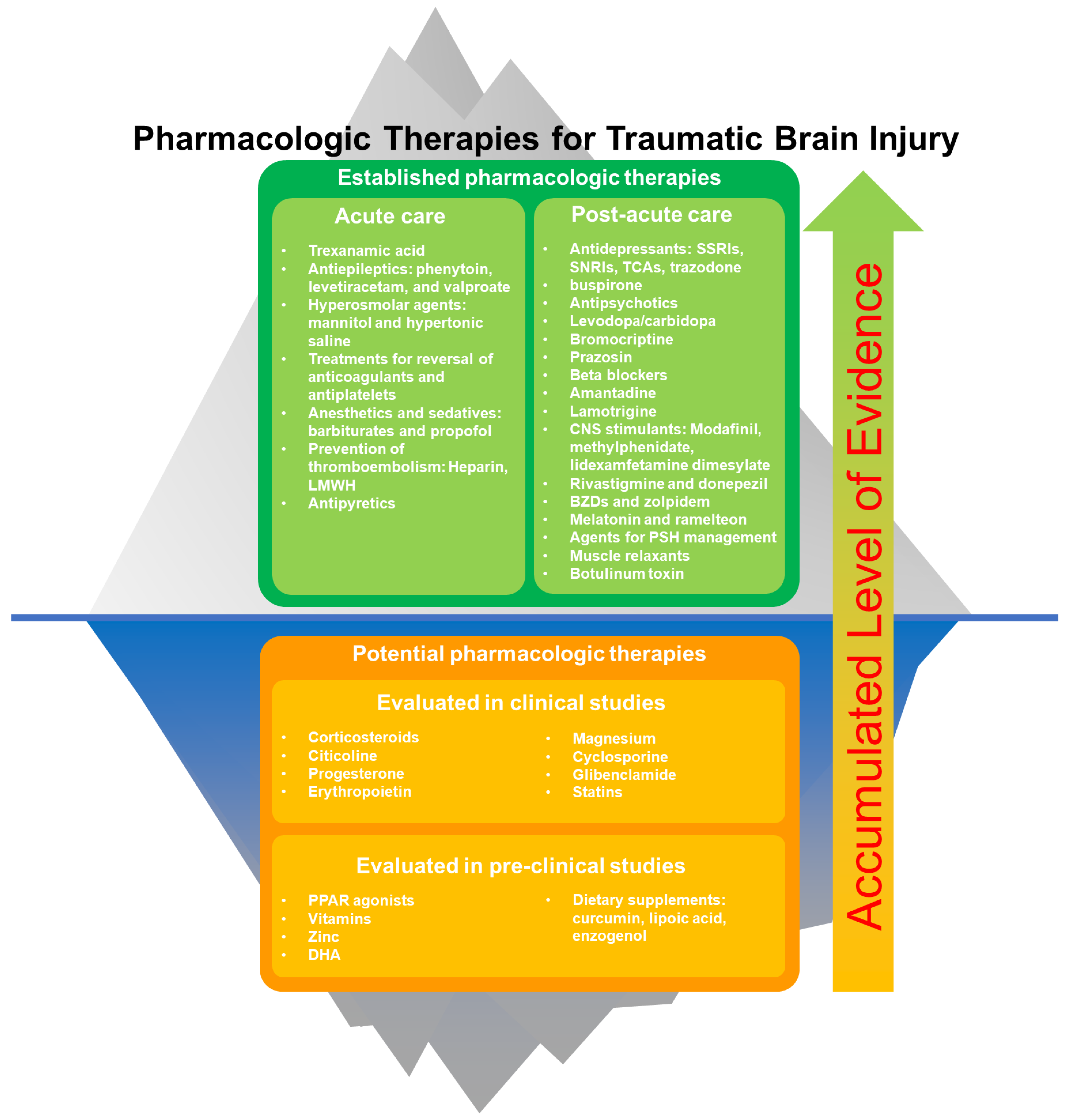
2. Established Pharmacologic Therapies for TBI
2.1. Acute Treatments for TBI
2.1.1. Tranexamic Acid
2.1.2. Treatments for Coagulopathies
2.1.3. Hyperosmolar Agents
2.1.4. Anesthetics and Sedatives
2.1.5. Drugs for Prevention of Thromboembolism
2.1.6. Antiepileptics
2.1.7. Antipyretics
2.2. Treatments for Post-TBI Neuropsychiatric Changes
2.2.1. SSRIs and SNRIs
2.2.2. Trazodone
2.2.3. TCAs
2.2.4. Buspirone
2.2.5. Antipsychotics
2.2.6. Levodopa/Carbidopa
2.2.7. Bromocriptine
2.2.8. Prazosin
2.2.9. Beta Blockers
2.2.10. Amantadine
2.2.11. Lamotrigine
2.2.12. Modafinil and Methylphenidate
2.2.13. Lisdexamfetamine Dimesylate
2.2.14. Rivastigmine and Donepezil
2.2.15. Benzodiazepines and Zolpidem
2.2.16. Melatonin and Ramelteon
2.3. Other Pharmaceutical Agents for Post-Acute TBI Care
2.3.1. Muscle Relaxants
2.3.2. Botulinum Toxin
2.3.3. Agents for Paroxysmal Sympathetic Hyperactivity Management
3. Potential Therapies for TBI
3.1. Neuroprotective Approaches Previously Evaluated in Clinical Studies
3.1.1. Corticosteroids
3.1.2. Citicoline
3.1.3. Progesterone
3.1.4. Erythropoietin
3.1.5. Magnesium
3.1.6. Cyclosporine
3.1.7. Glibenclamide
3.1.8. Statins
3.2. Neuroprotective Approaches and Natural Therapies Previously Evaluated in Pre-Clinical Studies
3.2.1. PPAR Agonists
3.2.2. Vitamins
3.2.3. Zinc
3.2.4. DHA
3.2.5. Dietary Supplements
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. 2018, 130, 1080–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carney, N.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Hawryluk, G.W.; Bell, M.J.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kissoon, N.; et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 2017, 80, 6–15. [Google Scholar] [CrossRef] [PubMed]
- dell’Aquila, M.; Maiese, A.; de Matteis, A.; Viola, R.V.; Arcangeli, M.; la Russa, R.; Fineschi, V. Traumatic brain injury: Estimate of the age of the injury based on neuroinflammation, endothelial activation markers and adhesion molecules. Histol. Histopathol. 2021, 36, 795–806. [Google Scholar] [PubMed]
- Rocchi, A.; Chiti, E.; Maiese, A.; Turillazzi, E.; Spinetti, I. MicroRNAs: An Update of Applications in Forensic Science. Diagnostics 2020, 11, 32. [Google Scholar] [CrossRef]
- Pinchi, E.; Frati, A.; Cantatore, S.; D’Errico, S.; Russa, R.; Maiese, A.; Palmieri, M.; Pesce, A.; Viola, R.V.; Frati, P.; et al. Acute Spinal Cord Injury: A Systematic Review Investigating miRNA Families Involved. Int. J. Mol. Sci. 2019, 20, 1841. [Google Scholar] [CrossRef] [Green Version]
- Biegon, A. Considering Biological Sex in Traumatic Brain Injury. Front. Neurol. 2021, 12, 576366. [Google Scholar] [CrossRef] [PubMed]
- Mikolić, A.; van Klaveren, D.; Groeniger, J.O.; Wiegers, E.J.A.; Lingsma, H.F.; Zeldovich, M.; von Steinbüchel, N.; Maas, A.I.R.; van Lennep, J.E.R.; Polinder, S. Differences between Men and Women in Treatment and Outcome after Traumatic Brain Injury. J. Neurotrauma 2021, 38, 235–251. [Google Scholar] [CrossRef] [PubMed]
- Crash, T. Effects of tranexamic acid on death, disability, vascular occlusive events and other morbidities in patients with acute traumatic brain injury (CRASH-3): A randomised, placebo-controlled trial. Lancet 2019, 394, 1713–1723. [Google Scholar]
- Santing, J.A.L.; van den Brand, C.L.; Jellema, K. Traumatic Brain Injury in Patients Receiving Direct Oral Anticoagulants. J. Emerg. Med. 2021, 60, 285–291. [Google Scholar] [CrossRef]
- Frontera, J.A.; Lewin, J.J., 3rd; Rabinstein, A.A.; Aisiku, I.P.; Alexandrov, A.W.; Cook, A.M.; del Zoppo, G.J.; Kumar, M.A.; Peerschke, E.I.; Stiefel, M.F.; et al. Guideline for Reversal of Antithrombotics in Intracranial Hemorrhage: A Statement for Healthcare Professionals from the Neurocritical Care Society and Society of Critical Care Medicine. Neurocritical Care 2016, 24, 6–46. [Google Scholar] [CrossRef]
- Shin, S.S.; Marsh, E.B.; Ali, H.; Nyquist, P.A.; Hanley, D.F.; Ziai, W.C. Comparison of Traumatic Intracranial Hemorrhage Expansion and Outcomes Among Patients on Direct Oral Anticoagulants Versus Vitamin k Antagonists. Neurocritical Care 2020, 32, 407–418. [Google Scholar] [CrossRef] [PubMed]
- Yasaka, M.; Sakata, T.; Minematsu, K.; Naritomi, H. Correction of INR by prothrombin complex concentrate and vitamin K in patients with warfarin related hemorrhagic complication. Thromb. Res. 2002, 108, 25–30. [Google Scholar] [CrossRef]
- Joseph, B.; Pandit, V.; Meyer, D.; Butvidas, L.; Kulvatunyou, N.; Khalil, M.; Tang, A.; Zangbar, B.; O’Keeffe, T.; Gries, L.; et al. The significance of platelet count in traumatic brain injury patients on antiplatelet therapy. J. Trauma Acute Care Surg. 2014, 77, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Alnemari, A.M.; Krafcik, B.M.; Mansour, T.R.; Gaudin, D. A Comparison of Pharmacologic Therapeutic Agents Used for the Reduction of Intracranial Pressure After Traumatic Brain Injury. World Neurosurg. 2017, 106, 509–528. [Google Scholar] [CrossRef] [PubMed]
- Burgess, S.; Abu-Laban, R.B.; Slavik, R.S.; Vu, E.N.; Zed, P.J. A Systematic Review of Randomized Controlled Trials Comparing Hypertonic Sodium Solutions and Mannitol for Traumatic Brain Injury: Implications for Emergency Department Management. Ann. Pharm. 2016, 50, 291–300. [Google Scholar] [CrossRef]
