Preliminary Results of the FASM Study, an On-Going Italian Active Pharmacovigilance Project

 , , and
, , and
Abstract
1. Introduction
2. Results
2.1. Overall Results
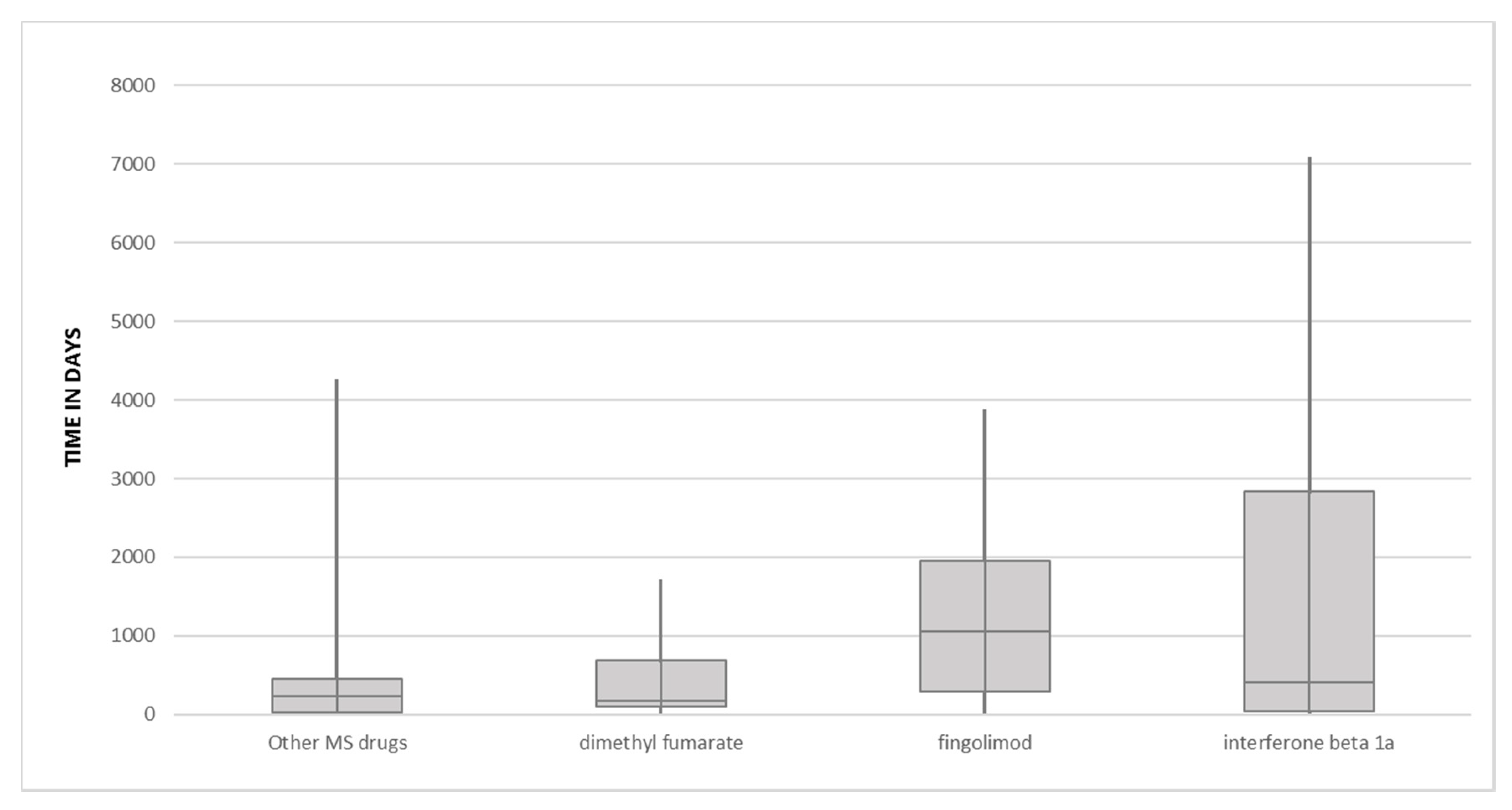
2.2. Focus on Drugs Most Commonly Reported as Suspected
3. Discussion
3.1. Overall Results
3.2. Dimethyl Fumarate, Fingolimod and IFN Beta1a-Related ICSRs
4. Materials and Methods
4.1. FASM Project
4.1.1. Collection of Individual Case Safety Reports
4.1.2. Data Analysis
4.1.3. Compliance with Ethical Standard
5. Study Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. The FASM Group: Full List of Consortium Members and Their Affiliations
- 20
- I Division of Neurology Department of Advanced Medical and Surgical Sciences—“DAMSS” School of Medicine and Surgery University of Campania Luigi Vanvitelli, 81100 Naples, Italy
- 21
- Complex Operating Unit of Pharmacy, AORN A Cardarelli, 80131 Naples, Italy
- 22
- Department of Advanced Biomedical Sciences, University Federico II of Naples, 80131 Naples, Italy
- 23
- Azienda Ospedaliera S.G. Moscati, 83100 Avellino, Italy
- 24
- Azienda Ospedaliera R.N. dei Colli, 80131 Naples, Italy
- 25
- A.S.L. Caserta, 81100 Caserta, Italy
- 26
- Azienda Ospedaliera di Caserta, 81100 Caserta, Italy
- 27
- OO.RR. San Giovanni di Dio Ruggi d’Aragona, 84131 Salerno, Italy
- 28
- A.S.L. Napoli 1 Centro, 80145 Naples, Italy
References
- Auricchio, F.; Scavone, C.; Cimmaruta, D.; Di Mauro, G.; Capuano, A.; Sportiello, L.; Rafaniello, C. Drugs approved for the treatment of multiple sclerosis: Review of their safety profile. Expert Opin. Drug Saf. 2017, 16, 1359–1371. [Google Scholar] [CrossRef] [PubMed]
- Faissner, S.; Gold, R. Efficacy and Safety of the Newer Multiple Sclerosis Drugs Approved Since 2010. CNS Drugs 2018, 32, 269–287. [Google Scholar] [CrossRef] [PubMed]
- Bivona, G.; Gambino, C.M.; Iacolino, G.; Ciaccio, M. Vitamin D and the nervous system. Neurol. Res. 2019, 41, 827–835. [Google Scholar] [CrossRef] [PubMed]
- Bivona, G.; Agnello, L.; Bellia, C.; Iacolino, G.; Scazzone, C.; Sasso, B.L.; Ciaccio, M. Non-Skeletal Activities of Vitamin D: From Physiology to Brain Pathology. Medicina 2019, 55, 341. [Google Scholar] [CrossRef] [PubMed]
