
Individualized versus Standardized Risk Assessment in Patients at High Risk for Adverse Drug Reactions (The IDrug Randomized Controlled Trial)–Never Change a Running System?

 , , ,
, , , 
Abstract
:1. Introduction
2. Results
Secondary Analyses
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Study Population
4.3. Study Centers
4.4. Intervention
4.5. Data Collection
4.6. Laboratory Methods
4.7. Phenotype Assessments
4.8. Antithrombotic Treatment
4.9. Study Outcome
4.10. Randomization, Allocation to Study Arm, and Blinding
4.11. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Budnitz, D.S.; Lovegrove, M.C.; Shehab, N.; Richards, C.L. Emergency hospitalizations for adverse drug events in older Americans. N. Engl. J. Med. 2011, 365, 2002–2012. [Google Scholar] [CrossRef]
- Budnitz, D.S.; Shehab, N.; Kegler, S.R.; Richards, C.L. Medication use leading to emergency department visits for adverse drug events in older adults. Ann. Intern. Med. 2007, 147, 755–765. [Google Scholar] [CrossRef]
- Pirmohamed, M.; James, S.; Meakin, S.; Green, C.; Scott, A.K.; Walley, T.J.; Farrar, K.; Park, B.K.; Breckenridge, A.M. Adverse drug reactions as cause of admission to hospital: Prospective analysis of 18,820 patients. BMJ 2004, 329, 15–19. [Google Scholar] [CrossRef] [Green Version]
- Oscanoa, T.J.; Lizaraso, F.; Carvajal, A. Hospital admissions due to adverse drug reactions in the elderly. A meta-analysis. Eur. J. Clin. Pharmacol. 2017, 73, 759–770. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.; Nicklason, F.; Vial, J.H. Adverse drug events as a cause of hospital admission in the elderly. Intern. Med. J. 2001, 31, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Just, K.S.; Dormann, H.; Schurig, M.; Böhme, M.; Steffens, M.; Plank-Kiegele, B.; Ettrich, K.; Seufferlein, T.; Gräff, I.; Igel, S.; et al. The phenotype of adverse drug effects: Do emergency visits due to adverse drug reactions look different in older people? Results from the ADRED study. Br. J. Clin. Pharmacol. 2020, 86, 2144–2154. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, F.J.; Rosendaal, F.R.; Vandenbroucke, J.P.; Briët, E. Bleeding complications in oral anticoagulant therapy. An analysis of risk factors. Arch. Intern. Med. 1993, 153, 1557–1562. [Google Scholar] [CrossRef] [PubMed]
- Ruff, C.T.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B.; Deenadayalu, N.; Ezekowitz, M.D.; Camm, A.J.; Weitz, J.I.; Lewis, B.S.; Parkhomenko, A.; et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef]
