
Comparison of ECG Saline-Conduction Technique and ECG Wire-Based Technique for Peripherally Inserted Central Catheter Insertion: A Randomized Controlled Trial


Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. PICC Placement
2.3. Wire-Based Technique (WT)
2.4. Saline Conduction Technique (ST)
2.5. Data Collection and Statistical Analysis
3. Results
4. Discussion
4.1. Navigation Capacities
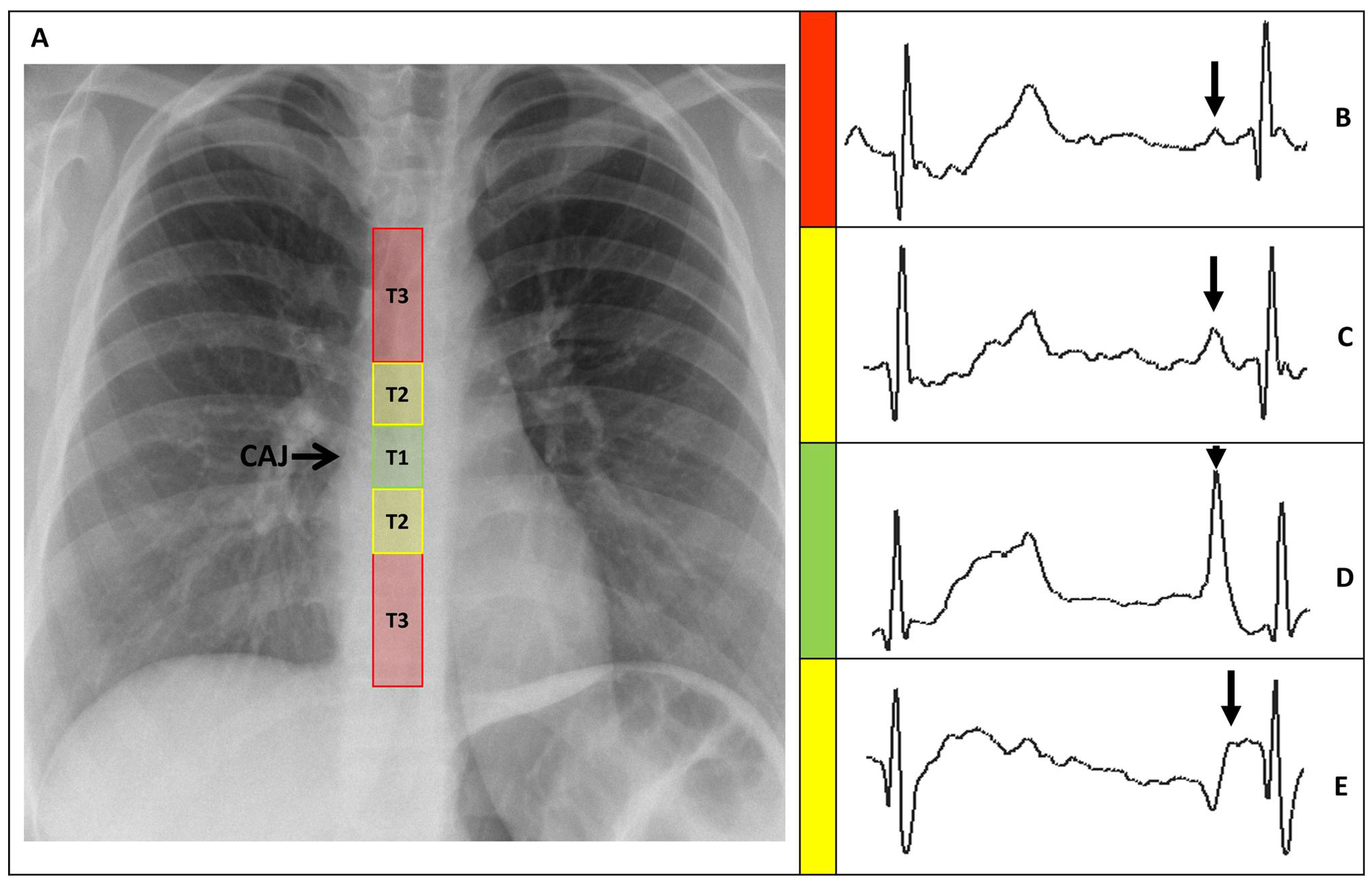
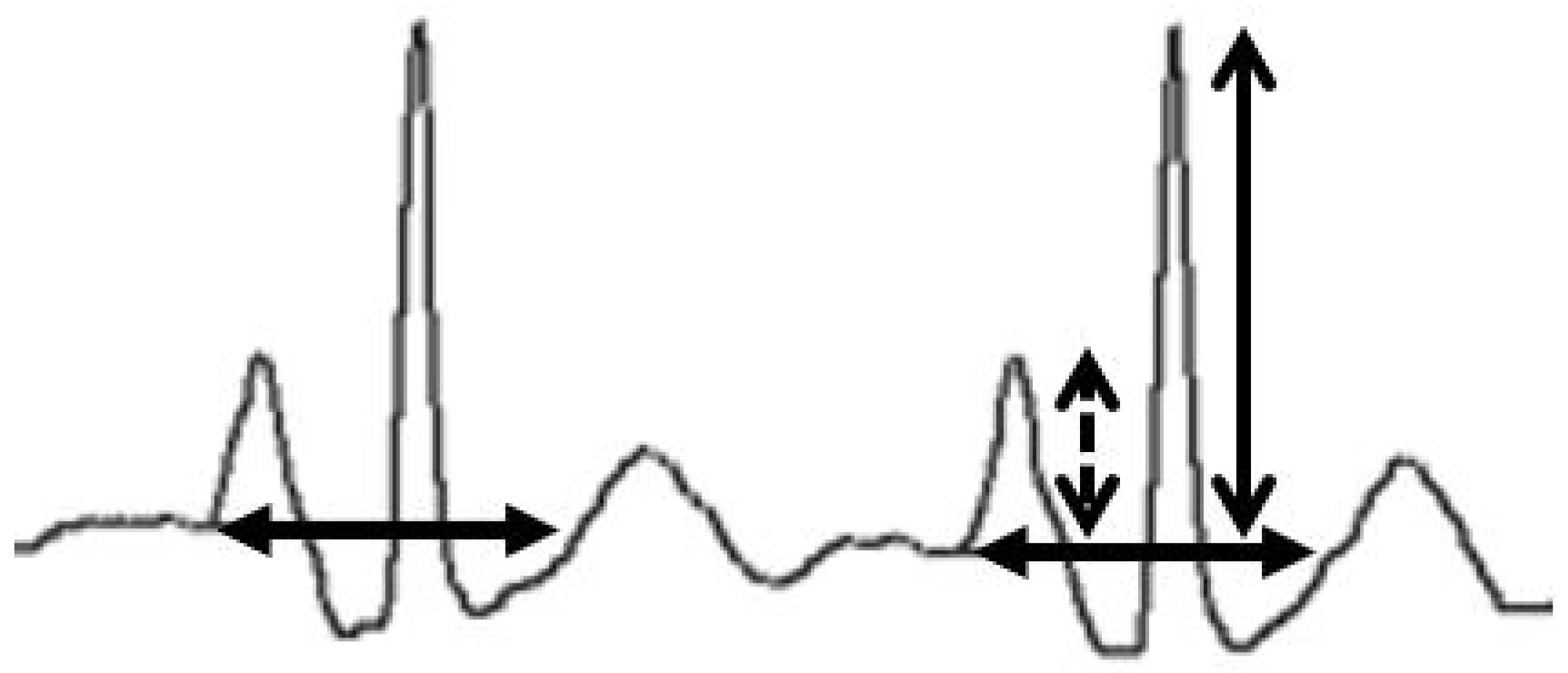
4.2. Positioning Capacities
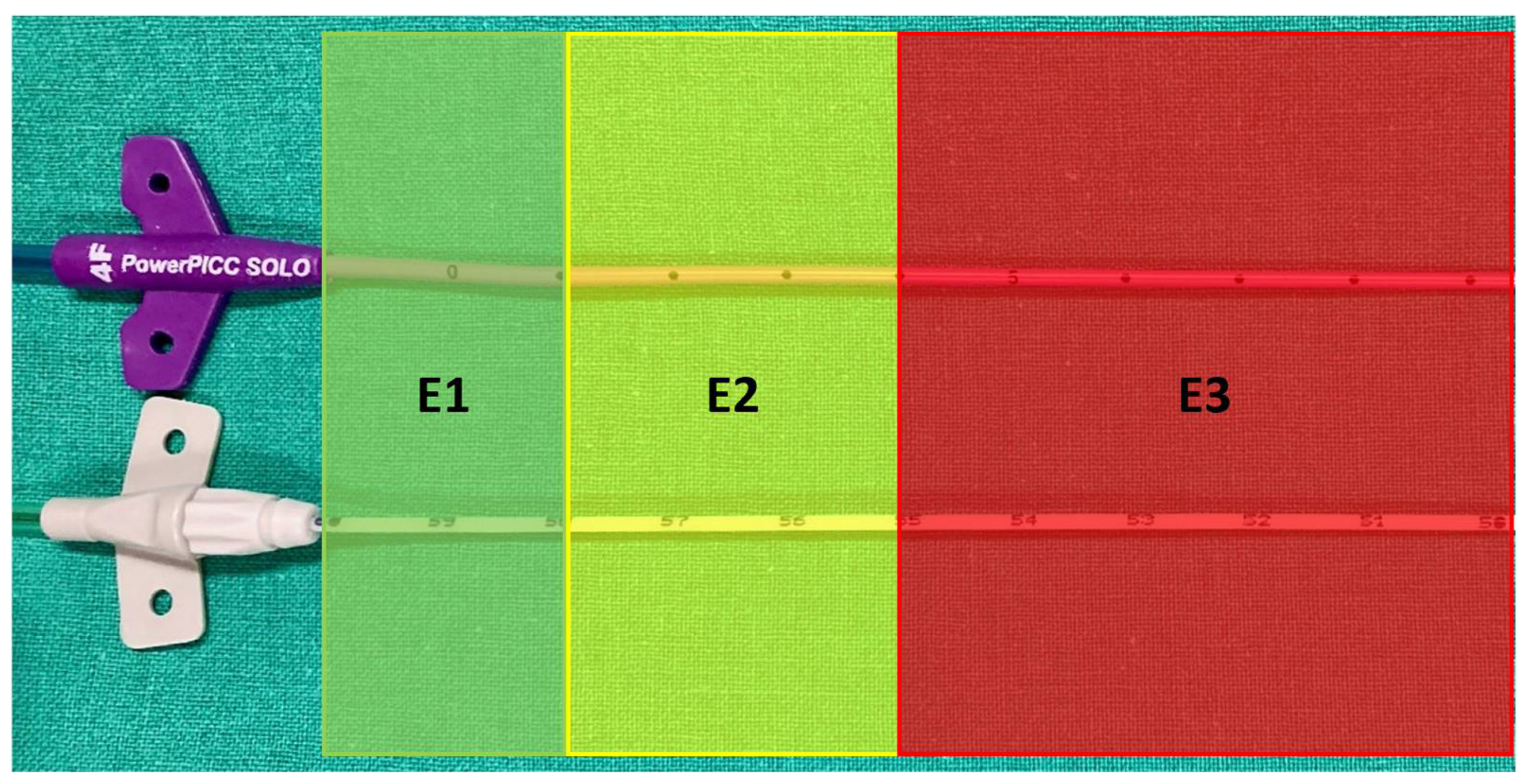
4.3. Hemostasis and Extracorporeal Catheter at Insertion Point
4.4. Accessibility and Usability
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bleichröder, F. Intraarterielle Therapie. Berl. Klin. Wochenschr. 1912, 49, 1504. [Google Scholar]
- Hellerstein, H.K.; Pritchard, W.H.; Lewis, R.L. Recording of Intracavity Potentials through a Single Lumen, Saline Filled Cardiac Catheter. Proc. Soc. Exp. Biol. Med. 1949, 71, 58–61. [Google Scholar] [CrossRef]
- Kisch, B.; Schwartz, B.M. A Method of Obtaining Intracardial Electrograms during Cardiac Catheterization. J. Mt. Sinai Hosp. N. Y. 1948, 15, 257–259. [Google Scholar]
