Effect of Tibialis Anterior Neuromuscular Electrical Stimulation-Induced Eccentric Contraction Training on Single-Leg Standing: A Pilot Study




Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
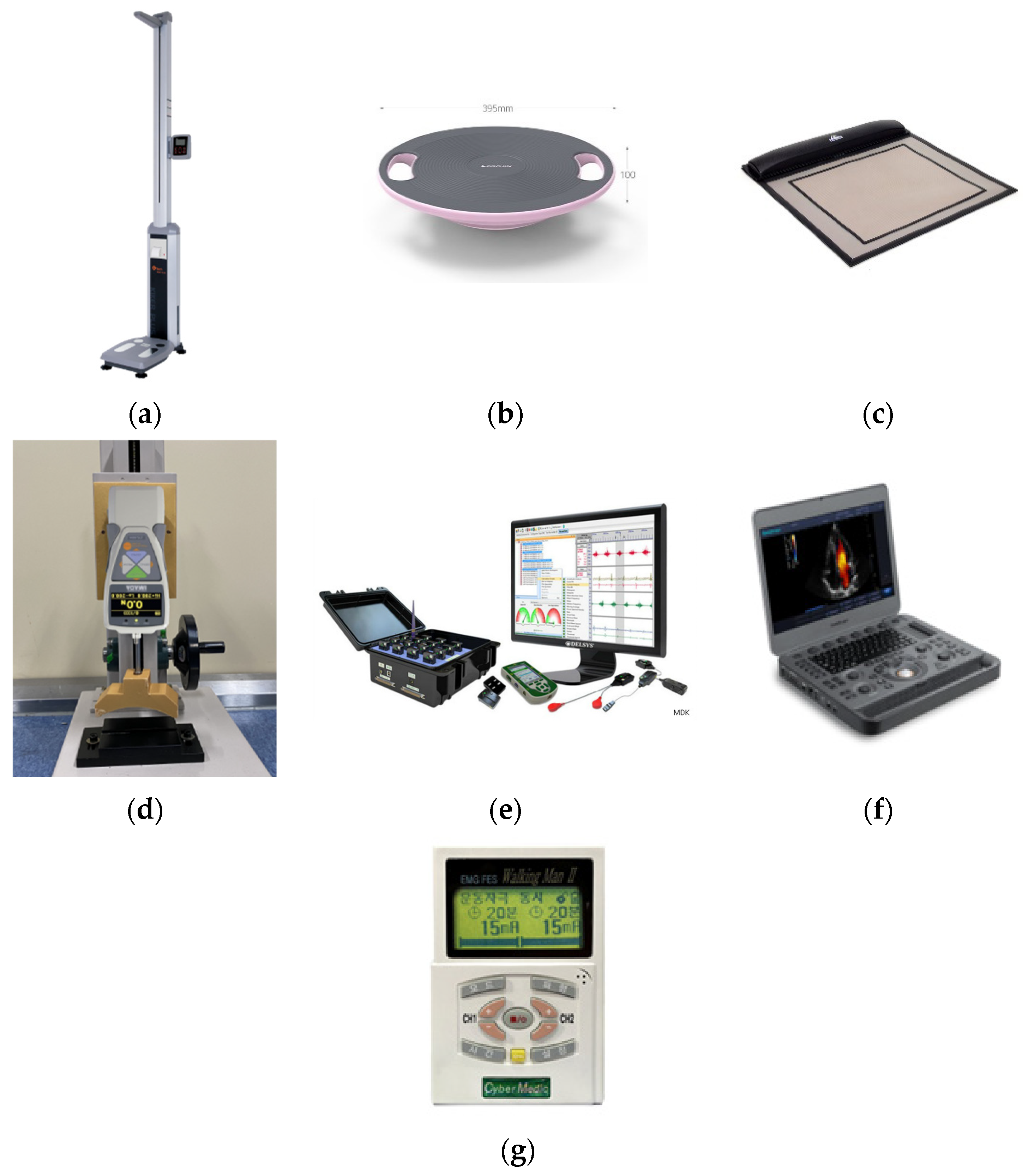
2.2. Devices and Equipment
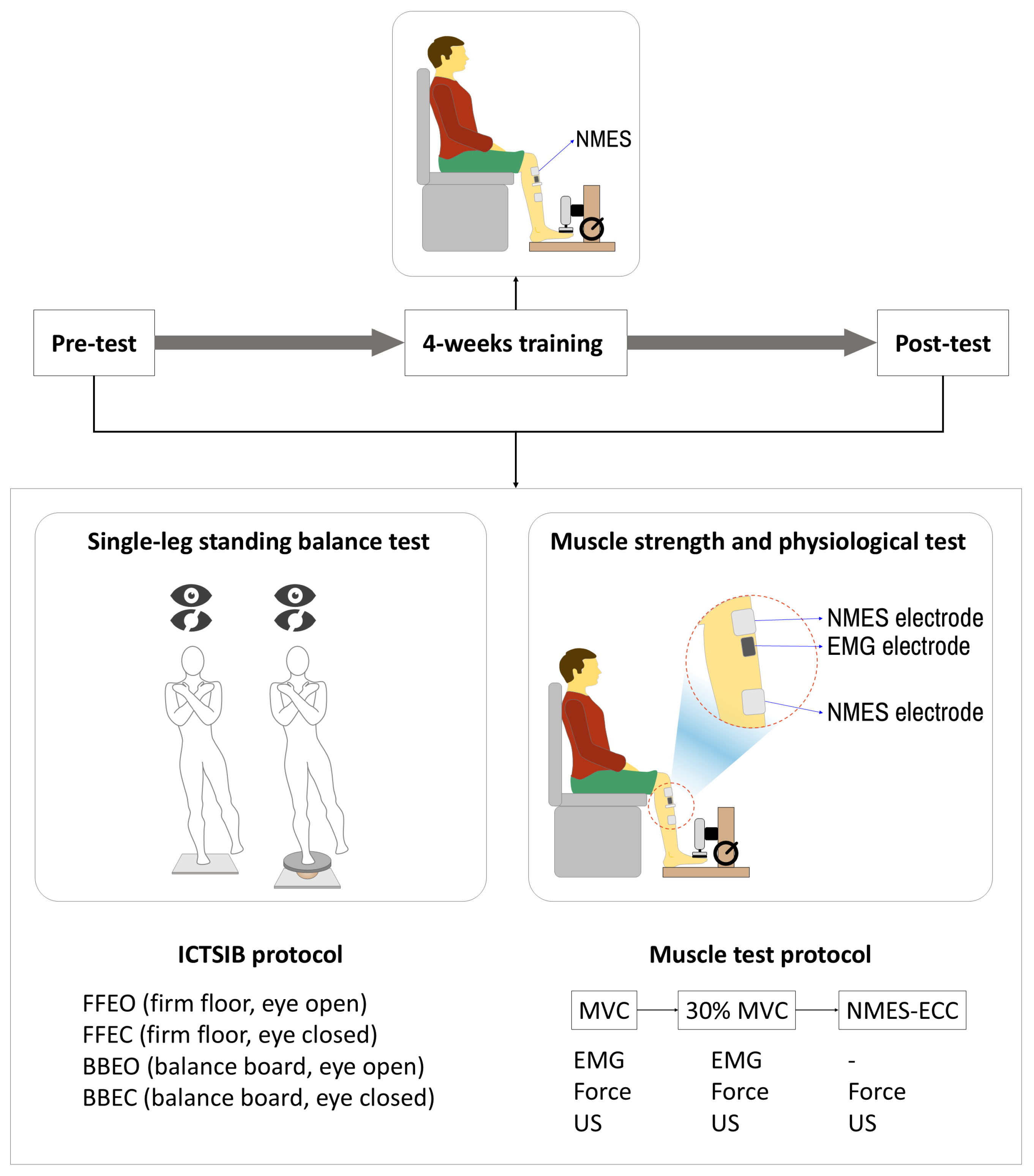
2.3. Experimental Protocol
2.3.1. Pre-Test
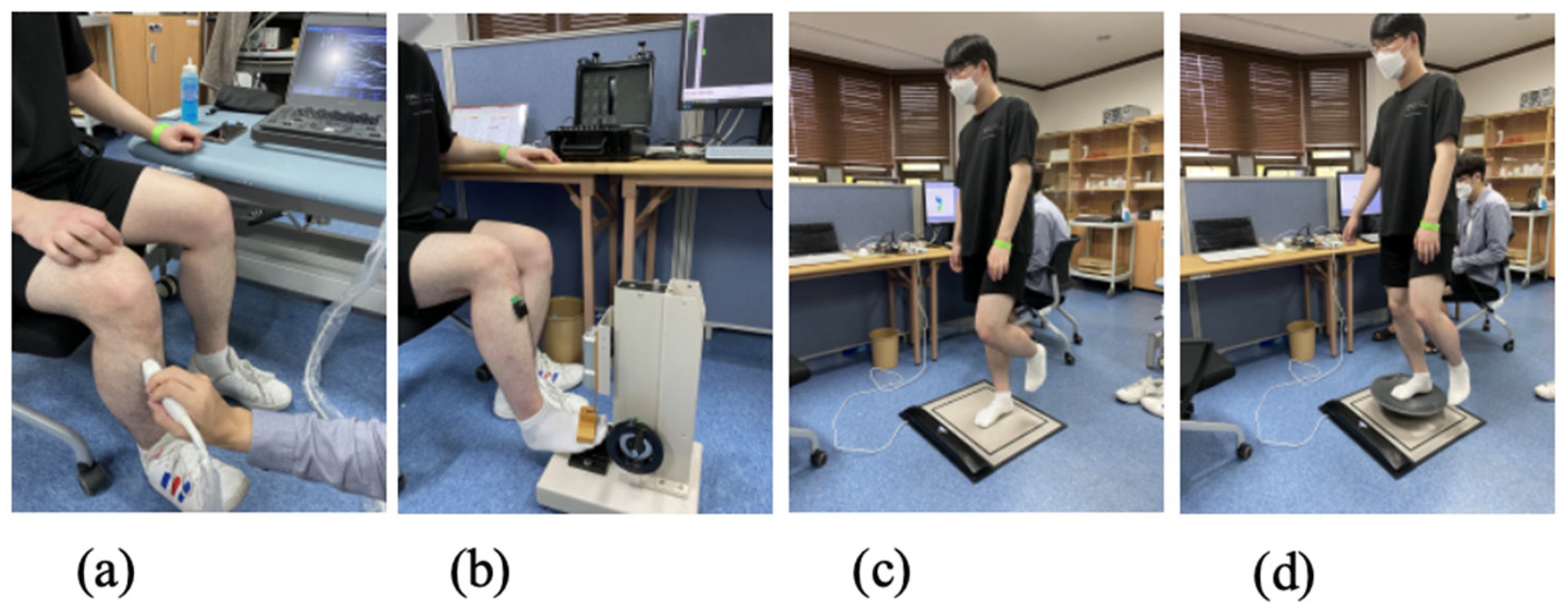
Single-Leg Balance Test
Muscle Physiology Examination
Determining NMES Intensity
NMES-Induced Eccentric Contraction Training
2.3.2. Post-Test
2.4. Data Processing and Analysis
2.4.1. Single-Leg Stance Evaluation
2.4.2. Dorsiflexion (TA Muscle) Force
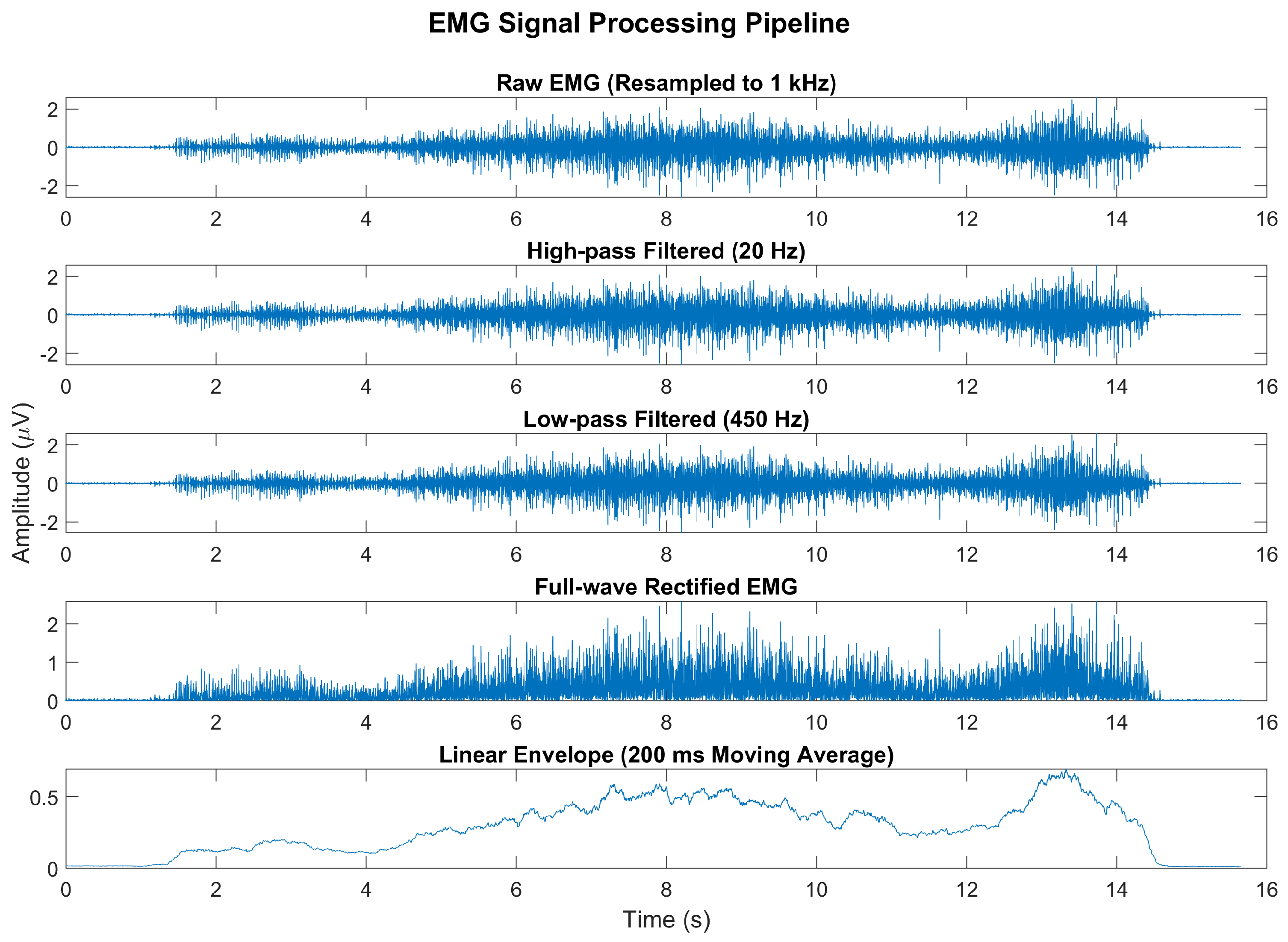
2.4.3. sEMG Signal Processing
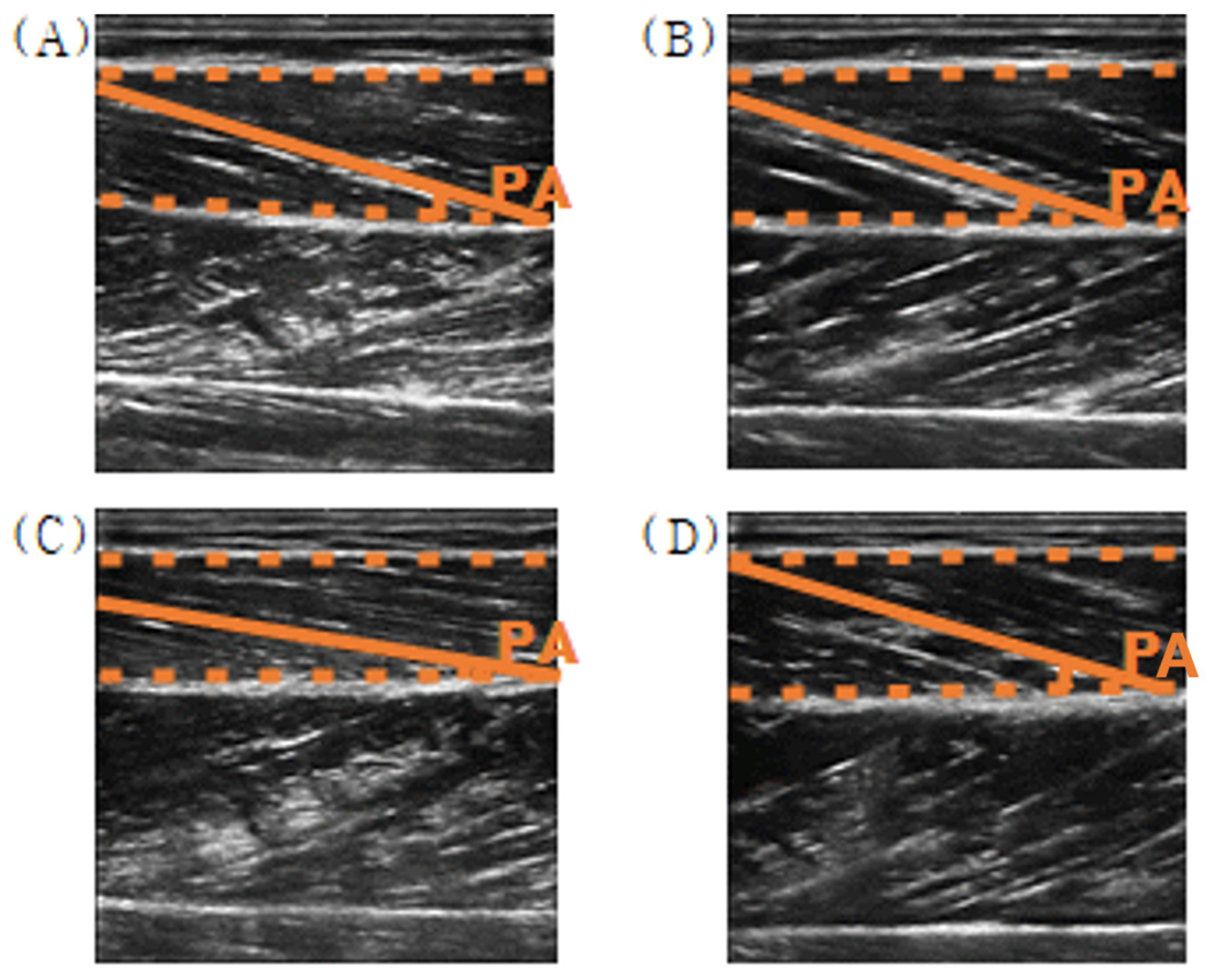
2.4.4. Pennation Angles of TA from the Ultrasound Images
2.4.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jones, S.; Man, W.D.C.; Gao, W.; Higginson, I.J.; Wilcock, A.; Maddocks, M. Neuromuscular electrical stimulation for muscle weakness in adults with advanced disease. Cochrane Database Syst. Rev. 2016, 2016, CD009419. [Google Scholar] [CrossRef] [PubMed]
- Delitto, A.; Rose, S.J.; McKowen, J.M.; Lehman, R.C.; Thomas, J.A.; Shively, R.A. Electrical stimulation versus voluntary exercise in strengthening thigh musculature after anterior cruciate ligament surgery. Phys. Ther. 1988, 68, 660–663. [Google Scholar] [CrossRef] [PubMed]
- Bickel, C.S.; Gregory, C.M.; Dean, J.C. Motor unit recruitment during neuromuscular electrical stimulation: A critical appraisal. Eur. J. Appl. Physiol. 2011, 111, 2399–2407. [Google Scholar] [CrossRef]
- Maffiuletti, N.A. Physiological and methodological considerations for the use of neuromuscular electrical stimulation. Eur. J. Appl. Physiol. 2010, 110, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Enoka, R.M. Activation order of motor axons in electrically evoked contractions. Muscle Nerve 2002, 25, 763–764. [Google Scholar] [CrossRef]
- Lagerquist, O.; Collins, D.F. Influence of stimulus pulse width on M-waves, H-reflexes, and torque during tetanic low-intensity neuromuscular stimulation. Muscle Nerve 2010, 42, 886–893. [Google Scholar] [CrossRef]
