
Non-Athletic Cohorts Enrolled in Longitudinal Whole-Body Electromyostimulation Trials—An Evidence Map
 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Search
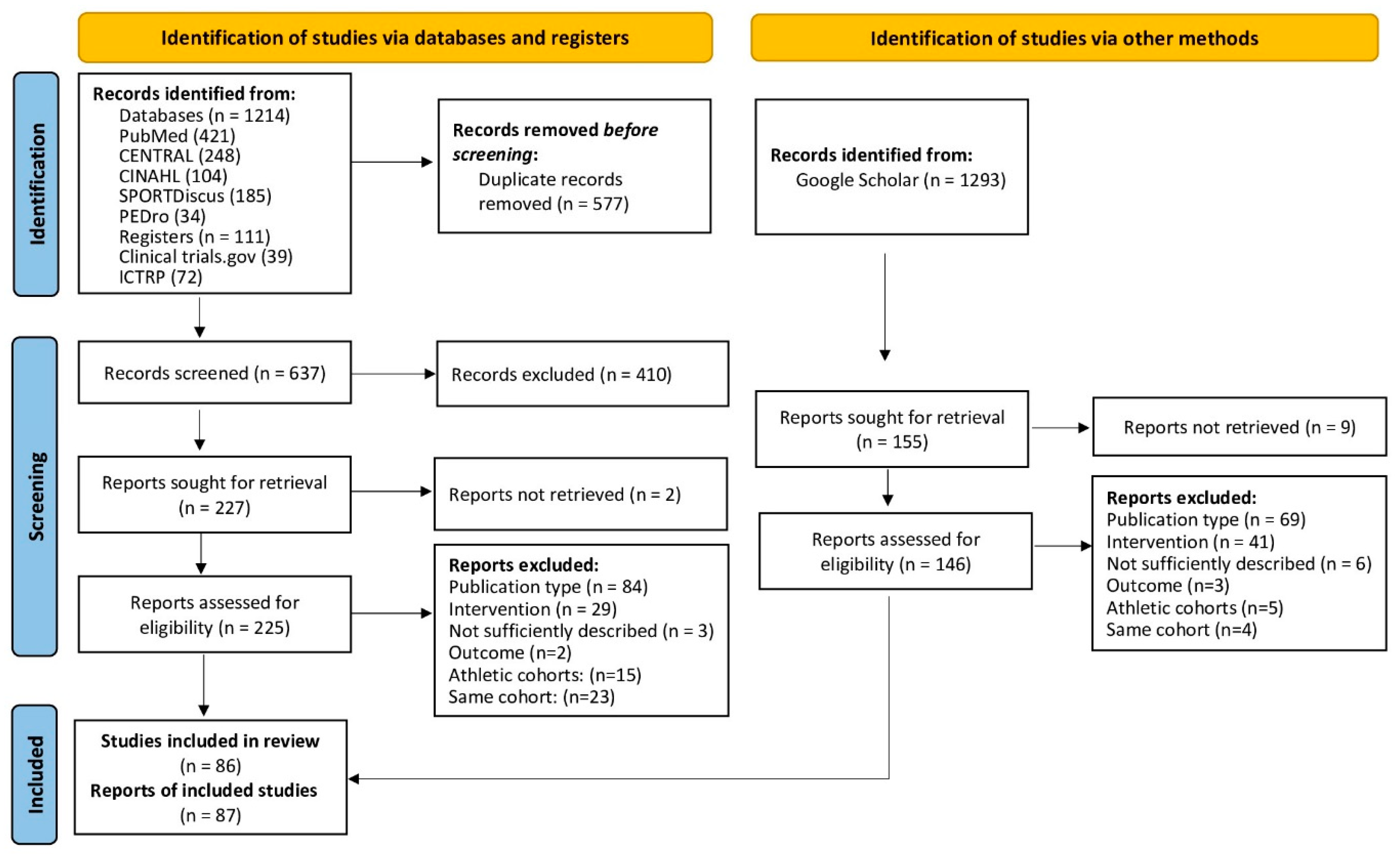
2.2. Selection Process
2.3. Eligibility Criteria
2.3.1. Study Design
2.3.2. Population
2.3.3. Comparators
2.3.4. Intervention
2.3.5. Outcomes
2.4. Data Management
2.5. Data Items
2.6. Quality Assessment
2.7. Data Synthesis
3. Results
3.1. Publication and Study Characteristics
3.2. Exercise and WB-EMS Characteristics
3.3. Participant and Cohort Characteristics
3.4. Neoplasms
3.5. Endocrine, Nutritional and Metabolic Diseases
3.6. Diseases of the Nervous System
3.7. Cardiovascular Diseases
3.8. Diseases of the Respiratory System
3.9. Musculoskeletal and Connective Tissue Diseases
3.10. Diseases of the Genitourinary System
3.11. Critical Illness, Multi-Morbidity
3.12. Frailty, Functional Limitation
3.13. Adverse Effects
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kemmler, W.; Kleinoder, H.; Fröhlich, M. Editorial: Whole-body electromyostimulation: A training technology to improve health and performance in humans? volume II. Front. Physiol. 2022, 13, 972011. [Google Scholar] [CrossRef]
- Eifler, C. Marktsituation, Trends und Entwicklungen. In Ganzkörper-EMS; Kemmler, W., Fröhlich, M., Eifler, C., Eds.; Springer Spektrum: Wiesbaden, Germany, 2022; Volume Essentials. [Google Scholar]
- Kemmler, W.; Weissenfels, A.; Willert, S.; Fröhlich, M.; Ludwig, O.; Berger, J.; Zart, S.; Becker, S.; Backfisch, M.; Kleinöder, H.; et al. Recommended Contraindications for the Use of Non-Medical WB-Electromyostimulation. Dtsch Z Sport. 2019, 70, 278–281. [Google Scholar] [CrossRef]
- Miake-Lye, I.M.; Hempel, S.; Shanman, R.; Shekelle, P.G. What is an evidence map? A systematic review of published evidence maps and their definitions, methods, and products. Syst. Rev. 2016, 5, 28. [Google Scholar] [CrossRef] [PubMed]
- Schmucker, C.; Motschall, E.; Antes, G.; Meerpohl, J.J. Methods of evidence mapping. A systematic review. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2013, 56, 1390–1397. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Kleinoder, H.; Fröhlich, M. Editorial: Whole-Body Electromyostimulation: A Training Technology to Improve Health and Performance in Humans? Front. Physiol. 2020, 11, 523. [Google Scholar] [CrossRef] [PubMed]
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. J. Med. Libr. Assoc. 2016, 104, 240–243. [Google Scholar] [CrossRef]
- Kemmler, W.; Kohl, M.; Freiberger, E.; Sieber, C.; von Stengel, S. Effect of whole-body electromyostimulation and/or protein supplementation on obesity and cardiometabolic risk in older men with sarcopenic obesity: The randomized controlled FranSO trial. BMC Geriatr. 2018, 18, 70. [Google Scholar] [CrossRef]
- Kemmler, W.; von Stengel, S.; Kohl, M.; Rohleder, N.; Bertsch, T.; Sieber, C.C.; Freiberger, E.; Kob, R. Safety of a Combined WB-EMS and High-Protein Diet Intervention in Sarcopenic Obese Elderly Men. Clin. Interv. Aging 2020, 15, 953–967. [Google Scholar] [CrossRef]
- Kemmler, W.; von Stengel, S.; Teschler, M.; Weissenfels, A.; Bebenek, M.; Freiberger, E.; Sieber, C.; Kohl, M. Ganzkörper-Elektromyostimulation, Sarkopenie und Adipositas. Ergebnisse der randomisierten kontrollierten “Franconia Sarcopenic Obesity Study” (FRANSO). Osteoporose Rheuma Aktuell 2017, 15, 12–18. [Google Scholar]
- Kemmler, W.; Weissenfels, A.; Teschler, M.; Willert, S.; Bebenek, M.; Shojaa, M.; Kohl, M.; Freiberger, E.; Sieber, C.; von Stengel, S. Whole-body Electromyostimulation and protein supplementation favorably affect Sarcopenic Obesity in community-dwelling older men at risk. The Randomized Controlled FranSO Study. Clin. Interv. Aging 2017, 12, 1503–1513. [Google Scholar] [CrossRef]
- Mages, M.; Shojaa, M.; Kohl, M.; von Stengel, S.; Becker, C.; Gosch, M.; Jakob, F.; Kerschan-Schindl, K.; Kladny, B.; Klockner, N.; et al. Exercise Effects on Bone Mineral Density in Men. Nutrients 2021, 13, 4244. [Google Scholar] [CrossRef] [PubMed]
- Mohebbi, R.; Shojaa, M.; Kohl, M.; von Stengel, S.; Jakob, F.; Kerschan-Schindl, K.; Lange, U.; Peters, S.; Thomasius, F.; Uder, M.; et al. Exercise training and bone mineral density in postmenopausal women: An updated systematic review and meta-analysis of intervention studies with emphasis on potential moderators. Osteo. Int. 2023, 4, 1145–1178. [Google Scholar] [CrossRef] [PubMed]
- ICD-10-GM. International Statistical Classification of Diseases and Related Health Problems, 10. Revision, German Modification. 2022. Available online: https://www.bfarm.de/EN/Code-systems/Classifications/ICD/ICD-10-GM/_node.html (accessed on 11 October 2023).
