
Janus Kinase Inhibitors and Coronavirus Disease (COVID)-19: Rationale, Clinical Evidence and Safety Issues

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Pharmacological Aspects of JAK Inhibitors
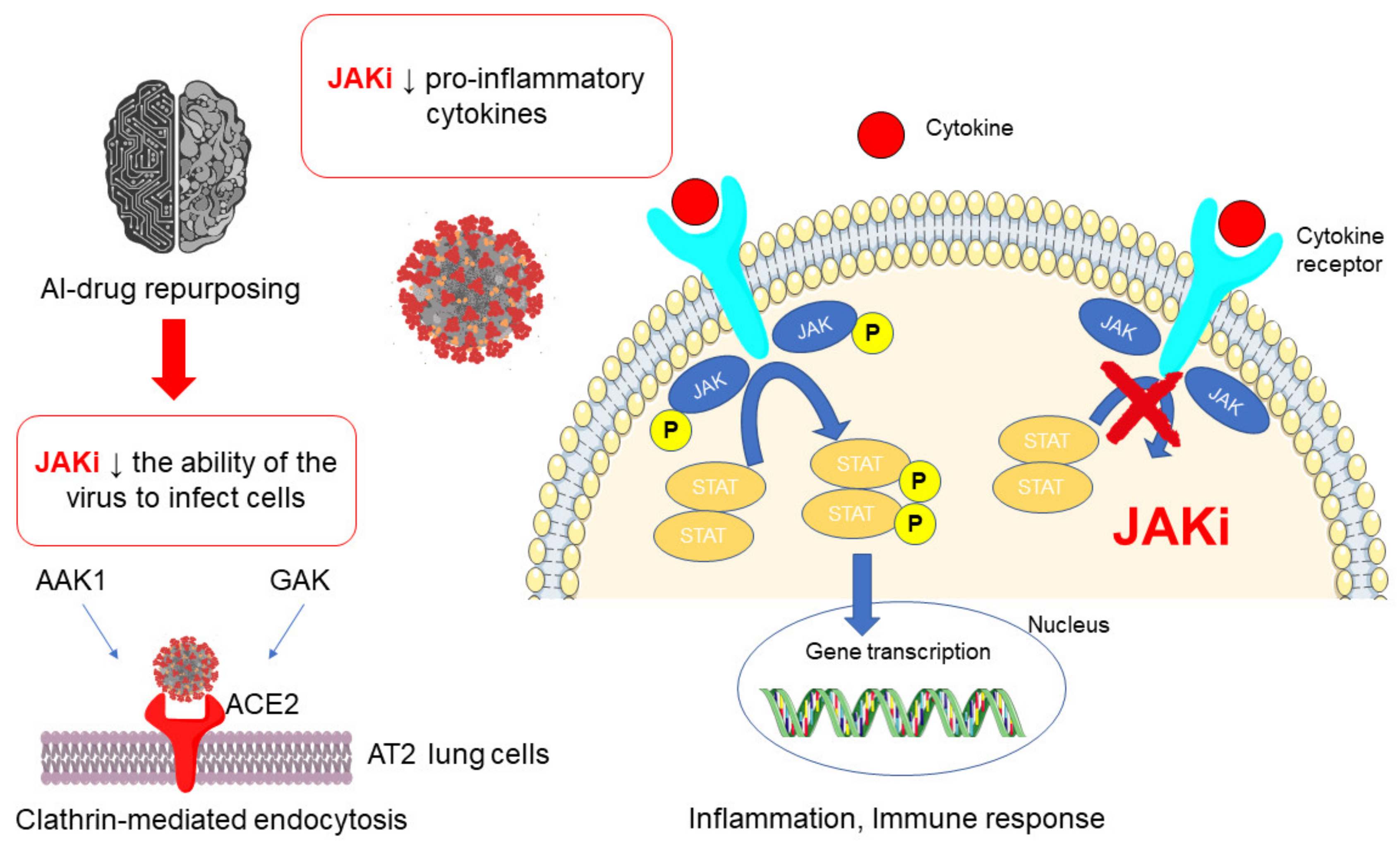
3. JAK Inhibitors and SARS-CoV-2: Rationale and Regulatory Affairs
4. Clinical Evidence with JAK Inhibitors in COVID-19 Settings
4.1. Baricitinib
4.2. Ruxolitinib
5. Safety issues
5.1. Safety Profile of JAK Inhibitors in Immune-Mediated Diseases
5.2. Cardiovascular Risk with JAK Inhibitors in Immune-Mediated Diseases
5.3. Safety Issues with JAK Inhibitors of Interest in the Setting of COVID-19
5.4. Adverse Events of Clinical Interest with Baricitinib from Pharmacovigilance
6. Conclusions and Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siemieniuk, R.A.; Bartoszko, J.J.; Ge, L.; Zeraatkar, D.; Izcovich, A.; Kum, E.; Pardo-Hernandez, H.; Qasim, A.; Martinez, J.P.D.; Rochwerg, B. Update to living systematic review on drug treatments for COVID-19. BMJ 2021, 372, n858. [Google Scholar] [CrossRef]
- Sultana, J.; Crisafulli, S.; Gabbay, F.; Lynn, E.; Shakir, S.; Trifirò, G. Challenges for drug repurposing in the COVID-19 pandemic era. Front. Pharmacol. 2020, 11, 1657. [Google Scholar] [CrossRef] [PubMed]
- Pushpakom, S.; Iorio, F.; Eyers, P.A.; Escott, K.J.; Hopper, S.; Wells, A.; Doig, A.; Guilliams, T.; Latimer, J.; McNamee, C.; et al. Drug repurposing: Progress, challenges and recommendations. Nat. Rev. Drug Discov. 2019, 18, 41–58. [Google Scholar] [CrossRef] [PubMed]
- Jourdan, J.P.; Bureau, R.; Rochais, C.; Dallemagne, P. Drug repositioning: A brief overview. J. Pharm. Pharmacol. 2020, 72, 1145–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghofrani, H.A.; Osterloh, I.H.; Grimminger, F. Sildenafil: From angina to erectile dysfunction to pulmonary hypertension and beyond. Nat. Rev. Drug Discov. 2006, 5, 689–702. [Google Scholar] [CrossRef]
- Gatti, M.; De Ponti, F. Drug Repurposing in the COVID-19 Era: Insights from Case Studies Showing Pharmaceutical Peculiarities. Pharmaceutics 2021, 13, 302. [Google Scholar] [CrossRef] [PubMed]
- Scavone, C.; Mascolo, A.; Rafaniello, C.; Sportiello, L.; Trama, U.; Zoccoli, A.; Bernardi, F.F.; Racagni, G.; Berrino, L.; Castaldo, G.; et al. Therapeutic strategies to fight COVID-19: Which is the status artis? Br. J. Pharmacol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, F.R.; Meylan, F.; O’Shea, J.J.; Gadina, M. JAK inhibitors: Ten years after. Eur. J. Immunol. 2021, 51, 1615–1627. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.M.; Cooles, F.A.; Isaacs, J.D. Basic Mechanisms of JAK Inhibition. Mediterr. J. Rheumatol. 2020, 31, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Muller, R. JAK inhibitors in 2019, synthetic review in 10 points. Eur. J. Intern. Med. 2019, 66, 9–17. [Google Scholar] [CrossRef]
- Veeravalli, V.; Dash, R.P.; Thomas, J.A.; Babu, R.J.; Madgula, L.M.V.; Srinivas, N.R. Critical Assessment of Pharmacokinetic Drug—Drug Interaction Potential of Tofacitinib, Baricitinib and Upadacitinib, the Three Approved Janus Kinase Inhibitors for Rheumatoid Arthritis Treatment. Drug Saf. 2020, 43, 711–725. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, F.; Tang, J.; Nussinov, R.; Cheng, F. Artificial intelligence in COVID-19 drug repurposing. Lancet Digit. Health 2020, 2, e667–e676. [Google Scholar] [CrossRef]
- Richardson, P.; Griffin, I.; Tucker, C.; Smith, D.; Oechsle, O.; Phelan, A.; Rawling, M.; Savory, E.; Stebbing, J. Baricitinib as potential treatment for 2019-nCoV acute respiratory disease. Lancet 2020, 395, e30–e31. [Google Scholar] [CrossRef] [Green Version]
- Stebbing, J.; Krishnan, V.; de Bono, S.; Ottaviani, S.; Casalini, G.; Richardson, P.J.; Monteil, V.; Lauschke, V.M.; Mirazimi, A.; Youhanna, S.; et al. Mechanism of baricitinib supports artificial intelligence—Predicted testing in COVID-19 patients. EMBO Mol. Med. 2020, 12, e12697. [Google Scholar] [CrossRef]
- Stebbing, J.; Phelan, A.; Griffin, I.; Tucker, C.; Oechsle, O.; Smith, D.; Richardson, P. COVID-19: Combining antiviral and anti-inflammatory treatments. Lancet Infect. Dis. 2020, 20, 400–402. [Google Scholar] [CrossRef]
- Botta, C.; Indrieri, A.; Garofalo, E.; Biamonte, F.; Bruni, A.; Pasqua, P.; Cesario, F.; Costanzo, F.S.; Longhini, F.; Mendicino, F. COVID-19: High-JAKing of the Inflammatory “Flight” by Ruxolitinib to Avoid the Cytokine Storm. Front. Oncol. 2020, 10, 599502. [Google Scholar] [CrossRef]
