
Nuclear Imaging in Infective Endocarditis



Abstract
1. Introduction
2. Rationale for the Use of Nuclear Medicine Imaging
2.1. F-FDG PET
2.2. WBC Scintigraphy
3. Diagnostic Performances
3.1. F-FDG PET/CT
3.1.1. Native Valve Endocarditis
3.1.2. Prosthetic Valve Endocarditis
3.1.3. Cardiac Implanted Electronic Device Infective Endocarditis (CIED-IE)
3.1.4. Left Ventricular Assistance Device Infective Endocarditis (LVAD-IE)
3.1.5. Vascular Graft Infection
3.2. WBC Scintigraphy
3.2.1. PVE and NVE
3.2.2. CIED-IE, LVAD-IE and VGI
4. Septic Emboli
4.1. F-FDG-PET
4.2. WBC Scintigraphy
5. Portal of Entry
6. Prognosis
7. Comparison of 18F-FDG-PET/CT and WBC-SPECT Imaging in IE
7.1. Diagnosis
7.2. Septic Emboli
8. Practical Approach
8.1. F-FDG-PET/CT
8.1.1. Patient Preparation
8.1.2. Acquisition
8.1.3. Image Analysis
Cardiac Analysis
Extra-Cardiac Analysis
8.2. WBC-SPECT
8.2.1. Patient Preparation
8.2.2. Acquisition
8.2.3. Image Analysis
Cardiac Analysis
Extra-Cardiac Analysis
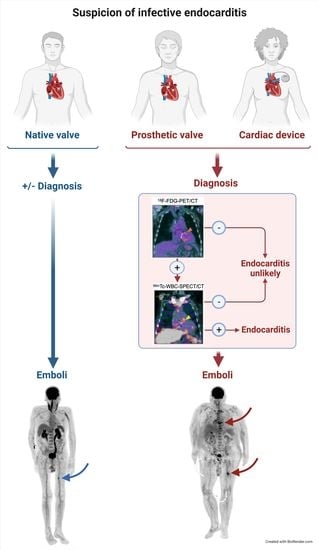
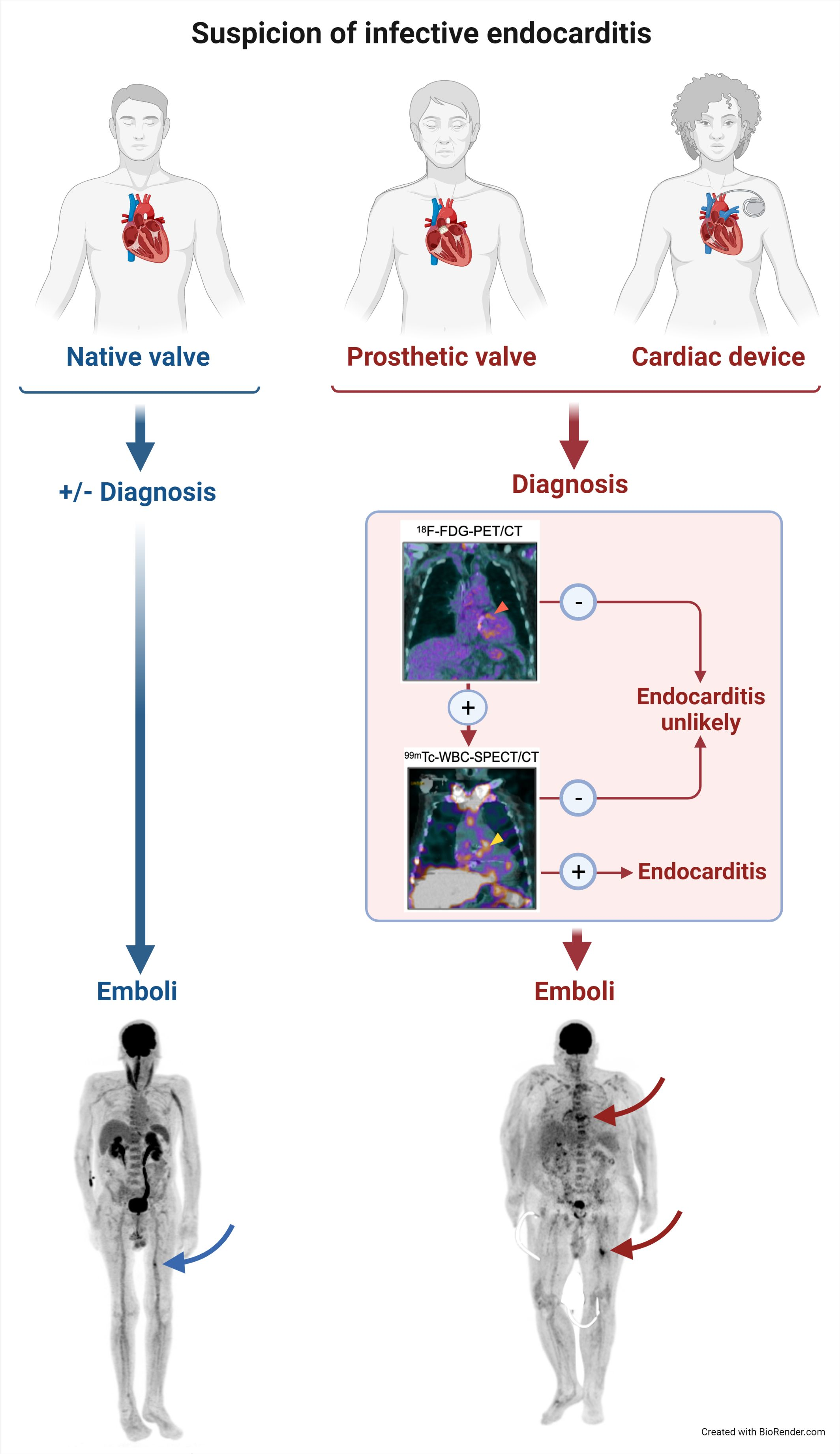
9. Diagnostic Imaging Algorithm
9.1. For NVE and PVE
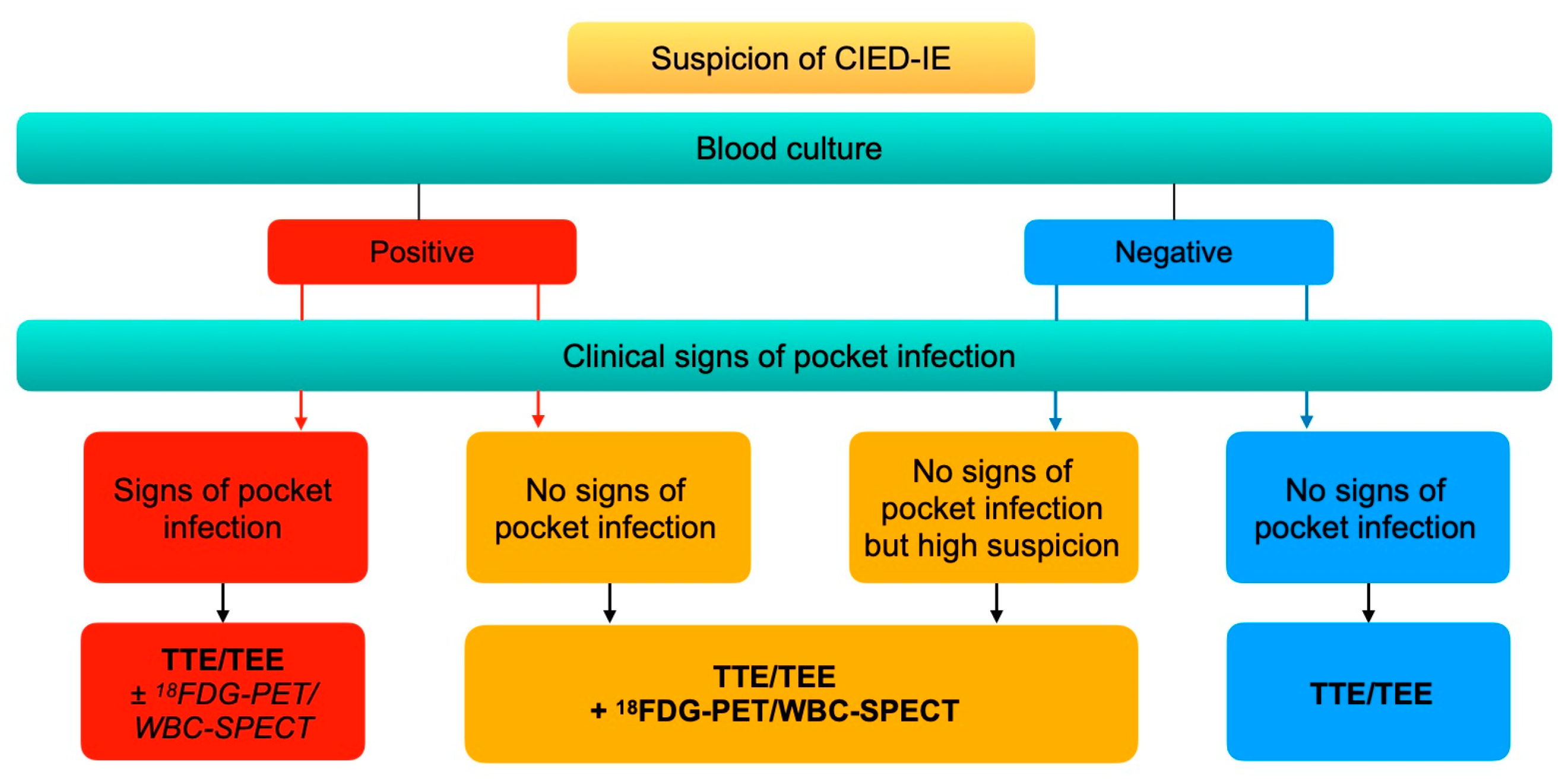
9.2. For CIED-IE
10. Potential Impact of Nuclear Medicine Tools on Treatment Strategy
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 18F-FDG | 18Fluor radiolabeled fluorodeoxyglucose |
| 111In | 111Indium-oxine |
| 99mTc-HMPAO | 99mTechnetium-hexamethylpropyleneamine oxime |
| AC | attenuation corrected |
| CIED | cardiac implantable electronic device |
| CTA | computed tomography angiography |
| CZT | cadmium-zinc-telluride |
| HF/LCD | high fat/low carbohydrates diet |
| IE | infective endocarditis |
| LVAD | left ventricular assistance device |
| NAC | non-attenuation corrected |
| NLR | negative likelihood ratio |
| NPV | negative predictive value |
| NVE | native valve endocarditis |
| OR | odds ratio |
| PET | positron emission tomography combined with computed tomography |
| PLR | positive likelihood ratio |
| PPV | positive predictive value |
| PVE | prosthetic valve endocarditis |
| Se | sensitivity |
| Sp | specificity |
| SPECT | single photon emission computed tomography |
| TEE | transesophageal echocardiography |
| TTE | transthoracic echocardiography |
| VGI | vascular graft infection |
| WBC | white blood cell |
| 18F-FDG-PET | 18F-fluorodeoxyglucose positron emission tomography |
| 99mTc-WBC | 99mTechnetium radiolabeled white blood cells |
| AC | attenuation correction |
| CIED | cardiac implanted electronic device |
| CT | computed tomography; IE: infective endocarditis |
| MIP | maximal intensity projection |
| NAC | non-attenuation correction |
| PVE | prosthetic valve endocarditis |
| SPECT | single photon emission computed tomography |
| TEE | transesophageal echocardiography |
| TTE | transthoracic echocardiography. |
References
- Habib, G.; Erba, P.A.; Iung, B.; Donal, E.; Cosyns, B.; Laroche, C.; Popescu, B.A.; Prendergast, B.; Tornos, P.; Sadeghpour, A.; et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: A prospective cohort study. Eur. Heart J. 2019, 40, 3222–3232. [Google Scholar] [CrossRef]
- Abegaz, T.M.; Bhagavathula, A.S.; Gebreyohannes, E.A.; Mekonnen, A.B.; Abebe, T.B. Short- and long-term outcomes in infective endocarditis patients: A systematic review and meta-analysis. BMC Cardiovasc. Disord. 2017, 17, 291. [Google Scholar] [CrossRef] [PubMed]
- Cahill, T.J.; Prendergast, B.D. Infective endocarditis. Lancet 2016, 387, 882–893. [Google Scholar] [CrossRef]
- Pant, S.; Patel, N.J.; Deshmukh, A.; Golwala, H.; Patel, N.; Badheka, A.; Hirsch, G.A.; Mehta, J.L. Trends in infective endocarditis incidence, microbiology, and valve replacement in the United States from 2000 to 2011. J. Am. Coll. Cardiol. 2015, 65, 2070–2076. [Google Scholar] [CrossRef] [PubMed]
- Mostaghim, A.S.; Lo, H.Y.A.; Khardori, N. A retrospective epidemiologic study to define risk factors, microbiology, and clinical outcomes of infective endocarditis in a large tertiary-care teaching hospital. SAGE Open Med. 2017, 5, 2050312117741772. [Google Scholar] [CrossRef]
- Toyoda, N.; Chikwe, J.; Itagaki, S.; Gelijns, A.C.; Adams, D.H.; Egorova, N.N. Trends in Infective Endocarditis in California and New York State, 1998–2013. JAMA 2017, 317, 1652–1660. [Google Scholar] [CrossRef]
- Murdoch, D.R.; Corey, G.R.; Hoen, B.; Miró, J.M.; Fowler, V.G., Jr.; Bayer, A.S.; Karchmer, A.W.; Olaison, L.; Pappas, P.A.; Moreillon, P.; et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: The International Collaboration on Endocarditis-Prospective Cohort Study. Arch. Intern. Med. 2009, 169, 463–473. [Google Scholar] [CrossRef]
- Chirouze, C.; Alla, F.; Fowler, V.G., Jr.; Sexton, D.J.; Corey, G.R.; Chu, V.H.; Wang, A.; Erpelding, M.L.; Durante-Mangoni, E.; Fernández-Hidalgo, N.; et al. Impact of early valve surgery on outcome of Staphylococcus aureus prosthetic valve infective endocarditis: Analysis in the International Collaboration of Endocarditis-Prospective Cohort Study. Clin. Infect. Dis. 2015, 60, 741–749. [Google Scholar] [CrossRef]
- Rieg, S.; von Cube, M.; Kaasch, A.J.; Bonaventura, B.; Bothe, W.; Wolkewitz, M.; Peyerl-Hoffmann, G.; Deppe, A.C.; Wahlers, T.; Beyersdorf, F.; et al. Investigating the Impact of Early Valve Surgery on Survival in Staphylococcus aureus Infective Endocarditis Using a Marginal Structural Model Approach: Results of a Large, Prospectively Evaluated Cohort. Clin. Infect. Dis. 2019, 69, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, R.; Wardman, D.; Cordato, D.J.; Bhaskar, S.M.M. Acute Ischaemic Stroke in Infective Endocarditis: Pathophysiology and Clinical Outcomes in Patients Treated with Reperfusion Therapy. Immuno 2021, 1, 347–359. [Google Scholar] [CrossRef]
- Baddour, L.M.; Wilson, W.R.; Bayer, A.S.; Fowler, V.G.; Tleyjeh, I.M., Jr.; Rybak, M.J.; Barsic, B.; Lockhart, P.B.; Gewitz, M.H.; Levison, M.E.; et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals From the American Heart Association. Circulation 2015, 132, 1435–1486. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef] [PubMed]
- Vieira, M.L.; Grinberg, M.; Pomerantzeff, P.M.; Andrade, J.L.; Mansur, A.J. Repeated echocardiographic examinations of patients with suspected infective endocarditis. Heart 2004, 90, 1020–1024. [Google Scholar] [CrossRef]