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro de Avila, V.; Bento, T.; Gomes, W.; Leitao, J.; Fortuna de Sousa, N. Functional Outcomes and Quality of Life After Ankle Fracture Surgically Treated: A Systematic Review. J. Sport Rehabil. 2018, 27, 274–283. [Google Scholar] [CrossRef]
- Afsharnezhad, T.; Soumander, S. The Effects of Resistance Training With and Without Electrical Muscle Stimulation on Body Composition of Obese Women. Iran. J. Health Sci. 2022, 10, 51–62. [Google Scholar] [CrossRef]
- Akçay, N.; Güney, H.; Kaplan, S.; Akgül, M. Electromyostimulation Exercise with Diet Program is More Effective on Body Composition than its Exercise without Diet. Mediterr. J. Sport Sci. 2022, 4, 814–822. [Google Scholar] [CrossRef]
- Almada, R.; Molina Martín, J.J.; Tregón, P.S.; García, J.L. Comparación Entre los Efectos de un Programa de Entrenamiento de Fuerza Explosiva Mediante Bandas Elásticas y un Programa de Entrenamiento con Electro-Estimulación de Cuerpo Completo. Rev. Kronos 2016, 15, 1. [Google Scholar]
- Amaro-Gahete, F.J.; De-la, O.A.; Jurado-Fasoli, L.; Dote-Montero, M.; Gutierrez, A.; Ruiz, J.R.; Castillo, M.J. Changes in Physical Fitness After 12 Weeks of Structured Concurrent Exercise Training, High Intensity Interval Training, or Whole-Body Electromyostimulation Training in Sedentary Middle-Aged Adults: A Randomized Controlled Trial. Front. Physiol. 2019, 10, 451. [Google Scholar] [CrossRef]
- Amaro-Gahete, F.J.; De-la, O.A.; Sanchez-Delgado, G.; Robles-Gonzalez, L.; Jurado-Fasoli, L.; Ruiz, J.R.; Gutierrez, A. Functional Exercise Training and Undulating Periodization Enhances the Effect of Whole-Body Electromyostimulation Training on Running Performance. Front. Physiol. 2018, 9, 720. [Google Scholar] [CrossRef]
- Andre, L.D.; Basso-Vanelli, R.P.; Ricci, P.A.; Di Thommazo-Luporini, L.; de Oliveira, C.R.; Haddad, G.F.; Haddad, J.M.; Parizotto, N.A.; de Vieira, R.; Arena, R.; et al. Whole-body electrical stimulation as a strategy to improve functional capacity and preserver lean mass after bariatric surgery: A randomized triple-blind controlled trial. Int. J. Obes. 2021, 45, 1476–1487. [Google Scholar] [CrossRef]
- Bellia, A.; Ruscello, B.; Bolognino, R.; Briotti, G.; Gabrielli, P.R.; Silvestri, A.; Rosazza, C.; Ambruoso, F.; Lombardo, M.; Bernardini, A.; et al. Whole-body Electromyostimulation plus Caloric Restriction in Metabolic Syndrome. Int. J. Sports Med. 2020, 41, 751–758. [Google Scholar] [CrossRef]
- Berger, J.; Ludwig, O.; Becker, S.; Backfisch, M.; Kemmler, W.; Frohlich, M. Effects of an Impulse Frequency Dependent 10-Week Whole-body Electromyostimulation Training Program on Specific Sport Performance Parameters. J. Sports Sci. Med. 2020, 19, 271–281. [Google Scholar]
- Bloeckl, J.; Raps, S.; Weineck, M.; Kob, R.; Bertsch, T.; Kemmler, W.; Schoene, D. Feasibility and Safety of Whole-Body Electromyostimulation in Frail Older People-A Pilot Trial. Front. Physiol. 2022, 13, 856681. [Google Scholar] [CrossRef]
- Bostan, G.; Gümüş, M. Effects of fitness and electromyostimulation (EMS) training techniques on body composition [Antrenman Tekniklerinin Vücut Kompozisyonu Üzerine Etkileri]. Turk. J. Diabetes Obes. 2022, 6, 149–158. [Google Scholar] [CrossRef]
- Boutry-Regard, C.; Vinyes-Pares, G.; Breuille, D.; Moritani, T. Supplementation with Whey Protein, Omega-3 Fatty Acids and Polyphenols Combined with Electrical Muscle Stimulation Increases Muscle Strength in Elderly Adults with Limited Mobility: A Randomized Controlled Trial. Nutrients 2020, 12, 1866. [Google Scholar] [CrossRef]
- Çetin, E.; Özdol Pinar, Y.; Deniz, S. Effects of Whole-Body Electromyostimulation on body composition in women of different age [Tüm Beden Elektromiyostimülasyon Uygulamasinin Farkli Yaş Gruplarindaki Kadinlarda Beden Kompozisyonu Üzerine Etkisi]. J. Phys. Educ. Sports Sci. 2017, 15, 173–177. [Google Scholar]
- di Cagno, A.; Buonsenso, A.; Centorbi, M.; Manni, L.; Di Costanzo, A.; Casazza, G.; Parisi, A.; Guerra, G.; Calcagno, G.; Iuliano, E.; et al. Whole body-electromyostimulation effects on serum biomarkers, physical performances and fatigue in Parkinson’s patients: A randomized controlled trial. Front. Aging Neurosci. 2023, 15, 1086487. [Google Scholar] [CrossRef] [PubMed]
- Dyaksa, R.S.; Susilo, E.A.; Virdianto, A.W. The Effect of EMS Exercise on Body Circumstances in Sedentary Women [Pengaruh Latihan Ems Terhadap Lingkar Tubuh Pada Wanita Sedentary]. J. Phys. Educ. Sports Health 2022, 5, 264–270. [Google Scholar] [CrossRef]
- Ethem, H.; Orhan, İ.; ÇAnakci, G. Investigation of the Effect of 6 Weeks Whole-Body Electromyostimulation and with Body Weight Strength Training on some Motoric Properties in Sedantery Women [Sedanter Kadınlarda Tüm Beden Elektromyostimülasyonla Kombine Dinamik Kuvvet Alıştırmalarının Bazı Motorik Özellikler Üzerine Etkisinin İncelenmesi]. Eurasian Res. Sport Sci. 2019, 2, 83–96. [Google Scholar] [CrossRef]
- Evangelista, A.L.; Alonso, A.C.; Ritti-Dias, R.M.; Barros, B.M.; de Souza, C.R.; Braz, T.V.; Bocalini, D.S.; Greve, J.M.D. Effects of Whole Body Electrostimulation Associated With Body Weight Training on Functional Capacity and Body Composition in Inactive Older People. Front. Physiol. 2021, 12, 638936. [Google Scholar] [CrossRef] [PubMed]
- Evangelista, A.L.; Teixeira, C.V.S.; Barros, B.M.; de Azevedo, J.B.; Paunksnis, M.R.R.; Souza, C.R.; Wadhi, T.; Rica, R.L.; Braz, T.V.; Bocalini, D.S. Does whole-body electrical muscle stimulation combined with strength training promote morphofunctional alterations? Clinics 2019, 74, e1334. [Google Scholar] [CrossRef]
- Fritzsche, D.; Fruend, A.; Schenk, S.; Mellwig, K.; Keinöder, H.; Gummert, J.; Horstkotte, D. Elektromyostimulation (EMS) bei kardiologischen Patienten. Wird das EMS-Training bedeutsam für die Sekundärprävention? Herz 2010, 35, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Ghannadi, S.; Halabchi, F.; Maleklou, F.; Tavakol, Z.; Rajabian Tabesh, M.; Bala, D.; Alizadeh, Z. The effect of 6 weeks electrical muscle stimulation training and aerobic exercise on body composition of overweight women: A randomized controlled study. Sport Sci. Health 2022, 18, 1387–1395. [Google Scholar] [CrossRef]
- Hamada, R.; Sato, S.; Miyasaka, J.; Murao, M.; Matsushita, M.; Kajimoto, T.; Otagaki, A.; Asano, T.; Nankaku, M.; Kondo, T.; et al. Belt Electrode-Skeletal Muscle Electrical Stimulation During Early Hematopoietic Post-Transplantation To Prevent Skeletal Muscle Atrophy and Weakness. Transpl. Cell Ther. 2023, 29, 51 e51–51 e57. [Google Scholar] [CrossRef] [PubMed]
- Homma, M.; Miura, M.; Hirayama, Y.; Takahashi, T.; Miura, T.; Yoshida, N.; Miyata, S.; Kohzuki, M.; Ebihara, S. Belt Electrode-Skeletal Muscle Electrical Stimulation in Older Hemodialysis Patients with Reduced Physical Activity: A Randomized Controlled Pilot Study. J. Clin. Med. 2022, 11, 622–630. [Google Scholar] [CrossRef]