- Maffiuletti, N.A.; Herrero, A.J.; Jubeau, M.; Impellizzeri, F.M.; Bizzini, M. Electromyostimulation of skeletal muscle: Review of the state of the art. Eur. J. Appl. Physiol. 2008, 103, 247–272. [Google Scholar]
- Nussbaum, E.L.; Houghton, P.; Anthony, J.; Rennie, S.; Shay, B.L.; Hoens, A.M. Neuromuscular electrical stimulation for treatment of muscle impairment: Critical review and recommendations for clinical practice. Physiother. Can. 2017, 69, 1–76. [Google Scholar] [CrossRef]
- Roig, M.; O’Brien, K.; Kirk, G.; Murray, R.; McKinnon, P.; Shadgan, B.; Reid, W.D. The effects of eccentric versus concentric resistance training on muscle strength and mass in healthy adults: A systematic review with meta-analysis. Br. J. Sports Med. 2009, 43, 556–568. [Google Scholar] [CrossRef]
- Schoenfeld, B.J.; Ogborn, D.I.; Vigotsky, A.D.; Franchi, M.V.; Krieger, J.W. Hypertrophic effects of concentric vs. eccentric muscle actions: A systematic review and meta-analysis. J. Strength Cond. Res. 2017, 31, 2599–2608. [Google Scholar] [CrossRef]
- Lepley, L.K.; Wojtys, E.M.; Palmieri-Smith, R.M. Combination of eccentric exercise and neuromuscular electrical stimulation to improve quadriceps function post-ACL reconstruction. Knee 2015, 22, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Snyder-Mackler, L.; Delitto, A.; Bailey, S.L.; Stralka, S.W. Strength of the quadriceps femoris muscle and functional recovery after reconstruction of the anterior cruciate ligament. A prospective, randomized clinical trial of electrical stimulation. JBJS 1995, 77, 1166–1173. [Google Scholar] [CrossRef] [PubMed]
- Baroni, B.M.; Pinto, R.S.; Herzog, W.; Vaz, M.A. Eccentric resistance training of the knee extensor muscle: Training programs and neuromuscular adaptations. Isokinet. Exerc. Sci. 2015, 23, 183–198. [Google Scholar] [CrossRef]
- Douglas, J.; Pearson, S.; Ross, A.; McGuigan, M. Chronic adaptations to eccentric training: A systematic review. Sports Med. 2017, 47, 917–941. [Google Scholar] [CrossRef]
- Duchateau, J.; Enoka, R.M. Neural control of lengthening contractions. J. Exp. Biol. 2016, 219, 197–204. [Google Scholar] [CrossRef]
