


Wearable Devices for Arrhythmia Detection: Advancements and Clinical Implications

 , , , , , , and
, , , , , , and
Abstract
1. Introduction
1.1. Overview of Arrhythmias and Need for Continuous Monitoring
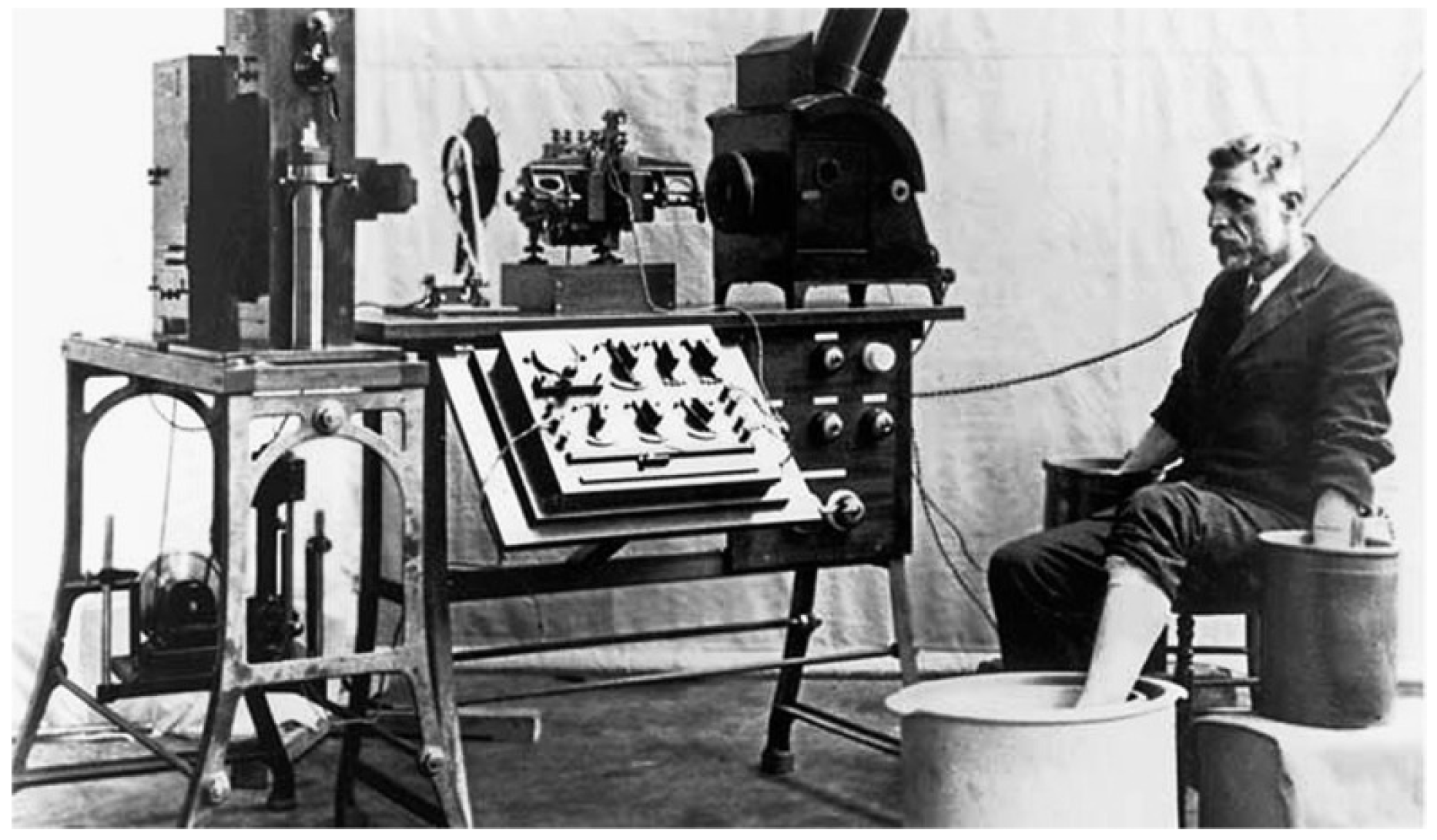
1.2. History and Development of ECG
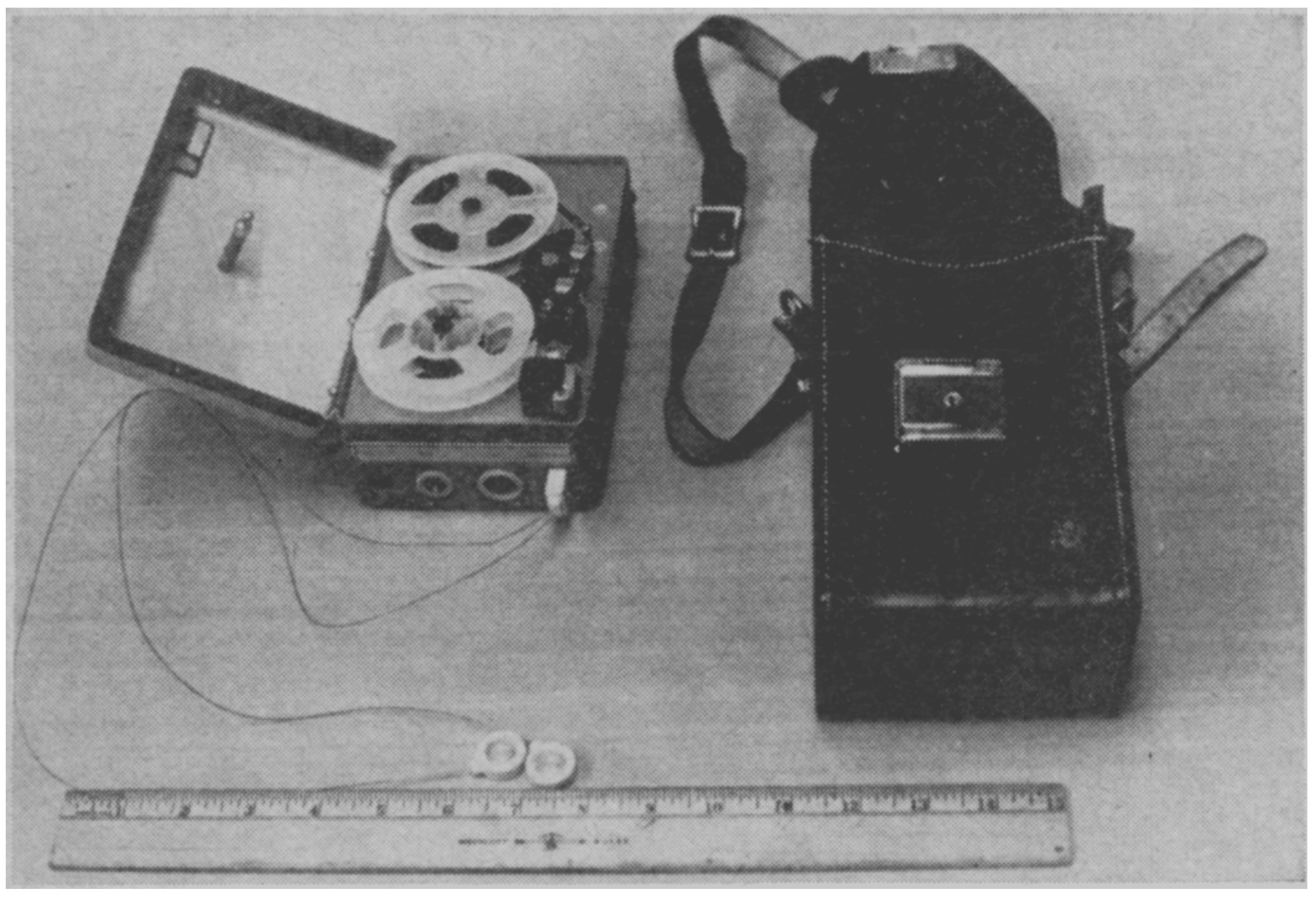
1.3. Development of Continuous Monitoring Device: Holter Monitor
1.4. Advancements in Wearable Devices in Enhancing Arrhythmia Detection and Management
1.5. Objectives of This Review
2. Smartwatches
2.1. Introduction to Smartwatch
2.2. Smartwatch Technology
2.3. Comparative Analysis of PPG and ECG Technologies in Wearable Devices
2.4. Different Smartwatches and AF Detection
2.4.1. Apple Watch
2.4.2. Fitbit
2.4.3. Samsung Galaxy
2.4.4. Withings ScanWatch Horizon
2.4.5. Huawei Smartwatches
2.4.6. Garmin Smartwatches
2.4.7. Other Arrhythmia Detection
3. Smart Rings
3.1. Background
3.2. Advantages of Smart Rings
3.2.1. Stable Positioning and Skin Contact
3.2.2. Enhanced Signal Clarity
3.2.3. Continuous Health Monitoring
3.2.4. Compact and Comfortable
3.2.5. Blood Pressure Estimation
3.3. Disadvantages of Smart Rings
3.3.1. Limited Functionalities Compared to Smartwatches
3.3.2. No Built-In ECG for Some Models

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Smart Ring | FDA | CE | Cost | Subscription Fee | PPG | ECG | System Compatibility | Sizes | Average Battery Life |
|---|---|---|---|---|---|---|---|---|---|
| Oura Ring 4 [45] | ✕ | ✓ | GBP 349 | GBP 5.99/month | ✓ | ✕ | iOS and Android systems | 4–15, no half sizes | 7–8 days |
| Samsung Galaxy Ring [48] | ✕ | ✓ | GBP 399 | None | ✓ | ✕ | Android system only | 5–15, no half sizes | Up to 7 days |
| Ultrahuman Ring Air [49] | ✕ | ✓ | GBP 329 | None | ✓ | ✕ | iOS and Android systems | 5–14, no half-sizes | 4–6 days |
| Amazfit Helio Ring [50] | ✕ | ✓ | GBP269 | None | ✓ | ✕ | iOS and Android systems | 8, 10, and 12 sizes only | 1–3 days |
3.3.3. Battery Life and Charging
3.3.4. Comfort and Fit
4. Patch Monitors
4.1. Overview
4.2. Reliability
4.3. Performance
4.4. Feasibility
4.5. Cost
4.6. Additional Uses
4.7. Challenges
5. Smart Shirts
5.1. Clinical Evidence for Smart Shirts in Arrhythmia Detection
5.2. Advantages of Smart Shirts
5.3. Disadvantages of Smart Shirts
| Smart Shirt | FDA | CE | Cost | Parameters | Compatibility | Average Battery Life |
|---|---|---|---|---|---|---|
| Hexoskin Smart Shirt [126] | ✕ | ✓ | USD 249 | Cardiac (ECG, HR, HRV, and QRS events), respiratory, activity, and sleep data | iOS and Android Systems | 12–24 h |
