
Effect of MDI Actuation Timing on Inhalation Dosimetry in a Human Respiratory Tract Model



Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Results
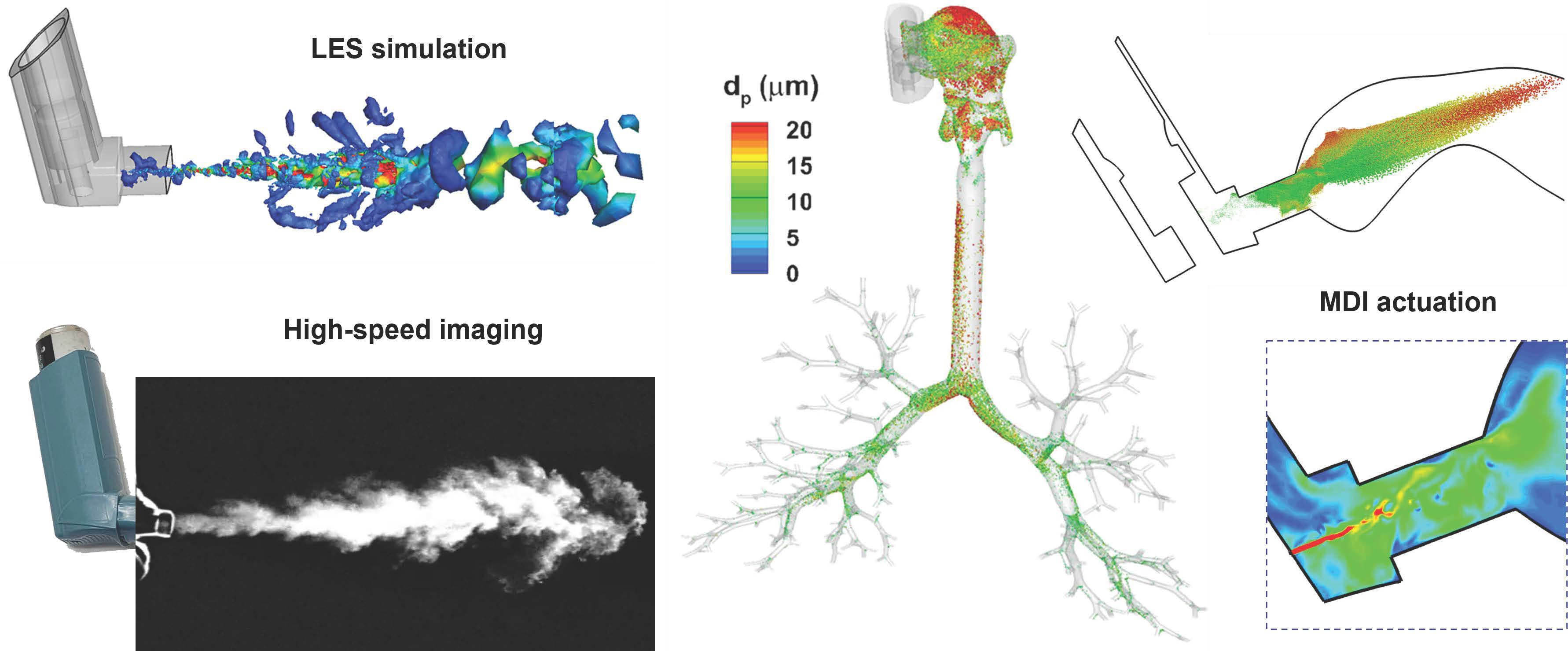
2.1. High-Speed Imaging of MDI Releasing
2.2. Measurement-Based Computational Platform for MDI Delivery
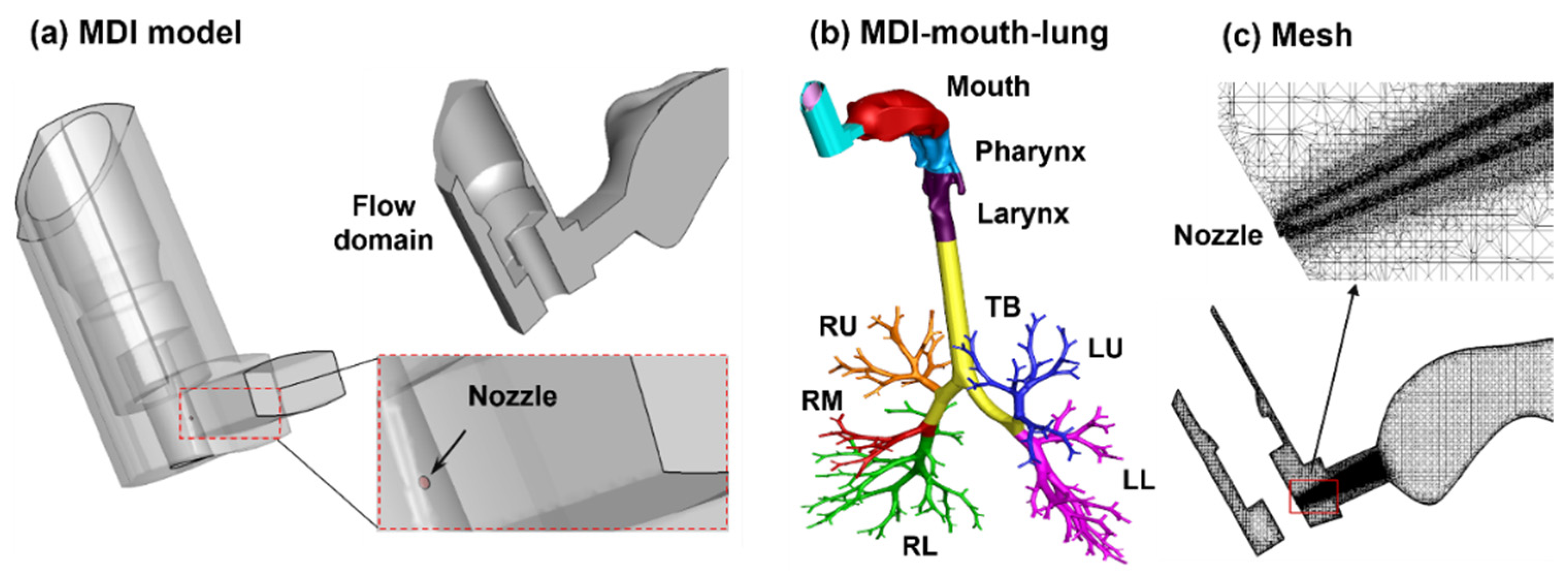
2.2.1. Integrated MDI–Mouth–Lung Model and Waveforms
2.2.2. Measurement-Based Aerosol Size Distribution
2.2.3. Mesh and Aerosol-Count Sensitivity Analysis
2.2.4. Determining the Droplet Discharging Velocity at the Orifice