- Houdijk, A.P.J.; Bos, N.; Verduin, W.M.; Hijdendaal, M.M.; Zwartkruis, M.A.L. Visceral fat loss by whole-body electromyostimulation is attenuated in male and absent in female older Non-Insulin-Dependent diabetes patients. Endocrinol. Diabetes Metab. 2022, 5, e377. [Google Scholar] [CrossRef]
- Imaoka, S.; Kudou, G.; Tsugiyama, K.; Minata, S.; Teroh, T.; Ootsuka, M.; Furukawa, M.; Higashi, T.; Okita, M. Efficacy of Belt Electrode Skeletal Muscle Electrical Stimulation in the Postoperative Rest Period in Patients with Diabetes who Have Undergone minor Amputations: A Randomized Controlled Trial. Int. J. Low. Extrem. Wounds 2022, 15347346221077491. [Google Scholar] [CrossRef]
- Jee, Y.-S. The effect of high-impulse-electromyostimulation on adipokine profiles, body composition and strength: A pilot study. J. Isokinet. 2019, 27, 163–176. [Google Scholar] [CrossRef]
- Junger, J.; Junger, A.; Ostrowski, P. Body composition of trainees undergoing EMS training with respect to their nutrition. J. Phys. Educ. Sport 2020, 20, 97–101. [Google Scholar] [CrossRef]
- Kataoka, H.; Nakashima, S.; Aoki, H.; Goto, K.; Yamashita, J.; Honda, Y.; Kondo, Y.; Hirase, T.; Sakamoto, J.; Okita, M. Electrical stimulation in addition to passive exercise has a small effect on spasticity and range of motion in bedridden elderly patients: A pilot randomized crossover study. Health 2019, 11, 1072–1086. [Google Scholar] [CrossRef][Green Version]
- Kemmler, W.; Birlauf, A.; von Stengel, S. Einfluss von Ganzkörper-Elektromyostimulation auf das Metabolische Syndrom bei älteren Männern mit metabolischem Syndrom. Dtsch. Z. Sportmed. 2010, 61, 117–123. [Google Scholar]
- Kemmler, W.; Schliffka, R.; Mayhew, J.L.; von Stengel, S. Effects of Whole-Body-Electromyostimulation on Resting Metabolic Rate, Anthropometric and Neuromuscular Parameters in the Elderly. The Training and ElectroStimulation Trial (TEST). J. Strength Cond. Res. 2010, 24, 1880–1886. [Google Scholar] [CrossRef]
- Kemmler, W.; Teschler, M.; Weissenfels, A.; Bebenek, M.; Frohlich, M.; Kohl, M.; von Stengel, S. Effects of Whole-Body Electromyostimulation versus High-Intensity Resistance Exercise on Body Composition and Strength: A Randomized Controlled Study. Evid. -Based Complement. Altern. Med. Ecam 2016, 2016, 9236809. [Google Scholar] [CrossRef]
- Kemmler, W.; Teschler, M.; Weissenfels, A.; Bebenek, M.; von Stengel, S.; Kohl, M.; Freiberger, E.; Goisser, S.; Jakob, F.; Sieber, C.; et al. Whole-body electromyostimulation to fight sarcopenic obesity in community-dwelling older women at risk. Resultsof the randomized controlled FORMOsA-sarcopenic obesity study. Osteoporos. Int. 2016, 27, 3261–3270. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; von Stengel, S. Whole-body electromyostimulation as a means to impact muscle mass and abdominal body fat in lean, sedentary, older female adults: Subanalysis of the TEST-III trial. Clin. Interv. Aging 2013, 8, 1353–1364. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Jee, Y. EMS-effect of Exercises with Music on Fatness and Biomarkers of Obese Elderly Women. Medicina 2020, 56, 156. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Eun, D.; Jee, Y.S. Higher Impulse Electromyostimulation Contributes to Psychological Satisfaction and Physical Development in Healthy Men. Medicina 2021, 57, 197. [Google Scholar] [CrossRef]
- Kirişcioğlu, M.; Bicer, M.; Pancar, Z.; Doğan, İ. Effects of electromyostımulatıon traınıng on body composıtıon. Turk. J. Sport Exerc. 2019, 21, 34–37. [Google Scholar] [CrossRef]
- Konrad, K.L.; Baeyens, J.-P.; Birkenmaier, C.; Ranker, A.H.; Widmann, J.; Leukert, J.; Wenisch, L.; Kraft, E.; Jansson, V.; Wegener, B. The effects of whole-body electromyostimulation (WB-EMS) in comparison to a multimodal treatment concept in patients with non-specific chronic back pain—A prospective clinical intervention study. PLoS ONE 2020, 15, e0236780. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, O.; Berger, J.; Becker, S.; Kemmler, W.; Frohlich, M. The Impact of Whole-Body Electromyostimulation on Body Posture and Trunk Muscle Strength in Untrained Persons. Front. Physiol. 2019, 10, 1020. [Google Scholar] [CrossRef]
- Lukashevich, U.A.; Ponomarev, V.V.; Tarasevich, M.I.; Zhivolupov, S.A. Functional reciprocal neuromuscular electric stimulation in adaptive kinesitherapy in post-stress patients. Sci. Healthc. 2020, 22, 80–88. [Google Scholar] [CrossRef]
- Matsumoto, J.M.; Terabe, S.Y.; Sakaki, R.H. Experience of Belt Electrode Skeletal Muscle Electrical Stimulation Method for Severe Lower Limb Ischemic Patients: A Case Report. Phys. Ther. Clin. Pract. Res. Educ. 2020, 27, 81–85. [Google Scholar]
- Matsuo, K.; Yoneki, K.; Tatsuki, H.; Mibu, K.; Furuzono, K.; Kobayashi, K.; Yasuda, S.; Tamiya, S. Effect of Electrical Muscle Stimulation on the Reduction of Muscle Volume Loss in Acute Heart Failure Patients. Int. Heart J. 2022, 63, 1141–1149. [Google Scholar] [CrossRef]
- Micke, F.; Weissenfels, A.; Wirtz, N.; Von Stengel, S.; Dörmann, U.; Kohl, M.; Kleinöder, H.; Donath, L.; Kemmler, W. Similar Pain Intensity Reductions and Trunk Strength Improvements following Whole-Body Electromyostimulation vs. Whole-Body Vibration vs. Conventional Back-Strengthening Training in Chronic Non-specific Low Back Pain Patients: A 3-armed randomized controlled trial. Front. Physiol. 2021, 13, 664991. [Google Scholar] [CrossRef]
- Miyamoto, T.; Kamada, H.; Tamaki, A.; Moritani, T. Low-intensity electrical muscle stimulation induces significant increases in muscle strength and cardiorespiratory fitness. Eur. J. Sport Sci. 2016, 16, 1104–1110. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.; Tamura, Y.; Deguchi, K.; Miura, Y.; Yura, Y.T.K. Effect of belt electrode skeletal muscle electrical stimulation during hemodialysis on the endothelial function in hemodialysis. Jpn. J. Electrophysical Agents 2020, 27, 78–81. [Google Scholar]
- Müllerová, M.; Vaculíková, P.; Potúčková, A.; Struhár, I.; Balousová, D.N. Impact of Whole-Body Electromyostimulation and Resistance Training Programme on Strength Parameters and Body Composition in Group of Elderly Women at Risk of Sarcopenia. Stud. Sport. 2022, 16, 292–304. [Google Scholar] [CrossRef]
