
Plasma Rich in Growth Factors in the Treatment of Endodontic Periapical Lesions in Adult Patients: A Narrative Review


Abstract
:1. Introduction
2. Molecular Background of the Endodontic Periapical Lesions
2.1. Pro-Inflammatory and Anti-Inflammatory Cytokines
2.2. The Role of MicroRNA (miRNA) in Bone Resorption and Pathogenesis of Apical Periodontitis
3. Endodontic Treatment of Periapical Lesions
4. Platelet Concentrates–General Characteristics, and Role in the Endodontic Treatment
5. Mesenchymal Stem Cells and Platelet Concentrates
6. PRF in the Endodontic Treatment of Permanent Teeth with Closed Apexes
7. Materials and Methods
7.1. Clinical Question
7.2. Inclusion and Exclusion Criteria for the Narrative Review
7.3. The PICO Approach
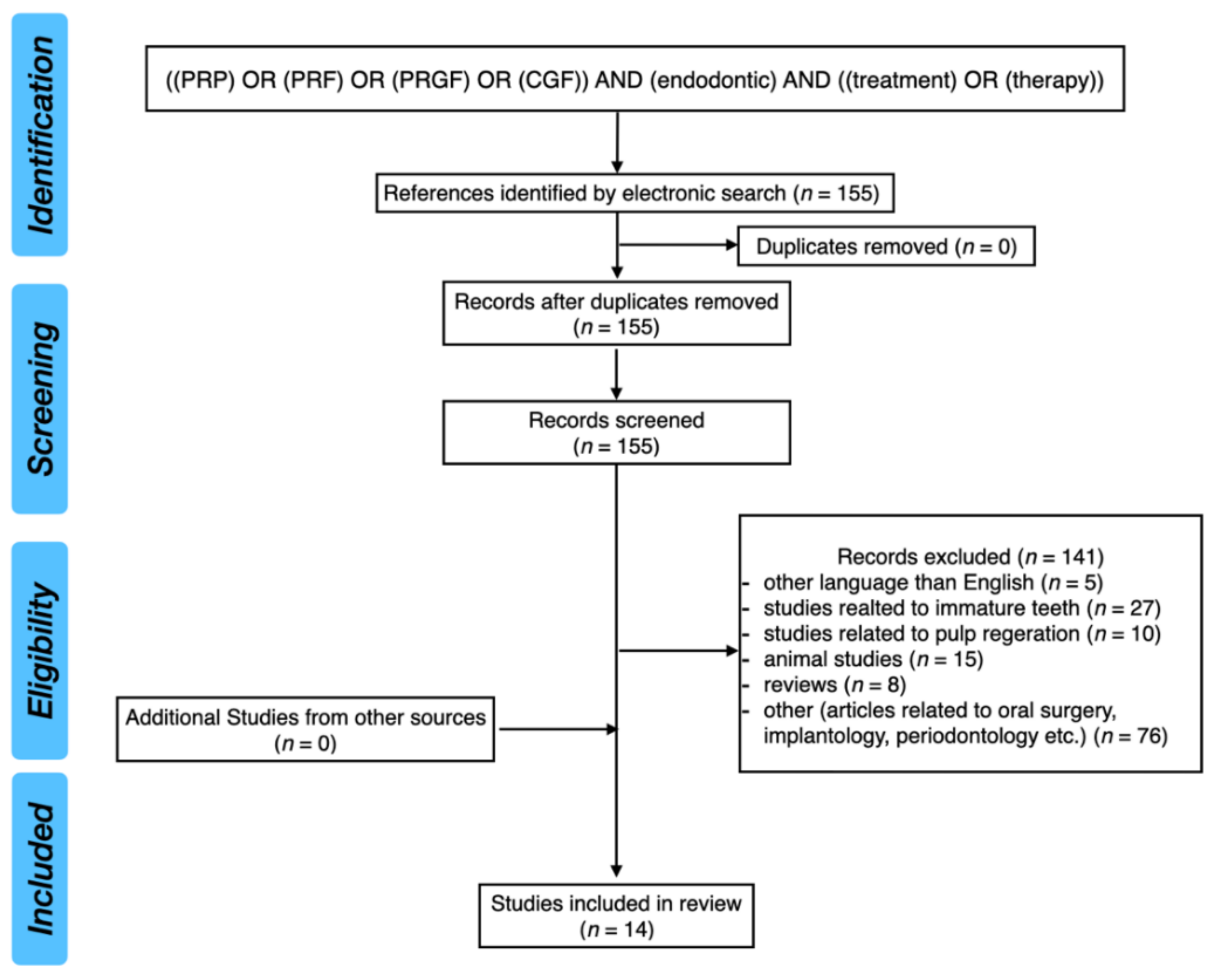
7.4. Search Strategy
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cho, M.I.; Garant, P.R. Development and general structure of the periodontium. Periodontology 2000 2000, 24, 9–27. [Google Scholar] [CrossRef] [PubMed]
- Abbott, P.V. The periapical space—A dynamic interface. Aust. Endod. J. 2002, 28, 96–107. [Google Scholar] [CrossRef]
- Nair, P.N. Apical periodontitis: A dynamic encounter between root canal infection and host response. Periodontology 2000 1997, 13, 121–148. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F., Jr.; Rôças, I.N.; Ricucci, D.; Hülsmann, M. Causes and management of post-treatment apical periodontitis. Br. Dent. J. 2014, 216, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Jiang, Y.; Chen, W.; Zhu, C.; Liang, J. Bacterial flora and extraradicular biofilm associated with the apical segment of teeth with post-treatment apical periodontitis. J. Endod. 2012, 38, 954–959. [Google Scholar] [CrossRef] [PubMed]
- Ricucci, D.; Candeiro, G.T.; Bugea, C.; Siqueira, J.F., Jr. Complex Apical Intraradicular Infection and Extraradicular Mineralized Biofilms as the Cause of Wet Canals and Treatment Failure: Report of 2 Cases. J. Endod. 2016, 42, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Nair, P.N. Pathogenesis of apical periodontitis and the causes of endodontic failures. Crit. Rev. Oral Biol. Med. 2004, 15, 348–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karamifar, K.; Tondari, A.; Saghiri, M.A. Endodontic Periapical Lesion: An Overview on the Etiology, Diagnosis and Current Treatment Modalities. Eur. Endod. J. 2020, 5, 54–67. [Google Scholar] [CrossRef] [PubMed]
- Cekici, A.; Kantarci, A.; Hasturk, H.; Van Dyke, T.E. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontology 2000 2014, 64, 57–80. [Google Scholar] [CrossRef] [Green Version]
- Noguchi, N.; Noiri, Y.; Narimatsu, M.; Ebisu, S. Identification and localization of extraradicular biofilm-forming bacteria associated with refractory endodontic pathogens. Appl. Environ. Microbiol. 2005, 71, 8738–8743. [Google Scholar] [CrossRef] [Green Version]
- Del Fabbro, M.; Corbella, S.; Sequeira-Byron, P.; Tsesis, I.; Rosen, E.; Lolato, A.; Taschieri, S. Endodontic procedures for retreatment of periapical lesions. Cochrane Database Syst Rev. 2016, 10, CD005511. [Google Scholar] [CrossRef]
- Alghamdi, F.; Alhaddad, A.J.; Abuzinadah, S. Healing of Periapical Lesions After Surgical Endodontic Retreatment: A Systematic Review. Cureus 2020, 12, e6916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uppada, U.K.; Kalakonda, B.; Koppolu, P.; Varma, N.; Palakurthy, K.; Manchikanti, V.; Prasad, S.; Samar, S.; Swapna, L.A. Combination of hydroxyapatite, platelet rich fibrin and amnion membrane as a novel therapeutic option in regenerative periapical endodontic surgery: Case series. Int. J. Surg. Case Rep. 2017, 37, 139–144. [Google Scholar] [CrossRef]
- Restrepo-Restrepo, F.A.; Cañas-Jiménez, S.J.; Romero-Albarracín, R.D.; Villa-Machado, P.A.; Pérez-Cano, M.I.; Tobón-Arroyave, S.I. Prognosis of root canal treatment in teeth with preoperative apical periodontitis: A study with cone-beam computed tomography and digital periapical radiography. Int. Endod. J. 2019, 52, 1533–1546. [Google Scholar] [CrossRef] [PubMed]
- Metin, R.; Tatli, U.; Evlice, B. Effects of low-level laser therapy on soft and hard tissue healing after endodontic surgery. Lasers Med. Sci. 2018, 33, 1699–1706. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.; Nawal, R.R.; Talwar, S.; Verma, M. Low-level laser therapy for management of large periapical lesions associated with open apex cases. Indian J. Dent. Res. 2020, 31, 334–336. [Google Scholar] [CrossRef]
- Kitchens, J.A.; Schwartz, S.A.; Schindler, W.G.; Hargreaves, K.M. Iontophoresis significantly increases the trans-dentinal delivery of osteoprotegerin, alendronate, and calcitonin. J. Endod. 2007, 33, 1208–1211. [Google Scholar] [CrossRef]
- Lietz-Kijak, D.; Kijak, E.; Śliwiński, Z.; Opalko, K. The use of physiotherapy in the regeneration of periapical bone structures of the teeth, prepared to load the prosthetic. Postepy. Hig. Med. Dosw. 2013, 67, 643–647. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Bortolinm, M.; Taschieri, S. Is autologous platelet concentrate beneficial for post-extraction socket healing? A systematic review. Int. J. Oral Maxillofac. Surg. 2011, 40, 891–900. [Google Scholar] [CrossRef]
- Panda, S.; Doraiswamy, J.; Malaiappan, S.; Varghese, S.S.; Del Fabbro, M. Additive effect of autologous platelet concentrates in treatment of intrabony defects: A systematic review and meta-analysis. J. Investig. Clin. Dent. 2016, 7, 13–26. [Google Scholar] [CrossRef]
- Gremmel, T.; Frelinger, A.L., 3rd; Michelson, A.D. Platelet Physiology. Semin. Thromb. Hemost. 2016, 42, 191–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, S.M.; Reed, G.L. Development of platelet secretory granules. Semin. Cell Dev. Biol. 2002, 13, 293–302. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part I: Technological concepts and evolution. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e37–e44. [Google Scholar] [CrossRef]
- Kao, R.T.; Murakami, S.; Beirne, O.R. The use of biologic mediators and tissue engineering in dentistry. Periodontology 2000 2009, 50, 127–153. [Google Scholar] [CrossRef] [PubMed]
- Choukroun, J.; Diss, A.; Simonpieri, A.; Girard, M.O.; Schoeffler, C.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Dohan, D.M. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part V: Histologic evaluations of PRF effects on bone allograft maturation in sinus lift. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, 299–303. [Google Scholar] [CrossRef]