- Cavatorta, F.; Zollo, A.; Galli, S.; Dionisio, P. Central Venous Catheter Placement in Hemodialysis: Evaluation of Electrocardiography Using a Guide-Wire. J. Vasc. Access 2001, 2, 45–50. [Google Scholar] [CrossRef]
- Pittiruti, M.; Scoppettuolo, G.; La Greca, A.; Emoli, A.; Brutti, A.; Migliorini, I.; Dolcetti, L.; Taraschi, C.; De Pascale, G. The EKG Method for Positioning the Tip of PICCs: Results from Two Preliminary Studies. J. Assoc. Vasc. Access 2008, 13, 179–186. [Google Scholar] [CrossRef]
- Duszak, R.; Bilal, N.; Picus, D.; Hughes, D.R.; Xu, B.J. Central Venous Access: Evolving Roles of Radiology and Other Specialties Nationally over Two Decades. J. Am. Coll. Radiol. JACR 2013, 10, 603–612. [Google Scholar] [CrossRef]
- Dale, M.; Higgins, A.; Carolan-Rees, G. Sherlock 3CG® Tip Confirmation System for Placement of Peripherally Inserted Central Catheters: A NICE Medical Technology Guidance. Appl. Health Econ. Health Policy 2015, 14, 41–49. [Google Scholar] [CrossRef]
- Chopra, V.; Kuhn, L.; Ratz, D.; Winter, S.; Carr, P.J.; Paje, D.; Krein, S.L. Variation in Use of Technology among Vascular Access Specialists: An Analysis of the PICC1 Survey. J. Vasc. Access 2017, 18, 243–249. [Google Scholar] [CrossRef]
