Wheatgrass Juice Administration and Immune Measures during Adjuvant Chemotherapy in Colon Cancer Patients: Preliminary Results

Abstract
1. Introduction
2. Results
Clinical Outcomes
3. Discussion
4. Methods
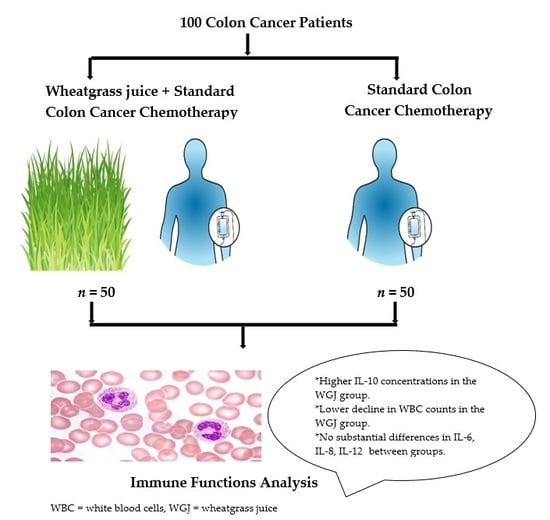
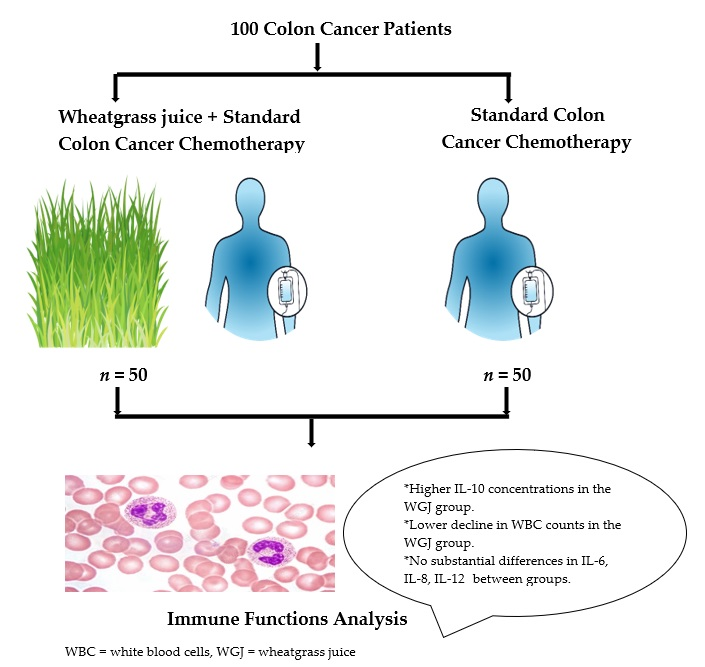
4.1. Patients and Procedure
4.2. Study Intervention
4.3. Blood Samples
4.4. Cytokines Assessment
4.5. Statistical Analysis
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Karanikas, M.; Esebidis, A. Increasing incidence of colon cancer in patients <50 years old: A new entity? Ann. Transl. Med. 2016, 4, 164. [Google Scholar] [CrossRef] [PubMed]
- Taieb, J.; André, T.; Auclin, E. Refining adjuvant therapy for non-metastatic colon cancer, new standards and perspectives. Cancer Treat. Rev. 2019, 75, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Morris, R.; Kershaw, N.J.; Babon, J.J. The molecular details of cytokine signaling via the JAK/STAT pathway. Protein Sci. 2018, 27, 1984–2009. [Google Scholar] [CrossRef] [PubMed]
- Holdsworth, S.R.; Can, P.Y. Cytokines: Names and numbers you should care about. Clin. J. Am. Soc. Nephrol. 2015, 10, 2243–2254. [Google Scholar] [CrossRef]
- Arita, M. Mediator lipidomics in acute inflammation and resolution. J. Biochem. 2012, 152, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Kadl, A.; Leitinger, N. The role of endothelial cells in the resolution of acute inflammation. Antioxid. Redox Signal. 2005, 7, 1744–1754. [Google Scholar] [CrossRef]
- Tuomisto, A.E.; Mäkinen, M.J.; Väyrynen, J.P. Systemic inflammation in colorectal cancer: Underlying factors, effects, and prognostic significance. World J. Gastroenterol. 2019, 25, 4383–4404. [Google Scholar] [CrossRef]
- Opal, S.M.; DePalo, V.A. Anti-inflammatory cytokines. Chest 2000, 117, 1162–1172. [Google Scholar] [CrossRef] [PubMed]
- Sultani, M.; Stringer, A.M.; Bowen, J.M.; Gibson, R.J. Anti-Inflammatory Cytokines: Important immunoregulatory factors contributing to chemotherapy-induced gastrointestinal mucositis. Chemother. Res. Pract. 2012, 2012, 490804. [Google Scholar] [CrossRef]
- Oun, R.; Moussa, Y.E.; Wheate, N.J. The side effects of platinum-based chemotherapy drugs: A review for chemists. Dalt. Trans. 2018, 47, 6645–6653. [Google Scholar] [CrossRef]
- Weissinger, F.; Heinz, W.J. Prevention and treatment of febrile neutropenia. Memo Mag. Eur. Med. Oncol. 2012, 5, 30–34. [Google Scholar] [CrossRef]
- Chen, Y.M.; Whang-Peng, J.; Liu, J.M.; Kuo, B.I.T.; Wang, S.Y.; Tsai, C.M.; Perng, R.P. Serum cytokine level fluctuations in chemotherapy-induced myelosuppression. Jpn. J. Clin. Oncol. 1996, 26, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Kasai, C.; Takeuchi, S.; Takemura, M.; Shimokawa, K.; Noma, A. Changes in serum cytokine levels in patients with malignant bone and soft tissue tumors in the course of chemotherapy. Jpn. J. Cancer Chemother 1992, 19, 1449–1452. (In Japanese) [Google Scholar]
- Lai, C.N. Chlorophyll: The Active factor in wheat sprout extract inhibiting the metabolic activation of carcinogens In Vitro. Nutr. Cancer 1979, 1, 19–21. [Google Scholar] [CrossRef]