- Sakellaridis, N.; Pavlou, E.; Karatzas, S.; Chroni, D.; Vlachos, K.; Chatzopoulos, K.; Dimopoulou, E.; Kelesis, C.; Karaouli, V. Comparison of mannitol and hypertonic saline in the treatment of severe brain injuries. J. Neurosurg. 2011, 114, 545–548. [Google Scholar] [CrossRef]
- Cottenceau, V.; Masson, F.; Mahamid, E.; Petit, L.; Shik, V.; Sztark, F.; Zaaroor, M.; Soustiel, J.F. Comparison of effects of equiosmolar doses of mannitol and hypertonic saline on cerebral blood flow and metabolism in traumatic brain injury. J. Neurotrauma 2011, 28, 2003–2012. [Google Scholar] [CrossRef]
- Roberts, I.; Sydenham, E. Barbiturates for acute traumatic brain injury. Cochrane Database Syst. Rev. 2012, 12, Cd000033. [Google Scholar] [CrossRef]
- Margolick, J.; Dandurand, C.; Duncan, K.; Chen, W.; Evans, D.C.; Sekhon, M.S.; Garraway, N.; Griesdale, D.E.G.; Gooderham, P.; Hameed, S.M. A Systematic Review of the Risks and Benefits of Venous Thromboembolism Prophylaxis in Traumatic Brain Injury. Can. J. Neurol. Sci. 2018, 45, 432–444. [Google Scholar] [CrossRef]
- Chen, J.W.; Ruff, R.L.; Eavey, R.; Wasterlain, C.G. Posttraumatic epilepsy and treatment. J. Rehabil. Res. Dev. 2009, 46, 685–696. [Google Scholar] [CrossRef]
- Vaaramo, K.; Puljula, J.; Tetri, S.; Juvela, S.; Hillbom, M. Predictors of new-onset seizures: A 10-year follow-up of head trauma subjects with and without traumatic brain injury. J. Neurol. Neurosurg. Psychiatry 2014, 85, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Annegers, J.F.; Hauser, W.A.; Coan, S.P.; Rocca, W.A. A population-based study of seizures after traumatic brain injuries. N. Engl. J. Med. 1998, 338, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Arndt, D.H.; Lerner, J.T.; Matsumoto, J.H.; Madikians, A.; Yudovin, S.; Valino, H.; McArthur, D.L.; Wu, J.Y.; Leung, M.; Buxey, F.; et al. Subclinical early posttraumatic seizures detected by continuous EEG monitoring in a consecutive pediatric cohort. Epilepsia 2013, 54, 1780–1788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, K.; Pohlmann-Eden, B.; Campbell, L.A.; Abel, H. Pharmacological treatments for preventing epilepsy following traumatic head injury. Cochrane Database Syst. Rev. 2015, 8, Cd009900. [Google Scholar] [CrossRef]
- Temkin, N.R.; Dikmen, S.S.; Wilensky, A.J.; Keihm, J.; Chabal, S.; Winn, H.R. A randomized, double-blind study of phenytoin for the prevention of post-traumatic seizures. N. Engl. J. Med. 1990, 323, 497–502. [Google Scholar] [CrossRef]
- Schierhout, G.; Roberts, I. Anti-epileptic drugs for preventing seizures following acute traumatic brain injury. Cochrane Database Syst. Rev. 2001, 4, Cd000173. [Google Scholar]
- Hicks, A.J.; Clay, F.J.; Hopwood, M.; James, A.C.; Jayaram, M.; Perry, L.A.; Batty, R.; Ponsford, J.L. The Efficacy and Harms of Pharmacological Interventions for Aggression After Traumatic Brain Injury-Systematic Review. Front. Neurol. 2019, 10, 1169. [Google Scholar] [CrossRef]
- Zafar, S.N.; Khan, A.A.; Ghauri, A.A.; Shamim, M.S. Phenytoin versus Leviteracetam for seizure prophylaxis after brain injury—A meta analysis. BMC Neurol. 2012, 12, 30. [Google Scholar] [CrossRef] [Green Version]
- Chang, B.S.; Lowenstein, D.H. Practice parameter: Antiepileptic drug prophylaxis in severe traumatic brain injury: Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2003, 60, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Perron, A.D.; Brady, W.J.; Huff, J.S. Concussive convulsions: Emergency department assessment and management of a frequently misunderstood entity. Acad. Emerg. Med. 2001, 8, 296–298. [Google Scholar] [CrossRef] [Green Version]
- Wat, R.; Mammi, M.; Paredes, J.; Haines, J.; Alasmari, M.; Liew, A.; Lu, V.M.; Arnaout, O.; Smith, T.R.; Gormley, W.B.; et al. The Effectiveness of Antiepileptic Medications as Prophylaxis of Early Seizure in Patients with Traumatic Brain Injury Compared with Placebo or No Treatment: A Systematic Review and Meta-Analysis. World Neurosurg. 2019, 122, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Puccio, A.M.; Fischer, M.R.; Jankowitz, B.T.; Yonas, H.; Darby, J.M.; Okonkwo, D.O. Induced normothermia attenuates intracranial hypertension and reduces fever burden after severe traumatic brain injury. Neurocritical Care 2009, 11, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Oddo, M.; Nduom, E.; Frangos, S.; MacKenzie, L.; Chen, I.; Maloney-Wilensky, E.; Kofke, W.A.; Levine, J.M.; LeRoux, P.D. Acute lung injury is an independent risk factor for brain hypoxia after severe traumatic brain injury. Neurosurgery 2010, 67, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Selassie, A.W.; Zaloshnja, E.; Langlois, J.A.; Miller, T.; Jones, P.; Steiner, C. Incidence of long-term disability following traumatic brain injury hospitalization, United States, 2003. J. Head Trauma. Rehabil. 2008, 23, 123–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haarbauer-Krupa, J.; Pugh, M.J.; Prager, E.M.; Harmon, N.; Wolfe, J.; Yaffe, K. Epidemiology of Chronic Effects of Traumatic Brain Injury. J. Neurotrauma 2021, 38, 3235–3247. [Google Scholar] [CrossRef]
- Ashman, T.A.; Cantor, J.B.; Gordon, W.A.; Spielman, L.; Flanagan, S.; Ginsberg, A.; Engmann, C.; Egan, M.; Ambrose, F.; Greenwald, B. A Randomized Controlled Trial of Sertraline for the Treatment of Depression in Persons With Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2009, 90, 733–740. [Google Scholar] [CrossRef]