2.3. Flow and Aerosol Dynamics of the Control Case (Triggering at 0.63 s)
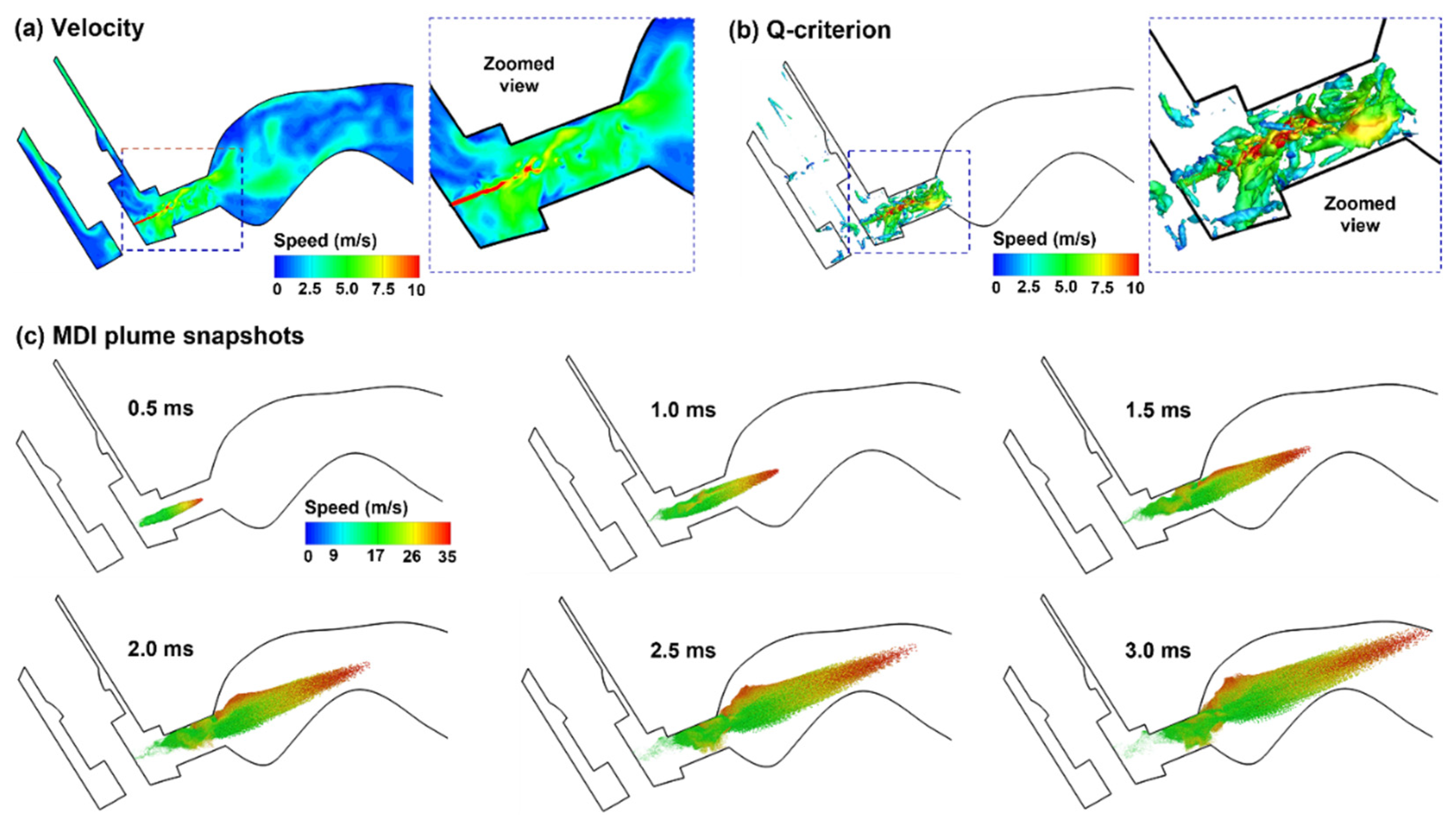
2.3.1. Aerosol Discharging from the Orifice: 0.5–3.0 ms after Actuation Onset
2.3.2. Aerosol Dispersion in the Upper Airway: 20–60 ms after Actuation Onset
2.3.3. Aerosol Dispensing into the Lung: 200 ms after Actuation Onset
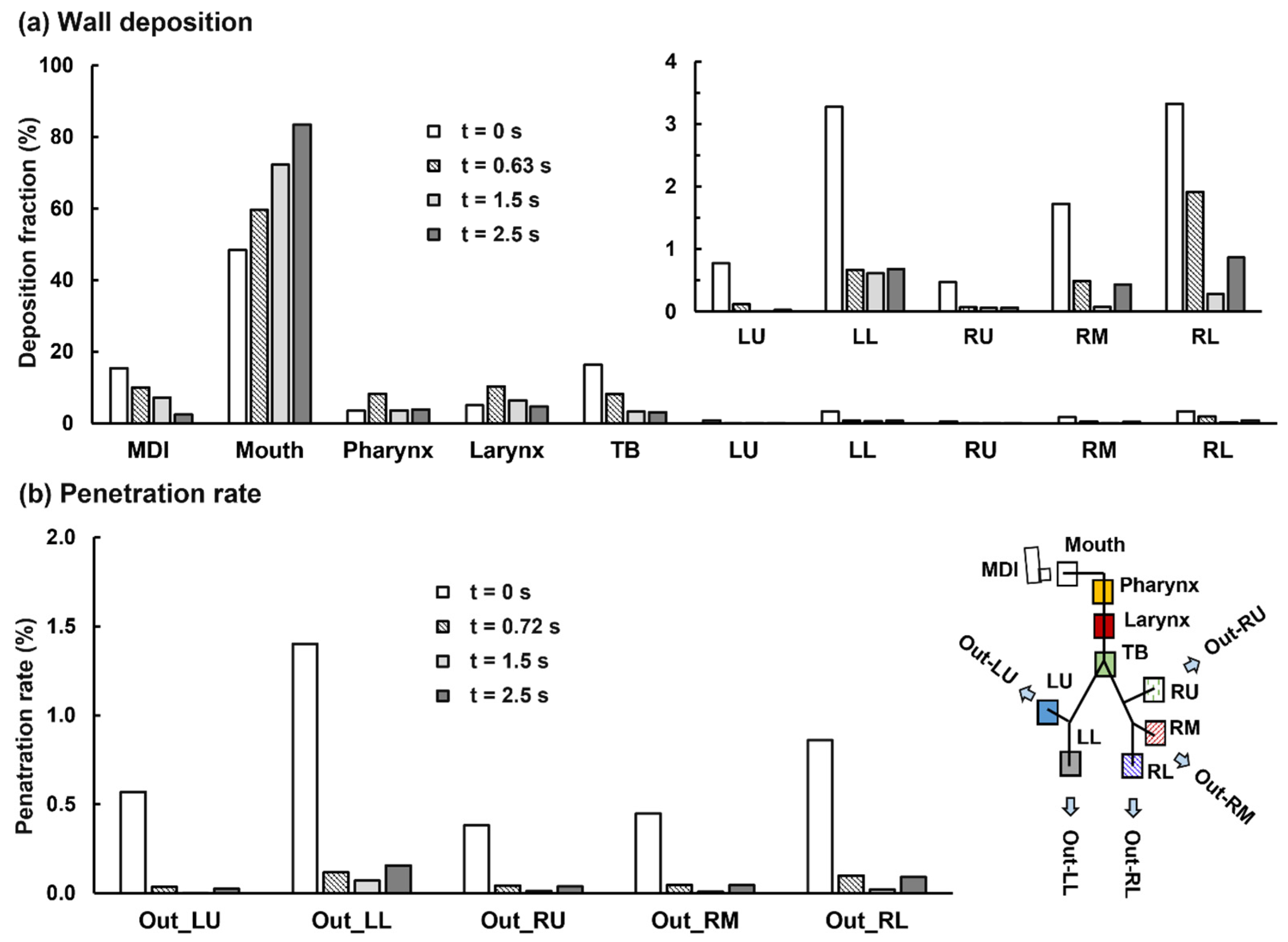
2.3.4. Aerosol Deposition
2.4. Effect of Early and Delayed Actuation Times
2.4.1. Airflow and Droplet Dynamics during 0.5–5 ms for 0 s Actuation
2.4.2. Airflow and Droplet Dynamics during 20–400 ms for 0 s Actuation
2.4.3. MDI Actuation Time Effects on Drug Dosimetry
2.4.4. MDI Actuation Time Effects on Deposition Distribution
3. Discussion
3.1. Deposition Validation against Experiments
3.2. Three Phases of Aerosol Dynamics during MDI Delivery
3.3. Effect of Actuation–Inhalation Coordination on Deposition Distribution
3.4. Limitations
4. Materials and Methods
4.1. MDI–Mouth–Lung Model Development
4.2. High-Speed Imaging
4.3. Numerical Methods
5. Conclusions
- The discharging velocity of the CFC-albuterol MDI aerosols was reversely determined to be 40 m/s to match the PDA measurements at 3 and 6 cm from the mouthpiece.
