
Therapeutic Use of Valproic Acid and All-Trans Retinoic Acid in Acute Myeloid Leukemia—Literature Review and Discussion of Possible Use in Relapse after Allogeneic Stem Cell Transplantation


 ,
,  and
and
Abstract
1. Introduction
2. Experimental and Clinical Studies of Valproic Acid in Non-APL Variants of AML
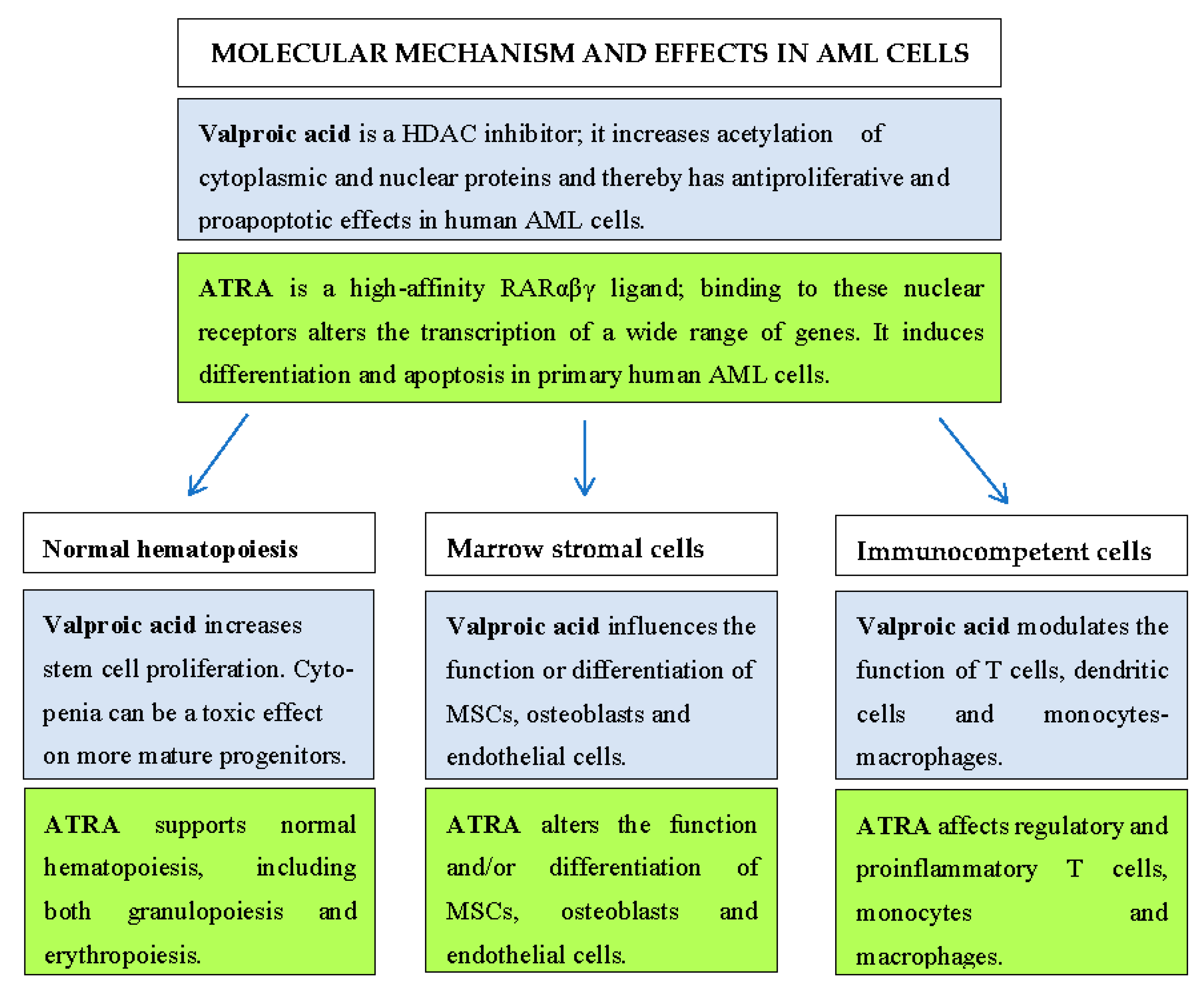
2.1. Experimental Studies of Valproic Acid Effects on AML Cells
2.2. In Vivo Effects of Valproic Acid in AML: Clinical Studies and Animal Models
2.3. Effects of Valproic Acid on Normal Hematopoietic and Bone Marrow STROMAL cells
2.4. Effects of Valproic Acid on Normal Immunocompetent Cells
- T cells. Valproic acid has strong antiproliferative but not proapoptotic effects on T cells in the presence of cytarabine, and it can also alter the expression of the activation markers CD38 and CD69 as well as the release of FasL, heat shock protein (HSP)90, and various cytokines [36]. The levels of regulatory T cells are increased during AML stabilizing treatment with ATRA and valproic acid [37].
- Dendritic cells. Valproic acid inhibits the release of IFN-α, TNFα, and IL-6 by plasmacytoid dendritic cells; reduces their expression of costimulatory molecules as well as their capacity to promote CD4+ T cell proliferation and IFN-γ production; and increases the proportion of anti-inflammatory IL-10-positive T cells [38]. The drug also downregulates group I CD1 expression; reduces the secretions of IL-6, IL-10, and IL-23 and TNF-α release; increases IL-8 release; and reduces the capacity to promote differentiation of Th17 cells in human monocyte-derived immature dendritic cells [39]. Furthermore, a third study showed that valproic acid causes downregulation of the (co)stimulatory molecules CD40, CD80, CD83, CD86, and HLA-DR and decreases IL-10 and IL-12p70 production in mature dendritic cells [40]. These last authors also suggested that the proportion of IFN-γ+CD4+ alloreactive T cells and the granzyme B expression by CD8+ T cells were both decreased when these cells were cocultured with dendritic cells that were previously exposed to valproic acid. Finally, HDAC inhibition can reduce CD1a expression together with the capacity of chemokine-induced migration, immunostimulatory capacity, and cytokine release in monocyte-derived dendritic cells [41]. These last effects seem to be caused by inhibited signaling through NFκB, IRF-3, and IRF-8.
- Monocytes/macrophages. Low levels of valproic acid alter the differentiation of human monocyte-derived macrophages and their expressions of CXCL8/IL-8, IL-1β, IL-6, TNFα, and IL-10 (but not IL-12), whereas higher valproic acid levels reduce the release of cytokines in general [42]. Furthermore, valproic acid can enhance the expansion of nonclassical macrophages [43], with an overexpression of CD163 (but no effect on CD86 expression), decreased IL1-β and TNFα expression, as well as increased expressions of anti-inflammatory IL-10 and TGF-β1.
2.5. Altered Systemic Mediator Levels and Metabolic Regulation during Treatment with Valproic Acid in AML Patients
3. Experimental and Clinical Studies of ATRA in Non-APL Variants of AML
3.1. Experimental and Clinical Studies of ATRA Effects on AML Cells
- FLT3-ITD. Studies in an animal model of FLT3-ITD/NPM1c-driven AML suggest that ATRA has an antileukemic effect in this AML model through effects on leukemic stem cells, but this pharmacological effect is counteracted by experimental expression of the stem cell-associated transcription factor EVI1 [58].
- NPM1 mutations. Experimental studies suggest that ATRA can lead to degradation of mutated NPM1 with re-localization of NPM1-wt encoded by the second gene and therefore can induce cell cycle arrest, differentiation, and increased sensitivity to conventional cytotoxic drugs [68,69]. These observations are supported by certain clinical studies, as described above [59,60].
- IDH1 mutations. Experimental studies suggest that patients with IDH1 mutations are more sensitive to ATRA [70].
- High MN1 expression. MN1 encodes a transcription cofactor that is a member of the RAR/RXR complex, and high expression is associated with resistance to ATRA [61].
- High EVI1 expression. This gene encodes a stem cell-associated transcription factor that is downregulated during hematopoietic differentiation. High expression is observed for 10% of AML patients and is associated with an adverse prognosis [58,71,72,73]. This factor is upregulated by ATRA [74,75,76], and high EVI1 levels seem to enhance the transcriptional response to ATRA [77], thereby causing differentiation induction, decreased clonogenic proliferation, and decreased AML engraftment in immunocompromised mice [78]. These antileukemic effects seem to be caused by the effects of ATRA on the AML stem cells for patients with stem cell-derived leukemia and therefore high EVI1 expression, but the effect is weak or absent in AML derived from progenitor cell transformation and shows low EVI1 expression [79]. However, this effect of EVF1 expression is probably more complex because it may be further modulated by other genetic abnormalities [58].
3.2. Effects of ATRA on Normal Hematopoietic and Bone Marrow Stromal Cells
3.3. Effects of Vitamin A/ATRA on Normal Immunocompetent Cells
3.4. Altered Metabolic Regulation during Treatment with ATRA in AML Patients
3.5. The Complexity of Combining Valproic Acid and ATRA in the Treatment of AML
3.6. Valproic Acid/ATRA Based Anti-AML Therapy: What Can We Learn from Proteomic and Phosphoproteomic Studies
4. Clinical Studies of Valproic Acid and ATRA in AML
- Only a minority of patients (approximately 25–35%) respond to this treatment.
- Most responders show stabilized disease when using the MDS response criteria (see Section 6.2). Exceptional patients achieve complete hematological remission, but this is usually seen when valproic acid is combined with ATRA plus low-toxicity chemotherapy.
- The most common response is stabilized/increased peripheral blood platelet counts, and for most patients, the duration of such responses is 2–5 months, although exceptional patients without complete hematological remission have responses that last for 12–18 months. The improvement in platelet counts can be from pretreatment levels below 10 × 109/L to stabilization at or above 20–50 × 109/L.
- Toxic effects are usually dose-dependent and reversible, and the most common toxicities are gastrointestinal side effects and fatigue.
5. Panobinostat—An Alternative HDAC Inhibitor to Valproic Acid in AML Therapy
6. The Treatment of Post-Allotransplant AML Relapse with ATRA, Valproic Acid, Hydroxyurea, and Azacitidine Illustrated by Four Case Reports