- Nakamura, K.; Kihata, A.; Naraba, H.; Kanda, N.; Takahashi, Y.; Sonoo, T.; Hashimoto, H.; Morimura, N. Efficacy of belt electrode skeletal muscle electrical stimulation on reducing the rate of muscle volume loss in critically ill patients: A randomized controlled trial. J. Rehabil. Med. 2019, 51, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Nakano, H.; Naraba, H.; Mochizuki, M.; Takahashi, Y.; Sonoo, T.; Hashimoto, H.; Morimura, N. High protein versus medium protein delivery under equal total energy delivery in critical care: A randomized controlled trial. Clin. Nutr. 2021, 40, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Nejad, M.D.; Nikbakht, M.; Ghanbarzadeh, M.; Ranjbar, R. Effect of Concurrent Training Order With Electromyostimulation on Physical Performance in Young Elderly Women. Arch. Rehabil. 2021, 21, 508–525. [Google Scholar] [CrossRef]
- Noguchi, Y.; Hirano, H.; Mizutani, C.; Ito, T.; Kawamura, N. Die Wirkung der elektrischen Stimulation der Skelettmuskulatur mit Gürtelelektroden während der Hämodialyse auf die körperliche Funktion von Hämodialysepatienten. J. Dial. Soc. 2018, 51, 87–91. [Google Scholar] [CrossRef]
- Nonoyama, T.; Shigemi, H.; Kubota, M.; Matsumine, A.; Shigemi, K.; Ishizuka, T. Neuromuscular electrical stimulation in the intensive care unit prevents muscle atrophy in critically ill older patients: A retrospective cohort study. Medicine 2022, 101, e29451. [Google Scholar] [CrossRef]
- Ochiai, K.; Tamura, Y.; Ehara, K.; Shimizu, R.; Matushita, Y.; Yasu, T. Bridging Therapy Using B-SES for Peripheral Arterial Disease Patients with Severe Lower Limb Ischemia. J. Phys. Ther. Sci. 2018, 33, 545–548. [Google Scholar] [CrossRef]
- Öktem, U.; Akin, M. Investigation of the Effects of Electrical Muscle Stimulation (EMS) and Traditional Training on Strength Gain and Anthropometric Properties in Sedentary Women [Sedanter Kadınlarda Elektriksel Kas Uyarımı (EMS) ve Geleneksel Antrenmanın Kuvvet Kazanımı ve Antropometrik Özellikler Üzerine Etkisinin İncelenmesi]. CBU J. Phys. Educ. Sport Sci. 2022, 17, 70–79. [Google Scholar]
- Özdal, M.; Bostanci, Ö. Effects of whole-body electromyostimulation with and without voluntary muscular contractions on total and regional fat mass of women. Arch. Appl. Sci. Res. 2016, 8, 75–79. [Google Scholar]
- Pano-Rodriguez, A.; Beltran-Garrido, J.V.; Hernandez-Gonzalez, V.; Reverter-Masia, J. Effects of Whole-Body Electromyostimulation on Physical Fitness in Postmenopausal Women: A Randomized Controlled Trial. Sensors 2020, 20, 1482. [Google Scholar] [CrossRef] [PubMed]
- Park, H.K.; Na, S.M.; Choi, S.L.; Seon, J.K.; Do, W.H. Physiological Effect of Exercise Training with Whole Body Electric Muscle Stimulation Suit on Strength and Balance in Young Women: A Randomized Controlled Trial. Chonnam Med. J. 2021, 57, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Min, S.; Park, S.H.; Yoo, J.; Jee, Y.S. Influence of Isometric Exercise Combined with Electromyostimulation on Inflammatory Cytokine Levels, Muscle Strength, and Knee Joint Function in Elderly Women with Early Knee Osteoarthritis. Front. Physiol. 2021, 12, 688260. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Park, J.; Ham, J.A.; Jee, Y. Effects of aerobic dance with electrical stimulant on body composition and radiological circumference of obese elderly women. Gazz. Medica Ital. Arch. Sci. Mediche 2021, 180, 87–95. [Google Scholar] [CrossRef]
- Park, W.; Lee, J.; Hong, K.; Park, H.Y.; Park, S.; Kim, N.; Park, J. Protein-Added Healthy Lunch-Boxes Combined with Exercise for Improving Physical Fitness and Vascular Function in Pre-Frail Older Women: A Community-Based Randomized Controlled Trial. Clin. Interv. Aging 2023, 18, 13–27. [Google Scholar] [CrossRef]
- Qin, Y.; Chen, H.; Liu, X.; Wu, J.; Zhang, Y. Effects of whole-body electromyostimulation training on upper limb muscles strength and body composition in moderately trained males: A randomized controlled study. Front. Public Health 2022, 10, 982062. [Google Scholar] [CrossRef]
- Reljic, D.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Iron Beats Electricity: Resistance Training but not Whole-Body Electromyostimulation Improves Cardiometabolic Health in Obese Metabolic Syndrome Patients during Caloric Restriction-A Randomized-Controlled Study. Nutrients 2021, 13, 1640. [Google Scholar] [CrossRef]
- Ricci, P.A.; Di Thommazo-Luporini, L.; Jurgensen, S.P.; Andre, L.D.; Haddad, G.F.; Arena, R.; Borghi-Silva, A. Effects of Whole-Body Electromyostimulation Associated with Dynamic Exercise on Functional Capacity and Heart Rate Variability After Bariatric Surgery: A Randomized, Double-Blind, and Sham-Controlled Trial. Obes. Surg. 2020, 30, 3862–3871mats. [Google Scholar] [CrossRef]
- Richter, H. Effect of Electromyostimulation Training and High-Protein Diet on Gastrointestinal Tumor Patients in Palliative and Curative Treatment Settings. [Einfluss von Elektromyostimulationstraining und Proteinreicher Ernährung auf Gastrointestinale Tumorpatienten in Palliativer und Kurativer Behandlungssituation]; Friedrich-Alexander-University Erlangen-Nürnberg: Erlangen, Germany, 2019. [Google Scholar]
- Sadeghipour, S.; Mirzaei, B. Effects of whole-body electromyostimulation with two different frequencies and combined training on lipid profile and body composition in overweight women. Physiother. Q. 2022, 30, 79–85. [Google Scholar] [CrossRef]
- Sadeghipour, S.; Mirzaei, B.; Korobeynikov, G.; Tropin, Y. Effects of Whole-Body Electromyostimulation and Resistance Training on Body Composition and Maximal Strength in Trained Women. Health Sport Rehabil. 2021, 7, 18–28. [Google Scholar] [CrossRef]
- Sánchez-Infante, J.; Bravo-Sáncheza, A.; Abiánb, P.; Estebana, P.; Jimeneza, J.; Abián-Vicén, J. The influence of whole-body electromyostimulation training in middle-aged women. Isokinet. Exerc. Sci. 2020, 1, 1–9. [Google Scholar] [CrossRef]
- Schink, K.; Herrmann, H.J.; Schwappacher, R.; Meyer, J.; Orlemann, T.; Waldmann, E.; Wullich, B.; Kahlmeyer, A.; Fietkau, R.; Lubgan, D.; et al. Effects of whole-body electromyostimulation combined with individualized nutritional support on body composition in patients with advanced cancer: A controlled pilot trial. BMC Cancer 2018, 18, 886. [Google Scholar] [CrossRef] [PubMed]
- Schink, K.; Reljic, D.; Herrmann, H.J.; Meyer, J.; Mackensen, A.; Neurath, M.F.; Zopf, Y. Whole-Body Electromyostimulation Combined With Individualized Nutritional Support Improves Body Composition in Patients With Hematological Malignancies—A Pilot Study. Front. Physiol. 2018, 9, 1808. [Google Scholar] [CrossRef] [PubMed]
- Schwappacher, R.; Schink, K.; Sologub, S.; Dieterich, W.; Reljic, D.; Friedrich, O.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Physical activity and advanced cancer: Evidence of exercise-sensitive genes regulating prostate cancer cell proliferation and apoptosis. J. Physiol. 2020, 598, 3871–3889. [Google Scholar] [CrossRef] [PubMed]
- Schwappacher, R.; Dieterich, W.; Reljic, D.; Pilarsky, C.; Mukhopadhyay, D.; Chang, D.K.; Biankin, A.V.; Siebler, J.; Herrmann, H.J.; Neurath, M.F.; et al. Muscle-Derived Cytokines Reduce Growth, Viability and Migratory Activity of Pancreatic Cancer Cells. Cancers 2021, 13, 3820. [Google Scholar] [CrossRef] [PubMed]