- Douglas, J.; Pearson, S.; Ross, A.; McGuigan, M. Eccentric exercise: Physiological characteristics and acute responses. Sports Med. 2017, 47, 663–675. [Google Scholar] [CrossRef]
- LaStayo, P.C.; Woolf, J.M.; Lewek, M.D.; Snyder-Mackler, L.; Reich, T.; Lindstedt, S.L. Eccentric muscle contractions: Their contribution to injury, prevention, rehabilitation, and sport. J. Orthop. Sports Phys. Ther. 2003, 33, 557–571. [Google Scholar] [CrossRef]
- Fitts, R.H. Effects of regular exercise training on skeletal muscle contractile function. Am. J. Phys. Med. Rehabil. 2003, 82, 320–331. [Google Scholar] [CrossRef]
- Szűcs, G.; Pipicz, M.; Szabó, M.R.; Csont, T.; Török, L.; Csonka, C. Effect of eccentric exercise on metabolic health in diabetes and obesity. Sports Med. Open 2023, 9, 91. [Google Scholar] [CrossRef]
- Proske, U.; Morgan, D.L. Muscle damage from eccentric exercise: Mechanism, mechanical signs, adaptation and clinical applications. J. Physiol. 2001, 537, 333–345. [Google Scholar] [CrossRef]
- Moore, D.R.; Phillips, S.M.; Babraj, J.A.; Smith, K.; Rennie, M.J. Myofibrillar and collagen protein synthesis in human skeletal muscle in young men after maximal shortening and lengthening contractions. Am. J. Physiol.-Endocrinol. Metab. 2005, 288, E1153–E1159. [Google Scholar] [CrossRef] [PubMed]
- Touron, J.; Costes, F.; Coudeyre, E.; Perrault, H.; Richard, R. Aerobic metabolic adaptations in endurance eccentric exercise and training: From whole body to mitochondria. Front. Physiol. 2021, 11, 596351. [Google Scholar] [CrossRef]
- Häkkinen, K.; Newton, R.U.; Walker, S.; Häkkinen, A.; Krapi, S.; Rekola, R.; Koponen, P.; Kraemer, W.J.; Haff, G.G.; Blazevich, A.J.; et al. Effects of upper body eccentric versus concentric strength training and detraining on maximal force, muscle activation, hypertrophy, and serum hormones in women. J. Sports Sci. Med. 2022, 21, 200–213. [Google Scholar] [CrossRef] [PubMed]
- Reid, D.A.; Dunning, S.M.; Duran, R.S.; Higgs, A.A.; Jacobs, R.L. The effects of neuromuscular electrical stimulation on strength and hypertrophy: A systematic review. Phys. Ther. Sport 2018, 32, 1–10. [Google Scholar]
