
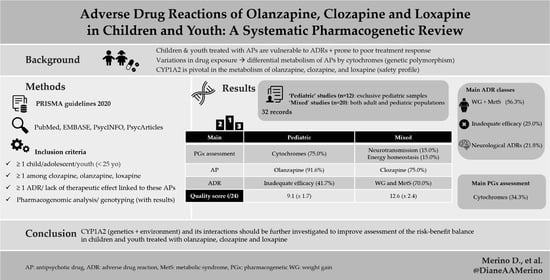
Adverse Drug Reactions of Olanzapine, Clozapine and Loxapine in Children and Youth: A Systematic Pharmacogenetic Review

 ,
,  ,
,  , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Research
2.2. Selection Criteria
- Studies including at least one child and/or adolescent and/or youth, therefore aged under 25, following the United Nations definition [45].
- Receiving at least one atypical antipsychotic that is metabolized by CYP1A2 (clozapine, olanzapine, loxapine).
- Having experienced an adverse drug reaction/a lack of therapeutic effect linked to at least one of these treatments.
- Having undergone pharmacogenomic analysis/genotyping, the results of which are mentioned.
- Record issued from an English-language and peer-reviewed journal, for which full-text was available
2.3. Quality Assessment
- 1.
- Choosing the genes/SNPs to genotype (4 binary questions).
- 2.
- Sample size (3 questions: 2 binary and 1 open).
- 3.
- Study design (1 open question).
- 4.
- Reliability of genotypes (5 binary questions).
- 5.
- Missing genotype data (6 binary questions).
- 6.
- Population stratification (2 binary questions).
- 7.
- Hardy–Weinberg Equilibrium (2 binary questions).
- 8.
- Choice and definition of outcomes (3 binary questions).
- ‘Yes’ if the study provided an adequate response.
- ‘No’ if the response was not mentioned in the manuscript nor a method publication referenced by the authors.
- ‘N/A’ (not applicable) if the response to the main (first) question of the issue of concern addressed is ‘No’.
3. Results
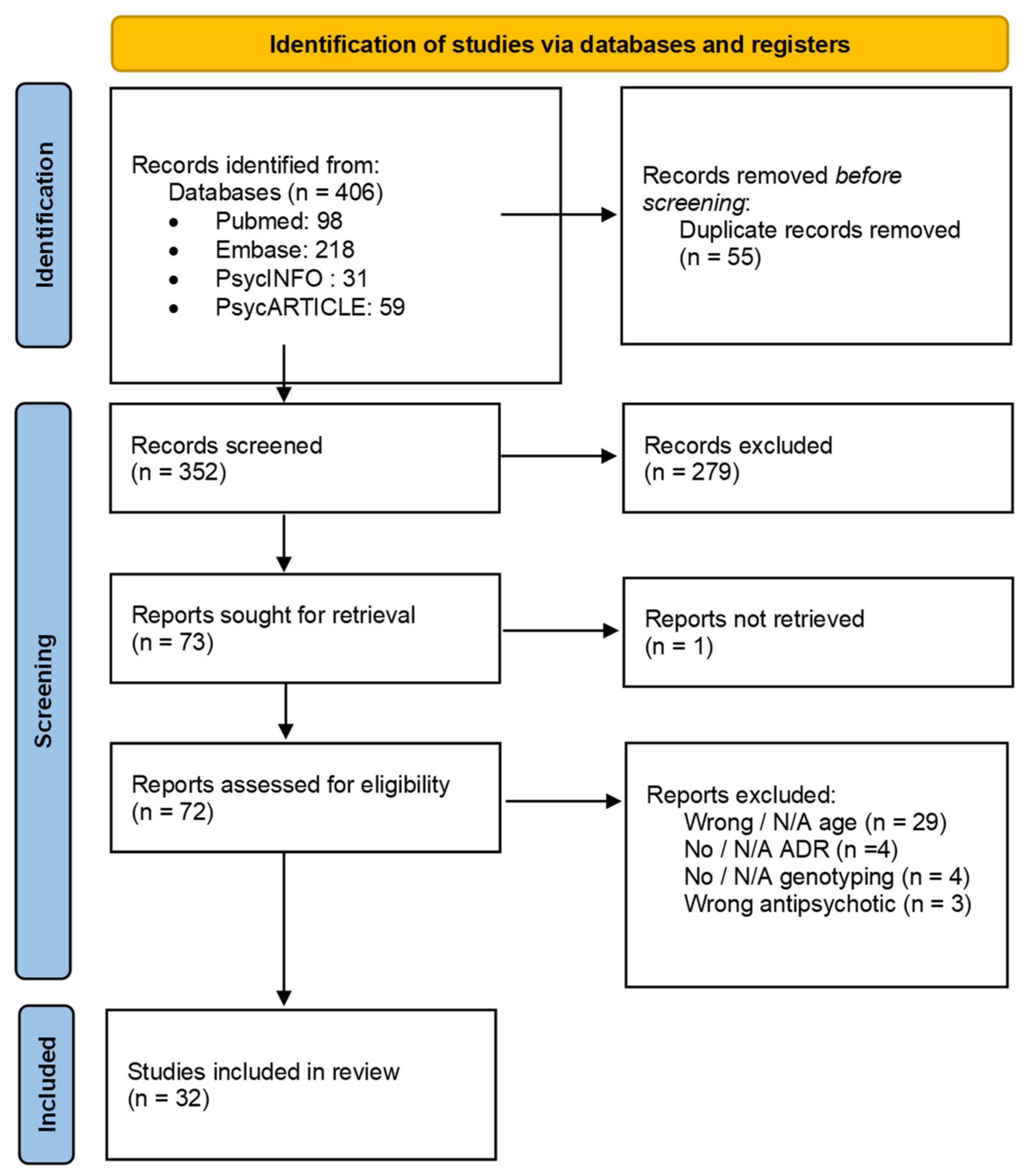
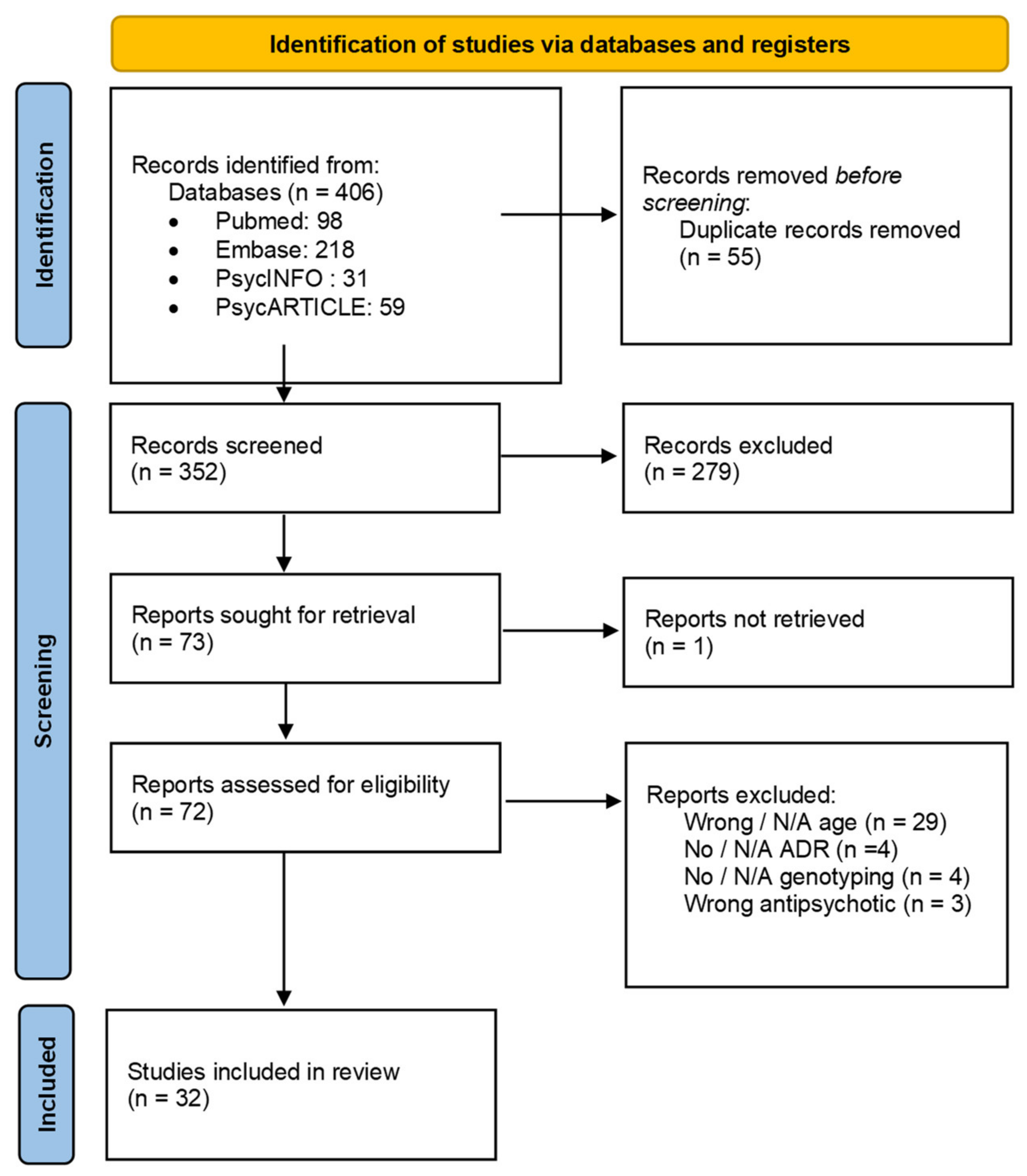
3.1. Study Selection
3.2. Characteristics of Studies
3.2.1. General Characteristics
3.2.2. Pediatric Studies

{kind=link}
{kind=link}
{kind=link}
| Study | Design | N | Age (Years) | Male (%) | Ancestry | Diagnosis | Antipsychotic | Gene Variant | ADR | Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| Baumann et al. (2006) | Case Report | 1 | 14 | 0 | Swiss? | OCD | Olanzapine | CYP2D6 XN; *4; CYP3A5 *3; CYP2B6 *6; CYP2C9 *1; CYP2C19 *1 | Generalized tonic–clonic seizure | 8 |
| Prows et al. (2009) | Cohort study | 279 (18 OLZ) | 3 to 18; mean (12.7 ± 3.2) | 50.9% | White 72.4%; Black 22.6%; Other 5.0% | Mood disorders; Disruptive behavior; Anxiety, ICD; Psychotic disorders; PDD; ED; Adjustment disorders; Other | Olanzapine | CYP2D6 *1, *3, *4, *5, Dup; CYP2C19 *1, *2 | Sleep disturbances; gastro-intestinal symptoms; headache, difficulty concentrating; mood change; dizziness; extrapyramidal symptoms; aggressive behavior; rash; shortness of breath; lack of therapeutic effect | 9 |
| Devlin et al. (2012) | Case–control study | 105 (4 OLZ) | mean (12.58 ± 3.14) | 66.7% | European 74%; Asian 8.7%; Aboriginal 2.9%; South Asian 2.9%; African/Caribbean 10.7%; Hispanic 4.8% | Non provided | Olanzapine | MTHFR (rs1801133) C677T C;T | Metabolic syndrome | 9 |
| Nussbaum et al. (2014) | Cohort study | 81 | 9 to 20; median (15.74) | 46% | Romanian? | Schizophrenia; BD | Olanzapine | CYP2D6 *4 | Weight gain | 9 |
| Nussbaum et al. (2014) | Cohort study | 81 | 9 to 20; median (15.74) | 46% | Romanian? | Schizophrenia; BD | Olanzapine | CYP2D6 *4 | Lack of therapeutic effect | 8 |
| Butwicka et al. (2014) | Case Report | 1 | 16 | 100% | Polish? | Schizophreniform disorder | Olanzapine | CYP2D6 *4 | Neuroleptic Malignant Syndrome | 8 |
| Cote et al. (2015) | Case–control study | 134 (5 OLZ) | mean (12.5 ± 3.1) | 68.7% | European 73.9%; African 7.5%; Asian 9.0%; Hispanic 5.2%; South Asian 2.2%; First Nations 2.2% | Anxiety, Depression, ADHD, Mood disorder, Psychotic disorder, Adjustment disorder, PDD, Other | Olanzapine | COMT Val158Met (rs4680) Met; Val | Cardiometabolic risk factors | 10 |
| Ocete-Hita et al. (2017) | Case–control study | 92: 30 cases (1 OLZ); 62 controls | 0 to 15; mean (8.3 ± 3) | 36.7% | White 90%; Black 3.3%; Other 6.6% | ADHD | Olanzapine | Class I HLA-A, B, C* loci, class II HLA-DRB1, DQB1, DQA1, DP loci, KIR: 14 KIR genes and 2 pseudo-KIR genes; TNFα (rs1800629); TGFβ1 (-10T/A; 25C/G); IL-10 ((rs1800896); -819T/C; -(rs1800872)); IL-6 (rs1800795); IFNγ (rs2430561) | DILI: Idiosyncratic Drug-Induced Liver Injury | 10 |
| Thümmler et al. (2018) | Case series | 9 (3 OLZ, CLZ, LOX) | 11 to 16; mean (14.1 ± 1.8) (13 to 16 OLZ, CLZ, LOX) | 55.5% (33% OLZ, CLZ, LOX) | French? | COS, ASD, ODD (OLZ, CLZ, LOX); COS, PTSD, behavioral disorder, ASD, ODD, ID | Olanzapine; Clozapine; Loxapine | CYP2D6 *3, *4, *5, *6, *41, Dup | EPS, weight gain, hepatic cytolysis, akathisia, dystonia, galactorrhea, binge eating, weight gain, constipation, lack of therapeutic effect | 9 |
| Grădinaru et al. (2019) | Cohort study | 81 | 9 to 20; median (15.74) | 54% | Romanian? | Schizophrenia; BD | Olanzapine | CYP2D6 *3, *4, *5, *41 | Hyperprolactinemia | 10 |
| Ivashchenko et al. (2020) | Cohort study | 53 (6 CLZ) (5 OLZ) | mean (15.08 ± 1.70) | 52.8% | Russian? | BPD; schizophrenia; schizoaffective disorder; schizotypal disorder; MDD; delusional disorders | Clozapine; Olanzapine | CYP2D6 *4, *9, *10; CYP3A4 *22, CYP3A5 *3; ABCB1 (rs1128503, rs2032582, rs1045642); DRD2 (rs1800497); DRD4 (rs1800955); HTR2A (rs6313) | Lack of therapeutic effect; decreased/increased salivation, increased/reduced duration of sleep, tremor, constipation, subjective akathisia; polyuria/polydipsia; increased dream activity | 13 |
| Berel et al. (2021) | Case series | 4 | 9; 10; 11; 14; | 75% | 2 Caucasian, 1 Caucasian/Indian, 1 African | Tourette syndrome and ID; behavioral disorders and neurodevelopmental delay; EOS; ASD with catatonia | Clozapine | CYP1A2 *1F, *1; CYP2D6 *1, *4, *10, *41; CYP2C19 *1, *2; CYP3A5 *1, *3; CYP3A4 *1; CYP2C9 *1, *3 | Lack of therapeutic effect (low concentrations) | 6 |
3.2.3. Mixed Population Studies
| Study | Design | N | Age (Years) | Male (%) | Ancestry | Diagnosis | Antipsychotic | Gene Variant | ADR | Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| Vandel et al. (1999) | Case–control study | 65: 22 cases (1 OLZ); 43 controls | 16 to 75; mean (41.9 ± 1.9) | 35% | French? | MDD, dysthymia, OCD, schizophrenia | Olanzapine | CYP2D6 *1A, *2, *2B, *3, *4A, *4D *5, *6B, *9, *10B | EPS: akathisia, dystonia, parkinsonism, dyskinesia | 8 |
| Hong et al. (2002) | Cohort study | 88 | 18 to 66; mean (37.1 ± 8.2) | 66% | Han Chinese | schizophrenic disorders | Clozapine | H1 receptor (rs2067467) Glu, Asp | Weight gain | 11 |
| Mosyagin et al. (2004) | Case–control study | 159: 81 cases (49 CLZ), (2 OLZ); 78 controls | Female: 22 to 85; mean (48); Male: 18 to 77; mean (47) | 36% | German Whites | schizophrenia paranoid type | Clozapine, Olanzapine | MPO (rs2333227) G,A; CYBA (rs4673) C,T; (rs1049255) A,G | Agranulocytosis | 13 |
| Theisen et al. (2004) | Cohort study | 97 | 14 to 45; mean (22.1 ± 7.7) | 59% | German | schizophrenia spectrum disorders | Clozapine | 5-HT2CR (rs3813929)-759C/T C,T | Weight gain | 11 |
| Kohlrausch et al. (2008) | Cohort study | 121: (55 NR), (27 NOGS) | 16 to 64: mean (34.02 ± 8.79) total; mean (34.13 ± 9.84) NR; mean (34.37 ± 9.41) NOGS | total 83.5%; NR 81.8%; NOGS 70.4% | European | schizophrenia | Clozapine | GNB3 (rs5443) 825C > T | Lack of therapeutic effect, NOGS: new onset generalized seizures | 12 |
| Godlewska et al. (2009) | Cohort study | 107 | mean (29.3 ± 10.0) | 49% | Caucasian, Polish | schizophrenia (mostly paranoid) | Olanzapine | 5-HT2CR (rs3813929) 759C/T C,T; 5-HT2CR (rs518147) 697G/C G,C | Weight gain | 13 |
| Le Hellard et al. (2009) | Cohort study | 160 | 10 to 64; mean (21.9 ± 8.9) | 61% | German | schizophrenia spectrum disorders | Clozapine | 44 SNPs: 3 SNPs in INSIG1; 21 SNPs in INSIG2; 3 SNPs in SCAP; 4 SNPs in SREBF1; 13 SNPs in SREBF2 | Weight gain | 14 |