- Rapoport, M.J.; Chan, F.; Lanctot, K.; Herrmann, N.; McCullagh, S.; Feinstein, A. An open-label study of citalopram for major depression following traumatic brain injury. J. Psychopharmacol. 2008, 22, 860–864. [Google Scholar] [CrossRef]
- Novack, T.A.; Baños, J.H.; Brunner, R.; Renfroe, S.; Meythaler, J.M. Impact of early administration of sertraline on depressive symptoms in the first year after traumatic brain injury. J. Neurotrauma 2009, 26, 1921–1928. [Google Scholar] [CrossRef]
- Jorge, R.E.; Acion, L.; Burin, D.I.; Robinson, R.G. Sertraline for Preventing Mood Disorders Following Traumatic Brain Injury: A Randomized Clinical Trial. JAMA Psychiatry 2016, 73, 1041–1047. [Google Scholar] [CrossRef]
- Meythaler, J.M.; Depalma, L.; Devivo, M.J.; Guin-Renfroe, S.; Novack, T.A. Sertraline to improve arousal and alertness in severe traumatic brain injury secondary to motor vehicle crashes. Brain Inj. 2001, 15, 321–331. [Google Scholar] [CrossRef]
- Wortzel, H.S.; Oster, T.J.; Anderson, C.A.; Arciniegas, D.B. Pathological Laughing and Crying. CNS Drugs 2008, 22, 531–545. [Google Scholar] [CrossRef] [PubMed]
- Kaschka, W.P.; Meyer, A.; Schier, K.R.; Fröscher, W. Treatment of Pathological Crying with Citalopram. Pharmacopsychiatry 2001, 34, 254–258. [Google Scholar] [CrossRef] [PubMed]
- Nahas, Z.; Arlinghaus, K.A.; Kotrla, K.J.; Clearman, R.R.; George, M.S. Rapid response of emotional incontinence to selective serotonin reuptake inhibitors. J. Neuropsychiatry Clin. Neurosci. 1998, 10, 453–455. [Google Scholar] [CrossRef] [PubMed]
- Müller, U.; Murai, T.; Bauer-Wittmund, T.; von Cramon, D.Y. Paroxetine versus citalopram treatment of pathological crying after brain injury. Brain Inj. 1999, 13, 805–811. [Google Scholar] [CrossRef]
- Hoehn-Saric, R.; Lipsey, J.R.; McLeod, D.R. Apathy and indifference in patients on fluvoxamine and fluoxetine. J. Clin. Psychopharmacol. 1990, 10, 343–345. [Google Scholar] [CrossRef]
- Kanetani, K.; Kimura, M.; Endo, S. Therapeutic effects of milnacipran (serotonin noradrenalin reuptake inhibitor) on depression following mild and moderate traumatic brain injury. J. Nippon. Med. Sch. 2003, 70, 313–320. [Google Scholar] [CrossRef] [Green Version]
- Ripley, D.L.; Morey, C.E.; Gerber, D.; Harrison-Felix, C.; Brenner, L.A.; Pretz, C.R.; Cusick, C.; Wesnes, K. Atomoxetine for attention deficits following traumatic brain injury: Results from a randomized controlled trial. Brain Inj. 2014, 28, 1514–1522. [Google Scholar] [CrossRef]
- Curran, H.V.; Sakulsriprong, M.; Lader, M. Antidepressants and human memory: An investigation of four drugs with different sedative and anticholinergic profiles. Psychopharmacology 1988, 95, 520–527. [Google Scholar] [CrossRef]
- Larson, E.B.; Zollman, F.S. The effect of sleep medications on cognitive recovery from traumatic brain injury. J. Head Trauma. Rehabil. 2010, 25, 61–67. [Google Scholar] [CrossRef]
- Wroblewski, B.A.; Joseph, A.B.; Cornblatt, R.R. Antidepressant pharmacotherapy and the treatment of depression in patients with severe traumatic brain injury: A controlled, prospective study. J. Clin. Psychiatry 1996, 57, 582–587. [Google Scholar] [CrossRef]
- Dinan, T.G.; Mobayed, M. Treatment resistance of depression after head injury: A preliminary study of amitriptyline response. Acta Psychiatr. Scand. 1992, 85, 292–294. [Google Scholar] [CrossRef] [PubMed]
- Fann, J.R.; Hart, T.; Schomer, K.G. Treatment for depression after traumatic brain injury: A systematic review. J. Neurotrauma 2009, 26, 2383–2402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wroblewski, B.A.; McColgan, K.; Smith, K.; Whyte, J.; Singer, W.D. The incidence of seizures during tricyclic antidepressant drug treatment in a brain-injured population. J. Clin. Psychopharmacol. 1990, 10, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.; Berson, A.; Cook, T.; Bollegala, N.; Seto, E.; Tursanski, S.; Kim, J.; Sockalingam, S.; Rajput, A.; Krishnadev, N.; et al. Treatment of agitation following traumatic brain injury: A review of the literature. NeuroRehabilitation 2005, 20, 279–306. [Google Scholar] [CrossRef]
- Maryniak, O.; Manchanda, R.; Velani, A. Methotrimeprazine in the treatment of agitation in acquired brain injury patients. Brain Inj. 2001, 15, 167–174. [Google Scholar] [CrossRef]
- Stanislav, S.W.; Childs, A. Evaluating the usage of droperidol in acutely agitated persons with brain injury. Brain Inj. 2000, 14, 261–265. [Google Scholar]
- Krieger, D.; Hansen, K.; McDermott, C.; Matthews, R.; Mitchell, R.; Bollegala, N.; Bhalerao, S. Loxapine versus olanzapine in the treatment of delirium following traumatic brain injury. NeuroRehabilitation 2003, 18, 205–208. [Google Scholar] [CrossRef]
- Kim, E.; Bijlani, M. A pilot study of quetiapine treatment of aggression due to traumatic brain injury. J. Neuropsychiatry Clin. Neurosci. 2006, 18, 547–549. [Google Scholar] [CrossRef]
- Michals, M.L.; Crismon, M.L.; Roberts, S.; Childs, A. Clozapine response and adverse effects in nine brain-injured patients. J. Clin. Psychopharmacol. 1993, 13, 198–203. [Google Scholar] [CrossRef]
- Noé, E.; Ferri, J.; Trénor, C.; Chirivella, J. Efficacy of ziprasidone in controlling agitation during post-traumatic amnesia. Behav. Neurol. 2007, 18, 7–11. [Google Scholar] [CrossRef]
- Umene-Nakano, W.; Yoshimura, R.; Okamoto, T.; Hori, H.; Nakamura, J. Aripiprazole improves various cognitive and behavioral impairments after traumatic brain injury: A case report. Gen. Hosp. Psychiatry 2013, 35, e7–e9. [Google Scholar] [CrossRef] [PubMed]