- Scazzone, C.; Agnello, L.; Sasso, B.L.; Ragonese, P.; Bivona, G.; Realmuto, S.; Iacolino, G.; Gambino, C.M.; Bellia, C.; Salemi, G.; et al. Klotho and vitamin D in multiple sclerosis: An Italian study. Arch. Med Sci. 2020, 16, 842–847. [Google Scholar] [CrossRef] [PubMed]
- Scazzone, C.; Agnello, L.; Bivona, G.; Sasso, B.L.; Ciaccio, M. Vitamin D and Genetic Susceptibility to Multiple Sclerosis. Biochem. Genet. 2020. [Google Scholar] [CrossRef] [PubMed]
- Tullman, M.J. Overview of the epidemiology, diagnosis, and disease progression associated with multiple sclerosis. Am. J. Manag. Care 2013, 19 (Suppl. 2), S15–S20. [Google Scholar]
- Gugliandolo, A.; Longo, F.; Marrosu, M.G.; Mancardi, G.L.; Gandoglia, I.; Melis, M.; Giudice, F.L.; Bramanti, P.; Mazzon, E. A multicentric pharmacovigilance study: Collection and analysis of adverse drug reactions in relapsing-remitting multiple sclerosis patients. Ther. Clin. Risk Manag. 2018, 14, 1765–1788. [Google Scholar] [CrossRef]
- Tintoré, M.; Vidal-Jordana, A.; Sastre-Garriga, J. Treatment of multiple sclerosis—Success from bench to bedside. Nat. Rev. Neurol. 2019, 15, 53–58. [Google Scholar] [CrossRef]
- PRISMS (Prevention of Relapses and Disability by Interferon Beta-1a Subcutaneously in Multiple Sclerosis) Study Group. Randomised double-blind placebo-controlled study of interferon beta-1a in relapsing/remitting multiple sclerosis. Lancet 1998, 352, 1498–1504. [Google Scholar] [CrossRef]
- Comi, G.; Filippi, M.; Wolinsky, J.S. European/Canadian multicenter, double-blind, randomized, placebo-controlled study of the effects of glatiramer acetate on magnetic resonance imaging—Measureddisease activity and burden in patients with relapsing multiple sclerosis. Ann. Neurol. 2001, 49, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Guarnera, C.; Bramanti, P.; Mazzon, E. Comparison of efficacy and safety of oral agents for the treatment of relapsing–remitting multiple sclerosis. Drug Des. Dev. Ther. 2017, 11, 2193–2207. [Google Scholar] [CrossRef] [PubMed]
- European Medicine Agency. Measures to Minimise Risk of Serious Side Effects of Multiple Sclerosis Medicine Lemtrada. Available online: https://www.ema.europa.eu/en/documents/press-release/measures-minimise-risk-serious-side-effects-multiple-sclerosis-medicine-lemtrada_en.pdf (accessed on 21 July 2020).