| Tiwari et al. (2010) | Cohort study | 183 | 18 to 60; mean (36.12 ± 10.17) | 67.8% | European-American 63.9%; African-American 30.1%; Others 6.0% | schizophrenia or schizoaffective disorders | Clozapine, Olanzapine | 20 SNPs in CNR1 | Weight gain | 17 |
| Lencz et al. (2010) | Cohort study | 58 | 16 to 38; mean (23.5 ± 4.9) | 76.8% | African-American 40%; Caucasian (European) 28%; Hispanic 19%; Asian 5%; Other 8% | schizophrenia, schizoaffective or schizophreniform disorder | Olanzapine | DRD2 (rs1799732) 141C Ins; Del | Weight gain | 12 |
| Kohlrausch et al. (2010) | Cohort study | 116 (52 NR) | 16 to 64; mean (33.82 ± 8.51)/R: mean (33.89 ± 8.04)/NR: mean (33.73 ± 9.14) | 85.3%/R 85.9%/NR 84.6% | European | schizophrenia | Clozapine | 5-HTT HTTLPR (rs25531) LA, LG, S; VNTR Stin2 9, 10, 12 repeats | Lack of therapeutic effect | 11 |
| Jassim et al. (2011) | Cohort study | 160 | 10 to 64; mean (21.9 ± 8.9) | 61% | Central European | schizophrenia spectrum disorders | Clozapine | 96 SNPs: 13 for ADIPOQ; 10 for FABP3; 7 for PRKAA1; 14 for PRKAA2; 3 for PRKAB1; 4 for PRKAG1; 40 for PRKAG2; 4 for PRKAG3; 1 for FTO | Weight gain | 12 |
| Choong et al. (2013) | Cohort study | 444; S1: 152; S2: 174; S3: 118 | S1: 19 to 64, median (42); S2: 12 to 69, median (35); S3: 19 to 69, median (42) | S1: 52%; S2: 49%; S3: 67% | Swiss? | Psychotic disorders, mood disorders, others | Clozapine, Olanzapine | 3 CRTC1 SNPs: rs10402536 G > A; rs8104411 C > T; rs3746266 A >G | Weight gain | 13 |
| Gagliano et al. (2014) | Cohort study | 99 | 18 to 65 median (34) | 44% | Caucasian | schizophrenia or schizoaffective disorders | Clozapine, Olanzapine | 16 PRKAR2B SNPs | Weight gain | 18 |
| Dong et al. (2015) | Cohort study | 536: D: 328; R: 208 | D: 18 to 45 mean (29.1 ± 7.6); R: 18 to 60 mean (21.3 ± 8.2) | D: 48.7%; R 57.2% | Chinese Han | schizophrenia | Olanzapine | 4 A2BP1 SNPs: rs10500331, rs4786847, rs8048076, rs1478697, rs10500331 | Weight gain | 14 |
| Pouget et al. (2015) | Case–control study | 1445: 670 cases; 775 controls | 18 to 60; (38.54 ± 10.4) | 71% | European | schizophrenia of schizoaffective disorders | Clozapine, Olanzapine | TSPO 8 SNPs: rs739092, rs5759197, rs138911, rs113515, rs6971, rs6973, rs80411, rs138926 | Weight gain; lack of therapeutic effect | 16 |
| Quteineh et al. (2015) | Cohort study | 834: 478 + 168 + 188 | main: 12 to 97 median 50; S1 19.5 to 64, median (42.2); S2: 19 to 69, median (42.3) | main: 43.7%; S1 52.9%; S2 62.2% | White | Psychotic disorders, mood disorders, schizoaffective disorders, others | Clozapine, Olanzapine | HSD11B1 7 variants: rs12565406 G > T, rs10863782 G > A, rs846910 G > A, rs375319 G > A, rs12086634 T > G, rs4844488 A > G, rs84690 C > T | MetS | 11 |
| Saigi et al. (2016) | Cohort study | 750: S1: 425; S2:148; S3: 177 | combined 13 to 97 median 45; S1 13 to 97 median 51; S2 19 to 64 median 42; S3 18 to 69 median 42 | combined 50%; s1 43% s2 55% s3 62% | White | psychotic disorders, schizoaffective disorders, BD, depression, other | Clozapine, Olanzapine | 52 SNPs previously associated with BMI/21 associated with type 2 diabetes/9 associated with psychiatric disorders | Weight gain | 14 |
| Nelson et al. (2018) | Case–control study | 71: cases 32 (1 OLZ); controls 39 | 15 to 55 Met FEP mean 25.15 ± 7.20, Val FEP mean 22.92 ± 7.08 | FEP Met 75%; FEP Val 58% | Caucasian, African American, Other | schizophrenia spectrum, BD with psychosis, MDD with psychosis, psychotic disorder NOS | Olanzapine | COMT Val158Met (rs4680) Met; Val | alteration of cognitive flexibility | 11 |
| Menus et al. (2020) | Cohort study | 96 | 18 to 74, median (39) | 40% | Hungarian? | schizophrenia | Clozapine | CYP1A2 *1C, *1F, *1; CYP3A5 *1, *3; CYP3A4 *1, *1B, *22 | MetS, altered concentration, hypersalivation, blurred vision, constipation, fatigue | 11 |
| Nicotera et al. (2021) | Case–control study | 21: 4 cases; 17 controls | 16 to 46 | 62% | Caucasian | ID, psychotic disorder, schizophrenia spectrum, gait disorder, specific learning disorder, schizotypal personality disorder | Clozapine, Olanzapine | COMT Val158Met (rs4680) Met; Val COMT L136L (rs4818) G,C | Dystonia | 11 |
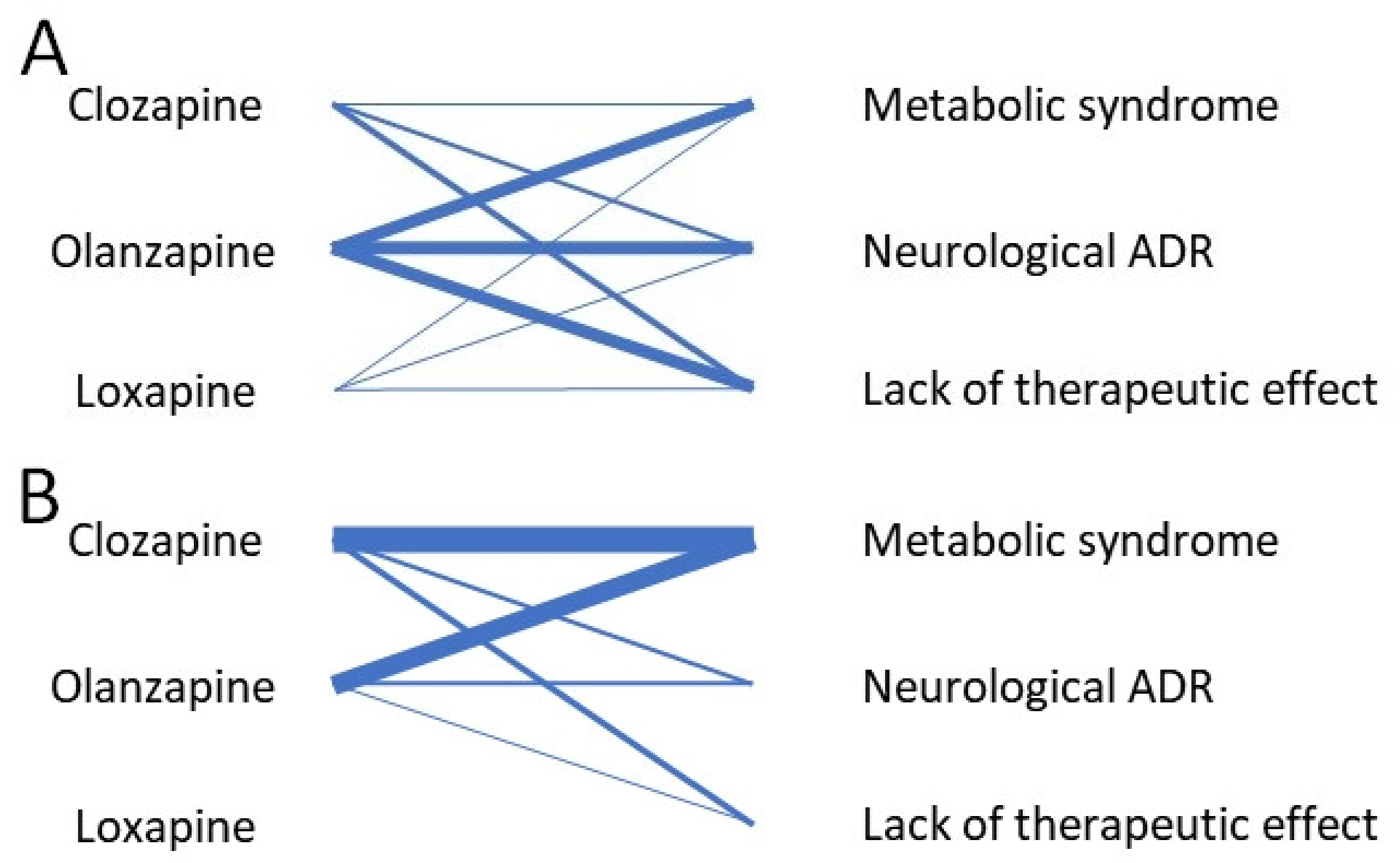
3.3. Main Adverse Drug Reactions
3.3.1. Weight Gain and Metabolic Syndrome
| Study | Diagnosis | Antipsychotic | Dosing | Outcome Measured | Gene Variant | Role of the Genes | Association | Pathophysiology |
|---|---|---|---|---|---|---|---|---|
| Devlin et al. (2012) | Not provided | Olanzapine | Not provided | MetS: weight; waist circumference; BMI; DBP and SBP; plasma glucose, insulin, TC; LDL; HDL; TG; ALAT; ASAT | MTHFR (rs1801133) C677T C;T | Conversion of folate to 5-methyltetrahydrofolate (active form) | SGA-treated children with T-allele: ↑ prevalence of MetS, ↑ diastolic blood pressure Z-scores, and fasting plasma glucose | Changes in DNA methylation + gene expression profile that favors development of MetS characteristics. |
| Nussbaum et al. (2014) A | Schizophrenia; BD | Olanzapine | Not provided | Weight gain; BMI; insulin variations | CYP2D6 *4 | Drug and steroid metabolism | Patients with the genotype wt/*4, IM have significantly ↑ WG values than the patients without *4 allele. | Nonfunctional CYP2D6 alleles increase exposure to antipsychotics. |
| Cote et al. (2015) | Anxiety, Depression, ADHD, Mood disorder, Psychotic disorder, Adjustment disorder, PDD, Other | Olanzapine | Not provided | Cardiometabolic risk factors: Plasma glucose, insulin, TC, LDL, HDL, TG; weight, waist circumference, BMI, DBP and SBP | COMT Val158Met (rs4680) Met; Val | Degradation of catecholamines | No significant findings. Interaction observed for SBP z-score. Children with Met allele had ↑ fasting plasma glucose and ↓ HDL | COMT Val158Met genotype may influence epigenetic regulation and ↓ activity of COMT = deleterious effect on cardiometabolic dysfunction and BP regulation. |
| Thümmler et al. (2018) | COS, ASD, ODD (OLZ, CLZ, LOX); COS, PTSD, behavior disorders, ASD, ODD, ID | Olanzapine; Clozapine; Loxapine | Not provided | Lack of therapeutic effect, various ADRs (weight gain, dystonia...) | CYP2D6 *3, *4, *5, *6, *41, Dup | Drug and steroid metabolism | Major adverse events in 4/9 patients | Accumulation of metabolites, CYP expression variation with age, drugs which are CYP inhibitors |
| Hong et al. (2002) | schizophrenic disorders | Clozapine | Not provided | Body weight change; BMI | H1 (rs2067467): Glu, Asp | H1 (histamine) receptor | No significant correlation between BWC and H1 genotypes. | In animal studies, blocking the H1 receptor = stimulation of feeding behaviors, and ↑ weight gain. |
| Theisen et al. (2004) | schizophrenia spectrum disorders | Clozapine | mean clozapine dose: 302 ± 128 mg/day (range 100–800 mg/day) | Weight gain; BMI change | 5-HT2CR (rs3813929)-759C/T C,T | 5-HT2CR: serotonin receptor | Higher proportion of patients with the CC genotypes with weight gain when compared with those with a T allele, this result was not significant. | Serotonin has been suggested to play an important role in the regulation of feeding behavior. |
| Godlewska et al. (2009) | schizophrenia (mostly paranoid) | Olanzapine | Olanzapine monotherapy: range 20–25mg/day | Weight gain; BMI change | 5-HT2CR (rs3813929) 759C/T C,T; 5-HT2CR (rs518147) 697G/C G,C | 5-HT2CR: serotonin receptor | A protective effect of -759T and -697C alleles was found: significantly less patients with -697C and no patient with -759T alleles experienced body mass index increase above 10%. | Serotonin could play an important role in the regulation of feeding behavior, especially particular through 5-HT2C receptors. |