- Caers, J.; Fontaine, C.; Vinh-Hung, V.; De Mey, J.; Ponnet, G.; Oost, C.; Lamote, J.; De Greve, J.; Van Camp, B.; Lacor, P. Catheter Tip Position as a Risk Factor for Thrombosis Associated with the Use of Subcutaneous Infusion Ports. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2005, 13, 325–331. [Google Scholar] [CrossRef]
- Meyer, B.M. Managing Peripherally Inserted Central Catheter Thrombosis Risk: A Guide for Clinical Best Practice. J. Assoc. Vasc. Access 2011, 16, 144–147. [Google Scholar] [CrossRef]
- Gapp, J.; Krishnan, M.; Ratnaraj, F.; Schroell, R.P.; Moore, D. Cardiac Arrhythmias Resulting from a Peripherally Inserted Central Catheter: Two Cases and a Review of the Literature. Cureus 2017, 9, e1308. [Google Scholar] [CrossRef]
- Orme, R.M.L.; McSwiney, M.M.; Chamberlain-Webber, R.F.O. Fatal Cardiac Tamponade as a Result of a Peripherally Inserted Central Venous Catheter: A Case Report and Review of the Literature. Br. J. Anaesth. 2007, 99, 384–388. [Google Scholar] [CrossRef]
- Liu, G.; Hou, W.; Zhou, C.; Yin, Y.; Lu, S.; Duan, C.; Li, M.; Toft, E.S.; Zhang, H. Meta-Analysis of Intracavitary Electrocardiogram Guidance for Peripherally Inserted Central Catheter Placement. J. Vasc. Access 2019, 20, 577–582. [Google Scholar] [CrossRef]
