
Development of Capsaicin-Containing Analgesic Silicone-Based Transdermal Patches

 , ,
, ,
Abstract

1. Introduction
2. Results
2.1. In Vitro Experiments
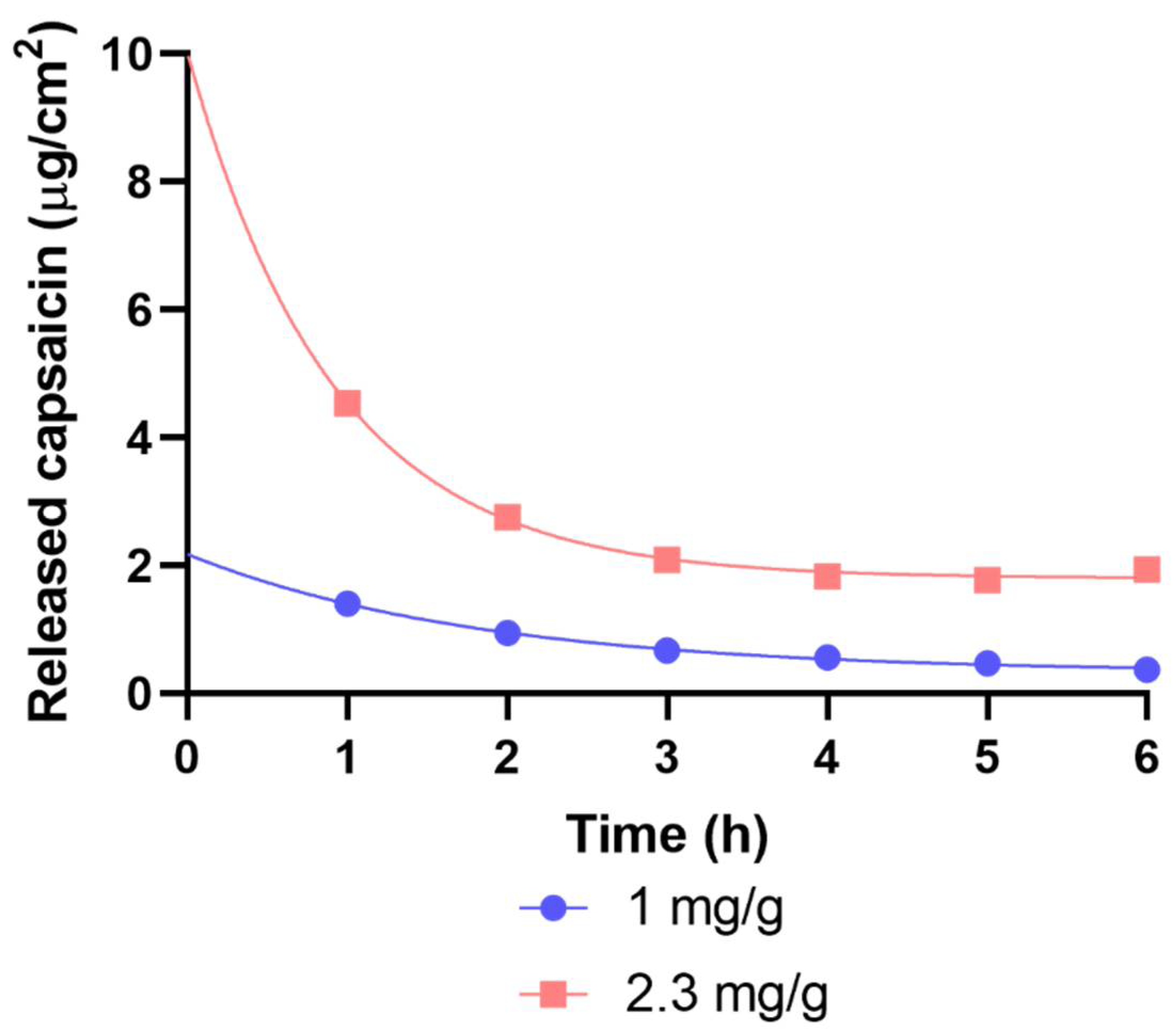
2.1.1. Drug Release and Permeation Investigated with Franz Diffusion Cell
2.1.2. Results of Drug Release with Flow-Through Cell
2.1.3. Results of Raman Spectroscopy
2.2. Results of In Vivo Experiments
2.2.1. The Capsaicin-Containing Dermal Patch Alleviates Heat Hyperalgesia
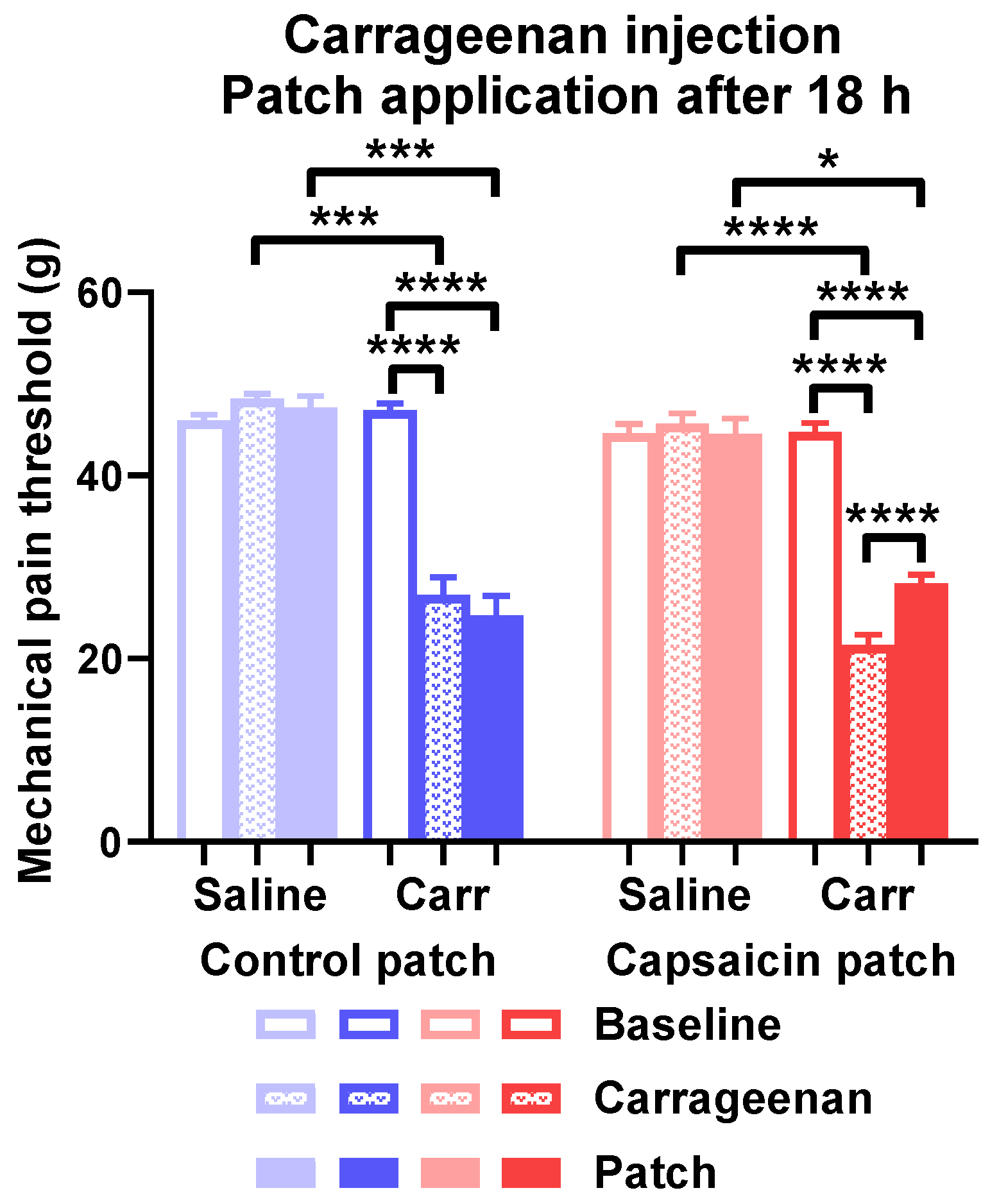
2.2.2. The Capsaicin-Containing Dermal Patch Mitigates Carrageenan-Evoked Mechanical Hyperalgesia
3. Discussion
4. Materials and Methods
4.1. Chemicals
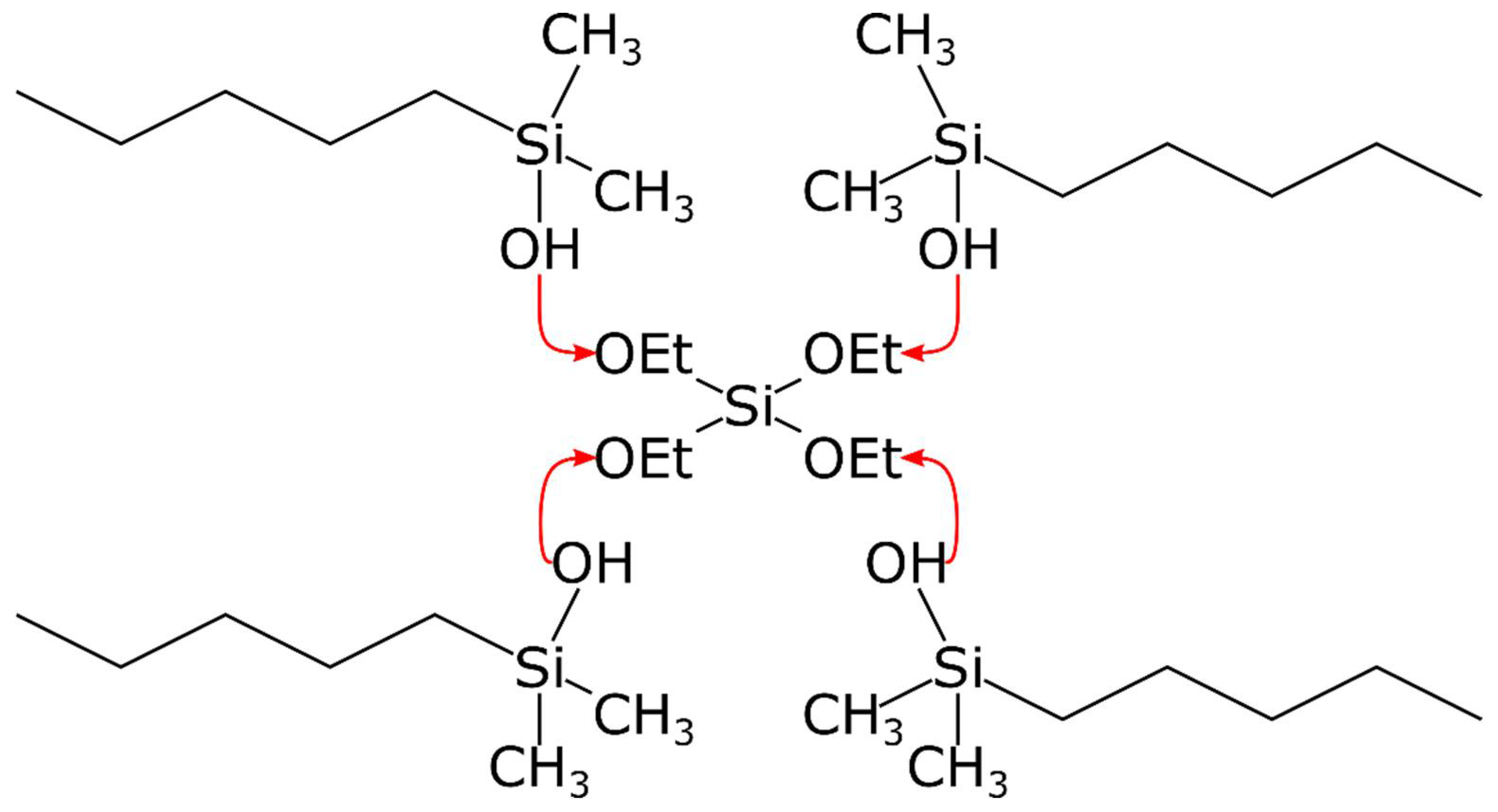
4.2. Production of Capsaicin-Containing Transdermal Patches
4.3. Measurement of the In Vitro Release of Capsaicin-Containing Transdermal Patches
4.3.1. Investigation of Drug Release and Permeation with Franz Diffusion Cell
4.3.2. Mathematical Evaluation
4.3.3. Flow-Through Cell
4.4. Investigation of Skin Permeation with Raman Microscopy
4.5. In Vitro Measurement
4.5.1. Animals
4.5.2. Surgical Incision of the Hind Paw
4.5.3. Carrageenan-Induced Paw Inflammation
4.5.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Izgelov, D.; Davidson, E.; Barasch, D.; Regev, A.; Domb, A.J.; Hoffman, A. Pharmacokinetic Investigation of Synthetic Cannabidiol Oral Formulations in Healthy Volunteers. Eur. J. Pharm. Biopharm. 2020, 154, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Tanner, T.; Marks, R. Delivering Drugs by the Transdermal Route: Review and Comment. Ski. Res. Technol. 2008, 14, 249–260. [Google Scholar] [CrossRef]