- Bortolotti, A.; Negrini, S.; Monticone, M.; Ferrante, S. Neuromuscular electrical stimulation for improving function and reducing spasticity in patients with hemiparetic stroke: A systematic review and meta-analysis. Neurorehabil. Neural Repair 2019, 33, 123–133. [Google Scholar]
- McDowell, B.; Fadke, C.; Sandoval, B. Effect of neuromuscular electrical stimulation on muscle strength in adults with chronic hemiparetic stroke: A systematic review. Neurorehabil. Neural Repair 2021, 35, 858–869. [Google Scholar]
- Stecker, M.M.; Vannucci, A.C.; Housley, S.R. Effect of electrical stimulation on quadriceps strength, spasticity, and functional performance in individuals with multiple sclerosis: A systematic review. Neurorehabil. Neural Repair 2015, 29, 443–452. [Google Scholar]
- Moore, D.R.; Young, M.; Phillips, S.M. Similar increases in muscle size and strength in young men after training with maximal shortening or lengthening contractions when matched for total work. Eur. J. Appl. Physiol. 2012, 112, 1587–1592. [Google Scholar] [CrossRef]
- Adams, G.R.; Cheng, D.C.; Haddad, F.; Baldwin, K.M. Skeletal muscle hypertrophy in response to isometric, lengthening, and shortening training bouts of equivalent duration. J. Appl. Physiol. 2004, 96, 1613–1618. [Google Scholar] [CrossRef]
- Ashida, Y.; Himori, K.; Tatebayashi, D.; Yamada, R.; Ogasawara, R.; Yamada, T. Effects of contraction mode and stimulation frequency on electrical stimulation-induced skeletal muscle hypertrophy. J. Appl. Physiol. 2018, 124, 341–348. [Google Scholar] [CrossRef]
- Lee, S.Y.; Choi, M.B.; Lee, K.H.; Jeong, S.I.; Kim, D.H. Effect of balance training using vibration platform on postural stability in stroke patients. J. Phys. Ther. Sci. 2017, 29, 1539–1542. [Google Scholar]
- Lehmann, T.; Paschen, L.; Baumeister, J. Single-leg assessment of postural stability after anterior cruciate ligament injury: A systematic review and meta-analysis. Sports Med. Open 2017, 3, 32. [Google Scholar] [CrossRef]
- Lindemann, U.; Schwenk, M.; Dummert, T.; Steinhagen-Thiessen, R.; Siber, W.; Becker, C. A comparison of standing balance, mobility, and cognitive function in older adults before and after training with neuromuscular electrical stimulation. Gerontology 2012, 58, 179–187. [Google Scholar]