6.1. A Treatment Protocol for the Use of Valproic Acid and ATRA in Low-Toxicity Combination Therapy
6.2. What Should the Response Criteria Be for Patients Receiving AML Stabilizing Treatment?
6.3. Case Reports
6.3.1. Case Report 1
6.3.2. Case Report 2
6.3.3. Case Report 3
6.3.4. Case Report 4
6.3.5. Comments to the Case Reports
7. The Current Treatment for AML Relapse after Allogeneic Stem Cell Transplantation
7.1. The Hypomethylating Agents Azacitidine and Decitabine
7.2. Posttransplant Immunomodulation
7.3. Intensive Induction Chemotherapy and Retransplantation
8. Quality of Life for AML Patients
8.1. Quality of Life for AML Patients Receiving Intensive and Leukemia-Stabilizing Therapy
8.2. Quality of Life after Allogeneic Stem Cell Transplantation
9. Summarizing Comments
9.1. Alternative Pharmacological Combinations
9.2. Alternative HDAC Inhibitors
9.3. Possible Effects on Graft Versus Leukemia (GVL) Effects
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reivam, H.; Kittang, A.O.; Melve, G.; Mosevoll, K.A.; Bentsen, P.T.; Ersvaer, E.; Gjertsen, B.T.; Bruserud, Ø. Targeted anti-leukemic therapy as disease-stabilizing treatment for acute myeloid leukemia relapse after allogeneic stem cell transplantation: Will it be possible to combine these strategies with retransplantation or donor lymphocyte infusions? Curr. Cancer Drug Targets 2013, 13, 30–47. [Google Scholar] [CrossRef]
- Rautenberg, C.; Germing, U.; Haas, R.; Kobbe, G.; Schroeder, T. Relapse of acute myeloid leukemia after allogeneic stem cell transplantation: Prevention, detection, and treatment. Int. J. Mol. Sci. 2019, 20, 228. [Google Scholar] [CrossRef]
- Fredly, H.; Gjertsen, B.T.; Bruserud, Ø. Histone deacetylase inhibition in the treatment of acute myeloid leukemia: The effects of valproic acid on leukemic cells, and the clinical and experimental evidence for combining valproic acid with other antileukemic agents. Clin. Epigenetics 2013, 5, 12. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.H.; Grandits, A.M.; Purton, L.E.; Sill, H.; Wieser, R. All-trans retinoic acid in non-promyelocytic acute myeloid leukemia: Driver lesion dependent effects on leukemic stem cells. Cell. Cycle 2020, 19, 2573–2588. [Google Scholar] [CrossRef]
- Gronningsaeter, I.S.; Fredly, H.K.; Gjertsen, B.T.; Hatfield, K.J.; Bruserud, Ø. Systemic metabolomic profiling of acute myeloid leukemia patients before and during disease-stabilizing treatment based on all-trans retinoic acid, valproic acid, and low-dose chemotherapy. Cells 2019, 8, 1229. [Google Scholar] [CrossRef]
- Martino, O.D.; Welch, J.S. Retinoic acid receptors in acute myeloid leukemia therapy. Cancers 2019, 11, 1915. [Google Scholar] [CrossRef] [PubMed]
- Acharya, S.; Bussel, J.B. Hematologic toxicity of sodium valproate. J. Pediatr. Hematol. Oncol. 2000, 22, 62–65. [Google Scholar] [CrossRef]
- Zimran, E.; Papa, L.; Djedaini, M.; Patel, A.; Iancu-Rubin, C.; Hoffman, R. Expansion and preservation of the functional activity of adult hematopoietic stem cells cultured ex vivo with a histone deacetylase inhibitor. Stem. Cells. Transl. Med. 2020, 9, 531–542. [Google Scholar] [CrossRef]
- Shah, R.R.; Koniski, A.; Shinde, M.; Blythe, S.A.; Fass, D.M.; Haggarty, S.J.; Palis, J.; Klein, P.S. Regulation of primitive hematopoiesis by class I histone deacetylases. Dev. Dyn. 2013, 242, 108–121. [Google Scholar] [CrossRef] [PubMed]
- Chateauvieux, S.; Eifes, S.; Morceau, F.; Grigorakaki, C.; Schnekenburger, M.; Henry, E.; Dicato, M.; Diederich, M. Valproic acid perturbs hematopoietic homeostasis by inhibition of erythroid differentiation and activation of the myelo-monocytic pathway. Biochem. Pharmacol. 2011, 81, 498–509. [Google Scholar] [CrossRef]
- Bug, G.; Gül, H.; Schwarz, K.; Pfeifer, H.; Kampfmann, M.; Zheng, X.; Beissert, T.; Boehrer, S.; Hoelzer, D.; Ottmann, O.G.; et al. Valproic acid stimulates proliferation and self-renewal of hematopoietic stem cells. Cancer Res. 2005, 65, 2537–2541. [Google Scholar] [CrossRef] [PubMed]
- Passeri, D.; Marcucci, A.; Rizzo, G.; Billi, M.; Panigada, M.; Leonardi, L.; Tirone, F.; Grignani, F. Btg2 enhances retinoic acid-induced differentiation by modulating histone H4 methylation and acetylation. Mol. Cell. Biol. 2006, 26, 5023–5032. [Google Scholar] [CrossRef][Green Version]
- Urvalek, A.; Laursen, K.B.; Gudas, L.J. The roles of retinoic acid and retinoic acid receptors in inducing epigenetic changes. Subcell. Biochem. 2014, 70, 129–149. [Google Scholar] [PubMed]
- Qi, H.; Ratnam, M. Synergistic induction of folate receptor beta by all-trans retinoic acid and histone deacetylase inhibitors in acute myelogenous leukemia cells: Mechanism and utility in enhancing selective growth inhibition by antifolates. Cancer Res. 2006, 66, 5875–5882. [Google Scholar] [CrossRef]
- Trus, M.R.; Yang, L.; Suarez Saiz, F.; Bordeleau, L.; Jurisica, I.; Minden, M.D. The histone deacetylase inhibitor valproic acid alters sensitivity towards all trans retinoic acid in acute myeloblastic leukemia cells. Leukemia 2005, 19, 1161–1168. [Google Scholar] [CrossRef]
- Lakshmaiah, K.C.; Jacob, L.A.; Aparna, S.; Lokanatha, D.; Saldanha, S.C. Epigenetic therapy of cancer with histone deacetylase inhibitors. J. Cancer Res. Ther. 2014, 10, 469–478. [Google Scholar]
- Chateauvieux, S.; Morceau, F.; Dicato, M.; Diederich, M. Molecular and therapeutic potential and toxicity of valproic acid. J. Biomed. Biotechnol. 2010, 2010, 479364. [Google Scholar] [CrossRef] [PubMed]
- Bradbury, C.A.; Khanim, F.L.; Hayden, R.; Bunce, C.M.; White, D.A.; Drayson, M.T.; Craddock, C.; Turner, B.M. Histone deacetylases in acute myeloid leukaemia show a distinctive pattern of expression that changes selectively in response to deacetylase inhibitors. Leukemia 2005, 19, 1751–1759. [Google Scholar] [CrossRef]
- Lübbert, M.; Grishina, O.; Schmoor, C.; Schlenk, R.F.; Jost, E.; Crysandt, M.; Heuser, M.; Thol, F.; Salih, H.R.; Schittenhelm, M.M.; et al. DECIDER study team. Valproate and retinoic acid in combination with decitabine in elderly nonfit patients with acute myeloid leukemia: Results of a multicenter, randomized, 2 × 2, Phase II Trial. J. Clin. Oncol. 2020, 38, 257–270. [Google Scholar] [CrossRef]
- Zhang, Z.H.; Hao, C.L.; Liu, P.; Tian, X.; Wang, L.H.; Zhao, L.; Zhu, C.-M. Valproic acid inhibits tumor angiogenesis in mice transplanted with Kasumi1 leukemia cells. Mol. Med. Rep. 2014, 9, 443–449. [Google Scholar] [CrossRef][Green Version]
- Liu, S.; Klisovic, R.B.; Vukosavljevic, T.; Yu, J.; Paschka, P.; Huynh, L.; Pang, J.; Neviani, P.; Liu, Z.; Blum, W.; et al. Targeting AML1/ETO-histone deacetylase repressor complex: A novel mechanism for valproic acid-mediated gene expression and cellular differentiation in AML1/ETO-positive acute myeloid leukemia cells. J. Pharmacol. Exp. Ther. 2007, 321, 953–960. [Google Scholar] [CrossRef] [PubMed]
- Ryningen, A.; Stapnes, C.; Paulsen, K.; Lassalle, P.; Gjertsen, B.T.; Bruserud, Ø. In vivo biological effects of ATRA in the treatment of AML. Expert. Opin. Investig. Drugs 2008, 17, 1623–1633. [Google Scholar] [CrossRef] [PubMed]
- Davood, Z.A.; Shamsi, S.; Ghaedi, H.; Sahand, R.I.; Mojtaba, G.; Mahdi, T.; Reza, M.; Ebrahimi, M.J.; Miri-Moosavi, R.S.; Boosaliki, S.; et al. Valproic acid may exerts its cytotoxic effect through rassf1a expression induction in acute myeloid leukemia. Tumour. Biol. 2016, 37, 11001–11006. [Google Scholar] [CrossRef] [PubMed]
- Forthun, R.B.; Sengupta, T.; Skjeldam, H.K.; Lindvall, J.M.; McCormack, E.; Gjertsen, B.T.; Nilsen, H. Cross-species functional genomic analysis identifies resistance genes of the histone deacetylase inhibitor valproic acid. PLoS ONE 2012, 7, e48992. [Google Scholar]
- Gul, H.; Marquez-Curtis, L.A.; Jahroudi, N.; Larratt, L.M.; Janowska-Wieczorek, A. Valproic acid exerts differential effects on CXCR4 expression in leukemic cells. Leuk. Res. 2010, 34, 235–242. [Google Scholar] [CrossRef]
- Stapnes, C.; Ryningen, A.; Hatfield, K.; Øyan, A.M.; Eide, G.E.; Corbascio, M.; Kalland, K.H.; Gjertsen, B.T.; Bruserud, Ø. Functional characteristics and gene expression profiles of primary acute myeloid leukaemia cells identify patient subgroups that differ in susceptibility to histone deacetylase inhibitors. Int. J. Oncol. 2007, 31, 1529–1538. [Google Scholar] [CrossRef]
- Cimino, G.; Lo-Coco, F.; Fenu, S.; Travaglini, L.; Finolezzi, E.; Mancini, M.; Nanni, M.; Careddu, A.; Fazi, F.; Padula, F.; et al. Sequential valproic acid/all-trans retinoic acid treatment reprograms differentiation in refractory and high-risk acute myeloid leukemia. Cancer Res. 2006, 66, 8903–8911. [Google Scholar] [CrossRef]
- Reikvam, H.; Hovland, R.; Forthun, R.B.; Erdal, S.; Gjertsen, B.T.; Fredly, H.; Bruserud, Ø. Disease-stabilizing treatment based on all-trans retinoic acid and valproic acid in acute myeloid leukemia—identification of responders by gene expression profiling of pretreatment leukemic cells. BMC Cancer 2017, 17, 630. [Google Scholar] [CrossRef]
- Rücker, F.G.; Lang, K.M.; Fütterer, M.; Komarica, V.; Schmid, M.; Döhner, H.; Schlenk, R.F.; Döhner, K.; Knudsen, S.; Bullinger, L. Molecular dissection of valproic acid effects in acute myeloid leukemia identifies predictive networks. Epigenetics 2016, 11, 517–525. [Google Scholar] [CrossRef]
- Zhang, Z.; Hao, C.; Wang, L.; Liu, P.; Zhao, L.; Zhu, C.; Tian, X. Inhibition of leukemic cells by valproic acid, an HDAC inhibitor, in xenograft tumors. Onco. Targets Ther. 2013, 6, 733–740. [Google Scholar]
- Forthun, R.B.; Hellesøy, M.; Sulen, A.; Kopperud, R.K.; Sjøholt, G.; Bruserud, Ø.; McCormack, E.; Gjertsen, B.T. Modulation of phospho-proteins by interferon-alpha and valproic acid in acute myeloid leukemia. J. Cancer Res. Clin. Oncol. 2019, 145, 1729–1749. [Google Scholar] [CrossRef]
- Hernandez-Valladares, M.; Wangen, R.; Aasebø, E.; Reikvam, H.; Berven, F.S.; Selheim, F.; Bruserud, Ø. Proteomic studies of primary acute myeloid leukemia cells derived from patients before and during disease-stabilizing treatment based on all-trans retinoic acid and valproic acid. Cancers 2021, 13, 2143. [Google Scholar] [CrossRef]
- Cho, H.H.; Park, H.T.; Kim, Y.; Bae, Y.C.; Suh, K.T.; Jung, J.S. Induction of osteogenic differentiation of human mesenchymal stem cells by histone deacetylase inhibitors. J. Cell. Biochem. 2005, 96, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Kvestad, H.; Evensen, L.; Lorens, J.B.; Bruserud, Ø.; Hatfield, K.J. In Vitro characterization of valproic acid, atra, and cytarabine used for disease-stabilization in human acute myeloid leukemia: Antiproliferative effects of drugs on endothelial and osteoblastic cells and altered release of angioregulatory mediators by endothelial cells. Leuk. Res. Treat. 2014, 2014, 143479. [Google Scholar]
- Ryningen, A.; Stapnes, C.; Lassalle, P.; Corbascio, M.; Gjertsen, B.T.; Bruserud, Ø. A subset of patients with high-risk acute myelogenous leukemia shows improved peripheral blood cell counts when treated with the combination of valproic acid, theophylline and all-trans retinoic acid. Leuk. Res. 2009, 33, 779–787. [Google Scholar] [CrossRef]