- Pastore, M.N.; Kalia, Y.N.; Horstmann, M.; Roberts, M.S. Transdermal Patches: History, Development and Pharmacology: History of Transdermal Patches. Br. J. Pharmacol. 2015, 172, 2179–2209. [Google Scholar] [CrossRef] [PubMed]
- Mojsiewicz-Pieńkowska, K.; Jamrógiewicz, M.; Zebrowska, M.; Sznitowska, M.; Centkowska, K. Technology of an Adhesive Silicone Film as Drug Carrier in Transdermal Therapy. I: Analytical Methods Used for Characterization and Design of the Universal Elastomer Layers. J. Pharm. Biomed. Anal. 2011, 56, 131–138. [Google Scholar] [CrossRef]
- Tomanek, A. Silicone und Technik; Hanser, Carl: München, Germany, 1990; ISBN 978-3-446-16032-3. [Google Scholar]
- Deal, C.L.; Schnitzer, T.J.; Lipstein, E.; Seibold, J.R.; Stevens, R.M.; Levy, M.D.; Albert, D.; Renold, F. Treatment of Arthritis with Topical Capsaicin: A Double-Blind Trial. Clin. Ther. 1991, 13, 383–395. [Google Scholar]
- Cameron, M.; Gagnier, J.J.; Little, C.V.; Parsons, T.J.; Blümle, A.; Chrubasik, S. Evidence of Effectiveness of Herbal Medicinal Products in the Treatment of Arthritis—Part 1: Osteoarthritis. Phytother. Res. 2009, 23, 1497–1515. [Google Scholar] [CrossRef]
- De Leon-Casasola, O. New Developments in the Treatment Algorithm for Peripheral Neuropathic Pain. Pain Med. 2011, 12, S100–S108. [Google Scholar] [CrossRef]
- Chrubasik, S.; Weiser, T.; Beime, B. Effectiveness and Safety of Topical Capsaicin Cream in the Treatment of Chronic Soft Tissue Pain. Phytother. Res. 2010, 24, 1877–1885. [Google Scholar] [CrossRef]
- Guedes, V.; Castro, J.P.; Brito, I. Topical Capsaicin for Pain in Osteoarthritis: A Literature Review. Reumatol. Clin. 2018, 14, 40–45. [Google Scholar] [CrossRef]