- Silvestri, A.; Ruscello, B.; Rosazza, C.; Briotti, G.; Gabrielli, P.R.; Tudisco, C.; D’Ottavio, S. Acute Effects of Whole-Body Electrostimulation Combined with Stretching on Lower Back Pain. Int. J. Sports Med. 2023, 44, 820–829. [Google Scholar] [CrossRef]
- Song, J.; Heo, S.Y.K. Effects of short-term whole-body electrical stimulation training on metabolic syndrome risk factors and fitness in obese female college students J. Coach. Dev. 2020, 22, 140–148. [Google Scholar] [CrossRef]
- Stephan, H.; Wehmeier, U.F.; Forster, T.; Tomschi, F.; Hilberg, T. Additional Active Movements Are Not Required for Strength Gains in the Untrained during Short-Term Whole-Body Electromyostimulation Training. Healthcare 2023, 11, 741. [Google Scholar] [CrossRef]
- Struhár, I.; Vaculíková, P.; Gimunová, M.; Minster, D.; Körnerová, V. Effects of whole-body electrostimulation and acroyoga based exercise programme on blood pressure in a group of young women. J. Phys. Educ. Sport 2019, 19, 49–57. [Google Scholar]
- Suzuki, T.; Ikeda, M.; Minami, M.; Matayoshi, Y.; Nakao, M.; Nakamura, T.; Abo, M. Beneficial Effect of Intradialytic Electrical Muscle Stimulation in Hemodialysis Patients: A Randomized Controlled Trial. Artif. Organs 2018, 42, 899–910. [Google Scholar] [CrossRef]
- Suzuki, Y.; Suzuki, H.; Yato, S.; Iwasaki, H.; Eguchi, K.; Haneda, K.; Shimano, H. Mittelfristige Auswirkungen der Elektrotherapie der Skeletmuskulatur mit Gürtelelektroden auf den Glukose und Fettstoffwechsel die Körperzusammensetzung, die Muskelkraft und die Muskelausdauer bei Patienten mit Typ-2 Diabetes. Phys. Ther. Sci. 2019, 33, 53–59. [Google Scholar]
- Tanaka, S.; Kamiya, K.; Matsue, Y.; Yonezawa, R.; Saito, H.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Yamashita, M.; Wakaume, K.; et al. Effects of electrical muscle stimulation on physical function in frail older patients with acute heart failure: A randomized controlled trial. Eur. J. Prev. Cardiol. 2022, 29, e286–e288. [Google Scholar] [CrossRef] [PubMed]
- Teschler, M.; Heimer, M.; Schmitz, B.; Kemmler, W.; Mooren, F.C. Four weeks of electromyostimulation improves muscle function and strength in sarcopenic patients: A three-arm parallel randomized trial. J. Cachexia Sarcopenia Muscle 2021, 12, 843–854. [Google Scholar] [CrossRef] [PubMed]
- Teschler, M.; Weissenfels, A.; Bebenek, M.; Frohlich, M.; Kohl, M.; von Stengel, S.; Kemmler, W. Very high creatine kinase CK levels after WB_EMS. Are there implications for health. Int. J. Clin. Exp. Med. 2016, 9, 22841–22850. [Google Scholar]
- Tsurumi, T.; Tamura, Y.; Nakatani, Y.; Furuya, T.; Tamiya, H.; Terashima, M.; Tomoe, T.; Ueno, A.; Shimoyama, M.; Yasu, T. Neuromuscular Electrical Stimulation during Hemodialysis Suppresses Postprandial Hyperglycemia in Patients with End-Stage Diabetic Kidney Disease: A Crossover Controlled Trial. J. Clin. Med. 2022, 11, 6239. [Google Scholar] [CrossRef]
- Vaculikova, P.P.; Kotkova, M.A.; Struhar, I.; Balousova, D.N. Impact of Whole-Body Electromyostimulation and Resistance Training on Bone Mineral Density in women at risk for Osteopororosis. IJPESS 2022, 16, 69–79. [Google Scholar] [CrossRef]
- Vaculikova, P.P.; Kotkova, M.A.; Struhar, I.; Balousova, D.; Rozsypal, R. Impact of Whole-Body Electromyostimulation and Resistance Training on the Level of Functional Fitness in Elderly Women. Stud. Sport. 2023, 16, 115–126. [Google Scholar] [CrossRef]
- van Buuren, F.; Horstkotte, D.; Mellwig, K.; Fruend, A.; Bogunovic, N.; Dimitriadis, Z.; Vortherms, J.; Humphrey, R.; Niebauer, J. Electrical Myostimulation (EMS) Improves Glucose Metabolism and Oxygen Uptake in Type 2 Diabetes Mellitus Patients—Results from the EMS Study. Diabetes Technol. Ther. 2015, 17, 413–419. [Google Scholar] [CrossRef] [PubMed]
- van Buuren, F.; Mellwig, K.P.; Prinz, C.; Korber, B.; Frund, A.; Fritzsche, D.; Faber, L.; Kottmann, T.; Bogunovic, N.; Dahm, J.; et al. Electrical myostimulation improves left ventricular function and peak oxygen consumption in patients with chronic heart failure: Results from the exEMS study comparing different stimulation strategies. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2013, 102, 523–534. [Google Scholar] [CrossRef]
- von Stengel, S.; Bebenek, M.; Engelke, K.; Kemmler, W. Whole-Body Electromyostimulation to Fight Osteopenia in Elderly Females: The Randomized Controlled Training and Electrostimulation Trial (TEST-III). J. Osteoporos. 2015, 2015, 643520. [Google Scholar] [CrossRef]
- Weissenfels, A.; Teschler, M.; Willert, S.; Hettchen, M.; Frohlich, M.; Kleinoder, H.; Kohl, M.; von Stengel, S.; Kemmler, W. Effects of whole-body electromyostimulation on chronic nonspecific low back pain in adults: A randomized controlled study. J. Pain Res. 2018, 11, 1949–1957. [Google Scholar] [CrossRef] [PubMed]
- Willert, S.; Weissenfels, A.; Kohl, M.; von Stengel, S.; Fröhlich, M.; Kleinöder, H.; Schöne, D.; Teschler, M.; Kemmler, W. Effects of Whole-Body Electromyostimulation (WB-EMS) on the energy-restriction-induced reduction of muscle mass during intended weight loss. Front. Physiol. 2019, 10, 1012. [Google Scholar] [CrossRef]
- Zink-Rückel, C.; Kohl, M.; von Stengel, S.; Kemmler, W. Once weekly whole-body electromyostimulation increase strength, stability and body composition in amateur golfers. A randomized controlled study. Int. J. Environ. Res. Public Health 2021, 18, 5628. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Asano, T.; Hamada, R.; Sato, S.; Miyasaka, J.; Murao, M.; Matsushita, M.; Kajimoto, T.; Otagaki, A.; Nankaku, M.; Kondo, T. Effects of early post-transplant belt electrode skeletal muscle electrical stimulation therapy on an allogeneic hematopoietic stem cell transplant recipient: A case study. Jpn. J. Tranplant 2022, 11, 206–210. [Google Scholar] [CrossRef]
- Michibata, A.; Haraguchi, M.; Murakawa, Y.; Ishikawa, H. Electrical stimulation and virtual reality-guided balance training for managing paraplegia and trunk dysfunction due to spinal cord infarction. BMJ Case Rep. 2022, 15, e244091. [Google Scholar] [CrossRef] [PubMed]
- Recker, R.R. Early postmenopausal bone loss and what to do about it. Ann. N. Y. Acad. Sci. 2011, 1240, E26–E30. [Google Scholar] [CrossRef] [PubMed]
- Scherer, M.; Wagner, H.; Lühmann, D.; Muche-Borowski, C.; Schäfer, I.; Dubben, H.; Hansen, H.; Thiesemann, R.; von Renteln-Kruse, W.; Hofmann, W. Multimorbidity S3 Guideline AWMF Register No. 053-047 DEGAM Guideline No. 20. Deutsche Gesellschaft für Allgemeinmedizin und Familienmedizin. 2017. Available online: www.degam-leitlinien.de (accessed on 11 October 2023).