- Gore, R.D.; Palaskar, S.J.; Bartake, A.R. Wheatgrass: Green blood can help to fight cancer. J. Clin. Diagn. Res. 2017, 11, ZC40–ZC42. [Google Scholar] [CrossRef]
- Bar-Sela, G.; Cohen, M.; Ben-Arye, E.; Epelbaum, R. The medical use of wheatgrass: Review of the gap between basic and clinical applications. Mini Rev. Med. Chem. 2015, 15, 1. [Google Scholar] [CrossRef] [PubMed]
- Rajoria, A.; Mehta, A.; Mehta, P.; Ahirwal, L.; Shukla, S.; Bajpai, V.K. Evaluation of antiproliferative and hepatoprotective effects of wheat grass (Triticum aestivum). Acta Biol. Hung. 2017, 68, 150–161. [Google Scholar] [CrossRef][Green Version]
- Shakya, G.; Balasubramanian, S.; Hoda, M.; Rajagopalan, R. Inhibition of metastasis and angiogenesis in Hep-2 cells by wheatgrass extract–an in vitro and in silico approach. Toxicol. Mech. Methods 2018, 28, 205–218. [Google Scholar] [CrossRef]
- Illmer, C.; Madlener, S.; Horvath, Z.; Saiko, P.; Losert, A.; Herbacek, I.; Grusch, M.; Krupitza, G.; Fritzer-Szekeres, M.; Szekeres, T. Immunologic and biochemical effects of the fermented wheat germ extract avemar. Exp. Biol. Med. 2005, 230, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.N.; Park, H.; Lee, K.E. Cytotoxic activities of fermented wheat germ extract on human gastric carcinoma cells by induction of apoptosis. J. Clin. Oncol. 2005, 23, 4254. [Google Scholar] [CrossRef]
- Saiko, P.; Ozsvar-Kozma, M.; Graser, G.; Lackner, A.; Grusch, M.; Madlener, S.; Krupitza, G.; Jaeger, W.; Hidvegi, M.; Agarwal, R.P.; et al. Avemar, a nontoxic fermented wheat germ extract, attenuates the growth of sensitive and 5-FdUrd/Ara-C cross-resistant H9 human lymphoma cells through induction of apoptosis. Oncol. Rep. 2009, 21, 787–791. [Google Scholar] [PubMed]
- Judson, P.L.; Al Sawah, E.; Marchion, D.C.; Xiong, Y.; Bicaku, E.; Zgheib, N.B.; Chon, H.S.; Stickles, X.B.; Hakam, A.; Wenham, R.M.; et al. Characterizing the efficacy of fermented wheat germ extract against ovarian cancer and defining the genomic basis of its activity. Int. J. Gynecol. Cancer 2012, 22, 960–967. [Google Scholar] [CrossRef]
- Jakab, F.; Shoenfeld, Y.; Balogh, Á.; Nichelatti, M.; Hoffmann, A.; Kahán, Z.; Lapis, K.; Mayer, Á.; Sápy, P.; Szentpétery, F.; et al. A medical nutriment has supportive value in the treatment of colorectal cancer. Br. J. Cancer 2003, 89, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Bar-Sela, G.; Tsalic, M.; Fried, G.; Goldberg, H. Wheat grass juice may improve hematological toxicity related to chemotherapy in breast cancer patients: A pilot study. Nutr. Cancer 2007, 58, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Garami, M.; Schuler, D.; Babosa, M.; Borgulya, G.; Hauser, P.; Müller, J.; Paksy, A.; Szabó, E.; Hidvégi, M.; Fekete, G. Fermented wheat germ extract reduces chemotherapy-induced febrile neutropenia in pediatric cancer patients. J. Pediatr. Hematol. Oncol. 2004, 26, 631–635. [Google Scholar] [CrossRef]
- Demidov, L.V.; Manziuk, L.V.; Kharkevitch, G.Y.; Pirogova, N.A.; Artamonova, E.V. Adjuvant fermented wheat germ extract (AvemarTM) nutraceutical improves survival of high-risk skin melanoma patients: A randomized, pilot, phase II clinical study with a 7-year follow-up. Cancer Biother. Radiopharm. 2008, 23, 477–482. [Google Scholar] [CrossRef]