- Lanzillo, R.; Moccia, M.; Palladino, R.; Signoriello, E.; Carotenuto, A.; Maniscalco, G.T.; Saccà, F.; Bonavita, S.; Russo, C.; Iodice, R.; et al. Clinical predictors of Dimethyl Fumarate response in multiple sclerosis: A real life multicentre study. Mult. Scler. Relat. Disord. 2020, 38, 101871. [Google Scholar] [CrossRef] [PubMed]
- Maniscalco, G.T.; Cerillo, I.; Servillo, G.; Napolitano, M.; Guarcello, G.; Abate, V.; Improta, G.; Florio, C. Early neutropenia with thrombocytopenia following alemtuzumab treatment for multiple sclerosis: Case report and review of literature. Clin. Neurol. Neurosurg. 2018, 175, 134–136. [Google Scholar] [CrossRef]
- Maniscalco, G.T.; Annunziata, M.; Ranieri, A.; Alfieri, G.; Renna, R.; Di Iorio, W.; Guarcello, G.; Cerillo, I.; Improta, G.; Florio, C. Remission of early persistent cladribine-induced neutropenia after filgrastim therapy in a patient with Relapsing—Remitting Multiple Sclerosis. Mult. Scler. Relat. Disord. 2020, 43, 102151. [Google Scholar] [CrossRef] [PubMed]
- Frau, J.; The i-MuST Study Group; Saccà, F.; Signori, A.; Baroncini, D.; Fenu, G.; Annovazzi, P.; Capobianco, M.; Signoriello, E.; Laroni, A.; et al. Outcomes after fingolimod to alemtuzumab treatment shift in relapsing–remitting MS patients: A multicentre cohort study. J. Neurol. 2019, 266, 2440–2446. [Google Scholar] [CrossRef] [PubMed]
- Buonomo, A.R.; Saccà, F.; Zappulo, E.; De Zottis, F.; Lanzillo, R.; Gentile, I.; Carotenuto, A.; Borgia, G.; Russo, C.V. Bacterial and CMV pneumonia in a patient treated with alemtuzumab for multiple sclerosis. Mult. Scler. Relat. Disord. 2019, 27, 44–45. [Google Scholar] [CrossRef]
- Russo, C.V.; Saccà, F.; Paternoster, M.; Buonomo, A.R.; Gentile, I.; Scotto, R.; Morra, V.B.; Mansueto, G. Post-mortem diagnosis of invasive pulmonary aspergillosis after alemtuzumab treatment for multiple sclerosis. Mult. Scler. J. 2019, 26, 123–126. [Google Scholar] [CrossRef]
- Koutsouraki, E.; Costa, V.; Baloyannis, S.J.; Koutsouraki, E. Epidemiology of multiple sclerosis in Europe: A Review. Int. Rev. Psychiatry 2010, 22, 2–13. [Google Scholar] [CrossRef]
- Grassivaro, F.; Puthenparampil, M.; Pengo, M.; Saiani, M.; Venturini, M.; Stropparo, E.; Perini, P.; Rinaldi, F.; Freddi, N.; Cadaldini, M.; et al. Multiple Sclerosis Incidence and Prevalence Trends in the Province of Padua, Northeast Italy, 1965–2018. Neuroepidemiology 2019, 52, 41–46. [Google Scholar] [CrossRef]
- Harbo, H.F.; Gold, R.; Tintoré, M. Sex and gender issues in multiple sclerosis. Ther. Adv. Neurol. Disord. 2013, 6, 237–248. [Google Scholar] [CrossRef]
- Zucker, I.; Prendergast, B.J. Sex differences in pharmacokinetics predict adverse drug reactions in women. Biol. Sex Differ. 2020, 11, 32. [Google Scholar] [CrossRef] [PubMed]
- Rademaker, M. Do Women Have More Adverse Drug Reactions? Am. J. Clin. Dermatol. 2001, 2, 349–351. [Google Scholar] [CrossRef]
- Scavone, C.; Sessa, M.; Clementi, E.; Corrao, G.; Leone, R.; Mugelli, A.; Rossi, F.; Spina, E.; Capuano, A. Real World Data on the Utilization Pattern and Safety Profile of Infliximab Originator Versus Biosimilars in Italy: A Multiregional Study. BioDrugs 2018, 32, 607–617. [Google Scholar] [CrossRef] [PubMed]
- Scavone, C.; Di Mauro, C.; Ruggiero, R.; Bernardi, F.F.; Trama, U.; Aiezza, M.L.; Rafaniello, C.; Capuano, A. Severe Cutaneous Adverse Drug Reactions Associated with Allopurinol: An Analysis of Spontaneous Reporting System in Southern Italy. Drugs Real World Outcomes 2019, 7, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Scavone, C.; Rafaniello, C.; Berrino, L.; Rossi, F.; Capuano, A. Strengths, weaknesses and future challenges of biosimilars’ development. An opinion on how to improve the knowledge and use of biosimilars in clinical practice. Pharmacol. Res. 2017, 126, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Scavone, C.; Sportiello, L.; Sullo, M.G.; Ferrajolo, C.; Ruggiero, R.; Sessa, M.; Berrino, P.M.; Di Mauro, G.; Berrino, L.; Rossi, F.; et al. Safety Profile of Anticancer and Immune-Modulating Biotech Drugs Used in a Real World Setting in Campania Region (Italy): BIO-Cam Observational Study. Front. Pharmacol. 2017, 8, 607. [Google Scholar] [CrossRef]
