
Mono or Dual Antiplatelet Therapy for Treating Patients with Peripheral Artery Disease after Lower Extremity Revascularization: A Systematic Review and Meta-Analysis

 ,
,
Abstract
1. Introduction
2. Materials and Methods
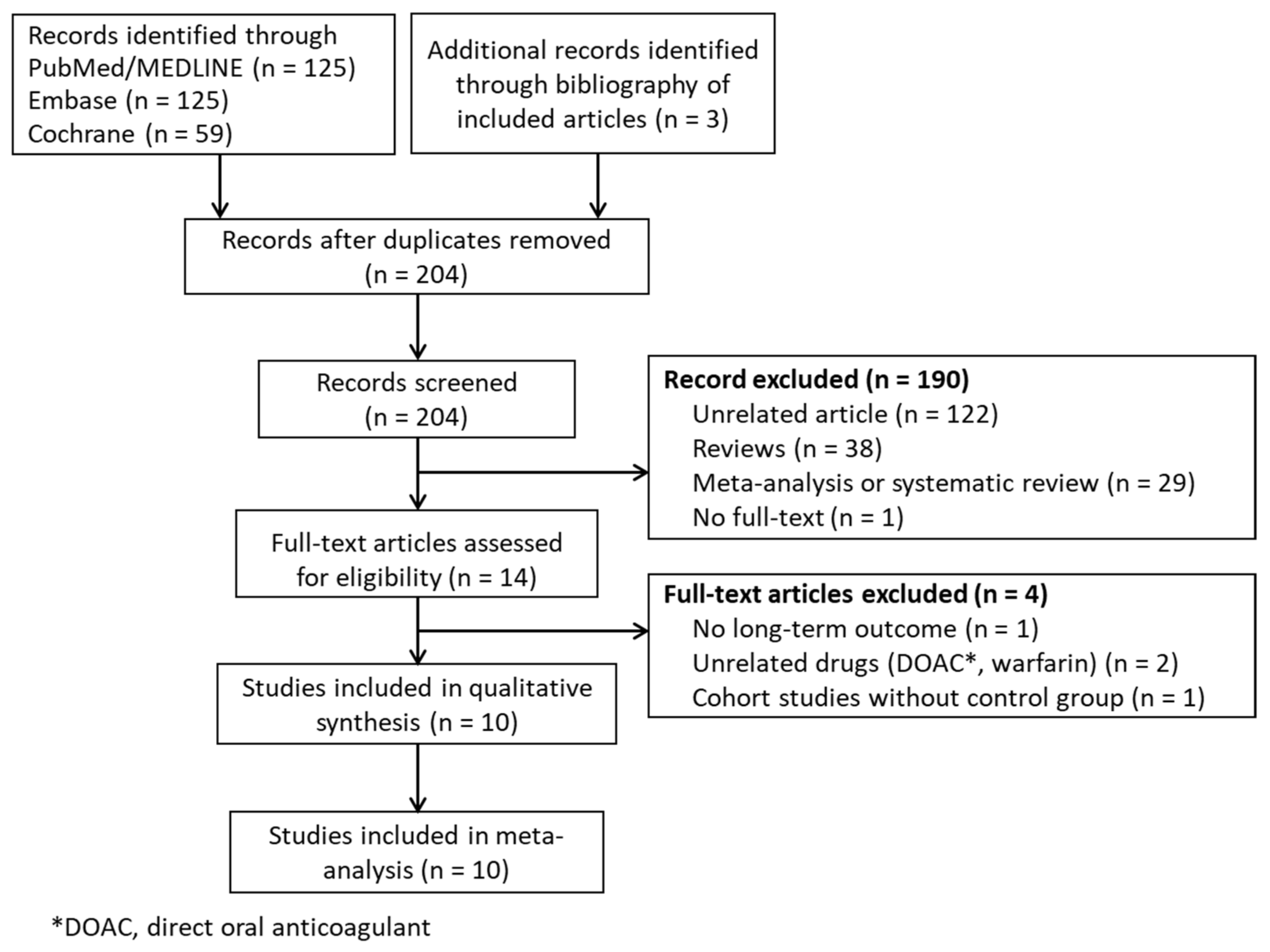
2.1. Search Sources and Strategy
2.2. Study Selection and Data Extraction
2.3. Outcomes
2.4. Assessment of Methodological Quality
2.5. Data Synthesis and Analysis
3. Results
3.1. Studies and Patient Characteristics
3.2. Risk of Bias
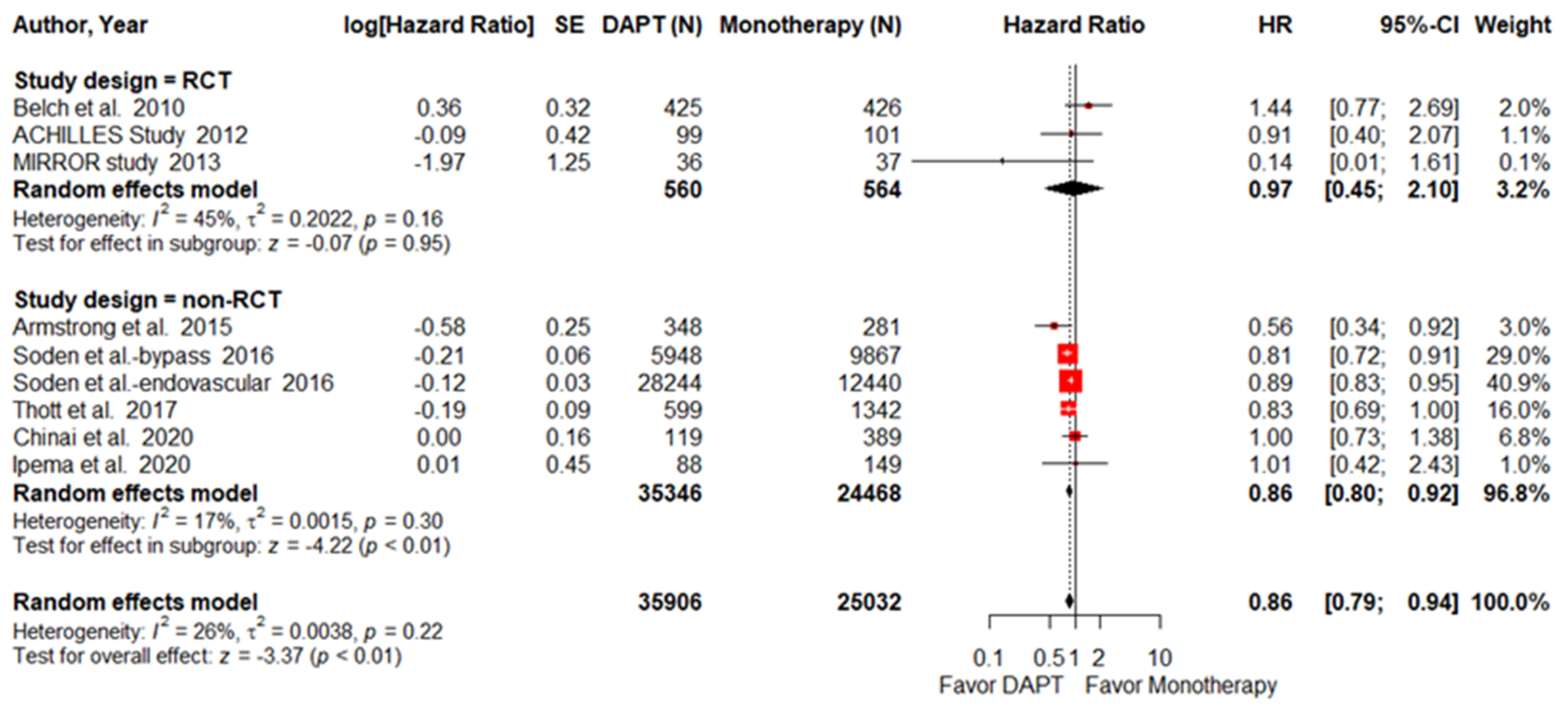
3.3. All-Cause Mortality
3.3.1. MACCEs
3.3.2. MI
3.3.3. Stroke
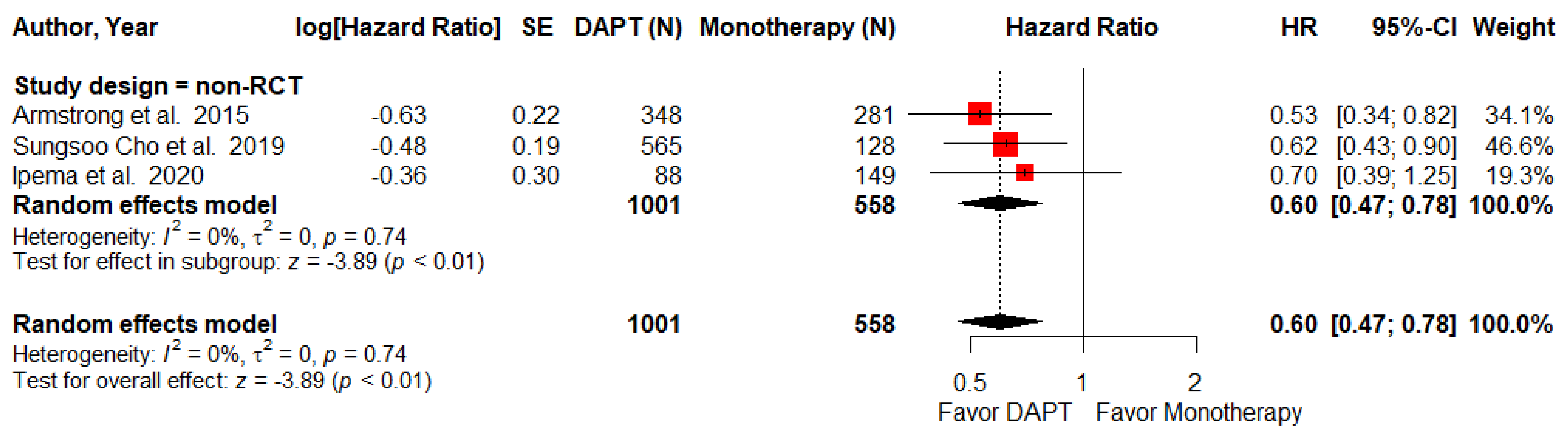
3.4. Major Adverse Limb Events
3.4.1. Major Amputation
3.4.2. Re-Intervention
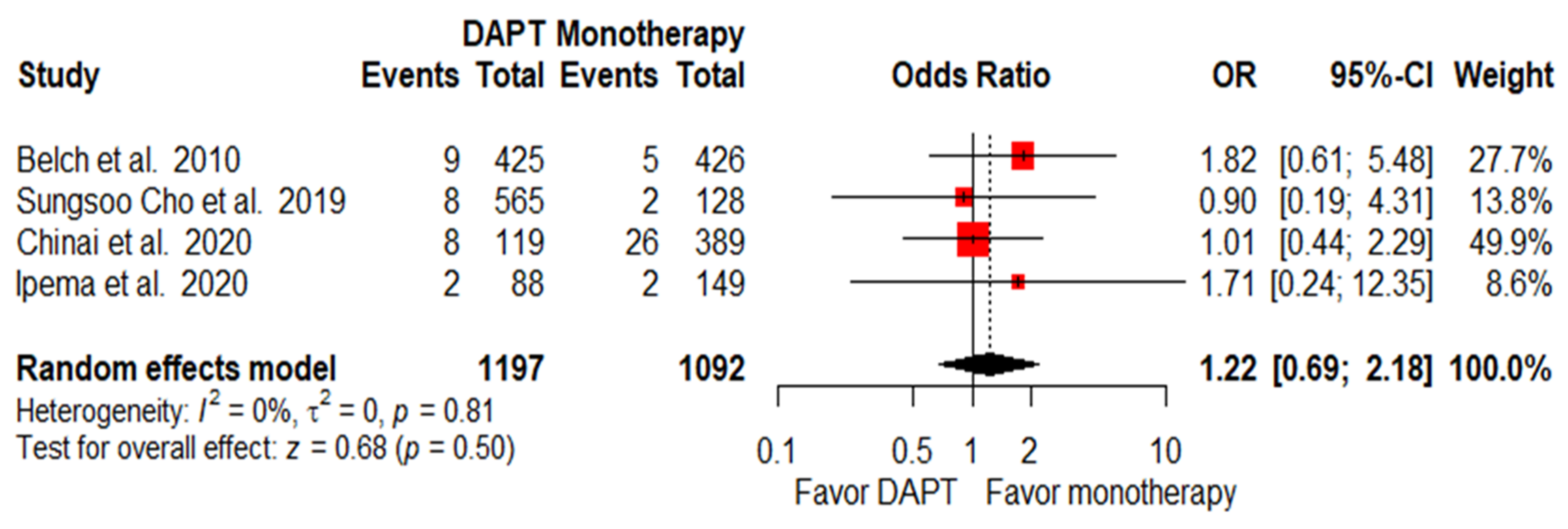
3.5. Bleeding Complications
4. Discussion
4.1. Controversy about DAPT on Reduction in MACCEs
4.2. DAPT on MALEs Reduction
4.3. Safety Concerns about DAPT
4.4. Protective Effects of DAPT on Different Revascularization Procedures
4.5. Duration of Antiplatelet Treatment
4.6. Novel Dual Pathway Regimen on PAD Patients
4.7. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACC | American college of cardiology |
| AHA | American heart association |
| AIOD | Aortoiliac occlusive disease |
| CI | Confidence intervals |
| CLI | Critical limb ischemia |
| CAD | Coronary artery disease |
| CVD | Cerebrovascular disease |
| DAPT | Dual antiplatelet therapy |
| DM | Diabetic mellitus |
| DOAC | Direct oral anticoagulant |
| ESC | European society of cardiology |
| ESVS | European society for vascular surgery |
| HR | Hazard ratio |
| IC | Intermittent claudication |
| MACCEs | Major adverse cardiac and cerebrovascular events |
| MALEs | Major adverse limb events |
| MI | Myocardial infarction |
| NRCTs | Nonrandomized controlled trials |
| OR | Odd ratio |
| PAD | Peripheral artery disease |
| PCI | Percutaneous coronary intervention |
| PSM | Propensity-score-weighted matching |
| RCTs | Randomized control trials |
| TLR | Target lesion revascularization |
References
- Fowkes, F.G.R.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.A.; Williams, L.J.; Mensah, G.A.; et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef]
