
Analyzing the Difference in the Length of Stay (LOS) in Moderate to Severe COVID-19 Patients Receiving Hydroxychloroquine or Favipiravir

 ,
,  , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Results
3. Discussion
4. Methodology
4.1. Study Design and Setting
4.2. Selection Criteria
4.3. Definitions
4.4. Study Outcomes
4.5. Baseline Information Collection
4.6. Sample Size Calculation and Statistical Analysis
4.7. Software Used
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Coronavirus Disease (COVID-19) Situation Report; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 4 April 2022).
- Alotaibi, M.; Ali, A.; Bakhshwin, D.; Alatawi, Y.; Alotaibi, S.; Alhifany, A.; Alharthi, B.; Alharthi, N.; Alyazidi, A.; Alharthi, Y.; et al. Effectiveness and Safety of Favipiravir Compared to Hydroxychloroquine for Management of COVID-19: A Retrospective Study. Int. J. Gen. Med. 2021, 14, 5597–5606. [Google Scholar] [CrossRef] [PubMed]
- Costanzo, M.; De Giglio, M.A.R.; Roviello, G.N. SARS-CoV-2: Recent Reports on Antiviral Therapies Based on Lopinavir/Ritonavir, Darunavir/Umifenovir, Hydroxychloroquine, Remdesivir, Favipiravir and other Drugs for the Treatment of the New Coronavirus. Curr. Med. Chem. 2020, 27, 4536–4541. [Google Scholar] [CrossRef]
- Group, T.R.C. Dexamethasone in hospitalized patients with COVID-19—Preliminary report. N. Engl. J. Med. 2020, 384, 693–704. [Google Scholar]
- Wei, P.F. Diagnosis and Treatment Protocol for Novel Coronavirus Pneumonia (Trial Version 7). Chin. Med. J. 2020, 133, 1087–1095. [Google Scholar] [CrossRef]
- Udwadia, Z.F.; Singh, P.; Barkate, H.; Patil, S.; Rangwala, S.; Pendse, A.; Kadam, J.; Wu, W.; Caracta, C.F.; Tandon, M. Efficacy and safety of favipiravir, an oral RNA-dependent RNA polymerase inhibitor, in mild-to-moderate COVID-19: A randomized, comparative, open-label, multicenter, phase 3 clinical trial. Int. J. Infect. Dis. 2020, 103, 62–71. [Google Scholar] [CrossRef]
- Saudi Arabia Ministry of Health (MOH). Saudi MoH Protocol for Patients Suspected of/Confirmed with COVID-19. Available online: https://www.moh.gov.sa/Ministry/MediaCenter/Publications/Documents/MOH-therapeutic-protocol-for-COVID-19.pdf (accessed on 2 September 2020).
- Saudi Arabia Ministry of Health (MOH). Coronavirus Disease COVID-19 Guidelines, v1.3. Available online: https://www.moh.gov.sa/Ministry/MediaCenter/Publications/Documents/Coronavirus-Disease-2019-Guidelines-v1.2.pdf (accessed on 2 September 2020).
- Kohl, M. Package MKpower: Wilcoxon Rank Sum and Signed Rank Tests. 2020. Available online: https://cran.r-project.org/web/packages/MKpower/vignettes/MKpower.html#wilcoxon-rank-sum-and-signed-rank-tests (accessed on 19 July 2022).
- Scheff, S. Fundamental Statistical Principles for the Neurobiologist, Chapter 8—Nonparametric Statistics; Academic Press: Cambridge, MA, USA, 2016. [Google Scholar] [CrossRef]
- Austin, P.C. A Tutorial and Case Study in Propensity Score Analysis: An Application to Estimating the Effect of In-Hospital Smoking Cessation Counseling on Mortality. Multivar. Behav. Res. 2011, 46, 119–151. [Google Scholar] [CrossRef]
- Wickham, H. ggplot2: Create Elegant Data Visualisations Using the Grammar of Graphics. 2020. Available online: https://cran.r-project.org/web/packages/ggplot2/index.html (accessed on 19 July 2022).
- Pishgar, F. MatchThem: Matching and Weighting Multiply Imputed Datasets. 2020. Available online: https://cran.r-project.org/web/packages/MatchThem/index.html (accessed on 19 July 2022).