- Horgan, S.J.; Mediratta, A.; Gillam, L.D. Cardiovascular Imaging in Infective Endocarditis: A Multimodality Approach. Circ. Cardiovasc. Imaging 2020, 13, e008956. [Google Scholar] [CrossRef]
- Sivak, J.A.; Vora, A.N.; Navar, A.M.; Schulte, P.J.; Crowley, A.L.; Kisslo, J.; Corey, G.R.; Liao, L.; Wang, A.; Velazquez, E.J.; et al. An Approach to Improve the Negative Predictive Value and Clinical Utility of Transthoracic Echocardiography in Suspected Native Valve Infective Endocarditis. J. Am. Soc. Echocardiogr. 2016, 29, 315–322. [Google Scholar] [CrossRef]
- Habets, J.; Tanis, W.; Reitsma, J.B.; van den Brink, R.B.; Mali, W.P.; Chamuleau, S.A.; Budde, R.P. Are novel non-invasive imaging techniques needed in patients with suspected prosthetic heart valve endocarditis? A systematic review and meta-analysis. Eur. Radiol. 2015, 25, 2125–2133. [Google Scholar] [CrossRef] [PubMed]
- Fukuchi, T.; Iwata, K.; Ohji, G. Failure of early diagnosis of infective endocarditis in Japan--a retrospective descriptive analysis. Medicine 2014, 93, e237. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., III; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Thorac. Cardiovasc. Surg. 2021, 162, e183–e353. [Google Scholar] [CrossRef] [PubMed]
- Blomström-Lundqvist, C.; Traykov, V.; Erba, P.A.; Burri, H.; Nielsen, J.C.; Bongiorni, M.G.; Poole, J.; Boriani, G.; Costa, R.; Deharo, J.C.; et al. European Heart Rhythm Association (EHRA) international consensus document on how to prevent, diagnose, and treat cardiac implantable electronic device infections-endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), the Latin American Heart Rhythm Society (LAHRS), International Society for Cardiovascular Infectious Diseases (ISCVID) and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Europace 2020, 22, 515–549. [Google Scholar] [CrossRef]
- Hamacher, K.; Coenen, H.H.; Stöcklin, G. Efficient stereospecific synthesis of no-carrier-added 2-[18F]-fluoro-2-deoxy-D-glucose using aminopolyether supported nucleophilic substitution. J. Nucl. Med. 1986, 27, 235–238. [Google Scholar]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef] [PubMed]
- Besson, F.L.; Chaumet-Riffaud, P.; Playe, M.; Noel, N.; Lambotte, O.; Goujard, C.; Prigent, A.; Durand, E. Contribution of (18)F-FDG PET in the diagnostic assessment of fever of unknown origin (FUO): A stratification-based meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1887–1895. [Google Scholar] [CrossRef] [PubMed]
- Taegtmeyer, H.; Young, M.E.; Lopaschuk, G.D.; Abel, E.D.; Brunengraber, H.; Darley-Usmar, V.; Des Rosiers, C.; Gerszten, R.; Glatz, J.F.; Griffin, J.L.; et al. Assessing Cardiac Metabolism: A Scientific Statement From the American Heart Association. Circ. Res. 2016, 118, 1659–1701. [Google Scholar] [CrossRef] [PubMed]
- Slart, R.; Glaudemans, A.; Gheysens, O.; Lubberink, M.; Kero, T.; Dweck, M.R.; Habib, G.; Gaemperli, O.; Saraste, A.; Gimelli, A.; et al. Procedural recommendations of cardiac PET/CT imaging: Standardization in inflammatory-, infective-, infiltrative-, and innervation (4Is)-related cardiovascular diseases: A joint collaboration of the EACVI and the EANM. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1016–1039. [Google Scholar] [CrossRef] [PubMed]
- Roca, M.; de Vries, E.F.; Jamar, F.; Israel, O.; Signore, A. Guidelines for the labelling of leucocytes with (111)In-oxine. Inflammation/Infection Taskgroup of the European Association of Nuclear Medicine. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 835–841. [Google Scholar] [CrossRef] [PubMed]
- de Vries, E.F.; Roca, M.; Jamar, F.; Israel, O.; Signore, A. Guidelines for the labelling of leucocytes with (99m)Tc-HMPAO. Inflammation/Infection Taskgroup of the European Association of Nuclear Medicine. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 842–848. [Google Scholar] [CrossRef]
- Sánchez-Enrique, C.; Olmos, C.; Jiménez-Ballvé, A.; Fernández-Pérez, C.; Ferrera, C.; Pérez-Castejón, M.J.; Ortega Candil, A.; Delgado-Bolton, R.; Carnero, M.; Maroto, L.; et al. Usefulness of (18)F Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in Infective Endocarditis in Daily Practice: Individualized Analysis of Each Potential Focus of Infection: A Prospective Cohort Study. JACC Cardiovasc. Imaging 2018, 11, 1920–1922. [Google Scholar] [CrossRef]
- Kamani, C.H.; Allenbach, G.; Jreige, M.; Pavon, A.G.; Meyer, M.; Testart, N.; Firsova, M.; Fernandes Vieira, V.; Boughdad, S.; Nicod Lalonde, M.; et al. Diagnostic Performance of (18)F-FDG PET/CT in Native Valve Endocarditis: Systematic Review and Bivariate Meta-Analysis. Diagnostics 2020, 10, 754. [Google Scholar] [CrossRef]
- Wang, T.K.M.; Sánchez-Nadales, A.; Igbinomwanhia, E.; Cremer, P.; Griffin, B.; Xu, B. Diagnosis of Infective Endocarditis by Subtype Using (18)F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography: A Contemporary Meta-Analysis. Circ. Cardiovasc. Imaging 2020, 13, e010600. [Google Scholar] [CrossRef]
- Abikhzer, G.; Martineau, P.; Grégoire, J.; Finnerty, V.; Harel, F.; Pelletier-Galarneau, M. [(18)F]FDG-PET CT for the evaluation of native valve endocarditis. J. Nucl. Cardiol. 2020. [Google Scholar] [CrossRef]
- De Camargo, R.A.; Sommer Bitencourt, M.; Meneghetti, J.C.; Soares, J.; Gonçalves, L.F.T.; Buchpiguel, C.A.; Paixão, M.R.; Felicio, M.F.; de Matos Soeiro, A.; Varejão Strabelli, T.M.; et al. The Role of 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in the Diagnosis of Left-sided Endocarditis: Native vs Prosthetic Valves Endocarditis. Clin. Infect. Dis. 2020, 70, 583–594. [Google Scholar] [CrossRef] [PubMed]
- Duval, X.; Le Moing, V.; Tubiana, S.; Esposito-Farèse, M.; Ilic-Habensus, E.; Leclercq, F.; Bourdon, A.; Goehringer, F.; Selton-Suty, C.; Chevalier, E.; et al. Impact of Systematic Whole-body 18F-Fluorodeoxyglucose PET/CT on the Management of Patients Suspected of Infective Endocarditis: The Prospective Multicenter TEPvENDO Study. Clin. Infect. Dis. 2021, 73, 393–403. [Google Scholar] [CrossRef]