| Cardioskin [127] | ✓ | ✓ | Not commercially available, intended for clinical use | 12-lead continuous ECG, HR, activity, and respiratory data | N/A | N/A |
| Athos Smart Shirt [128] | ✕ | ✕ | USD 398 | No ECG, targeted more towards activity and respiratory data. Measures muscle activity through EMG | iOS Systems only | 6–12 h |
- Traditional Rule-Based Algorithms were the first generation of detection systems used in early wearable monitors. These algorithms employ predefined thresholds and decision trees based on established electrophysiological parameters, such as RR interval variability, to detect arrhythmias. While computationally efficient and interpretable, their performance is limited by rigid decision boundaries that may not accommodate the physiological variability across different patient populations.
- Feature-Based Machine Learning approaches extract hand-crafted features from the cardiac signal (e.g., heart rate variability metrics, wavelet coefficients, spectral characteristics) and employ classifiers such as support vector machines or random forests. These algorithms offer an improved performance over rule-based systems, with Wasserlauf et al. (2019) reporting a sensitivity of 94.3% and specificity of 95.8% for AF detection in smartwatch data [29]. However, their effectiveness remains dependent on the quality of feature engineering and may not generalise well across different populations.
- Deep Learning Neural Networks represent the current state of the art in wearable arrhythmia detection. Hannun et al. (2019) demonstrated a deep neural network that could classify 12 rhythm classes from a single-lead ECG with a performance exceeding that of cardiologists [129]. Their network achieved an F1 score exceeding 0.80 for detecting AF, atrial flutter, and other arrhythmias, demonstrating the potential of these approaches for the automated interpretation of data from wearable monitors.
- Hybrid and Ensemble Systems combine multiple algorithmic approaches to improve robustness. These systems often employ a two-stage architecture: a computationally efficient algorithm for continuous screening and a more sophisticated algorithm for detailed analysis when irregularities are detected. Torres-Soto and Ashley (2020) demonstrated that multi-task deep learning approaches that simultaneously detect multiple cardiac abnormalities can improve performance by leveraging shared signal characteristics across different arrhythmias [130].