- García Rodríguez, L.A.; Lin, K.J.; Hernández-Díaz, S.; Johansson, S. Risk of upper gastrointestinal bleeding with low-dose acetylsalicylic acid alone and in combination with clopidogrel and other medications. Circulation 2011, 123, 1108–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamburg, M.A.; Collins, F.S. The path to personalized medicine. N. Engl. J. Med. 2010, 363, 301–304. [Google Scholar] [CrossRef]
- Edwards, I.R.; Aronson, J.K. Adverse drug reactions: Definitions, diagnosis, and management. Lancet 2000, 356, 1255–1259. [Google Scholar] [CrossRef]
- Johnson, J.A.; Caudle, K.E.; Gong, L.; Whirl-Carrillo, M.; Stein, C.M.; Scott, S.A.; Lee, M.T.; Gage, B.F.; Kimmel, S.E.; Perera, M.A.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for Pharmacogenetics-Guided Warfarin Dosing: 2017 Update. Clin. Pharmacol. Ther. 2017, 102, 397–404. [Google Scholar] [CrossRef] [Green Version]
- Glaeske, G.; Schicktanz, C. Barmer GEK Arzneimittelreport 2015; Barmer GEK: St. Augustin, Germany, 2015. [Google Scholar]
- Schneider, K.L.; Kunst, M.; Leuchs, A.K.; Bohme, M.; Weckbecker, K.; Kastenmuller, K.; Bleckwenn, M.; Holdenrieder, S.; Coch, C.; Hartmann, G.; et al. Phenprocoumon Dose Requirements, Dose Stability and Time in Therapeutic Range in Elderly Patients With CYP2C9 and VKORC1 Polymorphisms. Front. Pharmacol. 2019, 10, 1620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sconce, E.A.; Kamali, F. Appraisal of current vitamin K dosing algorithms for the reversal of over-anticoagulation with warfarin: The need for a more tailored dosing regimen. Eur. J. Haematol. 2006, 77, 457–462. [Google Scholar] [CrossRef]
- Dücker, C.M.; Brockmöller, J. Genomic Variation and Pharmacokinetics in Old Age: A Quantitative Review of Age- vs. Genotype-Related Differences. Clin. Pharmacol. Ther. 2019, 105, 625–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banovac, M.; Candore, G.; Slattery, J.; Houÿez, F.; Haerry, D.; Genov, G.; Arlett, P. Patient Reporting in the EU: Analysis of EudraVigilance Data. Drug Saf. 2017, 40, 629–645. [Google Scholar] [CrossRef]
- Stingl, J.C.; Kaumanns, K.L.; Claus, K.; Lehmann, M.L.; Kastenmüller, K.; Bleckwenn, M.; Hartmann, G.; Steffens, M.; Wirtz, D.; Leuchs, A.K.; et al. Individualized versus standardized risk assessment in patients at high risk for adverse drug reactions (IDrug)—Study protocol for a pragmatic randomized controlled trial. BMC Fam. Pr. 2016, 17, 49. [Google Scholar] [CrossRef] [Green Version]