- Malyar, N.; Fürstenberg, T.; Wellmann, J.; Meyborg, M.; Lüders, F.; Gebauer, K.; Bunzemeier, H.; Roeder, N.; Reinecke, H. Recent trends in morbidity and in-hospital outcomes of in-patients with peripheral arterial disease: A nationwide population-based analysis. Eur. Heart J. 2013, 34, 2706–2714. [Google Scholar] [CrossRef] [PubMed]
- Faxon, D.P.; Creager, M.A.; Smith, S.C.; Pasternak, R.C.; Olin, J.W.; Bettmann, M.A.; Criqui, M.H.; Milani, R.V.; Loscalzo, J.; Kaufman, J.A.; et al. Atherosclerotic Vascular Disease Conference. Circulation 2004, 109, 2595–2604. [Google Scholar] [CrossRef] [PubMed]
- Fowkes, F.G.R.; Aboyans, V.; Fowkes, F.J.I.; McDermott, M.M.; Sampson, U.K.A.; Criqui, M.H. Peripheral artery disease: Epidemiology and global perspectives. Nat. Rev. Cardiol. 2017, 14, 156–170. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Steg, P.G.; Ohman, E.M.; Hirsch, A.T.; Ikeda, Y.; Mas, J.L.; Goto, S.; Liau, C.S.; Richard, A.J.; Röther, J.; et al. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA 2006, 295, 180–189. [Google Scholar] [CrossRef]
- Criqui, M.H.; Aboyans, V. Epidemiology of Peripheral Artery Disease. Cir. Res. 2015, 116, 1509–1526. [Google Scholar] [CrossRef]
- Fowkes, F.G. Epidemiology of atherosclerotic arterial disease in the lower limbs. Eur. J. Vasc. Surg. 1988, 2, 283–291. [Google Scholar] [CrossRef]
- Pande, R.L.; Perlstein, T.S.; Beckman, J.A.; Creager, M.A. Secondary prevention and mortality in peripheral artery disease: National Health and Nutrition Examination Study, 1999 to 2004. Circulation 2011, 124, 17–23. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C. Guidelines: Editor’s choice: 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315. [Google Scholar]
- Mahoney, E.M.; Wang, K.; Keo, H.H.; Duval, S.; Smolderen, K.G.; Cohen, D.J.; Steg, G.; Bhatt, D.L.; Hirsch, A.T. Vascular hospitalization rates and costs in patients with peripheral artery disease in the United States. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 642–651. [Google Scholar] [CrossRef]
- Goodney, P.P.; Tarulli, M.; Faerber, A.E.; Schanzer, A.; Zwolak, R.M. Fifteen-year trends in lower limb amputation, revascularization, and preventive measures among medicare patients. JAMA Surg. 2015, 150, 84–86. [Google Scholar] [CrossRef] [PubMed]
- Steinhubl, S.R.; Berger, P.B.; Mann, J.T., 3rd; Fry, E.T.; DeLago, A.; Wilmer, C.; Topol, E.J.; for the CREDO Investigators. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: A randomized controlled trial. JAMA 2002, 288, 2411–2420. [Google Scholar] [CrossRef] [PubMed]