- Highly trainset evolution of the MDI plume was recorded by using a high-speed camera at 4000 fps, which compared favorably with complementary LES simulations.
- Good agreement was attained between CFD predictions and measured doses in the device, mouth–throat, and lung.
- Delayed MDI triggering increased drug loss in the mouth and reduced doses in the lung.
- MDI actuation just before the inhalation increased drug loss in the device, but led to improved dosimetry in the airway, including a reduced loss in the mouth–throat region and a higher delivery efficiency to the five lobes in both central and peripheral regions.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McCabe, J.C.; Koppenhagen, F.; Blair, J.; Zeng, X.M. ProAir HFA delivers warmer, lower-impact, longer-duration plumes containing higher fine particle dose than Ventolin HFA. J. Aerosol Med. Pulm. Drug Deliv. 2012, 25, 104–109. [Google Scholar] [CrossRef]
- Cheng, Y.S. Mechanisms of pharmaceutical aerosol deposition in the respiratory tract. AAPS PharmSciTech 2014, 15, 630–640. [Google Scholar] [CrossRef] [PubMed]
- Jacob, R.E.; Lamm, W.J.; Einstein, D.R.; Krueger, M.A.; Glenny, R.W.; Corley, R.A. Comparison of CT-derived ventilation maps with deposition patterns of inhaled microspheres in rats. Exp. Lung Res. 2015, 41, 135–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinchurkar, S.; Backer, L.D.; Vos, W.; Holsbeke, C.V.; Backer, J.D.; Backer, W.D. A case series on lung deposition analysis of inhaled medication using functional imaging based computational fluid dynamics in asthmatic patients: Effect of upper airway morphology and comparison with in vivo data. Inhal. Toxicol. 2012, 24, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Dugernier, J.; Hesse, M.; Vanbever, R.; Depoortere, V.; Roeseler, J.; Michotte, J.B.; Laterre, P.F.; Jamar, F.; Reychler, G. SPECT-CT Comparison of Lung Deposition using a System combining a Vibrating-mesh Nebulizer with a Valved Holding Chamber and a Conventional Jet Nebulizer: A Randomized Cross-over Study. Pharm. Res. 2017, 34, 290–300. [Google Scholar] [CrossRef]
- Venegas, J.; Winkler, T.; Harris, R.S. Lung physiology and aerosol deposition imaged with positron emission tomography. J. Aerosol Med. Pulm. Drug Deliv. 2013, 26, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hochhaus, G.; Chen, M.J.; Kurumaddali, A.; Schilling, U.; Jiao, Y.; Drescher, S.K.; Amini, E.; Berger, S.M.; Kandala, B.; Tabulov, C.; et al. Can pharmacokinetic studies assess the pulmonary fate of dry powder inhaler formulations of fluticasone propionate? AAPS J. 2021, 23, 48. [Google Scholar] [CrossRef] [PubMed]
- Tian, G.; Hindle, M.; Lee, S.; Longest, P.W. Validating CFD Predictions of Pharmaceutical Aerosol Deposition with In Vivo Data. Pharm. Res. 2015, 32, 3170–3187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Movia, D.; Prina-Mello, A. Preclinical Development of Orally Inhaled Drugs (OIDs)-Are Animal Models Predictive or Shall We Move Towards In Vitro Non-Animal Models? Animals 2020, 10, 1259. [Google Scholar] [CrossRef]
- Hens, B.; Sinko, P.D.; Job, N.; Dean, M.; Al-Gousous, J.; Salehi, N.; Ziff, R.M.; Tsume, Y.; Bermejo, M.; Paixão, P.; et al. Formulation predictive dissolution (fPD) testing to advance oral drug product development: An introduction to the US FDA funded ‘21st Century BA/BE’ project. Int. J. Pharm. 2018, 548, 120–127. [Google Scholar] [CrossRef]
- Fernández-Parra, R.; Pey, P.; Reinero, C.; Malvè, M. Salbutamol transport and deposition in the upper and lower airway with different devices in cats: A computational fluid dynamics approach. Animals 2021, 11, 2431. [Google Scholar] [CrossRef]