- Philip, M.; Delcourt, S.; Mancini, J.; Tessonnier, L.; Cammilleri, S.; Arregle, F.; Martel, H.; Oliver, L.; Hubert, S.; Renard, S.; et al. (18)F-fluorodeoxyglucose positron emission tomography/computed tomography for the diagnosis of native valve infective endocarditis: A prospective study. Arch. Cardiovasc. Dis. 2021, 114, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Boursier, C.; Duval, X.; Bourdon, A.; Imbert, L.; Mahida, B.; Chevalier, E.; Claudin, M.; Hoen, B.; Goehringer, F.; Selton-Suty, C.; et al. ECG-Gated Cardiac FDG PET Acquisitions Significantly Improve Detectability of Infective Endocarditis. JACC Cardiovasc. Imaging 2020, 13, 2691–2693. [Google Scholar] [CrossRef]
- Gomes, A.; Glaudemans, A.; Touw, D.J.; van Melle, J.P.; Willems, T.P.; Maass, A.H.; Natour, E.; Prakken, N.H.J.; Borra, R.J.H.; van Geel, P.P.; et al. Diagnostic value of imaging in infective endocarditis: A systematic review. Lancet Infect. Dis. 2017, 17, e1–e14. [Google Scholar] [CrossRef]
- Juneau, D.; Golfam, M.; Hazra, S.; Erthal, F.; Zuckier, L.S.; Bernick, J.; Wells, G.A.; Beanlands, R.S.B.; Chow, B.J.W. Molecular Imaging for the diagnosis of infective endocarditis: A systematic literature review and meta-analysis. Int. J. Cardiol. 2018, 253, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, M.; Kendi, A.T.; Ajmal, S.; Farid, S.; O’Horo, J.C.; Chareonthaitawee, P.; Baddour, L.M.; Sohail, M.R. Meta-analysis of 18F-FDG PET/CT in the diagnosis of infective endocarditis. J. Nucl. Cardiol. 2019, 26, 922–935. [Google Scholar] [CrossRef] [PubMed]
- Saby, L.; Laas, O.; Habib, G.; Cammilleri, S.; Mancini, J.; Tessonnier, L.; Casalta, J.P.; Gouriet, F.; Riberi, A.; Avierinos, J.F.; et al. Positron emission tomography/computed tomography for diagnosis of prosthetic valve endocarditis: Increased valvular 18F-fluorodeoxyglucose uptake as a novel major criterion. J. Am. Coll. Cardiol. 2013, 61, 2374–2382. [Google Scholar] [CrossRef]
- Pizzi, M.N.; Roque, A.; Fernández-Hidalgo, N.; Cuéllar-Calabria, H.; Ferreira-González, I.; Gonzàlez-Alujas, M.T.; Oristrell, G.; Gracia-Sánchez, L.; González, J.J.; Rodríguez-Palomares, J.; et al. Improving the Diagnosis of Infective Endocarditis in Prosthetic Valves and Intracardiac Devices With 18F-Fluordeoxyglucose Positron Emission Tomography/Computed Tomography Angiography: Initial Results at an Infective Endocarditis Referral Center. Circulation 2015, 132, 1113–1326. [Google Scholar] [CrossRef]
- Sag, S.J.M.; Menhart, K.; Grosse, J.; Hitzenbichler, F.; Hanses, F.; Mohr, A.; Salzberger, B.; Zerdzitzki, M.; Hilker, M.; Rupprecht, L.; et al. Diagnostic value of FDG PET/CT imaging in patients with surgically managed infective endocarditis: Results of a retrospective analysis at a tertiary center. J. Nucl. Cardiol. 2020. [Google Scholar] [CrossRef]
- Philip, M.; Tessonier, L.; Mancini, J.; Mainardi, J.L.; Fernandez-Gerlinger, M.P.; Lussato, D.; Attias, D.; Cammilleri, S.; Weinmann, P.; Hagege, A.; et al. Comparison Between ESC and Duke Criteria for the Diagnosis of Prosthetic Valve Infective Endocarditis. JACC Cardiovasc. Imaging 2020, 13, 2605–2615. [Google Scholar] [CrossRef]
- Boursier, C.; Duval, X.; Mahida, B.; Hoen, B.; Goehringer, F.; Selton-Suty, C.; Chevalier, E.; Roch, V.; Lamiral, Z.; Bourdon, A.; et al. Hypermetabolism of the spleen or bone marrow is an additional albeit indirect sign of infective endocarditis at FDG-PET. J. Nucl. Cardiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Miura, S.; Naya, M.; Yamashita, T.; Ohkawa, Y. Usefulness of (18)F-fluorodeoxyglucose positron emission tomography/computed tomography angiography in a patient with blood culture-negative prosthetic valve endocarditis complicated with perivalvular abscess: A case report. Eur. Heart J. Case Rep. 2019, 3, 1–5. [Google Scholar] [CrossRef]
- Dafaalla, M.; Weight, N.; Cajic, V.; Dandekar, U.; Gopalakrishnan, K.; Adesanya, O.; Low, C.S.; Banerjee, P. The utility of 18F-fluorodeoxyglucose positron emission tomography with computed tomography in Mycobacterium chimaera endocarditis: A case series. Eur. Heart J. Case Rep. 2019, 3, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Lwin, M.T.; Tsoi, V.; Yam, T.; Carroll, A.; Salmon, T.; Harden, S.; Smith, L. Blood culture negative infective endocarditis in adult congenital heart disease patients with prosthetic grafts: A case series. Eur. Heart J. Case Rep. 2021, 5, ytab106. [Google Scholar] [CrossRef]
- Swart, L.E.; Gomes, A.; Scholtens, A.M.; Sinha, B.; Tanis, W.; Lam, M.; van der Vlugt, M.J.; Streukens, S.A.F.; Aarntzen, E.; Bucerius, J.; et al. Improving the Diagnostic Performance of (18)F-Fluorodeoxyglucose Positron-Emission Tomography/Computed Tomography in Prosthetic Heart Valve Endocarditis. Circulation 2018, 138, 1412–1427. [Google Scholar] [CrossRef] [PubMed]
- Scholtens, A.M.; van Aarnhem, E.E.; Budde, R.P. Effect of antibiotics on FDG-PET/CT imaging of prosthetic heart valve endocarditis. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1223. [Google Scholar] [CrossRef] [PubMed]
- Calais, J.; Touati, A.; Grall, N.; Laouénan, C.; Benali, K.; Mahida, B.; Vigne, J.; Hyafil, F.; Iung, B.; Duval, X.; et al. Diagnostic Impact of (18)F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography and White Blood Cell SPECT/Computed Tomography in Patients With Suspected Cardiac Implantable Electronic Device Chronic Infection. Circ. Cardiovasc. Imaging 2019, 12, e007188. [Google Scholar] [CrossRef]
- Ten Hove, D.; Slart, R.; Sinha, B.; Glaudemans, A.; Budde, R.P.J. (18)F-FDG PET/CT in Infective Endocarditis: Indications and Approaches for Standardization. Curr. Cardiol. Rep. 2021, 23, 130. [Google Scholar] [CrossRef] [PubMed]
- Schouten, L.R.; Verberne, H.J.; Bouma, B.J.; van Eck-Smit, B.L.; Mulder, B.J. Surgical glue for repair of the aortic root as a possible explanation for increased F-18 FDG uptake. J. Nucl. Cardiol. 2008, 15, 146–147. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, C.; Mikaïl, N.; Benali, K.; Iung, B.; Duval, X.; Nataf, P.; Jondeau, G.; Hyafil, F.; Le Guludec, D.; Rouzet, F. Characterization of (18)F-Fluorodeoxyglucose Uptake Pattern in Noninfected Prosthetic Heart Valves. Circ. Cardiovasc. Imaging 2017, 10, e005585. [Google Scholar] [CrossRef] [PubMed]