- Butler, P.V. Diurnal variation in Cotard’s syndrome (copresent with Capgras delusion) following traumatic brain injury. Aust. N. Z. J. Psychiatry 2000, 34, 684–687. [Google Scholar] [CrossRef] [PubMed]
- Bde, M.V.; Prais, H.A.; Nicolato, R.; Caramelli, P. Posttraumatic brain injury psychosis successfully treated with olanzapine. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2010, 34, 233–235. [Google Scholar]
- Arciniegas, D.B.; Harris, S.N.; Brousseau, K.M. Psychosis following traumatic brain injury. Int. Rev. Psychiatry 2003, 15, 328–340. [Google Scholar] [CrossRef] [PubMed]
- Krimchansky, B.Z.; Keren, O.; Sazbon, L.; Groswasser, Z. Differential time and related appearance of signs, indicating improvement in the state of consciousness in vegetative state traumatic brain injury (VS-TBI) patients after initiation of dopamine treatment. Brain Inj. 2004, 18, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Passler, M.A.; Riggs, R.V. Positive outcomes in traumatic brain injury-vegetative state: Patients treated with bromocriptine. Arch. Phys. Med. Rehabil. 2001, 82, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Whyte, J.; Vaccaro, M.; Grieb-Neff, P.; Hart, T.; Polansky, M.; Coslett, H.B. The effects of bromocriptine on attention deficits after traumatic brain injury: A placebo-controlled pilot study. Am. J. Phys. Med. Rehabil. 2008, 87, 85–99. [Google Scholar] [CrossRef]
- Ruff, R.L.; Riechers, R.G., II.; Wang, X.F.; Piero, T.; Ruff, S.S. For veterans with mild traumatic brain injury, improved posttraumatic stress disorder severity and sleep correlated with symptomatic improvement. J. Rehabil. Res. Dev. 2012, 49, 1305–1320. [Google Scholar] [CrossRef]
- Fleminger, S.; Greenwood, R.J.; Oliver, D.L. Pharmacological management for agitation and aggression in people with acquired brain injury. Cochrane Database Syst. Rev. 2006, Cd003299. [Google Scholar] [CrossRef]
- Rappaport, M.; Hall, K.M.; Hopkins, K.; Belleza, T.; Cope, D.N. Disability rating scale for severe head trauma: Coma to community. Arch. Phys. Med. Rehabil. 1982, 63, 118–123. [Google Scholar]
- Zafonte, R.D.; Watanabe, T.; Mann, N.R. Amantadine: A potential treatment for the minimally conscious state. Brain Inj. 1998, 12, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Meythaler, J.M.; Brunner, R.C.; Johnson, A.; Novack, T.A. Amantadine to improve neurorecovery in traumatic brain injury-associated diffuse axonal injury: A pilot double-blind randomized trial. J. Head Trauma Rehabil. 2002, 17, 300–313. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, E.; Mauro, L.S.; Ohlinger, M.J. Amantadine enhancement of arousal and cognition after traumatic brain injury. Ann. Pharm. 2008, 42, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Pachet, A.; Friesen, S.; Winkelaar, D.; Gray, S. Beneficial behavioural effects of lamotrigine in traumatic brain injury. Brain Inj. 2003, 17, 715–722. [Google Scholar] [CrossRef]
- Kaiser, P.R.; Valko, P.O.; Werth, E.; Thomann, J.; Meier, J.; Stocker, R.; Bassetti, C.L.; Baumann, C.R. Modafinil ameliorates excessive daytime sleepiness after traumatic brain injury. Neurology 2010, 75, 1780–1785. [Google Scholar] [CrossRef] [Green Version]
- Jha, A.; Weintraub, A.; Allshouse, A.; Morey, C.; Cusick, C.; Kittelson, J.; Harrison-Felix, C.; Whiteneck, G.; Gerber, D. A randomized trial of modafinil for the treatment of fatigue and excessive daytime sleepiness in individuals with chronic traumatic brain injury. J. Head Trauma Rehabil. 2008, 23, 52–63. [Google Scholar] [CrossRef]
- Menn, S.J.; Yang, R.; Lankford, A. Armodafinil for the treatment of excessive sleepiness associated with mild or moderate closed traumatic brain injury: A 12-week, randomized, double-blind study followed by a 12-month open-label extension. J. Clin. Sleep Med. 2014, 10, 1181–1191. [Google Scholar] [CrossRef] [Green Version]
- Whyte, J.; Hart, T.; Vaccaro, M.; Grieb-Neff, P.; Risser, A.; Polansky, M.; Coslett, H.B. Effects of methylphenidate on attention deficits after traumatic brain injury: A multidimensional, randomized, controlled trial. Am. J. Phys. Med. Rehabil. 2004, 83, 401–420. [Google Scholar] [CrossRef]
- Willmott, C.; Ponsford, J. Efficacy of methylphenidate in the rehabilitation of attention following traumatic brain injury: A randomised, crossover, double blind, placebo controlled inpatient trial. J. Neurol. Neurosurg. Psychiatry 2009, 80, 552–557. [Google Scholar] [CrossRef] [Green Version]
- Sivan, M.; Neumann, V.; Kent, R.; Stroud, A.; Bhakta, B.B. Pharmacotherapy for treatment of attention deficits after non-progressive acquired brain injury. A systematic review. Clin. Rehabil. 2010, 24, 110–121. [Google Scholar] [CrossRef]
- McAllister, T.W.; Zafonte, R.; Jain, S.; Flashman, L.A.; George, M.S.; Grant, G.A.; He, F.; Lohr, J.B.; Andaluz, N.; Summerall, L.; et al. Stein, Randomized Placebo-Controlled Trial of Methylphenidate or Galantamine for Persistent Emotional and Cognitive Symptoms Associated with PTSD and/or Traumatic Brain Injury. Neuropsychopharmacology 2016, 41, 1191–1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tramontana, M.G.; Cowan, R.L.; Zald, D.; Prokop, J.W.; Guillamondegui, O. Traumatic brain injury-related attention deficits: Treatment outcomes with lisdexamfetamine dimesylate (Vyvanse). Brain Inj. 2014, 28, 1461–1472. [Google Scholar] [CrossRef] [PubMed]