- Handal, T.; Caugant, D.A.; Olsen, I.; Sunde, P.T. Bacterial diversity in persistent periapical lesions on root-filled teeth. J. Oral Microbiol. 2009, 1, 1946. [Google Scholar] [CrossRef]
- Eriksen, H.M.; Kirkevang, L.-L.; Petersson, K. Endodontic epidemiology and treatment outcome: General considerations. Endod. Top. 2002, 2, 1–9. [Google Scholar] [CrossRef]
- Colić, M.; Gazivoda, D.; Vucević, D.; Vasilijić, S.; Rudolf, R.; Lukić, A. Proinflammatory and immunoregulatory mechanisms in periapical lesions. Mol. Immunol. 2009, 47, 101–113. [Google Scholar] [CrossRef] [PubMed]
- Dessaune Neto, N.; Porpino, M.T.M.; Antunes, H.D.S.; Rodrigues, R.C.V.; Perez, A.R.; Pires, F.R.; Siqueira, J.F., Jr.; Armada, L. Pro-inflammatory and anti-inflammatory cytokine expression in post-treatment apical periodontitis. J. Appl. Oral Sci. 2018, 26, e20170455. [Google Scholar] [CrossRef] [Green Version]
- Gazivoda, D.; Dzopalic, T.; Bozic, B.; Tatomirovic, Z.; Brkic, Z.; Colic, M. Production of proinflammatory and immunoregulatory cytokines by inflammatory cells from periapical lesions in culture. J. Oral Pathol. Med. 2009, 38, 605–611. [Google Scholar] [CrossRef]
- Jakovljevic, A.; Knezevic, A.; Karalic, D.; Soldatovic, I.; Popovic, B.; Milasin, J.; Andric, M. Pro-inflammatory cytokine levels in human apical periodontitis: Correlation with clinical and histological findings. Aust. Endod. J. 2015, 41, 72–77. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho Fraga, C.A.; Alves, L.R.; de Sousa, A.A.; de Jesus, S.F.; Vilela, D.N.; Pereira, C.S.; Batista Domingos, P.L.; Viana, A.G.; Jham, B.C.; Batista de Paula, A.M.; et al. Th1 and Th2-like protein balance in human inflammatory radicular cysts and periapical granulomas. J. Endod. 2013, 39, 453–455. [Google Scholar] [CrossRef] [PubMed]
- Walker, K.F.; Lappin, D.F.; Takahashi, K.; Hope, J.; Macdonald, D.G.; Kinane, D.F. Cytokine expression in periapical granulation tissue as assessed by immunohistochemistry. Eur. J. Oral Sci. 2000, 108, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Yang, X.G.; Wang, F.; Ma, X.Y. IL-1α induces apoptosis and inhibits the osteoblast differentiation of MC3T3-E1 cells through the JNK and p38 MAPK pathways. Int. J. Mol. Med. 2016, 38, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, E.; Anan, H.; Matsumoto, N.; Hatakeyama, J.; Minakami, M.; Izumi, T. Immunopathology of Apical Periodontitis and Refractory Cases. J. Tissue Sci. Eng. 2016, 7, 184. [Google Scholar] [CrossRef] [Green Version]
- Garlet, G.P.; Aranha, A.M.F.; Silveira, E.M.; Vieira, A.E.; Queiroz-Junior, C.M.; Madeira, M.F.M.; Fukada, S.Y.; Silva, T.A. The Role of Chemokines and Cytokines in the Pathogenesis of Periodontal and Periapical Lesions: Current Concepts. In Inflammation, Chronic Diseases and Cancer—Cell and Molecular Biology, Immunology and Clinical Bases, 1st ed.; Khatami, M., Ed.; IntechOpen: London, UK, 2012; Volume 1, pp. 219–241. [Google Scholar] [CrossRef] [Green Version]
- Braz-Silva, P.H.; Bergamini, M.L.; Mardegan, A.P.; De Rosa, C.S.; Hasseus, B.; Jonasson, P. Inflammatory profile of chronic apical periodontitis: A literature review. Acta Odontol. Scand. 2019, 77, 173–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graunaite, I.; Lodiene, G.; Maciulskiene, V. Pathogenesis of apical periodontitis: A literature review. J. Oral Maxillofac. Res. 2012, 2, e1. [Google Scholar] [CrossRef] [PubMed]
- Cheng, R.; Wu, Z.; Li, M.; Shao, M.; Hu, T. Interleukin-1β is a potential therapeutic target for periodontitis: A narrative review. Int. J. Oral Sci. 2020, 12, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaneko, N.; Kurata, M.; Yamamoto, T.; Morikawa, S.; Masumoto, J. The role of interleukin-1 in general pathology. Inflamm. Regen. 2019, 39, 12. [Google Scholar] [CrossRef] [Green Version]
- Yamada, A.; Takami, M.; Kawawa, T.; Yasuhara, R.; Zhao, B.; Mochizuki, A.; Miyamoto, Y.; Eto, T.; Yasuda, H.; Nakamichi, Y.; et al. Interleukin-4 inhibition of osteoclast differentiation is stronger than that of interleukin-13 and they are equivalent for induction of osteoprotegerin production from osteoblasts. Immunology 2007, 120, 573–579. [Google Scholar] [CrossRef]
- AlShwaimi, E.; Berggreen, E.; Furusho, H.; Rossall, J.C.; Dobeck, J.; Yoganathan, S.; Stashenko, P.; Sasaki, H. IL-17 receptor A signaling is protective in infection-stimulated periapical bone destruction. J. Immunol. 2013, 191, 1785–1791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fettelschoss, A.; Kistowska, M.; LeibundGut-Landmann, S.; Beer, H.D.; Johansen, P.; Senti, G.; Contassot, E.; Bachmann, M.F.; French, L.E.; Oxenius, A.; et al. Inflammasome activation and IL-1β target IL-1α for secretion as opposed to surface expression. Proc. Natl. Acad. Sci. USA 2011, 108, 18055–18060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, S.M.; Nishioka, K.; Yudoh, K. Interleukin (IL) 18 stimulates osteoclast formation through synovial T cells in rheumatoid arthritis: Comparison with IL1 beta and tumour necrosis factor alpha. Ann. Rheum. Dis. 2004, 63, 1379–1386. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Chen, B.; Yan, F.; Guo, J.; Zhu, X.; Ma, S.; Yang, W. Interleukin-10 inhibits bone resorption: A potential therapeutic strategy in periodontitis and other bone loss diseases. Biomed Res. Int. 2014, 2014, 284836. [Google Scholar] [CrossRef] [PubMed]
- Bendre, M.S.; Montague, D.C.; Peery, T.; Akel, N.S.; Gaddy, D.; Suva, L.J. Interleukin-8 stimulation of osteoclastogenesis and bone resorption is a mechanism for the increased osteolysis of metastatic bone disease. Bone 2003, 33, 28–37. [Google Scholar] [CrossRef]
- Ruef, N.; Dolder, S.; Aeberli, D.; Seitz, M.; Balani, D.; Hofstetter, W. Granulocyte-macrophage colony-stimulating factor-dependent CD11c-positive cells differentiate into active osteoclasts. Bone 2017, 97, 267–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.S.; Kim, H.S.; Yeon, J.T.; Choi, S.W.; Chun, C.H.; Kwak, H.B.; Oh, J. GM-CSF regulates fusion of mononuclear osteoclasts into bone-resorbing osteoclasts by activating the Ras/ERK pathway. J. Immunol. 2009, 183, 3390–3399. [Google Scholar] [CrossRef] [Green Version]
- Zhao, B. TNF and Bone Remodeling. Curr. Osteoporos. Rep. 2017, 15, 126–134. [Google Scholar] [CrossRef]