- Sukkar, S.G.; Cella, F.; Rovera, G.M.; Nichelatti, M.; Ragni, G.; Chiavenna, G.; Giannoni, A.; Ronzani, G.; Ferrari, C. A multicentric prospective open trial on the quality of life and oxidative stress in patients affected by advanced head and neck cancer treated with a new benzoquinone-rich product derived from fermented wheat germ (Avemar). Med. J. Nutr. Metab. 2008, 1, 37–42. [Google Scholar] [CrossRef]
- Forget, P.; Simonet, O.; De Kock, M. Cancer surgery induces inflammation, immunosuppression and neo-angiogenesis, but is it influenced by analgesics? F1000Research 2013, 2, 102. [Google Scholar] [CrossRef]
- Vyas, D.; Laput, G.; Vyas, A.K. Chemotherapy-enhanced inflammation may lead to the failure of therapy and metastasis. Onco. Targets. Ther. 2014, 7, 1015–1023. [Google Scholar] [CrossRef]
- Seruga, B.; Zhang, H.; Bernstein, L.J.; Tannock, I.F. Cytokines and their relationship to the symptoms and outcome of cancer. Nat. Rev. Cancer 2008, 8, 887–899. [Google Scholar] [CrossRef]
- Laird, B.J.; McMillan, D.C.; Fayers, P.; Fearon, K.; Kaasa, S.; Fallon, M.T.; Klepstad, P. The systemic inflammatory response and its relationship to pain and other symptoms in advanced cancer. Oncologist 2013, 18, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Kamp, D.W.; Shacter, E.; Weitzman, S.A. Chronic inflammation and cancer: The role of the mitochondria. Oncology 2011, 25, 400–410, 413. [Google Scholar] [PubMed]
- Atretkhany, K.N.; Drutskaya, M.S. Myeloid-derived suppressor cells and proinflammatory cytokines as targets for cancer therapy. Biochemistry 2016, 81, 1274–1283. [Google Scholar] [CrossRef]
- Petersen, A.M.W.; Pedersen, B.K. The role of IL-6 in mediating the anti-inflammatory effects of exercise. Proc. J. Physiol. Pharmacol. 2006, 57, 43–51. [Google Scholar]
- Salvioli, S.; Capri, M.; Bucci, L.; Lanni, C.; Racchi, M.; Uberti, D.; Memo, M.; Mari, D.; Govoni, S.; Franceschi, C. Why do centenarians escape or postpone cancer? The role of IGF-1, inflammation and p53. Proc. Cancer Immunol. Immunother. 2009, 58, 1909–1917. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Kariyazono, H.; Komokata, T.; Hamada, N.; Sakata, R.; Yamada, K. Influence of preoperative administration of ω-3 fatty acid-enriched supplement on inflammatory and immune responses in patients undergoing major surgery for cancer. Nutrition 2005, 21, 639–649. [Google Scholar] [CrossRef]
- Wang, D.; Zhang, H.; Zhang, Y.; Li, W.; Sun, X.; Xing, Y.; Suo, J. Effects of omega-3 polyunsaturated fatty acids on postoperative inflammatory reaction and clinical efficacy. Zhonghua Wei Chang Wai Ke Za Zhi 2015, 18, 651–655. [Google Scholar]
- Lee, J.J. A phase II study of an herbal decoction that includes astragali radix for cancer-associated anorexia in patients with advanced cancer. Integr. Cancer Ther. 2010, 9, 24–31. [Google Scholar]