- Kudiarasu, C.; Rohadhia, W.; Katsura, Y.; Koeda, T.; Singh, F.; Nosaka, K. Eccentric-only versus concentric-only resistance training effects on biochemical and physiological parameters in patients with type 2 diabetes. BMC Sports Sci. Med. Rehabil. 2021, 13, 162. [Google Scholar] [CrossRef] [PubMed]
- Mike, J.N.; Cole, N.; Herrera, C.; VanDusseldorp, T.; Kravitz, L.; Kerksick, C.M. The effects of eccentric contraction duration on muscle strength, power production, vertical jump, and soreness. J. Strength Cond. Res. 2017, 31, 773–786. [Google Scholar] [CrossRef]
- Maffiuletti, N.A.; Roig, M.; Karatzanos, E.; Nanas, S. Neuromuscular electrical stimulation for preventing skeletal-muscle weakness and wasting in critically ill patients: A systematic review. BMC Med. 2013, 11, 137. [Google Scholar] [CrossRef] [PubMed]
- Seger, J.; Thorstensson, A. Electrically evoked eccentric and concentric torque–velocity relationships in human knee extensor muscles. Acta Physiol. Scand. 2000, 169, 63–69. [Google Scholar] [CrossRef]
- Westing, S.; Seger, J.; Thorstensson, A. Effects of electrical stimulation on eccentric and concentric torque-velocity relationships during knee extension in man. Acta Physiol. Scand. 1990, 140, 17–22. [Google Scholar] [CrossRef]
- Da Silva, C.F.G.; e Silva, F.X.d.L.; Vianna, K.B.; dos Santos Oliveira, G.; Vaz, M.A.; Baroni, B.M. Eccentric training combined to neuromuscular electrical stimulation is not superior to eccentric training alone for quadriceps strengthening in healthy subjects: A randomized controlled trial. Braz. J. Phys. Ther. 2018, 22, 502–511. [Google Scholar] [CrossRef]
- Quijoux, F.; Nicolaï, A.; Chairi, I.; Bargiotas, I.; Ricard, D.; Yelnik, A.; Oudre, L.; Bertin-Hugault, F.; Vidal, P.P.; Vayatis, N. A review of center of pressure (COP) variables to quantify standing balance in elderly people: Algorithms and open-access code. Physiol. Rep. 2021, 9, e15067. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Horak, F.B. Assessing the influence of sensory interaction of balance. Suggestion from the field. Phys. Ther. 1986, 66, 1548–1550. [Google Scholar] [CrossRef] [PubMed]
- ImageJ. Available online: https://imagej.net/ij/ (accessed on 19 October 2022).