- Scheffler, J.M.; Grahnemo, L.; Engdahl, C.; Drevinge, C.; Gustafsson, K.L.; Corciulo, C.; Lawenius, L.; Iwakura, Y.; Sjögren, K.; Lagerquist, M.K.; et al. Interleukin 17A: A Janus-faced regulator of osteoporosis. Sci. Rep. 2020, 10, 5692. [Google Scholar] [CrossRef]
- He, L.; Hannon, G.J. MicroRNAs: Small RNAs with a big role in gene regulation. Nat. Rev. Genet. 2004, 5, 522–531. [Google Scholar] [CrossRef]
- Kaeuferle, T.; Bartel, S.; Dehmel, S.; Krauss-Etschmann, S. MicroRNA methodology: Advances in miRNA technologies. Methods Mol. Biol. 2014, 1169, 121–130. [Google Scholar] [CrossRef]
- Sontheimer, E.J. Assembly and function of RNA silencing complexes. Nat. Rev. Mol. Cell Biol. 2005, 6, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Gu, S.; Jin, L.; Zhang, F.; Sarnow, P.; Kay, M.A. Biological basis for restriction of microRNA targets to the 3′ untranslated region in mammalian mRNAs. Nat. Struct. Mol. Biol. 2009, 16, 144–150. [Google Scholar] [CrossRef] [Green Version]
- Bracht, J.; Hunter, S.; Eachus, R.; Weeks, P.; Pasquinelli, A.E. Trans-splicing and polyadenylation of let-7 microRNA primary transcripts. RNA 2004, 10, 1586–1594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macfarlane, L.A.; Murphy, P.R. MicroRNA: Biogenesis, Function and Role in Cancer. Curr Genom. 2010, 11, 537–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, J.S.; Langlois, R.A.; Pham, A.M.; Tenoever, B.R. Evidence for a cytoplasmic microprocessor of pri-miRNAs. RNA 2012, 18, 1338–1346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bushati, N.; Cohen, S.M. microRNA functions. Annu. Rev. Cell Dev. Biol. 2007, 23, 175–205. [Google Scholar] [CrossRef]
- Baek, D.; Villén, J.; Shin, C.; Camargo, F.D.; Gygi, S.P.; Bartel, D.P. The impact of microRNAs on protein output. Nature 2008, 455, 64–71. [Google Scholar] [CrossRef] [Green Version]
- Dave, R.S.; Khalili, K. Morphine treatment of human monocyte-derived macrophages induces differential miRNA and protein expression: Impact on inflammation and oxidative stress in the central nervous system. J. Cell Biochem. 2010, 110, 834–845. [Google Scholar] [CrossRef] [Green Version]
- Chan, L.T.; Zhong, S.; Naqvi, A.R.; Self-Fordham, J.; Nares, S.; Bair, E.; Khan, A.A. MicroRNAs: New insights into the pathogenesis of endodontic periapical disease. J. Endod. 2013, 39, 1498–1503. [Google Scholar] [CrossRef] [Green Version]
- Gao, B.; Zheng, L. microRNA Expression in Rat Apical Periodontitis Bone Lesion. Bone Res. 2013, 1, 170–185. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, K.; Sørensen, M.G.; Nielsen, R.H.; Gram, J.; Schaller, S.; Dziegiel, M.H.; Everts, V.; Bollerslev, J.; Karsdal, M.A. Degradation of the organic phase of bone by osteoclasts: A secondary role for lysosomal acidification. J. Bone Miner. Res. 2006, 21, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.H.; Sui, B.D.; Du, F.Y.; Shuai, Y.; Zheng, C.X.; Zhao, P.; Yu, X.R.; Jin, Y. miR-21 deficiency inhibits osteoclast function and prevents bone loss in mice. Sci. Rep. 2017, 7, 43191. [Google Scholar] [CrossRef] [Green Version]
- Baćević, M.; Brković, B.; Lambert, F.; Djukić, L.; Petrović, N.; Roganović, J. Leukocyte- and platelet-rich fibrin as graft material improves microRNA-21 expression and decreases oxidative stress in the calvarial defects of diabetic rabbits. Arch. Oral Biol. 2019, 102, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Feng, Y.; Sun, H.; Zhang, L.; Hao, L.; Shi, C.; Wang, J.; Li, R.; Ran, X.; Su, Y.; et al. miR-21 regulates skin wound healing by targeting multiple aspects of the healing process. Am. J. Pathol. 2012, 181, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Chien, H.Y.; Lee, T.P.; Chen, C.Y.; Chiu, Y.H.; Lin, Y.C.; Lee, L.S.; Li, W.C. Circulating microRNA as a diagnostic marker in populations with type 2 diabetes mellitus and diabetic complications. J. Chin. Med. Assoc. 2015, 78, 204–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yue, J.; Song, D.; Lu, W.; Lu, Y.; Zhou, W.; Tan, X.; Zhang, L.; Huang, D. Expression Profiles of Inflammation-associated microRNAs in Periapical Lesions and Human Periodontal Ligament Fibroblasts Inflammation. J. Endod. 2016, 42, 1773–1778. [Google Scholar] [CrossRef]
- Wang, X.; Sun, H.; Liu, H.; Ma, L.; Jiang, C.; Liao, H.; Xu, S.; Xiang, J.; Cao, Z. MicroRNA-181b-5p modulates tumor necrosis factor-α-induced inflammatory responses by targeting interleukin-6 in cementoblasts. J. Cell. Physiol. 2019, 234, 22719–22730. [Google Scholar] [CrossRef]
- Shen, Z.; Silva, R.M. MicroRNAs: Emerging players in apical periodontitis. J. Appl. Oral Sci. 2021, 29, e20201058. [Google Scholar] [CrossRef]
- Lin, Y.; Xing, Q.; Qin, W.; de Melo, M.A.S.; Zou, R.; Xu, M.; Zhang, X.; Xu, H.H.K.; Lin, Z. Decreased Expression of Semaphorin3A/Neuropilin-1 Signaling Axis in Apical Periodontitis. Biomed Res. Int. 2017, 2017, 8724503. [Google Scholar] [CrossRef] [PubMed]
- Shen, Z.; Wichnieski, C.; Carneiro, E.; Garlet, G.P.; Letra, A.; Silva, R.M. Expression Profiling and Functional Characterization of MicroRNAs in Apical Periodontitis. J. Endod. 2021, 47, 263–271. [Google Scholar] [CrossRef]
- Mohammadi, Z.; Dummer, P.M. Properties and applications of calcium hydroxide in endodontics and dental traumatology. Int. Endod. J. 2011, 44, 697–730. [Google Scholar] [CrossRef] [PubMed]
- Sathorn, C.; Parashos, P.; Messer, H. Antibacterial efficacy of calcium hydroxide intracanal dressing: A systematic review and meta-analysis. Int. Endod. J. 2007, 40, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Peters, L.B.; Wesselink, P.R. Periapical healing of endodontically treated teeth in one and two visits obturated in the presence or absence of detectable microorganisms. Int. Endod. J. 2002, 35, 660–667. [Google Scholar] [CrossRef]
- Haapasalo, M.; Shen, Y.; Wang, Z.; Gao, Y. Irrigation in endodontics. Br. Dent. J. 2014, 216, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, R.C.; Antunes, H.S.; Neves, M.A.; Siqueira, J.F., Jr.; Rôças, I.N. Infection Control in Retreatment Cases: In Vivo Antibacterial Effects of 2 Instrumentation Systems. J. Endod. 2015, 41, 1600–1605. [Google Scholar] [CrossRef] [PubMed]
- Nagendrababu, V.; Jayaraman, J.; Suresh, A.; Kalyanasundaram, S.; Neelakantan, P. Effectiveness of ultrasonically activated irrigation on root canal disinfection: A systematic review of in vitro studies. Clin Oral Investig. 2018, 22, 655–670. [Google Scholar] [CrossRef]