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; Abellan van Kan, G.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An undiagnosed condition in older adults. Current consensus definition: Prevalence, etiology, and consequences. International working group on sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Shojaa, M.; Steele, J.; Berger, J.; Fröhlich, M.; Schoene, D.; von Stengel, S.; Kleinöder, H.M. Efficacy of Whole-Body Electromyostimulation (WB-EMS) on body composition and muscle strength in non-athletic adults. A systematic review and meta-analysis. Front. Physiol. 2021, 12, 640657. [Google Scholar] [CrossRef]
- Berger, J.; Fröhlich, M.; Kemmler, W. WB-EMS Market Development—Perspectives and Threats. Int. J. Environ. Res. Public Health 2022, 19, 14211. [Google Scholar] [CrossRef]
- BMU. Regulation on Protection against Harmful Effects of Non-Ionizing Radiation in Human Applications (NiSV) [Verordnung zum Schutz vor schädlichen Wirkungen nichtionisierender Strahlung bei der Anwendung am Menschen (NiSV)]; Bundesministerium-für-Umwelt-Naturschutz-und-nukleare-Sicherheit: Bonn, Germany, 2019. [Google Scholar]
- BMU. Requirements for the Acquisition of Expertise for Applications of non-Ionizing Radiation Sources on Humans [Anforderungen an den Erwerb der Fachkunde für Anwendungen nichtionisierender Strahlungsquellen am Menschen]; Bundesministerium-für-Umwelt-Naturschutz-und-nukleare-Sicherheit: Bonn, Germany, 2020. [Google Scholar]
- Galicia Ernst, I.; Torbahn, G.; Schwingshackl, L.; Knuttel, H.; Kob, R.; Kemmler, W.; Sieber, C.C.; Batsis, J.A.; Villareal, D.T.; Stroebele-Benschop, N.; et al. Outcomes addressed in randomized controlled lifestyle intervention trials in community-dwelling older people with (sarcopenic) obesity-An evidence map. Obes. Rev. 2022, 23, e13497. [Google Scholar] [CrossRef]
- Gotz, M.; Heiss, R.; von Stengel, S.; Roemer, F.; Berger, J.; Nagel, A.; Uder, M.; Kemmler, W. Spatial Distribution of Muscular Effects of Acute Whole-Body Electromyostimulation at the Mid-Thigh and Lower Leg-A Pilot Study Applying Magnetic Resonance Imaging. Sensors 2022, 22, 10017. [Google Scholar] [CrossRef]
- Numata, H.; Nakase, J.; Inaki, A.; Mochizuki, T.; Oshima, T.; Takata, Y.; Kinuya, S.; Tsuchiya, H. Effects of the belt electrode skeletal muscle electrical stimulation system on lower extremity skeletal muscle activity: Evaluation using positron emission tomography. J. Orthop. Sci. 2016, 21, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Stollberger, C.; Finsterer, J. Side effects of and contraindications for whole-body electro-myo-stimulation: A viewpoint. BMJ Open Sport Exerc. Med. 2019, 5, e000619. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Fröhlich, M.; Ludwig, O.; Eifler, C.; von Stengel, S.; Willert, S.; Teschler, M.; Weissenfels, A.; Kleinoder, H.; Micke, F.; et al. Position statement and updated international guideline for safe and effective whole-body electromyostimulation training-the need for common sense in WB-EMS application. Front. Physiol. 2023, 14, 1174103. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Study- Design | Study Arms (n) | Total Sample Size (n) | Active Control | Methodological Quality | |
|---|---|---|---|---|---|---|---|---|
| 1 | Afsharnezhad et al. [17] | 2022 | IRN | RCT | 3 | 36 | yes | low |
| 2 | Akcay et al. [18] | 2022 | TUR | RCT | 2 | 104 | yes | moderate |
| 3 | Almada et al. [19] | 2016 | ESP | RCT | 2 | 10 | yes | low |
| 4 | Amaro-Gahete et al. [21] | 2018 | ESP | RCT | 2 | 12 | yes | moderate |
| 5 | Amaro-Gahete et al. [20] | 2019 | ESP | RCT | 4 | 89 | no | moderate |
| 6 | Andre et al. [22] | 2021 | BRA | RCT | 2 | 39 | no | high |
| 7 | Bellia et al. [23] | 2020 | ITA | RCT | 2 | 25 | no | low |
| 8 | Berger et al. [24] | 2020 | GER | RCT | 3 | 51 | no | moderate |
| 9 | Blöckl et al. [25] a | 2022 | GER | NRCT | 2a | 18 | yes | low |
| 10 | Bostan et al. [26] | 2022 | TUR | RCT | 2 | 128 | yes | low |
| 11 | Bouty-Regard et al. [27] | 2020 | JPN | RCT | 3 | 41 | yes | moderate |
| 12 | Cetin et al. et al. [28] | 2017 | TUR | IS without CG- | 3 | 24 | n.a. | low |
| 13 | DiCagno et al. [29] | 2023 | ITA | RCT | 3 | 24 | no | high |
| 14 | Dyaksa et al. [30] | 2022 | IDN | IS without CG- | 1 | 10 | n.a. | low |
| 15 | Ethem et al. [31] | 2019 | IND | RCT | 2 | 18 | no | low |
| 16 | Evangelista et al. [33] | 2019 | BRA | RCT | 3 | 58 | no | low |
| 17 | Evangelista et al. [32] | 2021 | BRA | RCT | 2 | 30 | yes | moderate |
| 18 | Fritzsche et al. [34] | 2010 | GER | IS without CG- | 1 | 15 | n.a. | low |
| 19 | Ghannadi et al. [35] | 2022 | IRN | RCT | 2 | 40 | yes | low |
| 20 | Hamada et al. [36] | 2023 | JPN | NRCT | 2 | 43 | yes | low |
| 21 | Homma et al. [37] | 2022 | JPN | RCT | 2 | 27 | no | moderate |
| 22 | Houdjijk et al. [38] | 2022 | NL | NRCT | 4 | 75 | yes | low |
| 23 | Imaoka et al. [39] | 2022 | JPN | RCT | 2 | 49 | yes | moderate |
| 24 | Jee et al. [40] | 2019 | KOR | RCT | 4 | 54 | no | moderate |
| 25 | Junger et al. [41] | 2020 | SVKi | NRCT | 2 | 86 | yes | low |
| 26 | Kataoka et al. [42] | 2019 | JPN | RCT | 2 | 16 | yes | moderate |
| 27 | Kemmler et al. [44] | 2010 | GER | RCT | 2 | 30 | yes | moderate |
| 28 | Kemmler et al. [43] | 2012 | GER | RCT | 2 | 28 | yes | moderate |
| 29 | Kemmler et al. [47] | 2013 | GER | RCT | 2 | 46 | yes | moderate |
| 30 | Kemmler et al. [45] | 2016 | GER | RCT | 2 | 46 | yes | moderate |
| 31 | Kemmler et al. [46] | 2016 | GER | RCT | 3 | 75 | no | high |
| 32 | Kemmler et al. [11] | 2017 | GER | RCT | 3 | 100 | no | high |
| 33 | Kim et al. [48] | 2020 | KOR | RCT | 2 | 25 | yes | moderate |
| 34 | Kim et al. [49] | 2021 | KOR | RCT | 4 | 54 | no | moderate |
| 35 | Kiriscioglu et al. [50] | 2019 | TUR | NRCT | 2 | 41 | no | low |
| 36 | Konrad et al. [51] | 2020 | GER | NRCT | 2 | 128 | yes | low |
| 37 | Ludwig et al. [52] | 2019 | GER | RCT | 3 | 58 | no | low |
| 38 | Lukashevich et al. [53] | 2020 | BLR | RCT | 3 | 52 | no | low |
| 39 | Matsumoto et al. [54] | 2020 | JPN | IS without CG- | 1 | 4 | n.a. | low |
| 40 | Matsuo et al. [55] | 2022 | JPN | NRCT | 2 | 90 | yes | low |
| 41 | Micke et al. [56] | 2021 | GER | RCT | 3 | 240 | yes | high |