- Frerick, H.; Keitel, W.; Kuhn, U.; Schmidt, S.; Bredehorst, A.; Kuhlmann, M. Topical Treatment of Chronic Low Back Pain with a Capsicum Plaster. PAIN 2003, 106, 59–64. [Google Scholar] [CrossRef]
- Persson, M.S.M.; Stocks, J.; Walsh, D.A.; Doherty, M.; Zhang, W. The Relative Efficacy of Topical Non-Steroidal Anti-Inflammatory Drugs and Capsaicin in Osteoarthritis: A Network Meta-Analysis of Randomised Controlled Trials. Osteoarthr. Cartil. 2018, 26, 1575–1582. [Google Scholar] [CrossRef]
- Ercan, N.; Uludag, M.O.; Agis, E.R.; Demirel-Yilmaz, E. The Anti-Inflammatory Effect of Diclofenac Is Considerably Augmented by Topical Capsaicinoids-Containing Patch in Carrageenan-Induced Paw Oedema of Rat. Inflammopharmacology 2013, 21, 413–419. [Google Scholar] [CrossRef]
- Szolcsányi, J. Forty Years in Capsaicin Research for Sensory Pharmacology and Physiology. Neuropeptides 2004, 38, 377–384. [Google Scholar] [CrossRef]
- Silverman, H.A.; Chen, A.; Kravatz, N.L.; Chavan, S.S.; Chang, E.H. Involvement of Neural Transient Receptor Potential Channels in Peripheral Inflammation. Front. Immunol. 2020, 11, 590261. [Google Scholar] [CrossRef]
- Horváth, K.; Boros, M.; Bagoly, T.; Sándor, V.; Kilár, F.; Kemény, Á.; Helyes, Z.; Szolcsányi, J.; Pintér, E. Analgesic Topical Capsaicinoid Therapy Increases Somatostatin-like Immunoreactivity in the Human Plasma. Neuropeptides 2014, 48, 371–378. [Google Scholar] [CrossRef]
- Nalamachu, S.; Gudin, J. Characteristics of Analgesic Patch Formulations. JPR 2020, 13, 2343–2354. [Google Scholar] [CrossRef]