- Greife, N. Cobalt: Covariate Balance Tables and Plots. 2020. Available online: https://cran.r-project.org/web/packages/cobalt/index.html (accessed on 19 July 2022).
- Buuren, S.V. Mice: Multivariate Imputation by Chained Equations. 2020. Available online: https://cran.r-project.org/web/packages/mice/index.html (accessed on 19 July 2022).
- Therneau, T. Survival: Survival Analysis. 2020. Available online: https://cran.r-project.org/web/packages/survival/index.html (accessed on 19 July 2022).
- Eroglu, A.; Kartal, S.; Kongur, E. Comparison of the intensive care unit admission rate and mortalities of COVID-19 patients who received Hydroxychloroquine and Favipiravir in the ward. J. Anesth. Crit. Care Open Access 2022, 14, 40–43. [Google Scholar] [CrossRef]
- Turan, D.B.; Menteş, M.; Özel, Y.; Şerefhanoğlu, K.; Aydoğan, B.; İbil, N.; Güneşdoğdu, F.; Orucova, H.M.; Saltürk, C.; Çelik, H. The effect of favipiravir versus hydroxychloroquine on clinical and laboratory findings in COVID-19 in healthcare workers. Braz. J. Infect. Dis. 2022, 26, 102328. [Google Scholar] [CrossRef]
- Abd-Elsalam, S.; Esmail, E.S.; Khalaf, M.; Abdo, E.F.; Medhat, M.A.; Abd El Ghafar, M.S.; Ahmed, O.A.; Soliman, S.; Serangawy, G.N.; Alboraie, M. Hydroxychloroquine in the treatment of COVID-19: A multicenter randomized controlled study. Am. J. Trop. Med. Hyg. 2020, 103, 1635–1639. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ader, F.; Peiffer-Smadja, N.; Poissy, J.; Bouscambert-Duchamp, M.; Belhadi, D.; Diallo, A.; Delmas, C.; Saillard, J.; Dechanet, A.; Mercier, N.; et al. An open-label randomized controlled trial of the effect of lopinavir/ritonavir, lopinavir/ritonavir plus IFN-β-1a and hydroxychloroquine in hospitalized patients with COVID-19. Clin. Microbiol. Infect. 2021, 27, 1826–1837. [Google Scholar] [CrossRef] [PubMed]