- Van der Sijs, H.; Mulder, A.; van Gelder, T.; Aarts, J.; Berg, M.; Vulto, A. Drug safety alert generation and overriding in a large Dutch university medical centre. Pharm. Drug Saf. 2009, 18, 941–947. [Google Scholar] [CrossRef]
- Phansalkar, S.; Zachariah, M.; Seidling, H.M.; Mendes, C.; Volk, L.; Bates, D.W. Evaluation of medication alerts in electronic health records for compliance with human factors principles. J. Am. Med. Inform. Assoc. 2014, 21, e332–e340. [Google Scholar] [CrossRef] [Green Version]
- Hylek, E.M.; Evans-Molina, C.; Shea, C.; Henault, L.E.; Regan, S. Major hemorrhage and tolerability of warfarin in the first year of therapy among elderly patients with atrial fibrillation. Circulation 2007, 115, 2689–2696. [Google Scholar] [CrossRef] [Green Version]
- Van der Wouden, C.H.; Bohringer, S.; Cecchin, E.; Cheung, K.C.; Davila-Fajardo, C.L.; Deneer, V.H.M.; Dolzan, V.; Ingelman-Sundberg, M.; Jonsson, S.; Karlsson, M.O.; et al. Generating evidence for precision medicine: Considerations made by the Ubiquitous Pharmacogenomics Consortium when designing and operationalizing the PREPARE study. Pharmacogenet. Genom. 2020, 30, 130. [Google Scholar] [CrossRef]
- Dunnenberger, H.M.; Crews, K.R.; Hoffman, J.M.; Caudle, K.E.; Broeckel, U.; Howard, S.C.; Hunkler, R.J.; Klein, T.E.; Evans, W.E.; Relling, M.V. Preemptive Clinical Pharmacogenetics Implementation: Current Programs in Five US Medical Centers. Annu. Rev. Pharmacol. Toxicol. 2015, 55, 89–106. [Google Scholar] [CrossRef] [Green Version]
- Chao, T.F.; Lip, G.Y.H.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; Tuan, T.C.; Liao, J.N.; Chung, F.P.; Chen, T.J.; et al. Incident Risk Factors and Major Bleeding in Patients with Atrial Fibrillation Treated with Oral Anticoagulants: A Comparison of Baseline, Follow-up and Delta HAS-BLED Scores with an Approach Focused on Modifiable Bleeding Risk Factors. Thromb. Haemost. 2018, 118, 768–777. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Wan, Y.; Heneghan, C.; Perera, R.; Roberts, N.; Hollowell, J.; Glasziou, P.; Bankhead, C.; Xu, Y. Anticoagulation control and prediction of adverse events in patients with atrial fibrillation: A systematic review. Circ. Cardiovasc. Qual. Outcomes 2008, 1, 84–91. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; de Boer, A.; Verhoef, T.I.; van der Meer, F.J.; Le Cessie, S.; Manolopoulos, V.G.; Maitland-van der Zee, A.H. Age-stratified outcome of a genotype-guided dosing algorithm for acenocoumarol and phenprocoumon. J. Thromb. Haemost. 2017, 15, 454–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, F.; Byrne, S.; O’Shea, S. Managing oral anticoagulation therapy: Improving clinical outcomes. A review. J. Clin. Pharm. Ther. 2008, 33, 581–590. [Google Scholar] [CrossRef]
- Just, K.S.; Dormann, H.; Schurig, M.; Böhme, M.; Fracowiak, J.; Steffens, M.; Scholl, C.; Seufferlein, T.; Gräff, I.; Schwab, M.; et al. Adverse Drug Reactions in the Emergency Department: Is There a Role for Pharmacogenomic Profiles at Risk?—Results from the ADRED Study. J. Clin. Med. 2020, 9, 1801. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.A.; Sangkuhl, K.; Gardner, E.E.; Stein, C.M.; Hulot, J.S.; Johnson, J.A.; Roden, D.M.; Klein, T.E.; Shuldiner, A.R. Clinical Pharmacogenetics Implementation Consortium guidelines for cytochrome P450-2C19 (CYP2C19) genotype and clopidogrel therapy. Clin. Pharmacol. Ther. 2011, 90, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Van Booven, D.; Marsh, S.; McLeod, H.; Carrillo, M.W.; Sangkuhl, K.; Klein, T.E.; Altman, R.B. Cytochrome P450 2C9-CYP2C9. Pharmacogenet. Genom. 2010, 20, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Annotation of DPWG Guideline for Phenprocoumon and CYP2C9. Available online: https://www.pharmgkb.org/guidelineAnnotation/PA166105004 (accessed on 20 September 2021).
- Schneider, K.L.; Kastenmüller, K.; Weckbecker, K.; Bleckwenn, M.; Böhme, M.; Stingl, J.C. Potential Drug-Drug Interactions in a Cohort of Elderly, Polymedicated Primary Care Patients on Antithrombotic Treatment. Drugs Aging 2018, 35, 559–568. [Google Scholar] [CrossRef] [Green Version]
- Lamberts, M.; Olesen, J.B.; Ruwald, M.H.; Hansen, C.M.; Karasoy, D.; Kristensen, S.L.; Køber, L.; Torp-Pedersen, C.; Gislason, G.H.; Hansen, M.L. Bleeding after initiation of multiple antithrombotic drugs, including triple therapy, in atrial fibrillation patients following myocardial infarction and coronary intervention: A nationwide cohort study. Circulation 2012, 126, 1185–1193. [Google Scholar] [CrossRef] [Green Version]
- Klomp, S.D.; Manson, M.L.; Guchelaar, H.J.; Swen, J.J. Phenoconversion of Cytochrome P450 Metabolism: A Systematic Review. J. Clin. Med. 2020, 9, 2890. [Google Scholar] [CrossRef]
- Shah, R.R.; Smith, R.L. Addressing phenoconversion: The Achilles’ heel of personalized medicine. Br. J. Clin. Pharmacol. 2015, 79, 222–240. [Google Scholar] [CrossRef] [Green Version]