- Cantini, F.; Niccoli, L.; Matarrese, D.; Nicastri, E.; Stobbione, P.; Goletti, D. Baricitinib therapy in COVID-19: A pilot study on safety and clinical impact. J. Infect. 2020, 81, 318–356. [Google Scholar] [CrossRef]
- Jorgensen, S.C.; Tse, C.L.; Burry, L.; Dresser, L.D. Baricitinib: A review of pharmacology, safety, and emerging clinical experience in COVID-19. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2020, 40, 843–856. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, C.G.; Allon, S.J.; Nyquist, S.K.; Mbano, I.M.; Miao, V.N.; Tzouanas, C.N.; Cao, Y.; Yousif, A.S.; Bals, J.; Hauser, B.M. SARS-CoV-2 receptor ACE2 is an interferon-stimulated gene in human airway epithelial cells and is detected in specific cell subsets across tissues. Cell 2020, 181, 1016–1035.e19. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Vardeny, O.; Michel, T.; McMurray, J.J.; Pfeffer, M.A.; Solomon, S.D. Renin–angiotensin–aldosterone system inhibitors in patients with COVID-19. N. Engl. J. Med. 2020, 382, 1653–1659. [Google Scholar] [CrossRef] [PubMed]
- Bronte, V.; Ugel, S.; Tinazzi, E.; Vella, A.; De Sanctis, F.; Canè, S.; Batani, V.; Trovato, R.; Fiore, A.; Petrova, V.; et al. Baricitinib restrains the immune dysregulation in patients with severe COVID-19. J. Clin. Investig. 2020, 130, 6409–6416. [Google Scholar] [CrossRef] [PubMed]
- Cantini, F.; Niccoli, L.; Nannini, C.; Matarrese, D.; Natale, M.E.D.; Lotti, P.; Aquilini, D.; Landini, G.; Cimolato, B.; Pietro, M.A.D.; et al. Beneficial impact of Baricitinib in COVID-19 moderate pneumonia; multicentre study. J. Infect. 2020, 81, 647–679. [Google Scholar] [CrossRef]
- Cingolani, A.; Tummolo, A.M.; Montemurro, G.; Gremese, E.; Larosa, L.; Cipriani, M.C.; Pasciuto, G.; Liperoti, R.; Murri, R.; Pirronti, T.; et al. Baricitinib as rescue therapy in a patient with COVID-19 with no complete response to sarilumab. Infection 2020, 48, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Rosas, J.; Liaño, F.P.; Cantó, M.L.; Barea, J.M.C.; Beser, A.R.; Rabasa, J.T.A.; Adsuar, F.M.; Auli, B.V.; López, I.F.; Sainz, A.M.G.; et al. Experience With the Use of Baricitinib and Tocilizumab Monotherapy or Combined, in Patients With Interstitial Pneumonia Secondary to Coronavirus COVID19: A Real-World Study. Reumatol. Clin. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Stebbing, J.; Nievas, G.S.; Falcone, M.; Youhanna, S.; Richardson, P.; Ottaviani, S.; Shen, J.X.; Sommerauer, C.; Tiseo, G.; Ghiadoni, L.; et al. JAK inhibition reduces SARS-CoV-2 liver infectivity and modulates inflammatory responses to reduce morbidity and mortality. Sci. Adv. 2021, 7, eabe4724. [Google Scholar] [CrossRef] [PubMed]
- Titanji, B.K.; Farley, M.M.; Mehta, A.; Connor-Schuler, R.; Moanna, A.; Cribbs, S.K.; O’Shea, J.; DeSilva, K.; Chan, B.; Edwards, A.; et al. Use of baricitinib in patients with moderate to severe coronavirus disease 2019. Clin. Infect. Dis. 2021, 72, 1247–1250. [Google Scholar] [CrossRef] [PubMed]
- Hasan, M.J.; Rabbani, R.; Anam, A.M.; Huq, S.M.R. Additional baricitinib loading dose improves clinical outcome in COVID-19. Open Med. 2021, 16, 41–46. [Google Scholar] [CrossRef]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus Remdesivir for Hospitalized Adults with COVID-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Garcia, J.L.; Sanchez-Nievas, G.; Arevalo-Serrano, J.; Garcia-Gomez, C.; Jimenez-Vizuete, J.M.; Martinez-Alfaro, E. Baricitinib improves respiratory function in patients treated with corticosteroids for SARS-CoV-2 pneumonia: An observational cohort study. Rheumatology 2021, 60, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Betelli, M.; De Stefano, F.; Tedeschi, A. Late Worsening of COVID-19 Pneumonia: Successful Treatment with Ruxolitinib and Steroid. Eur. J. Case Rep. Intern. Med. 2020, 7, 001938. [Google Scholar] [CrossRef]
- Cao, Y.; Wei, J.; Zou, L.; Jiang, T.; Wang, G.; Chen, L.; Huang, L.; Meng, F.; Wang, N.; Zhou, X.; et al. Ruxolitinib in treatment of severe coronavirus disease 2019 (COVID-19): A multicenter, single-blind, randomized controlled trial. J. Allergy Clin. Immunol. 2020, 146, 137–146.e3. [Google Scholar] [CrossRef]
- Capochiani, E.; Frediani, B.; Iervasi, G.; Paolicchi, A.; Sani, S.; Roncucci, P.; Cuccaro, A.; Franchi, F.; Simonetti, F.; Carrara, D.; et al. Ruxolitinib Rapidly Reduces Acute Respiratory Distress Syndrome in COVID-19 Disease. Analysis of Data Collection From RESPIRE Protocol. Front. Med. 2020, 7, 466. [Google Scholar] [CrossRef]