- Gullo, G.; Qanadli, S.D. ECG-Based Techniques to Optimize Peripherally Inserted Central Catheters: Rationale for Tip Positioning and Practical Use. Front. Cardiovasc. Med. 2022, 9, 765935. [Google Scholar] [CrossRef]
- Gullo, G.; Colin, A.; Frossard, P.; Jouannic, A.M.; Knebel, J.F.; Qanadli, S.D. Appropriateness of Replacing Fluoroscopic Guidance With ECG-Electromagnetic Guidance for PICC Insertion: A Randomized Controlled Trial. AJR Am. J. Roentgenol. 2021, 216, 981–988. [Google Scholar] [CrossRef]
- Johnston, A.J.; Holder, A.; Bishop, S.M.; See, T.C.; Streater, C.T. Evaluation of the Sherlock 3CG Tip Confirmation System on Peripherally Inserted Central Catheter Malposition Rates. Anaesthesia 2014, 69, 1322–1330. [Google Scholar] [CrossRef]
- BARD, C.R. Bard PowerPICC SOLO2. Polyurethane Valved PICC IFU. Available online: https://www.bd.com/en-us/resource-and-education/documentation-landing-page?associatedProductBrands_fullstring=PowerPICC+SOLO%E2%84%A2&associatedProductCategories_fullstring=I.R.+PICC+catheters&associatedProductFamilies_fullstring=PowerPICC+SOLO%E2%84%A2+2+Catheter%2C+I.R.&lastUpdate=all-dates (accessed on 22 June 2022).