- Ponsford, J.; Spitz, G.; Hicks, A.J. Highlights in traumatic brain injury research in 2021. Lancet Neurol. 2022, 21, 5–6. [Google Scholar] [CrossRef]
- Tenovuo, O.; Alin, J.; Helenius, H. A randomized controlled trial of rivastigmine for chronic sequels of traumatic brain injury-what it showed and taught? Brain Inj. 2009, 23, 548–558. [Google Scholar] [CrossRef] [PubMed]
- Silver, J.M.; Koumaras, B.; Meng, X.; Potkin, S.G.; Reyes, P.F.; Harvey, P.D.; Katz, D.I.; Gunay, I.; Arciniegas, D.B. Long-term effects of rivastigmine capsules in patients with traumatic brain injury. Brain Inj. 2009, 23, 123–132. [Google Scholar] [CrossRef]
- Barker, M.J.; Greenwood, K.M.; Jackson, M.; Crowe, S.F. Persistence of cognitive effects after withdrawal from long-term benzodiazepine use: A meta-analysis. Arch. Clin. Neuropsychol. 2004, 19, 437–454. [Google Scholar] [CrossRef] [Green Version]
- Barker, M.J.; Greenwood, K.M.; Jackson, M.; Crowe, S.F. Cognitive effects of long-term benzodiazepine use: A meta-analysis. CNS Drugs 2004, 18, 37–48. [Google Scholar] [CrossRef]
- Ouellet, M.C.; Beaulieu-Bonneau, S.; Morin, C.M. Sleep-wake disturbances after traumatic brain injury. Lancet Neurol. 2015, 14, 746–757. [Google Scholar] [CrossRef]
- Whyte, J.; Rajan, R.; Rosenbaum, A.; Katz, D.; Kalmar, K.; Seel, R.; Greenwald, B.; Zafonte, R.; Demarest, D.; Brunner, R.; et al. Zolpidem and restoration of consciousness. Am. J. Phys. Med. Rehabil. 2014, 93, 101–113. [Google Scholar] [CrossRef]
- Williams, S.T.; Conte, M.M.; Goldfine, A.M.; Noirhomme, Q.; Gosseries, O.; Thonnard, M.; Beattie, B.; Hersh, J.; Katz, D.I.; Victor, J.D.; et al. Common resting brain dynamics indicate a possible mechanism underlying zolpidem response in severe brain injury. Elife 2013, 2, e01157. [Google Scholar] [CrossRef]
- Du, B.; Shan, A.; Zhang, Y.; Zhong, X.; Chen, D.; Cai, K. Zolpidem arouses patients in vegetative state after brain injury: Quantitative evaluation and indications. Am. J. Med. Sci. 2014, 347, 178–182. [Google Scholar] [CrossRef]
- Kemp, S.; Biswas, R.; Neumann, V.; Coughlan, A. The value of melatonin for sleep disorders occurring post-head injury: A pilot RCT. Brain Inj. 2004, 18, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Lequerica, A.; Jasey, N.; Tremont, J.N.P.; Chiaravalloti, N.D. Pilot Study on the Effect of Ramelteon on Sleep Disturbance After Traumatic Brain Injury: Preliminary Evidence From a Clinical Trial. Arch. Phys. Med. Rehabil. 2015, 96, 1802–1809. [Google Scholar] [CrossRef] [PubMed]
- Meythaler, J.M.; Clayton, W.; Davis, L.K.; Guin-Renfroe, S.; Brunner, R.C. Orally delivered baclofen to control spastic hypertonia in acquired brain injury. J. Head Trauma Rehabil. 2004, 19, 101–108. [Google Scholar] [CrossRef]
- Posteraro, F.; Calandriello, B.; Galli, R.; Logi, F.; Iardella, L.; Bordi, L. Timing of intrathecal baclofen therapy in persons with acquired brain injury: Influence on outcome. Brain Inj. 2013, 27, 1671–1675. [Google Scholar] [CrossRef] [PubMed]
- Meythaler, J.M.; Guin-Renfroe, S.; Johnson, A.; Brunner, R.M. Prospective assessment of tizanidine for spasticity due to acquired brain injury. Arch. Phys Med. Rehabil. 2001, 82, 1155–1163. [Google Scholar] [CrossRef]
- Yablon, S.A.; Agana, B.T.; Ivanhoe, C.B.; Boake, C. Botulinum toxin in severe upper extremity spasticity among patients with traumatic brain injury: An open-labeled trial. Neurology 1996, 47, 939–944. [Google Scholar] [CrossRef]
- Yerry, J.A.; Kuehn, D.; Finkel, A.G. Onabotulinum toxin a for the treatment of headache in service members with a history of mild traumatic brain injury: A cohort study. Headache 2015, 55, 395–406. [Google Scholar] [CrossRef]
- Lump, D.; Moyer, M. Paroxysmal sympathetic hyperactivity after severe brain injury. Curr. Neurol. Neurosci. Rep. 2014, 14, 494. [Google Scholar] [CrossRef]
- Blackman, J.A.; Patrick, P.D.; Buck, M.L.; Rust, R.S., Jr. Paroxysmal autonomic instability with dystonia after brain injury. Arch. Neurol. 2004, 61, 321–328. [Google Scholar] [CrossRef] [Green Version]
- Baguley, I.J.; Heriseanu, R.E.; Gurka, J.A.; Nordenbo, A.; Cameron, I.D. Gabapentin in the management of dysautonomia following severe traumatic brain injury: A case series. J. Neurol. Neurosurg. Psychiatry 2007, 78, 539–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, I.; Yates, D.; Sandercock, P.; Farrell, B.; Wasserberg, J.; Lomas, G.; Cottingham, R.; Svoboda, P.; Brayley, N.; Mazairac, G.; et al. Effect of intravenous corticosteroids on death within 14 days in 10,008 adults with clinically significant head injury (MRC CRASH trial): Randomised placebo-controlled trial. Lancet 2004, 364, 1321–1328. [Google Scholar] [PubMed]
- Edwards, P.; Arango, M.; Balica, L.; Cottingham, R.; El-Sayed, H.; Farrell, B.; Fernandes, J.; Gogichaisvili, T.; Golden, N.; Hartzenberg, B.; et al. Final results of MRC CRASH, a randomised placebo-controlled trial of intravenous corticosteroid in adults with head injury-outcomes at 6 months. Lancet 2005, 365, 1957–1959. [Google Scholar] [PubMed]
- Zafonte, R.D.; Bagiella, E.; Ansel, B.M.; Novack, T.A.; Friedewald, W.T.; Hesdorffer, D.C.; Timmons, S.D.; Jallo, J.; Eisenberg, H.; Hart, T. Effect of citicoline on functional and cognitive status among patients with traumatic brain injury: Citicoline Brain Injury Treatment Trial (COBRIT). Jama 2012, 308, 1993–2000. [Google Scholar] [CrossRef] [PubMed]