- Scavone, C.; Sportiello, L.; Berrino, L.; Rossi, F.; Capuano, A. Biosimilars in the European Union from comparability exercise to real world experience: What we achieved and what we still need to achieve. Pharmacol. Res. 2017, 119, 265–271. [Google Scholar] [CrossRef]
- Fragoso, Y.D. Adverse events and monitoring requirements associated with monoclonal antibody therapy in patients with multiple sclerosis. Drugs Ther. Perspect. 2019, 35, 627–634. [Google Scholar] [CrossRef]
- Berenguer-Ruiz, L.; Gimenez-Martinez, J.; Palazón-Bru, A.; Sempere, Á.P. Relapses and obstetric outcomes in women with multiple sclerosis planning pregnancy. J. Neurol. 2019, 266, 2512–2517. [Google Scholar] [CrossRef]
- Triplett, J.D.; Vijayan, S.; Rajanayagam, S.; Tuch, P.; Kermode, A.G.; Sivaajani, R.; Phillip, T. Pregnancy outcomes amongst multiple sclerosis females with third trimester natalizumab use. Mult. Scler. Relat. Disord. 2020, 40, 101961. [Google Scholar] [CrossRef]
- Haghikia, A.; Langer-Gould, A.; Rellensmann, G.; Schneider, H.; Tenenbaum, T.; Elias-Hamp, B.; Menck, S.; Zimmermann, J.; Herbstritt, S.; Marziniak, M.; et al. Natalizumab Use During the Third Trimester of Pregnancy. JAMA Neurol. 2014, 71, 891–895. [Google Scholar] [CrossRef]
- Friend, S.; Richman, S.; Bloomgren, G.; Cristiano, L.M.; Wenten, M. Evaluation of pregnancy outcomes from the Tysabri® (natalizumab) pregnancy exposure registry: A global, observational, follow-up study. BMC Neurol. 2016, 16, 150. [Google Scholar] [CrossRef]
- Dobson, R.; Dassan, P.; Roberts, M.; Giovannoni, G.; Nelson-Piercy, C.; Brex, P.A. UK consensus on pregnancy in multiple sclerosis: ‘Association of British Neurologists’ guidelines. Pract. Neurol. 2019, 19, 106–114. [Google Scholar] [CrossRef]
- Cree, B.A.; Mares, J.; Hartung, H.-P. Current therapeutic landscape in multiple sclerosis. Curr. Opin. Neurol. 2019, 32, 365–377. [Google Scholar] [CrossRef]
- Rau, D.; Lang, M.; Harth, A.; Naumann, M.; Weber, F.; Tumani, H.; Bayas, A. Listeria Meningitis Complicating Alemtuzumab Treatment in Multiple Sclerosis—Report of Two Cases. Int. J. Mol. Sci. 2015, 16, 14669–14676. [Google Scholar] [CrossRef]
- Giarola, B.; Massey, J.C.; Barnett, Y.; Rodrigues, M.; Sutton, I. Autoimmune encephalitis following alemtuzumab treatment of multiple sclerosis. Mult. Scler. Relat. Disord. 2019, 28, 31–33. [Google Scholar] [CrossRef]
- Baker, D.; Herrod, S.S.; Alvarez-Gonzalez, C.; Giovannoni, G.; Schmierer, K. Interpreting Lymphocyte Reconstitution Data From the Pivotal Phase 3 Trials of Alemtuzumab. JAMA Neurol. 2017, 74, 961–969. [Google Scholar] [CrossRef]
- Cossburn, M.; Pace, A.A.; Jones, J.; Ali, R.; Ingram, G.; Baker, K.; Hirst, C.L.; Zajicek, J.; Scolding, N.; Boggild, M.; et al. Autoimmune disease after alemtuzumab treatment for multiple sclerosis in a multicenter cohort. Neurology 2011, 77, 573–579. [Google Scholar] [CrossRef]
- Klotz, L.; Havla, J.; Schwab, N.; Hohlfeld, R.; Barnett, M.; Reddel, S.; Wiendl, H. Risks and risk management in modern multiple sclerosis immunotherapeutic treatment. Ther. Adv. Neurol. Disord. 2019, 12. [Google Scholar] [CrossRef]
- Arvin, A.M.; Wolinsky, J.S.; Kappos, L.; Morris, M.I.; Reder, A.T.; Tornatore, C.; Gershon, A.; Gershon, M.; Levin, M.J.; Bezuidenhoudt, M.; et al. Varicella-zoster virus infections in patients treated with fingolimod: Risk assessment and consensus recommendations for management. JAMA Neurol. 2015, 72, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Samaraweera, A.P.; Cohen, S.N.; Akay, E.M.; Evangelou, N. Lymphomatoid papulosis: A cutaneous lymphoproliferative disorder in a patient on fingolimod for multiple sclerosis. Mult. Scler. J. 2015, 22, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Product Monograph Including Patient Medication Information OCREVUS®. Available online: https://www.rochecanada.com/PMs/Ocrevus/OCREVUS_PM_E.pdf (accessed on 14 December 2020).