| Le Hellard et al. (2009) | schizophrenia spectrum disorders | Clozapine | range 20–25 mg/day | Weight gain; BMI | 44 SNPs: 3 SNPs in INSIG1; 21 SNPs in INSIG2; 3 SNPs in SCAP; 4 SNPs in SREBF1; 13 SNPs in SREBF2 | INSIG1; INSIG2; SCAP; SREBF1 and SREBF2: regulation of biosynthesis and uptake of lipids | Strong association between 3 markers localized within or near the INSIG2 gene (rs17587100, rs10490624 and rs17047764) and AIWG. | SREBP mediated activation of lipid biosynthesis in cultured cells. INSIG2 has recently been implicated as a susceptibility gene in obesity |
| Tiwari et al. (2010) | schizophrenia or schizoaffective disorders | Clozapine, Olanzapine | mean clozapine dose: 285 ± 121 mg/day (range 50–800 mg/day | Weight gain | 20 SNPs in CNR1 | CNR1: cannabinoid receptor | No association of any of the polymorphisms with weight change In the European subgroup, the polymorphism rs806378 was the only significant SNP in genotypic comparison. Carriers of the ‘T’ allele gained more weight than the CC genotype carriers. In African-Americans a significant association was observed only for rs1049353 (increased risk for CT vs. CC). | The T allele created a binding site for arylhydrocarbon receptor translocator, a member of the basic helix–loop–helix/Per–Arnt–Sim protein family. Genetic polymorphisms in the CNR1 gene have been associated with basal metabolic index, obesity and various metabolic parameters. |
| Lencz et al. (2010) | schizophrenia, schizoaffective or schizophreniform disorder | Olanzapine | Patients randomly assigned to receive either clozapine (500 mg/day), olanzapine (20 mg/day) | Weight gain; BMI change | DRD2 (rs1799732) 141C Ins;Del | DRD2: dopamine receptor | Deletion carriers gained significantly more weight; they began to separate from Ins/Ins homozygotes after 6 weeks of treatment on either medication. | Liability to antipsychotic-induced weight gain may be related to variation in density of D2 receptors. |
| Jassim et al. (2011) | schizophrenia spectrum disorders | Clozapine | Not provided | Weight gain; BMI change as BMI-1_2 (from the start of the AP until prior to the clozapine administration), Δ BMI-2_3 (during the clozapine administration) and Δ BMI-1_3 (the whole AP treatment) period | 96 SNPs: 13 for ADIPOQ; 10 for FABP3; 7 for PRKAA1; 14 for PRKAA2; 3 for PRKAB1; 4 for PRKAG1; 40 for PRKAG2; 4 for PRKAG3; 1 for FTO | ADIPOQ; FABP3; PRKAA1; PRKAA2; PRKAB1; PRKAG1; PRKAG2; PRKAG3; FTO: regulation of lipid and energy homeostasis | Allelic and genotypic association between rs17300539 in the ADIPOQ gene and Δ BMI-1_2 and Δ BMI-1_3. 4 other ADIPOQ markers showed nominal allelic association to Δ BMI-1_2 (rs17373414) or Δ BMI-2_3 (rs864265, rs1501299 and rs6773957). rs6773957 also displayed genotypic association for Δ BMI-2_3, together with rs3821799. 1 marker in PRKAA1 (rs10074991) displayed allelic and genotypic association to Δ BMI-1_3. In PRKAA2, 3 markers demonstrated weak association either to Δ BMI-1_2 (rs4912411) or Δ BMI-1_3 (rs7519509 and rs10489617). In PRKAG2, one marker (rs17714947) demonstrated allelic, and another marker (rs7800069) genotypic association with Δ BMI-2_3. | Adiponectin has recently been suggested as a biomarker for AP-induced metabolic disturbances: negative correlation between circulating levels of adiponectin and BMI, TG and insulin levels in patients taking AP. Variants of AMPK-encoding genes influence the baseline BMI, with limited if any direct effects upon AIWG. |
| Choong et al. (2013) | Psychotic disorders, mood disorders, others | Clozapine, Olanzapine | Not provided | Weight gain; BMI change | 3 CRTC1 SNPs: rs10402536 G > A; rs8104411 C > T; rs3746266 A >G | CREB co-activator (mood, memory, energy metabolism...) | Significant association between CRTC1 rs3746266A > G and BMI, with G carriers having a lower BMI. After adjustment for the severity of the psychiatric disorder, the association between BMI and CRTC1 rs3746266A > G is even stronger. Stronger association in women, especially < 45 years. The T allele of rs6510997C > T (a proxy of the rs3746266 G allele) was associated with lower BMI and fat mass. | Role for the CRTC1 gene in the regulation of human bodyweight and fat mass consistent with animal models. Psychiatric illness and/or weight gain–inducing psychotropic drugs might play a role in genetically mediated energy homeostasis |
| Gagliano et al. (2014) | schizophrenia or schizoaffective disorders | Clozapine, Olanzapine | Not provided | Weight gain | 16 PRKAR2B SNPs | PRKAR2B: regulation of lipid homeostasis | One SNPs in PRKAR2B (rs9656135) was significantly associated with AIWG before correcting for multiple testing, but lost significance when adjusting for the 176 effective tests. | Evidence was provided by animal studies suggesting a role of the PRKAR2B gene in energy metabolism. |
| Dong et al. (2015) | schizophrenia | Olanzapine | Not provided | Weight gain; BMI | 4 A2BP1 SNPs: rs10500331, rs4786847, rs8048076, rs1478697, rs10500331 | A2BP1: regulates tissue-specific splicing, involved in neurological function | The SNP rs1478697 in the A2BP1 gene was associated with olanzapine-induced WG. The association of rs8048076 did not remain significant after correction for multiple comparisons. | A2BP1 gene was preferentially expressed in the human brain; it might affect adiposity via the hypothalamic MC4R pathway, explaining the role of A2BP1 in olanzapine induced AIWG. |
| Pouget et al. (2015) | schizophrenia of schizoaffective disorders | Clozapine, Olanzapine | Olanzapine dose (mg/d) D: 10.2 ± 2.3 R: 11.8 ± 3.1 | Weight gain; lack of therapeutic effect through treatment response (BPRS) | TSPO 8 SNPs: rs739092, rs5759197, rs138911, rs113515, rs6971, rs6973, rs80411, rs138926 | TSPO: translocator protein, peripheral benzodiazepine receptor | No association between any of the TSPO SNPs and change in overall BPRS. Non significant trend for association between rs6971 and WG, with an increase in weight for each Thr allele an individual carried. In the subset of 78 subjects treated with clozapine or olanzapine, rs6971 was nominally associated with weight gain, but did not remain significant after multiple testing correction. | Unknown mechanism by which TSPO influences glucose lowering and activation of fasting metabolism, possibilities include the altering of steroid synthesis, cytokine production or ROS levels. |
| Quteineh et al. (2015) | Psychotic disorders, mood disorders, schizoaffective disorders, others | Clozapine, Olanzapine | Not provided | Weight gain, blood pressure and the other components of MetS | HSD11B1 7 variants: rs12565406 G > T, rs10863782 G > A, rs846910 G > A, rs375319 G > A, rs12086634 T > G, rs4844488 A > G, rs84690 C > T | HSD11B1: cortisone reductase, reduces cortisone to the active hormone cortisol | Carriers of the variant rs846910-A, rs375319-A, and rs4844488-G alleles showed lower BMI values and lower WC, compared with patients with the wild-type genotypes. Association was exclusively detected in women. For the rs846906C > T SNP, only men carrying the T-allele showed higher WC compared with noncarriers. Among women, carriers of the rs846910-A, rs375319-A, and rs4844488-G alleles had lower DBP compared with noncarriers. Among men, carriers of the T-allele had higher TG levels compared with noncarriers. Men carrying the T-allele of rs846906C > T showed lower HDL-C levels compared with noncarriers. | A direct relationship between aromatase activity and body weight was proposed + estrogen may increase cortisone to cortisol conversion mediated by 11β-HSD1 and cortisol may increase aromatase activity = more estrogen in the tissues. Findings between rs846906C > T and lipid traits and BWC in men are not explained. |
