
Effect of Norelgestromin and Ethinylestradiol in Transdermal Patches on the Clinical Outcomes and Biochemical Parameters of COVID-19 Patients: A Clinical Trial Pilot Study


 , , , ,
, , , , 
Abstract
:1. Introduction
2. Results
2.1. Clinical and Demographic Data
2.2. Follow-Up and Outcomes
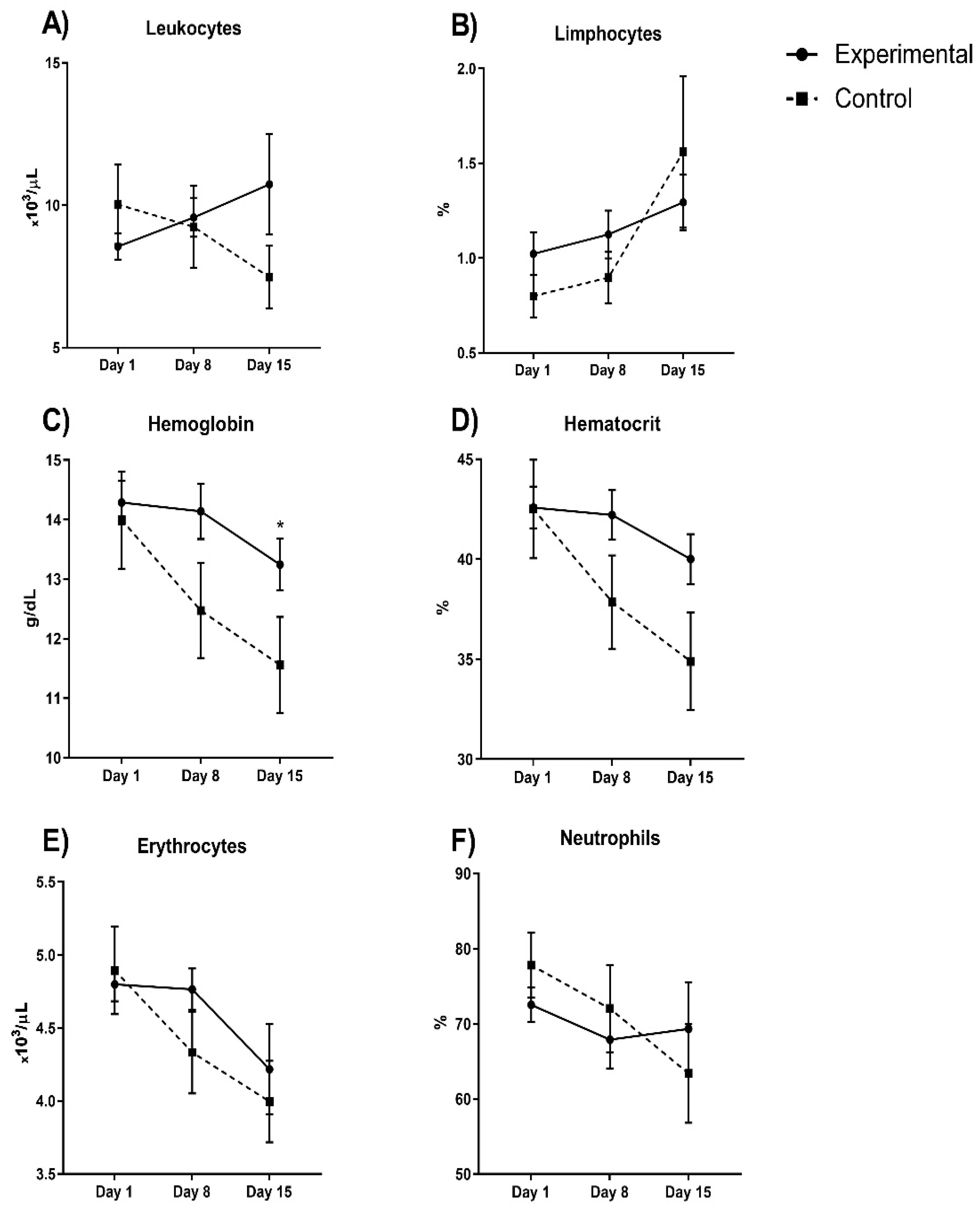
2.2.1. Principal Outcomes
2.2.2. Clinical Signs
2.2.3. Safety Outcomes
3. Discussion
4. Materials and Methods
4.1. Trial Oversight
4.2. Patients
4.3. Trial Procedures
4.4. Outcomes
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Harvey, W.T.; Carabelli, A.M.; Jackson, B.; Gupta, R.K.; Thomson, E.C.; Harrison, E.M.; Ludden, C.; Reeve, R.; Rambaut, A.; Peacock, S.J.; et al. SARS-CoV-2 variants, spike mutations and immune escape. Nat. Rev. Microbiol. 2021, 19, 409–424. [Google Scholar] [CrossRef]
- Grosser, M.R.; Hale, R.E. Analysis of a COVID-19 Clinical Trial to Emphasize Experimental Design and Quantitative Reasoning in an Introductory Biology Course. J. Microbiol. Biol. Educ. 2021, 22, ev22i1.2389. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.B.; Zhong, J.C.; Grant, M.B.; Oudit, G.Y. Role of the ACE2/Angiotensin 1-7 Axis of the Renin-Angiotensin System in Heart Failure. Circ. Res. 2016, 118, 1313–1326. [Google Scholar] [CrossRef] [Green Version]
- Donoghue, M.; Hsieh, F.; Baronas, E.; Godbout, K.; Gosselin, M.; Stagliano, N.; Donovan, M.; Woolf, B.; Robison, K.; Jeyaseelan, R.; et al. A novel angiotensin-converting enzyme-related carboxypeptidase (ACE2) converts angiotensin I to angiotensin 1–9. Circ. Res. 2000, 87, E1–E9. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Pineda, J.A.; Albaghdadi, M.; Jiang, W.; Vera-Lopez, K.J.; Nieto-Montesinos, R.; Alvarez, K.L.F.; Del-Caprio, G.D.; Gómez, B.; Lindsay, M.E.; Malhotra, R.; et al. Structural and Functional Analysis of Female Sex Hormones against SARS-CoV-2 Cell Entry. Int. J. Mol. Sci. 2021, 22, 11508. [Google Scholar] [CrossRef] [PubMed]
- Fagyas, M.; Fejes, Z.; Sütő, R.; Nagy, Z.; Székely, B.; Pócsi, M.; Ivády, G.; Bíró, E.; Bekő, G.; Nagy, A.; et al. Circulating ACE2 activity predicts mortality and disease severity in hospitalized COVID-19 patients. Int. J. Infect. Dis. 2022, 115, 8–16. [Google Scholar] [CrossRef]
- Chen, F.; Zhang, Y.; Li, X.; Li, W.; Liu, X.; Xue, X. The Impact of ACE2 Polymorphisms on COVID-19 Disease: Susceptibility, Severity, and Therapy. Front. Cell Infect. Microbiol. 2021, 11, 753721. [Google Scholar] [CrossRef]