- Narapureddy, B.; Dubey, D. Clinical evaluation of dimethyl fumarate for the treatment of relapsing-remitting multiple sclerosis: Efficacy, safety, patient experience and adherence. Patient Prefer. Adherence 2019, 13, 1655–1666. [Google Scholar] [CrossRef] [PubMed]
- Gold, R.; Kappos, L.; Arnold, D.L.; Bar-Or, A.; Giovannoni, G.; Selmaj, K.; Tornatore, C.; Sweetser, M.T.; Yang, M.S.M.; Sheikh, S.I.; et al. Placebo-Controlled Phase 3 Study of Oral BG-12 for Relapsing Multiple Sclerosis. N. Engl. J. Med. 2012, 367, 1098–1107. [Google Scholar] [CrossRef]
- Fox, R.J.; Miller, D.H.; Phillips, J.T.; Hutchinson, M.; Havrdova, E.; Kita, M.; Yang, M.; Raghupathi, K.; Novas, M.; Sweetser, M.T.; et al. Placebo-Controlled Phase 3 Study of Oral BG-12 or Glatiramer in Multiple Sclerosis. N. Engl. J. Med. 2012, 367, 1087–1097. [Google Scholar] [CrossRef]
- Karussis, D.; Teitelbaum, D.; Sicsic, C.; Brenner, T. Long-term treatment of multiple sclerosis with glatiramer acetate: Natural history of the subtypes of anti-glatiramer acetate antibodies and their correlation with clinical efficacy. J. Neuroimmunol. 2010, 220, 125–130. [Google Scholar] [CrossRef]
- Sandberg-Wollheim, M.; Neudorfer, O.; Grinspan, A.; Weinstock-Guttman, B.; Haas, J.; Izquierdo, G.; Riley, C.; Ross, A.P.; Baruch, P.; Drillman, T.; et al. Pregnancy Outcomes from the Branded Glatiramer Acetate Pregnancy Database. Int. J. MS Care 2018, 20, 9–14. [Google Scholar] [CrossRef]
- Jacobs, L.D.; Cookfair, D.L.; Rudick, R.A.; Herndon, R.M.; Richert, J.R.; Salazar, A.M.; Fischer, J.S.; Goodkin, D.E.; Granger, C.V.; Simon, J.H.; et al. Intramuscular interferon beta-1a for disease progression in relapsing multiple sclerosis. Ann. Neurol. 1996, 39, 285–294. [Google Scholar] [CrossRef]
- Kretzschmar, B.; Pellkofer, H.; Weber, M.S. The Use of Oral Disease-Modifying Therapies in Multiple Sclerosis. Curr. Neurol. Neurosci. Rep. 2016, 16. [Google Scholar] [CrossRef]
- Gajofatto, A.; Benedetti, M.D. Treatment strategies for multiple sclerosis: When to start, when to change, when to stop? World J. Clin. Cases 2015, 3, 545–555. [Google Scholar] [CrossRef]
- Marangi, A.; Farina, G.; Vicenzi, V.; Forlivesi, S.; Calabria, F.; Marchioretto, F.; Forgione, A.; Rossi, F.; Stenta, G.; Vianello, M.; et al. Changing therapeutic strategies and persistence to disease-modifying treatments in a population of multiple sclerosis patients from Veneto region, Italy. Mult. Scler. Relat. Disord. 2020, 41, 102004. [Google Scholar] [CrossRef]
- Linker, R.A.; Haghikia, A. Dimethyl fumarate in multiple sclerosis: Latest developments, evidence and place in therapy. Ther. Adv. Chronic Dis. 2016, 7, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Morales, F.S.; Koralnik, I.J.; Gautam, S.; Samaan, S.; Sloane, J.A. Risk factors for lymphopenia in patients with relapsing–remitting multiple sclerosis treated with dimethyl fumarate. J. Neurol. 2019, 267, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Briner, M.; Bagnoud, M.; Miclea, A.; Friedli, C.; Diem, L.; Chan, A.; Hoepner, R.; Salmen, A. Time course of lymphocyte repopulation after dimethyl fumarate-induced grade 3 lymphopenia: Contribution of patient age. Ther. Adv. Neurol. Disord. 2019, 12. [Google Scholar] [CrossRef] [PubMed]
- Min, J.; Cohan, S.; Alvarez, E.; Sloane, J.; Phillips, J.T.; Van Der Walt, A.; Koulinska, I.; Fang, F.; Miller, C.; Chan, A. Real-World Characterization of Dimethyl Fumarate-Related Gastrointestinal Events in Multiple Sclerosis: Management Strategies to Improve Persistence on Treatment and Patient Outcomes. Neurol. Ther. 2019, 8, 109–119. [Google Scholar] [CrossRef]
- Phillips, J.T.; Selmaj, K.W.; Gold, R.; Fox, R.J.; Havrdova, E.K.; Giovannoni, G.; Abourjaily, H.; Pace, A.; Novas, M.; Hotermans, C.; et al. Clinical Significance of Gastrointestinal and Flushing Events in Patients with Multiple Sclerosis Treated with Delayed-Release Dimethyl Fumarate. Int. J. MS Care 2015, 17, 236–243. [Google Scholar] [CrossRef]