- Siqueira, J.F., Jr.; Rôças, I.N.; Favieri, A.; Lima, K.C. Chemomechanical reduction of the bacterial population in the root canal after instrumentation and irrigation with 1%, 2.5%, and 5.25% sodium hypochlorite. J. Endod. 2000, 26, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Orstavik, D. Time-course and risk analyses of the development and healing of chronic apical periodontitis in man. Int. Endod. J. 1996, 29, 150–155. [Google Scholar] [CrossRef]
- Mokbel, N.; Kassir, A.R.; Naaman, N.; Megarbane, J.M. Root Resection and Hemisection Revisited. Part I: A Systematic Review. Int. J. Periodontics Restor. Dent. 2019, 39, e11–e31. [Google Scholar] [CrossRef] [PubMed]
- Jadun, S.; Monaghan, L.; Darcey, J. Endodontic microsurgery. Part two: Armamentarium and technique. Br. Dent. J. 2019, 227, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Von Arx, T. Apical surgery: A review of current techniques and outcome. Saudi Dent. J. 2011, 23, 9–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Floratos, S.; Kim, S. Modern Endodontic Microsurgery Concepts: A Clinical Update. Dent. Clin. N. Am. 2017, 61, 81–91. [Google Scholar] [CrossRef]
- Hawkins, T.K.; Wealleans, J.A.; Pratt, A.M.; Ray, J.J. Targeted endodontic microsurgery and endodontic microsurgery: A surgical simulation comparison. Int. Endod. J. 2020, 53, 715–722. [Google Scholar] [CrossRef]
- Pinto, D.; Marques, A.; Pereira, J.F.; Palma, P.J.; Santos, J.M. Long-Term Prognosis of Endodontic Microsurgery-A Systematic Review and Meta-Analysis. Medicina 2020, 56, 447. [Google Scholar] [CrossRef]
- Sebring, D.; Kvist, T.; Derks, J. Indications for Extraction before Implant Therapy: Focus on Endodontic Status. J. Endod. 2019, 45, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Palma, P.J.; Marques, J.A.; Casau, M.; Santos, A.; Caramelo, F.; Falacho, R.I.; Santos, J.M. Evaluation of Root-End Preparation with Two Different Endodontic Microsurgery Ultrasonic Tips. Biomedicines 2020, 8, 383. [Google Scholar] [CrossRef] [PubMed]
- Craddock, H.L.; Youngson, C.C.; Manogue, M.; Blance, A. Occlusal changes following posterior tooth loss in adults. Part 1: A study of clinical parameters associated with the extent and type of supraeruption in unopposed posterior teeth. J. Prosthodont. 2007, 16, 485–494. [Google Scholar] [CrossRef]
- Craddock, H.L.; Youngson, C.C.; Manogue, M.; Blance, A. Occlusal changes following posterior tooth loss in adults. Part 2. Clinical parameters associated with movement of teeth adjacent to the site of posterior tooth loss. J. Prosthodont. 2007, 16, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Craddock, H.L. Occlusal changes following posterior tooth loss in adults. Part 3. A study of clinical parameters associated with the presence of occlusal interferences following posterior tooth loss. J. Prosthodont. 2008, 17, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Thon, J.N.; Italiano, J.E. Platelet formation. Semin. Hematol. 2010, 47, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Cognasse, F.; Hamzeh, H.; Chavarin, P.; Acquart, S.; Genin, C.; Garraud, O. Evidence of Toll-like receptor molecules on human platelets. Immunol. Cell Biol. 2005, 83, 196–198. [Google Scholar] [CrossRef]
- Ross, R.; Glomset, J.; Kariya, B.; Harker, L. A platelet-dependent serum factor that stimulates the proliferation of arterial smooth muscle cells in vitro. Proc. Natl. Acad. Sci. USA 1974, 71, 1207–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dohan Ehrenfest, D.M.; Rasmusson, L.; Albrektsson, T. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends Biotechnol. 2009, 27, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Dohan Ehrenfest, D.M.; Del Corso, M.; Diss, A.; Mouhyi, J.; Charrier, J.B. Three-dimensional architecture and cell composition of a Choukroun’s platelet-rich fibrin clot and membrane. J. Periodontol. 2010, 81, 546–555. [Google Scholar] [CrossRef] [PubMed]
- Dohan Ehrenfest, D.M.; Andia, I.; Zumstein, M.A.; Zhang, C.Q.; Pinto, N.R.; Bielecki, T. Classification of platelet concentrates (Platelet-Rich Plasma-PRP, Platelet-Rich Fibrin-PRF) for topical and infiltrative use in orthopedic and sports medicine: Current consensus, clinical implications and perspectives. Muscles Ligaments Tendons J. 2014, 4, 3–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujioka-Kobayashi, M.; Miron, R.J.; Hernandez, M.; Kandalam, U.; Zhang, Y.; Choukroun, J. Optimized Platelet-Rich Fibrin With the Low-Speed Concept: Growth Factor Release, Biocompatibility, and Cellular Response. J. Periodontol. 2017, 88, 112–121. [Google Scholar] [CrossRef]
- Miron, R.J.; Xu, H.; Chai, J.; Wang, J.; Zheng, S.; Feng, M.; Zhang, X.; Wei, Y.; Chen, Y.; Mourão, C.F.A.B.; et al. Comparison of platelet-rich fibrin (PRF) produced using 3 commercially available centrifuges at both high (~700 g) and low (~200 g) relative centrifugation forces. Clin. Oral Investig. 2020, 24, 1171–1182. [Google Scholar] [CrossRef]
- Ghanaati, S.; Booms, P.; Orlowska, A.; Kubesch, A.; Lorenz, J.; Rutkowski, J.; Landes, C.; Sader, R.; Kirkpatrick, C.; Choukroun, J. Advanced platelet-rich fibrin: A new concept for cell-based tissue engineering by means of inflammatory cells. J. Oral Implantol. 2014, 40, 679–689. [Google Scholar] [CrossRef]
- Kobayashi, E.; Flückiger, L.; Fujioka-Kobayashi, M.; Sawada, K.; Sculean, A.; Schaller, B.; Miron, R.J. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin. Oral Investig. 2016, 20, 2353–2360. [Google Scholar] [CrossRef]
- Canellas, J.V.D.S.; Medeiros, P.J.D.; Figueredo, C.M.D.S.; Fischer, R.G.; Ritto, F.G. Platelet-rich fibrin in oral surgical procedures: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2019, 48, 395–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Zhang, Y.; Choukroun, J.; Ghanaati, S.; Miron, R.J. Effects of an injectable platelet-rich fibrin on osteoblast behavior and bone tissue formation in comparison to platelet-rich plasma. Platelets 2018, 29, 48–55. [Google Scholar] [CrossRef]
- Hu, K.; Olsen, B.R. The roles of vascular endothelial growth factor in bone repair and regeneration. Bone 2016, 91, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Moojen, D.J.; Everts, P.A.; Schure, R.M.; Overdevest, E.P.; van Zundert, A.; Knape, J.T.; Castelein, R.M.; Creemers, L.B.; Dhert, W.J. Antimicrobial activity of platelet-leukocyte gel against Staphylococcus aureus. J. Orthop. Res. 2008, 26, 404–410. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part III: Leucocyte activation: A new feature for platelet concentrates? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e51–e55. [Google Scholar] [CrossRef]