- Kim, K.C.; Yook, J.H.; Eisenbraun, J.; Kim, B.S.; Huber, R. Quality of life, immunomodulation and safety of adjuvant mistletoe treatment in patients with gastric carcinoma-a randomized, controlled pilot study. BMC Complement. Altern. Med. 2012, 12, 172. [Google Scholar] [CrossRef]
- Paixão, E.M.D.S.; Oliveira, A.C.D.M.; Pizato, N.; Muniz-Junqueira, M.I.; Magalhães, K.G.; Nakano, E.Y.; Ito, M.K. The effects of EPA and DHA enriched fish oil on nutritional and immunological markers of treatment naïve breast cancer patients: A randomized double-blind controlled trial. Nutr. J. 2017, 16, 71. [Google Scholar] [CrossRef]
- Gianotti, L.; Braga, M.; Fortis, C.; Soldini, L.; Vignali, A.; Colombo, S.; Radaelli, G.; Di Carlo, V. A prospective, randomized clinical trial on perioperative feeding with an arginine-, omega-3 fatty acid-, and RNA-enriched enteral diet: Effect on host response and nutritional status. J. Parenter. Enter. Nutr. 1999, 23, 314–320. [Google Scholar] [CrossRef]
- Chen, X.; Hu, Z.P.; Yang, X.X.; Huang, M.; Gao, Y.; Tang, W.; Chan, S.Y.; Dai, X.; Ye, J.; Ho, P.C.L.; et al. Monitoring of immune responses to a herbal immuno-modulator in patients with advanced colorectal cancer. Int. Immunopharmacol. 2006, 6, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Ostadrahimi, A.; Ziaei, J.E.; Esfahani, A.; Jafarabadi, M.A.; Movassaghpourakbari, A.; Farrin, N. Effect of beta glucan on white blood cell counts and serum levels of IL-4 and IL-12 in women with breast cancer undergoing chemotherapy: A randomized double-blind placebo-controlled clinical trial. Asian Pac. J. Cancer Prev. 2014, 15, 5733–5739. [Google Scholar] [CrossRef]
- Ben-Arye, E.; Goldin, E.; Wengrower, D.; Stamper, A.; Kohn, R.; Berry, E. Wheat grass juice in the treatment of active distal ulcerative colitis: A randomized double-blind placebo-controlled trial. Scand. J. Gastroenterol. 2002, 37, 444–449. [Google Scholar] [CrossRef]
- Bálint, G.; Apáthy, Á.; Gaál, M.; Telekes, A.; Resetár, Á.; Blazsó, G.; Falkay, G.; Szende, B.; Paksy, A.; Ehrenfeld, M.; et al. Effect of Avemar®—A fermented wheat germ extract—On rheumatoid arthritis. Preliminary data. Clin. Exp. Rheumatol. 2006, 24, 325–328. [Google Scholar]
- Lee, J.H.; Ki, H.H.; Kim, D.K.; Lee, Y.M. Triticum aestivum sprout extract attenuates 2,4-dinitrochlorobenzene-induced atopic dermatitis-like skin lesions in mice and the expression of chemokines in human keratinocytes. Mol. Med. Rep. 2018, 18, 3461–3468. [Google Scholar] [CrossRef] [PubMed]
- Parit, S.B.; Dawkar, V.V.; Tanpure, R.S.; Pai, S.R.; Chougale, A.D. Nutritional quality and antioxidant activity of wheatgrass (triticum aestivum) unwrap by proteome profiling and DPPH and FRAP assays. J. Food Sci. 2018, 83, 2127–2139. [Google Scholar] [CrossRef]
- Azizullah, A.; Rehman, Z.U.; Ali, I.; Murad, W.; Muhammad, N.; Ullah, W.; Häder, D.P. Chlorophyll derivatives can be an efficient weapon in the fight against dengue. Parasitol. Res. 2014, 113, 4321–4326. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.M.; Wang, L.; Zhu, W.; Gao, Y.H.; Wu, H.M.; Wang, M.; Hu, T.S.; Yan, Y.J.; Chen, Z.L. Preparation of a chlorophyll derivative and investigation of its photodynamic activities against cholangiocarcinoma. Biomed. Pharmacother. 2017, 92, 285–292. [Google Scholar] [CrossRef]