- Coste, J.; Valderas, J.M.; Carcaillon-Bentata, L. Estimating and characterizing the burden of multimorbidity in the community: A comprehensive multistep analysis of two large nationwide representative surveys in France. PLoS Med. 2021, 18, e1003584. [Google Scholar] [CrossRef] [PubMed]
- Kouladjian O’Donnell, L.; Gnjidic, D.; Sawan, M.; Reeve, E.; Kelly, P.J.; Chen, T.F.; Bell, J.S.; Hilmer, S.N. Impact of the Goal-directed Medication Review Electronic Decision Support System on Drug Burden Index: A cluster-randomised clinical trial in primary care. Br. J. Clin. Pharmacol. 2020, 87, 1499–1511. [Google Scholar] [CrossRef] [PubMed]
- Godwin, M.; Ruhland, L.; Casson, I.; MacDonald, S.; Delva, D.; Birtwhistle, R.; Lam, M.; Seguin, R. Pragmatic controlled clinical trials in primary care: The struggle between external and internal validity. BMC Med. Res. Methodol. 2003, 3, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Andrea, G.; D’Ambrosio, R.L.; Di Perna, P.; Chetta, M.; Santacroce, R.; Brancaccio, V.; Grandone, E.; Margaglione, M. A polymorphism in the VKORC1 gene is associated with an interindividual variability in the dose-anticoagulant effect of warfarin. Blood 2005, 105, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.Y.; Chen, J.J.; Lee, M.T.; Wung, J.C.; Chen, Y.F.; Charng, M.J.; Lu, M.J.; Hung, C.R.; Wei, C.Y.; Chen, C.H.; et al. A novel functional VKORC1 promoter polymorphism is associated with inter-individual and inter-ethnic differences in warfarin sensitivity. Hum. Mol. Genet. 2005, 14, 1745–1751. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parameter | Missing, n (%) | Total Population, N = 340 | Individualized Risk Assessment Group, n = 167 | Standardized Risk Assessment Group, n = 173 | p-Value |
|---|---|---|---|---|---|
| Age (years), median (IQR) | - | 75 (71; 80) | 75 (70; 78) | 77 (72; 81) | 0.002 |
| Sex (female), n (%) | - | 138 (40.6) | 65 (38.9) | 73 (42.2) | 0.539 |
| Number of drugs, median (IQR) | - | 13 (8; 18) | 13 (8; 18) | 13 (8; 19) | 0.955 |
| HAS BLED (score), median (IQR) | - | 2 (1; 3) | 2 (1; 3) | 2 (1; 3) | 0.653 |
| CHA2DS2 VASc (score), median (IQR) | - | 4 (3; 5) | 4 (3; 5) | 4 (3; 5) | 0.432 |
| SF-36 score, median (IQR) | |||||
| Vitality | 4 (1.2) | 65 (50; 75) | 65 (50; 80) | 63 (45; 75) | 0.212 |
| Physical functioning | 4 (1.2) | 75 (55; 90) | 80 (60; 91) | 70 (50; 90) | 0.017 |