- Herrero, A.J.; Martín, J.; Martín, T.; Abadía, O.; Fernández, B.; García-López, D. Short-term effect of strength training with and without superimposed electrical stimulation on muscle strength and anaerobic performance. J. Strength Cond. Res. 2010, 24, 1609–1615. [Google Scholar] [CrossRef] [PubMed]
- Peñailillo, L.; Valladares-Ide, D.; Jannas-Velas, S.; Flores-Opazo, M.; Jalón, M.; Mendoza, L.; Nuñez, I.; Diaz-Patiño, O. Effects of eccentric, concentric, and eccentric/concentric training on muscle function and mass, functional performance, cardiometabolic health, quality of life, and molecular adaptations of skeletal muscle in COPD patients: A multicentre randomised trial. BMC Pulm. Med. 2022, 22, 278. [Google Scholar] [CrossRef]
- Mettler, J.A.; Bennett, S.M.; Doucet, B.M.; Magee, D.M. Neuromuscular electrical stimulation and anabolic signaling in patients with stroke. J. Stroke Cerebrovasc. Dis. 2017, 26, 2954–2963. [Google Scholar] [CrossRef] [PubMed]
- Gondin, J.; Guette, M.; Ballay, Y.; Martin, A. Electromyostimulation training effects on neural drive and muscle architecture. Med. Sci. Sports Exerc. 2005, 37, 1291–1299. [Google Scholar] [CrossRef]
- Lanza, I.R.; Short, D.K.; Short, K.R.; Raghavakaimal, S.; Basu, R.; Joyner, M.J.; McConnell, J.P.; Nair, K.S. Endurance exercise as a countermeasure to aging. Diabetes 2008, 57, 2933–2942. [Google Scholar] [CrossRef]
- Peterka, R.J. Sensorimotor integration in human postural control. J. Neurophysiol. 2002, 88, 1097–1118. [Google Scholar] [CrossRef]
- Arazi, H.; Khoshnoud, A.; Asadi, A.; Tufano, J.J. The effect of resistance training set configuration on strength and muscular performance adaptations in male powerlifters. Sci. Rep. 2021, 11, 7844. [Google Scholar] [CrossRef]