| Saigi et al. (2016) | psychotic disorders, schizoaffective disorders, BD, depression, other | Clozapine, Olanzapine | Not provided | Weight gain, waist circumference, serum lipids, glucose | 52 SNPs previously associated with BMI | Weight regulation; glycemia regulation; psychiatric disorders | w-GRS of 32 polymorphisms significantly associated with BMI in men 1 SNP in CADM2 gene showed a nominal association with BMI over time. At 12 months of treatment, the rs13078807 polymorphism showed an increase in BMI for each additional risk allele. HSD11β1 rs3753519 showed an association with lower BMI for rs3753519 in patients homozygous for the variant allele compared to wild types. | The HSD11β1 gene codes for a microsomal enzyme-catalyzing tissue regeneration of active cortisol from the inactive form cortisone. It is highly expressed in metabolic tissues such as the liver and adipose tissue. ↑ plasma cortisol levels have been associated with visceral obesity and metabolic syndrome. An overexpression of this gene has been associated with hyperphagia and obesity in mice. CADM2 plays an important role in systemic energy homeostasis. |
| Menus et al. (2020) | schizophrenia | Clozapine | Clozapine daily dose (mg): 194.3 ± 130.5 | Structured questionnaire + BMI, bodyweight (obesity), fasting glucose concentrations, TG, TC, HDL, LDL | CYP1A2 *1C, *1F, *1; CYP3A5 *1, *3; CYP3A4 *1, *1B, *22 | Drug and steroid metabolism | No association between CYP1A2 or CYP3A4 expression and blood glucose, TG or cholesterol levels in patients. Moderate/high risk obesity was significantly more frequent in low CYP3A4 expressers. In low CYP3A4 expressers, a significant correlation was found between clozapine serum concentration (or daily dose) and blood glucose level | The relative activity of CYP1A2 and CYP3A4 is assumed to determine which enzyme has a greater role in clozapine metabolism. 5-HT2C antagonism has been reported to be a mechanism underlying atypical AIWG + norclozapine has a greater antagonist effect on 5-HT2C receptors than the parent compound = positive correlation between BMI and norclozapine/clozapine ratios. |
3.3.2. Neurological Symptoms: Movement Abnormalities and Seizures
| Study | Diagnosis | Antipsychotic | Dosing | Outcome Measured | Gene Variant | Role of the Genes | Association | Pathophysiology |
|---|---|---|---|---|---|---|---|---|
| Baumann et al. (2006) | OCD | Olanzapine | Olanzapine at 2.5 mg/d (day 1) and titrated until 10 mg/d on day 42 | Epileptiform seizure | CYP2D6 *4; CYP3A5 *3; CYP2B6 *6; CYP2C9 *1; CYP2C19 *1 | Drug and steroid metabolism | CYP3A5: PM 100% (but normal CYP3A activity); CYP2B6: PM 100% and CYP2D6: PM 100% (may explain high sertraline plasma levels) | Seizure favored by high sertraline concentrations + olanzapine |
| Prows et al. (2009) | Mood disorders; Disruptive behavior; Anxiety, ICD; Psychotic disorders; PDD; ED; Adjustment disorders; Other | Olanzapine | Not provided | Behavioral Intervention Score (BIS); number of PRN doses; LOS; change in GAF from admission to discharge; number of ADRs (sleep disturbances, EPS...) | CYP2D6 *1, *3, *4, *5, Dup; CYP2C19 *1, *2 | Drug and steroid metabolism | Significant relationship between combined predicted phenotype and the number of ADRs. Relationship between CYP2C19-predicted metabolizing phenotype and number and severity of ADRs. | Increased metabolizing capacity leads to a decrease in drug efficacy and number of ADRs. Regarding CYP2C19, its decreased metabolizing ability led to an increase in the number/severity of ADRs |
| Thümmler et al. (2018) | COS, ASD, ODD (OLZ, CLZ, LOX); COS, PTSD, behavioral disorders, ASD, ODD, ID | Olanzapine; Clozapine; Loxapine | Not provided | Lack of therapeutic effect, various ADRs (EPS, dystonia...) | CYP2D6 *3, *4, *5, *6, *41, Dup | Drug and steroid metabolism | Major adverse events were described in 4/9 patients representing 1/2 of PM and 2/3 of UM. | Accumulation of metabolites + CYP expression patterns alter with age + some drugs are inhibitors of CYP = might be related to pharmacoresistance. |
| Ivashchenko et al. (2020) | BPD; schizophrenia; schizoaffective disorder; schizotypal disorder; MDD; delusional disorders | Clozapine; Olanzapine | mean (SGA) (50 [50; 180] mg/day) | Tolerability of psychopharmacology: UKU SERS (salivation, duration of sleep, tremor, akathisia...), SAS, BARS; effectiveness of antipsychotics: PANSS; | CYP2D6 *4, *9, *10; CYP3A4 *22, CYP3A5 *3; ABCB1 (rs1128503, rs2032582, rs1045642); DRD2 (rs1800497); DRD4 (rs1800955); HTR2A (rs6313) | CYP2D6, CYP3A4, CYP3A5: drug and steroid metabolism; ABCB1: ATP-dependent efflux pump; DRD2 and DRD4: dopamine receptors; HTR2A: serotonin receptor | Patients with HTR2A rs6313 more often complained of tremor. DRD2 rs1800497 was significantly associated with tremor. | Associations of DRD2 rs1800497 and HTR2A rs6313 with ADEs could not be confirmed because there was coincidence with higher daily doses of antipsychotics. |
| Vandel et al. (1999) | MDD, dysthymia, OCD, schizophrenia | Olanzapine | Olanzapine 10 | EPS (SAS, Leo’s criteria) | CYP2D6 *1A, *2, *2B, *3, *4A, *4D *5, *6B, *9, *10B | Drug and steroid metabolism | Higher % of genotypes with no (extensive) functional alleles in the group of patients suffering from extrapyramidal side effects. | Increased exposure |
| Kohlrausch et al. (2008) | schizophrenia | Clozapine | Mean daily dose of clozapine: 540.91 mg/day, but varied from 100 to 900 mg/day | Clozapine response (BPRS ↓ 30% = appropriate response); occurrence of clozapine- induced NOGS (clinical interviews) | GNB3 (rs5443) 825C > T | GNB3: G-protein (G-protein-coupled receptors GPCRs) | Carriers of the T825 allele showed an increased risk for a convulsive episode. | Since dopamine and serotonin receptor subtypes activate intracellular pathways through GPCRs, the effect of the variability in the GNB3 gene might affect CNS toxicity of clozapine. |
| Nicotera et al. (2021) | ID, psychotic disorder, schizophrenia spectrum, gait disorder, specific learning disorder, schizotypal personality disorder | Clozapine, Olanzapine | Not provided | Dystonia (review of medical records) | COMT Val158Met (rs4680) Met; Val COMT L136L (rs4818) G,C | Degradation of catecholamines | G/G and A/A genotype polymorphisms of COMT gene are associated with a protective effect for developing EPS. G/A genotype, almost exclusively present in sensible patients, could be a risk factor for developing dystonia after administration of APs. | The V158M polymorphism of the COMT = low enzymatic activity and ↑ dopamine levels in the CNS = this can cause or aggravate EPS in these patients (including parkinsonism, akathisia, dystonia, and dyskinesia). |
3.3.3. Lack of Therapeutic Effect
| Study | Diagnosis | Antipsychotic | Dosing | Outcome Measured | Gene Variant | Role of the Genes | Association | Pathophysiology |
|---|---|---|---|---|---|---|---|---|
| Prows et al. (2009) | Mood disorders; Disruptive behavior; Anxiety, ICD; Psychotic disorders; PDD; ED; Adjustment disorders; Other | Olanzapine | Not provided | Behavioral Intervention Score (BIS); number of PRN doses; LOS; change in GAF from admission to discharge; number of ADRs (including sleep disturbances, EPS...) | CYP2D6 *1, *3, *4, *5, Dup; CYP2C19 *1, *2 | Drug and steroid metabolism | C-PM group had lower BIS (higher efficacy), C-UM group had highest BIS (lowest efficacy). Significant relationship between combined predicted phenotype and the number of ADRs. Relationship between CYP2C19-predicted metabolizing phenotype and number and severity of ADRs. | Increased metabolizing --> decrease in drug efficacy and number of ADRs. CYP2C19′s decreased metabolizing ability --> ↑ in the number/severity of ADRs |