- Kytariolos, J.; Dokoumetzidis, A.; Macheras, P. Power law IVIVC: An application of fractional kinetics for drug release and absorption. Eur. J. Pharm. Sci. 2010, 41, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Zhu, Q.; Zhou, X.; Gou, D.; Yu, J.; Li, R.; Tong, Z.; Yang, R. Role of CFD based in silico modelling in establishing an in vitro-in vivo correlation of aerosol deposition in the respiratory tract. Adv. Drug Deliv. Rev. 2021, 170, 369–385. [Google Scholar] [CrossRef] [PubMed]
- Sou, T.; Bergström, C.A.S. Contemporary formulation development for inhaled pharmaceuticals. J. Pharm. Sci. 2021, 110, 66–86. [Google Scholar] [CrossRef]
- Longest, P.W.; Bass, K.; Dutta, R.; Rani, V.; Thomas, M.L.; El-Achwah, A.; Hindle, M. Use of computational fluid dynamics deposition modeling in respiratory drug delivery. Expert Opin. Drug Deliv. 2019, 16, 7–26. [Google Scholar] [CrossRef] [PubMed]
- Kleinstreuer, C.; Feng, Y. Lung deposition analyses of inhaled toxic aerosols in conventional and less harmful cigarette smoke: A review. Int. J. Environ. Res. Public Health 2013, 10, 4454–4485. [Google Scholar] [CrossRef] [PubMed]
- Velsor-Friedrich, B.; Militello, L.K.; Zinn, K.K.; DeWolff, D.K. Switching from CFC to HFA Inhalers: What NPs and Their Patients Need to Know. Am. J. Nurse Pract. 2009, 13, 45–50. [Google Scholar]
- Ross, D.L.; Gabrio, B.J. Advances in metered dose inhaler technology with the development of a chlorofluorocarbon-free drug delivery system. J. Aerosol Med. 1999, 12, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Elbeddini, A. Sterilization plan of the used metered dose inhalers (MDI) to avoid wastage amid COVID-19 pandemic drug shortage. J. Pharm. Policy Pract. 2020, 13, 19. [Google Scholar] [CrossRef] [PubMed]
- Elbeddini, A.; Tayefehchamani, Y.; Yang, L. Strategies to conserve salbutamol pressurized metered-dose inhaler stock levels amid COVID-19 drug shortage. Drugs Ther. Perspect. 2020, 36, 451–454. [Google Scholar] [CrossRef]
- Panos, R.J. Efficacy and safety of eco-friendly inhalers: Focus on combination ipratropium bromide and albuterol in chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2013, 8, 221–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchis, J.; Gich, I.; Pedersen, S. Systematic Review of Errors in Inhaler Use: Has Patient Technique Improved Over Time? Chest 2016, 150, 394–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kellman, D.A.; Iserson, K.V.; Levy, R.D.; McIntosh, B.; Maxwell, Y. Brief education improves proper metered-dose inhaler use. J. Emerg. Med. 2020, 58, 667–672. [Google Scholar] [CrossRef]
- Farkas, Á.; Horváth, A.; Kerekes, A.; Nagy, A.; Kugler, S.; Tamási, L.; Tomisa, G. Effect of delayed pMDI actuation on the lung deposition of a fixed-dose combination aerosol drug. Int. J. Pharm. 2018, 547, 480–488. [Google Scholar] [CrossRef] [Green Version]
- Stein, S.W.; Sheth, P.; Hodson, P.D.; Myrdal, P.B. Advances in metered dose inhaler technology: Hardware development. AAPS PharmSciTech 2014, 15, 326–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hochrainer, D.; Holz, H.; Kreher, C.; Scaffidi, L.; Spallek, M.; Wachtel, H. Comparison of the aerosol velocity and spray duration of Respimat soft mist inhaler and pressurized metered dose inhalers. J. Aerosol Med. 2005, 18, 273–282. [Google Scholar] [CrossRef]
- Liao, Y.H.; Zeng, X.M. Advances in studies of pressurized metered dose formulations containing hydrofluoroalkane propellants. Acta Pharm. Sin. 2006, 41, 197–202. [Google Scholar]
- Ivey, J.W.; Vehring, R.; Finlay, W.H. Understanding pressurized metered dose inhaler performance. Expert Opin. Drug Deliv. 2015, 12, 901–916. [Google Scholar] [CrossRef] [PubMed]
- Schroeter, J.D.; Sheth, P.; Hickey, A.J.; Asgharian, B.; Price, O.T.; Holt, J.T.; Conti, D.S.; Saluja, B. Effects of formulation variables on lung dosimetry of albuterol sulfate suspension and beclomethasone dipropionate solution metered dose inhalers. AAPS PharmSciTech 2018, 19, 2335–2345. [Google Scholar] [CrossRef]