- McConville, C.; Andrews, G.P.; Woolfson, A.D.; Karl Malcolm, R. Effect of the Incorporation of Hydroxy-Terminated Liquid Silicones on the Cure Characteristics, Morphology, and Release of a Model Protein from Silicone Elastomer-Covered Rods. J. Appl. Polym. Sci. 2012, 124, 805–812. [Google Scholar] [CrossRef]
- Abrams, R.M.C.; Pedowitz, E.J.; Simpson, D.M. A Critical Review of the Capsaicin 8% Patch for the Treatment of Neuropathic Pain Associated with Diabetic Peripheral Neuropathy of the Feet in Adults. Expert Rev. Neurother. 2021, 21, 259–266. [Google Scholar] [CrossRef]
- Bley, K.R. TRPV1 Agonist Approaches for Pain Management. In Vanilloid Receptor TRPV1 in Drug Discovery: Targeting Pain and Other Pathological Disorders; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2010; pp. 325–347. [Google Scholar]
- Kaale, E.; Van Schepdael, A.; Roets, E.; Hoogmartens, J. Determination of Capsaicinoids in Topical Cream by Liquid-Liquid Extraction and Liquid Chromatography. J. Pharm. Biomed. Anal. 2002, 30, 1331–1337. [Google Scholar] [CrossRef]
- Hill, R. NK1 (Substance P) Receptor Antagonists—Why Are They Not Analgesic in Humans? Trends Pharmacol. Sci. 2000, 21, 244–246. [Google Scholar] [CrossRef]
- Anand, P.; Bley, K. Topical Capsaicin for Pain Management: Therapeutic Potential and Mechanisms of Action of the New High-Concentration Capsaicin 8% Patch. Br. J. Anaesth. 2011, 107, 490–502. [Google Scholar] [CrossRef]
- Martini, C.H.; Yassen, A.; Krebs-Brown, A.; Passier, P.; Stoker, M.; Olofsen, E.; Dahan, A. A Novel Approach to Identify Responder Subgroups and Predictors of Response to Low- and High-Dose Capsaicin Patches in Postherpetic Neuralgia: Capsaicin in Postherpetic Neuralgia. EJP 2013, 17, 1491–1501. [Google Scholar] [CrossRef]