- Jamar, F.; Buscombe, J.; Chiti, A.; Christian, P.E.; Delbeke, D.; Donohoe, K.J.; Israel, O.; Martin-Comin, J.; Signore, A. EANM/SNMMI guideline for 18F-FDG use in inflammation and infection. J. Nucl. Med. 2013, 54, 647–658. [Google Scholar] [CrossRef] [PubMed]
- Roque, A.; Pizzi, M.N.; Fernández-Hidalgo, N.; Permanyer, E.; Cuellar-Calabria, H.; Romero-Farina, G.; Ríos, R.; Almirante, B.; Castell-Conesa, J.; Escobar, M.; et al. Morpho-metabolic post-surgical patterns of non-infected prosthetic heart valves by [18F]FDG PET/CTA: "normality" is a possible diagnosis. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 24–33. [Google Scholar] [CrossRef]
- Galea, N.; Bandera, F.; Lauri, C.; Autore, C.; Laghi, A.; Erba, P.A. Multimodality Imaging in the Diagnostic Work-Up of Endocarditis and Cardiac Implantable Electronic Device (CIED) Infection. J. Clin. Med. 2020, 9, 2237. [Google Scholar] [CrossRef] [PubMed]
- Tanis, W.; Scholtens, A.; Habets, J.; van den Brink, R.B.; van Herwerden, L.A.; Chamuleau, S.A.; Budde, R.P. CT angiography and ¹⁸F-FDG-PET fusion imaging for prosthetic heart valve endocarditis. JACC Cardiovasc. Imaging 2013, 6, 1008–1013. [Google Scholar] [CrossRef] [PubMed]
- Harding, D.; Cahill, T.J.; Redwood, S.R.; Prendergast, B.D. Infective endocarditis complicating transcatheter aortic valve implantation. Heart 2020, 106, 493–498. [Google Scholar] [CrossRef]
- Butt, J.H.; Ihlemann, N.; De Backer, O.; Søndergaard, L.; Havers-Borgersen, E.; Gislason, G.H.; Torp-Pedersen, C.; Køber, L.; Fosbøl, E.L. Long-Term Risk of Infective Endocarditis After Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2019, 73, 1646–1655. [Google Scholar] [CrossRef]
- Wahadat, A.R.; Tanis, W.; Swart, L.E.; Scholtens, A.; Krestin, G.P.; van Mieghem, N.; Schurink, C.A.M.; van der Spoel, T.I.G.; van den Brink, F.S.; Vossenberg, T.; et al. Added value of (18)F-FDG-PET/CT and cardiac CTA in suspected transcatheter aortic valve endocarditis. J. Nucl. Cardiol. 2019, 28, 2072–2082. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, M.; Kendi, A.T.; Farid, S.; Ajmal, S.; Johnson, G.B.; Baddour, L.M.; Chareonthaitawee, P.; Friedman, P.A.; Sohail, M.R. Role of (18)F-FDG PET/CT in the diagnosis of cardiovascular implantable electronic device infections: A meta-analysis. J. Nucl. Cardiol. 2019, 26, 958–970. [Google Scholar] [CrossRef]
- Juneau, D.; Golfam, M.; Hazra, S.; Zuckier, L.S.; Garas, S.; Redpath, C.; Bernick, J.; Leung, E.; Chih, S.; Wells, G.; et al. Positron Emission Tomography and Single-Photon Emission Computed Tomography Imaging in the Diagnosis of Cardiac Implantable Electronic Device Infection: A Systematic Review and Meta-Analysis. Circ. Cardiovasc. Imaging 2017, 10, e005772. [Google Scholar] [CrossRef] [PubMed]
- Sarrazin, J.F.; Philippon, F.; Tessier, M.; Guimond, J.; Molin, F.; Champagne, J.; Nault, I.; Blier, L.; Nadeau, M.; Charbonneau, L.; et al. Usefulness of fluorine-18 positron emission tomography/computed tomography for identification of cardiovascular implantable electronic device infections. J. Am. Coll. Cardiol. 2012, 59, 1616–1625. [Google Scholar] [CrossRef] [PubMed]
- Salomäki, S.P.; Saraste, A.; Kemppainen, J.; Hurme, S.; Knuuti, J.; Nuutila, P.; Seppänen, M.; Roivainen, A.; Airaksinen, J.; Salo, T.; et al. (18)F-FDG positron emission tomography/computed tomography of cardiac implantable electronic device infections. J. Nucl. Cardiol. 2020. [Google Scholar] [CrossRef]
- Rubini, G.; Ferrari, C.; Carretta, D.; Santacroce, L.; Ruta, R.; Iuele, F.; Lavelli, V.; Merenda, N.; D’Agostino, C.; Sardaro, A.; et al. Usefulness of (18)F-FDG PET/CT in Patients with Cardiac Implantable Electronic Device Suspected of Late Infection. J. Clin. Med. 2020, 9, 2246. [Google Scholar] [CrossRef] [PubMed]
- Graziosi, M.; Nanni, C.; Lorenzini, M.; Diemberger, I.; Bonfiglioli, R.; Pasquale, F.; Ziacchi, M.; Biffi, M.; Martignani, C.; Bartoletti, M.; et al. Role of ¹⁸F-FDG PET/CT in the diagnosis of infective endocarditis in patients with an implanted cardiac device: A prospective study. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1617–1623. [Google Scholar] [CrossRef]
- Holcman, K.; Małecka, B.; Rubiś, P.; Ząbek, A.; Szot, W.; Boczar, K.; Leśniak-Sobelga, A.; Hlawaty, M.; Wiśniowska-Śmiałek, S.; Stępień, A.; et al. The role of 99mTc-HMPAO-labelled white blood cell scintigraphy in the diagnosis of cardiac device-related infective endocarditis. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 1022–1030. [Google Scholar] [CrossRef]
- Jerónimo, A.; Olmos, C.; Vilacosta, I.; Ortega-Candil, A.; Rodríguez-Rey, C.; Pérez-Castejón, M.J.; Fernández-Pérez, C.; Pérez-García, C.N.; García-Arribas, D.; Ferrera, C.; et al. Accuracy of (18)F-FDG PET/CT in patients with the suspicion of cardiac implantable electronic device infections. J. Nucl. Cardiol. 2020. [Google Scholar] [CrossRef]
- Leccisotti, L.; Perna, F.; Lago, M.; Leo, M.; Stefanelli, A.; Calcagni, M.L.; Pelargonio, G.; Narducci, M.L.; Bencardino, G.; Bellocci, F.; et al. Cardiovascular implantable electronic device infection: Delayed vs standard FDG PET-CT imaging. J. Nucl. Cardiol. 2014, 21, 622–632. [Google Scholar] [CrossRef]
- Pizzi, M.N.; Dos-Subirà, L.; Roque, A.; Fernández-Hidalgo, N.; Cuéllar-Calabria, H.; Pijuan Domènech, A.; Gonzàlez-Alujas, M.T.; Subirana-Domènech, M.T.; Miranda-Barrio, B.; Ferreira-González, I.; et al. (18)F-FDG-PET/CT angiography in the diagnosis of infective endocarditis and cardiac device infection in adult patients with congenital heart disease and prosthetic material. Int. J. Cardiol. 2017, 248, 396–402. [Google Scholar] [CrossRef]
- Pizzi, M.N.; Roque, A.; Cuéllar-Calabria, H.; Fernández-Hidalgo, N.; Ferreira-González, I.; González-Alujas, M.T.; Igual-Barceló, A.; Garcia-Dorado, D.; Almirante, B.; Castell-Conesa, J.; et al. (18)F-FDG-PET/CTA of Prosthetic Cardiac Valves and Valve-Tube Grafts: Infective Versus Inflammatory Patterns. JACC Cardiovasc. Imaging 2016, 9, 1224–1227. [Google Scholar] [CrossRef]
- Goldstein, D.J.; Meyns, B.; Xie, R.; Cowger, J.; Pettit, S.; Nakatani, T.; Netuka, I.; Shaw, S.; Yanase, M.; Kirklin, J.K. Third Annual Report From the ISHLT Mechanically Assisted Circulatory Support Registry: A comparison of centrifugal and axial continuous-flow left ventricular assist devices. J. Heart Lung Transpl. 2019, 38, 352–363. [Google Scholar] [CrossRef] [PubMed]