- Kour, P.; Pudakalkatti, P.S.; Vas, A.M.; Das, S.; Padmanabhan, S. Comparative Evaluation of Antimicrobial Efficacy of Platelet-rich Plasma, Platelet-rich Fibrin, and Injectable Platelet-rich Fibrin on the Standard Strains of Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans. Contemp. Clin. Dent. 2018, 9 (Suppl. S2), S325–S330. [Google Scholar] [CrossRef]
- Everts, P.; Onishi, K.; Jayaram, P.; Lana, J.F.; Mautner, K. Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. Int. J. Mol. Sci. 2020, 21, 7794. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Gou, L.; Zhang, P.; Li, H.; Qiu, S. Platelet-rich plasma and regenerative dentistry. Aust. Dent. J. 2020, 65, 131–142. [Google Scholar] [CrossRef]
- Borie, E.; Oliví, D.G.; Orsi, I.A.; Garlet, K.; Weber, B.; Beltrán, V.; Fuentes, R. Platelet-rich fibrin application in dentistry: A literature review. Int. J. Clin. Exp. Med. 2015, 8, 7922–7929. [Google Scholar]
- Miron, R.J.; Zucchelli, G.; Pikos, M.A.; Salama, M.; Lee, S.; Guillemette, V.; Fujioka-Kobayashi, M.; Bishara, M.; Zhang, Y.; Wang, H.L.; et al. Use of platelet-rich fibrin in regenerative dentistry: A systematic review. Clin. Oral Investig. 2017, 21, 1913–1927. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Sun, X.; Yu, J.; Wang, J.; Zhai, P.; Chen, S.; Liu, M.; Zhou, Y. Platelet-Rich Fibrin as a Bone Graft Material in Oral and Maxillofacial Bone Regeneration: Classification and Summary for Better Application. Biomed Res. Int. 2019, 2019, 3295756. [Google Scholar] [CrossRef]
- Fan, Y.; Perez, K.; Dym, H. Clinical Uses of Platelet-Rich Fibrin in Oral and Maxillofacial Surgery. Dent. Clin. N. Am. 2020, 64, 291–303. [Google Scholar] [CrossRef] [PubMed]
- Metlerska, J.; Fagogeni, I.; Nowicka, A. Efficacy of Autologous Platelet Concentrates in Regenerative Endodontic Treatment: A Systematic Review of Human Studies. J. Endod. 2019, 45, 20–30.e1. [Google Scholar] [CrossRef]
- Kim, S.G.; Malek, M.; Sigurdsson, A.; Lin, L.M.; Kahler, B. Regenerative endodontics: A comprehensive review. Int. Endod. J. 2018, 51, 1367–1388. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Guan, J.; Zhang, C. Mesenchymal stem cells: Mechanisms and role in bone regeneration. Postgrad. Med. J. 2014, 90, 643–647. [Google Scholar] [CrossRef]
- Yagi, H.; Soto-Gutierrez, A.; Parekkadan, B.; Kitagawa, Y.; Tompkins, R.G.; Kobayashi, N.; Yarmush, M.L. Mesenchymal stem cells: Mechanisms of immunomodulation and homing. Cell Transplant. 2010, 19, 667–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maria, O.M.; Khosravi, R.; Mezey, E.; Tran, S.D. Cells from bone marrow that evolve into oral tissues and their clinical applications. Oral Dis. 2007, 13, 11–16. [Google Scholar] [CrossRef]
- Tian, S.; Wang, J.; Dong, F.; Du, N.; Li, W.; Song, P.; Liu, Y. Concentrated Growth Factor Promotes Dental Pulp Cells Proliferation and Mineralization and Facilitates Recovery of Dental Pulp Tissue. Med. Sci. Monit. 2019, 25, 10016–10028. [Google Scholar] [CrossRef]
- Hu, L.; Zhao, B.; Gao, Z.; Xu, J.; Fan, Z.; Zhang, C.; Wang, J.; Wang, S. Regeneration characteristics of different dental derived stem cell sheets. J. Oral Rehabil. 2020, 47 (Suppl. S1), 66–72. [Google Scholar] [CrossRef]
- Salamanna, F.; Del Piccolo, N.; Sartori, M.; Giavaresi, G.; Martini, L.; Di Sante, G.; Stagni, C.; Dallari, D.; Fini, M. Effects of Autologous Bone Marrow Mesenchymal Stem Cells and Platelet-Rich Plasma on Bone Regeneration and Osseointegration of a Hydroxyapatite-Coated Titanium Implant. Coatings 2021, 11, 840. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Doglioli, P.; de Peppo, G.M.; Del Corso, M.; Charrier, J.B. Choukroun’s platelet-rich fibrin (PRF) stimulates in vitro proliferation and differentiation of human oral bone mesenchymal stem cell in a dose-dependent way. Arch. Oral Biol. 2010, 55, 185–194. [Google Scholar] [CrossRef]
- Sequeira, D.B.; Oliveira, A.R.; Seabra, C.M.; Palma, P.J.; Ramos, C.; Figueiredo, M.H.; Santos, A.C.; Cardoso, A.L.; Peça, J.; Santos, J.M. Regeneration of pulp-dentin complex using human stem cells of the apical papilla: In vivo interaction with two bioactive materials. Clin. Oral Investig. 2021, 25, 5317–5329. [Google Scholar] [CrossRef]
- Xu, F.; Qiao, L.; Zhao, Y.; Chen, W.; Hong, S.; Pan, J.; Jiang, B. The potential application of concentrated growth factor in pulp regeneration: An in vitro and in vivo study. Stem Cell Res. Ther. 2019, 10, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rochira, A.; Siculella, L.; Damiano, F.; Palermo, A.; Ferrante, F.; Carluccio, M.A.; Calabriso, N.; Giannotti, L.; Stanca, E. Concentrated Growth Factors (CGF) Induce Osteogenic Differentiation in Human Bone Marrow Stem Cells. Biology 2020, 9, 370. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Li, X.; Zhao, J.; Jia, W.; Wang, Z. Effect of autogenous growth factors released from platelet concentrates on the osteogenic differentiation of periodontal ligament fibroblasts: A comparative study. PeerJ 2019, 7, e7984. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Liu, L.; Wang, L.; Song, D. The effects and potential applications of concentrated growth factor in dentin-pulp complex regeneration. Stem Cell Res. Ther. 2021, 12, 357. [Google Scholar] [CrossRef] [PubMed]
- Machut, K.; Zoltowska, A.; Pawlowska, E.; Derwich, M. Plasma Rich in Growth Factors in the Treatment of Endodontic Periapical Lesions in Adult Patients: Case Reports. Int. J. Mol. Sci. 2021, 22, 9458. [Google Scholar] [CrossRef] [PubMed]
- Soto-Peñaloza, D.; Peñarrocha-Diago, M.; Cervera-Ballester, J.; Peñarrocha-Diago, M.; Tarazona-Alvarez, B.; Peñarrocha-Oltra, D. Pain and quality of life after endodontic surgery with or without advanced platelet-rich fibrin membrane application: A randomized clinical trial. Clin. Oral Investig. 2020, 24, 1727–1738. [Google Scholar] [CrossRef]
- Kavitha, M.; Krishnaveni, R.; Swathi, A.M.; Abubacker, M.H.M. Evaluation of healing by Cone Beam Computed Tomography (CBCT) using Platelet-Rich Plasma (PRP) + β -Tricalcium Phosphate (β -TCP) and Platelet Rich Fibrin (PRF) + β -Tricalcium Phosphate (β-TCP) in periapical lesions: Case report. Niger J. Clin. Pract. 2020, 23, 1026–1029. [Google Scholar] [CrossRef] [PubMed]