- Caradec, E.; Mouren, D.; Zrounba, M.; Azoulay, L.D.; Blandin, C.; Ivanoff, S.; Levy, V.; Brillet, P.Y.; Nunes, H.; Uzunhan, Y. COVID-19 in a patient with idiopathic pulmonary fibrosis successfully treated with Ruxolitinib. Respir. Med. Res. 2020, 79, 100799. [Google Scholar] [CrossRef] [PubMed]
- Foss, F.M.; Rubinowitz, A.; Landry, M.L.; Isufi, I.; Gowda, L.; Seropian, S.; Perreault, S.; Shenoi, S.V. Attenuated Novel SARS Coronavirus 2 Infection in an Allogeneic Hematopoietic Stem Cell Transplant Patient on Ruxolitinib. Clin. Lymphoma Myeloma Leuk. 2020, 20, 720–723. [Google Scholar] [CrossRef] [PubMed]
- Gaspari, V.; Zengarini, C.; Greco, S.; Vangeli, V.; Mastroianni, A. Side effects of ruxolitinib in patients with SARS-CoV-2 infection: Two case reports. Int. J. Antimicrob. Agents 2020, 56, 106023. [Google Scholar] [CrossRef]
- Giudice, V.; Pagliano, P.; Vatrella, A.; Masullo, A.; Poto, S.; Polverino, B.M.; Gammaldi, R.; Maglio, A.; Sellitto, C.; Vitale, C.; et al. Combination of Ruxolitinib and Eculizumab for Treatment of Severe SARS-CoV-2-Related Acute Respiratory Distress Syndrome: A Controlled Study. Front. Pharmacol. 2020, 11, 857. [Google Scholar] [CrossRef]
- Innes, A.J.; Cook, L.B.; Marks, S.; Bataillard, E.; Crossette-Thambiah, C.; Sivasubramaniam, G.; Apperley, J.; Milojkovic, D. Ruxolitinib for tocilizumab-refractory severe COVID-19 infection. Br. J. Haematol. 2020, 190, e198–e200. [Google Scholar] [CrossRef]
- Koschmieder, S.; Jost, E.; Cornelissen, C.; Müller, T.; Schulze-Hagen, M.; Bickenbach, J.; Marx, G.; Kleines, M.; Marx, N.; Brümmendorf, T.H.; et al. Favorable COVID-19 course despite significant comorbidities in a ruxolitinib—Treated patient with primary myelofibrosis. Eur. J. Haematol. 2020, 105, 655–658. [Google Scholar] [CrossRef] [PubMed]
- La Rosée, F.; Bremer, H.; Gehrke, I.; Kehr, A.; Hochhaus, A.; Birndt, S.; Fellhauer, M.; Henkes, M.; Kumle, B.; Russo, S.; et al. The Janus kinase 1/2 inhibitor ruxolitinib in COVID-19 with severe systemic hyperinflammation. Leukemia 2020, 34, 1805–1815. [Google Scholar] [CrossRef] [PubMed]
- Sammartano, V.; Santoni, A.; Frediani, B.; Sicuranza, A.; Emanuele, C.; Franchi, F.; Capochiani, E.; Bocchia, M. Efficacy and safety of ruxolitinib for COVID-19 related acute respiratory distress syndrome in a patient with blastic plasmacytoid dendritic cell neoplasm (leukemic variant). Leuk. Lymphoma 2020, 61, 3523–3525. [Google Scholar] [CrossRef]
- Vannucchi, A.M.; Sordi, B.; Morettini, A.; Nozzoli, C.; Poggesi, L.; Pieralli, F.; Bartoloni, A.; Atanasio, A.; Miselli, F.; Paoli, C.; et al. Compassionate use of JAK1/2 inhibitor ruxolitinib for severe COVID-19: A prospective observational study. Leukemia 2021, 35, 1121–1133. [Google Scholar] [CrossRef]
- Mortara, A.; Mazzetti, S.; Margonato, D.; Delfino, P.; Bersano, C.; Catagnano, F.; Lauriola, M.; Grosso, P.; Perseghin, G.; Ippoliti, G. Compassionate use of Ruxolitinib in patients with SarsCov-2 infection not on mechanical ventilation. Short-term effects on inflammation and ventilation. Clin. Transl. Sci. 2021, 14, 1062–1068. [Google Scholar] [CrossRef]
- Saraceni, F.; Scortechini, I.; Mancini, G.; Mariani, M.; Federici, I.; Gaetani, M.; Barbatelli, P.; Minnucci, M.L.; Bagnarelli, P.; Olivieri, A. Severe COVID-19 in a patient with chronic graft-versus-host disease after hematopoietic stem cell transplant successfully treated with ruxolitinib. Transpl. Infect. Dis. 2021, 23, e13401. [Google Scholar] [CrossRef]
- Gatti, M.; Raschi, E.; Moretti, U.; Ardizzoni, A.; Poluzzi, E.; Diemberger, I. Influenza Vaccination and Myo-Pericarditis in Patients Receiving Immune Checkpoint Inhibitors: Investigating the Likelihood of Interaction through the Vaccine Adverse Event Reporting System and VigiBase. Vaccines 2021, 9, 19. [Google Scholar] [CrossRef] [PubMed]
- Araujo, A.G.; Borba, H.H.; Tonin, F.S.; Lenzi, L.; Venson, R.; Pontarolo, R.; Wiens, A. Safety of biologics approved for the treatment of rheumatoid arthritis and other autoimmune diseases: A disproportionality analysis from the FDA Adverse Event Reporting System (FAERS). BioDrugs 2018, 32, 377–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raschi, E.; Gatti, M.; Gelsomino, F.; Ardizzoni, A.; Poluzzi, E.; De Ponti, F. Lessons to be learnt from real-world studies on immune-related adverse events with checkpoint inhibitors: A clinical perspective from Pharmacovigilance. Target. Oncol. 2020, 15, 449–466. [Google Scholar] [CrossRef]