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fung, E.; Järvelin, M.-R.; Doshi, R.N.; Shinbane, J.S.; Carlson, S.K.; Grazette, L.P.; Chang, P.M.; Sangha, R.S.; Huikuri, H.V.; Peters, N.S. Electrocardiographic patch devices and contemporary wireless cardiac monitoring. Front. Physiol. 2015, 6, 149. [Google Scholar] [CrossRef] [PubMed]
- Yenikomshian, M.; Jarvis, J.; Patton, C.; Yee, C.; Mortimer, R.; Birnbaum, H.; Topash, M. Cardiac arrhythmia detection outcomes among patients monitored with the Zio patch system: A systematic literature review. Curr. Med. Res. Opin. 2019, 35, 1659–1670. [Google Scholar] [CrossRef] [PubMed]
- Antoun, I.; Aljabal, M.; Alkhayer, A.; Mahfoud, Y.; Alkhayer, A.; Simon, P.; Kotb, A.; Barker, J.; Mavilakandy, A.; Naseer, M.U. Atrial fibrillation inpatient management patterns and clinical outcomes during the conflict in Syria: An observational cohort study. Perfusion 2025, 40, 711–719. [Google Scholar] [CrossRef]
- Antoun, I.; Alkhayer, A.; Aljabal, M.; Mahfoud, Y.; Alkhayer, A.; Simon, P.; Kotb, A.; Barker, J.; Mavilakandy, A.; Hani, R. Thirty-day unplanned readmissions following hospitalization for atrial fibrillation in a tertiary Syrian center: A real-world observational cohort study. Heart Rhythm O2 2024, 5, 854–859. [Google Scholar] [CrossRef]
- Antoun, I.; Alkhayer, A.; Aljabal, M.; Mahfoud, Y.; Alkhayer, A.; Kotb, A.I.; Barker, J.; Somani, R.; Ng, G.A.; Zakkar, M. Incidence, outcomes, and predictors of new heart failure in syrian conflict-affected population following hospitalization for atrial fibrillation: A retrospective cohort study. Perfusion 2024, 02676591241283883. [Google Scholar] [CrossRef]
- Antoun, I.; Alkhayer, A.; Eldin, A.J.; Alkhayer, A.; Yazji, K.; Somani, R.; Ng, G.A.; Zakkar, M. Gender disparity in quality of life in patients with atrial fibrillation during the Syrian conflict: An observational cohort study. Heart Rhythm O2 2025, 6, 362–367. [Google Scholar] [CrossRef]
- Antoun, I.; Alkhayer, A.; Alkhayer, A.; Yazji, K.; Somani, R.; Ng, G.A.; Zakkar, M. Six-Month Emergent Readmissions Following Hospitalization for Atrial Fibrillation Amid the Syrian Conflict: A Real-World Observational Cohort Study. J. Cardiovasc. Electrophysiol. 2025, 36, 582–588. [Google Scholar] [CrossRef]
- Antoun, I.; Alkhayer, A.; Eldin, A.J.; Alkhayer, A.; Yazji, K.; Somani, R.; André Ng, G.; Zakkar, M. The Prevalence and Predictors of Atrioventricular Blocks in Syrian Patients Reporting to the Emergency Department During the Ongoing Conflict: A Cross-Sectional Study. J. Cardiovasc. Electrophysiol. 2025, 36, 576–581. [Google Scholar] [CrossRef]
- Antoun, I.; Alkhayer, A.; Eldin, A.J.; Alkhayer, A.; Yazji, K.; Somani, R.; Ng, G.A.; Zakkar, M. Gender Disparity in Oral Anticoagulation Therapy in Hospitalised Patients with Atrial Fibrillation During the Ongoing Syrian Conflict: Unbalanced Treatment in Turbulent Times. J. Clin. Med. 2025, 14, 1173. [Google Scholar] [CrossRef]
- Chugh, S.S.; Havmoeller, R.; Narayanan, K.; Singh, D.; Rienstra, M.; Benjamin, E.J.; Gillum, R.F.; Kim, Y.-H.; McAnulty, J.H.; Zheng, Z.-J.; et al. Worldwide Epidemiology of Atrial Fibrillation: A Global Burden of Disease 2010 Study. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef]
- Surawicz, B.; Knilans, T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric; Elsevier Health Sciences: Amsterdam, The Netherlands, 2008. [Google Scholar]
- Einthoven, W. The different forms of the human electrocardiogram and their signification. Lancet 1912, 179, 853–861. [Google Scholar] [CrossRef]
- AlGhatrif, M.; Lindsay, J. A brief review: History to understand fundamentals of electrocardiography. J. Community Hosp. Intern. Med. Perspect. 2012, 2, 14383. [Google Scholar] [CrossRef] [PubMed]
- Sivakumaran, S.; Krahn, A.D.; Klein, G.J.; Finan, J.; Yee, R.; Renner, S.; Skanes, A.C. A prospective randomized comparison of loop recorders versus Holter monitors in patients with syncope or presyncope. Am. J. Med. 2003, 115, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Reynolds, K.; Yang, J.; Gupta, N.; Lenane, J.; Sung, S.H.; Harrison, T.N.; Liu, T.I.; Solomon, M.D. Association of Burden of Atrial Fibrillation With Risk of Ischemic Stroke in Adults with Paroxysmal Atrial Fibrillation: The KP-RHYTHM Study. JAMA Cardiol. 2018, 3, 601. [Google Scholar] [CrossRef]
- Holter, N.J. New Method for Heart Studies. Science 1961, 134, 1214–1220. [Google Scholar] [CrossRef]
- Krasnow, A.Z.; Bloomfield, D.K. Artifacts in portable electrocardiographic monitoring. Am. Heart J. 1976, 91, 349–357. [Google Scholar] [CrossRef]
- Kennedy, H.L. The history, science, and innovation of Holter technology. Ann. Noninvasive Electrocardiol. 2006, 11, 85–94. [Google Scholar] [CrossRef]
- Barrett, P.M.; Komatireddy, R.; Haaser, S.; Topol, S.; Sheard, J.; Encinas, J.; Fought, A.J.; Topol, E.J. Comparison of 24-hour Holter monitoring with 14-day novel adhesive patch electrocardiographic monitoring. Am. J. Med. 2014, 127, 95.e11–95.e17. [Google Scholar] [CrossRef]
- Rosenberg, M.A.; Samuel, M.; Thosani, A.; Zimetbaum, P.J. Use of a noninvasive continuous monitoring device in the management of atrial fibrillation: A pilot study. Pacing Clin. Electrophysiol. 2013, 36, 328–333. [Google Scholar] [CrossRef]
- Cheung, C.C.; Krahn, A.D.; Andrade, J.G. The Emerging Role of Wearable Technologies in Detection of Arrhythmia. Can. J. Cardiol. 2018, 34, 1083–1087. [Google Scholar] [CrossRef]
- Global Smart Watch Market Report (2021 to 2030)—COVID-19 Growth and Change—ResearchAndMarkets.com. Available online: https://www.businesswire.com/news/home/20210526005524/en/Global-Smart-Watch-Market-Report-2021-to-2030---COVID-19-Growth-and-Change---ResearchAndMarkets.com-4 (accessed on 7 February 2025).