- Dong, H.-M.; Zhu, Y.-X.; Yin, X.-X.; Zhang, X. Clinical Significance of Different Atlas of Intracavitary Electrocardiogram for PICC Localization in 961 Cases. Ann. Noninvasive Electrocardiol. 2021, 27, e12904. [Google Scholar] [CrossRef]
- Smith, S.L.; Albin, M.S.; Ritter, R.R.; Bunegin, L. CVP Catheter Placement from the Antecubital Veins Using a J-Wire Catheter Guide. Anesthesiology 1984, 60, 238–240. [Google Scholar] [CrossRef]
- Yin, Y.-X.; Gao, W.; Li, X.-Y.; Lu, W.; Deng, Q.-H.; Zhao, C.-Y.; Liu, X.-R.; Cao, M.-K.; Wang, L.-N.; Zhang, H.-J. Randomized Multicenter Study on Long-Term Complications of Peripherally Inserted Central Catheters Positioned by Electrocardiographic Technique. Phlebology 2020, 35, 614–622. [Google Scholar] [CrossRef]
- Pittiruti, M.; Bertollo, D.; Briglia, E.; Buononato, M.; Capozzoli, G.; De Simone, L.; La Greca, A.; Pelagatti, C.; Sette, P. The Intracavitary ECG Method for Positioning the Tip of Central Venous Catheters: Results of an Italian Multicenter Study. J. Vasc. Access 2012, 13, 357–365. [Google Scholar] [CrossRef]
- Kremser, J.; Kleemann, F.; Reinhart, K.; Schummer, W. Optimized Method for Correct Left-Sided Central Venous Catheter Placement under Electrocardiographic Guidance. Br. J. Anaesth. 2011, 107, 567–572. [Google Scholar] [CrossRef]
- Wang, D.; Niu, F.; Gao, H.; Yu, M.; Li, Y.; Xu, L.; Cao, H.; Wang, L.; Liu, J.; Ding, X.; et al. Influence of Guide Wire Removal on Tip Location in Peripherally Inserted Central Catheters (PICCs): A Retrospective Cross-Sectional Study. BMJ Open 2019, 9, e027278. [Google Scholar] [CrossRef]
- Baxi, S.M.; Shuman, E.K.; Scipione, C.A.; Chen, B.; Sharma, A.; Rasanathan, J.J.K.; Chenoweth, C.E. Impact of Postplacement Adjustment of Peripherally Inserted Central Catheters on the Risk of Bloodstream Infection and Venous Thrombus Formation. Infect. Control Hosp. Epidemiol. 2013, 34, 785–792. [Google Scholar] [CrossRef]
- Cales, Y.K.; Rheingans, J.; Steves, J.; Moretti, M. Electrocardiogram-Guided Peripherally Inserted Central Catheter Tip Confirmation Using a Standard Electrocardiogram Machine and a Wide-Mouth Electrocardiogram Clip Compared with Traditional Chest Radiograph. J. Assoc. Vasc. Access 2016, 21, 44–54. [Google Scholar] [CrossRef]
- Cheng, K.I.; Chu, K.S.; Chen, L.T.; Tang, C.S. Correct Positioning of the Venous Port-a-Cath Catheter: Comparison of Intravascular Electrocardiography Signal from Guidewire and Sodium Bicarbonate Flushed Catheter. Anaesth. Intensive Care 2002, 30, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Pawlik, M.T.; Lemberger, P.; Hansen, E. Evaluation eines ZVK-Komplett-Sets. AINS—Anästhesiol. Intensivmed. Notfallmedizin Schmerzther. 2006, 41, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Ling, Q.; Chen, H.; Tang, M.; Qu, Y.; Tang, B. Accuracy and Safety Study of Intracavitary Electrocardiographic Guidance for Peripherally Inserted Central Catheter Placement in Neonates. J. Perinat. Neonatal Nurs. 2019, 33, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.; Neuharth, R.M.; Hendrix, M.A.; McDonnall, D.; Michaels, A.D. Intravenous Electrocardiographic Guidance for Placement of Peripherally Inserted Central Catheters. J. Electrocardiol. 2010, 43, 274–278. [Google Scholar] [CrossRef]