- Moon, J.-Y.; Lee, P.-B.; Kim, Y.-C.; Lee, S.-C.; Nahm, F.S.; Choi, E. Efficacy and Safety of 0.625% and 1.25% Capsaicin Patch in Peripheral Neuropathic Pain: Multi-Center, Randomized, and Semi-Double Blind Controlled Study. Pain Physician 2017, 20, 27–35. [Google Scholar]
- Pethő, G.; Bölcskei, K.; Füredi, R.; Botz, B.; Bagoly, T.; Pintér, E.; Szolcsányi, J. Evidence for a Novel, Neurohumoral Antinociceptive Mechanism Mediated by Peripheral Capsaicin-Sensitive Nociceptors in Conscious Rats. Neuropeptides 2017, 62, 1–10. [Google Scholar] [CrossRef]
- Spampinato, S.; Romualdi, P.; Candeletti, S.; Cavicchini, E.; Ferri, S. Distinguishable Effects of Intrathecal Dynorphins, Somatostatin, Neurotensin and s-Calcitonin on Nociception and Motor Function in the Rat. Pain 1988, 35, 95–104. [Google Scholar] [CrossRef]
- Rosenthal, B.M.; Ho, R.H. An Electron Microscopic Study of Somatostatin Immunoreactive Structures in Lamina II of the Rat Spinal Cord. Brain Res. Bull. 1989, 22, 439–451. [Google Scholar] [CrossRef]
- Kecskés, A.; Pohóczky, K.; Kecskés, M.; Varga, Z.V.; Kormos, V.; Szőke, É.; Henn-Mike, N.; Fehér, M.; Kun, J.; Gyenesei, A.; et al. Characterization of Neurons Expressing the Novel Analgesic Drug Target Somatostatin Receptor 4 in Mouse and Human Brains. Int. J. Mol. Sci. 2020, 21, 7788. [Google Scholar] [CrossRef]
- Brennan, T.J.; Vandermeulen, E.P.; Gebhart, G.F. Characterization of a Rat Model of Incisional Pain. Pain 1996, 64, 493–502. [Google Scholar] [CrossRef]
- Morris, C.J. Carrageenan-Induced Paw Edema in the Rat and Mouse. Methods Mol. Biol. 2003, 225, 115–121. [Google Scholar] [CrossRef]
- Ng, S.-F.; Rouse, J.J.; Sanderson, F.D.; Meidan, V.; Eccleston, G.M. Validation of a Static Franz Diffusion Cell System for In Vitro Permeation Studies. AAPS PharmSciTech 2010, 11, 1432–1441. [Google Scholar] [CrossRef]