- Winthrop, K.L. The emerging safety profile of JAK inhibitors in rheumatic disease. Nat. Rev. Rheumatol. 2017, 13, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Olivera, P.A.; Lasa, J.S.; Bonovas, S.; Danese, S.; Peyrin-Biroulet, L. Safety of Janus kinase inhibitors in patients with inflammatory bowel diseases or other immune-mediated diseases: A systematic review and meta-analysis. Gastroenterology 2020, 158, 1554–1573.e12. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Xiao, K.; Ottaviani, S.; Stebbing, J.; Wang, Y.-J. A real-world disproportionality analysis of FDA Adverse Event Reporting System (FAERS) events for baricitinib. Expert Opin. Drug Saf. 2020, 19, 1505–1511. [Google Scholar] [CrossRef]
- Anand, K.; Burns, E.A.; Ensor, J.; Rice, L.; Pingali, S.R. Mycobacterial infections with ruxolitinib: A retrospective pharmacovigilance review. Clin. Lymphoma Myeloma Leuk. 2020, 20, 18–23. [Google Scholar] [CrossRef] [Green Version]
- Scott, I.C.; Hider, S.L.; Scott, D.L. Thromboembolism with Janus kinase (JAK) inhibitors for rheumatoid arthritis: How real is the risk? Drug Saf. 2018, 41, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.; Huang, Y.; Xiao, S.; Sun, X.; Fan, Y.; Zhang, Z. Impact of Janus kinase inhibitors on risk of cardiovascular events in patients with rheumatoid arthritis: Systematic review and meta-analysis of randomised controlled trials. Ann. Rheum. Dis. 2019, 78, 1048–1054. [Google Scholar] [CrossRef]
- Nurmohamed, M.; Choy, E.; Lula, S.; Kola, B.; DeMasi, R.; Accossato, P. The impact of biologics and tofacitinib on cardiovascular risk factors and outcomes in patients with rheumatic disease: A systematic literature review. Drug Saf. 2018, 41, 473–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, F.; Scott, D.L. Thromboembolism and Janus Kinase Inhibitors. Drug Saf. 2020, 43, 831–833. [Google Scholar] [CrossRef] [PubMed]
- Kotyla, P.J.; Engelmann, M.; Giemza-Stokłosa, J.; Wnuk, B.; Islam, M.A. Thromboembolic adverse drug reactions in Janus Kinase (JAK) inhibitors: Does the inhibitor specificity play a role? Int. J. Mol. Sci. 2021, 22, 2449. [Google Scholar] [CrossRef]
- Verden, A.; Dimbil, M.; Kyle, R.; Overstreet, B.; Hoffman, K.B. Analysis of spontaneous postmarket case reports submitted to the FDA regarding thromboembolic adverse events and JAK inhibitors. Drug Saf. 2018, 41, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Vallejo-Yagüe, E.; Weiler, S.; Micheroli, R.; Burden, A.M. Thromboembolic safety reporting of tofacitinib and baricitinib: An analysis of the WHO VigiBase. Drug Saf. 2020, 43, 881–891. [Google Scholar] [CrossRef]
- Setyawan, J.; Azimi, N.; Strand, V.; Yarur, A.; Fridman, M. Reporting of Thromboembolic Events with JAK Inhibitors: Analysis of the FAERS Database 2010–2019. Drug Saf. 2021, 44, 889–897. [Google Scholar] [CrossRef]
- Kulkarni, A.V.; Kumar, P.; Tevethia, H.V.; Premkumar, M.; Arab, J.P.; Candia, R.; Talukdar, R.; Sharma, M.; Qi, X.; Rao, P.N.; et al. Systematic review with meta-analysis: Liver manifestations and outcomes in COVID-19. Aliment. Pharmacol. Ther. 2020, 52, 584–599. [Google Scholar] [CrossRef] [PubMed]
- Raschi, E.; Caraceni, P.; Poluzzi, E.; De Ponti, F. Baricitinib, JAK inhibitors and liver injury: A cause for concern in COVID-19? Expert Opin. Drug Saf. 2020, 19, 1367–1369. [Google Scholar] [CrossRef]
- Gatti, M.; Raschi, E.; Poluzzi, E.; Martignani, C.; Salvagni, S.; Ardizzoni, A.; Diemberger, I. The Complex Management of Atrial Fibrillation and Cancer in the COVID-19 Era: Drug Interactions, Thromboembolic Risk, and Proarrhythmia. Curr. Heart Fail. Rep. 2020, 17, 365–383. [Google Scholar] [CrossRef] [PubMed]
- Alim, K.; Bruyère, A.; Lescoat, A.; Jouan, E.; Lecureur, V.; Le Vée, M.; Fardel, O. Interactions of janus kinase inhibitors with drug transporters and consequences for pharmacokinetics and toxicity. Expert Opin. Drug Metab. Toxicol. 2021, 17, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Umehara, K.; Huth, F.; Jin, Y.; Schiller, H.; Aslanis, V.; Heimbach, T.; He, H. Drug-drug interaction (DDI) assessments of ruxolitinib, a dual substrate of CYP3A4 and CYP2C9, using a verified physiologically based pharmacokinetic (PBPK) model to support regulatory submissions. Drug Metab. Pers. Ther. 2019, 34. [Google Scholar] [CrossRef]
- Gatti, M.; Fusaroli, M.; Caraceni, P.; Poluzzi, E.; De Ponti, F.; Raschi, E. Serious adverse events with tocilizumab: Pharmacovigilance as an aid to prioritize monitoring in COVID-19. Br. J. Clin. Pharmacol. 2021, 87, 1533–1540. [Google Scholar] [CrossRef] [PubMed]