- Akbari, A.; Razmi, M.; Sedaghat, A.; Dana, S.M.M.A.; Amiri, M.; Halvani, A.M.; Yazdani, S.; Sahab-Negah, S. Comparative effectiveness of pharmacological interventions on mortality and the average length of hospital stay of patients with COVID-19: A systematic review and meta-analysis of randomized controlled trials. Expert Rev. Anti-Infect. Ther. 2021, 20, 585–609. [Google Scholar] [CrossRef] [PubMed]
- Alamer, A.; Alrashed, A.A.; Alfaifi, M.; Alosaimi, B.; AlHassar, F.; Almutairi, M.M.; Howaidi, J.; Almutairi, W.; Mohzari, Y.; Sulaiman, T.; et al. Effectiveness and safety of favipiravir compared to supportive care in moderately to critically ill COVID-19 patients: A retrospective study with propensity score matching sensitivity analysis. Curr. Med. Res. Opin. 2021, 37, 1085–1097. [Google Scholar] [CrossRef]
- Membrillo, F.J.; Ramírez-Olivencia, G.; Estébanez, M.; de Dios, B.; Herrero, M.D.; Mata, T.; Borobia, A.M.; Gutiérrez, C.; Simón, M.; Ochoa, A.; et al. Early hydroxychloroquine is associated with an increase of survival in COVID-19 patients: An observational study. Preprints 2020, 2020050057. [Google Scholar] [CrossRef]
- Mahévas, M.; Tran, V.T.; Roumier, M.; Chabrol, A.; Paule, R.; Guillaud, C.; Gallien, S.; Lepeule, R.; Szwebel, T.A.; Lescure, X.; et al. No evidence of clinical efficacy of hydroxychloroquine in patients hospitalised for COVID-19 infection and requiring oxygen: Results of a study using routinely collected data to emulate a target trial. MedRxiv 2020. [Google Scholar] [CrossRef]
- Geleris, J.; Sun, Y.; Platt, J.; Zucker, J.; Baldwin, M.; Hripcsak, G.; Labella, A.; Manson, D.K.; Kubin, C.; Barr, R.G.; et al. Observational study of hydroxychloroquine in hospitalized patients with COVID-19. N. Engl. J. Med. 2020, 382, 2411–2418. [Google Scholar] [CrossRef]