- Wright, D.W.; Kellermann, A.L.; Hertzberg, V.S.; Clark, P.L.; Frankel, M.; Goldstein, F.C.; Salomone, J.P.; Dent, L.L.; Harris, O.A.; Ander, D.S.; et al. ProTECT: A randomized clinical trial of progesterone for acute traumatic brain injury. Ann. Emerg. Med. 2007, 49, 391–402. [Google Scholar] [CrossRef]
- Xiao, G.; Wei, J.; Yan, W.; Wang, W.; Lu, Z. Improved outcomes from the administration of progesterone for patients with acute severe traumatic brain injury: A randomized controlled trial. Crit. Care 2008, 12, R61. [Google Scholar] [CrossRef] [Green Version]
- Skolnick, B.E.; Maas, A.I.; Narayan, R.K.; van der Hoop, R.G.; MacAllister, T.; Ward, J.D.; Nelson, N.R.; Stocchetti, N. A clinical trial of progesterone for severe traumatic brain injury. N. Engl. J. Med. 2014, 371, 2467–2476. [Google Scholar] [CrossRef] [Green Version]
- Wright, D.W.; Yeatts, S.D.; Silbergleit, R.; Palesch, Y.Y.; Hertzberg, V.S.; Frankel, M.; Goldstein, F.C.; Caveney, A.F.; Howlett-Smith, H.; Bengelink, E.M.; et al. Very early administration of progesterone for acute traumatic brain injury. N. Engl. J. Med. 2014, 371, 2457–2466. [Google Scholar] [CrossRef] [Green Version]
- Soltani, Z.; Shahrokhi, N.; Karamouzian, S.; Khaksari, M.; Mofid, B.; Nakhaee, N.; Reihani, H. Does progesterone improve outcome in diffuse axonal injury? Brain Inj. 2017, 31, 16–23. [Google Scholar] [CrossRef]
- Sinha, S.; Raheja, A.; Samson, N.; Goyal, K.; Bhoi, S.; Selvi, A.; Sharma, P.; Sharma, B.S. A randomized placebo-controlled trial of progesterone with or without hypothermia in patients with acute severe traumatic brain injury. Neurol. India 2017, 65, 1304–1311. [Google Scholar] [CrossRef]
- Nichol, A.; French, C.; Little, L.; Haddad, S.; Presneill, J.; Arabi, Y.; Bailey, M.; Cooper, D.J.; Duranteau, J.; Huet, O.; et al. Erythropoietin in traumatic brain injury (EPO-TBI): A double-blind randomised controlled trial. Lancet 2015, 386, 2499–2506. [Google Scholar] [CrossRef]
- Lee, J.; Cho, Y.; Choi, K.S.; Kim, W.; Jang, B.H.; Shin, H.; Ahn, C.; Lim, T.H.; Yi, H.J. Efficacy and safety of erythropoietin in patients with traumatic brain injury: A systematic review and meta-analysis. Am. J. Emerg. Med. 2019, 37, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Wang, A.J.; Chen, Y.; Zhao, G.; Jiang, Z.; Wang, X.; Shi, D.; Zhang, T.; Sun, B.; He, H.; et al. Efficacy and safety of erythropoietin for traumatic brain injury. BMC Neurol. 2020, 20, 399. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.F.; Gao, Y.K. Recombinant human erythropoietin for treating severe traumatic brain injury. Medicine 2018, 97, e9532. [Google Scholar] [CrossRef] [PubMed]
- Lyons, M.W.H.; Blackshaw, W.J. Does magnesium sulfate have a role in the management of severe traumatic brain injury in civilian and military populations? A systematic review and meta-analysis. J. R. Army Med. Corp. 2018, 164, 442–449. [Google Scholar] [CrossRef]
- Temkin, N.R.; Anderson, G.D.; Winn, H.R.; Ellenbogen, R.G.; Britz, G.W.; Schuster, J.; Lucas, T.; Newell, D.W.; Mansfield, P.N.; Machamer, J.E.; et al. Magnesium sulfate for neuroprotection after traumatic brain injury: A randomised controlled trial. Lancet Neurol. 2007, 6, 29–38. [Google Scholar] [CrossRef]
- Hatton, J.; Rosbolt, B.; Empey, P.; Kryscio, R.; Young, B. Dosing and safety of cyclosporine in patients with severe brain injury. J. Neurosurg. 2008, 109, 699–707. [Google Scholar] [CrossRef] [Green Version]
- Aminmansour, B.; Fard, S.A.; Habibabadi, M.R.; Moein, P.; Norouzi, R.; Naderan, M. The efficacy of Cyclosporine-A on Diffuse Axonal Injury after Traumatic Brain Injury. Adv. Biomed. Res. 2014, 3, 35. [Google Scholar]
- Jha, R.M.; Bell, J.; Citerio, G.; Hemphill, J.C.; Kimberly, W.T.; Narayan, R.K.; Sahuquillo, J.; Sheth, K.N.; Simard, J.M. Role of Sulfonylurea Receptor 1 and Glibenclamide in Traumatic Brain Injury: A Review of the Evidence. Int. J. Mol. Sci. 2020, 21, 409. [Google Scholar] [CrossRef] [Green Version]
- Zafardoost, P.; Ghasemi, A.A.; Salehpour, F.; Piroti, C.; Ziaeii, E. Evaluation of the Effect of Glibenclamide in Patients With Diffuse Axonal Injury Due to Moderate to Severe Head Trauma. Trauma Mon. 2016, 21, e25113. [Google Scholar] [CrossRef] [Green Version]
- Khalili, H.; Derakhshan, N.; Niakan, A.; Ghaffarpasand, F.; Salehi, M.; Eshraghian, H.; Shakibafard, A.; Zahabi, B. Effects of Oral Glibenclamide on Brain Contusion Volume and Functional Outcome of Patients with Moderate and Severe Traumatic Brain Injuries: A Randomized Double-Blind Placebo-Controlled Clinical Trial. World Neurosurg. 2017, 101, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, H.M.; Shenton, M.E.; Pasternak, O.; Simard, J.M.; Okonkwo, D.O.; Aldrich, C.; He, F.; Jain, S.; Hayman, E.G. Magnetic Resonance Imaging Pilot Study of Intravenous Glyburide in Traumatic Brain Injury. J. Neurotrauma 2020, 37, 185–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sultan, W.; Sapkota, A.; Khurshid, H.; Qureshi, I.A.; Jahan, N.; Went, T.R.; Dominic, J.L.; Win, M.; Kannan, A.; Tara, A.; et al. Statins’ Effect on Cognitive Outcome After Traumatic Brain Injury: A Systematic Review. Cureus 2021, 13, e16953. [Google Scholar] [CrossRef] [PubMed]