| 42 | Miyamoto et al. [57] | 2016 | JPN | RCT | 2 | 19 | no | moderate |
| 43 | Mori 2020 et al. [58] | 2020 | JPN | NRCT | 1 | 14 | n.a. | low |
| 44 | Müllerova et al. [59] | 2022 | CZE | RCT | 2 | 21 | yes | low |
| 45 | Nakamura et al. [60] | 2019 | JPN | RCT | 2 | 94 | yes | low |
| 46 | Nakamura et al. [61] | 2021 | JPN | RCT | 2 | 68 | no | moderate |
| 47 | Nejad et al. [62] | 2021 | IRN | RCT | 5 | 40 | no | low |
| 48 | Noguchi et al. [63] | 2017 | JPN | IS without CG- | 1 | 8 | n.a. | low |
| 49 | Nonoyama et al. [64] | 2022 | JPN | NRCT | 2 | 42 | n.a | low |
| 50 | Ochiai et al. [65] | 2018 | JPN | NRCT | 2 | 6 | yes | low |
| 51 | Özdal et al. [67] | 2016 | TUR | RCT | 2 | 40 | yes | low |
| 52 | Öktem et al. [66] | 2022 | TUR | RCT | 2 | 20 | no | low |
| 53 | Pano-Rodriguez et al. [68] | 2020 | ESP | RCT | 2 | 34 | yes | moderate |
| 54 | Park et al. [71] | 2021 | KOR | RCT | 2 | 34 | no | high |
| 55 | Park et al. [70] | 2021 | KOR | RCT | 3 | 81 | no | moderate |
| 56 | Park et al. [69] | 2021 | KOR | RCT | 2 | 24 | no | moderate |
| 57 | Park et al. [72] | 2023 | KOR | RCT | 4 | 60 | yes | moderate |
| 58 | Qin et al. [73] | 2022 | CHN | RCT | 2 | 25 | yes | moderate |
| 59 | Reljic et al. [74] | 2022 | GER | RCT | 4 | 103 | no | moderate |
| 60 | Ricci et al. [75] | 2020 | BRA | RCT | 2 | 20 | no | high |
| 61 | Richter et al. [76] | 2019 | GER | NRCT | 2 | 75 | no | low |
| 62 | Sadeghipour et al. [78] | 2021 | IRN | RCT | 3 | 30 | no | moderate |
| 63 | Sadeghipour et al. [77] | 2022 | IRN | RCT | 3 | 45 | no | low |
| 64 | Sanchez-Infante et al. [79] | 2020 | ESP | RCT | 2 | 28 | yes | moderate |
| 65 | Schink et al. [80] | 2018 | GER | NRCT | 2 | 131 | no | low |
| 66 | Schink et al. [81] | 2018 | GER | NRCT | 2 | 31 | no | low |
| 67 | Schwappacher et al. [82] | 2020 | GER | NRCT | 2 | 18 | no | low |
| 68 | Schwappacher et al. [82] | 2020 | GER | NRCT | 2 | 12 | no | low |
| 69 | Schwappacher et al. [83] | 2021 | GER | NRCT | 2 | 12 | no | low |
| 70 | Silvestri et al. [84] | 2023 | ITA | NRCT | 2 | 52 | yes | low |
| 71 | Song et al.et al. [85] | 2020 | KOR | NRCT | 3 | 30 | yes | low |
| 72 | Stephan et al. [86] | 2023 | GER | RCT | 2 | 60 | yes | moderate |
| 73 | Struhar et al. [87] | 2019 | CZE | NRCT | 3 | 28 | no | low |
| 74 | Suzuki et al. [88] | 2018 | JPN | RCT | 2 | 29 | no | low |
| 75 | Suzuki. et al. [89] | 2018 | JPN | IS without CG- | 1 | 12 | 2 | low |
| 76 | Tanaka et al. [90] | 2022 | JPN | RCT | 2 | 39 | no | moderate |
| 77 | Teschler et al. [92] | 2016 | GER | IS without CG- | 1 | 11 | n.a. | low |
| 78 | Teschler et al. [91] | 2021 | GER | RCT | 3 | 134 | no | moderate |
| 79 | Tsurumi et al. [93] | 2022 | JPN | RCT | 2 | 22 | no | moderate |
| 80 | Vacoulikova et al. [95] | 2021 | CZE | RCT | 3 | 21 | no | low |
| 81 | Vacoulikova et al. [94] | 2021 | CZE | RCT | 3 | 63 | yes | low |
| 82 | van Buuren et al. [97] | 2014 | GER | NRCT | 3 | 59 | no | low |
| 83 | van Buuren et al. [96] | 2015 | GER | IS without CG- | 1 | 15 | n.a. | low |
| 84 | von Stengel et al. [98] | 2015 | GER | RCT | 2 | 76 | yes | moderate |
| 85 | Weissenfels et al. [99] | 2018 | GER | RCT | 2 | 30 | no | high |
| 86 | Willert et al. [100] | 2019 | GER | RCT | 3 | 90 | no | moderate |
| 87 | Zink et al. [101] | 2021 | GER | RCT | 2 | 54 | no | moderate |
| Author | Year | Gender | Age (Years) | BMI (kg/m2) 1 | Training-status 2 | Diseases | Drop-Out (%) 3 | Adherence (%) | Adverse Effects | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Afsharnezhad et al. [17] | 2022 | w | 29 ± 3 | 34.6 | well | yes | n.g. | n.g. | n.g. |
| 2 | Akcay et al. [18] | 2022 | m + w | 33 ± 1 | 27.2 | moderate | no | 0 | 90 | no |
| 3 | Almada et al. [19] | 2016 | m | 23 ± 3 | 23.7 | moderate | no | 0 | n.g. | n.g. |
| 4 | Amaro-Gahete et al. [21] | 2018 | m | 27 ± 7 | 23.8 | well | no | 14 | 96 | no |
| 5 | Amaro-Gahete et al. [20] | 2019 | m + w | 53 ± 5 | 26.8 | untrained | no | 17 | 99 | no |
| 6 | Andre et al. [22] | 2021 | m + w | 39 ± 2 | 40.5 | untrained | yes | 15 | 91 | no |
| 7 | Bellia et al. [23] | 2020 | m + w | 49 ± 7 | 40.1 | moderate | yes | 23 | 90 | no |
| 8 | Berger et al. [24] | 2020 | m + w | 26 ± 3 | 23.8 | moderate | no | 12 | 100 | no |
| 9 | Blöckl et al. [25] | 2022 | m + w | 80 ± 4 | 26.2 4 | untrained | yes | 14 | 88 | no |
| 10 | Bostan et al. [26] | 2022 | m + w | <30 to >50 | n.g. | untrained | no | n.g. | n.g. | no |
| 11 | Bouty-Regard et al. [27] | 2020 | m + w | 77 ± 2 | 21.5 | untrained | yes | 0 | 97 | no |
| 12 | Centin et al. [28] | 2017 | w | 25–40 | 27.6 5 | untrained | no | n.g. | n.g. | n.g. |
| 13 | DiCagno et al. [29] | 2023 | m + w | 72 ± 6 | n.g. | untrained | yes | 0 | 100 | no |
| 14 | Dyaksa et al. [30] | 2022 | w | n.g. | n.g. | untrained | no | n.g. | n.g. | no |
| 15 | Ethem et al. [31] | 2019 | w | 38 ± 5 | 23.7 | untrained | no | n.g. | n.g. | no |
| 16 | Evangelista et al. [33] | 2019 | m + w | 26 ± 4 | 25.2 | moderate | no | 16 | 95 | no |
| 17 | Evangelista et al. [32] | 2021 | m | 75 ± 7 | n.g. | untrained | no | 33 | 100 | no |
| 18 | Fritzsche et al. [34] | 2010 | m + w | 27–73 | 26.8 | untrained | yes | 0 | n.g. | no |
| 19 | Ghannadi et al. [35] | 2022 | w | 33 ± 6 | 27.3 | untrained | no | 15 | 80 | no |
| 20 | Hamada et al. [36] | 2023 | m + w | 20–69 | 21.4 | untrained | yes | 12 | 71 | no |
| 21 | Homma et al. [37] | 2022 | m + w | 79 ± 6 | 22.0 | untrained | yes | 29 | 100 | no |
| 22 | Houdjijk et al. [38] | 2022 | m + w | 45–75 | 31.8 6 | untrained | yes | 0 | 95 | no |
| 23 | Imaoka et al. [39] | 2022 | m + w | 64 ± 7 | 24.2 | untrained | yes | 27 | n.g. | no |
| 24 | Jee et al. [40] | 2019 | m | 25 ± 2 | 22.0 | untrained | no | 5 | 100 | no |
| 25 | Junger et al. [41] | 2020 | m + w | 18–62 | 23.0 | moderate | no | 0 | 100 | no |
| 26 | Kataoka et al. [42] | 2019 | m + w | 83 ± 6 | 16.7 | untrained | yes | 25 | n.g. | no |
| 27 | Kemmler et al. [44] | 2010 | w | 65 ± 6 | 26.0 | well | yes | 0 | 98 | no |
| 28 | Kemmler et al. [43] | 2010 | m | 69 ± 3 | 28.1 | untrained | yes | 7 | 78 | no |
| 29 | Kemmler et al. [47] | 2013 | w | 75 ± 4 | 22.1 | untrained | yes | 16 | 79 | no |
| 30 | Kemmler et al. [45] | 2016 | m | 30–50 | 28.5 | moderate | no | 13 | 90 | no |