- Goletti, D.; Cantini, F. Baricitinib Therapy in COVID-19 Pneumonia—An Unmet Need Fulfilled. N. Engl. J. Med. 2021, 384, 867–869. [Google Scholar] [CrossRef]
- Guimarães, P.O.; Quirk, D.; Furtado, R.H.; Maia, L.N.; Saraiva, J.F.; Antunes, M.O.; Kalil Filho, R.; Junior, V.M.; Soeiro, A.M.; Tognon, A.P.; et al. Tofacitinib in Patients Hospitalized with COVID-19 Pneumonia. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Chen, C.-x.; Wang, J.-j.; Li, H.; Yuan, L.-t.; Gale, R.P.; Liang, Y. JAK-inhibitors for coronavirus disease-2019 (COVID-19): A meta-analysis. Leukemia 2021, 1–5. [Google Scholar] [CrossRef]
- Singh, D.; Bogus, M.; Moskalenko, V.; Lord, R.; Moran, E.J.; Crater, G.D.; Bourdet, D.L.; Pfeifer, N.D.; Woo, J.; Kaufman, E.; et al. A phase 2 multiple ascending dose study of the inhaled pan-JAK inhibitor nezulcitinib (TD-0903) in severe COVID-19. Eur. Respir. J. 2021, 2100673. [Google Scholar] [CrossRef]


{kind=link}
| JAK Inhibitors | Main PK Features | PD Features/JAK Targeting | Approved Indication |
|---|---|---|---|
| Baricitinib | Protein binding: 50% t1/2: 12 h Metabolism: CYP3A4 Elimination: urinary (69%)/biliary (15%) | ATP competitive kinase inhibitor that selectively, strongly, and reversibly inhibits JAK1 (IC50 5.9 nM) and JAK2 (IC50 5.7 nM) | Rheumatoid arthritis (FDA, EMA) |
| Ruxolitinib | Protein binding: 97% t1/2: 3 h Metabolism: CYP3A4 (<50%) and CYP2C9 Elimination: urinary (74%)/biliary (22%) | Selective inhibitor of JAK1 (IC50 3.3 nM) and JAK2 (IC50 2.8 nM) | Myelofibrosis, polycythemia vera (FDA, EMA) |
| Fedratinib | Protein binding: 95% Terminal t1/2: 114 h Metabolism: CYP3A4 (major), CYP2C19 and FMOs Elimination: urinary (5%)/biliary (77%) | JAK2-selective inhibitor | Myelofibrosis (FDA, EMA) |
| Tofacitinib | Protein binding: 40% t1/2: 3 h Metabolism: CYP3A4 (major), CYP2C19 Elimination: urinary (30%)/biliary (70%) | Potent and selective inhibitor of JAK1 and JAK3 | Rheumatoid arthritis, psoriatic arthritis (FDA, EMA), and ulcerative colitis (EMA) |
| Upadacitinib | Protein binding: 52% t1/2: 9–14 h Metabolism: CYP3A4 (major), CYP2D6 Elimination: urinary (24%)/biliary (38%) | Selective and reversible inhibitor of JAK1 | Rheumatoid arthritis (FDA, EMA) |
| Filgotinib | Protein binding: 55–59% Terminal t1/2: 7 h Metabolism: CES2 (major), CES1 Elimination: urinary (87%)/biliary (15%) | Inhibitor of JAK1 | Rheumatoid arthritis (EMA) |
| Study Reference | Study Design | No. Patients | Intervention Group | Comparator Group | Primary Outcome | Secondary Outcome | Safety Assessment |
|---|---|---|---|---|---|---|---|
| Kalil et al., 2021 [28] | RCT, double-blind, multicenter (USA, Singapore, South Korea, Mexico, Japan, Spain, Denmark, and UK) | 1033 | Baricitinib + Remdesivir (n = 515) Baricitinib: 4 mg/day for 14 days Remdesivir: 200 mg day 1–100 mg day 2–10 | Placebo + Remdesivir (n = 518) Remdesivir: 200 mg day 1–100 mg day 2–10 | Median time to recovery: 7 days versus 8 days (RR 1.16; CI 1.01–1.32; p = 0.03) Median time to recovery (patients receiving non-invasive ventilation or high-flow oxygen): 10 days versus 18 days (RR 1.51; CI 1.10–2.08) No difference in median time to recovery in patients receiving mechanical ventilation or ECMO | Clinical status at day 15 (odds of improvement): OR 1.3 (CI 1.0–1.6) 14-day mortality rate: 1.6% versus 3.0% (HR 0.54; CI 0.23–1.28) 28-day mortality rate: 5.1% versus 7.8% (HR 0.65; CI 0.39–1.09) Incidence of new use of oxygen: (−17.4%; CI −31.6 to −2.1) Incidence of new use of invasive ventilation or ECMO: (−5.2%; CI −9.5 to −0.9) | Serious AEs 16.0% versus 21.0% (difference −5.0 percentage points; CI −9.8 to −0.3; p = 0.03) New infections 5.9% versus 11.2% (difference −5.3 percentage points; CI −8.7 to −1.9; p = 0.003) |
| Stebbing et al., 2021 [25] | Observational, prospective, multicenter, propensity score matching | 166 | Baricitinib 2–4 mg/day (n = 83) | Standard of care (Hydroxychloroquine + Lopinavir/Ritonavir + Corticosteroids) (n = 83) | Primary composite endpoint of death or invasive mechanical ventilation: 16.9% versus 34.9% (p < 0.001) | Baricitinib was independently associated as a protective variable with the primary outcome at multivariate regression analysis (HR 0.29; CI 0.15–0.58; p < 0.001) | Transaminase increase (19%) Bacterial infection(14%) |