- Calabresi, P.A.; Radue, E.-W.; Goodin, D.; Jeffery, D.; Rammohan, K.W.; Reder, A.T.; Vollmer, T.; Agius, A.; Kappos, L.; Stites, T.; et al. Safety and efficacy of fingolimod in patients with relapsing-remitting multiple sclerosis (FREEDOMS II): A double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Neurol. 2014, 13, 545–556. [Google Scholar] [CrossRef]
- Cohen, J.A.; Barkhof, F.; Comi, G.; Hartung, H.-P.; Khatri, B.O.; Montalban, X.; Pelletier, J.; Capra, R.; Gallo, P.; Izquierdo, G.; et al. Oral Fingolimod or Intramuscular Interferon for Relapsing Multiple Sclerosis. N. Engl. J. Med. 2010, 362, 402–415. [Google Scholar] [CrossRef]
- Alping, P.; Askling, J.; Burman, J.; Fink, K.; Fogdell-Hahn, A.; Gunnarsson, M.; Hillert, J.; Langer-Gould, A.; Lycke, J.; Nilsson, P.; et al. Cancer Risk for Fingolimod, Natalizumab, and Rituximab in Multiple Sclerosis Patients. Ann. Neurol. 2020, 87, 688–699. [Google Scholar] [CrossRef]
- Pellegrino, P.; Carnovale, C.; Perrone, V.; Pozzi, M.; Antoniazzi, S.; Radice, S.; Clementi, E. Efficacy of vaccination against influenza in patients with multiple sclerosis: The role of concomitant therapies. Vaccine 2014, 32, 4730–4735. [Google Scholar] [CrossRef]
- Mahajan, K.R.; Ko, J.S.; Tetzlaff, M.T.; Hudgens, C.W.; Billings, S.D.; Cohen, J.A. Merkel cell carcinoma with fingolimod treatment for multiple sclerosis: A case report. Mult. Scler. Relat. Disord. 2017, 17, 12–14. [Google Scholar] [CrossRef] [PubMed]
- Michiels, Y.; Bugnon, O.; Michiels, J.-F.; Mazellier, S. Detection of a new melanoma in a patient treated with fingolimod. BMJ Case Rep. 2019, 12, e227951. [Google Scholar] [CrossRef] [PubMed]
- Velter, C.; Thomas, M.; Cavalcanti, A.; Bastien, M.; Chochon, F.; Lubetzki, C.; Routier, E.; Robert, C. Melanoma during fingolimod treatment for multiple sclerosis. Eur. J. Cancer 2019, 113, 75–77. [Google Scholar] [CrossRef] [PubMed]
- The IFNB Multiple Sclerosis Study Group. Interferon beta-1b is effective in relapsing-remitting multiple sclerosis. Clinical results of a multicenter, randomized, double-blind, placebo-controlled trial. Neurology 1993, 43, 655–661. [Google Scholar] [CrossRef]
- Vermersch, P.; De Sèze, J.; Stojkovic, T.; Hautecoeur, P.; G-SEP (Groupe Septentrional d’Etudes et de Recherches sur la SEP). Interferon β1a (Avonex®) treatment in multiple sclerosis: Similarity of effect on progression of disability in patients with mild and moderate disability. J. Neurol. 2002, 249, 184–187. [Google Scholar] [CrossRef]
- Bayas, A.; Rieckmann, P. Managing the Adverse Effects of Interferon-?? Therapy in Multiple Sclerosis. Drug Saf. 2000, 22, 149–159. [Google Scholar] [CrossRef]
- Panitch, H.S.; Goodin, D.S.; Francis, G.; Chang, P.; Coyle, P.; O’Connor, P.; Monaghan, E.; Li, D.; Weinshenker, B.G. Randomized, comparative study of interferon-1a treatment regimens in MS: The EVIDENCE Trial. Neurology 2002, 59, 1496–1506. [Google Scholar] [CrossRef]
- Inácio, P.; Cavaco, A.; Airaksinen, M. The value of patient reporting to the pharmacovigilance system: A systematic review. Br. J. Clin. Pharmacol. 2017, 83, 227–246. [Google Scholar] [CrossRef]
- European Medicine Agency. Guideline on Good Pharmacovigilance Practices (GVP). Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-good-pharmacovigilance-practices-annex-i-definitions-rev-4_en.pdf (accessed on 20 August 2020).


{kind=link}
| All ICSRs (n = 272) | ALE (n = 11) | CLA (n = 7) | DMF (n = 41) | FIN (n = 62) | GLA (n = 27) | IFN Beta 1a (n = 41) | IFN Beta 1b (n = 5) | NAT (n = 21) | OCR (n = 25) | PegIFN Beta 1a (n = 13) | TER (n = 19) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median Age (IQR) | 42 (30–50) | 39 (27–52) | 27 (21–39) | 37 (28.5–48.5) | 46 (35–53) | 43 (37–50.75) | 40 (24.5–47.5) | 54 (48–63.5) | 31 (23–45) | 42 (34–59.5) | 47 (27.5–58.5) | 50 (37–60) |
| Sex | ||||||||||||
| Female | 184 (67.7) | 9 (82) | 5 (71) | 30 (73) | 39 (63) | 18 (67) | 31 (76) | 1 (20) | 15 (71) | 12 (48) | 10 (77) | 14 (74) |