- Joglar, J.A.; Chung, M.K.; Armbruster, A.L.; Benjamin, E.J.; Chyou, J.Y.; Cronin, E.M.; Deswal, A.; Eckhardt, L.L.; Goldberger, Z.D.; Gopinathannair, R.; et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2024, 83, 109–279. [Google Scholar] [CrossRef]
- Dilaveris, P.E.; Antoniou, C.K.; Caiani, E.G.; Casado-Arroyo, R.; Climent, A.Μ.; Cluitmans, M.; Cowie, M.R.; Doehner, W.; Guerra, F.; Jensen, M.T.; et al. ESC Working Group on e-Cardiology Position Paper: Accuracy and reliability of electrocardiogram monitoring in the detection of atrial fibrillation in cryptogenic stroke patients. Eur. Heart J. Digit. Health 2022, 3, 341–358. [Google Scholar] [CrossRef] [PubMed]
- Ghamari, M. A review on wearable photoplethysmography sensors and their potential future applications in health care. Int. J. Biosens. Bioelectron. 2018, 4, 195. [Google Scholar] [CrossRef] [PubMed]
- Pay, L. Arrhythmias Beyond Atrial Fibrillation Detection Using Smartwatches: A Systematic Review. Anatol. J. Cardiol. 2023, 27, 126–131. [Google Scholar] [CrossRef]
- Pereira, T.; Tran, N.; Gadhoumi, K.; Pelter, M.M.; Do, D.H.; Lee, R.J.; Colorado, R.; Meisel, K.; Hu, X. Photoplethysmography based atrial fibrillation detection: A review. NPJ Digit. Med. 2020, 3, 3. [Google Scholar] [CrossRef]
- Tison, G.H.; Sanchez, J.M.; Ballinger, B.; Singh, A.; Olgin, J.E.; Pletcher, M.J.; Vittinghoff, E.; Lee, E.S.; Fan, S.M.; Gladstone, R.A.; et al. Passive Detection of Atrial Fibrillation Using a Commercially Available Smartwatch. JAMA Cardiol. 2018, 3, 409–416. [Google Scholar] [CrossRef]
- Wasserlauf, J.; You, C.; Patel, R.; Valys, A.; Albert, D.; Passman, R. Smartwatch Performance for the Detection and Quantification of Atrial Fibrillation. Circ. Arrhythmia Electrophysiol. 2019, 12, e006834. [Google Scholar] [CrossRef]
- Nazarian, S.; Lam, K.; Darzi, A.; Ashrafian, H. Diagnostic Accuracy of Smartwatches for the Detection of Cardiac Arrhythmia: Systematic Review and Meta-analysis. J. Med. Internet Res. 2021, 23, e28974. [Google Scholar] [CrossRef]
- Van Der Zande, J.; Strik, M.; Dubois, R.; Ploux, S.; Alrub, S.A.; Caillol, T.; Nasarre, M.; Donker, D.W.; Oppersma, E.; Bordachar, P. Using a Smartwatch to Record Precordial Electrocardiograms: A Validation Study. Sensors 2023, 23, 2555. [Google Scholar] [CrossRef]
- Perez, M.V.; Mahaffey, K.W.; Hedlin, H.; Rumsfeld, J.S.; Garcia, A.; Ferris, T.; Balasubramanian, V.; Russo, A.M.; Rajmane, A.; Cheung, L.; et al. Large-Scale Assessment of a Smartwatch to Identify Atrial Fibrillation. N. Engl. J. Med. 2019, 381, 1909–1917. [Google Scholar] [CrossRef]
- Lubitz, S.A.; Faranesh, A.Z.; Selvaggi, C.; Atlas, S.J.; McManus, D.D.; Singer, D.E.; Pagoto, S.; McConnell, M.V.; Pantelopoulos, A.; Foulkes, A.S. Detection of Atrial Fibrillation in a Large Population Using Wearable Devices: The Fitbit Heart Study. Circulation 2022, 146, 1415–1424. [Google Scholar] [CrossRef] [PubMed]
- Abu-Alrub, S.; Strik, M.; Ramirez, F.D.; Moussaoui, N.; Racine, H.P.; Marchand, H.; Buliard, S.; Haïssaguerre, M.; Ploux, S.; Bordachar, P. Smartwatch Electrocardiograms for Automated and Manual Diagnosis of Atrial Fibrillation: A Comparative Analysis of Three Models. Front. Cardiovasc. Med. 2022, 9, 836375. [Google Scholar] [CrossRef] [PubMed]
- Campo, D.; Elie, V.; De Gallard, T.; Bartet, P.; Morichau-Beauchant, T.; Genain, N.; Fayol, A.; Fouassier, D.; Pasteur-Rousseau, A.; Puymirat, E.; et al. Atrial Fibrillation Detection With an Analog Smartwatch: Prospective Clinical Study and Algorithm Validation. JMIR Form. Res. 2022, 6, e37280. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Wang, H.; Zhang, H.; Liu, T.; Liang, Z.; Xia, Y.; Yan, L.; Xing, Y.; Shi, H.; Li, S.; et al. Mobile Photoplethysmographic Technology to Detect Atrial Fibrillation. J. Am. Coll. Cardiol. 2019, 74, 2365–2375. [Google Scholar] [CrossRef]
- Chang, P.-C.; Wen, M.-S.; Chou, C.-C.; Wang, C.-C.; Hung, K.-C. Atrial fibrillation detection using ambulatory smartwatch photoplethysmography and validation with simultaneous holter recording. Am. Heart J. 2022, 247, 55–62. [Google Scholar] [CrossRef]
- Antoun, I.; Layton, G.R.; Abdelrazik, A.; Eldesouky, M.; Zakkar, M.; Somani, R.; Ng, A. The Pathophysiology of Sex Differences in Stroke Risk and Prevention in Atrial Fibrillation: A Comprehensive Review. Medicina 2025, 61, 649. [Google Scholar] [CrossRef]
- Ploux, S.; Strik, M.; Caillol, T.; Ramirez, F.D.; Abu-Alrub, S.; Marchand, H.; Buliard, S.; Haïssaguerre, M.; Bordachar, P. Beyond the wrist: Using a smartwatch electrocardiogram to detect electrocardiographic abnormalities. Arch. Cardiovasc. Dis. 2022, 115, 29–36. [Google Scholar] [CrossRef]
- Caillol, T.; Strik, M.; Ramirez, F.D.; Abu-Alrub, S.; Marchand, H.; Buliard, S.; Welte, N.; Ploux, S.; Haïssaguerre, M.; Bordachar, P. Accuracy of a Smartwatch-Derived ECG for Diagnosing Bradyarrhythmias, Tachyarrhythmias, and Cardiac Ischemia. Circ. Arrhythmia Electrophysiol. 2021, 14, e009260. [Google Scholar] [CrossRef]
- Hwang, J.; Kim, J.; Choi, K.-J.; Cho, M.S.; Nam, G.-B.; Kim, Y.-H. Assessing Accuracy of Wrist-Worn Wearable Devices in Measurement of Paroxysmal Supraventricular Tachycardia Heart Rate. Korean Circ. J. 2019, 49, 437. [Google Scholar] [CrossRef]
- Bogár, B.; Pető, D.; Sipos, D.; Füredi, G.; Keszthelyi, A.; Betlehem, J.; Pandur, A.A. Detection of Arrhythmias Using Smartwatches—A Systematic Literature Review. Healthcare 2024, 12, 892. [Google Scholar] [CrossRef]
- Boo-Ho, Y.; Sokwoo, R.; Asada, H.H. A twenty-four hour tele-nursing system using a ring sensor. In Proceedings of the 1998 IEEE International Conference on Robotics and Automation (Cat. No.98CH36146), Leuven, Belgium, 20 May 1998; Volume 381, pp. 387–392. [Google Scholar]
- Wang, M.; Chen, C.; Wu, H.; Zhang, J.; Zhou, S.; Wang, G. Will Smart Ring be Next Wave of Wearables? In Proceedings of the 2024 IEEE Biomedical Circuits and Systems Conference (BioCAS), Xi’an, China, 24–26 October 2024; pp. 1–5. [Google Scholar]
- OURA. Oura Ring 4. Available online: https://support.ouraring.com/hc/en-us/articles/33045011508115-Oura-Ring-4 (accessed on 7 February 2025).
- Wang, M.; Atef, M.; Xie, Q.; Lian, Y.; Wang, G. Live demonstration: A ring-type blood pressure monitoring system based on photoplesthygraphy. In Proceedings of the 2017 IEEE Biomedical Circuits and Systems Conference (BioCAS), Turin, Italy, 19–21 October 2017. [Google Scholar]
- Briosa E Gala, A.; Sharp, A.J.; Schramm, D.; Ries, W.; Pope, M.T.B.; Leo, M.; Paisey, J.; Curzen, N.; Betts, T.R. Automated atrial fibrillation detection with a smartwatch and smart-ring in individuals with cardiovascular disease. EP Eur. 2023, 25, euad122.618. [Google Scholar] [CrossRef]
- Samsung. Galaxy Ring. Available online: https://www.samsung.com/uk/rings/galaxy-ring/galaxy-ring-titanium-black-size-5-sm-q505nzkaeub/?cid=UK_PPC_1294187870_ID~GLB0005Q64_CN~Galaxy+Ring_BS~mx_PR~ring_SB~wearoth_PH~on_KS~bap_MK~gb_OB~conv_FS~hobl_FF~-&gad_source=1&gclid=CjwKCAiAh6y9BhBREiwApBLHCwvuqh7G74ceF7AWFDMiKfcJGP3fk_bBrasfjvVCl_xtLY9g5aDYMBoCwRAQAvD_BwE&gclsrc=aw.ds (accessed on 7 February 2025).