- Ersvaer, E.; Brenner, A.K.; Vetas, K.; Reikvam, H.; Bruserud, Ø. Effects of cytarabine on activation of human T cells—Cytarabine has concentration-dependent effects that are modulated both by valproic acid and all-trans retinoic acid. BMC Pharmacol. Toxicol. 2015, 16, 12. [Google Scholar] [CrossRef] [PubMed]
- Fredly, H.; Ersvaer, E.; Kittang, A.O.; Tsykunova, G.; Gjertsen, B.T.; Bruserud, Ø. The combination of valproic acid, all-trans retinoic acid and low-dose cytarabine as disease-stabilizing treatment in acute myeloid leukemia. Clin. Epigenetics 2013, 5, 13. [Google Scholar] [CrossRef]
- Arbez, J.; Lamarthee, B.; Gaugler, B.; Saas, P. Histone deacetylase inhibitor valproic acid affects plasmacytoid dendritic cells phenotype and function. Immunobiology 2014, 219, 637–643. [Google Scholar] [CrossRef]
- Leu, S.J.; Yang, Y.Y.; Liu, H.C.; Cheng, C.Y.; Wu, Y.C.; Huang, M.C.; Lee, Y.L.; Chen, C.C.; Shen, W.W.; Liu, K.J. Valproic acid and lithium meditate anti-inflammatory effects by differentially modulating dendritic cell differentiation and function. J. Cell. Physiol. 2017, 232, 1176–1186. [Google Scholar] [CrossRef]
- Frikeche, J.; Simon, T.; Brissot, E.; Gregoire, M.; Gaugler, B.; Mohty, M. Impact of valproic acid on dendritic cells function. Immunobiology 2012, 217, 704–710. [Google Scholar] [CrossRef]
- Nencioni, A.; Beck, J.; Werth, D.; Grünebach, F.; Patrone, F.; Ballestrero, A.; Brossart, P. Histone deacetylase inhibitors affect dendritic cell differentiation and immunogenicity. Clin. Cancer Res. 2007, 13, 3933–3941. [Google Scholar] [CrossRef] [PubMed]
- Delgado, F.G.; Cardenas, P.; Castellanos, J.E. Valproic acid downregulates cytokine expression in human macrophages infected with dengue virus. Diseases 2018, 6, 59. [Google Scholar] [CrossRef]
- Mohammadi, S.; Saghaeian-Jazi, M.; Sedighi, S.; Memarian, A. Sodium valproate modulates immune response by alternative activation of monocyte-derived macrophages in systemic lupus erythematosus. Clin. Rheumatol. 2018, 37, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Killer, M.C.; Nold, P.; Henkenius, K.; Fritz, L.; Riedlinger, T.; Barckhausen, C.; Frech, M.; Hackstein, H.; Neubauer, A.; Brendel, C. Immunosuppressive capacity of mesenchymal stem cells correlates with metabolic activity and can be enhanced by valproic acid. Stem. Cell. Res. Ther. 2017, 8, 100. [Google Scholar] [CrossRef]
- Bidkhori, H.R.; Ahmadiankia, N.; Matin, M.M.; Heirani-Tabasi, A.; Farshchian, M.; Naderi-Meshkin, H.; Shahriyari, M.; Dastpak, M.; Bahrami, A.R. Chemically primed bone-marrow derived mesenchymal stem cells show enhanced expression of chemokine receptors contributed to their migration capability. Iran. J. Basic Med. Sci. 2016, 19, 14–19. [Google Scholar] [PubMed]
- Fredly, H.; Reikvam, H.; Gjertsen, B.T.; Bruserud, Ø. Disease-stabilizing treatment with all-trans retinoic acid and valproic acid in acute myeloid leukemia: Serum hsp70 and hsp90 levels and serum cytokine profiles are determined by the disease, patient age, and anti-leukemic treatment. Am. J. Hematol. 2012, 87, 368–376. [Google Scholar] [CrossRef]
- Pulliam, S.R.; Pellom, S.T., Jr.; Shanker, A.; Adunyah, S.E. Butyrate regulates the expression of inflammatory and chemotactic cytokines in human acute leukemic cells during apoptosis. Cytokine 2016, 84, 74–87. [Google Scholar] [CrossRef] [PubMed]
- Myzak, M.C.; Dashwood, R.H. Histone deacetylases as targets for dietary cancer preventive agents: Lessons learned with butyrate, diallyl disulfide, and sulforaphane. Curr. Drug Targets 2006, 7, 443–452. [Google Scholar] [CrossRef]
- Heidor, R.; Ortega, J.F.; de Conti, A.; Ong, T.P.; Moreno, F.S. Anticarcinogenic actions of tributyrin, a butyric acid prodrug. Curr. Drug Targets 2012, 13, 1720–1729. [Google Scholar] [CrossRef]
- Brenner, A.K.; Bruserud, Ø. Functional Toll-Like Receptors (TLRs) are expressed by a majority of primary human acute myeloid leukemia cells and inducibility of the tlr signaling pathway is associated with a more favorable phenotype. Cancers 2019, 11, 973. [Google Scholar] [CrossRef]
- Kopp, A.; Buechler, C.; Bala, M.; Neumeier, M.; Schölmerich, J.; Schäffler, A. Toll-like receptor ligands cause proinflammatory and prodiabetic activation of adipocytes via phosphorylation of extracellular signal-regulated kinase and c-Jun N-terminal kinase but not interferon regulatory factor-3. Endocrinology 2010, 151, 1097–1108. [Google Scholar] [CrossRef]
- Botteri, G.; Montori, M.; Gumà, A.; Pizarro, J.; Cedó, L.; Escolà-Gil, J.C.; Li, D.; Barroso, E.; Palomer, X.; Kohan, A.B.; et al. VLDL and apolipoprotein CIII induce ER stress and inflammation and attenuate insulin signalling via Toll-like receptor 2 in mouse skeletal muscle cells. Diabetologia 2017, 60, 2262–2273. [Google Scholar] [CrossRef]
- Kawakami, A.; Yoshida, M. Apolipoprotein CIII links dyslipidemia with atherosclerosis. J. Atheroscler. Thromb. 2009, 16, 6–11. [Google Scholar] [CrossRef]
- Van Gils, N.; Verhagen, H.J.M.P.; Smit, L. Reprogramming acute myeloid leukemia into sensitivity for retinoic-acid-driven differentiation. Exp. Hematol. 2017, 52, 12–23. [Google Scholar] [CrossRef]
- Rossetti, S.; Sacchi, N. Emerging cancer epigenetic mechanisms regulated by all-trans retinoic acid. Cancers 2020, 12, 2275. [Google Scholar] [CrossRef]
- Giuli, M.V.; Hanieh, P.N.; Giuliani, E.; Rinaldi, F.; Marianecci, C.; Screpanti, I.; Checquolo, S.; Carafa, M. Current trends in ATRA delivery for cancer therapy. Pharmaceutics 2020, 12, 707. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Zeng, T.; Lin, Z.; Yan, L.; Wang, F.; Tang, L.; Wang, L.; Tang, D.; Chen, P.; Yang, M. Long non-coding RNA SNHG5 regulates chemotherapy resistance through the miR-32/DNAJB9 axis in acute myeloid leukemia. Biomed. Pharm. 2020, 123, 109802. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.H.; Grandits, A.M.; Vassiliou, G.S.; Staber, P.B.; Heller, G.; Wieser, R. Evi1 Counteracts anti-leukemic and stem cell inhibitory effects of all-trans retinoic acid on Flt3-ITD/Npm1Driven acute myeloid leukemia cells. Biomedicines 2020, 8, 385. [Google Scholar] [CrossRef] [PubMed]
- Schlenk, R.F.; Fröhling, S.; Hartmann, F.; Fischer, J.T.; Glasmacher, A.; del Valle, F.; Grimminger, W.; Götze, K.; Waterhouse, C.; Schoch, R.; et al. Study Group Ulm. Phase III study of all-trans retinoic acid in previously untreated patients 61 years or older with acute myeloid leukemia. Leukemia 2004, 18, 1798–1803. [Google Scholar] [CrossRef]
- Schlenk, R.F.; Döhner, K.; Kneba, M.; Götze, K.; Hartmann, F.; Del Valle, F.; Kirchen, H.; Koller, E.; Fischer, J.T.; Bullinger, L.; et al. Gene mutations and response to treatment with all-trans retinoic acid in elderly patients with acute myeloid leukemia. Results from the AMLSG Trial AML HD98B. Haematologica 2009, 94, 54–60. [Google Scholar] [CrossRef]
- Heuser, M.; Argiropoulos, B.; Kuchenbauer, F.; Yung, E.; Piper, J.; Fung, S.; Schlenk, R.F.; Dohner, K.; Hinrichsen, T.; Rudolph, C.; et al. MN1 overexpression induces acute myeloid leukemia in mice and predicts ATRA resistance in patients with AML. Blood 2007, 110, 1639–1647. [Google Scholar] [CrossRef] [PubMed]
- Burnett, A.K.; Hills, R.K.; Green, C.; Jenkinson, S.; Koo, K.; Patel, Y.; Guy, C.; Gilkes, A.; Milligan, D.W.; Goldstone, A.H.; et al. The impact on outcome of the addition of all-trans retinoic acid to intensive chemotherapy in younger patients with nonacute promyelocytic acute myeloid leukemia: Overall results and results in genotypic subgroups defined by mutations in NPM1, FLT3, and CEBPA. Blood 2010, 115, 948–956. [Google Scholar] [PubMed]
- Schlenk, R.F.; Lübbert, M.; Benner, A.; Lamparter, A.; Krauter, J.; Herr, W.; Martin, H.; Salih, H.R.; Kündgen, A.; Horst, H.A.; et al. All-trans retinoic acid as adjunct to intensive treatment in younger adult patients with acute myeloid leukemia: Results of the randomized AMLSG 07-04 study. Ann. Hematol. 2016, 95, 1931–1942. [Google Scholar] [CrossRef] [PubMed]
- Küley-Bagheri, Y.; Kreuzer, K.A.; Monsef, I.; Lübbert, M.; Skoetz, N. Effects of all-trans retinoic acid (ATRA) in addition to chemotherapy for adults with acute myeloid leukaemia (AML) (non-acute promyelocytic leukaemia (non-APL)). Cochrane Database Syst. Rev. 2018, 8, CD011960. [Google Scholar] [CrossRef] [PubMed]
- McKeown, M.R.; Johannessen, L.; Lee, E.; Fiore, C.; di Tomaso, E. Antitumor synergy with SY-1425, a selective RARα agonist, and hypomethylating agents in retinoic acid receptor pathway activated models of acute myeloid leukemia. Haematologica 2019, 104, e138–e142. [Google Scholar] [CrossRef] [PubMed]
- Fazi, F.; Zardo, G.; Gelmetti, V.; Travaglini, L.; Ciolfi, A.; Di Croce, L.; Rosa, A.; Bozzoni, I.; Grignani, F.; Lo-Coco, F.; et al. Heterochromatic gene repression of the retinoic acid pathway in acute myeloid leukemia. Blood 2007, 109, 4432–4440. [Google Scholar] [CrossRef]
- Su, M.; Alonso, S.; Jones, J.W.; Yu, J.; Kane, M.A.; Jones, R.J.; Ghiaur, G. All-trans retinoic acid activity in acute myeloid leukemia: Role of cytochrome P450 enzyme expression by the microenvironment. PLoS ONE 2015, 10, e0127790. [Google Scholar] [CrossRef]
- Martelli, M.P.; Gionfriddo, I.; Mezzasoma, F.; Milano, F.; Pierangeli, S.; Mulas, F.; Pacini, R.; Tabarrini, A.; Pettirossi, V.; Rossi, R.; et al. Arsenic trioxide and all-trans retinoic acid target NPM1 mutant oncoprotein levels and induce apoptosis in NPM1-mutated AML cells. Blood 2015, 125, 3455–3465. [Google Scholar] [CrossRef]
- El Hajj, H.; Dassouki, Z.; Berthier, C.; Raffoux, E.; Ades, L.; Legrand, O.; Hleihel, R.; Sahin, U.; Tawil, N.; Salameh, A.; et al. Retinoic acid and arsenic trioxide trigger degradation of mutated NPM1, resulting in apoptosis of AML cells. Blood 2015, 125, 3447–3454. [Google Scholar] [CrossRef]
- Boutzen, H.; Saland, E.; Larrue, C.; de Toni, F.; Gales, L.; Castelli, F.A.; Cathebas, M.; Zaghdoudi, S.; Stuani, L.; Kaoma, T.; et al. Isocitrate dehydrogenase 1 mutations prime the all-trans retinoic acid myeloid differentiation pathway in acute myeloid leukemia. J. Exp. Med. 2016, 213, 483–497. [Google Scholar] [CrossRef]
- Haas, K.; Kundi, M.; Sperr, W.R.; Esterbauer, H.; Ludwig, W.D.; Ratei, R.; Koller, E.; Gruener, H.; Sauerland, C.; Fonatsch, C.; et al. Expression and prognostic significance of different mRNA 5′-end variants of the oncogene EVI1 in 266 patients with de novo AML: EVI1 and MDS1/EVI1 overexpression both predict short remission duration. Genes Chromosom. Cancer 2008, 47, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Lugthart, S.; van Drunen, E.; van Norden, Y.; van Hoven, A.; Erpelinck, C.A.; Valk, P.J.; Beverloo, H.B.; Löwenberg, B.; Delwel, R. High EVI1 levels predict adverse outcome in acute myeloid leukemia: Prevalence of EVI1 overexpression and chromosome 3q26 abnormalities underestimated. Blood 2008, 111, 4329–4337. [Google Scholar] [CrossRef]