- Sureshbabu, N.M.; Ranganath, A.; Jacob, B. Concentrated Growth Factor—Surgical Management of Large Periapical Lesion Using a Novel Platelet Concentrate in Combination with Bone Graft. Ann. Maxillofac. Surg. 2020, 10, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Taschieri, S.; Rosano, G.; Weinstein, T.; Bortolin, M.; Del Fabbro, M. Treatment of through-and-through bone lesion using autologous growth factors and xenogeneic bone graft: A case report. Oral Maxillofac. Surg. 2012, 16, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Shivashankar, V.Y.; Johns, D.A.; Vidyanath, S.; Sam, G. Combination of platelet rich fibrin, hydroxyapatite and PRF membrane in the management of large inflammatory periapical lesion. J. Conserv. Dent. 2013, 16, 261–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, J.H.; Tsai, C.H.; Chang, Y.C. Management of radicular cysts using platelet-rich fibrin and bioactive glass: A report of two cases. J. Formos. Med. Assoc. 2014, 113, 470–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dudeja, P.G.; Dudeja, K.K.; Garg, A.; Srivastava, D.; Grover, S. Management of a Previously Treated, Calcified, and Dilacerated Maxillary Lateral Incisor: A Combined Nonsurgical/Surgical Approach Assisted by Cone-beam Computed Tomography. J. Endod. 2016, 42, 984–988. [Google Scholar] [CrossRef]
- Wadhwa, J.; Gupta, A.; Hans, S. Evaluation of Periapical Healing of Apicomarginal Defect in Mandibular First Molar Treated with Platelet Rich Fibrin: A Case Report. J. Clin. Diagn. Res. 2017, 11, ZD01–ZD03. [Google Scholar] [CrossRef]
- Vidhale, G.; Jain, D.; Jain, S.; Godhane, A.V.; Pawar, G.R. Management of Radicular Cyst Using Platelet-Rich Fibrin & Iliac Bone Graft—A Case Report. J. Clin. Diagn. Res. 2015, 9, ZD34–ZD36. [Google Scholar] [CrossRef] [PubMed]
- Bains, R.; Bains, V.K.; Loomba, K.; Verma, K.; Nasir, A. Management of pulpal floor perforation and grade II Furcation involvement using mineral trioxide aggregate and platelet rich fibrin: A clinical report. Contemp. Clin. Dent. 2012, 3 (Suppl. S2), S223–S227. [Google Scholar] [CrossRef] [PubMed]
- Demiralp, B.; Ke√ßeli, H.G.; Muhtarońüullar, M.; Serper, A.; Demiralp, B.; Eratalay, K. Treatment of periapical inflammatory lesion with the combination of platelet-rich plasma and tricalcium phosphate: A case report. J. Endod. 2004, 30, 796–800. [Google Scholar] [CrossRef] [PubMed]
- Hiremath, H.; Motiwala, T.; Jain, P.; Kulkarni, S. Use of second-generation platelet concentrate (platelet-rich fibrin) and hydroxyapatite in the management of large periapical inflammatory lesion: A computed tomography scan analysis. Indian J. Dent. Res. 2014, 25, 517–520. [Google Scholar] [CrossRef] [PubMed]
- Parikh, B.; Navin, S.; Vaishali, P. A comparative evaluation of healing with a computed tomography scan of bilateral periapical lesions treated with and without the use of platelet-rich plasma. Indian J. Dent. Res. 2011, 22, 497–498. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Cytokine (Abbreviation) | Cytokine Receptors | Cytokine-Secreting Cells | Target Cells | Functions | Bone Effect |
|---|---|---|---|---|---|
| Interleukin-1 alpha (IL-1α) | Interleukin-1 receptor (IL-1R): type I (IL1R1) and type II (ILL1R2) | monocytes, macrophages, polymorphonuclear leucocytes (PMNs), fibroblasts, osteoclasts, epithelial cells, endothelial cells, B cells | T-cells, B-cells, neutrophils, osteoblasts, tissue cells | Induces the inflammation and regulates immune system by chemotactically activation of PMN. Stimulates the production of PG, proteolytic enzymes and proinflammatory cytokines IL-6, IL-8. | Bone destruction: stimulates bone resorption and inhibits bone formation. Inhibits osteoblasts differentiation and probably induces apoptosis of osteoblasts. |
| Interleukin-1 beta (IL-1β) | Interleukin-1 receptor (IL-1R): type I (IL1R1) and type II (ILL1R2) | macrophages, dendritic cells, osteoblasts, fibroblasts (i.e., gingival fibroblasts, periodontal ligament cells), osteoblasts, epithelial and endothelial cells | T-cells, fibroblasts, epithelial cells, endothelial cells | Induces the inflammation: accelerates blood flow in inflamed tissue, supports leucocyte recruitment and neutrophil diffusion and accumulation. | Bone destruction: promotes bone resorption by stimulating production of MMPs, (mainly MMP-9), RANKL, IL-6. |
| Interleukin-18 (IL-18) | Interleukin-18 receptor (IL-18R, CD218a) | macrophages, dendritic cells, monocytes, keratinocytes, CNS cells, osteoblasts, endothelial cells | T-cells (CD4 and CD8), NK-cells, basophils, mast cells | Induces the production of IFNγ by T-cells and NK-cells. Induces Th cell-mediated immunity. Promotes proliferation of Th1. | Bone destruction: promotes osteoclastogenesis by regulation of RANKL production. |
| Interleukin-6 (IL-6) | Interleukin-6 receptor (IL-6R, CD126) | monocytes, polymorphonuclear leucocytes (PMNs), osteoclasts, macrophages, T-cells (Th2), B-cells, fibroblasts, endothelial cells | T-cells, B-cells, neutrophils, osteoblasts, tissue cells | Acute phase of inflammation: activates PMNs and T-cells. Stimulates B-lymphocytes differentiation into plasma cell. Induces protein synthesis. Suppresses the production of IL-1. | Bone destruction: induces bone resorption by promoting osteoclast differentiation. |
| Interleukin-8 (IL-8) | Interleukin-8 receptor A (IL-8RA, CXCR1) and interleukin-8 receptor B (IL-8RB, CXCR2) | monocytes, macrophages, PMNs, bone marrow stromal cells, osteoblasts, osteoclasts, synovial fibroblasts, chondrocytes | neutrophils, basophils | Chemotactic factor: attracts and activates PMNs and osteoclasts. | Bone destruction (potentially): stimulates osteoclastogenesis by osteoclasts differentiation and production, by stimulating RANKL expression and directly by stimulation of osteoclasts pro-duction and activation. |
| Interleukin-10 (IL-10) | Interleukin-10 receptor: (IL-10R) type I (IL-10R1) and type II (IL-10R2) | T-cells, monocytes, dendritic cells, B-cells, mast-cells, eosinophils | Th1, macrophages, NK-cells | Inhibits the production of cytokines by Th1: IL-1, IL-6 and IFNγ. Inhibits synthesis of NO and proteases (such as collagenases). Stimulates the secretion of tissue inhibitors of metalloproteinases and osteoprotegerin. | Inhibits bone resorption, suppresses the osteoclastogenesis and activates proliferation of osteoblasts. |