- Mondal, S.; Rai, U. Sexual dimorphism in phagocytic activity of wall lizard‘s splenic macrophages and its control by sex steroids. Gen. Comp. Endocrinol. 1999, 116, 291–298. [Google Scholar] [CrossRef]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Scully, E.; Haverfield, J.; Ursin, R.; Tannenbaum, C.; Klein, S.L. Sex is a variable in immune responses and COVID-19 outcomes. Nat. Rev. Immunol. 2020, 20, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Scavini, M.; Piemonti, L. Gender and Age Effects on the Rates of Infection and Deaths in Individuals with Confirmed SARS-CoV-2 Infection in Six European Countries. Lancet 2020, 3576790. [Google Scholar] [CrossRef]
- Gebhard, C.; Regitz-Zagrosek, V.; Neuhauser, H.K.; Morgan, R.; Klein, S.L. Impact of Sex and Gender on COVID-19 Outcomes in Europe. Biol. Sex Differ. 2020, 11, 29. [Google Scholar] [CrossRef] [PubMed]
- Palaiodimos, L.; Kokkinidis, D.G.; Li, W.; Karamanis, D.; Ognibene, J.; Arora, S.; Southern, W.N.; Mantzoros, C.S. Severe Obesity, Increasing Age and Male Sex are Independently Associated with Worse in-Hospital Outcomes, and Higher in-Hospital Mortality, in a Cohort of Patients With COVID-19 in the Bronx, New York. Metabolism 2020, 108, 154262. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Dhakal, S.; Ursin, R.; Deshpande, S.; Sandberg, K.; Mauvais-Jarvis, F. Biological Sex Impacts COVID-19 Outcomes. PLoS Pathog. 2020, 16, e1008570. [Google Scholar] [CrossRef] [PubMed]
- Mauvais-Jarvis, F.; Klein, S.L.; Levin, E.R. Estradiol, progesterone, immunomodulation, and COVID-19 outcomes. Endocrinology 2020, 161, bqaa127. [Google Scholar] [CrossRef]
- Pazos, M.A.; Kraus, T.A.; Muñoz-Fontela, C.; Moran, T.M. Estrogen mediates innate and adaptive immune alterations to influenza infection in pregnant mice. PLoS ONE 2012, 7, e40502. [Google Scholar] [CrossRef] [Green Version]
- Vermillion, M.S.; Ursin, R.L.; Attreed, S.E.; Klein, S.L. Estriol reduces pulmonary immune cell recruitment and inflammation to protect female mice from severe influenza. Endocrinology 2018, 159, 3306–3320. [Google Scholar] [CrossRef] [Green Version]
- Samuel, R.M.; Majd, H.; Richter, M.N.; Ghazizadeh, Z.; Zekavat, S.M.; Navickas, A.; Ramirez, J.T.; Asgharian, H.; Simoneau, C.R.; Bonser, L.R. Androgen Signaling Regulates SARS-CoV-2 Receptor Levels and Is Associated with Severe COVID-19 Symptoms in Men. Cell Stem Cell. 2020, 27, 876–889. [Google Scholar] [CrossRef]