- Gröschel, S.; Lugthart, S.; Schlenk, R.F.; Valk, P.J.; Eiwen, K.; Goudswaard, C.; van Putten, W.J.; Kayser, S.; Verdonck, L.F.; Lübbert, M.; et al. High EVI1 expression predicts outcome in younger adult patients with acute myeloid leukemia and is associated with distinct cytogenetic abnormalities. J. Clin. Oncol. 2010, 28, 2101–2107. [Google Scholar] [CrossRef]
- Xi, Z.F.; Russell, M.; Woodward, S.; Thompson, F.; Wagner, L.; Taetle, R. Expression of the Zn finger gene, EVI-1, in acute promyelocytic leukemia. Leukemia 1997, 11, 212–220. [Google Scholar] [CrossRef][Green Version]
- Aytekin, M.; Vinatzer, U.; Musteanu, M.; Raynaud, S.; Wieser, R. Regulation of the expression of the oncogene EVI1 through the use of alternative mRNA 5′-ends. Gene 2005, 356, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Bingemann, S.C.; Konrad, T.A.; Wieser, R. Zinc finger transcription factor ecotropic viral integration site 1 is induced by all-trans retinoic acid (ATRA) and acts as a dual modulator of the ATRA response. FEBS J. 2009, 276, 6810–6822. [Google Scholar] [CrossRef][Green Version]
- Steinmetz, B.; Hackl, H.; Slabáková, E.; Schwarzinger, I.; Smějová, M.; Spittler, A.; Arbesu, I.; Shehata, M.; Souček, K.; Wieser, R. The oncogene EVI1 enhances transcriptional and biological responses of human myeloid cells to all-trans retinoic acid. Cell. Cycle 2014, 13, 2931–2943. [Google Scholar] [CrossRef]
- Verhagen, H.J.; Smit, M.A.; Rutten, A.; Denkers, F.; Poddighe, P.J.; Merle, P.A.; Ossenkoppele, G.J.; Smit, L. Primary acute myeloid leukemia cells with overexpression of EVI-1 are sensitive to all-trans retinoic acid. Blood 2016, 127, 458–463. [Google Scholar] [CrossRef]
- Nguyen, C.H.; Bauer, K.; Hackl, H.; Schlerka, A.; Koller, E.; Hladik, A.; Stoiber, D.; Zuber, J.; Staber, P.B.; Hoelbl-Kovacic, A.; et al. All-trans retinoic acid enhances, and a pan-RAR antagonist counteracts, the stem cell promoting activity of EVI1 in acute myeloid leukemia. Cell Death Dis. 2019, 10, 944. [Google Scholar] [CrossRef] [PubMed]
- Moreb, J.-S.; Ucar-Bilyeu, D.A.; Khan, A. Use of retinoic acid/aldehyde dehydrogenase pathway as potential targeted therapy against cancer stem cells. Cancer Chemother. Pharm. 2017, 79, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Gasparetto, M.; Smith, C.A. ALDHs in normal and malignant hematopoietic cells: Potential new avenues for treatment of AML and other blood cancers. Chem. Biol. Interact. 2017, 276, 46–51. [Google Scholar] [CrossRef]
- Hernandez-Valladares, M.; Aasebø, E.; Berven, F.; Selheim, F.; Bruserud, Ø. Biological characteristics of aging in human acute myeloid leukemia cells: The possible importance of aldehyde dehydrogenase, the cytoskeleton and altered transcriptional regulation. Aging 2020, 12, 24734–24777. [Google Scholar] [CrossRef] [PubMed]
- Rundberg Nilsson, A.; Pronk, C.J. Retinoic acid puts hematopoietic stem cells back to sleep. Cell. Stem. Cell. 2017, 21, 9–11. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cañete, A.; Cano, E.; Muñoz-Chápuli, R.; Carmona, R. Role of vitamin A/retinoic acid in regulation of embryonic and adult hematopoiesis. Nutrients 2017, 9, 159. [Google Scholar] [CrossRef]
- Bono, M.R.; Tejon, G.; Flores-Santibañez, F.; Fernandez, D.; Rosemblatt, M.; Sauma, D. Retinoic acid as a modulator of t cell immunity. Nutrients 2016, 8, 349. [Google Scholar] [CrossRef]
- Xie, L.; Zou, L.; Chen, J.; Liu, Y. All-trans retinoic acid inhibits bone marrow mesenchymal stem cell commitment to adipocytes via upregulating FRA1 signaling. Int. J. Endocrinol. 2020, 2020, 6525787. [Google Scholar] [CrossRef]
- Sun, W.; Shi, A.; Ma, D.; Bolscher, J.G.M.; Nazmi, K.; Veerman, E.C.I.; Bikker, F.J.; Lin, H.; Wu, G. All-trans retinoic acid and human salivary histatin-1 promote the spreading and osteogenic activities of pre-osteoblasts in vitro. FEBS Open Bio 2020, 10, 396–406. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Ma, X.; Guo, J.; Lin, Z.; Zhou, M.; Bi, W.; Liu, J.; Wang, J.; Lu, H.; Wu, G. All-trans retinoic acid can antagonize osteoblastogenesis induced by different BMPs irrespective of their dimerization types and dose-efficiencies. Drug Des. Devel. Ther. 2018, 12, 3419–3430. [Google Scholar] [CrossRef] [PubMed]
- Pawlikowski, B.; Wragge, J.; Siegenthaler, J.A. Retinoic acid signaling in vascular development. Genesis 2019, 57, e23287. [Google Scholar] [CrossRef]
- Li, N.; Lu, Y.; Li, D.; Zheng, X.; Lian, J.; Li, S.; Cui, H.; Zhang, L.; Sang, L.; Wang, Y.; et al. All-trans retinoic acid suppresses the angiopoietin-Tie2 pathway and inhibits angiogenesis and metastasis in esophageal squamous cell carcinoma. PLoS ONE 2017, 12, e0174555. [Google Scholar] [CrossRef] [PubMed]
- Erkelens, M.N.; Mebius, R.E. Retinoic acid and immune homeostasis: A balancing act. Trends Immunol. 2017, 38, 168–180. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Liu, Y.; Qi, G.; Brand, D.; Zheng, S.G. Role of vitamin A in the immune system. J. Clin. Med. 2018, 7, 258. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, L.M.; Teixeira, F.M.E.; Sato, M.N. Impact of retinoic acid on immune cells and inflammatory diseases. Mediat. Inflamm. 2018, 2018, 3067126. [Google Scholar] [CrossRef]
- Raverdeau, M.; Mills, K.H. Modulation of T cell and innate immune responses by retinoic Acid. J. Immunol. 2014, 192, 2953–2958. [Google Scholar] [CrossRef]
- Ross, A.C. Vitamin A and retinoic acid in T cell-related immunity. Am. J. Clin. Nutr. 2012, 96, 1166S–1172S. [Google Scholar] [CrossRef]
- Sun, X.; Xiao, Y.; Zeng, Z.; Shi, Y.; Tang, B.; Long, H.; Kanekura, T.; Wang, J.; Wu, H.; Zhao, M.; et al. All-trans retinoic acid induces CD4+CD25+FOXP3+ regulatory T cells by increasing FOXP3 demethylation in systemic sclerosis CD4+ T cells. J. Immunol. Res. 2018, 2018, 8658156. [Google Scholar] [CrossRef] [PubMed]
- Yin, W.; Song, Y.; Liu, Q.; Wu, Y.; He, R. Topical treatment of all-trans retinoic acid inhibits murine melanoma partly by promoting CD8+ T-cell immunity. Immunology 2017, 152, 287–297. [Google Scholar] [CrossRef]
- Long, A.H.; Highfill, S.L.; Cui, Y.; Smith, J.P.; Walker, A.J.; Ramakrishna, S.; El-Etriby, R.; Galli, S.; Tsokos, M.G.; Orentas, R.J.; et al. Reduction of MDSCs with all-trans retinoic acid improves CAR therapy efficacy for sarcomas. Cancer Immunol. Res. 2016, 4, 869–880. [Google Scholar] [CrossRef] [PubMed]
- Vellozo, N.S.; Pereira-Marques, S.T.; Cabral-Piccin, M.P.; Filardy, A.A.; Ribeiro-Gomes, F.L.; Rigoni, T.S.; DosReis, G.A.; Lopes, M.F. All-Trans retinoic acid promotes an M1- to M2-phenotype shift and inhibits macrophage-mediated immunity to leishmania major. Front. Immunol. 2017, 8, 1560. [Google Scholar] [CrossRef] [PubMed]
- Melve, G.K.; Ersvssr, E.; Kittang, A.O.; Bruserud, Ø. The chemokine system in allogeneic stem-cell transplantation: A possible therapeutic target? Expert Rev. Hematol. 2011, 4, 563–576. [Google Scholar] [CrossRef] [PubMed]
- Rundgren, I.M.; Ersvær, E.; Ahmed, A.B.; Ryningen, A.; Bruserud, Ø. A Pilot Study of Circulating Monocyte Subsets in Patients Treated with Stem Cell Transplantation for High-Risk Hematological Malignancies. Medicina 2020, 56, 36. [Google Scholar] [CrossRef] [PubMed]
- Rundgren, I.M.; Ersvær, E.; Ahmed, A.B.; Ryningen, A.; Bruserud, Ø. Circulating monocyte subsets in multiple myeloma patients receiving autologous stem cell transplantation—A study of the preconditioning status and the course until posttransplant reconstitution for a consecutive group of patients. BMC Immunol. 2019, 20, 39. [Google Scholar] [CrossRef] [PubMed]
- Tvedt, T.H.A.; Skaarud, K.J.; Tjønnfjord, G.E.; Gedde-Dahl, T.; Iversen, P.O.; Bruserud, Ø. The systemic metabolic profile early after allogeneic stem cell transplantation: Effects of adequate energy support administered through enteral feeding tube. Biol. Blood Marrow. Transplant. 2020, 26, 380–391. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Cibrian, N.; Zeiser, R.; Perez-Simon, J.A. Graft-versus-host disease prophylaxis: Pathophysiology-based review on current approaches and future directions. Blood Rev. 2020, 100792, Epub ahead of print. [Google Scholar] [CrossRef]
- Kim, M.H.; Taparowsky, E.J.; Kim, C.H. Retinoic acid differentially regulates the migration of innate lymphoid cell subsets to the gut. Immunity 2015, 43, 107–119. [Google Scholar] [CrossRef]
- Czarnewski, P.; Das, S.; Parigi, S.M.; Villablanca, E.J. Retinoic acid and its role in modulating intestinal innate immunity. Nutrients 2017, 9, 68. [Google Scholar] [CrossRef]
- Koenecke, C.; Prinz, I.; Bubke, A.; Schreder, A.; Lee, C.W.; Pabst, O.; Förster, R. Shift of graft-versus-host-disease target organ tropism by dietary vitamin A. PLoS ONE 2012, 7, e38252. [Google Scholar] [CrossRef]
- Dodge, J.; Stephans, A.; Lai, J.; Drobyski, W.R.; Chen, X. Effects of donor vitamin a deficiency and pharmacologic modulation of donor t cell retinoic acid pathway on the severity of experimental graft-versus-host disease. Biol. Blood Marrow. Transpl. 2016, 22, 2141–2148. [Google Scholar] [CrossRef]
- Chen, X.; Dodge, J.; Komorowski, R.; Drobyski, W.R. A critical role for the retinoic acid signaling pathway in the pathophysiology of gastrointestinal graft-versus-host disease. Blood 2013, 121, 3970–3980. [Google Scholar] [CrossRef]
- Thangavelu, G.; Lee, Y.C.; Loschi, M.; Schaechter, K.M.; Feser, C.J.; Koehn, B.H.; Nowak, E.C.; Zeiser, R.; Serody, J.S.; Murphy, W.J.; et al. Dendritic cell expression of retinal aldehyde dehydrogenase-2 controls graft-versus-host disease lethality. J. Immunol. 2019, 202, 2795–2805. [Google Scholar] [CrossRef]
- Lounder, D.T.; Khandelwal, P.; Dandoy, C.E.; Jodele, S.; Grimley, M.S.; Wallace, G.; Lane, A.; Taggart, C.; Teusink-Cross, A.C.; Lake, K.E.; et al. Lower levels of vitamin A are associated with increased gastrointestinal graft-versus-host disease in children. Blood 2017, 129, 2801–2807. [Google Scholar] [CrossRef]
- Tong, J.; Hu, R.; Zhao, Y.; Xu, Y.; Zhao, X.; Jin, X. Serum vitamin a levels may affect the severity of ocular graft-versus-host disease. Front. Med. 2017, 4, 67. [Google Scholar] [CrossRef] [PubMed]
- Kuendgen, A.; Bug, G.; Ottmann, O.G.; Haase, D.; Schanz, J.; Hildebrandt, B.; Nachtkamp, K.; Neukirchen, J.; Dienst, A.; Haas, R.; et al. Treatment of poor-risk myelodysplastic syndromes and acute myeloid leukemia with a combination of 5-azacytidine and valproic acid. Clin. Epigenetics 2011, 2, 389–399. [Google Scholar] [CrossRef]
- Kuendgen, A.; Schmid, M.; Schlenk, R.; Knipp, S.; Hildebrandt, B.; Steidl, C.; Germing, U.; Haas, R.; Dohner, H.; Gattermann, N. The histone deacetylase (HDAC) inhibitor valproic acid as monotherapy or in combination with all-trans retinoic acid in patients with acute myeloid leukemia. Cancer 2006, 106, 112–119. [Google Scholar] [CrossRef]