- Ultrahuman. Ultrahuman Ring AIR. Available online: https://www.ultrahuman.com/ (accessed on 7 February 2025).
- Amazfit. Amazfit Helio Ring. Available online: https://uk.amazfit.com/products/amazfit-helio-ring (accessed on 7 February 2025).
- Hermans, A.N.L.; Gawalko, M.; Dohmen, L.; Van Der Velden, R.M.J.; Betz, K.; Duncker, D.; Verhaert, D.V.M.; Heidbuchel, H.; Svennberg, E.; Neubeck, L.; et al. Mobile health solutions for atrial fibrillation detection and management: A systematic review. Clin. Res. Cardiol. 2022, 111, 479–491. [Google Scholar] [CrossRef] [PubMed]
- Duncker, D.; Ding, W.Y.; Etheridge, S.; Noseworthy, P.A.; Veltmann, C.; Yao, X.; Bunch, T.J.; Gupta, D. Smart Wearables for Cardiac Monitoring—Real-World Use beyond Atrial Fibrillation. Sensors 2021, 21, 2539. [Google Scholar] [CrossRef]
- Ho, J.S.; Ho, E.S.; Yeo, L.L.; Kong, W.K.; Li, T.Y.; Tan, B.Y.; Chan, M.Y.; Sharma, V.K.; Poh, K.-K.; Sia, C.-H. Use of wearable technology in cardiac monitoring after cryptogenic stroke or embolic stroke of undetermined source: A systematic review. Singap. Med. J. 2024, 65, 370–379. [Google Scholar] [CrossRef]
- Sajeev, J.K.; Koshy, A.N.; Teh, A.W. Wearable devices for cardiac arrhythmia detection: A new contender? Intern. Med. J. 2019, 49, 570–573. [Google Scholar] [CrossRef]
- Koshy, A.N.; Sajeev, J.K.; Negishi, K.; Wong, M.C.; Pham, C.B.; Cooray, S.P.; Khavar, Y.; Roberts, L.; Cooke, J.C.; Teh, A.W. Accuracy of blinded clinician interpretation of single-lead smartphone electrocardiograms and a proposed clinical workflow. Am. Heart J. 2018, 205, 149–153. [Google Scholar] [CrossRef]
- Hilbel, T.; Frey, N. Review of current ECG consumer electronics (pros and cons). J. Electrocardiol. 2023, 77, 23–28. [Google Scholar] [CrossRef]
- Manninger, M.; Kosiuk, J.; Zweiker, D.; Njeim, M.; Antolic, B.; Kircanski, B.; Larsen, J.M.; Svennberg, E.; Vanduynhoven, P.; Duncker, D. Role of wearable rhythm recordings in clinical decision making—The wEHRAbles project. Clin. Cardiol. 2020, 43, 1032–1039. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Zio XT for Detecting Cardiac Arrhythmias; MTG52; National Institute for Health and Care Excellence: London, UK, 2020. [Google Scholar]
- Zio® by iRhythm UK—Uninterrupted Cardiac Monitoring Service. Available online: https://irhythmtech.co.uk/ (accessed on 7 October 2024).
- Mezoo Co., Ltd. Available online: https://me-zoo.com/main/html.php?htmid=products/hicardisystem.html (accessed on 7 October 2024).
- SmartCardia. SmartCardia: 7-Lead ECG Patch for Remote Monitoring. Available online: https://www.smartcardia.com/ (accessed on 7 October 2024).
- Jewel Wearable Defibrillator Element Science. Available online: https://elementscience.com/product/ (accessed on 28 September 2023).
- EinarNilsen. ECG247. Available online: https://ecg247.com/en/ (accessed on 27 November 2024).
- Biomedical, S. Asia No.1 Arrhythmia Diagnostic Solution. Available online: https://www.sigknow.com/en/ezypro/ (accessed on 7 October 2024).
- FIRSTBEAT BODYGUARD 2 Round-the-Clock Heartbeat Monitoring; Firstbeat Technologies Oy: Jyväskylä, Finland; p. 2. Available online: https://www.firstbeat.com/wp-content/uploads/2015/09/Bodyguard-2-Brochure.pdf (accessed on 27 April 2025).
- Imec Embracing a Better Life Kapeldreef 75•3001 Leuven•Belgium: Imec. Available online: https://www.imec-int.com/sites/default/files/imported/HEALTH%2520PATCH.pdf (accessed on 27 November 2024).
- Cardiac Insight, Inc. Cardea SOLO System. Available online: https://www.cardiacinsightinc.com/cardea-solo/for-providers/ (accessed on 7 October 2024).
- Telemetry PMC. Philips Mobile Cardiac Telemetry—MCOT—My Heart Monitor. Available online: https://www.myheartmonitor.com/device/mcot-patch/ (accessed on 7 October 2024).
- SEERS. Mobicare. Available online: https://seerstech.com/lang_en/mobicare.php (accessed on 7 October 2024).
- MEMO. Memo Official Website. Available online: https://huinno.com/en (accessed on 7 October 2024).
- Acquisition SEWFC-FDE. Spyder ECG Solution. Available online: https://www.spyderecg.com/ (accessed on 7 November 2024).
- ATsens. Available online: https://www.atsens.com/en/ (accessed on 7 November 2024).
- VitalConnect. Available online: https://vitalconnect.com/ (accessed on 7 November 2024).
- CardioSTAT. Ambulatory Cardiac Monitoring Simplified|CardioSTAT. Available online: https://www.cardiostat.com/uki/home (accessed on 7 November 2024).
- S-Patch Cardio|Healthcare Solution|Samsung SDS|Europe. Available online: https://www.samsungsds.com/eu/cardio/cardio.html (accessed on 7 November 2024).
- Patients BMRCM-F. Available online: https://www.cdx.bostonscientific.com/us/en/patients/cardiac-monitor/bodyguardian-mini.html (accessed on 7 November 2024).
- Monitor PEHeMH. Available online: https://www.philips.co.uk/healthcare/resources/landing/epatch (accessed on 7 November 2024).