| Male | 86 (31.6) | 2 (18) | 2 (29) | 11 (27) | 23 (37) | 9 (33) | 9 (22) | 4 (80) | 6 (29) | 13 (52) | 2 (15) | 5 (26) |
| NA | 2 (0.7) | - | - | - | - | - | 1 (2) | - | - | - | 1 (8) | - |
| Seriousness | ||||||||||||
| Not serious | 138 (50.7) | 3 (27) | 3 (43) | 25 (61) | 26 (42) | 14 (52) | 24 (59) | 4 (80) | 8 (38) | 14 (56) | 8 (62) | 9 (47) |
| Serious | 134 (49.3) | 8 (73) | 4 (57) | 16 (39) | 36 (58) | 13 (48) | 17 (41) | 1 (20) | 13 (62) | 11 (44) | 5 (38) | 10 (53) |
| Outcome | ||||||||||||
| Favorable | 166 (61) | 6 (55) | 2 (29) | 21 (51) | 28 (45.2) | 21 (77.8) | 29 (70.7) | 5 (100) | 13 (62) | 18 (72) | 10 (77) | 13 (68) |
| Unfavorable | 57 (21) | 5 (45) | 1 (14) | 9 (22) | 17 (27.4) | 5 (18.5) | 8 (19.5) | - | 5 (24) | 4 (16) | - | 3 (16) |
| NA | 49 (18) | - | 4 (57) | 11 (27) | 17 (27.4) | 1 (3.7) | 4 (9.8) | - | 3 (14) | 3 (12) | 3 (23) | 3 (16) |
| N. Suspected Drugs Other Than MS Drugs | ||||||||||||
| 0 | 269 (99) | 11 (100) | 7 (100) | 41 (100) | 62 (100) | 26 (96.3) | 42 (100) | 5 (100) | 21 (100) | 25 (100) | 13 (100) | 17 (89) |
| 1 | 3 (1) | - | - | - | - | 1 (3.7) | - | - | - | - | - | 2 (11) |
| N. Concomitant Drugs | ||||||||||||
| 0 | 186 (68.4) | 10 (91) | 4 (57) | 23 (56) | 42 (68) | 21 (77.8) | 30 (73.1) | 3 (60) | 16 (76) | 15 (60) | 9 (69.2) | 13 (68) |
| 1 | 40 (14.7) | - | - | 11 (27) | 10 (16) | 4 (14.8) | 4 (9.8) | - | 4 (19) | 3 (12) | 2 (15.4) | 2 (11) |
| 2 | 20 (7.4) | 1 (9) | 2 (29) | 3 (7.3) | 5 (8) | 1 (3.7) | 2 (4.9) | 1 (20) | 1 (5) | - | 2 (15.4) | 2 (11) |
| 3 | 9 (3.3) | - | - | 1 (2.4) | 1 (1.6) | - | 2 (4.9) | 1 (20) | - | 3 (12) | - | 1 (5) |
| 4 | 9 (3.3) | - | - | 3 (7.3) | 1 (1.6) | - | 3 (7.3) | - | - | 2 (8) | - | - |
| ≥5 | 8 (2.9) | - | 1 (14) | - | 3 (4.8) | 1 (3.7) | - | - | - | 2 (8) | - | 1 (5) |
| Case No. | Age | Sex | Outcome | PT | Suspected Drug 1 | Suspected Drug 2 | Concomitant Medications | Causality Assessment |
|---|---|---|---|---|---|---|---|---|
| 1 | 0 | M | Death | Preterm birth | Natalizumab | - | - | Possible |
| 2 | 0 | F | Death | Preterm birth | Glatiramer acetate | Methylprednisolone | - | Possible |
| 3 | 53 | M | Death | Respiratory distress | Ocrelizumab | - | - | Possible |
| 4 | 42 | F | Unchanged | Bacterial meningitis, bacterial pneumonitis | Alemtuzumab | - | - | Possible |
| 5 | 68 | M | Improved | Generalized tonic–clonic seizure, autoimmune encephalitis | Alemtuzumab | - | - | Possible |
| 6 | 48 | M | Unchanged | Limbic encephalitis | Fingolimod | - | Tamsulosin | Possible |
| System Organ Class | DMF (n = 53; 100%) | FIN (n = 80; 100%) | IFN Beta 1a (n = 54; 100%) |
|---|---|---|---|
| Blood and Lymphatic System Disorders n. (%) | 17 (32.1) | 12 (15) | 11 (20) |
| Anemia | - | - | 1 |
| Leukocytosis | 1 | - | - |
| Leucopenia | 1 | 4 | 5 |
| Lymphocytopenia | 12 | 8 | 1 |
| Neutrophilia | 1 | - | - |
| Neutropenia | - | - | 3 |
| Thrombocytopenia | 2 | - | 1 |
| General Disorders and Administration site Conditions n. (%) | 1 (1.9) | 3 (3.75) | 24 (44) |
| Flu-like symptoms | 1 | - | 16 |
| Asthenia | - | 1 | 1 |
| Cyst | - | 1 | - |
| Wheezing | - | 1 | - |
| Pyrexia | - | - | 2 |
| Loss of response | 1 | ||
| Injection site reaction | - | - | 4 |
| Infections and Infestations n. (%) | 4 (7.5) | 15 (18.75) | 2 (4) |
| Sepsis | 1 | - | - |
| Spondylodiscitis | 1 | 1 | - |
| Rhinitis | 1 | - | - |
| Herpes zoster infection | 1 | 5 | - |
| Bronchitis | - | 1 | - |
| Cystitis | - | 4 | - |
| Encephalitis | - | 1 | - |
| Molluscum contagious | - | 2 | - |
| Pneumonitis | 1 | - | |
| Broncho-pneumonitis | - | - | 1 |
| Cutaneous abscess | - | - | 1 |
| Neoplasms Benign, Malignant and Unspecified n. (%) | 1 (1.9) | 17 (21.25) | 3 (6) |
| Lymphoma | 1 | - | - |
| Lung cancer | - | 1 | - |
| Breast cancer | - | 3 | - |
| Ovarian cancer | - | 1 | - |
| Thyroid cancer | - | 1 | - |
| Epithelioma | - | 1 | - |
| Melanoma | - | 3 | 1 |
| Metastatic gallbladder cancer | - | 1 | - |