| Interleukin-17 | Interleukin-17 receptor (IL-17R) | Th17, Tregs | T-cells, B-cells, osteoblasts, tissue cells | Induces the inflammation. Activates secretion of IL-1, IL-6, TNFα, GCP-2 and IL-8. Induces migration of neutrophils. | Bone destruction: stimulates bone resorption, stimulates the production of RANKL by osteoblast and mesenchymal stem cells, disturbs balance of RANKL/OPG, which promotes osteoclastogenesis. |
| Tumor Necrosis Factor α (TNFα) | Tumor necrosis factor receptor 1 (TNFR1, CD120a); Tumor necrosis factor receptor 2 (TNFR2, CD120b) | macrophages, monocytes, lymphocytes (Th1), mast cells | macrophages, granulocytes, endothelial cells | Induces the inflammation by activating lymphocytes and monocytes. | Bone destruction: stimulates bone resorption, supports osteoclastogenesis with RANKL, promotes differentiation of osteoclasts and suppresses formation of osteoblasts. |
| Interferon gamma (IFNγ) | Interferon gamma receptor 1 (IFNGR1, CD119) and Interferon gamma receptor 2 (IFNGR2) | T-cells (CD4+, CD8+), Treg cells, B-cells, NK cells | monocytes, lymphocytes, tissue cells, mesenchymal stem cells (MSCs) | Activation of macrophages and differentiation of B-cells. Induces production of IL-1, NO and oxygen. | Inhibits bone resorption: inhibits production and differentiation of osteoclasts, activates apoptosis of osteoclasts. Indirectly down-regulates RANKL-depended osteoclastogenesis. Promotes differentiation of osteoblast from MSCs. |
| Interleukin-4 (IL-4) | Interleukin-4 receptor (IL-4, CD124) | Th2 | Th17 | Suppresses Th17 formation and production of IL-1. Stimulates the secretion of tissue inhibitors of metalloproteinases and osteoprotegerin. | Inhibits bone resorption, inhibits the osteoclast differentiation. It may promote osteoprotegerin pro-duction. |
| Granulocyte-Macrophage Colony Stimulating Factor (GM-CSF aka CSF2) | GM-CSF receptor (GM-CSFR) | macrophages, mast cells, T-cells, fibroblasts, NK cells, endothelial cells | bone marrow stem cells, macrophages, neutrophils | Takes part in hematopoiesis. Induces production of granulocytes (neutrophils, basophils, eosinophils) and monocytes from bone marrow stem cells. Activates macrophages. Enhances neutrophils migration. | Inhibits formation of osteoclasts from progenitor cells, reduces the RANKL/RANK activity. The increased level of dendritic cells makes GM-CSF activate osteoclastogenesis. |
| MicroRNA (miRNA) | Gene | Effect |
|---|---|---|
| miRNA-155 | 21q21.3 | Inhibition of SEMA3A. Decreased expression of SEMA3A contributes to bone resorption. |
| miRNA-335-5p | 7q32.2 | In inflamed HPDLFs promotes bone resorption (RANKL). |
| miRNA-181b-5p | 1q32.1 | Positive regulation of: acute inflammation (activation of NK-cells, monocytes, T-cells), angiogenesis, macrophages differentiation. Cementoblasts apoptosis. |
| miRNA-146a | 5q33.3 | Anti-inflammatory activity. Negative regulation of IL-6, IL-1β and TNF-α. |
| miRNA-10a-5p | 17q21.32 | Reduction of inflammation. Healing of apical periodontitis. |
| Reference | Study Design | Participants and Intervention | Endpoint and Results |
|---|---|---|---|
| Machut et al. (2021) [128] | Case report | Case no 1: Patient: 45-year-old female Tooth/teeth: 23 Diagnosis: pulp necrosis with symptomatic apical periodontitis of tooth 23 Type of treatment: RCT with A-PRF membrane placed by the apical foramen to the periapical area Protocol to obtain A-PRF:
Patient: 42-year-old male Tooth/teeth: 23 Diagnosis: pulp necrosis with asymptomatic apical periodontitis of tooth 23 Type of treatment: RCT with A-PRF membrane placed by the apical foramen to the periapical area Protocol to obtain PRF:
| Endpoint: 6 months Additional application of A-PRF led to a significant decrease in the periapical lesions’ size. |
| Soto-Peñaloza et al. (2020) [129] | Randomized clinical trial | Patient: 50 patients who needed endodontic surgery of upper maxillary teeth; age range: 44.2–52.4 years old Tooth/teeth: upper maxillary teeth (second premolar to second premolar) Diagnosis: chronic apical periodontitis Type of treatment: RCT + endodontic surgery (resection) Retrograde filling material: MTA Bony defect filler: control group: n/a; study group: A-PRF+ membranes (approximately: 2 + additional 1 over the osteotomy) Protocol to obtain PRF:
| Endpoint: 7 days No significant differences between the groups regarding postoperative pain. Only sleep and speech functions presented more limitations in control group. |
| Kavitha et al. (2020) [130] | Case report | Case no 1: Patient: 23-year-old female Tooth/teeth: 11,12 Diagnosis: chronic periapical abscess in relation to nonvital teeth: 11, 12 Type of treatment: RCT + endodontic surgery (resection) Retrograde filling material: Glass Ionomer Cement (GC Fuji IX) Bony defect filler: PRP + small amount of bovine thrombin + a few drops of 10% calcium chloride + β-TCP Protocol to obtain PRP:
Case no 2: Patient: 23-year-old female Tooth/teeth: 22 Diagnosis: periapical abscess in relation to nonvital 22 Type of treatment: RCT + endodontic surgery (resection) Retrograde filling material: Glass Ionomer Cement (GC Fuji IX) Bony defect filler: PRF + β-TCP Protocol to obtain PRF:
| Endpoint: 1 year Both PRP and PRF mixed with β-TCP were effective in the treatment of periapical defects. |
| Sureshbabu et al. (2020) [131] | Case report | Patient: 26-year-old male Tooth/teeth: 43,44,45 Diagnosis: pulpal necrosis with a chronic apical abscess in 43, 44, 45 Type of treatment: RCT + endodontic surgery (resection) Retrograde filling material: MTA Bony defect filler: CGF + osseograft + CGF membrane Protocol to obtain CGF:
| Endpoint: 1 year and 2 years After 1 year, lesion reduction size was found to be 79%. |
| Taschieri et al. (2012) [132] | Case report | Patient: 28-year-old male Tooth/teeth: 21,22 Diagnosis: periradicular lesion of endodontic origin, vestibular sinus tract and an abscess on the palatal side, nonvital tooth 22, tooth 21 after RCT with large endodontic post Type of treatment: RCT + endodontic surgery (resection) Retrograde filling material: n/a Bony defect filler: PRGF + 50 μL of 10% CaCl2 were added per cubic centimeter of PRGF concentrate + Bio-Oss mixed with PRGF + BioGide membrane Protocol to obtain PRGF:
| Endpoint: 1 year After 1 year the authors noticed complete healing and functionality. |
| Shivashankar et al. (2013) [133] | Case report | Patient: 45-year-old male Tooth/teeth: 12,11 Diagnosis: exacerbated chronic periodontitis in relation to nonvital teeth: 11, 12 Type of treatment: RCT + endodontic surgery (resection) Retrograde filling material: MTA Bony defect filler: PRF + HA bone graft crystals + PRF membrane Protocol to obtain PRF:
| Endpoint: 2 years The authors noticed complete bone healing after 2 years. |
| Zhao et al. (2014) [134] | Case report | Case no 1: Patient: 28-year-old female Tooth/teeth: 13,12,21,22 Diagnosis: exacerbated chronic periodontitis in relation to nonvital teeth: 13,12, 21,22; incomplete root canal fillings of teeth no: 12,21,22 Type of treatment: RCT + endodontic surgery (resection) Retrograde filling material: amalgam Bony defect filler: minced PRF mixed with resorbable bioactive glass + PRF membrane Protocol to obtain PRF:
Case no 2: Patient: 27-year-old female Tooth/teeth: 14,13,12,21,22 Diagnosis: exacerbated chronic periodontitis in relation to nonvital teeth: 14,13, 12,11,21; incomplete root canal fillings of teeth no: 14,13,12,11,21 Type of treatment: RCT + endodontic surgery (resection) Retrograde filling material: amalgam Bony defect filler: minced PRF mixed with resorbable BG + PRF membrane Protocol to obtain PRF:
| Endpoint: 7 months (1st case) 4 months (2nd case) The authors noticed satisfactory bone healing at the endpoint examination. |
| Dudeja et al. (2017) [135] | Case report | Patient: 26-year-old female Tooth/teeth: 21,22 Diagnosis: chronic periodontitis in relation to nonvital teeth: 21,22; suppurative sinus tract between teeth 22 and 23 Type of treatment: RCT + endodontic surgery (resection) Retrograde filling material: MTA Bony defect filler: PRF membrane + PRF mixed with an irradiated FDBA + collagen membrane Protocol to obtain PRF:
| Endpoint: 1 year After 1 year the authors observed continuation of healing process and decrease in the size of radiolucency. |
| Wadhwa et al. (2017) [136] | Case report | Patient: 25-year-old male Tooth/teeth: 46 Diagnosis: exacerbated chronic periodontitis in relation to nonvital tooth: 46 Type of treatment: RCT + endodontic surgery (resection) Retrograde filling material: MTA Bony defect filler: PRF membrane Protocol to obtain PRF:
| Endpoint: 18 months After 18 months the authors observed successful outcome of the healing process. |
| Vidhale et al. (2015) [137] | Case report | Patient: 22-year-old male Tooth/teeth: 21,22,23 Diagnosis: exacerbated chronic periodontitis in relation to nonvital teeth: 21,22, 23, radicular cyst Type of treatment: RCT + endodontic surgery (resection) Retrograde filling material: n/a Bony defect filler: PRF + iliac bone graft Protocol to obtain PRF:
| Endpoint: 3 months The authors noticed the presence of bone healing. |
| Bains et al. (2012) [138] | Case report | Patient: 39-year-old male Tooth/teeth: 46 Diagnosis: retrograde periodontitis along with Grade II furcation involvement with definitive pulpal perforation in the tooth 46, incomplete root canal treatment of tooth 47 Type of treatment: RCT + regenerative periodontal surgery Retrograde filling material: n/a Bony defect filler: PRF gel mixed with hydroxyapatite graft material + PRF membrane Protocol to obtain PRF:
| Endpoint: 1.5 years The authors noticed significant limitation of the radiolucency area. |
| Demiralp et al. (2004) [139] | Case report | Patient: 45-year-old male Tooth/teeth: 11,21 Diagnosis: exacerbated chronic periodontitis in relation to nonvital teeth: 11,21 Type of treatment: RCT + surgery (scaling and root-planning, resection was not performed) Retrograde filling material: n/a Bony defect filler: PRP gel + PRP gel mixed with TCP + PRP gel Protocol to obtain PRP:
| Endpoint: 1 year The authors noticed almost complete resorption of TCP particles and new bone formation. |
| Hiremath et al. (2014) [140] | Case report | Patient: 20-year-old male Tooth/teeth: 11,21,22 Diagnosis: exacerbated chronic periodontitis in relation to nonvital teeth: 11,21,22 Type of treatment: RCT + surgery (curettage of the defect) Retrograde filling material: n/a Bony defect filler: PRF mixed with HA Protocol to obtain PRP:
| Endpoint: 18 months After 18 months the authors observed complete bone healing. |
| Parikh et al. (2011) [141] | Case report | Patient: 24-year-old male Tooth/teeth: 11,21 Diagnosis: exacerbated chronic periodontitis in relation to nonvital teeth: 11,21 Type of treatment: RCT + surgery (curettage of the defect) Retrograde filling material: MTA Bony defect filler: PRP gel was placed at the site of larger defect (left side) Protocol to obtain PRP:
| Endpoint: 2 years After 8 weeks the authors observed better bone healing at the site treated with PRP. |
| Criteria | List of Specific Criteria |
|---|---|
| Inclusion criteria | randomized controlled trials |
| randomized clinical trials | |
| case reports | |
| case–control studies | |
| study population: adult patients (aged: 18 years old or more); permanent teeth with closed apexes, diagnosed with periapical lesions | |
| methods of treatment: RCT with application of PRGF | |
| Exclusion criteria | systematic reviews and metanalyses |
| comments | |
| animal studies | |
| study population: children with deciduous teeth, children and adolescents with immature teeth (teeth with opened apexes), teeth without periapical lesions | |
| methods of treatment: endodontic procedures without application of PRGF, endodontic surgery | |
| papers written in languages other than English |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zoltowska, A.; Machut, K.; Pawlowska, E.; Derwich, M. Plasma Rich in Growth Factors in the Treatment of Endodontic Periapical Lesions in Adult Patients: A Narrative Review. Pharmaceuticals 2021, 14, 1041. https://doi.org/10.3390/ph14101041
Zoltowska A, Machut K, Pawlowska E, Derwich M. Plasma Rich in Growth Factors in the Treatment of Endodontic Periapical Lesions in Adult Patients: A Narrative Review. Pharmaceuticals. 2021; 14(10):1041. https://doi.org/10.3390/ph14101041
Chicago/Turabian StyleZoltowska, Agata, Katarzyna Machut, Elzbieta Pawlowska, and Marcin Derwich. 2021. "Plasma Rich in Growth Factors in the Treatment of Endodontic Periapical Lesions in Adult Patients: A Narrative Review" Pharmaceuticals 14, no. 10: 1041. https://doi.org/10.3390/ph14101041
APA StyleZoltowska, A., Machut, K., Pawlowska, E., & Derwich, M. (2021). Plasma Rich in Growth Factors in the Treatment of Endodontic Periapical Lesions in Adult Patients: A Narrative Review. Pharmaceuticals, 14(10), 1041. https://doi.org/10.3390/ph14101041