- Nelson, A.L. Transdermal contraception methods: Today’s patches and new options on the horizon. Expert. Opin. Pharmacother. 2015, 16, 863–873. [Google Scholar] [CrossRef]
- Dai, R.; Edwards, M.R.; Heid, B.; Ahmed, S.A. 17beta-Estradiol and 17alpha-Ethinyl Estradiol Exhibit Immunologic and Epigenetic Regulatory Effects in NZB/WF1 Female Mice. Endocrinology 2019, 160, 101–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, M.R.; Dai, R.; Heid, B.; Cowan, C.; Werre, S.R.; Cecere, T.; Ahmed, S.A. Low-dose 17alpha-ethinyl estradiol (EE) exposure exacerbates lupus renal disease and modulates immune responses to TLR7/9 agonists in genetically autoimmune-prone mice. Sci. Rep. 2020, 10, 5210. [Google Scholar] [CrossRef] [PubMed]
- Tian, W.; Jiang, W.; Yao, J.; Nicholson, C.J.; Li, R.H.; Sigurslid, H.H.; Wooster, L.; Rotter, J.I.; Guo, X.; Malhotra, R. Predictors of mortality in hospitalized COVID-19 patients: A systematic review and meta-analysis. J. Med. Virol. 2020, 92, 1875–1883. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.M.; Bai, P.; He, W.; Wu, F.; Liu, X.F.; Han, D.M.; Liu, S.; Yang, J.K. Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. Front. Public Health. 2020, 8, 152. [Google Scholar] [CrossRef]
- Seeland, U.; Coluzzi, F.; Simmaco, M.; Mura, C.; Bourne, P.E.; Heiland, M.; Preissner, R.; Preissner, S. Evidence for treatment with estradiol for women with SARS-CoV-2 infection. BMC Med. 2020, 18, 369. [Google Scholar] [CrossRef]
- Yanez, N.D.; Weiss, N.S.; Romand, J.A.; Treggiari, M.M. COVID-19 mortality risk for older men and women. BMC Public Health 2020, 20, 1742. [Google Scholar] [CrossRef]
- Ahrenfeldt, L.J.; Otavova, M.; Christensen, K.; Lindahl-Jacobsen, R. Sex and age differences in COVID-19 mortality in Europe. Wien. Klin. Wochenschr. 2021, 133, 393–398. [Google Scholar] [CrossRef]
- Zarulli, V.; Barthold-Jones, J.A.; Oksuzyan, A.; Lindahl-Jacobsen, R.; Christensen, K.; Vaupel, J.W. Women live longer than men even during severe famines and epidemics. Proc. Natl. Acad. Sci. USA 2018, 115, E832–E840. [Google Scholar] [CrossRef] [Green Version]
- Seth, S.; Sharma, R.; Mishra, P.; Solanki, H.K.; Singh, M.; Singh, M. Role of Short-Term Estradiol Supplementation in Symptomatic Postmenopausal COVID-19 Females: A Randomized Controlled Trial. J. Midlife Health 2021, 12, 211–218. [Google Scholar] [CrossRef]