- Kirklin, J.K.; Naftel, D.C.; Pagani, F.D.; Kormos, R.L.; Stevenson, L.W.; Blume, E.D.; Myers, S.L.; Miller, M.A.; Baldwin, J.T.; Young, J.B. Seventh INTERMACS annual report: 15,000 patients and counting. J. Heart Lung Transpl. 2015, 34, 1495–1504. [Google Scholar] [CrossRef] [PubMed]
- Dell’Aquila, A.M.; Avramovic, N.; Mastrobuoni, S.; Motekallemi, A.; Wisniewski, K.; Scherer, M.; Sindermann, J.R.; Wenning, C. Fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography for improving diagnosis of infection in patients on CF-LVAD: Longing for more ‘insights’. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 532–543. [Google Scholar] [CrossRef]
- Ten Hove, D.; Treglia, G.; Slart, R.; Damman, K.; Wouthuyzen-Bakker, M.; Postma, D.F.; Gheysens, O.; Borra, R.J.H.; Mecozzi, G.; van Geel, P.P.; et al. The value of (18)F-FDG PET/CT for the diagnosis of device-related infections in patients with a left ventricular assist device: A systematic review and meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 241–253. [Google Scholar] [CrossRef]
- Tam, M.C.; Patel, V.N.; Weinberg, R.L.; Hulten, E.A.; Aaronson, K.D.; Pagani, F.D.; Corbett, J.R.; Murthy, V.L. Diagnostic Accuracy of FDG PET/CT in Suspected LVAD Infections: A Case Series, Systematic Review, and Meta-Analysis. JACC Cardiovasc. Imaging 2020, 13, 1191–1202. [Google Scholar] [CrossRef]
- Kim, J.; Feller, E.D.; Chen, W.; Liang, Y.; Dilsizian, V. FDG PET/CT for Early Detection and Localization of Left Ventricular Assist Device Infection: Impact on Patient Management and Outcome. JACC Cardiovasc. Imaging 2019, 12, 722–729. [Google Scholar] [CrossRef]
- Avramovic, N.; Dell’Aquila, A.M.; Weckesser, M.; Milankovic, D.; Vrachimis, A.; Sindermann, J.R.; Wenning, C. Metabolic volume performs better than SUVmax in the detection of left ventricular assist device driveline infection. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1870–1877. [Google Scholar] [CrossRef]
- Lauri, C.; Iezzi, R.; Rossi, M.; Tinelli, G.; Sica, S.; Signore, A.; Posa, A.; Tanzilli, A.; Panzera, C.; Taurino, M.; et al. Imaging Modalities for the Diagnosis of Vascular Graft Infections: A Consensus Paper amongst Different Specialists. J. Clin. Med. 2020, 9, 1510. [Google Scholar] [CrossRef] [PubMed]
- Mikail, N.; Benali, K.; Dossier, A.; Bouleti, C.; Hyafil, F.; Le Guludec, D.; Rouzet, F.; Ou, P. Additional Diagnostic Value of Combined Angio-Computed Tomography and (18)F-Fluorodeoxyglucose Positron Emission Tomography in Infectious Aortitis. JACC Cardiovasc. Imaging 2018, 11, 361–364. [Google Scholar] [CrossRef]
- Reinders Folmer, E.I.; von Meijenfeldt, G.C.I.; Te Riet Ook Genaamd Scholten, R.S.; van der Laan, M.J.; Glaudemans, A.; Slart, R.; Zeebregts, C.J.; Saleem, B.R. A systematic review and meta-analysis of (18)F-fluoro-d-deoxyglucose positron emission tomography interpretation methods in vascular graft and endograft infection. J. Vasc. Surg. 2020, 72, 2174–2185.e2172. [Google Scholar] [CrossRef] [PubMed]
- Erba, P.A.; Conti, U.; Lazzeri, E.; Sollini, M.; Doria, R.; De Tommasi, S.M.; Bandera, F.; Tascini, C.; Menichetti, F.; Dierckx, R.A.; et al. Added value of 99mTc-HMPAO-labeled leukocyte SPECT/CT in the characterization and management of patients with infectious endocarditis. J. Nucl. Med. 2012, 53, 1235–1243. [Google Scholar] [CrossRef]
- Hyafil, F.; Rouzet, F.; Lepage, L.; Benali, K.; Raffoul, R.; Duval, X.; Hvass, U.; Iung, B.; Nataf, P.; Lebtahi, R.; et al. Role of radiolabelled leucocyte scintigraphy in patients with a suspicion of prosthetic valve endocarditis and inconclusive echocardiography. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 586–594. [Google Scholar] [CrossRef]
- Rouzet, F.; Chequer, R.; Benali, K.; Lepage, L.; Ghodbane, W.; Duval, X.; Iung, B.; Vahanian, A.; Le Guludec, D.; Hyafil, F. Respective performance of 18F-FDG PET and radiolabeled leukocyte scintigraphy for the diagnosis of prosthetic valve endocarditis. J. Nucl. Med. 2014, 55, 1980–1985. [Google Scholar] [CrossRef] [PubMed]
- Kooshki, N.; Grambow-Velilla, J.; Mahida, B.; Benali, K.; Nguyen, C.; Cimadevilla, C.; Braham, W.; Pisani, A.; Iung, B.; Raffoul, R.; et al. Diagnostic performance of White Blood Cell SPECT imaging against intra-operative findings in patients with a suspicion of prosthetic valve endocarditis. J. Nucl. Cardiol. 2021. [Google Scholar] [CrossRef]
- Holcman, K.; Rubiś, P.; Ząbek, A.; Ćmiel, B.; Szot, W.; Boczar, K.; Wiśniowska-Śmiałek, S.; Stępień, A.; Małecka, B.; Podolec, P.; et al. The Prognostic Value of (99)mTc-HMPAO-Labeled Leucocyte SPECT/CT in Cardiac Device-Related Infective Endocarditis. JACC Cardiovasc. Imaging 2020, 13, 1739–1751. [Google Scholar] [CrossRef] [PubMed]
- Imbert, L.; Poussier, S.; Franken, P.R.; Songy, B.; Verger, A.; Morel, O.; Wolf, D.; Noel, A.; Karcher, G.; Marie, P.Y. Compared performance of high-sensitivity cameras dedicated to myocardial perfusion SPECT: A comprehensive analysis of phantom and human images. J. Nucl. Med. 2012, 53, 1897–1903. [Google Scholar] [CrossRef]
- Ben-Haim, S.; Kennedy, J.; Keidar, Z. Novel Cadmium Zinc Telluride Devices for Myocardial Perfusion Imaging-Technological Aspects and Clinical Applications. Semin. Nucl. Med. 2016, 46, 273–285. [Google Scholar] [CrossRef]
- Caobelli, F.; Wollenweber, T.; Bavendiek, U.; Kühn, C.; Schütze, C.; Geworski, L.; Thackeray, J.T.; Bauersachs, J.; Haverich, A.; Bengel, F.M. Simultaneous dual-isotope solid-state detector SPECT for improved tracking of white blood cells in suspected endocarditis. Eur. Heart J. 2017, 38, 436–443. [Google Scholar] [CrossRef]
- de Vaugelade, C.; Mesguich, C.; Nubret, K.; Camou, F.; Greib, C.; Dournes, G.; Debordeaux, F.; Hindie, E.; Barandon, L.; Tlili, G. Infections in patients using ventricular-assist devices: Comparison of the diagnostic performance of (18)F-FDG PET/CT scan and leucocyte-labeled scintigraphy. J. Nucl. Cardiol. 2019, 26, 42–55. [Google Scholar] [CrossRef]
- Sollini, M.; Berchiolli, R.; Delgado Bolton, R.C.; Rossi, A.; Kirienko, M.; Boni, R.; Lazzeri, E.; Slart, R.; Erba, P.A. The “3M” Approach to Cardiovascular Infections: Multimodality, Multitracers, and Multidisciplinary. Semin. Nucl. Med. 2018, 48, 199–224. [Google Scholar] [CrossRef] [PubMed]