| Hasan et al., 2020 [27] | Observational, prospective, case–control (Bangladesh) | 37 COVID-19 moderate-severe pneumonia | Baricitinib 4 mg/day after 8 mg LD (n = 20) | Baricitinib 4 mg/day without LD (n = 17) | Median days required to stop the need of supplement oxygen: 5 versus 8 (p = 0.001) ICU admission rate: 10% versus 29.4% (p = 0.005) | Median length of hospital stay: 12 versus 15 (p = 0.028) No difference in 30-day mortality rate | - |
| Rodriguez-Garcia et al., 2020 [29] | Observational prospective (Spain) | 112 COVID-19 moderate-severe pneumonia | Baricitinib + standard of care (Hydroxychloroquine + Lopinavir/Ritonavir + corticosteroids) (n = 62) | Standard of care (n = 50) | Improvement in SpO2/FiO2: mean difference 49 (p < 0.001) No difference in mortality and ICU admission rate | Proportion of patients required supplemental oxygen: risk reduction of 82% and 69%, respectively at discharge (p < 0.001) and at 1 month (p = 0.024) | - |
| Cantini et al., 2020 [22] | Observational retrospective, multicenter, longitudinal (Italy) | 191 COVID-19 moderate pneumonia | Baricitinib 4 mg/day for 14 days + Lopinavir/Ritonavir 250 mg × 2/day for 14 days (n = 113) | Hydroxychloroquine 400 mg/day + Lopinavir/Ritonavir 250 mg × 2/day (n = 78) | 14-day mortality rate: 0.0% versus 6.4% (p = 0.01) | ICU admission: 0.88% versus 17.9% (p = 0.019) Hospital discharge rate (at 2 weeks): 77.8% versus 12.8% (p < 0.0001) | Transaminase increase (3.5%) |
| Cantini et al., 2020 [17] | Observational retrospective (Italy) | 24 COVID-19 moderate pneumonia | Baricitinib 4 mg/day for 14 days + Lopinavir/Ritonavir 250 mg × 2/day for 14 days (n = 12) | Hydroxychloroquine 400 mg/day + Lopinavir/Ritonavir 250 mg × 2/day (n= 12) | Hospital discharge at 2-week:58% versus 8% (p = 0.027) | Significant improvement in P/F ratio and CRP levels | No serious AEs One case of baricitinib withdrawal |
| Bronte et al., 2020 [21] | Observational retrospective, Longitudinal (Italy) | 76 | Baricitinib 4 mg × 2/day days 1–2 + 4 mg/day days 3–9 + standard of care (n = 20) | Standard of care (Hydroxychloroquine + Lopinavir/Ritonavir) (n = 56) | Mortality rate: 5% versus 45% (p < 0.001) No difference in ARDS incidence or disease duration | Faster reduction in the need for oxygen flow therapy (p < 0.001) and a more rapid increase in the P/F ratio compared with the control group (p = 0.02), as well as a reduction in serum levels of CRP (p < 0.001) | - |
| Rosas et al., 2020 [24] | Observational retrospective (Spain) | 60 | Baricitinib 2–4 mg/day ± Tocilizumab 400–600 mg single dose (n = 23) | Standard of care ± Tocilizumab (n = 37) | No difference in mortality or ICU admission rate | Significant reduction in mean respiratory rate at discharge (20 versus 24; p < 0.05) | No serious AEs |
| Titanji et al., 2020 [26] | Observational retrospective cohort, non-controlled (USA) | 15 COVID-19 moderate-severe pneumonia | Baricitinib 2–4 mg/day + Hydroxychloroquine 200–400 mg/day | - | ICU admission: 60% Overall mortality rate: 20% Reduction in CRP level: 86.7% Recovery rate: 80%Clinical improvement: 73.3% | - | - |
| Stebbing et al., 2020 [14] | Case series (Italy) | 4 | Baricitinib 2–4 mg/day for 10–12 days | - | Moderate-severe disease: 75% Clinical improvement: 100% | - | Transient increase in serum transaminases in all four patients |
| Cingolani et al., 2020 [23] | Case report (Italy) | 1 | Baricitinib 4 mg × 2/day for 14 days after sub-intensive care unit admission | Failure to standard of care (Lopinavir/Ritonavir + Hydroxychloroquine + Azithromycin) + Sarilumab 400 mg on day 1 and 4 | Constant increase in the pO2 coupled with progressive decrease in required FiO2 | - | - |
| Study Reference | Study Design | No. Patients | Intervention Group | Comparator Group | Primary Outcome | Secondary Outcome | Safety Assessment |
|---|---|---|---|---|---|---|---|
| Cao et al., 2020 [31] | Randomized controlled, multicentre, single-blind (China) | 43 severe COVID-19 pneumonia | Ruxolitinib 5 mg × 2/day + standard of care (antivirals + corticosteroids and supportive treatment) (n = 22) | Placebo + standard of care (antivirals + corticosteroids and supportive treatment) (n = 21) | Median time to clinical improvement: 12 days versus 15 days (p = 0.147) | Significant improvement on chest CT scan at 14 days: 90% vs. 61.9% (p = 0.0495) 28-day mortality rate: 0.0% vs. 14.3% (p = 0.232) | No difference in serious AEs |