- Costeira, R.; Lee, K.A.; Murray, B.; Christiansen, C.; Castillo-Fernandez, J.; Ni Lochlainn, M.; Pujol, J.C.; Macfarlane, H.; Kenny, L.C.; Buchan, I.; et al. Estrogen and COVID-19 symptoms: Associations in women from the COVID Symptom Study. PLoS ONE 2020, 16, e025705. [Google Scholar] [CrossRef]
- Ghandehari, S.; Matusov, Y.; Pepkowitz, S.; Stein, D.; Kaderi, T.; Narayanan, D.; Hwang, J.; Chang, S.; Goodman, R.; Ghandehari, H.; et al. Progesterone in addition to standard of care vs standard of care alone in the treatment of men hospitalized with moderate to severe COVID-19: A randomized, controlled pilot trial. Chest 2021, 160, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Lovre, D.; Bateman, K.; Sherman, M.; Fonseca, V.A.; Lefante, J.; Mauvais-Jarvis, F. Acute estradiol and progesterone therapy in hospitalised adults to reduce COVID-19 severity: A randomised control trial. BMJ Open 2021, 11, e053684. [Google Scholar] [CrossRef] [PubMed]
- Piccinni, M.P.; Giudizi, M.G.; Biagiotti, R.; Beloni, L.; Giannarini, L.; Sampognaro, S.; Parronchi, P.; Manetti, R.; Annunziato, F.; Livi, C. Progesterone favors the development of human T helper cells producing Th2-type cytokines and promotes both IL-4 production and membrane CD30 expression in established Th1 cell clones. J. Immunol. 1995, 155, 128–133. [Google Scholar] [PubMed]
- Haitao, T.; Vermunt, J.V.; Abeykoon, J.; Ghamrawi, R.; Gunaratne, M.; Jayachandran, M.; Narang, K.; Parashuram, S.; Suvakov, S.; Garovic, V.D. COVID-19 and Sex Differences: Mechanisms and Biomarkers. Mayo Clin. Proc. 2020, 95, 2189–2203. [Google Scholar] [CrossRef]
- Velavan, T.P.; Meyer, C.G. Mild versus severe COVID-19: Laboratory markers. Int. J. Infect. Dis. 2020, 95, 304–307. [Google Scholar] [CrossRef]
- Rehman, S.; Ravinayagam, V.; Nahvi, I.; Aldossary, H.; Al-Shammari, M.; Amiri, M.S.A.; Kishore, U.; Al-Suhaimi, E.A. Immunity, Sex Hormones, and Environmental Factors as Determinants of COVID-19 Disparity in Women. Front. Immunol. 2021, 12, 680845. [Google Scholar] [CrossRef]
- Lemes, R.M.R.; Costa, A.J.; Bartolomeo, C.S.; Bassani, T.B.; Nishino, M.S.; Pereira, G.; Smaili, S.S.; Maciel, R.M.B.; Braconi, C.T.; da Cruz, E.F.; et al. 17beta-estradiol reduces SARS-CoV-2 infection in vitro. Physiol. Rep. 2021, 9, e14707. [Google Scholar] [CrossRef]