| Nussbaum et al. (2014) B | Schizophrenia; BD | Olanzapine | Not provided | Lack of therapeutic effect: change in PANSS | CYP2D6 *4 | Drug and steroid metabolism | Significant correlations between wt/*4 genotype, ↑ PANSS scores, a poor clinical outcome and a bad drug response | Drug response to atypical APs correlated with the CYP2D6 genotype |
| Thümmler et al. (2018) | COS, ASD, ODD (OLZ, CLZ, LOX); COS, PTSD, behavioral disorders, ASD, ODD, ID | Olanzapine; Clozapine; Loxapine | Not provided | Lack of therapeutic effect, various ADRs (weight gain, dystonia...) | CYP2D6 *3, *4, *5, *6, *41, Dup | Drug and steroid metabolism | 5/9 patients with pharmacoresistant mental health disease presented functional CYP2D6 abnormalities. | CYP expression patterns varies with age, in addition to direct metabolism by CYP2D6, some drugs are inhibitors of CYPs |
| Ivashchenko et al. (2020) | BPD; schizophrenia; schizoaffective disorder; schizotypal disorder; MDD; delusional disorders | Clozapine; Olanzapine | mean (SGA) (50 [50; 180] mg/day) | Tolerability of psychopharmacology: UKU SERS, SAS, BARS; effectiveness of antipsychotics: PANSS; salivation, duration of sleep, tremor, akathisia... | CYP2D6 *4, *9, *10; CYP3A4 *22, CYP3A5 *3; ABCB1 (rs1128503, rs2032582, rs1045642); DRD2 (rs1800497); DRD4 (rs1800955); HTR2A (rs6313) | CYP2D6, CYP3A4, CYP3A5: drug and steroid metabolism; ABCB1: ATP-dependent efflux pump; DRD2 and DRD4: dopamine receptors; HTR2A: serotonin receptor | Carriers of DRD2 C2137T (rs1800497) had higher degree of productive symptoms subscale score change. Significant associations between the HTR2A T102C polymorphism (rs6313) and the subscale negative symptoms: the improvement in C-allele carriers significantly lower than in TT homozygotes. | DRD2 rs1800497 T-allele is associated with ↓ activity of D2 receptors (↓ binding to the ligand). ↓ in HTR2A expression in CNS may alter antipsychotics’ effect in terms of reducing negative symptoms. |
| Berel et al. (2021) | Tourette syndrome and ID; behavioral disorders and neurodevelopmental delay; EOS; ASD with catatonia | Clozapine | clozapine dosage (500 mg/day); clozapine dosage (300 mg/day); clozapine dosage between 400 and 500 mg/day; clozapine dosage (200 mg/day) | Clozapine plasma levels and clinical improvement (SAPS, ABC) with adjunction of fluvoxamine | CYP1A2 *1F, *1; CYP2D6 *1, *4, *10, *41; CYP2C19 *1, *2; CYP3A5 *1, *3; CYP3A4 *1; CYP2C9 *1, *3 | Drug and steroid metabolism | CYP1A2 UM: low clozapine plasma levels, ↑ with fluvoxamine addition (clinical improvement) CYP2D6 IM; CYP3A5 UM: low clozapine plasma levels --> fluvoxamine addition clozapine levels ↑ (clinical improvement) CYP2C9 IM: low clozapine plasma levels, ↑ with fluvoxamine addition (clinical improvement) CYP1A2 UM CYP2D6 IM CYP2C19 IM: low clozapine plasma levels, ↑ with fluvoxamine addition (clinical improvement) | Genotypes explaining low clozapine plasma level + lack of improvement with previous treatments |
| Kohlrausch et al. (2008) | schizophrenia | Clozapine | Mean daily dose of clozapine: 540.91 mg/day, but varied from 100 to 900 mg/day | Clozapine response (BPRS, reduction 30% = appropriate response); occurrence of clozapine induced new onset generalized seizures (clinical interviews) | GNB3 (rs5443) 825C > T | GNB3: G-protein (G-protein-coupled receptors GPCRs) | Homozygosis for the T825 allele more frequent among NR Homozygosis for the C825 allele more frequent among responders. | Dopamine and serotonin receptor subtypes activate intracellular pathways through GPCRs, the variability in GNB3 gene might affect medication response. |
| Kohlrausch et al. (2010) | schizophrenia | Clozapine | Patients received clozapine at doses ranging from 100 to 900 mg daily; mean daily dose of clozapine: 540.91 mg/day. | Lack of therapeutic effect: non responders/responders (30% reduction BPRS) | 5-HTT HTTLPR (rs25531) LA, LG, S; VNTR Stin2 9, 10, 12 repeats | 5-HTT: serotonin transporter | The S’-allele of HTTLPR/rs25531 was more frequent in NR. No significant association between the polymorphisms of VNTR Stin2 and clozapine response. | Carriers of the low expression allele S’ would be under increased risk for poor response to clozapine, through the influence in availability of extracellular serotonin concentrations at all synapses. Since the action of clozapine is by antagonism of serotonin receptors, the serotonin transporter coded by the L’L’ genotype (higher expression compared with the S’ allele), mediates more active re-uptake of serotonin --> less serotonin would be available to compete with clozapine for the serotonin receptors, facilitating its action. |
| Pouget et al. (2015) | schizophrenia of schizoaffective disorders | Clozapine, Olanzapine | Not provided | Weight gain; lack of therapeutic effect through treatment response (BPRS) | TSPO 8 SNPs: rs739092, rs5759197, rs138911, rs113515, rs6971, rs6973, rs80411, rs138926 | TSPO: translocator protein, peripheral benzodiazepine receptor | We found no association between any of the TSPO SNPs and change in overall BPRS. Nonsignificant trend for association between rs6971 and weight gain, with an increase in weight for each Thr allele an individual carried. In the subset of 78 subjects treated with clozapine or olanzapine, rs6971 was nominally associated with weight gain, but did not remain significant after multiple testing correction. | TSPO may act as a modifier gene, affecting clinical features of schizophrenia not investigated in the study. Although the mechanism by which TSPO influences glucose lowering and activation of fasting metabolism is unknown, possibilities include the altering of steroid synthesis, cytokine production or ROS levels. |
3.3.4. Others
3.4. Main Implications of Cytochromes Genotyping
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krause, M.; Zhu, Y.; Huhn, M.; Schneider-Thoma, J.; Bighelli, I.; Chaimani, A.; Leucht, S. Efficacy, acceptability, and tolerability of antipsychotics in children and adolescents with schizophrenia: A network meta-analysis. Eur. Neuropsychopharmacol. 2018, 28, 659–674. [Google Scholar] [CrossRef] [PubMed]
- Minjon, L.; van den Ban, E.; de Jong, E.; Souverein, P.C.; Egberts, T.C.; Heerdink, E.R. Reported Adverse Drug Reactions in Children and Adolescents Treated with Antipsychotics. J. Child Adolesc. Psychopharmacol. 2019, 29, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Thümmler, S.; Dor, E.; David, R.; Leali, G.; Battista, M.; David, A.; Askenazy, F.; Verstuyft, C. Pharmacoresistant Severe Mental Health Disorders in Children and Adolescents: Functional Abnormalities of Cytochrome P450 2D6. Front. Psychiatry 2018, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aichhorn, W.; Whitworth, A.B.; Weiss, E.M.; Marksteiner, J. Second-Generation Antipsychotics: Is There Evidence for Sex Differences in Pharmacokinetic and Adverse Effect Profiles? Drug Saf. 2006, 29, 587–598. [Google Scholar] [CrossRef]
- Becker, A.L.; Epperson, C.N. Female Puberty: Clinical Implications for the Use of Prolactin-Modulating Psychotropics. Child Adolesc. Psychiatr. Clin. N. Am. 2006, 15, 207–220. [Google Scholar] [CrossRef]
- Sagud, M.; Mihaljević-Peles, A.; Mück-Seler, D.; Pivac, N.; Vuksan-Cusa, B.; Brataljenović, T.; Jakovljević, M. Smoking and Schizophrenia. Psychiatr. Danub. 2009, 21, 371–375. [Google Scholar] [CrossRef]
- Barrangou-Poueys-Darlas, M.; Guerlais, M.; Laforgue, E.-J.; Bellouard, R.; Istvan, M.; Chauvin, P.; Guillet, J.-Y.; Jolliet, P.; Gregoire, M.; Victorri-Vigneau, C. CYP1A2 and tobacco interaction: A major pharmacokinetic challenge during smoking cessation. Drug Metab. Rev. 2021, 53, 30–44. [Google Scholar] [CrossRef]