- Willis, C.R.G.; Deane, C.S.; Ames, R.M.; Bass, J.J.; Wilkinson, D.J.; Smith, K.; Phillips, B.E.; Szewczyk, N.J.; Atherton, P.J.; Etheridge, T. Transcriptomic adaptation during skeletal muscle habituation to eccentric or concentric exercise training. Sci. Rep. 2021, 11, 23930. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject No. | Sex | Weekly NMES Intensity | Intensity Increase (%) | |||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 2–1 | 3–2 | 4–3 | ||
| 1 | M | 31 | 37 | 44 | 53 | 19.4 | 18.9 | 20.5 |
| 2 | M | 28 | 34 | 41 | 49 | 21.4 | 20.6 | 19.5 |
| 3 | M | 37 | 44 | 53 | 60 | 18.9 | 20.5 | 13.2 |
| 4 | M | 39 | 47 | 56 | 60 | 20.5 | 19.1 | 7.1 |
| 5 | M | 35 | 42 | 50 | 60 | 20 | 19 | 20 |
| 6 | M | 32 | 38 | 46 | 55 | 18.8 | 21.1 | 19.6 |
| 7 | M | 37 | 44 | 53 | 60 | 18.9 | 20.5 | 13.2 |
| 8 | M | 29 | 35 | 42 | 50 | 20.7 | 20 | 19 |
| 9 | M | 31 | 37 | 44 | 53 | 19.4 | 18.9 | 20.5 |
| 10 | M | 34 | 41 | 49 | 59 | 20.6 | 19.5 | 20.4 |
| 11 | F | 22 | 26 | 31 | 37 | 18.2 | 19.2 | 19.4 |
| 12 | F | 26 | 31 | 37 | 44 | 19.2 | 19.4 | 18.9 |
| 13 | F | 30 | 36 | 43 | 52 | 20 | 19.4 | 20.9 |
| 14 | F | 30 | 36 | 43 | 52 | 20 | 19.4 | 20.9 |
| 15 | F | 27 | 32 | 38 | 46 | 18.5 | 18.8 | 21.1 |
| 16 | F | 24 | 29 | 35 | 42 | 20.8 | 20.7 | 20 |
| 17 | F | 23 | 28 | 34 | 41 | 21.7 | 21.4 | 20.6 |
| Variables | Condition | Hedges’ g | M1 | M2 | SDpooled |
|---|---|---|---|---|---|
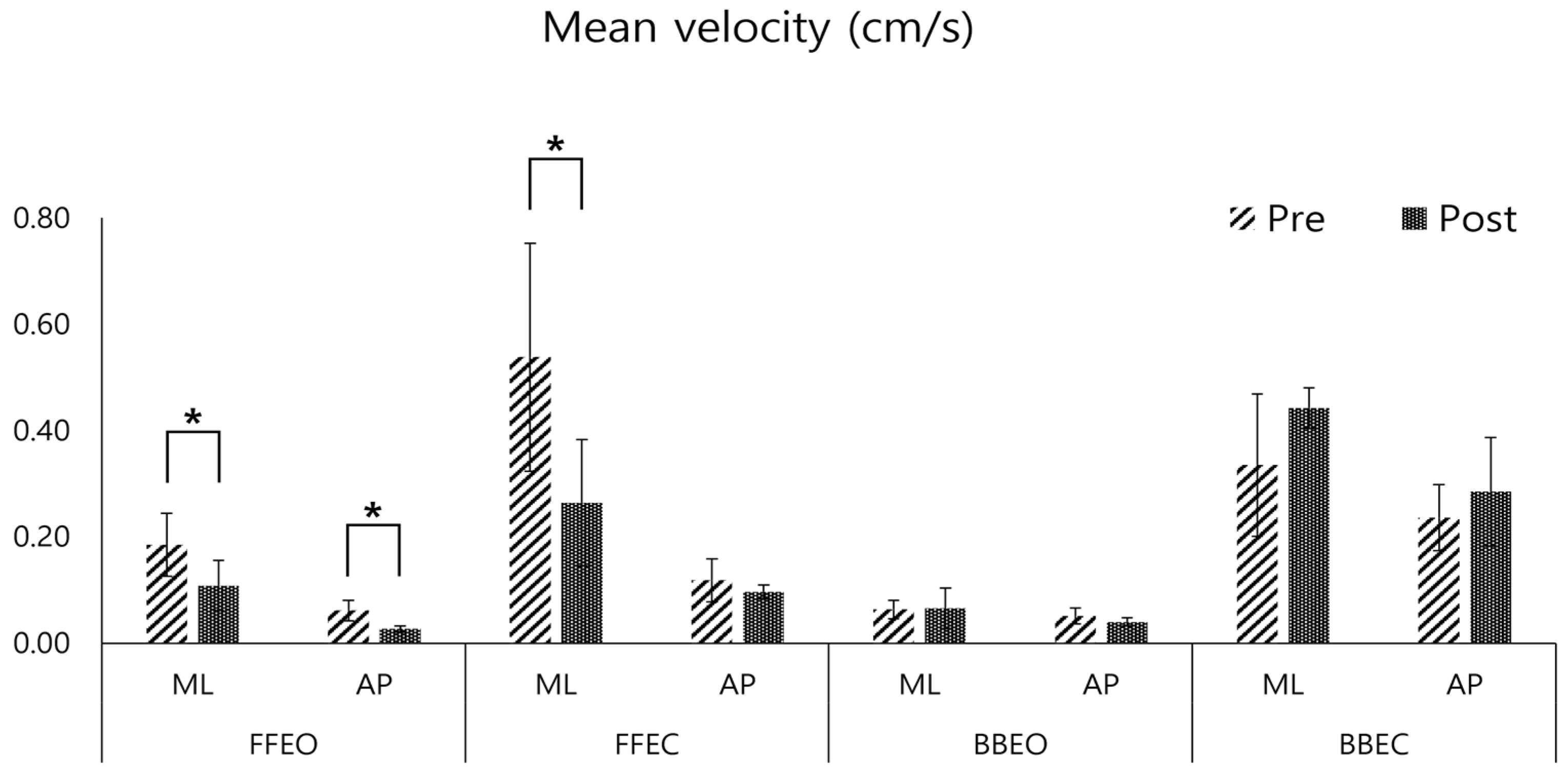
| CoP mean velocity (cm/s) | ML FFEO | 0.55 | 0.18 | 0.11 | 0.14 |
| AP FFEO | 0.74 | 0.06 | 0.03 | 0.05 | |
| ML FFEC | 0.51 | 0.54 | 0.26 | 0.53 | |
| AP FFEC | 0.17 | 0.12 | 0.10 | 0.13 | |
| ML BBEO | −0.03 | 0.06 | 0.07 | 0.09 | |
| AP BBEO | 0.15 | 0.05 | 0.04 | 0.07 | |
| ML BBEC | −0.29 | 0.33 | 0.44 | 0.37 | |
| AP BBEC | −0.19 | 0.24 | 0.29 | 0.25 | |
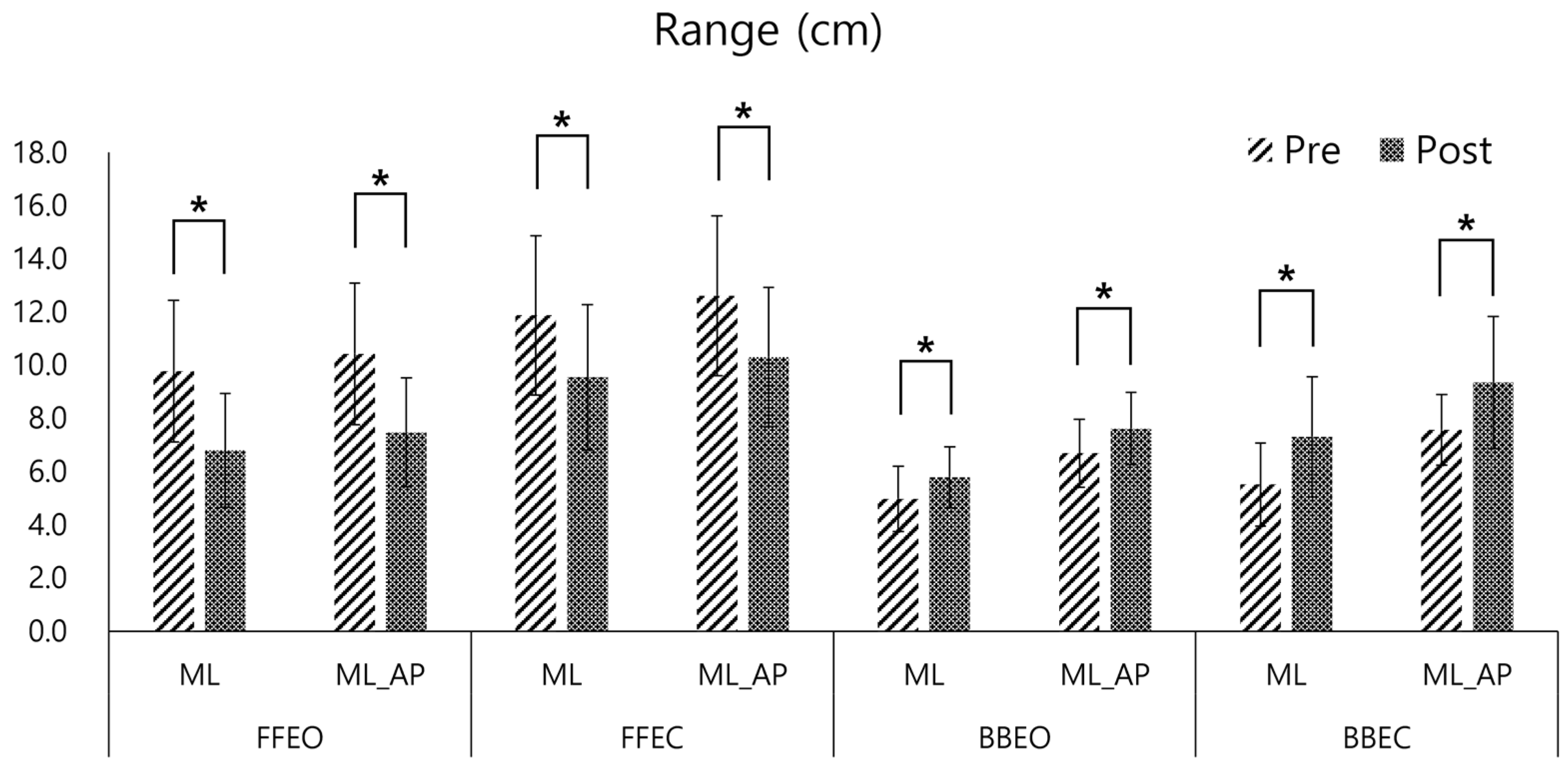
| COP mean range (cm) | ML FFEO | 1.03 | 9.77 | 6.79 | 2.83 |
| ML_AP FFEO | 1.04 | 10.42 | 7.46 | 2.79 | |