| Giudice et al., 2020 [36] | Observational prospective, monocentric (Italy) | 17 severe COVID-19 pneumonia | Ruxolitinib 10 mg × 2/day for 14 days + Eculizumab 900 mg/week (n = 7) | Best available therapy (Hydroxychloroquine + Azithromycin + Heparin) (n = 10) | Improvement in median PaO2 after 7 days: 94 versus 77 (p = 0.026) Improvement in median PaO2/FiO2 after 7 days: 370.5 versus 246 (p = 0.0395) | No significant difference in mortality rate and duration of hospitalization | Increase in transaminase levels: 71.4% |
| Vannucchi et al., 2020 [41] | Observational prospective, monocentric (Italy) | 34 | Ruxolitinib 5–10 mg × 2/day | - | Clinical improvement in 85.3% of cases (reduction of at least 2 points in seven-point ordinal scale) Less frequent clinical improvement in patients with more severe respiratory impairment HR 0.31 (CI 0.1–1.0) | CRP levels significantly decreased from a baseline median level of 72 mg/l (IQR, 39–111) to 26 mg/l (IQR, 5–76; p = 0.03) by day 7 and normalized by day 14 (12 mg/l, IQR, 6–21; p < 0.001) | Discontinuation of treatment in 14.7% |
| Mortara et al., 2021 [42] | Observational prospective, monocentric (Italy) | 31 | Ruxolitinib 5 mg × 2/day for 15 days | - | Improvement in symptoms (Likert scale) at 7 and 15 days: 80.6% and 90.3% | - | No AEs observed during treatment |
| Capochiani et al., 2020 [32] | Observational retrospective cohort, multicenter (Italy) | 18 ARDS due to COVID-19 | Ruxolitinib 20 mg × 2/day in day 1–2, 5–10 mg × 2/day up to day 14 (n = 18) | - | No evolution from NIV to mechanical ventilation: 88.9% Significant improvement in respiratory response within 48 h: 88.9% | 14-day complete respiratory function: 88.9% Rapid restoration within 48 h in PaO2/FiO2: 88.9% | No AEs observed during treatment and at the follow-up |
| La Rosée et al., 2020 [39] | Observational retrospective, monocentric (Germany) | 14 severe COVID-19 pneumonia | Ruxolitinib 7.5 mg × 2/day with subsequent reassessment for increase or decrease in dosage | - | Reduction by 25% in COVID-19 inflammatory score achieved after 5 days | - | One patient transient grade 3 liver toxicityTwo patients experienced grade 3 anaemia |
| Gaspari et al., 2020 [35] | Case report (Italy) | 2 | (a) Ruxolitinib 5 mg × 2/day on day 1–2 and 10 mg × 2/day on day 3–5 (b) Ruxolitinib 5 mg × 2/day on day 1–7 | - | - | - | (a) Skin purpuric lesion associated with reduction in platelet count (b) Erythrodermic rash on whole body surface |
| Sammartano et al., 2020 [40] | Case report (Italy) | 1 | Ruxolitinib 20 mg × 2/day | Prior clinical failure with therapy including Hydroxychloroquine, Azithromycin, Corticosteroids, and Tocilizumab | COVID-19 related ARDS in a patient with diagnosis of Blastic Plasmocitoid Dendritic Cell Neoplasm Clinical improvement after 48 h with CPAP discontinuation | - | - |
| Saraceni et al., 2021 [43] | Case report (Italy) | 1 | Ruxolitinib 5 mg × 2/day for chronic GVHD after allogeneic stem cell transplant, discontinued at hospital admission for COVID-19 pneumonia and re-started after clinical failure with standard of care | Hydroxychloroquine, Lopinavir-Ritonavir, and LMWH | Rapid improvement in respiratory function and hospital discharge at day 45 | - | No reported AEs |
| Innes et al., 2020 [37] | Case report (UK) | 1 | Ruxolitinib 5 mg × 2/day on day 1 × 3 and 10 mg × 2/day on day 4 × 21 | Prior clinical failure with intermediate dosage of LMWH and tocilizumab | Improvement in respiratory function and hospital discharge at day 28 | - | No reported AEs |
| Koschmieder et al., 2020 [38] | Case report (Germany) | 1 | Ruxolitinib 10 mg × 2/day chronic treatment (since 15 months) for myelofibrosis | - | ICU admission (no required mechanical ventilation) Rapid improvement in respiratory function and hospital discharge at day 15 | - | No reported AEs |
| Caradec et al., 2020 [33] | Case report (France) | 1 | Ruxolitinib 10 mg × 2/day | Prior clinical failure with Hydroxychloroquine + Azithromycin | Improvement in respiratory function after 48 h and CRP normalization at day 8 | - | No reported AEs |
| Foss et al., 2020 [34] | Case report (USA) | 1 | Ruxolitinib 10 mg × 2/day for chronic GVHD after allogeneic stem cell transplant | - | Attenuated COVID-19 infection in an immunosuppressed patient in chronic treatment with ruxolitinib | - | - |
| Betelli et al., 2020 [30] | Case report (Italy) | 1 | Ruxolitinib 5 mg × 2/day for 14 days + Dexamethasone 20 mg/day for 5 day and subsequent decalage | Prior clinical failure with standard of care (Hydroxychloroquine + Azithromycin) | Oxygen supplementation suspended after 14 days Hospital discharge after 23 days | - | - |