- Gerhard-Herman, M.D.; Gornik, H.L.; Barrett, C.; Barshes, N.R.; Corriere, M.A.; Drachman, D.E.; Fleisher, L.A.; Fowkes, F.G.; Hamburg, N.M.; Kinlay, S.; et al. 2016 AHA/ACC Guideline on the management of patients with lower extremity peripheral artery disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e726–e779. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.R.; Yusuf, S.; Peters, R.J.G.; Bertrand, M.E.; Lewis, B.S.; Natarajan, M.K.; Malmberg, K.; Rupprecht, H.-J.; Zhao, F.; Chrolavicius, S.; et al. Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: The PCI-CURE study. Lancet 2001, 358, 527–533. [Google Scholar] [CrossRef]
- Conte, M.S.; Pomposelli, F.B.; Clair, D.G.; Geraghty, P.J.; McKinsey, J.F.; Mills, J.L.; Moneta, G.L.; Murad, M.H.; Powell, R.J.; Reed, A.B.; et al. Society for Vascular Surgery practice guidelines for atherosclerotic occlusive disease of the lower extremities: Management of asymptomatic disease and claudication. J. Vasc. Surg. 2015, 61, 2s–41s. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The, P.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Investigators, T.G. An international randomized trial comparing four thrombolytic strategies for acute myocardial infarction. N. Engl. J. Med. 1993, 329, 673–682. [Google Scholar] [CrossRef]
- Schulman, S.; Kearon, C. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef] [PubMed]
- Tierney, J.F.; Stewart, L.A.; Ghersi, D.; Burdett, S.; Sydes, M.R. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007, 8, 16. [Google Scholar] [CrossRef] [PubMed]
- Belch, J.J.F.; Dormandy, J. Results of the randomized, placebo-controlled clopidogrel and acetylsalicylic acid in bypass surgery for peripheral arterial disease (CASPAR) trial. J. Vasc. Surg. 2010, 52, 825–833.e822. [Google Scholar] [CrossRef] [PubMed]
- Scheinert, D.; Katsanos, K.; Zeller, T.; Koppensteiner, R.; Commeau, P.; Bosiers, M.; Krankenberg, H.; Baumgartner, I.; Siablis, D.; Lammer, J.; et al. A prospective randomized multicenter comparison of balloon angioplasty and infrapopliteal stenting with the sirolimus-eluting stent in patients with ischemic peripheral arterial disease: 1-Year Results From the ACHILLES Trial. J. Am. Coll. Cardiol. 2012, 60, 2290–2295. [Google Scholar] [CrossRef]