- Litzler, P.Y.; Manrique, A.; Etienne, M.; Salles, A.; Edet-Sanson, A.; Vera, P.; Bessou, J.P.; Hitzel, A. Leukocyte SPECT/CT for detecting infection of left-ventricular-assist devices: Preliminary results. J. Nucl. Med. 2010, 51, 1044–1048. [Google Scholar] [CrossRef] [PubMed]
- Erba, P.A.; Leo, G.; Sollini, M.; Tascini, C.; Boni, R.; Berchiolli, R.N.; Menichetti, F.; Ferrari, M.; Lazzeri, E.; Mariani, G. Radiolabelled leucocyte scintigraphy versus conventional radiological imaging for the management of late, low-grade vascular prosthesis infections. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Liberatore, M.; Misuraca, M.; Calandri, E.; Rizzo, L.; Speziale, F.; Iurilli, A.P.; Anagnostou, C. White blood cell scintigraphy in the diagnosis of infection of endovascular prostheses within the first month after implantation. Med. Sci. Monit. 2006, 12, MT5–MT9. [Google Scholar]
- Jensen, A.G.; Wachmann, C.H.; Espersen, F.; Scheibel, J.; Skinhøj, P.; Frimodt-Møller, N. Treatment and outcome of Staphylococcus aureus bacteremia: A prospective study of 278 cases. Arch. Intern. Med. 2002, 162, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Orvin, K.; Goldberg, E.; Bernstine, H.; Groshar, D.; Sagie, A.; Kornowski, R.; Bishara, J. The role of FDG-PET/CT imaging in early detection of extra-cardiac complications of infective endocarditis. Clin. Microbiol. Infect. 2015, 21, 69–76. [Google Scholar] [CrossRef]
- Kestler, M.; Muñoz, P.; Rodríguez-Créixems, M.; Rotger, A.; Jimenez-Requena, F.; Mari, A.; Orcajo, J.; Hernández, L.; Alonso, J.C.; Bouza, E. Role of (18)F-FDG PET in Patients with Infectious Endocarditis. J. Nucl. Med. 2014, 55, 1093–1098. [Google Scholar] [CrossRef]
- Van Riet, J.; Hill, E.E.; Gheysens, O.; Dymarkowski, S.; Herregods, M.C.; Herijgers, P.; Peetermans, W.E.; Mortelmans, L. (18)F-FDG PET/CT for early detection of embolism and metastatic infection in patients with infective endocarditis. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 1189–1197. [Google Scholar] [CrossRef] [PubMed]
- Vilacosta, I.; Graupner, C.; San Román, J.A.; Sarriá, C.; Ronderos, R.; Fernández, C.; Mancini, L.; Sanz, O.; Sanmartín, J.V.; Stoermann, W. Risk of embolization after institution of antibiotic therapy for infective endocarditis. J. Am. Coll. Cardiol. 2002, 39, 1489–1495. [Google Scholar] [CrossRef]
- Mikail, N.; Benali, K.; Mahida, B.; Vigne, J.; Hyafil, F.; Rouzet, F.; Le Guludec, D. (18)F-FDG-PET/CT Imaging to Diagnose Septic Emboli and Mycotic Aneurysms in Patients with Endocarditis and Cardiac Device Infections. Curr. Cardiol. Rep. 2018, 20, 14. [Google Scholar] [CrossRef]
- Bonfiglioli, R.; Nanni, C.; Morigi, J.J.; Graziosi, M.; Trapani, F.; Bartoletti, M.; Tumietto, F.; Ambrosini, V.; Ferretti, A.; Rubello, D.; et al. ¹⁸F-FDG PET/CT diagnosis of unexpected extracardiac septic embolisms in patients with suspected cardiac endocarditis. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 1190–1196. [Google Scholar] [CrossRef]
- Asmar, A.; Ozcan, C.; Diederichsen, A.C.; Thomassen, A.; Gill, S. Clinical impact of 18F-FDG-PET/CT in the extra cardiac work-up of patients with infective endocarditis. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Özcan, C.; Asmar, A.; Gill, S.; Thomassen, A.; Diederichsen, A.C. The value of FDG-PET/CT in the diagnostic work-up of extra cardiac infectious manifestations in infectious endocarditis. Int. J. Cardiovasc. Imaging 2013, 29, 1629–1637. [Google Scholar] [CrossRef]
- García-Cabrera, E.; Fernández-Hidalgo, N.; Almirante, B.; Ivanova-Georgieva, R.; Noureddine, M.; Plata, A.; Lomas, J.M.; Gálvez-Acebal, J.; Hidalgo-Tenorio, C.; Ruíz-Morales, J.; et al. Neurological complications of infective endocarditis: Risk factors, outcome, and impact of cardiac surgery: A multicenter observational study. Circulation 2013, 127, 2272–2284. [Google Scholar] [CrossRef]
- Spence, A.M.; Muzi, M.; Mankoff, D.A.; O’Sullivan, S.F.; Link, J.M.; Lewellen, T.K.; Lewellen, B.; Pham, P.; Minoshima, S.; Swanson, K.; et al. 18F-FDG PET of gliomas at delayed intervals: Improved distinction between tumor and normal gray matter. J. Nucl. Med. 2004, 45, 1653–1659. [Google Scholar]
- Chakraborty, T.; Scharf, E.; DeSimone, D.; El Rafei, A.; Brinjikji, W.; Baddour, L.M.; Wilson, W.; Steckelberg, J.M.; Fugate, J.E.; Wijdicks, E.F.M.; et al. Variable Significance of Brain MRI Findings in Infective Endocarditis and Its Effect on Surgical Decisions. Mayo Clin. Proc. 2019, 94, 1024–1032. [Google Scholar] [CrossRef]
- Shakhnovich, I.; Seabrook, G.R.; Brown, K.R.; Lewis, B.D.; Rossi, P.J. Ruptured mycotic infrapopliteal aneurysm. J. Vasc. Surg. 2013, 58, 205–207. [Google Scholar] [CrossRef]
- Mikail, N.; Benali, K.; Ou, P.; Slama, J.; Hyafil, F.; Le Guludec, D.; Rouzet, F. Detection of Mycotic Aneurysms of Lower Limbs by Whole-Body (18)F-FDG-PET. JACC Cardiovasc. Imaging 2015, 8, 859–862. [Google Scholar] [CrossRef]
- Granados, U.; Fuster, D.; Pericas, J.M.; Llopis, J.L.; Ninot, S.; Quintana, E.; Almela, M.; Paré, C.; Tolosana, J.M.; Falces, C.; et al. Diagnostic Accuracy of 18F-FDG PET/CT in Infective Endocarditis and Implantable Cardiac Electronic Device Infection: A Cross-Sectional Study. J. Nucl. Med. 2016, 57, 1726–1732. [Google Scholar] [CrossRef] [PubMed]
- Tlili, G.; Amraoui, S.; Mesguich, C.; Rivière, A.; Bordachar, P.; Hindié, E.; Bordenave, L. High performances of (18)F-fluorodeoxyglucose PET-CT in cardiac implantable device infections: A study of 40 patients. J. Nucl. Cardiol. 2015, 22, 787–798. [Google Scholar] [CrossRef] [PubMed]
- Amraoui, S.; Tlili, G.; Sohal, M.; Berte, B.; Hindié, E.; Ritter, P.; Ploux, S.; Denis, A.; Derval, N.; Rinaldi, C.A.; et al. Contribution of PET Imaging to the Diagnosis of Septic Embolism in Patients With Pacing Lead Endocarditis. JACC Cardiovasc. Imaging 2016, 9, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Erba, P.A.; Sollini, M.; Conti, U.; Bandera, F.; Tascini, C.; De Tommasi, S.M.; Zucchelli, G.; Doria, R.; Menichetti, F.; Bongiorni, M.G.; et al. Radiolabeled WBC scintigraphy in the diagnostic workup of patients with suspected device-related infections. JACC Cardiovasc. Imaging 2013, 6, 1075–1086. [Google Scholar] [CrossRef]