- Lown, M.; Yue, A.M.; Shah, B.N.; Corbett, S.J.; Lewith, G.; Stuart, B.; Garrard, J.; Brown, M.; Little, P.; Moore, M. Screening for Atrial Fibrillation Using Economical and Accurate Technology (From the SAFETY Study). Am. J. Cardiol. 2018, 122, 1339–1344. [Google Scholar] [CrossRef]
- Campero Jurado, I.; Lorato, I.; Morales, J.; Fruytier, L.; Stuart, S.; Panditha, P.; Janssen, D.M.; Rossetti, N.; Uzunbajakava, N.; Serban, I.B.; et al. Signal Quality Analysis for Long-Term ECG Monitoring Using a Health Patch in Cardiac Patients. Sensors 2023, 23, 2130. [Google Scholar] [CrossRef]
- Jortveit, J.; Boskovic, M.; Sandberg, E.L.; Vegsundvåg, J.; Halvorsen, S. High Diagnostic Accuracy of Long-Term Electrocardiogram Interpretation by General Practitioners. Int. J. Telemed. Appl. 2024, 2024, 6624344. [Google Scholar] [CrossRef] [PubMed]
- Steinhubl, S.R.; Waalen, J.; Edwards, A.M.; Ariniello, L.M.; Mehta, R.R.; Ebner, G.S.; Carter, C.; Baca-Motes, K.; Felicione, E.; Sarich, T.; et al. Effect of a Home-Based Wearable Continuous ECG Monitoring Patch on Detection of Undiagnosed Atrial Fibrillation: The mSToPS Randomized Clinical Trial. JAMA 2018, 320, 146. [Google Scholar] [CrossRef] [PubMed]
- Gladstone, D.J.; Wachter, R.; Schmalstieg-Bahr, K.; Quinn, F.R.; Hummers, E.; Ivers, N.; Marsden, T.; Thornton, A.; Djuric, A.; Suerbaum, J.; et al. Screening for Atrial Fibrillation in the Older Population: A Randomized Clinical Trial. JAMA Cardiol. 2021, 6, 558. [Google Scholar] [CrossRef] [PubMed]
- Kwun, J.-S.; Lee, J.H.; Park, B.E.; Park, J.S.; Kim, H.J.; Kim, S.-H.; Jeon, K.-H.; Cho, H.-w.; Kang, S.-H.; Lee, W.; et al. Diagnostic Value of a Wearable Continuous Electrocardiogram Monitoring Device (AT-Patch) for New-Onset Atrial Fibrillation in High-Risk Patients: Prospective Cohort Study. J. Med. Internet Res. 2023, 25, e45760. [Google Scholar] [CrossRef]
- Cai, X.J.; Tay, J.C.K.; Jiang, Y.; Yeo, K.K.; Wong, P.E.H.; Ho, K.L.; Chong, D.T.T.; Ti, L.K.; Leong, G.; Wong, K.; et al. Non-invasive mid-term electrocardiogram patch monitoring is effective in detecting atrial fibrillation. J. Electrocardiol. 2023, 81, 230–236. [Google Scholar] [CrossRef]
- Lin, J.Y.; Larson, J.; Schoenberg, J.; Sepulveda, A.; Tinker, L.; Wheeler, M.; Albert, C.; Manson, J.E.; Wells, G.; Martin, L.W.; et al. Serial 7-Day Electrocardiogram Patch Screening for AF in High-Risk Older Women by the CHARGE-AF Score. JACC Clin. Electrophysiol. 2022, 8, 1523–1534. [Google Scholar] [CrossRef]
- Hibino, M.; Pandey, A.K.; Verma, S.; Puar, P.; Teoh, H.; Quan, A.; Verma, R.; Yau, T.M.; Bisleri, G.; Yanagawa, B.; et al. Wearable Cardiac Rhythm Monitoring Device for Detection of Postoperative Atrial Fibrillation. Ann. Thorac. Surg. 2023, 116, 854–858. [Google Scholar] [CrossRef]
- Lee, H.-Y.; Kim, Y.-J.; Lee, K.-H.; Lee, J.-H.; Cho, S.-P.; Park, J.; Park, I.-H.; Youk, H. Substantiation and Effectiveness of Remote Monitoring System Based on IoMT Using Portable ECG Device. Bioengineering 2024, 11, 836. [Google Scholar] [CrossRef]
- Heo, N.J.; Rhee, S.Y.; Waalen, J.; Steinhubl, S. Chronic kidney disease and undiagnosed atrial fibrillation in individuals with diabetes. Cardiovasc. Diabetol. 2020, 19, 157. [Google Scholar] [CrossRef]
- Chow, J.S.F.; D’Souza, A.; Ford, M.; Marshall, S.; San Miguel, S.; Parameswaran, A.; Parsons, M.; Ramirez, J.; Teramayi, R.; Maurya, N. A descriptive study of the clinical impacts on COVID-19 survivors using telemonitoring (The TeleCOVID Study). Front. Med. Technol. 2023, 5, 1126258. [Google Scholar] [CrossRef]
- Gomez, S.E.; Larson, J.; Hlatky, M.A.; Rodriguez, F.; Wheeler, M.; Greenland, P.; LaMonte, M.; Froelicher, V.; Stefanick, M.L.; Wallace, R.; et al. Prevalence of frequent premature ventricular contractions and nonsustained ventricular tachycardia in older women screened for atrial fibrillation in the Women’s Health Initiative. Heart Rhythm 2024, 21, 1280–1288. [Google Scholar] [CrossRef] [PubMed]
- Wineinger, N.E.; Barrett, P.M.; Zhang, Y.; Irfanullah, I.; Muse, E.D.; Steinhubl, S.R.; Topol, E.J. Identification of paroxysmal atrial fibrillation subtypes in over 13,000 individuals. Heart Rhythm 2019, 16, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Torfs, T.; Smeets, C.J.P.; Geng, D.; Berset, T.; Van Der Auwera, J.; Vandervoort, P.; Grieten, L. Clinical validation of a low-power and wearable ECG patch for long term full-disclosure monitoring. J. Electrocardiol. 2014, 47, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Hyun, S.; Lee, S.; Hong, Y.S.; Lim, S.-h.; Kim, D.J. Evaluation of the Diagnostic Performance and Efficacy of Wearable Electrocardiogram Monitoring for Arrhythmia Detection after Cardiac Surgery. J. Chest Surg. 2024, 57, 205–212. [Google Scholar] [CrossRef]
- Ahn, H.-J.; Choi, E.-K.; Lee, S.-R.; Kwon, S.; Song, H.-S.; Lee, Y.-S.; Oh, S. Three-Day Monitoring of Adhesive Single-Lead Electrocardiogram Patch for Premature Ventricular Complex: Prospective Study for Diagnosis Validation and Evaluation of Burden Fluctuation. J. Med. Internet Res. 2024, 26, e46098. [Google Scholar] [CrossRef]
- Pidoux, J.; Conus, E.; Blackman, N.; Orrit, J.; Khatchatourov, G.; Ruchat, P.; Puricel, S.; Cook, S.; Goy, J.-J. Comparison of Postoperative Continuous Wireless Cardiac Rhythm Monitoring with Traditional Telemetry in Cardiac Surgery Patients: The SMART-TEL Study. J. Innov. Card. Rhythm Manag. 2024, 15, 5997–6003. [Google Scholar] [CrossRef]
- Schultz, K.E.; Lui, G.K.; McElhinney, D.B.; Long, J.; Balasubramanian, V.; Sakarovitch, C.; Fernandes, S.M.; Dubin, A.M.; Rogers, I.S.; Romfh, A.W.; et al. Extended cardiac ambulatory rhythm monitoring in adults with congenital heart disease: Arrhythmia detection and impact of extended monitoring. Congenit. Heart Dis. 2019, 14, 410–418. [Google Scholar] [CrossRef]