- Zsikó, S.; Csányi, E.; Kovács, A.; Budai-Szűcs, M.; Gácsi, A.; Berkó, S. Methods to Evaluate Skin Penetration In Vitro. Sci. Pharm. 2019, 87, 19. [Google Scholar] [CrossRef]
- Bakonyi, M.; Gácsi, A.; Kovács, A.; Szűcs, M.-B.; Berkó, S.; Csányi, E. Following-up Skin Penetration of Lidocaine from Different Vehicles by Raman Spectroscopic Mapping. J. Pharm. Biomed. Anal. 2018, 154, 1–6. [Google Scholar] [CrossRef]
- Zsikó, S.; Csányi, E.; Kovács, A.; Budai-Szűcs, M.; Gácsi, A.; Berkó, S. Novel In Vitro Investigational Methods for Modeling Skin Permeation: Skin PAMPA, Raman Mapping. Pharmaceutics 2020, 12, 803. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dose | IVRT 1 | IVPT 2 |
|---|---|---|
| 1 mg/g patch | 3.2215 | 0.0466 |
| 2.3 mg/g patch | 8.233 | 0.1672 |
| Type of TTS | Drug Release Kinetics | Dosing by Cutting | Flexibility |
|---|---|---|---|
| Membrane-controlled | close to zero-order | no | good |
| Drug in adhesive | unregulated | yes | good |
| Micro-reservoir | regulated | no | poor |
| Classical matrix diffusion | regulated | yes | good |
| Modified silicone-polymer | close to zero-order | yes | good |
| Patch Layer | Layer Thickness | Component | Content |
|---|---|---|---|
| Drug carrier layer | 0.4 mm | Capsaicin (solid, triturated) | 3.60% |
| Capsaicin (solution) | 3.75% | ||
| Glycerol | 13.16% | ||
| Polysorbate 20 | 3.95% | ||
| RT 601 A | 69.32% | ||
| RT 601 B | 7.83% | ||
| Regulator layer | 0.1 mm | Glycerol | 12.05% |
| Polysorbate 20 | 4.00% | ||
| RT 601 A | 74.21% | ||
| RT 601 B | 9.69% | ||