- Carriere, F.; Longhi, S.; Record, M. The endosomal lipid bis(monoacylglycero) phosphate as a potential key player in the mechanism of action of chloroquine against SARS-COV-2 and other enveloped viruses hijacking the endocytic pathway. Biochimie 2020, 179, 237–246. [Google Scholar] [CrossRef]
- Liu, J.; Li, S.; Liu, J.; Liang, B.; Wang, X.; Wang, H.; Li, W.; Tong, Q.; Yi, J.; Zhao, L.; et al. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. EBioMedicine 2020, 55, 102763. [Google Scholar] [CrossRef]
- Hussman, J.P. Cellular and molecular pathways of COVID-19 and potential points of therapeutic intervention. Front. Pharmacol. 2020, 11, 1169. [Google Scholar] [CrossRef]
- Dahan, S.; Segal, G.; Katz, I.; Hellou, T.; Tietel, M.; Bryk, G.; Amital, H.; Shoenfeld, Y.; Dagan, A. Ferritin as a Marker of Severity in COVID-19 Patients: A Fatal Correlation. Isr. Med. Assoc. J. 2020, 22, 494–500. [Google Scholar] [PubMed]
- Cheng, L.; Li, H.; Li, L.; Liu, C.; Yan, S.; Chen, H.; Li, Y. Ferritin in the coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. J. Clin. Lab. Anal. 2020, 34, e23618. [Google Scholar] [CrossRef] [PubMed]
- Kaya, T.; Nalbant, A.; Kiliccioglu, G.K.; Cayir, K.T.; Yaylaci, S.; Varim, C. The prognostic significance of erythrocyte sedimentation rate in COVID-19. Rev. Assoc. Med. Bras. 2021, 67, 1305–1310. [Google Scholar] [CrossRef] [PubMed]
- Bochen, K.; Krasowska, A.; Milaniuk, S.; Kulczyńska, M.; Prystupa, A.; Dzida, G. Erythrocyte sedimentation rate—An old marker with new applications. J. Pre-Clin. Clin. Res. 2011, 5, 50–55. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Experimental Group (n = 30) | Control Group (n = 14) | p Value | |
|---|---|---|---|
| Age (mean ± SE) | 55.13 ± 2.5 | 54.5 ± 6.01 | 0.91 |
| Sex (n, women/men) | 12/18 | 1/13 | 0.02 |
| Overweight/obesity (n) | 2, 6.7% | 1, 7.1% | 0.69 |
| Diabetes mellitus (n) | 11, 36.7% | 4, 28.6% | 0.43 |
| Arterial hypertension (n) | 8, 36.7% | 5, 35.7% | 0.39 |
| Azithromycin 500 mg/kg (n) | 27, 90.0% | 14, 100% | 0.30 |
| Chloroquine 200 mg/kg (n) | 19, 63.3% | 10, 71.4% | 0.43 |
| Dexamethasone 8 mg/kg (n) | 19, 63.3% | 10, 71.4% | 0.43 |
| Experimental Group (n = 30) | Control Group (n = 14) | |||||
|---|---|---|---|---|---|---|
| Clinical signs (n, %) | Day 1 | Day 15 | p value | Day 1 | Day 15 | p value |
| Fever | 26 (86.67%) | 4 (13.79%) | 0.0001 | 14 (100%) | 2 (14.29%) | 0.0001 |