- Holcman, K.; Szot, W.; Rubiś, P.; Leśniak-Sobelga, A.; Hlawaty, M.; Wiśniowska-Śmiałek, S.; Małecka, B.; Ząbek, A.; Boczar, K.; Stępień, A.; et al. 99mTc-HMPAO-labeled leukocyte SPECT/CT and transthoracic echocardiography diagnostic value in infective endocarditis. Int. J. Cardiovasc. Imaging 2019, 35, 749–758. [Google Scholar] [CrossRef] [PubMed]
- Alagna, L.; Park, L.P.; Nicholson, B.P.; Keiger, A.J.; Strahilevitz, J.; Morris, A.; Wray, D.; Gordon, D.; Delahaye, F.; Edathodu, J.; et al. Repeat endocarditis: Analysis of risk factors based on the International Collaboration on Endocarditis—Prospective Cohort Study. Clin. Microbiol. Infect. 2014, 20, 566–575. [Google Scholar] [CrossRef] [PubMed]
- Delahaye, F.; M’Hammedi, A.; Guerpillon, B.; de Gevigney, G.; Boibieux, A.; Dauwalder, O.; Bouchiat, C.; Vandenesch, F. Systematic Search for Present and Potential Portals of Entry for Infective Endocarditis. J. Am. Coll. Cardiol. 2016, 67, 151–158. [Google Scholar] [CrossRef]
- Chu, V.H. When the Cat’s Out of the Bag: Searching for Portals of Entry in Infective Endocarditis. J. Am. Coll. Cardiol. 2016, 67, 159–161. [Google Scholar] [CrossRef][Green Version]
- Strum, W.B. Colorectal Adenomas. N. Engl. J. Med. 2016, 374, 1065–1075. [Google Scholar] [CrossRef]
- Gouriet, F.; Tissot-Dupont, H.; Casalta, J.P.; Hubert, S.; Cammilleri, S.; Riberi, A.; Lepidi, H.; Habib, G.; Raoult, D. FDG-PET/CT Incidental Detection of Cancer in Patients Investigated for Infective Endocarditis. Front. Med. 2020, 7, 535. [Google Scholar] [CrossRef] [PubMed]
- Holle, S.L.K.; Andersen, M.H.; Klein, C.F.; Bruun, N.E.; Tønder, N.; Haarmark, C.; Loft, A.; Høilund-Carlsen, P.F.; Bundgaard, H.; Iversen, K.K. Clinical usefulness of FDG-PET/CT for identification of abnormal extra-cardiac foci in patients with infective endocarditis. Int. J. Cardiovasc. Imaging 2020, 36, 939–946. [Google Scholar] [CrossRef]
- San, S.; Ravis, E.; Tessonier, L.; Philip, M.; Cammilleri, S.; Lavagna, F.; Norscini, G.; Arregle, F.; Martel, H.; Oliver, L.; et al. Prognostic Value of (18)F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in Infective Endocarditis. J. Am. Coll. Cardiol. 2019, 74, 1031–1040. [Google Scholar] [CrossRef]
- Diemberger, I.; Bonfiglioli, R.; Martignani, C.; Graziosi, M.; Biffi, M.; Lorenzetti, S.; Ziacchi, M.; Nanni, C.; Fanti, S.; Boriani, G. Contribution of PET imaging to mortality risk stratification in candidates to lead extraction for pacemaker or defibrillator infection: A prospective single center study. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 194–205. [Google Scholar] [CrossRef]
- Bergmans, T.; De Meester, P.; Herregods, M.C. Impact of nuclear imaging on diagnosis and management of infective endocarditis. Acta Cardiol. 2020, 75, 348–352. [Google Scholar] [CrossRef]
- Puges, M.; Bérard, X.; Ruiz, J.B.; Debordeaux, F.; Desclaux, A.; Stecken, L.; Pereyre, S.; Hocquelet, A.; Bordenave, L.; Pinaquy, J.B.; et al. Retrospective Study Comparing WBC scan and (18)F-FDG PET/CT in Patients with Suspected Prosthetic Vascular Graft Infection. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Lauridsen, T.K.; Iversen, K.K.; Ihlemann, N.; Hasbak, P.; Loft, A.; Berthelsen, A.K.; Dahl, A.; Dejanovic, D.; Albrecht-Beste, E.; Mortensen, J.; et al. Clinical utility of (18)F-FDG positron emission tomography/computed tomography scan vs. (99m)Tc-HMPAO white blood cell single-photon emission computed tomography in extra-cardiac work-up of infective endocarditis. Int. J. Cardiovasc. Imaging 2017, 33, 751–760. [Google Scholar] [CrossRef]
- Erba, P.A.; Lancellotti, P.; Vilacosta, I.; Gaemperli, O.; Rouzet, F.; Hacker, M.; Signore, A.; Slart, R.; Habib, G. Recommendations on nuclear and multimodality imaging in IE and CIED infections. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1795–1815. [Google Scholar] [CrossRef] [PubMed]
- Osborne, M.T.; Hulten, E.A.; Murthy, V.L.; Skali, H.; Taqueti, V.R.; Dorbala, S.; DiCarli, M.F.; Blankstein, R. Patient preparation for cardiac fluorine-18 fluorodeoxyglucose positron emission tomography imaging of inflammation. J. Nucl. Cardiol. 2017, 24, 86–99. [Google Scholar] [CrossRef]
- Scholtens, A.M.; Verberne, H.J.; Budde, R.P.; Lam, M.G. Additional Heparin Preadministration Improves Cardiac Glucose Metabolism Suppression over Low-Carbohydrate Diet Alone in ¹⁸F-FDG PET Imaging. J. Nucl. Med. 2016, 57, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Dietz, M.; Paulmier, B.; Berthier, F.; Civaia, F.; Mocquot, F.; Serrano, B.; Nataf, V.; Hugonnet, F.; Faraggi, M. An Intravenous 100-mL Lipid Emulsion Infusion Dramatically Improves Myocardial Glucose Metabolism Extinction in Cardiac FDG PET Clinical Practice. Clin. Nucl. Med. 2021, 46, e317–e324. [Google Scholar] [CrossRef]
- Casali, M.; Lauri, C.; Altini, C.; Bertagna, F.; Cassarino, G.; Cistaro, A.; Erba, A.P.; Ferrari, C.; Mainolfi, C.G.; Palucci, A.; et al. State of the art of (18)F-FDG PET/CT application in inflammation and infection: A guide for image acquisition and interpretation. Clin. Transl. Imaging 2021, 9, 299–399. [Google Scholar] [CrossRef]
- Jiménez-Ballvé, A.; Pérez-Castejón, M.J.; Delgado-Bolton, R.C.; Sánchez-Enrique, C.; Vilacosta, I.; Vivas, D.; Olmos, C.; Ferrer, M.E.; Carreras-Delgado, J.L. Assessment of the diagnostic accuracy of (18)F-FDG PET/CT in prosthetic infective endocarditis and cardiac implantable electronic device infection: Comparison of different interpretation criteria. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 2401–2412. [Google Scholar] [CrossRef]
- Friedman, S.N.; Mahmood, M.; Geske, J.R.; Sohail, M.R.; Johnson, G.B.; Stulak, J.M.; Kendi, A.T. Positron emission tomography objective parameters for assessment of left ventricular assist device infection using (18)F-FDG PET/CT. Am. J. Nucl. Med. Mol. Imaging 2020, 10, 301–311. [Google Scholar]
- Memmott, M.J.; James, J.; Armstrong, I.S.; Tout, D.; Ahmed, F. The performance of quantitation methods in the evaluation of cardiac implantable electronic device (CIED) infection: A technical review. J. Nucl. Cardiol. 2016, 23, 1457–1466. [Google Scholar] [CrossRef]