- Kuendgen, A.; Knipp, S.; Fox, F.; Strupp, C.; Hildebrandt, B.; Steidl, C.; Germing, U.; Haas, R.; Gattermann, N. Results of a phase 2 study of valproic acid alone or in combination with all-trans retinoic acid in 75 patients with myelodysplastic syndrome and relapsed or refractory acute myeloid leukemia. Ann. Hematol. 2005, 84, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Bug, G.; Schwarz, K.; Schoch, C.; Kampfmann, M.; Henschler, R.; Hoelzer, D.; Ottmann, O.G.; Ruthardt, M. Effect of histone deacetylase inhibitor valproic acid on progenitor cells of acute myeloid leukemia. Haematologica 2007, 92, 542–545. [Google Scholar] [CrossRef] [PubMed]
- Bug, G.; Ritter, M.; Wassmann, B.; Schoch, C.; Heinzel, T.; Schwarz, K.; Romanski, A.; Kramer, O.H.; Kampfmann, M.; Hoelzer, D.; et al. Clinical trial of valproic acid and all-trans retinoic acid in patients with poor-risk acute myeloid leukemia. Cancer 2005, 104, 2717–2725. [Google Scholar] [CrossRef]
- Raffoux, E.; Chaibi, P.; Dombret, H.; Degos, L. Valproic acid and all-trans retinoic acid for the treatment of elderly patients with acute myeloid leukemia. Haematologica 2005, 90, 986–988. [Google Scholar]
- Lane, S.; Gill, D.; McMillan, N.A.; Saunders, N.; Murphy, R.; Spurr, T.; Keane, C.; Fan, H.M.; Mollee, P. Valproic acid combined with cytosine arabinoside in elderly patients with acute myeloid leukemia has in vitro but limited clinical activity. Leuk. Lymphoma 2012, 53, 1077–1083. [Google Scholar] [CrossRef]
- Corsetti, M.T.; Salvi, F.; Perticone, S.; Baraldi, A.; De Paoli, L.; Gatto, S.; Pietrasanta, D.; Pini, M.; Primon, V.; Zallio, F.; et al. Hematologic improvement and response in elderly AML/RAEB patients treated with valproic acid and low-dose Ara-C. Leuk. Res. 2011, 35, 991–997. [Google Scholar] [CrossRef]
- Xie, C.; Drenberg, C.; Edwards, H.; Caldwell, J.T.; Chen, W.; Inaba, H.; Xu, X.; Buck, S.A.; Taub, J.W.; Baker, S.D.; et al. Panobinostat enhances cytarabine and daunorubicin sensitivities in AML cells through suppressing the expression of BRCA1, CHK1, and Rad51. PLoS ONE 2013, 8, e79106. [Google Scholar] [CrossRef]
- Blagitko-Dorfs, N.; Schlosser, P.; Greve, G.; Pfeifer, D.; Meier, R.; Baude, A.; Brocks, D.; Plass, C.; Lübbert, M. Combination treatment of acute myeloid leukemia cells with DNMT and HDAC inhibitors: Predominant synergistic gene downregulation associated with gene body demethylation. Leukemia 2019, 33, 945–956. [Google Scholar] [CrossRef]
- Ocio, E.M.; Herrera, P.; Olave, M.T.; Castro, N.; Perez-Simon, J.A.; Brunet, S.; Oriol, A.; Mateo, M.; Sanz, M.-A.; Lopez, J.; et al. Panobinostat as part of induction and maintenance for elderly patients with newly diagnosed acute myeloid leukemia: Phase Ib/II panobidara study. Haematologica. 2015, 100, 1294–1300. [Google Scholar] [CrossRef]
- Bug, G.; Burchert, A.; Wagner, E.M.; Kroger, N.; Berg, T.; Guller, S.; Metzelder, S.K.; Wolf, A.; Hunecke, S.; Bader, P.; et al. Phase I/II study of the deacetylase inhibitor panobinostat after allogeneic stem cell transplantation in patients with high-risk MDS or AML (PANOBEST trial). Leukemia 2017, 31, 2523–2525. [Google Scholar] [CrossRef]
- DeAngelo, D.J.; Spencer, A.; Bhalla, K.N.; Prince, H.M.; Fischer, T.; Kindler, T.; Giles, F.J.; Scott, J.W.; Parker, K.; Liu, A.; et al. Phase Ia/II, two-arm, open-label, dose-escalation study of oral panobinostat administered via two dosing schedules in patients with advanced hematologic malignancies. Leukemia 2013, 27, 1628–1636. [Google Scholar] [CrossRef]
- Giles, F.; Fischer, T.; Cortes, J.; Garcia-Manero, G.; Beck, J.; Ravandi, F.; Masson, E.; Rae, P.; Laird, G.; Sharma, S.; et al. A phase I study of intravenous LBH589, a novel cinnamic hydroxamic acid analogue histone deacetylase inhibitor, in patients with refractory hematologic malignancies. Clin. Cancer Res. 2006, 12, 4628–4635. [Google Scholar] [CrossRef]
- Govindaraj, C.; Tan, P.; Walker, P.; Wei, A.; Spencer, A.; Plebanski, M. Reducing TNF receptor 2+ regulatory T cells via the combined action of azacitidine and the HDAC inhibitor, panobinostat for clinical benefit in acute myeloid leukemia patients. Clin. Cancer Res. 2014, 20, 724–735. [Google Scholar] [CrossRef] [PubMed]
- Tao, R.; de Zoeten, E.F.; Ozkaynak, E.; Chen, C.; Wang, L.; Porrett, P.M.; Li, B.; Turka, L.A.; Olson, E.N.; Greene, M.I.; et al. Deacetylase inhibition promotes the generation and function of regulatory T cells. Nat. Med. 2007, 13, 1299–1307. [Google Scholar] [CrossRef] [PubMed]
- Hancock, W.W.; Akimova, T.; Beier, U.H.; Liu, Y.; Wang, L. HDAC inhibitor therapy in autoimmunity and transplantation. Ann. Rheum. Dis. 2012, 71, 46–54. [Google Scholar] [CrossRef]
- Wieduwilt, M.J.; Pawlowska, N.; Thomas, S.; Olin, R.; Logan, A.C.; Damon, L.E.; Martin, T.; Kang, M.; Sayre, P.H.; Boyer, W.; et al. Histone deacetylase inhibition with panobinostat combined with intensive induction chemotherapy in older patients with acute myeloid leukemia: Phase I study results. Clin. Cancer Res. 2019, 25, 4917–4923. [Google Scholar] [CrossRef] [PubMed]
- Kalin, B.; van Norden, Y.; van Gelder, M.; Breems, D.; Maertens, J.; Jongen-Lavrencic, M.; Broers, A.E.C.; Braakman, E.; Grob, T.; Zeijlemaker, W.; et al. Panobinostat and decitabine prior to donor lymphocyte infusion in allogeneic stem cell transplantation. Blood Adv. 2020, 4, 4430–4437. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Manero, G.; Sekeres, M.A.; Egyed, M.; Breccia, M.; Graux, C.; Cavenagh, J.D.; Salman, H.; Illes, A.; Fenaux, P.; DeAngelo, D.J.; et al. A phase 1b/2b multicenter study of oral panobinostat plus azacitidine in adults with MDS, CMML or AML with ⩽30% blasts. Leukemia 2017, 31, 2799–2806. [Google Scholar] [CrossRef]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [PubMed]
- Craddock, C.; Labopin, M.; Robin, M.; Finke, J.; Chevallier, P.; Yakoub-Agha, I.; Bourhis, J.H.; Sengelov, H.; Blaise, D.; Luft, T.; et al. Clinical activity of azacitidine in patients who relapse after allogeneic stem cell ransplantation for acute myeloid leukemia. Haematologica 2016, 101, 879–883. [Google Scholar] [CrossRef]
- Bruserud, Ø.; Stapnes, C.I.; Ersvaer, E.; Gjertsen., B.T.; Ryningen, A. Histone deacetylase inhibitors in cancer treatment: A review of the clinical toxicity and the modulation of gene expression in cancer cell. Curr. Pharm. Biotechnol. 2007, 8, 388–400. [Google Scholar] [CrossRef] [PubMed]
- Lubbert, M.; Bertz, H.; Wasch, R.; Marks, R.; Ruter, B.; Claus, R.; Finke, J. Efficacy of a 3-day, low-dose treatment with 5-azacytidine followed by donor lymphocyte infusions in older patients with acute myeloid leukemia or chronic myelomonocytic leukemia relapsed after allografting. Bone Marrow. Transplant. 2010, 45, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Fredly, H.; Stapnes Bjornsen, C.; Gjertsen, B.T.; Bruserud, Ø. Combination of the histone deacetylase inhibitor valproic acid with oral hydroxyurea or 6-mercaptopurin can be safe and effective in patients with advanced acute myeloid leukaemia—a report of five cases. Hematology 2010, 15, 338–343. [Google Scholar] [CrossRef]
- Grishina, O.; Schmoor, C.; Döhner, K.; Hackanson, B.; Lubrich, B.; May, A.M.; Cieslik, C.; Müller, M.J.; Lübbert, M. DECIDER: Prospective randomized multicenter phase II trial of low-dose decitabine (DAC) administered alone or in combination with the histone deacetylase inhibitor valproic acid (VPA) and all-trans retinoic acid (ATRA) in patients >60 years with acute myeloid leukemia who are ineligible for induction chemotherapy. BMC Cancer 2015, 15, 430. [Google Scholar]
- Garcia-Manero, G.; Kantarjian, H.M.; Sanchez-Gonzalez, B.; Yang, H.; Rosner, G.; Verstovsek, S.; Rytting, M.; Wierda, W.G.; Ravandi, F.; Koller, C.; et al. Phase 1/2 study of the combination of 5-aza-2′-deoxycytidine with valproic acid in patients with leukemia. Blood 2006, 108, 3271–3279. [Google Scholar] [CrossRef] [PubMed]
- Blum, W.; Klisovic, R.B.; Hackanson, B.; Liu, Z.; Liu, S.; Devine, H.; Vukosavljevic, T.; Huynh, L.; Lozanski, G.; Kefauver, C.; et al. Phase I study of decitabine alone or in combination with valproic acid in acute myeloid leukemia. J. Clin. Oncol. 2007, 25, 3884–3891. [Google Scholar] [CrossRef] [PubMed]
- Kuendgen, A.; Gattermann, N. Valproic acid for the treatment of myeloid malignancies. Cancer 2007, 110, 943–954. [Google Scholar] [CrossRef] [PubMed]
- Xuan, L.; Liu, Q. Maintenance therapy in acute myeloid leukemia after allogeneic hematopoietic stem cell transplantation. J. Hematol. Oncol. 2021, 14, 4. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, T.; Rautenberg, C.; Haas, R.; Germing, U.; Kobbe, G. Hypomethylating agents for treatment and prevention of relapse after allogeneic blood stem cell transplantation. Int. J. Hematol. 2018, 107, 138–150. [Google Scholar] [CrossRef]
- Czibere, A.; Bruns, I.; Kröger, N.; Platzbecker, U.; Lind, J.; Zohren, F.; Fenk, R.; Germing, U.; Schröder, T.; Gräf, T.; et al. 5-Azacytidine for the treatment of patients with acute myeloid leukemia or myelodysplastic syndrome who relapse after allo-SCT: A retrospective analysis. Bone Marrow. Transpl. 2010, 45, 872–876. [Google Scholar] [CrossRef]
- Steinmann, J.; Bertz, H.; Wäsch, R.; Marks, R.; Zeiser, R.; Bogatyreva, L.; Finke, J.; Lübbert, M. 5-Azacytidine and DLI can induce long-term remissions in AML patients relapsed after allograft. Bone Marrow. Transpl. 2015, 50, 690–695. [Google Scholar] [CrossRef]
- Tessoulin, B.; Delaunay, J.; Chevallier, P.; Loirat, M.; Ayari, S.; Peterlin, P.; Le Gouill, S.; Gastinne, T.; Moreau, P.; Mohty, M.; et al. Azacitidine salvage therapy for relapse of myeloid malignancies following allogeneic hematopoietic SCT. Bone Marrow Transpl. 2014, 49, 567–571. [Google Scholar] [CrossRef]
- Schroeder, T.; Rachlis, E.; Bug, G.; Stelljes, M.; Klein, S.; Steckel, N.K.; Wolf, D.; Ringhoffer, M.; Czibere, A.; Nachtkamp, K.; et al. Treatment of acute myeloid leukemia or myelodysplastic syndrome relapse after allogeneic stem cell transplantation with azacitidine and donor lymphocyte infusions—A retrospective multicenter analysis from the German Cooperative Transplant Study Group. Biol. Blood Marrow. Transpl. 2015, 21, 653–660. [Google Scholar] [CrossRef]
- Woo, J.; Deeg, H.J.; Storer, B.; Yeung, C.; Fang, M.; Mielcarek, M.; Scott, B.L. Factors determining responses to azacitidine in patients with myelodysplastic syndromes and acute myeloid leukemia with early post-transplantation relapse: A prospective trial. Biol. Blood Marrow. Transpl. 2017, 23, 176–179. [Google Scholar] [CrossRef]
- Sommer, S.; Cruijsen, M.; Claus, R.; Bertz, H.; Wäsch, R.; Marks, R.; Zeiser, R.; Bogatyreva, L.; Blijlevens, N.M.A.; May, A.; et al. Decitabine in combination with donor lymphocyte infusions can induce remissions in relapsed myeloid malignancies with higher leukemic burden after allogeneic hematopoietic cell transplantation. Leuk. Res. 2018, 72, 20–26. [Google Scholar] [CrossRef]