- Mansi, I.A.; English, J.L.; Alvarez, C.A.; Mortensen, E.M.; Pugh, M.J. Statins in survivors of traumatic brain injury: A propensity score-matched analysis. Brain Inj. 2020, 34, 1367–1374. [Google Scholar] [CrossRef]
- Gruenbaum, S.E.; Zlotnik, A.; Gruenbaum, B.F.; Hersey, D.; Bilotta, F. Pharmacologic Neuroprotection for Functional Outcomes After Traumatic Brain Injury: A Systematic Review of the Clinical Literature. CNS Drugs 2016, 30, 791–806. [Google Scholar] [CrossRef]
- Lerouet, D.; Marchand-Leroux, C.; Besson, V.C. Neuropharmacology in traumatic brain injury: From preclinical to clinical neuroprotection? Fundam. Clin. Pharmacol. 2021, 35, 524–538. [Google Scholar] [CrossRef]
- Wen, L.; You, W.; Wang, H.; Meng, Y.; Feng, J.; Yang, X. Polarization of Microglia to the M2 Phenotype in a Peroxisome Proliferator-Activated Receptor Gamma-Dependent Manner Attenuates Axonal Injury Induced by Traumatic Brain Injury in Mice. J. Neurotrauma 2018, 35, 2330–2340. [Google Scholar] [CrossRef]
- Yi, J.H.; Park, S.W.; Brooks, N.; Lang, B.T.; Vemuganti, R. PPARgamma agonist rosiglitazone is neuroprotective after traumatic brain injury via anti-inflammatory and anti-oxidative mechanisms. Brain Res. 2008, 1244, 164–172. [Google Scholar] [CrossRef] [Green Version]
- Cekic, M.; Cutler, S.M.; VanLandingham, J.W.; Stein, D.G. Vitamin D deficiency reduces the benefits of progesterone treatment after brain injury in aged rats. Neurobiol. Aging 2011, 32, 864–874. [Google Scholar] [CrossRef] [Green Version]
- Conte, V.; Uryu, K.; Fujimoto, S.; Yao, Y.; Rokach, J.; Longhi, L.; Trojanowski, J.Q.; Lee, V.M.; McIntosh, T.K.; Praticò, D. Vitamin E reduces amyloidosis and improves cognitive function in Tg2576 mice following repetitive concussive brain injury. J. Neurochem. 2004, 90, 758–764. [Google Scholar] [CrossRef]
- Peterson, T.C.; Hoane, M.R.; McConomy, K.S.; Farin, F.M.; Bammler, T.K.; MacDonald, J.W.; Kantor, E.D.; Anderson, G.D. A Combination Therapy of Nicotinamide and Progesterone Improves Functional Recovery following Traumatic Brain Injury. J. Neurotrauma 2015, 32, 765–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goffus, A.M.; Anderson, G.D.; Hoane, M. Sustained delivery of nicotinamide limits cortical injury and improves functional recovery following traumatic brain injury. Oxidative Med. Cell. Longev. 2010, 3, 145–152. [Google Scholar] [CrossRef] [Green Version]
- Haar, C.V.; Emery, M.A.; Hoane, M.R. Chronic folic acid administration confers no treatment effects in either a high or low dose following unilateral controlled cortical impact injury in the rat. Restor. Neurol. Neurosci. 2012, 30, 291–302. [Google Scholar]
- Naim, M.Y.; Friess, S.; Smith, C.; Ralston, J.; Ryall, K.; Helfaer, M.A.; Margulies, S.S. Folic acid enhances early functional recovery in a piglet model of pediatric head injury. Dev. Neurosci. 2010, 32, 466–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scrimgeour, A.G.; Condlin, M.L. Nutritional treatment for traumatic brain injury. J. Neurotrauma 2014, 31, 989–999. [Google Scholar] [CrossRef]
- McClain, C.J.; Twyman, D.L.; Ott, L.G.; Rapp, R.P.; Tibbs, P.A.; Norton, J.A.; Kasarskis, E.J.; Dempsey, R.J.; Young, B. Serum and urine zinc response in head-injured patients. J. Neurosurg. 1986, 64, 224–230. [Google Scholar] [CrossRef] [Green Version]
- Cope, E.C.; Morris, D.R.; Scrimgeour, A.G.; Levenson, C.W. Use of zinc as a treatment for traumatic brain injury in the rat: Effects on cognitive and behavioral outcomes. Neurorehabilit. Neural Repair 2012, 26, 907–913. [Google Scholar] [CrossRef]
- Cope, E.C.; Morris, D.R.; Gower-Winter, S.D.; Brownstein, N.C.; Levenson, C.W. Effect of zinc supplementation on neuronal precursor proliferation in the rat hippocampus after traumatic brain injury. Exp. Neurol. 2016, 279, 96–103. [Google Scholar] [CrossRef]
- Ménard, C.; Patenaude, C.; Gagné, A.M.; Massicotte, G. AMPA receptor-mediated cell death is reduced by docosahexaenoic acid but not by eicosapentaenoic acid in area CA1 of hippocampal slice cultures. J. Neurosci. Res. 2009, 87, 876–886. [Google Scholar] [CrossRef]
- Begum, G.; Yan, H.Q.; Li, L.; Singh, A.; Dixon, C.E.; Sun, D. Docosahexaenoic acid reduces ER stress and abnormal protein accumulation and improves neuronal function following traumatic brain injury. J. Neurosci. 2014, 34, 3743–3755. [Google Scholar] [CrossRef] [Green Version]
- Wu, A.; Ying, Z.; Schubert, D.; Gomez-Pinilla, F. Brain and spinal cord interaction: A dietary curcumin derivative counteracts locomotor and cognitive deficits after brain trauma. Neurorehabil. Neural. Repair 2011, 25, 332–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.J.; Chen, T.H.; Yang, L.Y.; Shih, C.M. Resveratrol protects astrocytes against traumatic brain injury through inhibiting apoptotic and autophagic cell death. Cell Death Dis. 2014, 5, e1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theadom, A.; Mahon, S.; Barker-Collo, S.; McPherson, K.; Rush, E.; Vandal, A.C.; Feigin, V.L. Enzogenol for cognitive functioning in traumatic brain injury: A pilot placebo-controlled RCT. Eur. J. Neurol. 2013, 20, 1135–1144. [Google Scholar] [CrossRef] [PubMed]
- Baltazar, G.A.; Pate, A.J.; Panigrahi, B.; LaBoy, S.; Prosniak, R.; Mody, A.; Chendrasekhar, A. Malnutrition as measured by albumin and prealbumin on admission is associated with poor outcomes after severe traumatic brain injury. Am. Surg. 2015, 81, E61-3. [Google Scholar] [CrossRef] [PubMed]