- Strobl, F.F.; Brechtel, K.; Schmehl, J.; Zeller, T.; Reiser, M.F.; Claussen, C.D.; Tepe, G. Twelve-month results of a randomized trial comparing mono with dual antiplatelet therapy in endovascularly treated patients with peripheral artery disease. J. Endovasc. Ther. 2013, 20, 699–706. [Google Scholar] [CrossRef]
- Armstrong, E.J.; Anderson, D.R.; Yeo, K.-K.; Singh, G.D.; Bang, H.; Amsterdam, E.A.; Freischlag, J.A.; Laird, J.R. Association of dual-antiplatelet therapy with reduced major adverse cardiovascular events in patients with symptomatic peripheral arterial disease. J. Vasc. Surg. 2015, 62, 157–165.e151. [Google Scholar] [CrossRef]
- Soden, P.A.; Zettervall, S.L.; Ultee, K.H.; Landon, B.E.; O’Malley, A.J.; Goodney, P.P.; DeMartino, R.R.; Arya, S.; Schermerhorn, M.L. Dual antiplatelet therapy is associated with prolonged survival after lower extremity revascularization. J. Vasc. Surg. 2016, 64, 1633–1644.e1631. [Google Scholar] [CrossRef]
- Cho, S.; Lee, Y.-J.; Ko, Y.-G.; Kang, T.S.; Lim, S.-H.; Hong, S.-J.; Ahn, C.-M.; Kim, J.-S.; Kim, B.-K.; Choi, D.; et al. Optimal Strategy for Antiplatelet Therapy After Endovascular Revascularization for Lower Extremity Peripheral Artery Disease. JACC Cardiovascr. Interv. 2019, 12, 2359–2370. [Google Scholar] [CrossRef]
- Thott, O.; Granath, F.; Malmstedt, J.; Wahlgren, C.M. Editor’s Choice—Dual antiplatelet therapy improves outcome in diabetic patients undergoing endovascular femoropopliteal stenting for critical limb ischaemia. Eur. J. Vasc. Endovasc. Surg. 2017, 53, 403–410. [Google Scholar] [CrossRef]
- Chinai, N.; Ambler, G.K.; Wardle, B.G.; Locker, D.; Bosanquet, D.; Goyal, N.; Chick, C.; Hinchliffe, R.J.; Twine, C.P. Single versus dual antiplatelet therapy following peripheral arterial endovascular intervention for chronic limb threatening ischaemia: Retrospective cohort study. PLoS ONE 2020, 15, e0234271. [Google Scholar] [CrossRef]
- Ipema, J.; Welling, R.H.A.; Bakker, O.J.; Bokkers, R.P.H.; de Vries, J.P.M.; Ünlü, Ç. Short-term clinical outcomes of single versus dual antiplatelet therapy after infrainguinal endovascular treatment for peripheral arterial disease. J. Clin. Med. 2020, 9, 3515. [Google Scholar] [CrossRef] [PubMed]