- Schroeder, T.; Rautenberg, C.; Krüger, W.; Platzbecker, U.; Bug, G.; Steinmann, J.; Klein, S.; Hopfer, O.; Nachtkamp, K.; Kondakci, M.; et al. Treatment of relapsed AML and MDS after allogeneic stem cell transplantation with decitabine and DLI-a retrospective multicenter analysis on behalf of the German Cooperative Transplant Study Group. Ann. Hematol. 2018, 97, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Craddock, C.; Slade, D.; De Santo, C.; Wheat, R.; Ferguson, P.; Hodgkinson, A.; Brock, K.; Cavenagh, J.; Ingram, W.; Dennis, M.; et al. Combination lenalidomide and azacitidine: A novel salvage therapy in patients who relapse after allogeneic stem-cell transplantation for acute myeloid leukemia. J. Clin. Oncol. 2019, 37, 580–588. [Google Scholar] [CrossRef] [PubMed]
- Thakar, M.S.; Forman, S.J. ASH evidence-based guidelines: Is there a role for second allogeneic transplant after relapse? Hematol. Am. Soc. Hematol. Educ. Program 2009, 414–418. [Google Scholar] [CrossRef]
- El-Jawahri, A.R.; Abel, G.A.; Steensma, D.P.; LeBlanc, T.W.; Fathi, A.T.; Graubert, T.A.; DeAngelo, D.J.; Wadleigh, M.; Ballen, K.K.; Foster, J.E.; et al. Health care utilization and end-of-life care for older patients with acute myeloid leukemia. Cancer 2015, 121, 2840–2848. [Google Scholar] [CrossRef]
- LeBlanc, T.W.; Wolf, S.P.; El-Jawahri, A.; Davis, D.M.; Locke, S.C.; Abernethy, A. Symptom burden, quality of life, and distress in acute myeloid leukemia patients receiving induction chemotherapy: Results of a prospective electronic patient-reported outcomes study. Blood 2015, 126, 4496. [Google Scholar] [CrossRef]
- Slavin, S.D.; Fenech, A.; Jankowski, A.L.; Abel, G.A.; Brunner, A.M.; Steensma, D.P.; Fathi, A.T.; DeAngelo, D.J.; Wadleigh, M.; Hobbs, G.S.; et al. Outcomes for older adults with acute myeloid leukemia after an intensive care unit admission. Cancer 2019, 125, 3845–3852. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.W.; Li, C.W.; Chan, K.Y.; Au, H.Y.; Chan, P.F.; Sin, Y.C.; Szeto, Y.; Sham, M.K. End-of-life characteristics and palliative care provision for elderly patients suffering from acute myeloid leukemia. Support Care Cancer 2015, 23, 111–116. [Google Scholar] [CrossRef]
- Lübbert, M.; Suciu, S.; Baila, L.; Rüter, B.H.; Platzbecker, U.; Giagounidis, A.; Selleslag, D.; Labar, B.; Germing, U.; Salih, H.R.; et al. Low-dose decitabine versus best supportive care in elderly patients with intermediate- or high-risk myelodysplastic syndrome (MDS) ineligible for intensive chemotherapy: Final results of the randomized phase III study of the European Organisation for Research and Treatment of Cancer Leukemia Group and the German MDS Study Group. J. Clin. Oncol. 2011, 29, 1987–1996. [Google Scholar]
- Kornblith, A.B.; Herndon, J.E., II; Silverman, L.R.; Demakos, E.P.; Odchimar-Reissig, R.; Holland, J.F.; Powell, B.L.; DeCastro, C.; Ellerton, J.; Larson, R.A.; et al. Impact of azacytidine on the quality of life of patients with myelodysplastic syndrome treated in a randomized phase III trial: A cancer and leukemia group B study. J. Clin. Oncol. 2002, 20, 2441–2452. [Google Scholar] [CrossRef]
- Bosshard, R.; O’Reilly, K.; Ralston, S.; Chadda, S.; Cork, D. Systematic reviews of economic burden and health-related quality of life in patients with acute myeloid leukemia. Cancer Treat. Rev. 2018, 69, 224–232. [Google Scholar] [CrossRef]
- Korol, E.E.; Wang, S.; Johnston, K.; Ravandi-Kashani, F.; Levis, M.; van Nooten, F. Health-related quality of life of patients with acute myeloid leukemia: A systematic literature. Rev. Oncol. Ther. 2017, 5, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, A.; Kessler, T.; Buchner, T.; Wewers, D.; van de Loo, J. Quality of life in adult patients with acute myeloid leukemia receiving intensive and prolonged chemotherapy—A longitudinal study. Leukemia 1998, 12, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Leunis, A.; Redekop, W.K.; Uyl-de Groot, C.A.; Lowenberg, B. Impaired health-related quality of life in acute myeloid leukemia survivors: A single-center study. Eur. J. Haematol. 2014, 93, 198–206. [Google Scholar] [CrossRef]
- Messerer, D.; Engel, J.; Hasford, J.; Schaich, M.; Ehninger, G.; Sauerland, C.; Büchner, T.; Schumacher, A.; Krahl, R.; Niederwieser, D.; et al. Impact of different post-remission strategies on quality of life in patients with acute myeloid leukemia. Haematologica 2008, 93, 826–833. [Google Scholar] [CrossRef]
- Gupta, V.; Panzarella, T.; Li, L.; Khan, J.; Sharma, A.; Lipton, J.H.; Kuruvilla, J.; Messner, H.; Alibhai, S.M. A prospective study comparing the outcomes and health-related quality of life in adult patients with myeloid malignancies undergoing allogeneic transplantation using myeloablative or reduced-intensity conditioning. Biol. Blood Marrow. Transpl. 2012, 18, 113–124. [Google Scholar] [CrossRef][Green Version]
- Watson, M.; Buck, G.; Wheatley, K.; Homewood, J.R.; Goldstone, A.H.; Rees, J.K.; Burnett, A.K. Adverse impact of bone marrow transplantation on quality of life in acute myeloid leukaemia patients: Analysis of the UK Medical Research Council AML 10 Trial. Eur. J. Cancer 2004, 40, 971–978. [Google Scholar] [CrossRef]
- Kurosawa, S.; Yamaguchi, T.; Mori, T.; Kanamori, H.; Onishi, Y.; Emi, N.; Fujisawa, S.; Kohno, A.; Nakaseko, C.; Saito, B.; et al. Patient-reported quality of life after allogeneic hematopoietic cell transplantation or chemotherapy for acute leukemia. Bone Marrow Transpl. 2015, 50, 1241–1249. [Google Scholar] [CrossRef]
- Bazarbachi, A.H.; Al Hamed, R.; Malard, F.; Mohty, M.; Bazarbachi, A. Allogeneic transplant for FLT3-ITD mutated AML: A focus on FLT3 inhibitors before, during, and after transplant. Ther. Adv. Hematol. 2019, 10. [Google Scholar] [CrossRef]
- Sockel, K.; Bornhaeuser, M.; Mischak-Weissinger, E.; Trenschel, R.; Wermke, M.; Unzicker, C.; Kobbe, G.; Finke, J.; Germing, U.; Mohr, B.; et al. Lenalidomide maintenance after allogeneic HSCT seems to trigger acute graft-versus-host disease in patients with high-risk myelodysplastic syndromes or acute myeloid leukemia and del(5q): Results of the LENAMAINT trial. Haematologica 2012, 97, e34–e35. [Google Scholar] [CrossRef] [PubMed]
- El-Cheikh, J.; Massoud, R.; Fares, E.; Kreidieh, N.; Mahfouz, R.; Charafeddine, M.; Kharfan-Dabaja, M.A.; Bazarbachi, A. Low-dose 5-azacytidine as preventive therapy for relapse of AML and MDS following allogeneic HCT. Bone Marrow Transpl. 2017, 52, 918–921. [Google Scholar] [CrossRef] [PubMed]
- De Lima, M.; Giralt, S.; Thall, P.F.; de Padua Silva, L.; Jones, R.B.; Komanduri, K.; Braun, T.M.; Nguyen, H.Q.; Champlin, R.; Garcia-Manero, G. Maintenance therapy with low-dose azacitidine after allogeneic hematopoietic stem cell transplantation for recurrent acute myelogenous leukemia or myelodysplastic syndrome: A dose and schedule finding study. Cancer 2010, 116, 5420–5431. [Google Scholar] [CrossRef]
- De Lima, M.; Oran, B.; Champlin, R.E.; Papadopoulos, E.B.; Giralt, S.A.; Scott, B.L.; William, B.M.; Hetzer, J.; Laille, E.; Hubbell, B.; et al. CC-486 maintenance after stem cell transplantation in patients with acute myeloid leukemia or myelodysplastic syndromes. Biol. Blood Marrow Transpl. 2018, 24, 2017–2024. [Google Scholar] [CrossRef] [PubMed]
- Pusic, I.; Choi, J.; Fiala, M.A.; Gao, F.; Holt, M.; Cashen, A.F.; Vij, R.; Abboud, C.N.; Stockerl-Goldstein, K.E.; Jacoby, M.A.; et al. Maintenance therapy with decitabine after allogeneic stem cell transplantation for acute myelogenous leukemia and myelodysplastic syndrome. Biol. Blood Marrow Transpl. 2015, 21, 1761–1769. [Google Scholar] [CrossRef] [PubMed]
- Oshikawa, G.; Kakihana, K.; Saito, M.; Aoki, J.; Najima, Y.; Kobayashi, T.; Doki, N.; Sakamaki, H.; Ohashi, K. Post-transplant maintenance therapy with azacitidine and gemtuzumab ozogamicin for high-risk acute myeloid leukaemia. Br. J. Haematol. 2015, 169, 756–759. [Google Scholar] [CrossRef]
- Schmid, C.; Labopin, M.; Schaap, N.; Veelken, H.; Schleuning, M.; Stadler, M.; Finke, J.; Hurst, E.; Baron, F.; Ringden, O.; et al. Prophylactic donor lymphocyte infusion after allogeneic stem cell transplantation in acute leukaemia—A matched pair analysis by the Acute Leukaemia Working Party of EBMT. Br. J. Haematol. 2019, 184, 782–787. [Google Scholar] [CrossRef]
- Platzbecker, U.; Middeke, J.M.; Sockel, K.; Herbst, R.; Wolf, D.; Baldus, C.D.; Oelschlägel, U.; Mütherig, A.; Fransecky, L.; Noppeney, R.; et al. Measurable residual disease-guided treatment with azacitidine to prevent haematological relapse in patients with myelodysplastic syndrome and acute myeloid leukaemia (RELAZA2): An open-label, multicentre, phase 2 trial. Lancet Oncol. 2018, 19, 1668–1679. [Google Scholar] [CrossRef]
- Platzbecker, U.; Wermke, M.; Radke, J.; Oelschlaegel, U.; Seltmann, F.; Kiani, A.; Klut, I.M.; Knoth, H.; Röllig, C.; Schetelig, J.; et al. Azacitidine for treatment of imminent relapse in MDS or AML patients after allogeneic HSCT: Results of the RELAZA trial. Leukemia 2012, 26, 381–389. [Google Scholar] [CrossRef]
- Liu, N.; Wang, C.; Wang, L.; Gao, L.; Cheng, H.; Tang, G.; Hu, X.; Wang, J. Valproic acid enhances the antileukemic effect of cytarabine by triggering cell apoptosis. Int. J. Mol. Med. 2016, 37, 1686–1696. [Google Scholar] [CrossRef][Green Version]
- Xie, C.; Edwards, H.; Xu, X.; Zhou, H.; Buck, S.A.; Stout, M.L.; Yu, Q.; Rubnitz, J.E.; Matherly, L.H.; Taub, J.W.; et al. Mechanisms of synergistic antileukemic interactions between valproic acid and cytarabine in pediatric acute myeloid leukemia. Clin. Cancer Res. 2010, 16, 5499–5510. [Google Scholar] [CrossRef]
- Leitch, C.; Osdal, T.; Andresen, V.; Molland, M.; Kristiansen, S.; Nguyen, X.N.; Bruserud, Ø.; Gjertsen, B.T.; McCormack, E. Hydroxyurea synergizes with valproic acid in wild-type p53 acute myeloid leukaemia. Oncotarget 2016, 7, 8105–8118. [Google Scholar] [CrossRef]
- Heo, S.K.; Noh, E.K.; Yoon, D.J.; Jo, J.C.; Park, J.H.; Kim, H. Dasatinib accelerates valproic acid-induced acute myeloid leukemia cell death by regulation of differentiation capacity. PLoS ONE 2014, 9, e98859. [Google Scholar] [CrossRef]
- McCormack, E.; Haaland, I.; Venås, G.; Forthun, R.B.; Huseby, S.; Gausdal, G.; Knappskog, S.; Micklem, D.R.; Lorens, J.B.; Bruserud, Ø.; et al. Synergistic induction of p53 mediated apoptosis by valproic acid and nutlin-3 in acute myeloid leukemia. Leukemia 2012, 26, 910–917. [Google Scholar] [CrossRef] [PubMed]
- Nie, D.; Huang, K.; Yin, S.; Li, Y.; Xie, S.; Ma, L.; Wang, X.; Wu, Y.; Xiao, J. Synergistic/additive interaction of valproic acid with bortezomib on proliferation and apoptosis of acute myeloid leukemia cells. Leuk. Lymphoma 2012, 53, 2487–2495. [Google Scholar] [CrossRef]
- Wang, A.H.; Wei, L.; Chen, L.; Zhao, S.Q.; Wu, W.L.; Shen, Z.X.; Li, J.M. Synergistic effect of bortezomib and valproic acid treatment on the proliferation and apoptosis of acute myeloid leukemia and myelodysplastic syndrome cells. Ann. Hematol. 2011, 90, 917–931. [Google Scholar] [CrossRef] [PubMed]