- Liu, X.; Doub, W.H.; Guo, C. Evaluation of metered dose inhaler spray velocities using phase Doppler anemometry (PDA). Int. J. Pharm. 2012, 423, 235–239. [Google Scholar] [CrossRef]
- Duke, D.J.; Scott, H.N.; Kusangaya, A.J.; Kastengren, A.L.; Matusik, K.; Young, P.; Lewis, D.; Honnery, D. Drug distribution transients in solution and suspension-based pressurised metered dose inhaler sprays. Int. J. Pharm. 2019, 566, 463–475. [Google Scholar] [CrossRef] [PubMed]
- McKiernan, A.P. Inhaler spray investigation using high-speed phase-contrast X-ray and schlieren imaging. Pharm. Res. 2019, 36, 120. [Google Scholar] [CrossRef]
- Mason-Smith, N.; Duke, D.J.; Kastengren, A.L.; Traini, D.; Young, P.M.; Chen, Y.; Lewis, D.A.; Edgington-Mitchell, D.; Honnery, D. Revealing pMDI spray initial conditions: Flashing, atomisation and the effect of ethanol. Pharm. Res. 2017, 34, 718–729. [Google Scholar] [CrossRef] [PubMed]
- Mason-Smith, N.; Duke, D.J.; Kastengren, A.L.; Stewart, P.J.; Traini, D.; Young, P.M.; Chen, Y.; Lewis, D.A.; Soria, J.; Edgington-Mitchell, D.; et al. Insights into spray development from metered-dose inhalers through quantitative X-ray radiography. Pharm. Res. 2016, 33, 1249–1258. [Google Scholar] [CrossRef]
- Tarara, T.E.; Hartman, M.S.; Gill, H.; Kennedy, A.A.; Weers, J.G. Characterization of suspension-based metered dose inhaler formulations composed of spray-dried budesonide microcrystals dispersed in HFA-134a. Pharm. Res. 2004, 21, 1607–1614. [Google Scholar] [CrossRef]
- D’Sa, D.; Chan, H.K. A review of methods for evaluating particle stability in suspension based pressurized metered dose inhalers. Curr. Pharm. Des. 2015, 21, 3955–3965. [Google Scholar] [CrossRef]
- Liao, Y.H.; Brown, M.B.; Jones, S.A.; Nazir, T.; Martin, G.P. The effects of polyvinyl alcohol on the in vitro stability and delivery of spray-dried protein particles from surfactant-free HFA 134a-based pressurised metered dose inhalers. Int. J. Pharm. 2005, 304, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Smyth, H.; Hickey, A.J.; Brace, G.; Barbour, T.; Gallion, J.; Grove, J. Spray pattern analysis for metered dose inhalers I: Orifice size, particle size, and droplet motion correlations. Drug Dev. Ind. Pharm. 2006, 32, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Longest, P.W.; Tian, G.; Walenga, R.L.; Hindle, M. Comparing MDI and DPI aerosol deposition using in vitro experiments and a new stochastic individual path (SIP) model of the conducting airways. Pharm. Res. 2012, 29, 1670–1688. [Google Scholar] [CrossRef]
- Oliveira, R.F.; Ferreira, A.C.; Teixeira, S.F.; Teixeira, J.C.; Cabral-Marques, H. A.C.; Teixeira, S.F.; Teixeira, J.C.; Cabral-Marques, H. A CFD study of a pMDI plume spray. In Transactions on Engineering Technologies; Yang, G.C., Ao, S.I., Gelman, L., Yang, G.-C., Ao, S.-I., Gelman, L., Eds.; Transactions on Engineering Technologies; Springer: Dordrecht, The Netherlands, 2014; pp. 163–176. [Google Scholar]
- Moraga-Espinoza, D.F.; Eshaghian, E.; Shaver, A.; Smyth, H.D.C. Effect of inhalation flow rate on mass-based plume geometry of commercially available suspension pMDIs. AAPS J. 2018, 20, 84. [Google Scholar] [CrossRef] [PubMed]
- Kleinstreuer, C.; Shi, H.; Zhang, Z. Computational analyses of a pressurized metered dose inhaler and a new drug-aerosol targeting methodology. J. Aerosol Med. 2007, 20, 294–309. [Google Scholar] [CrossRef]
- Tian, G.; Longest, P.W.; Su, G.; Walenga, R.L.; Hindle, M. Development of a stochastic individual path (SIP) model for predicting the tracheobronchial deposition of pharmaceutical aerosols: Effects of transient inhalation and sampling the airways. J. Aerosol Sci. 2011, 42, 781–799. [Google Scholar] [CrossRef]
- Melani, A.S. Inhalatory therapy training: A priority challenge for the physician. Acta Biomed. 2007, 78, 233–245. [Google Scholar]