| Pharmacokinetic Feature | DDIs with JAK-Inhibitors | Clinical Relevance and Literature Data | ||
|---|---|---|---|---|
| Baricitinib | Ruxolitinib | |||
| P-gp substrate | - | Weak inhibitor | ||
| CYP3A4 substrate | Minor (only 10%) | Major (CYP2C9/CYP2D9 minor) | ||
| BCRP substrate | Substrate Weak inhibitor (only in vitro) | Weak inhibitor | ||
| OAT substrate | OAT3 substrate OAT1/3 inhibitor (only in vitro) | Weak inhibitor (only in vitro) | ||
| COVID-19 agents | Metabolic pathway | |||
| Remdesivir | CYP2C8–CYP2C19–CYP3A4–P-gp–OATP1B1 substrate | No relevant interactions expected | ||
| Dexamethasone | CYP3A4 substrate–moderate CYP3A4 inducer | No relevant interactions expected | ||
| Colchicine | CYP3A4 and P-gp substrate | Risk of increased colchicine exposure with concomitant use of ruxolitinib, particularly in patients with renal or hepatic impairment | ||
| IL6 inhibitors | Restoration of CYP3A4 and CYP2C19 activity | Risk of additive immunosuppression | ||
| Favipiravir | CYP2C8, OAT1, and OAT3 moderate inhibitor | Favipiravir may increase baricitinib exposure, but not in a clinically relevant extent | ||
| Drug | QT prolongation */arrhythmia | Myo-pericarditis | MACE | VTE |
|---|---|---|---|---|
| JAK inhibitors | ||||
| Remdesivir | § | |||
| Dexamethasone | ||||
| Colchicine | # | |||
| IL6 inhibitors | ||||
| Favipiravir |
| Toxicity Areas | AE of Clinical Interest Reported with Baricitinib | No. Patients | No. Deaths | Proportion of Death | Seriousness | Mean Age | Sex | Weight (Kg) | Concomitant Drugs Used for COVID-19 Management | Other Relevant Concomitant Medications Implicated in Specific AE of Clinical Interest |
|---|---|---|---|---|---|---|---|---|---|---|
| Cardiotoxicity | Hypotension (6) Bradycardia (2) Tachycardia (1) Ventricular extrasystoles (1) Atrial fibrillation (1) Ventricular tachycardia (1) | 8 | 6 | 75.0% | 100.0% | 61.9 ± 16.6 | 4 M–4 F | 94.7 ± 28.1 | 8 Remdesivir 8 Dexamethasone 1 COVID-19 convalescent plasma1 Methylprednisone | - |
| Hepatotoxicity | Alanine aminotransferase increased (5) Aspartate aminotransferase increased (5) Liver function test increased (3) Drug-induced liver injury (1) Liver disorder (1) Transaminase increased (1) | 9 | 0 | 0.0% | 100.0% | 64.4 ± 12.8 | 4 M–5 F | 97.0 ± 37.4 | 8 Remdesivir 6 Dexamethasone 1 Enoxaparin | 1 Azithromycin 1 Ceftriaxone 1 Cefepime 1 Fluconazole |
| Infection | Septic shock (7) Sepsis (2) Infection (3) Pneumonia staphylococcal (4) Urinary tract infection (2) Candida infection (2) Pneumonia (2) Staphylococcal infection (2) Bacterial infection (2) Candida test positive (2) Other infections * | 25 | 8 | 32.0% | 100.0% | 59.4 ± 16.0 | 13 M–12 F | 102.5 ± 35.6 | 25 Remdesivir 21 Dexamethasone 5 Methylprednisone 2 Heparin 2 COVID-19 convalescent plasma1 Prednisone | - |
| Nephrotoxicity | Acute kidney injury (11) Renal impairment (3) Renal failure (1) Renal disorder (1) | 16 | 9 | 56.3% | 100.0% | 62.1 ± 14.6 | 7 M–9 F | 94.9 ± 23.7 | 15 Remdesivir 14 Dexamethasone 2 Methylprednisone 1 Prednisone 1 Heparin | 3 Piperacillin-tazobactam 1 Vancomycin |
| Thromboembolic events | Deep vein thrombosis (4) Pulmonary embolism (4) Embolism (2) Vena Cava thrombosis (1) Thrombosis (1) Embolism venous (1) | 13 | 5 | 38.5% | 100.0% | 65.2 ± 16.4 | 6 M–6 F–1 NS | 102.2 ± 50.0 | 10 Remdesivir 6 Dexamethasone 2 Methylprednisone 2 Enoxaparin 2 Heparin | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gatti, M.; Turrini, E.; Raschi, E.; Sestili, P.; Fimognari, C. Janus Kinase Inhibitors and Coronavirus Disease (COVID)-19: Rationale, Clinical Evidence and Safety Issues. Pharmaceuticals 2021, 14, 738. https://doi.org/10.3390/ph14080738
Gatti M, Turrini E, Raschi E, Sestili P, Fimognari C. Janus Kinase Inhibitors and Coronavirus Disease (COVID)-19: Rationale, Clinical Evidence and Safety Issues. Pharmaceuticals. 2021; 14(8):738. https://doi.org/10.3390/ph14080738
Chicago/Turabian StyleGatti, Milo, Eleonora Turrini, Emanuel Raschi, Piero Sestili, and Carmela Fimognari. 2021. "Janus Kinase Inhibitors and Coronavirus Disease (COVID)-19: Rationale, Clinical Evidence and Safety Issues" Pharmaceuticals 14, no. 8: 738. https://doi.org/10.3390/ph14080738
APA StyleGatti, M., Turrini, E., Raschi, E., Sestili, P., & Fimognari, C. (2021). Janus Kinase Inhibitors and Coronavirus Disease (COVID)-19: Rationale, Clinical Evidence and Safety Issues. Pharmaceuticals, 14(8), 738. https://doi.org/10.3390/ph14080738