| Bodily pain | 4 (1.2) | 80 (52; 100) | 84 (52; 100) | 74 (52; 100) | 0.672 |
| General health perception | 5 (1.5) | 65 (50; 67) | 65 (52; 77) | 62 (49; 77) | 0.531 |
| Physical role functioning | 5 (1.5) | 100 (50; 100) | 100 (50; 100) | 100 (50; 100) | 0.320 |
| Emotional role functioning | 5 (1.5) | 100 (100; 100) | 100 (100; 100) | 100 (100; 100) | 0.679 |
| Social role functioning | 4 (1.2) | 100 (88; 100) | 100 (97; 100) | 100 (88; 100) | 0.670 |
| Mental health | 4 (1.2) | 84 (68; 92) | 84 (71; 92) | 84 (68; 92) | 0.532 |
| Time in study (days), median (IQR) | - | 277 (259; 300) | 279 (261; 302) | 273 (254; 294) | 0.062 |
| GFR (mL/min/1.73m2) | 4 (1.2) | 66.2 (51.7; 81.3) | 67.4 (52.6; 81.5) | 66.2 (51.3; 82.3) | 0.424 |
| Renal function, n (%) | - | 0.240 | |||
| GFR ≥ 90 | 32 (9.5) | 14 (8.5) | 18 (10.5) | ||
| GFR 60–<90 | 178 (53.0) | 91 (55.2) | 87 (50.9) | ||
| GFR 30–<60 | 119 (35.4) | 59 (35.8) | 60 (35.1) | ||
| GFR 15–<30 | 5 (1.5) | 0 (0) | 5 (2.9) | ||
| GFR < 15 | 2 (0.6) | 1 (0.6) | 1 (0.6) | ||
| Highest educational degree, n (%) | 19 (5.6) | 0.925 | |||
| Major school diploma | 180 (56.1) | 89 (56.3) | 91 (55.8) | ||
| Secondary school diploma | 60 (18.7) | 30 (19.0) | 30 (18.4) | ||
| Technical college diploma | 16 (5.0) | 8 (5.1) | 8 (4.9) | ||
| High school diploma | 21 (6.5) | 9 (5.7) | 12 (7.4) | ||
| College degree | 43 (13.4) | 22 (13.9) | 21 (12.9) | ||
| No diploma | 1 (0.3) | 0 (0) | 1 (0.6) | ||
| Number of antithrombotic drugs used, median (IQR) | - | 1 (1; 1) | 1 (1; 1) | 1 (1; 1) | 0.883 |
| Antithrombotic drug use, n (%) | |||||
| VKA | - | 209 (61.5) | 103 (61.7) | 106 (61.3) | 0.997 |
| DOAC | 101 (29.7) | 49 (29.3) | 52 (30.1) | 0.976 | |
| ASA | 22 (6.5) | 11 (6.6) | 11 (6.5) | 0.995 | |
| P2Y12-inhibitor | 53 (15.6) | 28 (16.8) | 25 (14.5) | 0.831 | |
| PPI use, n (%) | - | 168 (49.4) | 78 (46.7) | 90 (52.0) | 0.327 |
| Statin use, n (%) | - | 187 (55.0) | 92 (55.1) | 95 (54.9) | 0.974 |
| CYP2C19 phenotype, n (%) | - | 0.911 | |||
| NM | 241 (70.9) | 120 (71.9) | 121 (69.9) | ||
| IM | 87 (25.6) | 41 (24.6) | 46 (26.6) | ||
| PM | 12 (3.5) | 6 (3.6) | 6 (3.5) | ||
| CYP2C9 phenotype, n (%) | - | 0.488 | |||
| NM | 223 (65.6) | 108 (64.7) | 115 (66.5) | ||
| IM | 110 (32.4) | 54 (32.3) | 56 (32.4) | ||
| PM | 7 (2.1) | 5 (3.0) | 2 (1.2) | ||
| VKORC1 phenotype, n (%) | - | 0.724 | |||
| Normal | 295 (86.8) | 146 (87.4) | 149 (86.1) | ||
| Poor | 45 (13.2) | 21 (12.6) | 24 (13.9) |