- Borba, M.G.S.; Val, F.F.A.; Sampaio, V.S.; Alexandre, M.A.A.; Melo, G.C.; Brito, M.; Mourão, M.P.G.; Brito-Sousa, J.D.; Baía-da-Silva, D.; Guerra, M.V.F.; et al. Chloroquine diphosphate in two different dosages as adjunctive therapy of hospitalized patients with severe respiratory syndrome in the context of coronavirus (SARS-CoV-2) infection: Preliminary safety results of a randomized, double-blinded, phase IIb clinical trial (CloroCOVID-19 Study). MedRxiv 2020. [Google Scholar] [CrossRef]
- Torjesen, I. COVID-19: Hydroxychloroquine does not benefit hospitalised patients, UK trial finds. BMJ 2020, 369, m2263. [Google Scholar] [CrossRef]
- Extance, A. COVID-19: What is the evidence for the antiviral Paxlovid? BMJ 2022, 37, o10377. [Google Scholar] [CrossRef]
- Gao, J.; Tian, Z.; Yang, X. Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies. Biosci. Trends 2020, 14, 72–73. [Google Scholar] [CrossRef]
- Gautret, P.; Lagier, J.C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 56, 105949. [Google Scholar] [CrossRef] [PubMed]
- Pilkington, V.; Pepperrell, T.; Hill, A. A review of the safety of favipiravir—A potential treatment in the COVID-19 pandemic? J. Virus Erad. 2020, 6, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Yan, V.C.; Muller, F.L. Why Remdesivir Failed: Preclinical Assumptions Overestimate the Clinical Efficacy of Remdesivir for COVID-19 and Ebola. Antimicrob. Agents Chemother. 2021, 65, e0111721. [Google Scholar] [CrossRef] [PubMed]
- Guo, A.; Lu, J.; Tan, H.; Kuang, Z.; Luo, Y.; Yang, T.; Xu, J.; Yu, J.; Wen, C.; Shen, A. Risk factors on admission associated with hospital length of stay in patients with COVID-19: A retrospective cohort study. Sci. Rep. 2021, 11, 7310. [Google Scholar] [CrossRef]