- David, R.N.; Nebert, D.W. Comparison of Cytochrome P450 (CYP) Genes from the Mouse and Human Genomes, Including Nomenclature Recommendations for Genes, Pseudogenes and Alternative-Splice Variants. Pharm. Genom. 2004, 14, 1–18. [Google Scholar]
- Waring, R.H. Cytochrome P450: Genotype to phenotype. Xenobiotica 2020, 50, 9–18. [Google Scholar] [CrossRef]
- Gaedigk, A.; Sangkuhl, K.; Whirl-Carrillo, M.; Klein, T.; Leeder, J.S. Prediction of CYP2D6 phenotype from genotype across world populations. Genet. Med. 2017, 19, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Berel, C.; Mossé, U.; Wils, J.; Cousin, L.; Imbert, L.; Gerardin, P.; Chaumette, B.; Lamoureux, F.; Ferrafiat, V. Interest of Fluvoxamine as an Add-On to Clozapine in Children with Severe Psychiatric Disorder According to CYP Polymorphisms: Experience from a Case Series. Front. Psychiatry 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Altar, C.A.; Hornberger, J.; Shewade, A.; Cruz, V.; Garrison, J.; Mrazek, D. Clinical validity of cytochrome P450 metabolism and serotonin gene variants in psychiatric pharmacotherapy. Int. Rev. Psychiatry 2013, 25, 509–533. [Google Scholar] [CrossRef] [PubMed]
- Maruf, A.A.; Stein, K.; Arnold, P.D.; Aitchison, K.J.; Müller, D.J.; Bousman, C. CYP2D6 and Antipsychotic Treatment Outcomes in Children and Youth: A Systematic Review. J. Child Adolesc. Psychopharmacol. 2021, 31, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Desta, Z.; Flockhart, D.A. Pharmacogenetics of Drug Metabolism. In Clinical and Translational Science, 2nd ed.; Robertson, D., Williams, G.H., Eds.; Academic Press: Cambridge, MA, USA, 2017; pp. 327–345. ISBN 978-0-12-802101-9. Chapter 18. [Google Scholar]
- Callaghan, J.T.; Bergstrom, R.F.; Ptak, L.R.; Beasley, C. Olanzapine. Pharmacokinetic and Pharmacodynamic Profile. Clin. Pharmacokinet. 1999, 37, 177–193. [Google Scholar] [CrossRef] [PubMed]
- Dean, L.; Kane, M. Clozapine Therapy and CYP Genotype. In Medical Genetics Summaries; Pratt, V.M., Scott, S.A., Pirmohamed, M., Esquivel, B., Kane, M.S., Kattman, B.L., Malheiro, A.J., Eds.; National Center for Biotechnology Information (US): Bethesda, MD, USA, 2012. [Google Scholar]
- Luo, J.P.; Vashishtha, S.C.; Hawes, E.M.; McKay, G.; Midha, K.K.; Fang, J. In vitro identification of the human cytochrome p450 enzymes involved in the oxidative metabolism of loxapine. Biopharm. Drug Dispos. 2011, 32, 398–407. [Google Scholar] [CrossRef]
- Glazer, W.M. Does loxapine have “atypical” properties? Clinical evidence. J. Clin. Psychiatry 1999, 60 (Suppl. 10), 42–46. [Google Scholar]
- Popovic, D.; Nuss, P.; Vieta, E. Revisiting loxapine: A systematic review. Ann. Gen. Psychiatry 2015, 14, 15. [Google Scholar] [CrossRef]
- Diazepines, Oxazepines and Thiazepines. Available online: https://www.pharmgkb.org/chemical/PA164712682 (accessed on 26 April 2022).
- Volavka, J. Violence in schizophrenia and bipolar disorder. Psychiatr. Danub. 2013, 25, 24–33. [Google Scholar]
- Wang, P.S.; Ganz, D.A.; Benner, J.S.; Glynn, R.J.; Avorn, J. Should clozapine continue to be restricted to third-line status for schizophrenia?: A decision-analytic model. J. Ment. Health Policy Econ. 2004, 7, 77–85. [Google Scholar]
- Lesem, M.D.; Tran-Johnson, T.K.; Riesenberg, R.A.; Feifel, D.; Allen, M.H.; Fishman, R.; Spyker, D.A.; Kehne, J.H.; Cassella, J.V. Rapid acute treatment of agitation in individuals with schizophrenia: Multicentre, randomised, placebo-controlled study of inhaled loxapine. Br. J. Psychiatry 2011, 198, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Bourdinaud, V.; Pochard, F. Survey of management methods for patients in a state of agitation at admission and emergency departments in France. Encephale 2003, 29, 89–98. [Google Scholar] [PubMed]
- FDA-Approved Drugs: Olanzapine. Available online: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=020592 (accessed on 11 April 2022).
- EMA Zyprexa. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/zyprexa (accessed on 15 April 2022).
- FDA-Approved Drugs: Clozapine. Available online: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=019758 (accessed on 11 April 2022).
- Rachamallu, V.; Elberson, B.W.; Vutam, E.; Aligeti, M. Off-Label Use of Clozapine in Children and Adolescents—A Literature Review. Am. J. Ther. 2019, 26, e406–e416. [Google Scholar] [CrossRef]
- EMA EMA: Leponex (Clozapine). Available online: https://www.ema.europa.eu/en/medicines/human/referrals/leponex (accessed on 11 April 2022).
- FDA-Approved Drugs: Loxapine. Available online: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=022549 (accessed on 11 April 2022).
- EMA Adasuve. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/adasuve (accessed on 15 April 2022).
- Résumé des Caractéristiques du Produit-LOXAPAC 100 Mg, Comprimé Pelliculé-Base de Données Publique des Médicaments. Available online: https://base-donnees-publique.medicaments.gouv.fr/affichageDoc.php?specid=69893582&typedoc=R (accessed on 11 April 2022).
- Solmi, M.; Murru, A.; Pacchiarotti, I.; Undurraga, J.; Veronese, N.; Fornaro, M.; Stubbs, B.; Monaco, F.; Vieta, E.; Seeman, M.V.; et al. Safety, tolerability, and risks associated with first- and second-generation antipsychotics: A state-of-the-art clinical review. Ther. Clin. Risk Manag. 2017, 13, 757–777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drici, M.-D.; Priori, S. Cardiovascular risks of atypical antipsychotic drug treatment. Pharmacoepidemiol. Drug Saf. 2007, 16, 882–890. [Google Scholar] [CrossRef] [PubMed]
- Sohn, M.; Moga, D.; Blumenschein, K.; Talbert, J. National trends in off-label use of atypical antipsychotics in children and adolescents in the United States. Medicine 2016, 95, e3784. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C.; Haight, R.J. Safety of olanzapine use in adolescents. Expert Opin. Drug Saf. 2013, 12, 777–782. [Google Scholar] [CrossRef]
- Selim, S.; Riesenberg, R.; Cassella, J.; Kunta, J.; Hellriegel, E.; Smith, M.A.; Vinks, A.A.; Rabinovich-Guilatt, L. Pharmacokinetics and Safety of Single-Dose Inhaled Loxapine in Children and Adolescents. J. Clin. Pharmacol. 2017, 57, 1244–1257. [Google Scholar] [CrossRef]
- Roses, A.D. Pharmacogenetics and the practice of medicine. Nature 2000, 405, 857–865. [Google Scholar] [CrossRef]
- Chaplin, M.H. Improving the Reporting of Pharmacogenetic Studies to Facilitate Evidence Synthesis: Anti-Tuberculosis Drug-Related Toxicity as an Example. Ph.D. Thesis, University of Liverpool, Liverpool, UK, 2021; p. 361. [Google Scholar]
- Alkelai, A.; Greenbaum, L.; Docherty, A.R.; Shabalin, A.A.; Povysil, G.; Malakar, A.; Hughes, D.; Delaney, S.L.; Peabody, E.P.; McNamara, J.; et al. The benefit of diagnostic whole genome sequencing in schizophrenia and other psychotic disorders. Mol. Psychiatry 2021, 27, 1435–1447. [Google Scholar] [CrossRef]
- Sanders, S.J.; Neale, B.M.; Huang, H.; Werling, D.M.; An, J.-Y.; Dong, S.; Abecasis, G.; Arguello, P.A.; Blangero, J.; Boehnke, M.; et al. Whole genome sequencing in psychiatric disorders: The WGSPD consortium. Nat. Neurosci. 2017, 20, 1661–1668. [Google Scholar] [CrossRef] [Green Version]
- Samer, C.F.; Lorenzini, K.I.; Rollason, V.; Daali, Y.; Desmeules, J.A. Applications of CYP450 Testing in the Clinical Setting. Mol. Diagn. Ther. 2013, 17, 165–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Farid-Kapadia, M.; Askie, L.; Hartling, L.; Contopoulos-Ioannidis, D.; Bhutta, Z.A.; Soll, R.; Moher, D.; Offringa, M. Do systematic reviews on pediatric topics need special methodological considerations? BMC Pediatr. 2017, 17, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nations, U. Youth. Available online: https://www.un.org/en/global-issues/youth (accessed on 6 April 2022).