- Erba, P.A.; Pizzi, M.N.; Roque, A.; Salaun, E.; Lancellotti, P.; Tornos, P.; Habib, G. Multimodality Imaging in Infective Endocarditis: An Imaging Team Within the Endocarditis Team. Circulation 2019, 140, 1753–1765. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.H.; Kim, Y.J.; Kim, S.H.; Sun, B.J.; Kim, D.H.; Yun, S.C.; Song, J.M.; Choo, S.J.; Chung, C.H.; Song, J.K.; et al. Early surgery versus conventional treatment for infective endocarditis. N. Engl. J. Med. 2012, 366, 2466–2473. [Google Scholar] [CrossRef] [PubMed]
- Andrews, M.M.; von Reyn, C.F. Patient selection criteria and management guidelines for outpatient parenteral antibiotic therapy for native valve infective endocarditis. Clin. Infect. Dis. 2001, 33, 203–209. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Major Criteria | 1. Microbiological Criteria |
| a. Microorganisms typical of IE evidenced from two separate blood cultures | |
| |
| b. Microorganisms consistent with IE evidenced from persistently positive blood cultures: | |
| |
| 2. Imaging Criteria | |
| a. Echocardiogram positive for IE showing one/several of the following typical findings | |
| |
| b. Nuclear medicine imaging positive for IE, i.e., abnormal uptake around the site of prosthetic valve implantation | |
| |
| c. Cardiac CT | |
| |
| Minor Criteria | 1. Predisposing condition such as heart condition, or intravenous drug use |
| 2. Fever defined as temperature >38 °C | |
| 3. Vascular phenomena including those detected only by imaging, major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, and Janeway’s lesions | |
| 4. Immunological phenomena: glomerulonephritis, Osler’s nodes, Roth’s spots, and rheumatoid factor | |
| 5. Microbiological evidence: positive blood culture, but does not meet a major criterion as noted above, or serological evidence of active infection with organism consistent with IE |
| Definite IE | Histopathological Criteria |
| Demonstration of a microorganism from a culture, a cardiac vegetation, an embolized vegetation, or an intracardiac abscess, OR Demonstration of an active endocarditis from a vegetation or an intracardiac abscess | |
| Clinical Criteria | |
| 2 major criteria, OR 1 major criterion AND 3 minor criteria, OR 5 minor criteria | |
| Possible IE | 1 major criterion AND 1 minor criterion, OR 3 minor criteria |
| Rejected IE | Firm alternate diagnosis, OR Resolution of symptoms within ≤4 days of antibiotherapy, OR No pathological evidence of IE (surgery or autopsy) after ≤4 days of antibiotherapy, OR No criteria for possible IE as defined above |
| Advantages | Drawbacks | |
| 18F-FDG-PET/CT | High sensitivity for PVE and device-related IE (CIED pocket and extracardiac lead) | Moderate sensitivity for NVE and intracardiac lead CIED-IE |
| Good spatial resolution (4–5 mm) | Moderate specificity for infection | |
| Short protocol (preparation and acquisition <2 h) | Requires a specific diet to suppress the physiological cardiac uptake of 18F-FDG | |
| Whole-body imaging in 15–20 min. allowing for the detection of device infection and septic emboli | Post-surgery inflammation in case of PVE (cautious interpretation 1–3 months after surgery) | |
| Identification of possible portal of entry | Limited sensitivity in organs with high FDG uptake, especially the brain | |
| Identification of alternate diagnosis for infectious or inflammatory syndrome than IE | Possible false-negative results in small vegetations and/or after prolonged antibiotherapy | |
| Radiation exposure | ||
| WBC-SPECT/CT | High specificity | Moderate sensitivity, especially for CIED-IE |
| No need for specific diet nor interaction with sugar levels for imaging | Long and complex procedure requiring blood handling | |
| Relatively low spatial resolution (8–10 mm) | Possible false-negative results in small vegetations and/or prolonged antibiotherapy | |
| Lower imaqe quality (late imaging time point and SPECT acquistions) | Radiation exposure | |
| Potential detection of septic emboli, but lower performance than 18F-FDG-PET/CT |
| Major Criteria | 1. Microbiological Criteria |
| a. Microorganisms typical of CIED-IE and/or IE (Coagulase-negative staphylococci, Staphylococcus aureus) | |
| b. Microorganisms typical of IE evidenced from two separate blood cultures | |
| |
| c. Microorganisms consistent with IE evidenced from persistently positive blood cultures: | |
| |
| 2. Imaging Criteria | |
| a. Echocardiogram positive for CIED-IE: | |
| clinical pocket/generator infectionlead-vegetation | |
| b. Nuclear medicine imaging positive for CIED-IE, i.e., abnormal uptake around pocket/generator site or along leads | |
| |
| Minor criteria | 1. Predisposing condition such as heart condition or intravenous drug use |
| 2. Fever defined as temperature >38 °C | |
| 3. Vascular phenomena including those detected only by imaging, major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, and Janeway’s lesions | |
| 4. Microbiological evidence: positive blood culture but does not meet a major criterion as noted above or serological evidence of active infection with organism consistent with CIED-IE |
| Echocardiography | CCTA | Cardiac MRI | 18F-FDG-PET/CT | WBC-SPECT/CT | |
|---|---|---|---|---|---|
| Diagnostic Performances for IE Diagnosis |
|
|
|
|
|
| Evaluation of Cardiac Complications |
|
|
|
|
|
| Cardiac Presurgical Assessment |
|
|
|
|
|
| Extracardiac Assessment |
|
|
|
|
|
| Contra-Indications |
|
|
|
|
|
| Availability |
|
|
|
|
|
| Limitations and drawbacks |
|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mikail, N.; Hyafil, F. Nuclear Imaging in Infective Endocarditis. Pharmaceuticals 2022, 15, 14. https://doi.org/10.3390/ph15010014
Mikail N, Hyafil F. Nuclear Imaging in Infective Endocarditis. Pharmaceuticals. 2022; 15(1):14. https://doi.org/10.3390/ph15010014
Chicago/Turabian StyleMikail, Nidaa, and Fabien Hyafil. 2022. "Nuclear Imaging in Infective Endocarditis" Pharmaceuticals 15, no. 1: 14. https://doi.org/10.3390/ph15010014
APA StyleMikail, N., & Hyafil, F. (2022). Nuclear Imaging in Infective Endocarditis. Pharmaceuticals, 15(1), 14. https://doi.org/10.3390/ph15010014