- Horsfield, S.A.; Rosse, R.B.; Tomasino, V.; Schwartz, B.L.; Mastropaolo, J.; Deutsch, S.I. Fluoxetine’s effects on cognitive performance in patients with traumatic brain injury. Int. J. Psychiatry Med. 2002, 32, 337–344. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Pharmaceutical Agents | Effects on CNS | Timing of Usage | Role in TBI Treatment | Reference |
|---|---|---|---|---|
| Acute phase | ||||
| Tranexamic acid | Antifibrinolytics | Within 3 h of injury | Reduces the risk of death in mild to moderate TBI | [8] |
| Vitamin K, FFP, Direct oral anticoagulants reversal agents | Coagulopathy reversal agents | Immediately after coagulopathy is identified | Reversal of coagulopathies | [9,10,11,12,13] |
| Mannitol and hypertonic saline | Elevates blood plasma osmolality, drawing water from brain and CSF | When impending cerebral herniation is noted; assessment in every 1–2 h | Management of intracranial hypertension and cerebral edema | [16,17] |
| Barbiturates and propofol | Anesthetics and sedatives | When there is elevated ICP refractory to other therapies | Depress cerebral metabolism, decreased oxygen consumption, lower ICP, and prevent seizures | [18] |
| Heparin, LMWH | Anticoagulants | Within 24–48 h of injury | Prevention of venous thromboembolism | [19] |
| Phenytoin, levetiracetam, and valproate | Antiepileptics | Within 7 days of injury | Reduce the incidence of early seizures but does not prevent the later development of epilepsy | [31] |
| Paracetamol and NSAIDs | Antipyretics | If fever | Maintenance of normothermia | [32,33] |
| Post-acute phase | ||||
| SSRIs | Block the reabsorption of serotonin into neurons. | Weeks to months | Improve post-TBI depression, apathy, pathological laughing and crying; prevent the later onset of depression | [36,37,38,39,41,42,43,44,45,145] |
| SNRIs | Block the reuptake of serotonin and noradrenaline | Weeks to months | Improve post-TBI depression | [46,47] |
| Trazodone | Serotonin antagonist and reuptake inhibitor | Weeks to months | Mixed results on sleep | [49] |
| TCAs | Block the reuptake of serotonin and norepinephrine | Weeks to months | Treatment of post-TBI depression | [50] |
| Buspirone | Agonist of 5-HT1A receptor | Weeks to months | Reduce anxiety in patients with TBI | [54] |
| Typical and atypical antipsychotics | Block the dopamine receptors | Weeks to months | Improve post-TBI psychosis | [55,56,57,58,59,60,61,62,63] |
| Levodopa/carbidopa | Agonist of Dopamine receptor | Weeks to months | To improve consciousness | [65] |
| Bromocriptine | Agonist of the D2 receptor | Weeks to months | To improve arousal | [66] |
| Prazosin | Block the α1 receptor | Weeks to months | Reduce daytime sleepiness, improve headaches, and improve cognition | [68] |
| Beta blockers | Block the β-adrenergic receptors | Weeks to months | Reduce post-TBI agitation | [69] |
| Amantadine | Antagonist of the NMDA-type glutamate receptor | Weeks to months | Improve the pace of functional recovery. Improve early arousal in the acute phase of TBI | [37,71,72,73] |
| Lamotrigine | Sodium channel blocker | Weeks to months | Reduce aggressive behavior in TBI patients | [74] |
| Modafinil | Central nervous system stimulant | Weeks to months | Could improve excessive daytime sleepiness and sleep latency | [75,77] |
| Methylphenidate | Central nervous system stimulant | Weeks to months | Could improve post-TBI attention and processing speed | [78,79,80,81] |
| Lisdexamfetamine dimesylate | Central nervous system stimulant | Weeks to months | improve attention and working memory | [82] |
| Rivastigmine and donepezil | Inactivate the cholinesterases | Weeks to months | Could improve memory in some subgroups of patients | [85] |
| Benzodiazepines | Agonist of GABA receptor | Weeks to months | Generally to be avoided; may impair attention, coordination, memory, and increase sedation | [86,87] |
| Zolpidem | Agonist of GABA receptor | Weeks to months | Could cause a temporary response in a fraction of patients with severe TBI | [89] |
| Melatonin | Agonist of melatonin receptors | Weeks to months | Improve daytime sleepiness. | [92] |
| Ramelteon | Agonist of melatonin receptors | Weeks to months | Could improve total sleep time | [93] |
| Balofen, tizanidine | Block transmission at the neuromuscular junction | Weeks to months | Decrease muscle spasm, reduce muscle tone | [94,95,96] |
| Botulinum toxin | Block presynaptic release of the acetylcholine at the neuromuscular junction | Weeks to months | Treatment of spasticity, improve post-TBI headache | [97,98] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tani, J.; Wen, Y.-T.; Hu, C.-J.; Sung, J.-Y. Current and Potential Pharmacologic Therapies for Traumatic Brain Injury. Pharmaceuticals 2022, 15, 838. https://doi.org/10.3390/ph15070838
Tani J, Wen Y-T, Hu C-J, Sung J-Y. Current and Potential Pharmacologic Therapies for Traumatic Brain Injury. Pharmaceuticals. 2022; 15(7):838. https://doi.org/10.3390/ph15070838
Chicago/Turabian StyleTani, Jowy, Ya-Ting Wen, Chaur-Jong Hu, and Jia-Ying Sung. 2022. "Current and Potential Pharmacologic Therapies for Traumatic Brain Injury" Pharmaceuticals 15, no. 7: 838. https://doi.org/10.3390/ph15070838
APA StyleTani, J., Wen, Y.-T., Hu, C.-J., & Sung, J.-Y. (2022). Current and Potential Pharmacologic Therapies for Traumatic Brain Injury. Pharmaceuticals, 15(7), 838. https://doi.org/10.3390/ph15070838