- Krumerman, A.; Di Biase, L.; Gerstenfeld, E.; Dickfeld, T.; Verma, N.; Liberman, L.; Amara, R.; Kacorri, A.; Crosson, L.; Wilk, A.; et al. Premature ventricular complexes: Assessing burden density in a large national cohort to better define optimal ECG monitoring duration. Heart Rhythm 2024, 21, 1289–1295. [Google Scholar] [CrossRef]
- Kaura, A.; Sztriha, L.; Chan, F.K.; Aeron-Thomas, J.; Gall, N.; Piechowski-Jozwiak, B.; Teo, J.T. Early prolonged ambulatory cardiac monitoring in stroke (EPACS): An open-label randomised controlled trial. Eur. J. Med. Res. 2019, 24, 25. [Google Scholar] [CrossRef]
- Kim, J.Y.; Oh, I.Y.; Lee, H.; Lee, J.H.; Cho, Y.; Gil, Y.; Jung, S.; Kim, D.I.; Shin, M.G.; Yoo, J.Y.; et al. The efficacy of detecting arrhythmia is higher with 7-day continuous electrocardiographic patch monitoring than with 24-h Holter monitoring. J. Arrhythmia 2023, 39, 422–429. [Google Scholar] [CrossRef]
- Kim, S.; Choi, Y.; Lee, K.; Kim, S.-H.; Kim, H.; Shin, S.; Park, S.; Oh, Y.-S. Comparison of the 11-Day Adhesive ECG Patch Monitor and 24-h Holter Tests to Assess the Response to Antiarrhythmic Drug Therapy in Paroxysmal Atrial Fibrillation. Diagnostics 2023, 13, 3078. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.C.; Wu, Y.L.; Hsu, Y.C.; Hsu, J.T.; Tseng, H.P.; Chen, C.C.; Chiang, M.H.; Hsiao, J.F.; Chin, S.K.; Huang, Y.L.; et al. Comparison of continuous 24-hour and 14-day ECG monitoring for the detection of cardiac arrhythmias in patients with ischemic stroke or syncope. Clin. Cardiol. 2024, 47, e24247. [Google Scholar] [CrossRef] [PubMed]
- Turakhia, M.P.; Ullal, A.J.; Hoang, D.D.; Than, C.T.; Miller, J.D.; Friday, K.J.; Perez, M.V.; Freeman, J.V.; Wang, P.J.; Heidenreich, P.A. Feasibility of Extended Ambulatory Electrocardiogram Monitoring to Identify Silent Atrial Fibrillation in High-risk Patients: The Screening Study for Undiagnosed Atrial Fibrillation (STUDY-AF). Clin. Cardiol. 2015, 38, 285–292. [Google Scholar] [CrossRef]
- Khan, A.; Abedi, V.; Ishaq, F.; Sadighi, A.; Adibuzzaman, M.; Matsumura, M.; Holland, N.; Zand, R. Fast-Track Long Term Continuous Heart Monitoring in a Stroke Clinic: A Feasibility Study. Front. Neurol. 2020, 10, 1400. [Google Scholar] [CrossRef]
- Pothineni, N.V.K.; Soliman, E.Z.; Cushman, M.; Howard, G.; Howard, V.J.; Kasner, S.E.; Judd, S.; Rhodes, J.D.; Marchlinski, F.E.; Deo, R. Continuous cardiac rhythm monitoring post-stroke: A feasibility study in REGARDS. J. Stroke Cerebrovasc. Dis. 2022, 31, 106662. [Google Scholar] [CrossRef]
- Lang, A.; Basyal, C.; Benger, M.; Bhalla, A.; Edwards, F.; Farag, M.; Gadapa, N.; Kee, Y.-Y.K.; Mahmood, S.; Semple, L.; et al. Process and Systems: Improving stroke pathways using an adhesive ambulatory ECG patch: Reducing time for patients to ECGs and subsequent results. Future Healthc. J. 2022, 9, 64–66. [Google Scholar] [CrossRef]
- Miki, T.; Senoo, K.; Ohkura, T.; Yashige, M.; Zen, K.; Shiraishi, H.; Nakamura, T.; Matoba, S. Importance of Monitoring Cardiac Arrhythmias Using 14-Day Patch Electrocardiography in Super Older Patients Who Underwent Transcatheter Aortic Valve Replacement. Am. J. Cardiol. 2023, 209, 57–59. [Google Scholar] [CrossRef]
- Patrick, P.A.; Flatley, A.J.; Obermeyer, I.S.; Lentnek, I.A. Adherence to adhesive patch electrocardiographic monitoring among adults with disabilities. Pacing Clin. Electrophysiol. 2024, 47, 702–705. [Google Scholar] [CrossRef]
- Sandberg, E.L.; Halvorsen, S.; Berge, T.; Grimsmo, J.; Atar, D.; Fensli, R.; Grenne, B.L.; Jortveit, J. Fully digital self-screening for atrial fibrillation with patch electrocardiogram. Europace 2023, 25, euad075. [Google Scholar] [CrossRef]
- Reynolds, M.R.; Stein, A.B.; Sun, X.; Hytopoulos, E.; Steinhubl, S.R.; Cohen, D.J. Cost-Effectiveness of AF Screening With 2-Week Patch Monitors: The mSToPS Study. Circ. Cardiovasc. Qual. Outcomes 2023, 16, e009751. [Google Scholar] [CrossRef]
- Medic, G.; Kotsopoulos, N.; Connolly, M.P.; Lavelle, J.; Norlock, V.; Wadhwa, M.; Mohr, B.A.; Derkac, W.M. Mobile Cardiac Outpatient Telemetry Patch vs Implantable Loop Recorder in Cryptogenic Stroke Patients in the US—Cost-Minimization Model. Med. Devices Evid. Res. 2021, 14, 445–458. [Google Scholar] [CrossRef] [PubMed]
- Verrier, R.L.; Varma, N.; Nearing, B.D. Continuous multi-day tracking of post-myocardial infarction recovery of cardiac electrical stability and autonomic tone using electrocardiogram patch monitors. Ann. Noninvasive Electrocardiol. 2023, 28, e13035. [Google Scholar] [CrossRef] [PubMed]
- Hummel, J.; Houmsse, M.; Tomassoni, G.; Nair, D.; Romero, J.; Hargrove, J.; Mathews, K.; Thakkar, A.B.; Ullery, S.; Eapen, Z.J.; et al. A Patch Wearable Cardioverter-Defibrillator for Patients at Risk of Sudden Cardiac Arrest. J. Am. Coll. Cardiol. 2024, 84, 525–536. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.D.; Atlas, S.J.; Go, A.S.; Lubitz, S.A.; McManus, D.D.; Dolor, R.J.; Chatterjee, R.; Rothberg, M.B.; Rushlow, D.R.; Crosson, L.A.; et al. Effect of Screening for Undiagnosed Atrial Fibrillation on Stroke Prevention. J. Am. Coll. Cardiol. 2024, 84, 2073–2084. [Google Scholar] [CrossRef]
- Goergen, J.A.; Peigh, G.; Hsu, M.; Wilk, A.; Nayak, T.; Crosson, L.; Lenane, J.; Knight, B.P.; Passman, R. Comparison of data quality and monitoring completion rates between clinic and self-applied ECG patches. Heart Rhythm 2023, 20, 407–413. [Google Scholar] [CrossRef]
- Sandberg, E.L.; Halvorsen, S.; Berge, T.; Grimsmo, J.; Atar, D.; Grenne, B.L.; Jortveit, J. Screening for Atrial Fibrillation by Digital Health Technology in Older People in Homecare Settings: A Feasibility Trial. Int. J. Telemed. Appl. 2024, 2024, 4080415. [Google Scholar] [CrossRef]
- Kim, S.; Lim, J.; Shin, M.; Jung, S. SE-ResNet-ViT Hybrid Model for Noise Classification in Adhesive Patch-type Wearable Electrocardiographs. In Proceedings of the 2023 45th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Sydney, Australia, 24–27 July 2023; pp. 1–4. [Google Scholar]