| Total capsaicin content | 1 mg/g patch |
| Patch Layer | Layer Thickness | Component | Content |
|---|---|---|---|
| Drug carrier layer | 0.4 mm | Capsaicin (solid, triturated) | 8.36% |
| Capsaicin (solution) | 5.58% | ||
| Glycerol | 10.52% | ||
| Polysorbate 20 | 5.69% | ||
| RT 601 A | 62.89% | ||
| RT 601 B | 6.98% | ||
| Regulator layer | 0.1 mm | Glycerol | 11.88% |
| Polysorbate 20 | 3.43% | ||
| RT 601 A | 76.21% | ||
| RT 601 B | 8.46% | ||
| Total capsaicin content | 2.3 mg/g patch |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
László, S.; Bátai, I.Z.; Berkó, S.; Csányi, E.; Dombi, Á.; Pozsgai, G.; Bölcskei, K.; Botz, L.; Wagner, Ö.; Pintér, E. Development of Capsaicin-Containing Analgesic Silicone-Based Transdermal Patches. Pharmaceuticals 2022, 15, 1279. https://doi.org/10.3390/ph15101279
László S, Bátai IZ, Berkó S, Csányi E, Dombi Á, Pozsgai G, Bölcskei K, Botz L, Wagner Ö, Pintér E. Development of Capsaicin-Containing Analgesic Silicone-Based Transdermal Patches. Pharmaceuticals. 2022; 15(10):1279. https://doi.org/10.3390/ph15101279
Chicago/Turabian StyleLászló, Szabolcs, István Z. Bátai, Szilvia Berkó, Erzsébet Csányi, Ágnes Dombi, Gábor Pozsgai, Kata Bölcskei, Lajos Botz, Ödön Wagner, and Erika Pintér. 2022. "Development of Capsaicin-Containing Analgesic Silicone-Based Transdermal Patches" Pharmaceuticals 15, no. 10: 1279. https://doi.org/10.3390/ph15101279
APA StyleLászló, S., Bátai, I. Z., Berkó, S., Csányi, E., Dombi, Á., Pozsgai, G., Bölcskei, K., Botz, L., Wagner, Ö., & Pintér, E. (2022). Development of Capsaicin-Containing Analgesic Silicone-Based Transdermal Patches. Pharmaceuticals, 15(10), 1279. https://doi.org/10.3390/ph15101279