- Xie, C.; Edwards, H.; Lograsso, S.B.; Buck, S.A.; Matherly, L.; Taub, J.W.; Ge, Y. Valproic acid synergistically enhances the cytotoxicity of clofarabine in pediatric acute myeloid leukemia cells. Pediatr. Blood Cancer 2012, 59, 1245–1251. [Google Scholar] [CrossRef]
- Stahl, M.; Gore, S.D.; Vey, N.; Prebet, T. Lost in translation? Ten years of development of histone deacetylase inhibitors in acute myeloid leukemia and myelodysplastic syndromes. Expert Opin. Investig. Drugs 2016, 25, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Morabito, F.; Voso, M.T.; Hohaus, S.; Gentile, M.; Vigna, E.; Recchia, A.G.; Iovino, L.; Benedetti, E.; Lo-Coco, F.; Galimberti, S. Panobinostat for the treatment of acute myelogenous leukemia. Expert Opin. Investig. Drugs 2016, 25, 1117–1131. [Google Scholar] [CrossRef]
- Ungerstedt, J.S. Epigenetic modifiers in myeloid malignancies: The role of histone deacetylase inhibitors. Int. J. Mol. Sci. 2018, 19, 3091. [Google Scholar] [CrossRef]
- Qin, H.T.; Li, H.Q.; Liu, F. Selective histone deacetylase small molecule inhibitors: Recent progress and perspectives. Expert Opin. Ther. Pat. 2017, 27, 621–636. [Google Scholar] [CrossRef]
- Cengiz Seval, G.; Beksac, M. A comparative safety review of histone deacetylase inhibitors for the treatment of myeloma. Expert Opin. Drug Saf. 2019, 18, 563–571. [Google Scholar] [CrossRef]
- Allen, P.B.; Lechowicz, M.J. Hematologic toxicity is rare in relapsed patients treated with belinostat: A systematic review of belinostat toxicity and safety in peripheral T-cell lymphomas. Cancer Manag. Res. 2018, 10, 6731–6742. [Google Scholar] [CrossRef] [PubMed]
- Leufven, E.; Bruserud, Ø. Immunosuppression and immunotargeted therapy in acute myeloid leukemia—The potential use of checkpoint inhibitors in combination with other treatments. Curr. Med. Chem. 2019, 26, 5244–5261. [Google Scholar] [CrossRef] [PubMed]
- Sterling, C.; Webster, J. Harnessing the immune system after allogeneic stem cell transplant in acute myeloid leukemia. Am. J. Hematol. 2020, 95, 529–547. [Google Scholar] [CrossRef] [PubMed]
- Merryman, R.W.; Castagna, L.; Giordano, L.; Ho, V.T.; Corradini, P.; Guidetti, A.; Casadei, B.; Bond, D.A.; Jaglowski, S.; Spinner, M.A.; et al. Allogeneic transplantation after PD-1 blockade for classic Hodgkin lymphoma. Leukemia 2021. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Advani, A.S.; Tse, W.; Li, H.; Jia, X.; Elson, P.; Cooper, B.; Ali-Osman, F.; Park, J.; Rao, A.V.; Rizzieri, D.A.; et al. A Phase II trial of imatinib mesylate as maintenance therapy for patients with newly diagnosed c-kit-positive acute myeloid leukemia. Clin. Lymphoma Myeloma Leuk. 2021, 21, 113–118. [Google Scholar] [CrossRef]
- Chang Muñoz, M.; Murphy, J.A.; Wolff, J.E.; Jonas, B.A. Prolonged response of a patient with relapsed acute myeloid leukemia to a novel oral bromodomain extraterminal inhibitor (BETi). Case Rep. Hematol. 2020, 2020, 8830123. [Google Scholar]
- DiNardo, C.D.; Maiti, A.; Rausch, C.R.; Pemmaraju, N.; Naqvi, K.; Daver, N.G.; Kadia, T.M.; Borthakur, G.; Ohanian, M.; Alvarado, Y.; et al. 10-day decitabine with venetoclax for newly diagnosed intensive chemotherapy ineligible, and relapsed or refractory acute myeloid leukaemia: A single-centre, phase 2 trial. Lancet. Haematol. 2020, 7, e724–e736. [Google Scholar] [CrossRef]


{kind=link}
| Valproic Acid | ATRA | |
|---|---|---|
| Chemical classification | Branched short-chain fatty acid | Vitamin A derivative/retinoid |
| Molecular target | Regulates transcription through inhibition of histone deacetylation and therefore increased gene transcription. HDACs are grouped into class I (HDACs 1/2/3/8), class II (HDACs 4/5/6/7/9/10), class III (the sirtuins SIRT1-7), and class IV (only HDAC11). Valproic acid inhibits class I and class II HDACs, but HDACs 9/11 are activated and HDACs 6/8/10 are not affected. | The retinoic acid receptors (RARs) and retinoid X receptors (RXRs) are ligand-activated nuclear receptors. ATRA is a high-affinity activating ligand of the three RARα/β/γ receptors and is involved in the transcriptional regulation of hundreds of genes. |
| Cellular effects | Altered protein acetylation, including altered histone acetylation and altered acetylation of many other cellular proteins including cytoplasmic proteins | Altered transcriptional regulation mediated by its binding to the nuclear RAR receptors |
| Possible interactions at the cellular level | Valproic acid seems to influence the differentiation-inducing effect of ATRA; it also increases aldehyde dehydrogenase activity and may therefore have effects on vitamin A metabolism. | There is a molecular crosstalk between HDACs/histone acetylases and ATRA; ATRA also influences gene expression through epigenetic modulation. |
| Effects on normal hematopoiesis | Valproic acid seems to stimulate stem cell proliferation. Experimental studies suggest that it upregulates genes important for myelomonocytic differentiation but inhibits expression of genes important for erythroid differentiation. Drug-induced cytopenias are usually dose-dependent and reversible. | A majority of studies suggest that ATRA promotes the activity of hematopoietic stem cells and regulates differentiation of hematopoietic progenitor cells. |
| Systemic metabolic effect | Altered serum levels of several amino acid and fatty acid metabolites | Altered serum levels of several amino acid and fatty acid metabolites |
| Administration | Oral or intravenous | Oral |
| Monitoring of doses | Defined therapeutic serum levels make monitoring possible | Dosing based on body surface area |
| Accepted indication | Epilepsy, depression | Treatment of APL |
| Previous clinical studies in non-APL variants of AML | Mainly phase I/II studies of AML-stabilizing treatment, often in combination with ATRA | Phase I/II clinical studies of AML stabilizing treatment and randomized clinical studies in combination with intensive chemotherapy |
| Pretreatment Differences between Responders and vs. Nonresponders | |
|---|---|
| Proteomic Effects | Phosphoproteomic Effects |
| Responders: High levels of proteins reflecting neutrophil differentiation, intracellular transport, p53 signaling, and amino acid metabolism Nonresponders: high levels of proteins involved in transcription, cytoplasmic organelles, and lipid metabolism | Responders: High phosphorylation of proteins reflecting cytoskeleton organization, cell cycle regulation, membrane bound, and extracellular organelles Nonresponders: high phosphorylation of proteins involved in RNA binding/splicing |
| in vivo effects of ATRA | |
| Responders: Altered ribonucleoprotein assembly, RNA biosynthetic process, histone modification, chromatin binding, kinase activity, and signal transduction Nonresponders: altered extracellular secretion/organelles, clathrin complex, cytoskeleton organization, and RNA function/synthesis | Responders: Altered RNA processing and splicing, Rho GTPase binding, Rac GTPase binding, transcription elongation, and ribosome Nonresponders: RNA splicing and processing, nuclear body, and plasma membrane |
| Further modulation by adding valproic acid to ATRA in vivo | |
| Responders: Further modulation of mitochondrial function, ribonucleoprotein assembly, and kinase activity Nonresponders: RNA binding and splicing, mRNA function, and clathrin complex | Responders: Altered RNA processing, nuclear speck, and actin filament binding; further modulation of Rac GTPase binding and transcription elongation Nonresponders: Altered cyclin-dependent protein ser/thr kinase activity, and cellular catabolic process; further modulation of RNA splicing/processing |
| Valproic acid [35,37,114,115] Treatment started on day 1 of the first cycle and continued until disease progression. Early start of valproic acid therapy was regarded as important because it will often take 2–3 weeks before a response can be detected. First administered as intravenous infusion to reach a relevant therapeutic level as early as possible. The dose was increased until one reached the highest level with acceptable toxicity or the recommended therapeutic serum level. Previous studies suggest that systemic levels lower than the therapeutic serum level can be effective. |
| ATRA [35,37] Administered for days 1–14 of each five-week cycle. The daily dose was 22.5 mg/m2 twice daily; this is similar to the dose used in APL. A fourteen day duration has been used in previous AML studies of ATRA/valproic acid therapy. ATRA syndrome has not been observed with this dose and duration of treatment. |
| Azacitidine [137] Included patients were regarded as unfit for more intensive treatment. The risk of severe toxicity was reduced using a fixed dose of 100 mg daily for the first three days of each cycle. The three-day low-toxicity regimen has a clinically relevant antileukemic effect in posttransplant AML relapse and can be effective even in patients with high-risk karyotypes. The interval (i.e., duration of each cycle) was increased to five weeks to further reduce the risk of severe toxicity. Azacitidine started early from day 1 because it may last several weeks before a response is seen (see Section 7.1). |
| Hydroxyurea [35,37,138] The use of hydroxyurea in addition to ATRA/valproic acid was allowed in previous studies. It started on day 15 of the first cycle to reduce the risk of initial severe toxicity. In later cycles, it was administered at days 5–35 to avoid overlap with the azacitidine. To reduce the risk of severe hematological toxicity, hydroxyurea dosing was guided by normal peripheral blood cell counts and the level of circulating AML blasts in peripheral blood. If this leukocytosis could not be controlled (defined as >50 × 109/L), we changed it to oral merkaptopurin or subcutaneous cytarabine, and we then used the same guideline as for hydroxyurea for dosing of these two drugs [138]. |
| CASE 1 | CASE 2 | CASE 3 | CASE 4 | |
|---|---|---|---|---|
| Age/gender | 22 years/male | 57 years/female | 63 years/male | 55 years, female |
| Status at inclusion | Second relapse 122 days after second allo-SCT | Second relapse 71 days after allo-SCT | First relapse 113 days after allo-SCT | AML relapse 20 months after allo-SCT for aCML |
| Status at allo-SCT | Second remission | Second remission | First remission | Remission |
| Stem cell donor | HLA identical sibling donor | MUD | HLA identical sibling | HLA identical sibling |
| Conditioning | Myeloablative | Myeloablative | Reduced intensity | Reduced intensity |
| Bone marrow blasts | 56% | 30% | >20% on biopsy | 21% |
| Acute GVHD | Skin, GI-tract | Skin, GI tract | Skin, GI tract | No |
| ECOG status | 0 | 2 | 0 | 0 |
| Pretreatment peripheral blood cells/transfusions | ||||
| Hemoglobin | 12.0 g/100 mL | 10.5 g/100 mL | 10.2 g/100 mL | 10.1 g/100 mL |
| Neutrophils (×109/L) | 2.4 × 109/L | 4.5 × 109/L | 1.0 × 109/L | 0.5 × 109/L |
| Platelets (×109/L) | 88 (decreasing to 21) × 109/L | 13 × 109/L | 6 × 109/L | 12 × 109/L |