- Belkin, N.; Stoecker, J.B.; Jackson, B.M.; Damrauer, S.M.; Glaser, J.; Kalapatapu, V.; Golden, M.A.; Wang, G.J. Effects of dual antiplatelet therapy on graft patency after lower extremity bypass. J. Vasc. Surg. 2021, 73, 930–939. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, R.B., Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]
- Navarese, E.P.; Wernly, B.; Lichtenauer, M.; Petrescu, A.M.; Kołodziejczak, M.; Lauten, A.; Frediani, L.; Veulemanns, V.; Wanha, W.; Wojakowski, W.; et al. Dual vs single antiplatelet therapy in patients with lower extremity peripheral artery disease—A meta-analysis. Int. J. Cardiol. 2018, 269, 292–297. [Google Scholar] [CrossRef]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [CrossRef]
- Hess Connie, N.; Wang Tracy, Y.; Weleski Fu, J.; Gundrum, J.; Allen LaPointe Nancy, M.; Rogers, R.K.; Hiatt William, R. Long-term outcomes and associations with major adverse limb events after peripheral artery revascularization. J. Am. Coll. Cardiol. 2020, 75, 498–508. [Google Scholar] [CrossRef]
- Anand Sonia, S.; Caron, F.; Eikelboom John, W.; Bosch, J.; Dyal, L.; Aboyans, V.; Abola Maria, T.; Branch Kelley, R.H.; Keltai, K.; Bhatt Deepak, L.; et al. Major adverse limb events and mortality in patients with peripheral artery disease. J. Am. Coll. Cardiol. 2018, 71, 2306–2315. [Google Scholar] [CrossRef]
- Singh, N.; Ding, L.; Magee, G.A.; Shavelle, D.M.; Kashyap, V.S.; Garg, P.K. Discharge prescription patterns for antiplatelet therapy following lower extremity peripheral vascular intervention. Circ. Cardiovasc. Interv. 2020, 13, e008791. [Google Scholar] [CrossRef]
- Beiswenger, A.C.; Jo, A.; Harth, K.; Kumins, N.H.; Shishehbor, M.H.; Kashyap, V.S. A systematic review of the efficacy of aspirin monotherapy versus other antiplatelet therapy regimens in peripheral arterial disease. J. Vasc. Surg. 2018, 67, 1922–1932.e1926. [Google Scholar] [CrossRef]
- Goodney, P.P.; Beck, A.W.; Nagle, J.; Welch, H.G.; Zwolak, R.M. National trends in lower extremity bypass surgery, endovascular interventions, and major amputations. J. Vasc. Surg. 2009, 50, 54–60. [Google Scholar] [CrossRef]
- Sachs, T.; Pomposelli, F.; Hamdan, A.; Wyers, M.; Schermerhorn, M. Trends in the national outcomes and costs for claudication and limb threatening ischemia: Angioplasty vs bypass graft. J. Vasc. Surg. 2011, 54, 1021–1031.e1021. [Google Scholar] [CrossRef] [PubMed]