| ML FFEC | 0.74 | 11.87 | 9.54 | 3.09 | |
| ML_AP FFEC | 0.74 | 12.60 | 10.30 | 3.04 | |
| ML BBEO | −0.64 | 4.97 | 5.78 | 1.25 | |
| ML_AP BBEO | −0.65 | 6.68 | 7.60 | 1.39 | |
| ML BBEC | −0.82 | 5.51 | 7.30 | 2.13 | |
| ML_AP BBEC | −0.80 | 7.56 | 9.35 | 2.17 | |
| Planar deviation (cm) | FFEO | 0.30 | 150.65 | 127.71 | 74.46 |
| FFEC | 0.15 | 248.81 | 233.64 | 99.73 | |
| BBEO | −0.35 | 160.43 | 190.62 | 83.94 | |
| BBEC | −0.68 | 158.68 | 243.49 | 122.32 | |
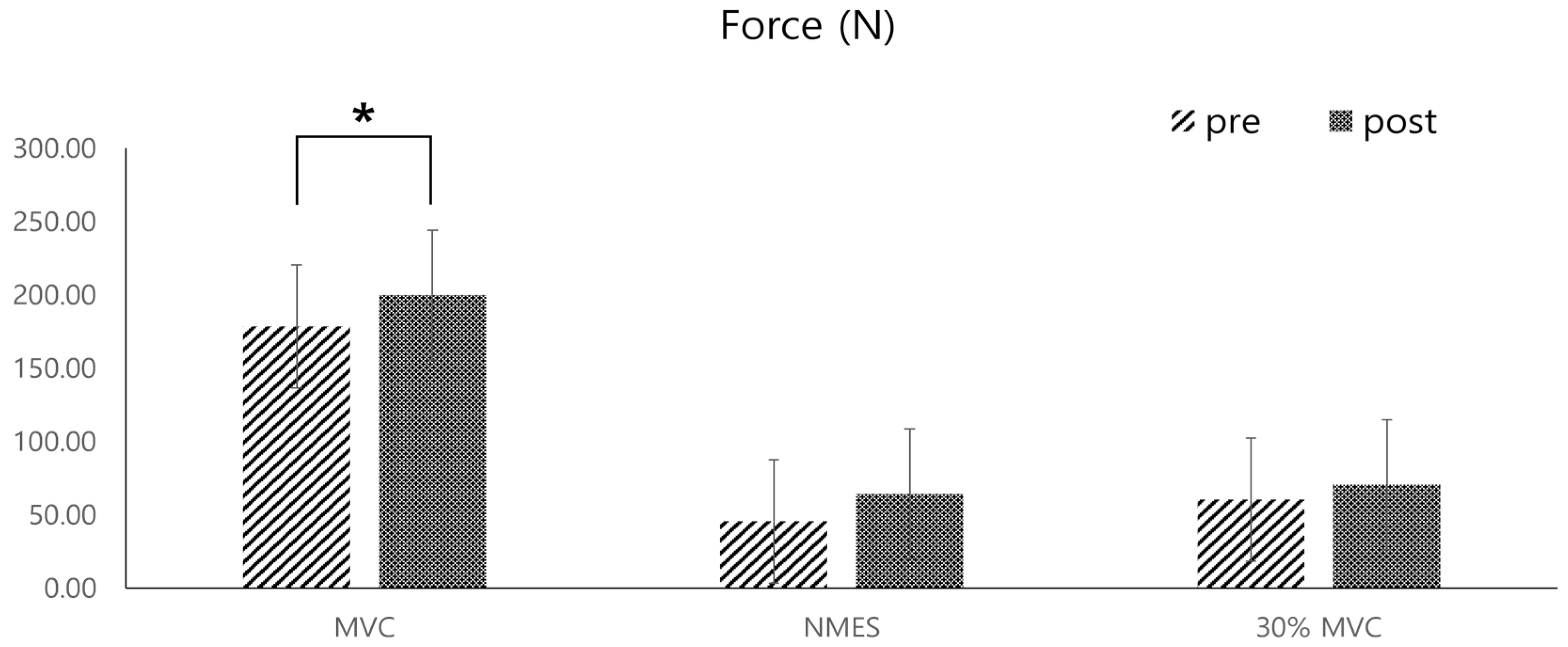
| Force (N) | MVC | −0.47 | 178.54 | 199.97 | 44.70 |
| NMES | −0.46 | 45.57 | 64.32 | 39.53 | |
| 30% MVC | −0.42 | 24.93 | 33.36 | 19.65 | |
| Pennation angle (deg) | VA | −0.22 | 2.75 | 3.18 | 1.96 |
| IA | −0.32 | 3.26 | 4.12 | 2.61 | |
| EA | 0.02 | 1.47 | 1.44 | 1.09 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, N.; Kim, D.; Hwang, S.; Son, J. Effect of Tibialis Anterior Neuromuscular Electrical Stimulation-Induced Eccentric Contraction Training on Single-Leg Standing: A Pilot Study. Sensors 2025, 25, 2455. https://doi.org/10.3390/s25082455
Jeong N, Kim D, Hwang S, Son J. Effect of Tibialis Anterior Neuromuscular Electrical Stimulation-Induced Eccentric Contraction Training on Single-Leg Standing: A Pilot Study. Sensors. 2025; 25(8):2455. https://doi.org/10.3390/s25082455
Chicago/Turabian StyleJeong, Nayoung, Doyeol Kim, Seonhong Hwang, and Jongsang Son. 2025. "Effect of Tibialis Anterior Neuromuscular Electrical Stimulation-Induced Eccentric Contraction Training on Single-Leg Standing: A Pilot Study" Sensors 25, no. 8: 2455. https://doi.org/10.3390/s25082455
APA StyleJeong, N., Kim, D., Hwang, S., & Son, J. (2025). Effect of Tibialis Anterior Neuromuscular Electrical Stimulation-Induced Eccentric Contraction Training on Single-Leg Standing: A Pilot Study. Sensors, 25(8), 2455. https://doi.org/10.3390/s25082455