| AML blasts (×109/L) | 2.5 × 109/L | 1.5 × 109/L | <1% of leukocytes | <0.2 × 109/L |
| Valproic acid levels during first cycle | 253 μmol/L after iv and 40–50 μmol/L after oral administration | Exceeding 400 μmol/L after iv but <100 μmol/L after oral administration | ||
| Red cell/platelet transfusions first cycle | 2/0 | Cycle 1 not completed | Cycle 1 not completed | |
| Survival | ||||
| From (last) allo-SCT | 240 days | 100 days | 132 days | 23 months |
| From relapse | 133 days | 29 days | 62 days | 110 days |
| From start of therapy | 128 days | 24 days | 46 days | 128 days |
| From progression | 29 days | No response | No response | 30 days |
| Morphological definition of AML relapse |
| At least 5% myeloblasts in the bone marrow in a patient with previous diagnosis of AML; if less than 10% of blasts, the increased blast count should be verified in a second bone marrow sample. |
| Therapeutic strategy depending on the status at the time of intervention |
| Maintenance therapy: No evidence for residual disease, i.e., molecular remission. Pre-emptive therapy: Detection of posttransplant minimal residual disease. Salvage therapy: Morphological signs of relapse. |
| Pharmacological strategies |
| Intensive chemotherapy, e.g., conventional induction chemotherapy that results in complete remission usually of short duration for 25–30% of patients. Low-toxicity chemotherapy, e.g., hypomethylating agents that results in 15–20% complete remissions. Targeted therapy: The pharmacological agent depends on the AML-associated genetic abnormalities, e.g., IDH1/IDH2 inhibitors when IDH mutations and Flt3 inhibitors in patients with Flt3-ITD. The bcl2-inhibitor venetoclax is now investigated in clinical trials. The HDAC inhibitor panobinostat is in clinical trials. |
| Antileukemic immunomodulation |
| Early reduction of GVHD prophylaxis Donor lymphocytes infusion Re-transplantation after remission induction |
| Study | Treatment | Effect | Toxicity and GVHD |
|---|---|---|---|
| Lübbert et al. [137]. Retrospective (n = 26). Time from transplant to relapse median 248 days (55–1412 days). | Azacitidine 100 mg total daily dose, days 1–3 with 21 days intervals, could be followed by DLI was allowed. Median number of cycles 2 (range 1–10). | Complete remission in 4 patients with duration 450–820 days. 50% with temporary disease control. Median survival 136 days | Neutropenic infections in 4 patients. Acute GVHD 2 patients. |
| Czibere et al. [145]. Retrospective (n = 22). Time from transplant to relapse|03 days (53–708 days). | Azacitidine 100 mg/m2 daily days 1–5, 2–5 weeks interval, DLI was allowed. Median number of cycles 2 (range 1–8). | Response to azacitidine: 16 patients. Median time to relapse 433 days (range 114–769 days); median survival 144 days. | Acute GVHD in 6 patients. Hematological toxicity grade 4 in 7 patient; neutropenic infections in 6 patients. |
| Steinmann et al. [146]. Retrospective (n = 72). Time from allograft to relapse 253 days (50–2126 days). | Azacitidine 100 mg daily for 3 days (5 days in first cycle if leukocytosis) and repeated every 3 weeks. Median number of cycles 2.7; 65 patients received DLI | Complete remission 9.7% (for two patients lasting >5 years), temporary disease control 44%. Median survival 108 days; peripheral blood blasts <1% predicted longer survival. | 10 patients developed acute GVHD; 9 patients with chronic GVHD. 2 patients with therapy-related sepsis. 28/72 hospitalized due to infections; 15 patients with grade 3/4 neutropenia. |
| Tessoulin et al. [147]. Retrospective (n = 31). Time from transplant to relapse median 3.7 months (range 1.7–37.6 months). | Azacitidine 75 mg/m2 daily for 7 days every 4 weeks. DLI was allowed. Median number of cycles 3 (range 1–12). | 4 complete remissions. 11/31 patients responded to the treatment. Median overall survival 153 days. | Grade 3/4 toxicities in 36% of patients. 38% readmitted to hospital, the most common reasons being fever, infection, or neutropenia. |
| Schroeder et al. [148]. Retrospective (n = 154). Time from transplant to relapse median 185 days (19–3349 days). | Azacitidine 50–100 mg/m2 for 5–7 days every 4 weeks. DLI allowed. Median number of cycles 4 (4–14). | Complete remission 27%; overall response rate 33%. Better overall survival for patients with MDS or <13% bone marrow blasts; 2-years survival 29%. | Acute GVHD 23%. Chronic GVHD 27%. |
| Craddock et al. [135]. Retrospective (n = 181). Time from transplant to relapse median 8 months (1–71 months). | Azacitidine 75 mg/m2 for 5–7 days every 4 weeks; DLI was allowed. Median duration of treatment 53 days (range 2–1196 days). | 29.3% with complete or partial remission. Higher response rates for patients transplanted in remission and for MDS. Longer survival for patients with low blast counts (<20%) or >6 month from transplant to relapse. | |
| Woo et al. [149]. Prospective (n = 39). Patients with morphological relapse or evidence for persisting disease (flow cytometry, karyotyping) before day +100. | Azacitidine 75 mg/m2 daily for 7 days every 4 weeks (≥6 cycles; DLI allowed). Median bone marrow blasts 1.4%. | 3 patients with complete remission; 9 patients with partial remission. 3 additional patients with stabilization. 2-years overall survival 25%. | Acute GVHD 29 patients, 4 with grade III. |
| Sommer et al. [150]. Retrospective (n = 26). Time from transplant to relapse median 306 days (76–4943). | Decitabine 20 mg/m2 daily for 5 or 10 days every 4 weeks; one DLI during each cycle was allowed. Median number of cycles 2 (range 1–13). | Complete remission 4/26, partial remission 1/26. Median overall survival 4.7 months. | Acute GVHD 17%. Chronic GVHD 6%. |
| Schroeder et al. [151]. Retrospective (n = 36). Median time to relapse 370 days (43 2623). | Decitabine 20 mg/m2 daily for 5 or 10 days with 4 weeks interval.; DLI was allowed Median number of cycles 2 (range 1 11). | Overall response rate 25% including 6 patients with complete remission. Two patients who failed azacitidine reached complete remission. | Acute GVHD in 7 patients; for 2 of them no previous DLI. 2 patients with symptoms of chronic GVHD. after DLI. |
| Craddock et al. [152]. Prospective (n = 29). Median time to relapse 10 months (1–39 months). | Azacitidine 75 mg/m2 days 1–7 followed by lenalidomide (25 mg daily determined as the maximal tolerated dose) days 10–30. Median number of cycles 3 (0–11). | Among 15 patients receiving at least 3 cycles, there were 3 complete remissions, 3 with complete remission without complete regeneration, and 1 partial remission. Median overall survival was 27 months for responders and 10 months for nonresponders. | 3 patients developed acute GVHD grade 2–4. Febrile neutropenia observed in 10 patients; documented infections in 3 patients and sepsis in 7 patients. |
| Study | Study Design | Observations |
|---|---|---|
| Liu et al. [178] Cytarabine | In vitro studies of AML cell lines and primary human AML cell lines | Increased BAX expression detected at the mRNA level leading to reduced AML cell proliferation, sub-G1 arrest, and apoptosis |
| Xie et al. [179] Cytarabine | In vitro studies of pediatric t(8;21) positive and negative AML cells | t(8;21)-positive cells were most susceptible to the combined treatment with induction of DNA double-stranded breaks together with induction of Bim-mediated and caspase-dependent apoptosis. |
| Leitch et al. [180] Hydroxyurea, an antimetabolite causing stalling of S-phase replication forks | AML cell lines and primary patient cells evaluated in vitro and in xenograft models | Valproic acid amplified the ability of hydroxyurea to slow S-phase progression; this effect was correlated with increased DNA damage. Reduced expression of the DNA repair protein Rad51 |
| Blagitko-Dorfs et al. [122] DNA methyl transferase inhibitors | AML cell lines | Combined treatment affected more transcripts than the sum of the genes altered by either treatment alone; downregulation of oncogenes and epigenetic modifiers |
| Xie et al. [185] Clofarabine, a second generation purine nucleoside analog | Pediatric cell lines and primary samples studied in vitro | Synergistic antileukemic effects in cells sensitive to valproic acid with Bax activation and apoptosis; for valproic acid-resistant cells, antagonistic effects were observed. |
| Heo et al. [181] Dasatinib, a multi-targeted kinase inhibitor | AML cell lines and patient samples investigated in vitro | Synergistic effects with G1 phase cell cycle arrest and induction of caspase-dependent apoptosis. The effects seemed to be mediated by MEK/ERK and p38 MAP kinases. |
| McCormack et al. [182] Nutlin 3, a MDM2 antagonist | AML cell lines and patient cells tested in vitro and in xenograft models | Cotreatment resulted in the induction of p53, acetylated p53, and p53 target genes compared with either agent tested alone; this was followed by p53-dependent cell death with autophagic features. |
| Wang et al. [184] Bortezomib, a proteasome inhibitor | In vitro studies of AML cell lines and primary AML cells | Antiproliferative and proapoptotic effects with increased mitochondrial injury and caspase activation. They observed reduced NFκB, Akt, and ERK signaling and activation of stress-induced pathways (e.g., JNK and p38). The combination caused G2/M arrest and increased p21. |
| Nie et al. [183] Bortezomib | The HL60 cell line | G0/G1 arrest with induction of apoptosis, inhibition of cyclin D1, and telomerase activity |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bruserud, Ø.; Tsykunova, G.; Hernandez-Valladares, M.; Reikvam, H.; Tvedt, T.H.A. Therapeutic Use of Valproic Acid and All-Trans Retinoic Acid in Acute Myeloid Leukemia—Literature Review and Discussion of Possible Use in Relapse after Allogeneic Stem Cell Transplantation. Pharmaceuticals 2021, 14, 423. https://doi.org/10.3390/ph14050423
Bruserud Ø, Tsykunova G, Hernandez-Valladares M, Reikvam H, Tvedt THA. Therapeutic Use of Valproic Acid and All-Trans Retinoic Acid in Acute Myeloid Leukemia—Literature Review and Discussion of Possible Use in Relapse after Allogeneic Stem Cell Transplantation. Pharmaceuticals. 2021; 14(5):423. https://doi.org/10.3390/ph14050423
Chicago/Turabian StyleBruserud, Øystein, Galina Tsykunova, Maria Hernandez-Valladares, Hakon Reikvam, and Tor Henrik Anderson Tvedt. 2021. "Therapeutic Use of Valproic Acid and All-Trans Retinoic Acid in Acute Myeloid Leukemia—Literature Review and Discussion of Possible Use in Relapse after Allogeneic Stem Cell Transplantation" Pharmaceuticals 14, no. 5: 423. https://doi.org/10.3390/ph14050423
APA StyleBruserud, Ø., Tsykunova, G., Hernandez-Valladares, M., Reikvam, H., & Tvedt, T. H. A. (2021). Therapeutic Use of Valproic Acid and All-Trans Retinoic Acid in Acute Myeloid Leukemia—Literature Review and Discussion of Possible Use in Relapse after Allogeneic Stem Cell Transplantation. Pharmaceuticals, 14(5), 423. https://doi.org/10.3390/ph14050423