- Dittmar, A.; Lymberis, A. Smart clothes and associated wearable devices for biomedical ambulatory monitoring. In Proceedings of the 13th International Conference on Solid-State Sensors, Actuators and Microsystems, 2005, Digest of Technical Papers. TRANSDUCERS’05, Seoul, Republic of Korea, 5–9 June 2005. [Google Scholar]
- Tada, Y.; Amano, Y.; Sato, T.; Saito, S.; Inoue, M. A Smart Shirt Made with Conductive Ink and Conductive Foam for the Measurement of Electrocardiogram Signals with Unipolar Precordial Leads. Fibers 2015, 3, 463–477. [Google Scholar] [CrossRef]
- Fukuma, N.; Hasumi, E.; Fujiu, K.; Waki, K.; Toyooka, T.; Komuro, I.; Ohe, K. Feasibility of a T-Shirt-Type Wearable Electrocardiography Monitor for Detection of Covert Atrial Fibrillation in Young Healthy Adults. Sci. Rep. 2019, 9, 11768. [Google Scholar] [CrossRef]
- Steinberg, C.; Philippon, F.; Sanchez, M.; Fortier-Poisson, P.; O’Hara, G.; Molin, F.; Sarrazin, J.-F.; Nault, I.; Blier, L.; Roy, K.; et al. A Novel Wearable Device for Continuous Ambulatory ECG Recording: Proof of Concept and Assessment of Signal Quality. Biosensors 2019, 9, 17. [Google Scholar] [CrossRef]
- Seshadri, D.R.; Li, R.T.; Voos, J.E.; Rowbottom, J.R.; Alfes, C.M.; Zorman, C.A.; Drummond, C.K. Wearable sensors for monitoring the physiological and biochemical profile of the athlete. npj Digit. Med. 2019, 2, 72. [Google Scholar] [CrossRef]
- Blachowicz, T.; Ehrmann, G.; Ehrmann, A. Textile-Based Sensors for Biosignal Detection and Monitoring. Sensors 2021, 21, 6042. [Google Scholar] [CrossRef] [PubMed]
- Boehm, A.; Yu, X.; Neu, W.; Leonhardt, S.; Teichmann, D. A Novel 12-Lead ECG T-Shirt with Active Electrodes. Electronics 2016, 5, 75. [Google Scholar] [CrossRef]
- Yu, F.; Chen, Z.; Jiang, M.; Tian, Z.; Peng, T.; Hu, X. Smart Clothing System With Multiple Sensors Based on Digital Twin Technology. IEEE Internet Things J. 2023, 10, 6377–6387. [Google Scholar] [CrossRef]
- De Fazio, R.; Al-Hinnawi, A.-R.; De Vittorio, M.; Visconti, P. An Energy-Autonomous Smart Shirt Employing Wearable Sensors for Users’ Safety and Protection in Hazardous Workplaces. Appl. Sci. 2022, 12, 2926. [Google Scholar] [CrossRef]
- AI Hhs. Hexoskin. Available online: https://hexoskin.com/?srsltid=AfmBOooTeCEhQkA78dBl6h6qJsL952X2ZWWV3qF0i_f4QTZG-tabOxJe (accessed on 7 February 2025).
- MedicalexpO. Servier. Available online: https://www.medicalexpo.com/prod/servier/product-126253-912419.html (accessed on 7 February 2025).
- Athos. Athos Shirt. Available online: https://www.liveathos.com/products/mens-upper-body-kit (accessed on 7 February 2025).
- Hannun, A.Y.; Rajpurkar, P.; Haghpanahi, M.; Tison, G.H.; Bourn, C.; Turakhia, M.P.; Ng, A.Y. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat. Med. 2019, 25, 65–69. [Google Scholar] [CrossRef]
- Torres-Soto, J.; Ashley, E.A. Multi-task deep learning for cardiac rhythm detection in wearable devices. npj Digit. Med. 2020, 3, 116. [Google Scholar] [CrossRef]
- Attia, Z.I.; Noseworthy, P.A.; Lopez-Jimenez, F.; Asirvatham, S.J.; Deshmukh, A.J.; Gersh, B.J.; Carter, R.E.; Yao, X.; Rabinstein, A.A.; Erickson, B.J.; et al. An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: A retrospective analysis of outcome prediction. Lancet 2019, 394, 861–867. [Google Scholar] [CrossRef]

| Manufacturer | Model | FDA | CE | Cost * | Af Detection Automatically ** | Core Study | PPG | ECG | Average Battery Life *** |
|---|---|---|---|---|---|---|---|---|---|
| Apple Inc. |
| ✓ | ✓ | GBP 300–800 | ✓ | Apple Heart Study | ✓ | ✓ | 18–36 h |
| Alphabet Inc. |
| ✓ | ✓ | GBP 150–400 | ✓ | Fitbit Heart Study | ✓ | ✓ | 2–7 days |
| Samsung Electronics |
| ✓ | ✓ | GBP 250–400 | ✓ | - | ✓ | ✓ | 1–3 days |
| Withings |
| ✓ | ✓ | GBP 250–400 | ✓ | - | ✓ | ✓ | 8–30 days |
| Huawei Technologies Co., |
| ✕ | ✓ | GBP 300–500 | ✓ | mAFA-II Trial | ✓ | ✓ | 5–9 days |
| Garmin Ltd. |
| ✓ | ✓ | GBP 350–700 | ✓ | - | ✓ | ✓ | 3–10 days |
| Device | Summary |
|---|---|
| ZIO® XT by iRHYTHM [59] |
|
| HiCardi® SmartPatch® [60] |
|
| SmartCardia™ [61] |
|
| Jewel® Wearable Defibrillator [62] |
|
| ECG247™ by Appsens AS [63] |
|
| EZYPRO® by SIGKNOW [64] |
|
| Firstbeat™ Bodyguard 2 [65] |
|
| Imec’s Health Patch [66] |
|
| Cardea SOLO™ [67] |
|
| Philips MCOT ™ [68] |
|
| mobiCARE™ by Seers [69] |
|
| MEMO® Patch 2 by HUINNO [70] |
|
| Spyder Wireless ECG [71] |
|
| AT Patch by ATsens [72] |
|
| VitalPatch® by VitalConnect [73] |
|
| CardioSTAT® [74] |
|
| S-Patch ExL by Wellysis [75] |
|
| BodyGuardian™ MINI [76] |
|
| Philips ePatch® [77] |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdelrazik, A.; Eldesouky, M.; Antoun, I.; Lau, E.Y.M.; Koya, A.; Vali, Z.; Suleman, S.A.; Donaldson, J.; Ng, G.A. Wearable Devices for Arrhythmia Detection: Advancements and Clinical Implications. Sensors 2025, 25, 2848. https://doi.org/10.3390/s25092848
Abdelrazik A, Eldesouky M, Antoun I, Lau EYM, Koya A, Vali Z, Suleman SA, Donaldson J, Ng GA. Wearable Devices for Arrhythmia Detection: Advancements and Clinical Implications. Sensors. 2025; 25(9):2848. https://doi.org/10.3390/s25092848
Chicago/Turabian StyleAbdelrazik, Ahmed, Mahmoud Eldesouky, Ibrahim Antoun, Edward Y. M. Lau, Abdulmalik Koya, Zakariyya Vali, Safiyyah A. Suleman, James Donaldson, and G. André Ng. 2025. "Wearable Devices for Arrhythmia Detection: Advancements and Clinical Implications" Sensors 25, no. 9: 2848. https://doi.org/10.3390/s25092848
APA StyleAbdelrazik, A., Eldesouky, M., Antoun, I., Lau, E. Y. M., Koya, A., Vali, Z., Suleman, S. A., Donaldson, J., & Ng, G. A. (2025). Wearable Devices for Arrhythmia Detection: Advancements and Clinical Implications. Sensors, 25(9), 2848. https://doi.org/10.3390/s25092848