- Fujiwara, T.; Nishida, N.; Nota, J.; Kitani, T.; Aoishi, K.; Takahashi, H.; Sugahara, T.; Hato, N. Efficacy of chlorophyll c2 for seasonal allergic rhinitis: Single-center double-blind randomized control trial. Eur. Arch. Oto Rhino Laryngol. 2016, 273, 4289–4294. [Google Scholar] [CrossRef]
- Song, B.H.; Lee, D.H.; Kim, B.C.; Ku, S.H.; Park, E.J.; Kwon, I.H.; Kim, K.H.; Kim, K.J. Photodynamic therapy using chlorophyll-a in the treatment of acne vulgaris: A randomized, single-blind, split-face study. J. Am. Acad. Dermatol. 2014, 71, 764–771. [Google Scholar] [CrossRef]
- Shyam, R.; Singh, S.N.; Vats, P.; Singh, V.K.; Bajaj, R.; Singh, S.B.; Banerjee, P.K. Wheat grass supplementation decreases oxidative stress in healthy subjects: A comparative study with Spirulina. J. Altern. Complement. Med. 2007, 13, 789–791. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, S.R.; Chiu, H.F.; Chen, S.L.; Tsai, J.H.; Lee, M.Y.; Lee, H.S.; Shen, Y.C.; Yan, Y.Y.; Shane, G.T.; Wang, C.K. Effects of a Chinese medical herbs complex on cellular immunity and toxicity-related conditions of breast cancer patients. Br. J. Nutr. 2012, 107, 712–718. [Google Scholar] [CrossRef]
- Loo, W.T.Y.; Jin, L.; Chow, L.W.C.; Cheung, M.N.B.; Wang, M. Rhodiola algida improves chemotherapy-induced oral mucositis in breast cancer patients. Expert Opin. Investig. Drugs 2010, 19, S91–S100. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Xu, Z.; Wang, Z.; Zhang, M.; Yan, G.; Hou, A.; Deng, H.; Wu, J.; Zhao, X.; Xiang, Y.; et al. Clinical observation of Shuanghuang Shengbai Granule (双黄升白颗粒) on prevention and treatment of myelosuppression caused by chemotherapy in cancer patients. Chin. J. Integr. Med. 2017, 23, 105–109. [Google Scholar] [CrossRef]
- Sethi, J.; Yadav, M.; Dahiya, K.; Sood, S.; Singh, V.; Bhattacharya, S.B. Antioxidant effect of triticum aestivium (wheat grass) in high-fat diet-induced oxidative stress in rabbits. Methods Find. Exp. Clin. Pharmacol. 2010, 32, 233–235. [Google Scholar] [CrossRef]
- Bagwe, S.M.; Kale, P.P.; Bhatt, L.K.; Prabhavalkar, K.S. Herbal approach in the treatment of pancytopenia. J. Complement. Integr. Med. 2017, 14. [Google Scholar] [CrossRef]
- Yang, Y.; Xu, Y. Clinical randomized double-blinded controlled study on Quxie Capsule in reducing post-operational relapse and metastasis of colorectal cancer. Zhongguo Zhong Xi Yi Jie He Za Zhi 2007, 27, 879–882. [Google Scholar] [PubMed]
- Chan, K.K.; Yao, T.J.; Jones, B.; Zhao, J.F.; Ma, F.K.; Leung, C.Y.; Lau, S.K.; Yip, M.W.; Ngan, H.Y. The use of Chinese herbal medicine to improve quality of life in women undergoing chemotherapy for ovarian cancer: A double-blind placebo-controlled randomized trial with immunological monitoring. Ann. Oncol. 2011, 22, 2241–2249. [Google Scholar] [CrossRef] [PubMed]
- Grossman, S.A.; Ellsworth, S.; Campian, J.; Wild, A.T.; Herman, J.M.; Laheru, D.; Brock, M.; Balmanoukian, A.; Ye, X. Survival in patients with severe lymphopenia following treatment with radiation and chemotherapy for newly diagnosed solid tumors. JNCCN J. Natl. Compr. Cancer Netw. 2015, 13, 1225–1231. [Google Scholar] [CrossRef]