| Endpoints | Total Population, N = 340 | Individualized Risk Assessment Group, n = 167 | Standardized Risk Assessment Group, n = 173 | OR [95% CI] | p-Value |
|---|---|---|---|---|---|
| Composite endpoint, n (%) | 195 (57.4) | 102 (61.1) | 93 (53.8) | 1.35 [0.88–2.08] | |
| Death, n (%) | 10 (2.9) | 4 (2.4) | 6 (3.5) | 0.68 [0.19–2.47] | |
| Patients with bleeding event, n (%) | 182 (53.5) | 91 (54.5) | 91 (52.6) | 1.08 [0.70–1.65] | |
| Number of bleeding events, mean (SD) | 0.68 (0.74) | 0.67 (0.72) | 0.68 (0.75) | 0.887 | |
| Skin or mucosal bleeding, n (%) | 160 (47.1) | 76 (45.5) | 84 (48.6) | 0.89 [0.58–1.36] | |
| Hematochezia | 15 (4.4) | 10 (6.0) | 5 (2.9) | 2.14 [0.72–6.40] | |
| Hematuria | 28 (8.2) | 12 (7.2) | 16 (9.2) | 0.76 [0.35–1.66] | |
| Muscle or intra-articular bleeding, n (%) | 6 (1.8) | 2 (1.2) | 4 (2.3) | 0.51 [0.09–2.83] | |
| Intra-cranial bleeding, n (%) | 1 (0.3) | 1 (0.6) | 0 (0) | - | 0.308 |
| Intra-ocular bleeding, n (%) | 8 (2.4) | 4 (2.4) | 4 (2.3) | 1.04 [0.26–4.22] | |
| Other bleeding, n (%) | 12 (3.5) | 7 (4.2) | 5 (2.9) | 1.47 [0.46–4.73] | |
| Patients with thromboembolic event, n (%) | 25 (7.4) | 16 (9.6) | 9 (5.2) | 1.93 [0.83–4.50] | |
| Number of thromboembolic events, mean (SD) | 0.08 (0.30) | 0.11 (0.37) | 0.05 (0.22) | 0.088 | |
| Superficial venous thrombosis, n (%) | 3 (0.9) | 2 (1.2) | 1 (0.6) | 2.09 [0.19–23.21] | |
| Deep venous thrombosis, n (%) | 2 (0.6) | 2 (1.2) | 0 (0) | - | 0.149 |
| Pulmonary embolism, n (%) | 1 (0.3) | 0 (0) | 1 (0.6) | - | 0.325 |
| Stroke/ TIA, n (%) | 4 (1.2) | 4 (2.4) | 0 (0) | - | 0.041 |
| Myocardial infarction, n (%) | 2 (0.6) | 1 (0.6) | 1 (0.6) | 1.04 [0.06–16.70] | |
| Other thromboembolic event, n (%) | 13 (3.8) | 7 (4.2) | 6 (3.5) |
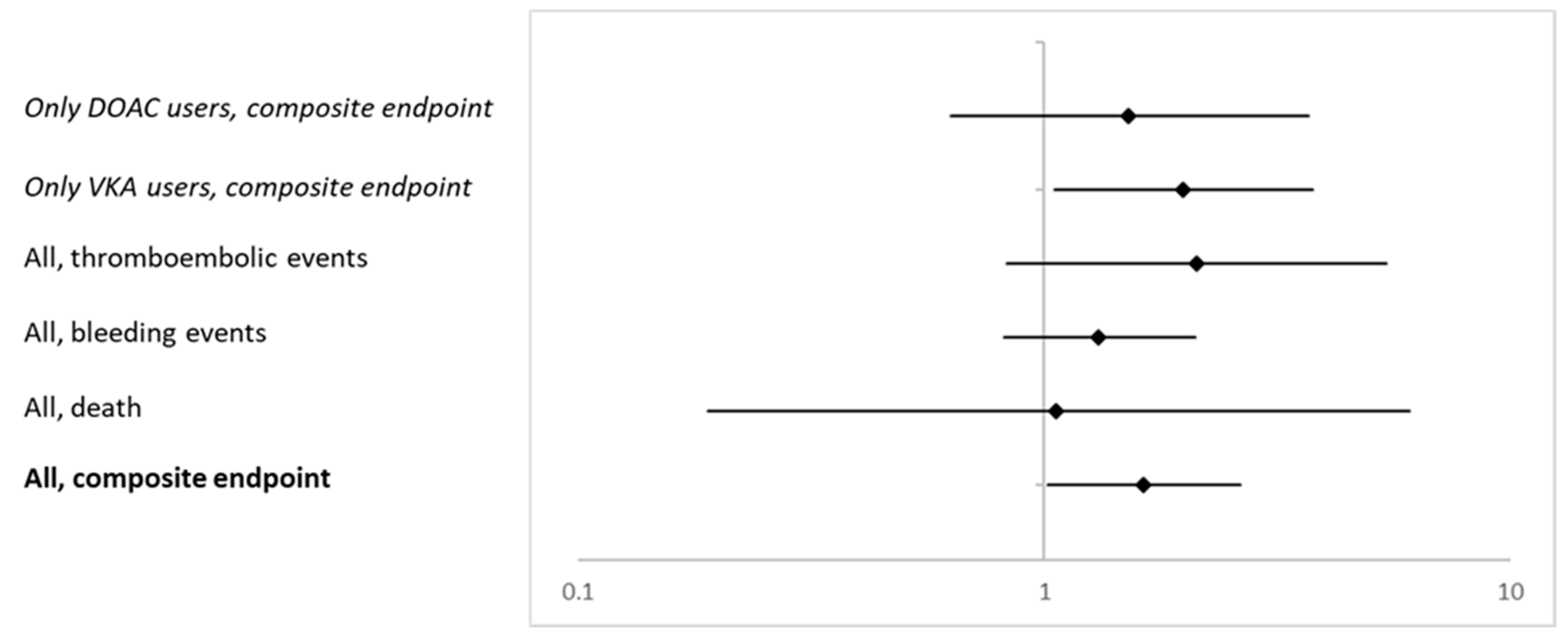
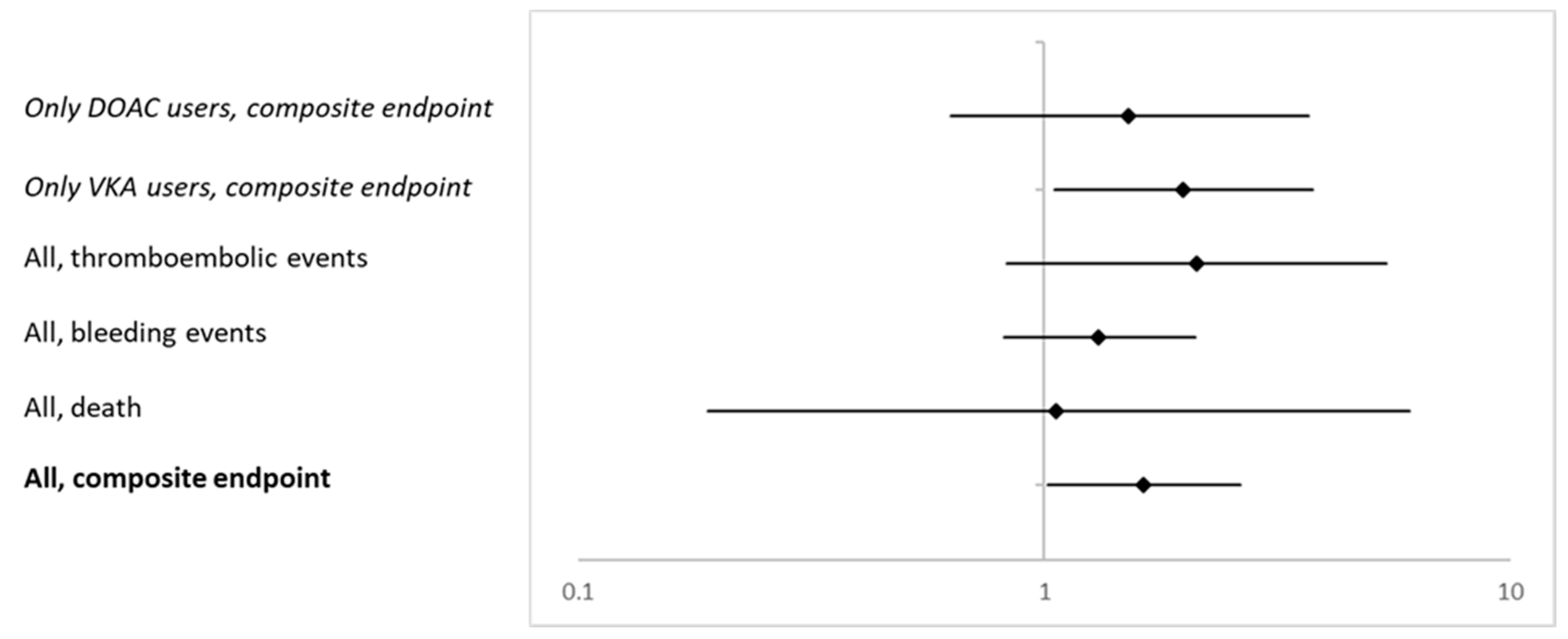
| Endpoints | OR [95% CI] Model 1 | OR [95% CI] Model 2 | OR [95% CI] Model 3 |
|---|---|---|---|
| Composite endpoint | 1.63 [1.03–2.60] | 1.61 [1.00–2.58] | 1.63 [1.02–2.63] |
| Death | 1.16 [0.22–6.08] | 1.12 [0.20–6.27] * | 1.06 [0.19–6.09] * |
| Bleeding event | 1.33 [0.84–2.10] | 1.30 [0.81–2.07] | 1.31 [0.82–2.11] |
| Thromboembolic event | 2.08 [0.84–5.11] | 2.20 [0.87–5.57] | 2.13 [0.83–5.44] |
| Parameters Included in Models | OR [95% CI] Model 1 | OR [95% CI] Model 2 | OR [95% CI] Model 3 |
|---|---|---|---|
| Individualized risk assessment | 1.88 [1.02–3.44] | 1.99 [1.06–3.74] | 1.99 [1.05–3.76] |