| Cough | 30 (100%) | 22 (75.86%) | 0.005 | 14 (100%) | 8 (57.14%) | 0.016 |
| Dyspnea | 26 (86.67%) | 6 (20.69%) | 0.0001 | 13 (92.86%) | 2 (14.29%) | 0.0001 |
| Diarrhea | 14 (46.67%) | 3 (10.34%) | 0.0001 | 9 (64.29%) | 3 (21.43%) | 0.02 |
| ARDS | 28 (93.33%) | 5 (16.67%) | 0.0001 | 11 (78.57%) | 4 (28.57%) | 0.008 |
| Safety outcomes (mean ± SD) | Day 1 | Day 15 | p value | Day 1 | Day 15 | p value |
| D dimer ng/dL | 5.34 ± 2.57 | 5.58 ± 2.18 | 1.0 | 6.49 ± 2.66 | 4.21 ± 2.26 | 1.0 |
| Fibrinogen mg/dL | 737.06 ± 220.9 | 569.46 ± 116.8 | 0.05 | 557.3 ± 204.05 | 482.27 ± 168.7 | 0.89 |
| Platelets ×103/µL | 300.56 ± 25.8 | 314.43 ± 36.16 | 1.0 | 228.78 ± 27.68 | 239.42 ± 38.65 | 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfredo, C.-A.; Noemí, C.-R.; Samuel, R.-L.; Daniel, O.-C.; Rodrigo, R.-B.; Paul, M.-T.; Mónica, E.-T.; José, C.-B.; Eleazar, L.-P.; Alfonso, A.-R.; et al. Effect of Norelgestromin and Ethinylestradiol in Transdermal Patches on the Clinical Outcomes and Biochemical Parameters of COVID-19 Patients: A Clinical Trial Pilot Study. Pharmaceuticals 2022, 15, 757. https://doi.org/10.3390/ph15060757
Alfredo C-A, Noemí C-R, Samuel R-L, Daniel O-C, Rodrigo R-B, Paul M-T, Mónica E-T, José C-B, Eleazar L-P, Alfonso A-R, et al. Effect of Norelgestromin and Ethinylestradiol in Transdermal Patches on the Clinical Outcomes and Biochemical Parameters of COVID-19 Patients: A Clinical Trial Pilot Study. Pharmaceuticals. 2022; 15(6):757. https://doi.org/10.3390/ph15060757
Chicago/Turabian StyleAlfredo, Cortés-Algara, Cárdenas-Rodríguez Noemí, Reyes-Long Samuel, Ortega-Cuellar Daniel, Ruz-Barros Rodrigo, Mondragón-Terán Paul, Escamilla-Tilch Mónica, Correa-Basurto José, Lara-Padilla Eleazar, Alfaro-Rodríguez Alfonso, and et al. 2022. "Effect of Norelgestromin and Ethinylestradiol in Transdermal Patches on the Clinical Outcomes and Biochemical Parameters of COVID-19 Patients: A Clinical Trial Pilot Study" Pharmaceuticals 15, no. 6: 757. https://doi.org/10.3390/ph15060757
APA StyleAlfredo, C.-A., Noemí, C.-R., Samuel, R.-L., Daniel, O.-C., Rodrigo, R.-B., Paul, M.-T., Mónica, E.-T., José, C.-B., Eleazar, L.-P., Alfonso, A.-R., Luis, C.-A. J., & Cindy, B. (2022). Effect of Norelgestromin and Ethinylestradiol in Transdermal Patches on the Clinical Outcomes and Biochemical Parameters of COVID-19 Patients: A Clinical Trial Pilot Study. Pharmaceuticals, 15(6), 757. https://doi.org/10.3390/ph15060757