| 31 | Kemmler et al. [46] | 2016 | w | 77 ± 4 | 25.1 | untrained | yes | 10 | 89 | no |
| 32 | Kemmler et al. [11] | 2017 | m | 77 ± 5 | 26.1 | moderate | yes | 9 | 91 | no |
| 33 | Kim et al. [48] | 2020 | w | 71 ± 3 | 30.9 | untrained | yes | 13 | n.g. | no |
| 34 | Kim et al. [49] | 2021 | m | 24 ± 2 | 25.1 | moderate | no | 7 | n.g. | no |
| 35 | Kiriscioglu et al. [50] | 2019 | w | 34 ± 9 | 25.3 7 | moderate | no | 0 | 95 | no |
| 36 | Konrad et al. [51] | 2020 | m + w | 56 ± 14 | n.g. | untrained | yes | 27 | 85 | no |
| 37 | Ludwig et al. [52] | 2019 | m + w | 25 ± 4 | 23.9 | moderate | no | 10 | 100 | no |
| 38 | Lukashevich et al. [53] | 2020 | w | 45–65 | n.g. | untrained | yes | n.g. | n.g. | no |
| 39 | Matsumoto et al. [54] | 2020 | m + w | 66 ± 6 | 24.0 | untrained | yes | n.g. | n.g. | no |
| 40 | Matsuo et al. [55] | 2022 | m + w | 77 ± 11 | 24.0 | untrained | yes | 6 | 94 | no |
| 41 | Micke et al. [56] | 2021 | m + w | 40–70 | 26.3 | moderate | yes | 9 | 92 | no |
| 42 | Miyamoto et al. [57] | 2016 | m | 22 ± 2 | 21.4 | moderate | no | 0 | n.g. | no |
| 43 | Mori et al. [58] | 2020 | m | 65 ± 13 | n.g. | untrained | yes | n.g. | n.g. | n.g. |
| 44 | Müllerova et al. [59] | 2022 | w | 63 ± 2 | 26.6 | untrained | no | 18 | n.g. | n.g. |
| 45 | Nakamura et al. [60] | 2019 | m + w | 76 ± 12 | 21.0 | untrained | yes | 55 | 100 | no |
| 46 | Nakamura et al. [61] | 2021 | m + w | 68 ± 15 | 21.4 | untrained | yes | 17 | 100 | n.g. |
| 47 | Nejad et al. [62] | 2021 | w | 60–70 | 28.2 | untrained | no | n.g. | n.g. | n.g. |
| 48 | Noguchi et al. [63] | 2017 | m + w | 69 ± 10 | n.g. | untrained | yes | 0 | no | |
| 49 | Nonoyama et al. [64] | 2022 | m + w | 72–84 | 24.4 | untrained | yes | n.g. | 97 | no |
| 50 | Ochiai et al. [65] | 2018 | m + w | 60–90 | n.g. | untrained | yes | 0 | n.g. | no |
| 51 | Özdal et al. [67] | 2016 | w | 32 ± 8 | 24.5 | untrained | no | 0 | n.g. | no |
| 52 | Öktem et al. [66] | 2022 | W | 22–27 | 23.6 | untrained | no | 0 | n.g. | no |
| 53 | Pano-Rodriguez et al. [68] | 2020 | w | 61 ± 4 | 26.5 | untrained | no | 6 | 93 | no |
| 54 | Park et al. [71] | 2021 | w | 70 ± 4 | 27.5 | untrained | yes | 6 | 100 | no |
| 55 | Park et al. [70] | 2021 | w | 61–79 | 24.4 | untrained | yes | 7 | 92 | no |
| 56 | Park et al. [69] | 2021 | w | 20–40 | 25.0 | untrained | no | 8 | 100 | no |
| 57 | Park et al. [72] | 2023 | W | ≥65 | 25.4 | untrained | No 8 | 3 | 97 | no |
| 58 | Qin et al. [73] | 2022 | m | 25 ± 4 | 24.0 | well | no | 15 | 100 | no |
| 59 | Reljic et al. [74] | 2022 | m + w | ≥18 | 37.2 | moderate | yes | 23 | 93 | no |
| 60 | Ricci et al. [75] | 2020 | m + w | 32–45 | 38.2 | moderate | yes | 0 | 100 | no |
| 61 | Richter et al. [76] | 2019 | m + w | ≥18 | 25.5 | untrained | yes | 19 | 88 | 0 |
| 62 | Sadeghipour et al. [78] | 2021 | w | 26 ± 2 | 21.7 | well | no | 0 | n.g. | n.g. |
| 63 | Sadeghipour et al. [77] | 2022 | w | 32 ± 5 | 27.8 | moderate | no | n.g. | 100 | no |
| 64 | Sanchez-Infante et al. [79] | 2020 | w | 40–60 | 25.5 | moderate | no | 0 | 100 | no |
| 65 | Schink et al. [80] | 2018 | m + w | ≥18 | 25.2 | untrained | yes | 40 | 87 | no |
| 66 | Schink et al. [81] | 2018 | m + w | ≥18 | 25.4 | untrained | yes | 59 | 77 | no |
| 67 | Schwappacher et al. [82] | 2020 | m | ≥18 | 28.0 | untrained | yes | n.g. | 88 | no |
| 68 | Schwappacher et al. [82] | 2020 | m + w | ≥18 | 26.8 | untrained | yes | n.g. | 85 | no |
| 69 | Schwappacher et al. [83] | 2021 | m + w | >18 | 24.6 | untrained | yes | n.g. | 79 | no |
| 70 | Silvestri et al. [84] | 2023 | m + w | 43–81 | 24.3 | untrained | yes | 23 | 91 | no |
| 71 | Song et al. [85] | 2020 | W | 20–25 4 | 26.1 | n.g. | no | n.g. | n.g. | no |
| 72 | Stephan et al. [86] | 2023 | m + w | 25–36 | 25.3 | untrained | no | 7 | 80 | no |
| 73 | Struhar et al. [87] | 2019 | w | 23 ± 2 | 23.2 | untrained | no | n.g. | n.g. | n.g. |
| 74 | Suzuki et al. [88] | 2018 | m + w | 65 ± 7 | 23.7 | n.g. | yes | 13 | 98 | no |
| 75 | Suzuki. et al. [89] | 2018 | m + w | 66 ± 10 | 26.7 | untrained | yes | 0 | n.g. | no |
| 76 | Tanaka et al. [90] | 2022 | m + w | >75 | 21.6 | untrained | yes | 25 | 86 | no |
| 77 | Teschler et al. [92] | 2016 | m | 20–50 | 24.9 | well | no | 0 | 100 | Yes 9 |
| 78 | Teschler et al. [91] | 2021 | m + w | 56 ± 7 | 35.7 | moderate | yes | 4 | 98 | no |
| 79 | Tsurumi et al. [93] | 2022 | m + w | 74 ± 5 | 22.7 | untrained | yes | 27 | n.g. | n.g. |
| 80 | Vacoulikova et al. [94] | 2021 | w | 60–65 | 27.1 | untrained | no | n.g. | 81 | no |
| 81 | Vacoulikova et al. [95] | 2021 | w | 60–65 | 27.0 | untrained | yes | 18 | 100 | no |
| 82 | van Buuren et al. [97] | 2014 | m + w | 61 ± 13 | 29.7 | untrained | yes | 0 | 100 | no |
| 83 | van Buuren et al. [96] | 2015 | m + w | 62 ± 3 | 34.6 | untrained | yes | 0 | 100 | no |
| 84 | von Stengel et al. [98] | 2015 | w | >70 | 22.2 | untrained | yes | 16 | 79 | no |
| 85 | Weissenfels et al. [99] | 2018 | m + w | 57 ± 7 | 27.9 | moderate | yes | 7 | 93 | no |
| 52 | Willert et al. [100] | 2019 | w | 25–50 | 31.3 | moderate | yes | 3 | 100 | no |
| 67 | Zink et al. [101] | 2021 | m | 18–70 | 27.4 | moderate | no | 33 | 95 | no |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beier, M.; Schoene, D.; Kohl, M.; von Stengel, S.; Uder, M.; Kemmler, W. Non-Athletic Cohorts Enrolled in Longitudinal Whole-Body Electromyostimulation Trials—An Evidence Map. Sensors 2024, 24, 972. https://doi.org/10.3390/s24030972
Beier M, Schoene D, Kohl M, von Stengel S, Uder M, Kemmler W. Non-Athletic Cohorts Enrolled in Longitudinal Whole-Body Electromyostimulation Trials—An Evidence Map. Sensors. 2024; 24(3):972. https://doi.org/10.3390/s24030972
Chicago/Turabian StyleBeier, Miriam, Daniel Schoene, Matthias Kohl, Simon von Stengel, Michael Uder, and Wolfgang Kemmler. 2024. "Non-Athletic Cohorts Enrolled in Longitudinal Whole-Body Electromyostimulation Trials—An Evidence Map" Sensors 24, no. 3: 972. https://doi.org/10.3390/s24030972
APA StyleBeier, M., Schoene, D., Kohl, M., von Stengel, S., Uder, M., & Kemmler, W. (2024). Non-Athletic Cohorts Enrolled in Longitudinal Whole-Body Electromyostimulation Trials—An Evidence Map. Sensors, 24(3), 972. https://doi.org/10.3390/s24030972