| Age (years) | 1.07 [1.02–1.12] | 1.05 [0.99–1.11] | 1.05 [0.99–1.11] |
| Sex (female) | 1.90 [1.03–3.53] | 2.02 [0.99–4.13] | 2.04 [0.98–4.26] |
| Educational degree | - | 1.07 [0.87–1.32] | 1.07 [0.86–1.32] |
| GFR (mL/min/1.73m2) | - | 0.99 [0.97–1.01] | 0.99 [0.97–1.01] |
| Antithrombotic drugs taken (number) | - | 1.20 [0.71–2.04] | 1.25 [0.73–2.14] |
| HAS BLED (score) | - | 0.97 [0.68–1.38] | 0.94 [0.65–1.35] |
| CHA2DS2 VASc (score) | - | 1.15 [0.87–1.52] | 1.15 [0.86–1.52] |
| Amount of patients enrolled in study center | - | 0.90 [0.75–1.07] | 0.89 [0.75–1.07] |
| Time in study (days) | - | 1.01 [1.00–1.01] | 1.01 [1.00–1.01] |
| CYP2C9 phenotype (IM/ PM) | - | - | 0.77 [0.39–1.52] |
| CYP2C19 phenotype (IM/ PM) | - | - | 0.80 [0.39–1.66] |
| VKORC1 phenotype (reduced) | - | - | 1.32 [0.51–3.41] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Just, K.S.; Scholl, C.; Boehme, M.; Kastenmüller, K.; Just, J.M.; Bleckwenn, M.; Holdenrieder, S.; Meier, F.; Weckbecker, K.; Stingl, J.C. Individualized versus Standardized Risk Assessment in Patients at High Risk for Adverse Drug Reactions (The IDrug Randomized Controlled Trial)–Never Change a Running System? Pharmaceuticals 2021, 14, 1056. https://doi.org/10.3390/ph14101056
Just KS, Scholl C, Boehme M, Kastenmüller K, Just JM, Bleckwenn M, Holdenrieder S, Meier F, Weckbecker K, Stingl JC. Individualized versus Standardized Risk Assessment in Patients at High Risk for Adverse Drug Reactions (The IDrug Randomized Controlled Trial)–Never Change a Running System? Pharmaceuticals. 2021; 14(10):1056. https://doi.org/10.3390/ph14101056
Chicago/Turabian StyleJust, Katja S., Catharina Scholl, Miriam Boehme, Kathrin Kastenmüller, Johannes M. Just, Markus Bleckwenn, Stefan Holdenrieder, Florian Meier, Klaus Weckbecker, and Julia C. Stingl. 2021. "Individualized versus Standardized Risk Assessment in Patients at High Risk for Adverse Drug Reactions (The IDrug Randomized Controlled Trial)–Never Change a Running System?" Pharmaceuticals 14, no. 10: 1056. https://doi.org/10.3390/ph14101056
APA StyleJust, K. S., Scholl, C., Boehme, M., Kastenmüller, K., Just, J. M., Bleckwenn, M., Holdenrieder, S., Meier, F., Weckbecker, K., & Stingl, J. C. (2021). Individualized versus Standardized Risk Assessment in Patients at High Risk for Adverse Drug Reactions (The IDrug Randomized Controlled Trial)–Never Change a Running System? Pharmaceuticals, 14(10), 1056. https://doi.org/10.3390/ph14101056