- Efficacy of oral anticoagulants compared with aspirin after infrainguinal bypass surgery (The Dutch Bypass Oral Anticoagulants or Aspirin Study): A randomised trial. Lancet 2000, 355, 346–351. [CrossRef]
- Sarode, K.; Mohammad, A.; Das, S.; Vinas, A.; Banerjee, A.; Tsai, S.; Armstrong, E.J.; Shammas, N.W.; Klein, A.; Brilakis, E.S.; et al. Comparison of dual-antiplatelet therapy durations after endovascular revascularization of infrainguinal arteries. Ann. Vasc. Surg. 2015, 29, 1235–1244. [Google Scholar] [CrossRef] [PubMed]
- Kronlage, M.; Wassmann, M.; Vogel, B.; Müller, O.J.; Blessing, E.; Katus, H.; Erbel, C. Short vs prolonged dual antiplatelet treatment upon endovascular stenting of peripheral arteries. Drug Des. Dev. Ther. 2017, 11, 2937–2945. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Bates, E.R.; Bittl, J.A.; Brindis, R.G.; Fihn, S.D.; Fleisher, L.A.; Granger , C.B.; Lange, R.A.; Mack, M.J.; Mauri, L.; et al. 2016 ACC/AHA Guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease. J. Am. Coll. Cardiol. 2016, 68, 1082–1115. [Google Scholar] [CrossRef]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.-P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2018, 39, 213–260. [Google Scholar] [CrossRef]
- Khan, S.U.; Singh, M.; Valavoor, S.; Khan, M.U.; Lone, A.N.; Khan, M.Z.; Khan, M.S.; Mani, P.; Kapadia, S.R.; Michos, E.D.; et al. Dual Antiplatelet Therapy After Percutaneous Coronary Intervention and Drug-Eluting Stents. Circulation 2020, 142, 1425–1436. [Google Scholar] [CrossRef]
- Bonaca, M.P.; Bauersachs, R.M.; Anand, S.S.; Debus, E.S.; Nehler, M.R.; Patel, M.R.; Fanelli, F.; Capell, W.H.; Diao, L.; Jaeger, N.; et al. Rivaroxaban in peripheral artery disease after revascularization. N. Engl. J. Med. 2020, 382, 1994–2004. [Google Scholar] [CrossRef]
- Moll, F.; Baumgartner, I.; Jaff, M.; Nwachuku, C.; Tangelder, M.; Ansel, G.; Adams, G.; Zeller, T.; Rundback, J.; Grosso, M.; et al. Edoxaban plus aspirin vs dual antiplatelet therapy in endovascular treatment of patients with peripheral artery disease: Results of the ePAD Trial. J. Endovasc. Ther. 2018, 25, 158–168. [Google Scholar] [CrossRef]
- Ellis, K.J.; Stouffer, G.A.; McLeod, H.L.; Lee, C.R. Clopidogrel pharmacogenomics and risk of inadequate platelet inhibition: US FDA recommendations. Pharmacogenomics 2009, 10, 1799–1817. [Google Scholar] [CrossRef]