- Hess, D.R. Aerosol delivery devices in the treatment of asthma. Respir. Care 2008, 53, 699–723. [Google Scholar] [PubMed]
- Barjaktarevic, I.Z.; Milstone, A.P. Nebulized therapies in COPD: Past, present, and the future. Int. J. Chron. Obstruct. Pulmon. Dis. 2020, 15, 1665–1677. [Google Scholar] [CrossRef] [PubMed]
- Xi, J.; Si, X.A.; Nagarajan, R. Effects of mask-wearing on the inhalability and deposition of airborne SARS-CoV-2 aerosols in human upper airway. Phy. Fluids 2020, 32, 123312. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Ye, W.; Kauffman, J.; Doub, W.H. Evaluation of impaction force of nasal sprays and metered-dose inhalers using the Texture Analyser. J. Pharm. Sci. 2009, 98, 2799–2806. [Google Scholar] [CrossRef]
- Xi, J.; Kim, J.; Si, X.; Corley, R.A.; Zhou, Y. Modeling of inertial depositions in scaled models of rat and human nasal airways: Towards in vitro regional dosimetry in small animals. J. Aerosol Sci. 2016, 99, 78–93. [Google Scholar] [CrossRef]
- Xi, J.; Longest, P.W.; Martonen, T.B. Effects of the laryngeal jet on nano- and microparticle transport and deposition in an approximate model of the upper tracheobronchial airways. J. Appl. Physiol. 2008, 104, 1761–1777. [Google Scholar] [CrossRef]
- Zhang, Z.; Kleinstreuer, C.; Kim, C.S. Cyclic micron-size particle inhalation and deposition in a triple bifurcation lung airway model. J. Aerosol Sci. 2002, 33, 257–281. [Google Scholar] [CrossRef]
- Li, Z. Particle deposition in oral-tracheal airway models with very low inhalation profiles. J. Bionic. Eng. 2012, 9, 252–261. [Google Scholar] [CrossRef]
- De Backer, J.W.; Vos, W.G.; Burnell, P.; Verhulst, S.L.; Salmon, P.; De Clerck, N.; De Backer, W. Study of the variability in upper and lower airway morphology in Sprague-Dawley rats using modern micro-CT scan-based segmentation techniques. Anat. Rec. 2009, 292, 720–727. [Google Scholar] [CrossRef]
- Cheng, Y.S.; Fu, C.S.; Yazzie, D.; Zhou, Y. Respiratory deposition patterns of salbutamol pMDI with CFC and HFA-134a formulations in a human airway replica. J. Aerosol Med. 2001, 14, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, R.F.; Silva, L.F.; Teixeira, J.C.; Antunes, H. Study of a pressurized metered-dose inhaler spray parameters in Fluent. In Proceedings of the World Congress on Engineering 2010, London, UK, 30 June–2 July 2010. [Google Scholar]
- Talaat, K.; Xi, J. Computational modeling of aerosol transport, dispersion, and deposition in rhythmically expanding and contracting terminal alveoli. J. Aerosol Sci. 2017, 112, 19–33. [Google Scholar] [CrossRef]
- He, C.; Ahmadi, G. Particle deposition with thermophoresis in laminar and turbulent duct flows. Aerosol Sci. Tech. 1998, 29, 525–546. [Google Scholar] [CrossRef]
- Yin, Z.-Q.; Li, X.-F.; Bao, F.-B.; Tu, C.-X.; Gao, X.-Y. Thermophoresis and Brownian motion effects on nanoparticle deposition inside a 90° square bend tube. Aerosol Air Qual. Res. 2018, 18, 1746–1755. [Google Scholar] [CrossRef] [Green Version]
- Xi, J.; Kim, J.; Si, X.A.; Zhou, Y. Hygroscopic aerosol deposition in the human upper respiratory tract under various thermo-humidity conditions. J. Environ. Sci. Health Part A 2013, 48, 1790–1805. [Google Scholar] [CrossRef] [PubMed]
- Kitaoka, H. The origin of frequency dependence of respiratory resistance: An airflow simulation study using a 4D pulmonary lobule model. Respirology 2011, 16, 517–522. [Google Scholar] [CrossRef]
- Kitaoka, H.; Nieman, G.F.; Fujino, Y.; Carney, D.; DiRocco, J.; Kawase, I. A 4-dimensional model of the alveolar structure. J. Physiol. Sci. 2007, 57, 175–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitaoka, H.; Takaki, R.; Suki, B. A three-dimensional model of the human airway tree. J. Appl. Physiol. 1985, 87, 2207–2217. [Google Scholar] [CrossRef] [PubMed]