- Patino, C.M.; Ferreira, J.C. Meeting the assumptions of statistical tests: An important and often forgotten step to reporting valid results. J. Bras. Pneumol. 2018, 44, 353. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, R.; Kiers, H.; Johnson, A. Are Assumptions of Well-Known Statistical Techniques Checked, and Why (Not)? Front. Psychol. 2012, 3, 137. [Google Scholar] [CrossRef]
- Kim, A.H.; Sparks, J.A.; Liew, J.W.; Putman, M.S.; Berenbaum, F.; Duarte-García, A.; Graef, E.R.; Korsten, P.; Sattui, S.E.; Sirotich, E.; et al. A Rush to Judgment? Rapid Reporting and Dissemination of Results and Its Consequences Regarding the Use of Hydroxychloroquine for COVID-19. Ann. Intern. Med. 2020, 172, 819–821. [Google Scholar] [CrossRef]
- Qualls, M.; Pallin, D.J.; Schuur, J.D. Parametric Versus Nonparametric Statistical Tests: The Length of Stay Example. Acad. Emerg. Med. 2010, 17, 1113–1121. [Google Scholar] [CrossRef]
- Chazard, E.; Ficheur, G.; Beuscart, J.-B.; Preda, C. How to Compare the Length of Stay of Two Samples of Inpatients? A Simulation Study to Compare Type I and Type II Errors of 12 Statistical Tests. Value Health 2017, 20, 992–998. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 200) | HCQ (n = 83) | FPV (n = 117) | p-Value | Unadjusted Absolute SMD | HCQ (n = 37) | FPV (n = 37) | p-Value | Adjusted SMD |
|---|---|---|---|---|---|---|---|---|---|
| Age (years), mean (SD) | 56.95 (16.9) | 49.48 (15.46) | 62.25 (15.9) | <0.001 | 0.8872 | 54.08 (17.49) | 57.38 (16.22) | 0.403 | 0.188 |
| Male, n (%) | 130 (65.0) | 59 (71.1) | 71 (60.7) | 0.171 | 26 (70.3) | 27 (73.0) | 1.000 | 0.0417 | |
| Saudi nationality, n (%) | 125 (62.5) | 30 (36.1) | 95 (81.2) | <0.001 | 0.4505 | 21 (56.8) | 22 (59.5) | 1.000 | 0.0487 |