- Mendez, J.S.; Govindan, A.; Leong, J.; Gao, F.; Huang, J.; Campian, J.L. Association between treatment-related lymphopenia and overall survival in elderly patients with newly diagnosed glioblastoma. J. Neurooncol. 2016, 127, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Kozak, M.M.; Von Eyben, R.; Pai, J.S.; Anderson, E.M.; Welton, M.L.; Shelton, A.A.; Kin, C.; Koong, A.C.; Chang, D.T. The prognostic significance of pretreatment hematologic parameters in patients undergoing resection for colorectal cancer. Am. J. Clin. Oncol. Cancer Clin. Trials 2017, 40, 405–412. [Google Scholar] [CrossRef]
- Chu-Yuan, H.; Jing, P.; Yi-Sheng, W.; He-Ping, P.; Hui, Y.; Chu-Xiong, Z.; Guo-Jian, L.; Guo-Qiang, W. The impact of chemotherapy-associated neutrophil/ lymphocyte counts on prognosis of adjuvant chemotherapy in colorectal cancer. BMC Cancer 2013, 13, 177. [Google Scholar] [CrossRef] [PubMed]
- Lalani, I.; Bhol, K.; Ahmed, A.R. Interleukin-10: Biology, role in inflammation and autoimmunity. Ann. Allergy Asthma Immunol. 1997, 79, 469–484. [Google Scholar] [CrossRef]
- Tsai, C.C.; Lin, C.R.; Tsai, H.Y.; Chen, C.J.; Li, W.T.; Yu, H.M.; Ke, Y.Y.; Hsieh, W.Y.; Chang, C.Y.; Wu, C.Y.; et al. The immunologically active oligosaccharides isolated from wheatgrass modulate monocytes via toll-like receptor2 signaling. J. Biol. Chem. 2013, 288, 17689–17697. [Google Scholar] [CrossRef]
- Kanter, M.H.; Poole, G.; Garratty, G. Misinterpretation and misapplication of p values in antibody identification: The lack of value of a p value. Transfusion 1997, 37, 816–822. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences; Lawrence Earlbaum Associates: Hillside, NJ, USA, 1988; pp. 278–280. ISBN 0805802835. [Google Scholar]

{kind=link}
| Variable | Intervention | Control | p | |
|---|---|---|---|---|
| (n = 50) | (n = 50) | |||
| Age (years), M (SD) | 63.2 (10.2) | 60.8 (10.4) | t = −1.16 | 0.25 |
| Gender, N (%) a | ||||
| Male | 36 (72.0) | 30 (60.0) | χ2 = 1.60 | 0.21 |
| Female | 14 (28.0) | 20 (40.0) | ||
| M (SD) Education (years), | 14.3 (4.9) | 14.0 (3.8) | t = −0.34 | 0.74 |
| Familial status, N (%) | ||||
| Married/cohabiting | 40 (80) | 37 (74.0) | χ2 = 3.38 | 0.34 |
| Not married/cohabiting | 10 (20.0) | 13 (26.0) | ||
| Employed, N (%) | 13 (26.5) | 16 (35.5) | χ2 = 8.23 | 0.22 |
| Smoking, N (%) | ||||
| Current | 6 (13.0) | 12 (25.5) | χ2 = 2.44 | 0.30 |
| Past | 19 (41.3) | 18 (38.3) | ||
| Never | 21 (45.7) | 17 (36.2) | ||
| Physical activity, N (%) | ||||
| Low | 24 (54.5) | 24 (61.5) | χ2 = 0.53 | 0.77 |
| Medium | 15 (34.1) | 12 (30.8) | ||
| High | 5 (11.4) | 3 (7.7) | ||
| Disease stage, N (%) | ||||
| Stage II | 10 (20.0) | 3 (6.0) | χ2 = 4.35 | 0.11 |
| Stage III | 40 (80.0) | 47 (94.0) | ||
| Chemotherapy regimen, N (%) | ||||
| Xeloda (Capecitabine) | 11 (22.0) | 3 (6.0) | χ2 = 6.21 | 0.10 |
| Xelox (Capecitabine, Oxaliplatin) | 35 (70.0) | 42 (84.0) | ||
| Folfox (5-fluorouracil, Leucovorin, Oxaliplatin) | 4 (8.0) | 4 (8.0) | ||
| Number of background diseases, N (SD) | 1.04 (1.16) | 1.10 (1.23) | t = −0.25 | 0.80 |