- Kitaoka, H.; Tamura, S.; Takaki, R. A three-dimensional model of the human pulmonary acinus. J. Appl. Physiol. 2000, 88, 2260–2268. [Google Scholar] [CrossRef]
- Xi, J.; Eddie Yuan, J.; Alshaiba, M.; Cheng, D.; Firlit, Z.; Johnson, A.; Nolan, A.; Su, W.-C. Design and testing of electric-guided delivery of charged particles to the olfactory region: Experimental and numerical studies. Curr. Drug Deliv. 2016, 13, 265–274. [Google Scholar] [CrossRef]
- Xi, J.; Yuan, J.E.; Si, X.A.; Hasbany, J. Numerical optimization of targeted delivery of charged nanoparticles to the ostiomeatal complex for treatment of rhinosinusitis. Int. J. Nanomed. 2015, 10, 4847–4861. [Google Scholar] [CrossRef] [Green Version]
- Azhdarzadeh, M.; Olfert, J.S.; Vehring, R.; Finlay, W.H. Effect of electrostatic charge on deposition of uniformly charged monodisperse particles in the nasal extrathoracic airways of an infant. J. Aerosol Med. Pulm. Drug Deliv. 2015, 28, 30–34. [Google Scholar] [CrossRef]
- Koullapis, P.G.; Kassinos, S.C.; Bivolarova, M.P.; Melikov, A.K. Particle deposition in a realistic geometry of the human conducting airways: Effects of inlet velocity profile, inhalation flowrate and electrostatic charge. J. Biomech. 2016, 49, 2201–2212. [Google Scholar] [CrossRef] [Green Version]
- Triep, M.; Brücker, C. Three-dimensional nature of the glottal jet. J. Acoust. Soc. Am. 2010, 127, 1537–1547. [Google Scholar] [CrossRef]
- Bailly, L.; Cochereau, T.; Orgéas, L.; Henrich Bernardoni, N.; Rolland du Roscoat, S.; McLeer-Florin, A.; Robert, Y.; Laval, X.; Laurencin, T.; Chaffanjon, P.; et al. 3D multiscale imaging of human vocal folds using synchrotron X-ray microtomography in phase retrieval mode. Sci. Rep. 2018, 8, 14003. [Google Scholar] [CrossRef]
- Zhao, J.; Feng, Y.; Fromen, C.A. Glottis motion effects on the particle transport and deposition in a subject-specific mouth-to-trachea model: A CFPD study. Comput. Biol. Med. 2020, 116, 103532. [Google Scholar] [CrossRef]
- Cheng, Y.S.; Zhou, Y.; Chen, B.T. Particle deposition in a cast of human oral airways. Aerosol Sci. Technol. 1999, 31, 286–300. [Google Scholar] [CrossRef]
- Xi, J.; Longest, P.W. Transport and deposition of micro-aerosols in realistic and simplified models of the oral airway. Ann. Biomed. Eng. 2007, 35, 560–581. [Google Scholar] [CrossRef]
- Nicoud, F.; Ducros, F. Subgrid-scale stress modelling based on the square of the velocity gradient tensor. Flow Turbul. Combust. 1999, 62, 183–200. [Google Scholar] [CrossRef]
- Longest, P.W.; Xi, J. Effectiveness of direct Lagrangian tracking models for simulating nanoparticle deposition in the upper airways. Aerosol Sci. Technol. 2007, 41, 380–397. [Google Scholar] [CrossRef]
- Xi, J.; Yuan, J.E.; Yang, M.; Si, X.; Zhou, Y.; Cheng, Y.-S. Parametric study on mouth–throat geometrical factors on deposition of orally inhaled aerosols. J. Aerosol Sci. 2016, 99, 94–106. [Google Scholar] [CrossRef]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Talaat, M.; Si, X.; Xi, J. Effect of MDI Actuation Timing on Inhalation Dosimetry in a Human Respiratory Tract Model. Pharmaceuticals 2022, 15, 61. https://doi.org/10.3390/ph15010061
Talaat M, Si X, Xi J. Effect of MDI Actuation Timing on Inhalation Dosimetry in a Human Respiratory Tract Model. Pharmaceuticals. 2022; 15(1):61. https://doi.org/10.3390/ph15010061
Chicago/Turabian StyleTalaat, Mohamed, Xiuhua Si, and Jinxiang Xi. 2022. "Effect of MDI Actuation Timing on Inhalation Dosimetry in a Human Respiratory Tract Model" Pharmaceuticals 15, no. 1: 61. https://doi.org/10.3390/ph15010061
APA StyleTalaat, M., Si, X., & Xi, J. (2022). Effect of MDI Actuation Timing on Inhalation Dosimetry in a Human Respiratory Tract Model. Pharmaceuticals, 15(1), 61. https://doi.org/10.3390/ph15010061