- Mega, J.L.; Simon, T.; Collet, J.P.; Anderson, J.L.; Antman, E.M.; Bliden, K.; Cannon, C.P.; Danchin, N.; Giusti, B.; Gurbel, P.; et al. Reduced-function CYP2C19 genotype and risk of adverse clinical outcomes among patients treated with clopidogrel predominantly for PCI: A meta-analysis. Jama 2010, 304, 1821–1830. [Google Scholar] [CrossRef] [PubMed]
- Yeh, C.H.; Chou, Y.J.; Tsai, T.H.; Hsu, P.W.; Li, C.H.; Chan, Y.H.; Tsai, S.F.; Ng, S.C.; Chou, K.M.; Lin, Y.C.; et al. Artificial-intelligence-assisted discovery of genetic factors for precision medicine of antiplatelet therapy in diabetic peripheral artery disease. Biomedicines 2022, 10, 116. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Type | Patients (n) | Setting | Intervention (%) | DAPT Therapy | DAPT Duration (Months) | Monotherapy | Follow-Up (Months) | Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Belch et al. 2010 [23] | Prospective multicenter RCT | 951 | Atherosclerotic PAD | Bypass surgery (100) | Asp and Clo | 6–24 | Aspirin | 6–24 | Graft occlusion, revascularization, amputation or death |
| ACHILLES study 2012 [24] | Prospective multicenter RCT | 200 | PAD, Rutherford class 3 to 5 | PTA only (50.5) or PTA plus stenting (49.5) | Asp and Clo or Ticl | 6 | Aspirin | 12 | Primary patency and binary restenosis |
| MIRROR study 2013 [25] | Prospective RCT | 80 | PAD, Rutherford class 3 to 5 | PTA only (37.5) or PTA plus stenting (62.5) | Asp and Clo | 6 | Aspirin | 12 | Platelet activation marker and all-cause mortality |
| Armstrong et al. 2015 [26] | PSM retrospective study | 629 | PAD, Rutherford class 1 to 6 | PTA only (80) | Asp and Clo (98.3%), Ticl (0.3%), or Pra (1.4%) | ≥6 | Asp | 36 | MACCEs |
| Soden et al. 2016 [27] | PSM retrospective study | 15,985 | PAD, Rutherford class 0 to 6 or ALI | Bypass surgery (100) | Asp and Clo, Pra, Ticl or Tica | ≥12 | Asp | 12–60 | All-cause mortality |
| Soden et al. 2016 [27] | PSM retrospective study | 40,684 | PAD, Rutherford class 0 to 6 or ALI | Endovascular (100) | Asp and Clo, Pra, Ticl or Tica | ≥12 | Asp | 12–60 | All-cause mortality |
| Thott et al. 2017 [29] | Retrospective study | 1941 | PAD, Rutherford class 4 to 6 | PTA only (58), PTA and stenting (33), and subintimal angioplasty (9) | Asp and Clo | ≥1 | Aspirin | 24 | Major amputation or mortality |