| Ethnicity, n(%) a | <0.001 | NA | NA | NA | |||||
| Middle Eastern | 136 (68.0) | 37 (44.6) | 99 (84.6) | 25 (67.6) | 25 (67.6) | ||||
| African | 19 (9.5) | 15 (18.1) | 4 (3.4) | 5 (13.5) | 3 (8.1) | ||||
| South/Southeast Asia | 43 (21.5) | 29 (34.9) | 14 (12.0) | 7 (18.9) | 9 (24.3) | ||||
| Central Asia | 1 (0.5) | 1 (1.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||||
| Unknown | 1 (0.5) | 1 (1.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||||
| BMI (kg/m2) | 29.40 (5.2) | 30.2 (7.1) | 28.83 (3.1) | 0.065 | 0.3039 | 28.89 (4.20) | 28.58 (2.91) | 0.717 | 0.0650 |
| Severe WHO classification, n (%) | 27 (16.1) | 14 (27.5) | 13 (11.1) | 0.015 | 0.1009 | 5 (13.5) | 4 (10.8) | 1.000 | 0.0208 |
| Steroid, n (%) | 38 (19.0) | 6 (7.2) | 32 (27.4) | 0.001 | 0.2012 | 4 (10.8) | 7 (18.9) | 0.513 | 0.0587 |
| Diabetes, n (%) | 69 (34.5) | 34 (41.0) | 35 (29.9) | 0.142 | 0.1105 | 8 (21.6) | 9 (24.3) | 1.000 | 0.0374 |
| Hypertension, n (%) | 82 (41.0) | 33 (39.8) | 49 (41.9) | 0.877 | 0.0212 | 14 (37.8) | 12 (32.4) | 0.808 | 0.0529 |
| Cardiovascular disease, n (%) | 10 (5.0) | 8 (9.6) | 2 (1.7) | 0.027 | 0.0793 | 1 (2.7) | 2 (5.4) | 1.000 | 0.0105 |
| Asthma n (%) | 21 (10.5) | 16 (19.3) | 5 (4.3) | <0.001 | 0.1500 | 5 (13.5) | 4 (10.8) | 1.000 | 0.0365 |
| Chronic kidney disease, n (%) | 5 (2.5) | 5 (6.0) | 0 (0.0) | 0.026 | 0.0602 | 0 (0.0) | 0 (0.0) | 1.000 | 0.0000 |
| Matched Sample | HCQ (n = 37) | FPV (n = 37) | p-Value |
|---|---|---|---|
| Outcome | |||
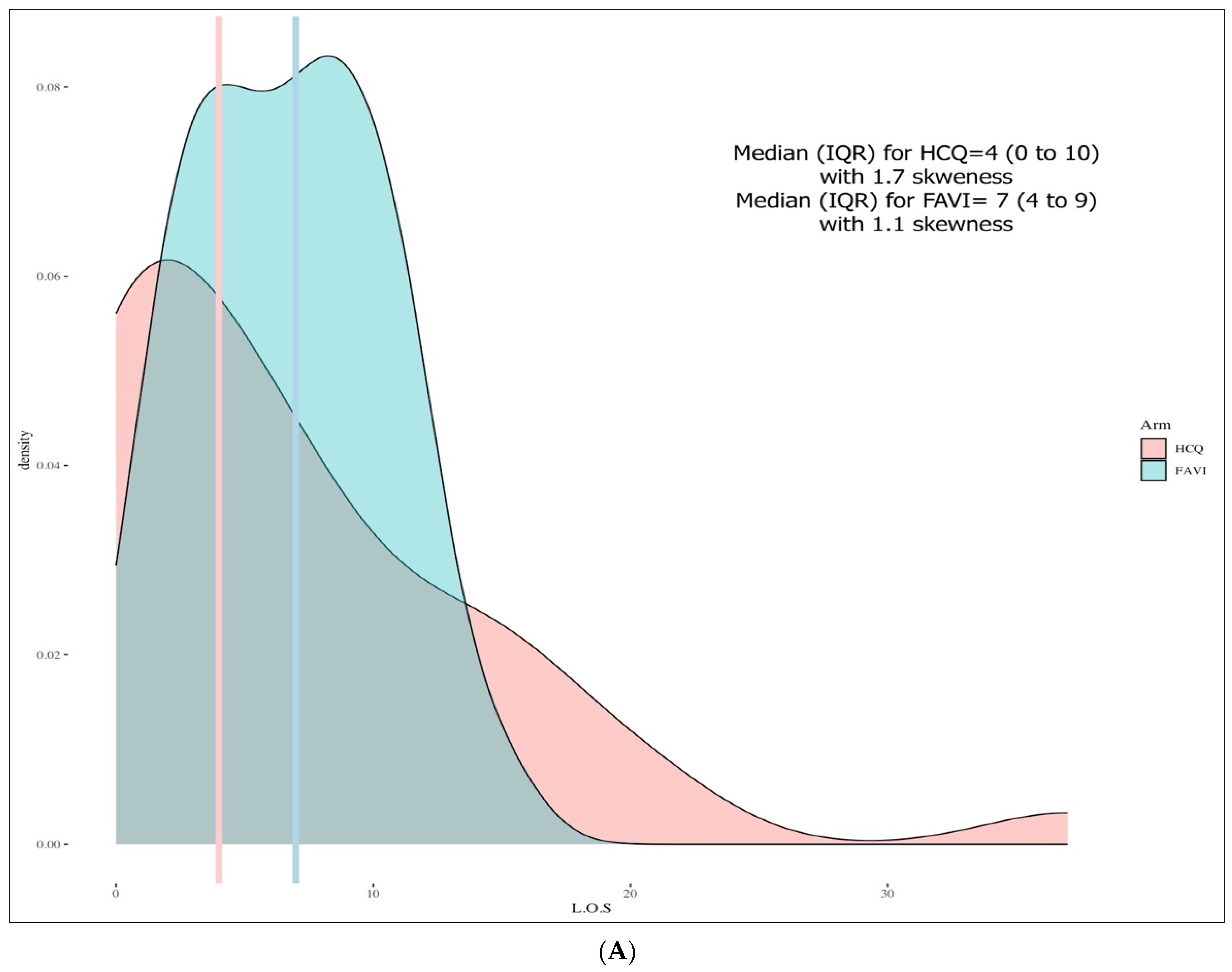
| LOS (days), median (IQR) a | 4 (0 to 10) | 7 (4 to 9) | p = 0.629 |
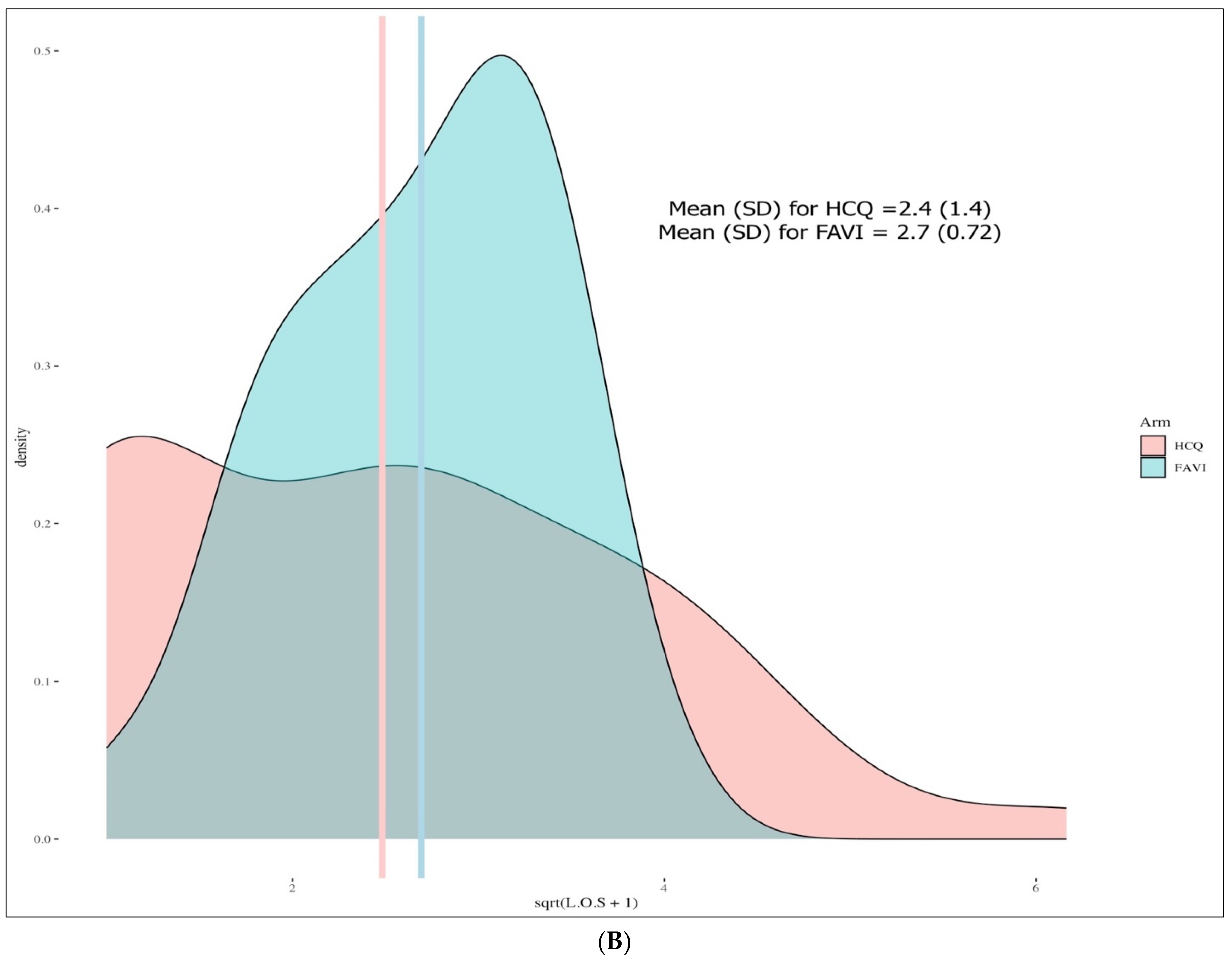
| Transformed LOS (days), mean (SD) b | 2.4(1.4) | 2.7 (0.72) | p = 0.391 |