- Newton, L. LibGuides: Original Research: Home. Available online: https://libguides.unf.edu/originalresearch/home (accessed on 18 March 2022).
- Scherer, R.W.; Saldanha, I.J. How should systematic reviewers handle conference abstracts? A view from the trenches. Syst. Rev. 2019, 8, 264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [Green Version]
- Ross, S.; Anand, S.S.; Joseph, P.; Paré, G. Promises and challenges of pharmacogenetics: An overview of study design, methodological and statistical issues. JRSM Cardiovasc. Dis. 2012, 1, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Jorgensen, A.L.; Williamson, P.R. Methodological quality of pharmacogenetic studies: Issues of concern. Stat. Med. 2008, 27, 6547–6569. [Google Scholar] [CrossRef]
- Nussbaum, L.A.; Dumitraşcu, V.; Tudor, A.; Grădinaru, R.; Andreescu, N.; Puiu, M. Molecular Study of Weight Gain Related to Atypical Antipsychotics: Clinical Implications of the CYP2D6 Genotype. Rom. J. Morphol. Embryol. 2014, 55, 877–884. [Google Scholar]
- Nussbaum, L.; Grădinaru, R.; Andreescu, N.; Dumitraşcu, V.; Tudor, A.; Suciu, L.; Ştefănescu, R.; Puiu, M. The Response to Atypical Antipsychotic Drugs in Correlation with the Cyp2d6 Genotype: Clinical Implications and Perspectives. Farmacia 2014, 62, 1191–1201. [Google Scholar]
- Le Hellard, S.; Theisen, F.M.; Haberhausen, M.; Raeder, M.B.; Fernø, J.; Gebhardt, S.; Hinney, A.; Remschmidt, H.; Krieg, J.C.; Mehler-Wex, C.; et al. Association between the insulin-induced gene 2 (INSIG2) and weight gain in a German sample of antipsychotic-treated schizophrenic patients: Perturbation of SREBP-controlled lipogenesis in drug-related metabolic adverse effects? Mol. Psychiatry 2009, 14, 308–317. [Google Scholar] [CrossRef]
- Jassim, G.; Fernø, J.; Theisen, F.M.; Haberhausen, M.; Christoforou, A.; Håvik, B.; Gebhardt, S.; Remschmidt, H.; Mehler-Wex, C.; Hebebrand, J.; et al. Association Study of Energy Homeostasis Genes and Antipsychotic-Induced Weight Gain in Patients with Schizophrenia. Pharmacopsychiatry 2011, 44, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Theisen, F.M.; Hinney, A.; Brömel, T.; Heinzel-Gutenbrunner, M.; Martin, M.; Krieg, J.-C.; Remschmidt, H.; Hebebrand, J. Lack of association between the –759C/T polymorphism of the 5-HT2C receptor gene and clozapine-induced weight gain among German schizophrenic individuals. Psychiatr. Genet. 2004, 14, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Gagliano, S.A.; Tiwari, A.K.; Freeman, N.; Lieberman, J.A.; Meltzer, H.Y.; Kennedy, J.L.; Knight, J.; Müller, D.J. Protein kinase cAMP-dependent regulatory type II beta (PRKAR2B) gene variants in antipsychotic-induced weight gain. Hum. Psychopharmacol. 2014, 29, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, A.K.; Zai, C.C.; Likhodi, O.; Lisker, A.; Singh, D.; Souza, R.P.; Batra, P.; Zaidi, S.H.E.; Chen, S.; Liu, F.; et al. A Common Polymorphism in the Cannabinoid Receptor 1 (CNR1) Gene is Associated with Antipsychotic-Induced Weight Gain in Schizophrenia. Neuropsychopharmacology 2010, 35, 1315–1324. [Google Scholar] [CrossRef] [PubMed]
- Quteineh, L.; Vandenberghe, F.; Morgui, N.S.; Delacrétaz, A.; Choong, E.; Gholam-Rezaee, M.; Magistretti, P.; Bondolfi, G.; Von Gunten, A.; Preisig, M.; et al. Impact of HSD11B1 polymorphisms on BMI and components of the metabolic syndrome in patients receiving psychotropic treatments. Pharm. Genom. 2015, 25, 246–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saigi-Morgui, N.; Vandenberghe, F.; Delacrétaz, A.; Quteineh, L.; Gholamrezaee, M.; Aubry, J.-M.; von Gunten, A.; Kutalik, Z.; Conus, P.; Eap, C.B. Association of genetic risk scores with body mass index in Swiss psychiatric cohorts. Pharm. Genom. 2016, 26, 208–217. [Google Scholar] [CrossRef] [Green Version]
- Choong, E.; Quteineh, L.; Cardinaux, J.-R.; Gholam-Rezaee, M.; Vandenberghe, F.; Dobrinas, M.; Bondolfi, G.; Etter, M.; Holzer, L.; Magistretti, P.; et al. Influence of CRTC1 Polymorphisms on Body Mass Index and Fat Mass in Psychiatric Patients and the General Adult Population. JAMA Psychiatry 2013, 70, 1011–1019. [Google Scholar] [CrossRef] [Green Version]
- Menus, Á.; Kiss, Á.; Tóth, K.; Sirok, D.; Déri, M.; Fekete, F.; Csukly, G.; Monostory, K. Association of clozapine-related metabolic disturbances with CYP3A4 expression in patients with schizophrenia. Sci. Rep. 2020, 10, 21283. [Google Scholar] [CrossRef]
- Godlewska, B.R.; Olajossy-Hilkesberger, L.; Ciwoniuk, M.; Olajossy, M.; Marmurowska-Michałowska, H.; Limon, J.; Landowski, J.; Marmurowska-Micha, H. Olanzapine-induced weight gain is associated with the −759C/T and −697G/C polymorphisms of the HTR2C gene. Pharm. J. 2009, 9, 234–241. [Google Scholar] [CrossRef]
- Hong, C.-J.; Lin, C.-H.; Yu, Y.W.-Y.; Chang, S.-C.; Wang, S.-Y.; Tsai, S.-J. Genetic variant of the histamine-1 receptor (glu349asp) and body weight change during clozapine treatment. Psychiatr. Genet. 2002, 12, 169–171. [Google Scholar] [CrossRef]
- Lencz, T.; Robinson, D.G.; Napolitano, B.; Sevy, S.; Kane, J.M.; Goldman, D.; Malhotra, A.K. DRD2 promoter region variation predicts antipsychotic-induced weight gain in first episode schizophrenia. Pharm. Genom. 2010, 20, 569–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cote, A.T.; Panagiotopoulos, C.; Devlin, A.M. Interaction between the Val158Met catechol-O-methyltransferase gene variant and second-generation antipsychotic treatment on blood pressure in children. Pharm. J. 2015, 15, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Devlin, A.M.; Ngai, Y.F.; Ronsley, R.; Panagiotopoulos, C. Cardiometabolic risk and the MTHFR C677T variant in children treated with second-generation antipsychotics. Transl. Psychiatry 2012, 2, e71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, L.; Yan, H.; Huang, X.; Hu, X.; Yang, Y.; Ma, C.; Du, B.; Lu, T.; Jin, C.; Wang, L.; et al. A2BP1 gene polymorphisms association with olanzapine-induced weight gain. Pharmacol. Res. 2015, 99, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Pouget, J.G.; Gonçalves, V.F.; Nurmi, E.L.; Laughlin, C.P.; Mallya, K.S.; McCracken, J.T.; Aman, M.G.; McDougle, C.J.; Scahill, L.; Misener, V.L.; et al. Investigation of TSPO variants in schizophrenia and antipsychotic treatment outcomes. Pharmacogenomics 2015, 16, 5–22. [Google Scholar] [CrossRef]
- Baumann, P.; Barbe, R.; Vabre-Bogdalova, A.; Garran, E.; Crettol, S.; Eap, C.B. Epileptiform Seizure after Sertraline Treatment in an Adolescent Experiencing Obsessive-Compulsive Disorder and Presenting a Rare Pharmacogenetic Status. J. Clin. Psychopharmacol. 2006, 26, 679–681. [Google Scholar] [CrossRef]
- Prows, C.A.; Nick, T.G.; Saldaña, S.N.; Pathak, S.; Liu, C.; Zhang, K.; Daniels, Z.S.; Vinks, A.A.; Glauser, T.A. Drug-Metabolizing Enzyme Genotypes and Aggressive Behavior Treatment Response in Hospitalized Pediatric Psychiatric Patients. J. Child Adolesc. Psychopharmacol. 2009, 19, 385–394. [Google Scholar] [CrossRef] [Green Version]
- Vandel, P.; Haffen, E.; Vandel, S.; Bonin, B.; Nezelof, S.; Sechter, D.; Broly, F.; Bizouard, P.; Dalery, J. Drug extrapyramidal side effects. CYP2D6 genotypes and phenotypes. Eur. J. Clin. Pharmacol. 1999, 55, 659–665. [Google Scholar] [CrossRef]
- Kohlrausch, F.B.; Salatino-Oliveira, A.; Gama, C.S.; Lobato, M.I.; Belmonte-de-Abreu, P.; Hutz, M.H. G-protein gene 825C>T polymorphism is associated with response to clozapine in Brazilian schizophrenics. Pharmacogenomics 2008, 9, 1429–1436. [Google Scholar] [CrossRef]