| Anticoagulant treatment, N (%) | 12 (24.0) | 14 (28.0) | χ2 = 0.21 | 0.65 |
| Intervention n = (50) | Control n = (50) | |||||||
|---|---|---|---|---|---|---|---|---|
| M | SD | CI | M | SD | CI | t (df) | p | |
| IL-6 | ||||||||
| Baseline (T0) | 21.16 | 8.51 | 18.98, 23.64 | 19 | 9.63 | 16.45, 21.92 | −1.17 (95) | 0.25 |
| Post intervention (T1) | 21.35 | 8.33 | 18.90, 24.07 | 20.12 | 9.25 | 16.88, 23.67 | −0.56 (62) | 0.58 |
| IL-8 | ||||||||
| Baseline (T0) | 21.93 | 14.06 | 18.07, 25.90 | 17.59 | 13.56 | 13.84, 21.28 | −1.55 (95) | 0.13 |
| Post intervention (T1) | 16.33 | 11.79 | 13.07, 20.21 | 16.08 | 13.53 | 11.25, 21.77 | −0.08 (62) | 0.94 |
| IL-10 | ||||||||
| Baseline (T0) | 4.62 | 2.66 | 3.89, 5.41 | 4.42 | 4.34 | 3.41, 5.84 | −0.28 (95) | 0.78 |
| Post intervention (T1) | 5.14 | 2.55 | 4.33, 5.93 | 3.8 | 2.18 | 2.95, 4.59 | −2.19 (62) | 0.03 |
| IL-12 | ||||||||
| Baseline (T0) | 26.51 | 15.2 | 22.16, 30.77 | 23.66 | 13.19 | 20.29, 27.86 | −0.98 (95) | 0.33 |
| Post intervention (T1) | 22.57 | 12.71 | 18.67, 26.91 | 23.45 | 15.33 | 18.24, 29.24 | 0.25 (63) | 0.8 |
| WBCs | ||||||||
| Baseline (T0) | 6.77 | 1.56 | 6.34, 7.22 | 6.92 | 2 | 6.38, 7.52 | 0.42 (92) | 0.67 |
| Post intervention (T1) | 6.2 | 2.07 | 5.54, 6.99 | 5.61 | 1.71 | 5.01, 6.20 | −1.27 (65) | 0.21 |
| Neutrophils | ||||||||
| Baseline (T0) | 3.78 | 1.28 | 3.42, 4.17 | 4.26 | 1.37 | 3.89, 4.68 | 1.76 (91) | 0.08 |
| Post intervention (T1) | 3.29 | 1.68 | 2.80, 3.87 | 3.09 | 1.3 | 2.68, 3.57 | −0.56 (65) | 0.58 |
| Lymphocytes | ||||||||
| Baseline (T0) | 2.01 | 0.74 | 1.80, 2.20 | 1.87 | 0.94 | 1.62, 2.15 | −0.75 (89) | 0.46 |
| Post intervention (T1) | 1.76 | 0.69 | 1.54, 1.98 | 1.61 | 0.75 | 1.36, 1.86 | −0.86 (64) | 0.4 |
| Monocytes | ||||||||
| Baseline (T0) | 0.68 | 0.23 | 0.61, 0.74 | 0.6 | 0.22 | 0.54, 0.67 | −1.60 (89) | 0.11 |
| Post intervention (T1) | 0.88 | 0.38 | 0.76, 1.01 | 0.71 | 0.26 | 0.63, 0.80 | −2.15 (64) | 0.04 |
| WBC difference a | −0.48 | 2.26 | −1.25, 0.32 | −1.48 | 1.63 | −2.08, −0.91 | −2.04 (63) | 0.046 |
| Neutrophil difference | −0.38 | 1.86 | −0.97, 0.23 | −1.13 | 1.38 | −1.62, −0.65 | −1.82 (63) | 0.07 |
| Lymphocytes difference | −0.26 | 0.54 | −0.46, 0.10 | −0.42 | 0.49 | −0.60, −0.24 | −1.17 (59) | 0.25 |
| Monocytes difference | 0.17 | 0.37 | 0.05, 0.31 | 0.09 | 0.24 | 0.00, 0.18 | −1.00 (59) | 0.32 |
| IL-6 (n = 90) | IL-8 (n = 90) | IL-10 (n = 97) | IL-12 (n = 87) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | 95% CI | p | B | SE | 95% CI | p | B | SE | 95% CI | p | B | SE | 95% CI | p | |
| Time a | −0.03 | 2.04 | −4.10, 4.05 | 0.99 | 4.22 | 3.43 | −2.60, 11.05 | 0.22 | 0.64 | 0.62 | −0.61, 1.88 | 0.31 | 2.68 | 3.82 | −4.92, 10.28 | 0.49 |
| Group b | 1.63 | 2.41 | −3.19, 6.46 | 0.50 | 0.95 | 3.53 | −6.13, 8.03 | 0.79 | 1.28 | 0.63 | 0.02, 2.55 | 0.046 | 1.28 | 3.83 | −6.39, 8.95 | 0.74 |
| Time*Group c | −0.40 | 2.64 | −5.67, 4.87 | 0.88 | 1.58 | 4.43 | −7.24, 10.41 | 0.72 | −1.17 | 0.83 | −2.84, 0.51 | 0.17 | 0.96 | 5.04 | −9.07, 11.00 | 0.85 |