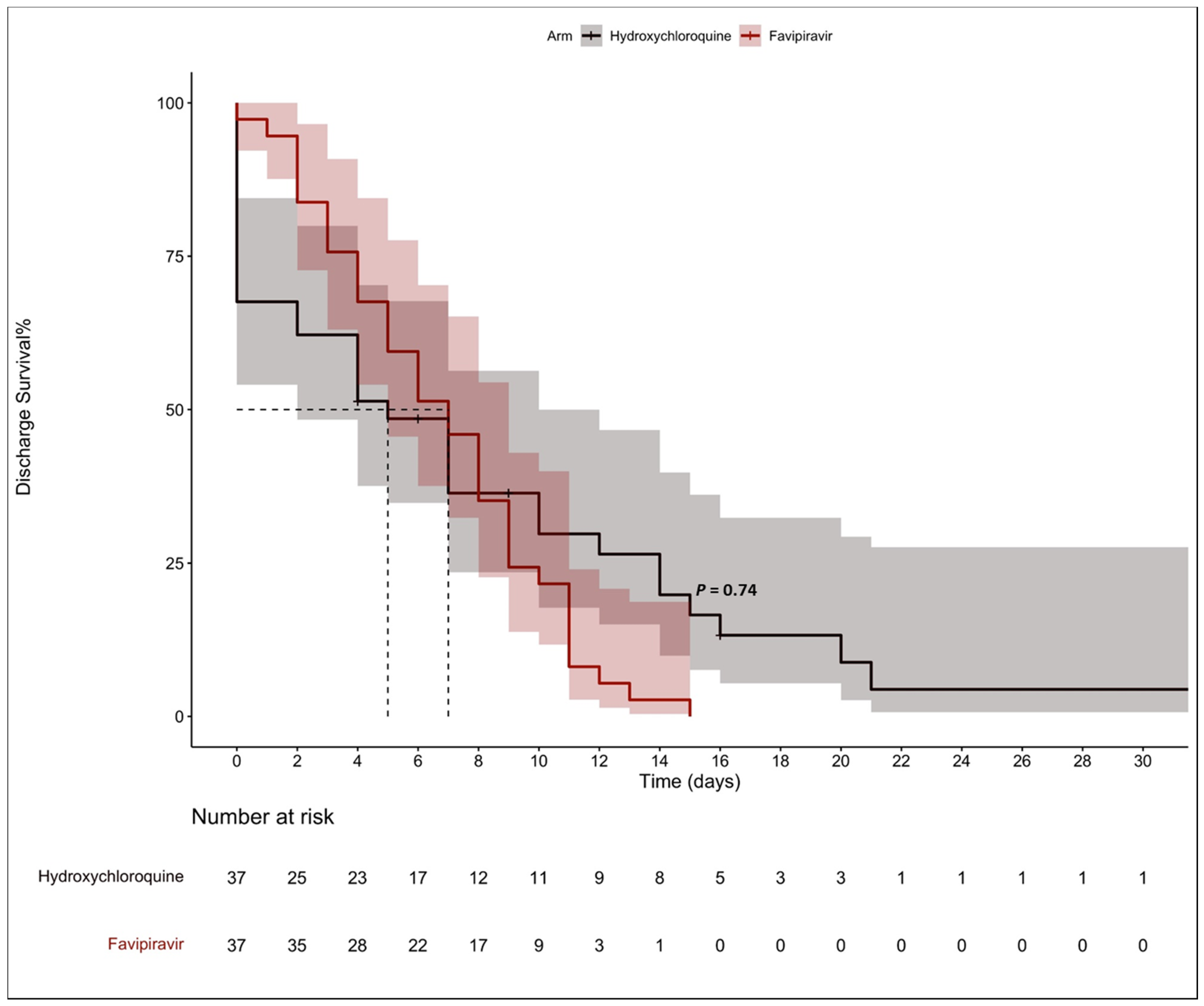
| Median time to discharge (95% CI) c | 5 (2 to 10) | 7 (5 to 10) | p = 0.740 |
| Death, n(%) d | 2 (5.4) | 0 (0.0) | p = 0.493 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alosaimi, B.; Alshanbari, H.M.; Alturaiqy, M.; AlRawi, H.Z.; Alamri, S.; Albujaidy, A.; Bin Sabaan, A.; Alrashed, A.A.; Alamer, A.; Alghofaili, F.; et al. Analyzing the Difference in the Length of Stay (LOS) in Moderate to Severe COVID-19 Patients Receiving Hydroxychloroquine or Favipiravir. Pharmaceuticals 2022, 15, 1456. https://doi.org/10.3390/ph15121456
Alosaimi B, Alshanbari HM, Alturaiqy M, AlRawi HZ, Alamri S, Albujaidy A, Bin Sabaan A, Alrashed AA, Alamer A, Alghofaili F, et al. Analyzing the Difference in the Length of Stay (LOS) in Moderate to Severe COVID-19 Patients Receiving Hydroxychloroquine or Favipiravir. Pharmaceuticals. 2022; 15(12):1456. https://doi.org/10.3390/ph15121456
Chicago/Turabian StyleAlosaimi, Bandar, Huda M. Alshanbari, Muath Alturaiqy, Halah Z. AlRawi, Saad Alamri, Asma Albujaidy, Aljawharah Bin Sabaan, Ahmed A. Alrashed, Ahmad Alamer, Fayez Alghofaili, and et al. 2022. "Analyzing the Difference in the Length of Stay (LOS) in Moderate to Severe COVID-19 Patients Receiving Hydroxychloroquine or Favipiravir" Pharmaceuticals 15, no. 12: 1456. https://doi.org/10.3390/ph15121456
APA StyleAlosaimi, B., Alshanbari, H. M., Alturaiqy, M., AlRawi, H. Z., Alamri, S., Albujaidy, A., Bin Sabaan, A., Alrashed, A. A., Alamer, A., Alghofaili, F., Al-Duraymih, K., Alshalani, A. J., & Alturaiki, W. (2022). Analyzing the Difference in the Length of Stay (LOS) in Moderate to Severe COVID-19 Patients Receiving Hydroxychloroquine or Favipiravir. Pharmaceuticals, 15(12), 1456. https://doi.org/10.3390/ph15121456