- Ivashchenko, D.V.; Khoang, S.Z.; Makhmudova, B.V.; Buromskaya, N.I.; Shimanov, P.V.; Deitch, R.V.; Akmalova, K.A.; Shuev, G.N.; Dorina, I.V.; Nastovich, M.I.; et al. Pharmacogenetics of antipsychotics in adolescents with acute psychotic episode during first 14 days after admission: Effectiveness and safety evaluation. Drug Metab. Pers. Ther. 2020, 35, 20200102. [Google Scholar] [CrossRef]
- Nicotera, A.G.; Di Rosa, G.; Turriziani, L.; Costanzo, M.C.; Stracuzzi, E.; Vitello, G.A.; Rando, R.G.; Musumeci, A.; Vinci, M.; Musumeci, S.A.; et al. Role of COMT V158M Polymorphism in the Development of Dystonia after Administration of Antipsychotic Drugs. Brain Sci. 2021, 11, 1293. [Google Scholar] [CrossRef] [PubMed]
- Kohlrausch, F.B.; Salatino-Oliveira, A.; Gama, C.S.; Lobato, M.I.; Belmonte-de-Abreu, P.; Hutz, M.H. Influence of serotonin transporter gene polymorphisms on clozapine response in Brazilian schizophrenics. J. Psychiatr. Res. 2010, 44, 1158–1162. [Google Scholar] [CrossRef] [PubMed]
- Butwicka, A.; Krystyna, S.; Retka, W.; Wolańczyk, T. Neuroleptic malignant syndrome in an adolescent with CYP2D6 deficiency. Eur. J. Pediatr. 2014, 173, 1639–1642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grădinaru, R.; Andreescu, N.; Nussbaum, L.; Suciu, L.; Puiu, M. Impact of the CYP2D6 phenotype on hyperprolactinemia development as an adverse event of treatment with atypical antipsychotic agents in pediatric patients. Ir. J. Med. Sci. 2019, 188, 1417–1422. [Google Scholar] [CrossRef]
- Mosyagin, I.; Dettling, M.; Roots, I.; Mueller-Oerlinghausen, B.; Cascorbi, I. Impact of Myeloperoxidase and NADPH-Oxidase Polymorphisms in Drug-Induced Agranulocytosis. J. Clin. Psychopharmacol. 2004, 24, 613–617. [Google Scholar] [CrossRef]
- Ocete-Hita, E.; Salmerón-Fernández, M.; Urrutia-Maldonado, E.; Muñoz-De-Rueda, P.; Salmerón-Ruiz, M.; Martinez-Padilla, M.; Ruiz-Extremera, O.A. Analysis of Immunogenetic Factors in Idiosyncratic Drug-induced Liver Injury in the Pediatric Population. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 742–747. [Google Scholar] [CrossRef]
- Nelson, C.L.M.; Amsbaugh, H.M.; Reilly, J.L.; Rosen, C.; Marvin, R.W.; Ragozzino, M.E.; Bishop, J.R.; Sweeney, J.A.; Hill, S.K. Beneficial and adverse effects of antipsychotic medication on cognitive flexibility are related to COMT genotype in first episode psychosis. Schizophr. Res. 2018, 202, 212–216. [Google Scholar] [CrossRef]
- Lott, S.A.; Burghardt, P.R.; Burghardt, K.J.; Bly, M.J.; Grove, T.B.; Ellingrod, V.L. The influence of metabolic syndrome, physical activity and genotype on catechol-O-methyl transferase promoter-region methylation in schizophrenia. Pharm. J. 2013, 13, 264–271. [Google Scholar] [CrossRef] [Green Version]
- Houston, J.P.; Kohler, J.; Bishop, J.R.; Ellingrod, V.L.; Ostbye, K.M.; Zhao, F.; Conley, R.R.; Hoffmann, V.P.; Fijal, B.A. Pharmacogenomic Associations with Weight Gain in Olanzapine Treatment of Patients without Schizophrenia. J. Clin. Psychiatry 2012, 73, 1077–1086. [Google Scholar] [CrossRef]
- Konte, B.; Walters, J.T.R.; Rujescu, D.; Legge, S.E.; Pardiñas, A.F.; Cohen, D.; Pirmohamed, M.; Tiihonen, J.; Hartmann, A.M.; Bogers, J.P.; et al. HLA-DQB1 6672G>C (rs113332494) is associated with clozapine-induced neutropenia and agranulocytosis in individuals of European ancestry. Transl. Psychiatry 2021, 11, 214. [Google Scholar] [CrossRef]
- Papazisis, G.; Goulas, A.; Sarrigiannidis, A.; Bargiota, S.; Antoniadis, D.; Raikos, N.; Basgiouraki, E.; Bozikas, V.P.; Garyfallos, G. ABCB1 and CYP2D6 polymorphisms and treatment response of psychotic patients in a naturalistic setting. Hum. Psychopharmacol. Clin. Exp. 2018, 33, e2644. [Google Scholar] [CrossRef] [PubMed]
- Crescenti, A.; Mas, S.; Gassó, P.; Parellada, E.; Bernardo, M.; Lafuente, A. Cyp2d6*3, *4, *5 and *6 Polymorphisms and Antipsychotic-Induced Extrapyramidal Side-Effects in Patients Receiving Antipsychotic Therapy. Clin. Exp. Pharmacol. Physiol. 2008, 35, 807–811. [Google Scholar] [CrossRef] [PubMed]
- Wannasuphoprasit, Y.; Andersen, S.E.; Arranz, M.J.; Catalan, R.; Jurgens, G.; Kloosterboer, S.M.; Rasmussen, H.B.; Bhat, A.; Irizar, H.; Koller, D.; et al. CYP2D6 Genetic Variation and Antipsychotic-Induced Weight Gain: A Systematic Review and Meta-Analysis. Front. Psychol. 2021, 12, 768748. [Google Scholar] [CrossRef] [PubMed]
- Calafato, M.S.; Austin-Zimmerman, I.; Thygesen, J.H.; Sairam, M.; Metastasio, A.; Marston, L.; Abad-Santos, F.; Bhat, A.; Harju-Seppänen, J.; Irizar, H.; et al. The effect of CYP2D6 variation on antipsychotic-induced hyperprolactinaemia: A systematic review and meta-analysis. Pharm. J. 2020, 20, 629–637. [Google Scholar] [CrossRef]
- Prior, T.I.; Baker, G.B. Interactions between the cytochrome P450 system and the second-generation antipsychotics. J. Psychiatry Neurosci. 2003, 28, 99–112. [Google Scholar]
- Olanzapine. Available online: https://www.pharmgkb.org/chemical/PA450688 (accessed on 26 April 2022).
- Clozapine Pathway, Pharmacokinetics. Available online: https://www.pharmgkb.org/pathway/PA166163661 (accessed on 26 April 2022).
- Ivanova, S.A.; Filipenko, M.L.; Vyalova, N.M.; Voronina, E.N.; Pozhidaev, I.V.; Osmanova, D.Z.; Ivanov, M.V.; Fedorenko, O.Y.; Semke, A.V.; Bokhan, N. CYP1A2 and CYP2D6 Gene Polymorphisms in Schizophrenic Patients with Neuroleptic Drug-Induced Side Effects. Bull. Exp. Biol. Med. 2016, 160, 687–690. [Google Scholar] [CrossRef]
- Fu, Y.; Fan, C.-H.; Deng, H.-H.; Hu, S.-H.; Lv, D.-P.; Li, L.-H.; Wang, J.-J.; Lu, X.-Q. Association of CYP2D6 and CYP1A2 gene polymorphism with tardive dyskinesia in Chinese schizophrenic patients. Acta Pharmacol. Sin. 2006, 27, 328–332. [Google Scholar] [CrossRef] [Green Version]
- Melkersson, K.I.; Scordo, M.G.; Gunes, A.; Dahl, M.-L. Impact of CYP1A2 and CYP2D6 polymorphisms on drug metabolism and on insulin and lipid elevations and insulin resistance in clozapine-treated patients. J. Clin. Psychiatry 2007, 68, 697–704. [Google Scholar] [CrossRef]
- What Is GRADE? | BMJ Best Practice.
- Corponi, F.; Fabbri, C.; Serretti, A. Pharmacogenetics in Psychiatry. Adv. Pharmacol. 2018, 83, 297–331. [Google Scholar] [CrossRef]
- Milosavljevic, F.; Bukvic, N.; Pavlovic, Z.; Miljevic, C.; Pešic, V.; Molden, E.; Ingelman-Sundberg, M.; Leucht, S.; Jukic, M.M. Association of CYP2C19 and CYP2D6 Poor and Intermediate Metabolizer Status with Antidepressant and Antipsychotic Exposure: A Systematic Review and Meta-Analysis. JAMA Psychiatry 2021, 78, 270. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merino, D.; Fernandez, A.; Gérard, A.O.; Ben Othman, N.; Rocher, F.; Askenazy, F.; Verstuyft, C.; Drici, M.-D.; Thümmler, S. Adverse Drug Reactions of Olanzapine, Clozapine and Loxapine in Children and Youth: A Systematic Pharmacogenetic Review. Pharmaceuticals 2022, 15, 749. https://doi.org/10.3390/ph15060749
Merino D, Fernandez A, Gérard AO, Ben Othman N, Rocher F, Askenazy F, Verstuyft C, Drici M-D, Thümmler S. Adverse Drug Reactions of Olanzapine, Clozapine and Loxapine in Children and Youth: A Systematic Pharmacogenetic Review. Pharmaceuticals. 2022; 15(6):749. https://doi.org/10.3390/ph15060749
Chicago/Turabian StyleMerino, Diane, Arnaud Fernandez, Alexandre O. Gérard, Nouha Ben Othman, Fanny Rocher, Florence Askenazy, Céline Verstuyft, Milou-Daniel Drici, and Susanne Thümmler. 2022. "Adverse Drug Reactions of Olanzapine, Clozapine and Loxapine in Children and Youth: A Systematic Pharmacogenetic Review" Pharmaceuticals 15, no. 6: 749. https://doi.org/10.3390/ph15060749
APA StyleMerino, D., Fernandez, A., Gérard, A. O., Ben Othman, N., Rocher, F., Askenazy, F., Verstuyft, C., Drici, M.-D., & Thümmler, S. (2022). Adverse Drug Reactions of Olanzapine, Clozapine and Loxapine in Children and Youth: A Systematic Pharmacogenetic Review. Pharmaceuticals, 15(6), 749. https://doi.org/10.3390/ph15060749