| Education (years) | 0.34 | 0.19 | −0.04, 0.71 | 0.08 | 0.70 | 0.25 | 0.21, 1.19 | 0.01 | - | - | - | - | 0.43 | 0.24 | −0.05, 0.90 | 0.08 |
| Gender | - | - | - | - | 2.37 | 2.34 | −2.28, 7.02 | 0.31 | 0.55 | 0.57 | −0.60, 1.69 | 0.34 | - | - | - | - |
| Smoking | - | - | - | - | - | - | - | - | - | - | - | - | 8.26 | 2.79 | 2.70, 13.82 | 0.00 |
| Background Diseases | - | - | - | - | −2.81 | 1.03 | −4.85, −0.77 | 0.01 | - | - | - | - | - | - | - | - |
| WBC (n = 91) | Neutrophils (n = 96) | Lymphocytes (n = 91) | Monocytes (n = 96) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | 95% CI | p | B | SE | 95% CI | p | B | SE | 95% CI | p | B | SE | 95% CI | p | |
| Time a | 1.43 | 0.37 | 0.68, 2.18 | 0.00 | 1.17 | 0.29 | 0.60, 1.74 | 0.00 | 0.36 | 0.09 | 0.17, 0.54 | 0.00 | −0.10 | 0.06 | −0.21, 0.02 | 0.1 |
| Group b | 0.83 | 0.51 | −0.19, 1.84 | 0.11 | 0.24 | 0.37 | −0.49, 0.97 | 0.52 | 0.33 | 0.16 | 0.01, 0.66 | 0.04 | 0.20 | 0.08 | 0.04, 0.35 | 0.02 |
| Time*Group c | −0.97 | 0.51 | −1.99, 0.06 | 0.07 | −0.72 | 0.40 | −1.51, 0.07 | 0.07 | −0.08 | 0.13 | −0.34, 0.17 | 0.51 | −0.10 | 0.08 | −0.26, 0.05 | 0.2 |
| Smoking | 1.08 | 0.47 | 0.15, 2.01 | 0.02 | - | - | - | - | - | - | - | - | - | - | - | - |
| Employment | - | - | - | - | - | - | - | - | −0.12 | 0.17 | −0.45, 0.22 | 0.49 | - | - | - | - |
| Gender | - | - | - | - | - | - | - | - | - | - | - | - | 0.10 | 0.05 | 0.01, 0.19 | 0.03 |
| Disease Stage | - | - | - | - | - | - | - | - | - | - | - | - | 0.19 | 0.06 | 0.07, 0.32 | 0 |
| Variable | Intervention (n = 50) | Control (n = 50) | p |
|---|---|---|---|
| Diarrhea grade I–II, N (%) | 9 (18%) | 9 (18%) | |
| Diarrhea grade ≥III, N (%) | 8 (16%) | 11 (22%) | 0.47 |
| Nausea and vomiting grade ≥II, N (%) | 3 (6%) | 8 (16%) | 0.12 |
| Number of hospitalizations during treatment, N (%) | 11 (22%) | 14 (28%) | 0.64 |
| Number of patients with relapse, N (%) | 14 (28%) | 9 (18%) | 0.24 |
| Overall survival 3rd year, N (%) | 47 (94%) | 42 (84%) | 0.14 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Avisar, A.; Cohen, M.; Katz, R.; Shentzer Kutiel, T.; Aharon, A.; Bar-Sela, G. Wheatgrass Juice Administration and Immune Measures during Adjuvant Chemotherapy in Colon Cancer Patients: Preliminary Results. Pharmaceuticals 2020, 13, 129. https://doi.org/10.3390/ph13060129
Avisar A, Cohen M, Katz R, Shentzer Kutiel T, Aharon A, Bar-Sela G. Wheatgrass Juice Administration and Immune Measures during Adjuvant Chemotherapy in Colon Cancer Patients: Preliminary Results. Pharmaceuticals. 2020; 13(6):129. https://doi.org/10.3390/ph13060129
Chicago/Turabian StyleAvisar, Adva, Miri Cohen, Rina Katz, Talia Shentzer Kutiel, Anat Aharon, and Gil Bar-Sela. 2020. "Wheatgrass Juice Administration and Immune Measures during Adjuvant Chemotherapy in Colon Cancer Patients: Preliminary Results" Pharmaceuticals 13, no. 6: 129. https://doi.org/10.3390/ph13060129
APA StyleAvisar, A., Cohen, M., Katz, R., Shentzer Kutiel, T., Aharon, A., & Bar-Sela, G. (2020). Wheatgrass Juice Administration and Immune Measures during Adjuvant Chemotherapy in Colon Cancer Patients: Preliminary Results. Pharmaceuticals, 13(6), 129. https://doi.org/10.3390/ph13060129