| Myomas | - | 1 | - |
| Mouth cancer | - | 1 | - |
| Melanocytic nevus | - | 2 | - |
| Dysplastic nevus | - | 1 | - |
| Anal warts | - | 1 | - |
| Colorectal cancer | - | - | 1 |
| Nodular fasciitis | - | - | 1 |
| Investigations n. (%) | 1 (1.9) | 12 (15) | 3 (6) |
| Increase in transaminases | 1 | 1 | 3 |
| ALT elevation | - | 2 | - |
| GGT elevation | - | 6 | - |
| Cholesterol elevation | - | 1 | - |
| GPT elevation | - | 2 | - |
| Gastrointestinal Disorders n. (%) | 11 (20.8) | 2 (2.5) | 1 (2) |
| Heartburn | 7 | - | - |
| Dysphagia | 1 | - | - |
| Diarrhea | 2 | - | - |
| Unspecified gastrointestinal disorder | 1 | - | - |
| Pancreatic insufficiency | 1 | - | |
| Nausea | 1 | - | |
| Oral lesion | - | - | 1 |
| Skin and Subcutaneous Tissue Disorders n. (%) | 6 (11.3) | 1 (1.25) | 5 (9) |
| Eczema | 2 | - | - |
| Skin eruption | 2 | - | - |
| Facial redness | 2 | - | - |
| Skin lesion | - | 1 | - |
| Sweating | - | - | 1 |
| Measles rash | - | - | 1 |
| Hair thinning | - | - | 1 |
| Skin induration | - | - | 1 |
| Skin pigmentation | - | - | 1 |
| Other SOCs n. (%) | 12 (22.6) | 18 (22.5) | 5 (9) |
| Congenital, familial and genetic disorders | 1 | - | - |
| Hepatobiliary disorders | 1 | 3 | 2 |
| Injury, poisoning and procedural complications | 2 | 2 | - |
| Renal and urinary disorders | 1 | - | - |
| Vascular disorders | 3 | - | - |
| Respiratory, thoracic and mediastinal disorders | 4 | 2 | - |
| Cardiac disorders | - | 2 | - |
| Eye disorders | - | 3 | - |
| Nervous system disorders | - | 6 | 1 |
| Endocrine disorders | - | - | 1 |
| Pregnancy, puerperium and perinatal conditions | - | - | 1 |
| Median and Range of TTE by SOCs and Suspected Drugs | Dimethyl Fumarate | Fingolimod | IFN Beta 1a |
|---|---|---|---|
| Blood and Lymphatic System Disorders Median (IQR) Range | 224 (145–621.5) 145–1629 | 1227 (500–1529.75) 74–2575 | 1518 (223–2860) 68–3061 |
| General Disorders and Administration Site Conditions Median (IQR) Range | - | 70 (0–679) 0–679 | 188 (0.25–4900) 0–706 |
| Infections and Infestations Median (IQR) Range | 943 (139.75–1598.75) 0–1689 | 1486.5 (769.25–2609.75) 212–3585 | - |
| Neoplasms Benign, Malignant and Unspecified Median (IQR) Range | - | 1589.5 (1040.75–2366) 464–2745 | 3681 (2760–3697) 2760–3697 |
| Investigations Median (IQR) Range | - | 1396 (116.75–2197.75) 64–2474 | - |
| Gastrointestinal Disorders Median (IQR) Range | 92 (33–646) 7–1460 | - | - |
| Skin and Subcutaneous Tissue Disorders Median (IQR) Range | 679 (145.25–1091) 122–1430 | - | 72 (0–583.5) 0–979 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maniscalco, G.T.; Brescia Morra, V.; Florio, C.; Lus, G.; Tedeschi, G.; Cianfrani, M.; Docimo, R.; Miniello, S.; Romano, F.; Sinisi, L.; et al. Preliminary Results of the FASM Study, an On-Going Italian Active Pharmacovigilance Project. Pharmaceuticals 2020, 13, 466. https://doi.org/10.3390/ph13120466
Maniscalco GT, Brescia Morra V, Florio C, Lus G, Tedeschi G, Cianfrani M, Docimo R, Miniello S, Romano F, Sinisi L, et al. Preliminary Results of the FASM Study, an On-Going Italian Active Pharmacovigilance Project. Pharmaceuticals. 2020; 13(12):466. https://doi.org/10.3390/ph13120466
Chicago/Turabian StyleManiscalco, Giorgia Teresa, Vincenzo Brescia Morra, Ciro Florio, Giacomo Lus, Gioacchino Tedeschi, Maddalena Cianfrani, Renato Docimo, Stefania Miniello, Felice Romano, Leonardo Sinisi, and et al. 2020. "Preliminary Results of the FASM Study, an On-Going Italian Active Pharmacovigilance Project" Pharmaceuticals 13, no. 12: 466. https://doi.org/10.3390/ph13120466
APA StyleManiscalco, G. T., Brescia Morra, V., Florio, C., Lus, G., Tedeschi, G., Cianfrani, M., Docimo, R., Miniello, S., Romano, F., Sinisi, L., Spitaleri, D. L. A., Longo, G., Trama, U., Triassi, M., FASM Group, Scavone, C., & Capuano, A. (2020). Preliminary Results of the FASM Study, an On-Going Italian Active Pharmacovigilance Project. Pharmaceuticals, 13(12), 466. https://doi.org/10.3390/ph13120466