| Cho et al. 2019 [28] | PSM retrospective study | 693 | PAD, Rutherford class 1 to 6 | Endovascular (100) | Asp and Clo | 1–12 | Asp or Clo | 40 | Major amputation or mortality |
| Chinai et al. 2020 [30] | Retrospective study | 508 | PAD, Rutherford class 4 to 6 | PTA only (61.2) or PTA plus stenting (38.8) | Asp and Clo (95.0%), Pra (4.2%), or Tica (0.8%) | 3 | Asp or Clo | 36 | Amputation-free survival |
| Ipema et al. 2020 [31] | Retrospective study | 237 | PAD, Rutherford class 1 to 6 | PTA only (45.3) or PTA plus stenting (54.7) | Asp and Clo | 3–12 | Asp or Clo | 12 | MALEs |
| Belkin et al. 2021 [32] | Retrospective study | 13,020 | PAD, Rutherford class 0 to 6 | Bypass surgery (100) | Asp and Clo (97.7%), Pra (1%), Tica (0.8%), or other (0.5%) | 12 | Asp | 9–21 | Patency of bypass graft |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, S.-Y.; Li, Y.-S.; Lee, C.-H.; Cha, S.-W.; Wang, Y.-C.; Su, T.-W.; Yu, S.-Y.; Yeh, C.-H. Mono or Dual Antiplatelet Therapy for Treating Patients with Peripheral Artery Disease after Lower Extremity Revascularization: A Systematic Review and Meta-Analysis. Pharmaceuticals 2022, 15, 596. https://doi.org/10.3390/ph15050596
Tsai S-Y, Li Y-S, Lee C-H, Cha S-W, Wang Y-C, Su T-W, Yu S-Y, Yeh C-H. Mono or Dual Antiplatelet Therapy for Treating Patients with Peripheral Artery Disease after Lower Extremity Revascularization: A Systematic Review and Meta-Analysis. Pharmaceuticals. 2022; 15(5):596. https://doi.org/10.3390/ph15050596
Chicago/Turabian StyleTsai, Shang-Yu, Ying-Sheng Li, Che-Hsiung Lee, Shion-Wei Cha, Yao-Chang Wang, Ta-Wei Su, Sheng-Yueh Yu, and Chi-Hsiao Yeh. 2022. "Mono or Dual Antiplatelet Therapy for Treating Patients with Peripheral Artery Disease after Lower Extremity Revascularization: A Systematic Review and Meta-Analysis" Pharmaceuticals 15, no. 5: 596. https://doi.org/10.3390/ph15050596
APA StyleTsai, S.-Y., Li, Y.-S., Lee, C.-H., Cha, S.-W., Wang, Y.-C., Su, T.-W., Yu, S.-Y., & Yeh, C.-H. (2022). Mono or Dual Antiplatelet Therapy for Treating Patients with Peripheral Artery Disease after Lower Extremity Revascularization: A Systematic Review and Meta-Analysis. Pharmaceuticals, 15(5), 596. https://doi.org/10.3390/ph15050596