- Pawlik, M.T.; Kutz, N.; Keyl, C.; Lemberger, P.; Hansen, E. Central Venous Catheter Placement: Comparison of the Intravascular Guidewire and the Fluid Column Electrocardiograms. Eur. J. Anaesthesiol. 2004, 21, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Xu, R.; Fan, D. Clinical Application of Electrocardiogram-Guided Tip Positioning in Peripheral Inserted Central Catheters Placement. J. Cancer Res. Ther. 2018, 14, 887–891. [Google Scholar] [CrossRef] [PubMed]
- Mazzola, J.R.; Schott-Baer, D.; Addy, L. Clinical Factors Associated with the Development of Phlebitis after Insertion of a Peripherally Inserted Central Catheter. J. Intraven. Nurs. Off. Publ. Intraven. Nurses Soc. 1999, 22, 36–42. [Google Scholar]
- Elli, S.; Bellani, G.; Cannizzo, L.; Giannini, L.; De Felippis, C.; Vimercati, S.; Madotto, F.; Lucchini, A. Reliability of Cutaneous Landmarks for the Catheter Length Assessment during Peripherally Inserted Central Catheter Insertion: A Retrospective Observational Study. J. Vasc. Access 2020, 21, 917–922. [Google Scholar] [CrossRef] [PubMed]
- Itkin, M.; Mondshein, J.I.; Stavropoulos, S.W.; Shlansky-Goldberg, R.D.; Soulen, M.C.; Trerotola, S.O. Peripherally Inserted Central Catheter Thrombosis—Reverse Tapered versus Nontapered Catheters: A Randomized Controlled Study. J. Vasc. Interv. Radiol. 2014, 25, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Simonova, G.; Rickard, C.M.; Dunster, K.R.; Smyth, D.J.; McMillan, D.; Fraser, J.F. Cyanoacrylate Tissue Adhesives—Effective Securement Technique for Intravascular Catheters: In Vitro Testing of Safety and Feasibility. Anaesth. Intensive Care 2012, 40, 460–466. [Google Scholar] [CrossRef]
- Pittiruti, M.; Scoppettuolo, G.; Dolcetti, L.; Emoli, A. Clinical Use of Sherlock-3CG® for Positioning Peripherally Inserted Central Catheters. J. Vasc. Access 2019, 20, 356–361. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Saline (n = 160) | Wire (n = 159) | p Value |
|---|---|---|---|
| Demographics | |||
| Men | 96 (60) | 98 (61.6) | 0.819 |
| Age (years) | 62.08 ± 15.3 {25–97} | 61.01 ± 16.0 {18–93} | 0.768 |
| Anatomical considerations | |||
| Left arm access | 113 (70.6) | 109 (68.6) | 0.716 |
| Basilic vein access | 107 (66.9) | 104 (65.4) | 0.814 |
| Therapeutic indications | |||
| Antibiotic therapy | 115 (71.9) | 155 (72.3) | |
| Repeated blood draws/Low venous capital | 14 (8.8) | 8 (5.0) | |
| Chemotherapy | 12 (7.5) | 21 (13.2) | |
| Parenteral nutrition | 13 (8.1) | 7 (4.4) | |
| Other | 6 (3.8) | 8 (5.0) | 0.189 |
| Procedural Assessment | Saline | Wire | p Value | |
|---|---|---|---|---|
| Analyzed patients | 160 | 159 | ||
| Technical Success | 160 (100) | 159 (99.4) | 1.000 | |
| J wire assistance | 12 (7.5) | 4 (2.5) | 0.070 | |
| Analyzed patients | 160 | 159 | ||
| Procedure duration (min) | 40.3 ± 8.0 {23–67} | 36.1 ± 7.2 {18–54} | <0.001 | |
| Analyzed patients | 147 | 145 | ||
| Intraprocedural recut | 0 (0) | 80 (55.2) {0–11} | <0.001 | |
| Placement side | Wire left side | Wire right side | ||
| Analyzed patients | N/A | 99 | 46 | |
| Intraprocedural recut | N/A | 48 (48.5) | 32 (69.6) | 0.018 |
| Analyzed patients | 147 | 130 | ||
| Wave ratio (P wave/QRS complex) | 87.1 ± 40.3 {13.3–247.3} | 81.5 ± 37.3 {18.8–224.1} | 0.124 | |
| Combined | 84.45 ± 38.9 | |||
| P5 * | 39.05 | |||
| P10 * | 46.16 | |||
| P25 * | 59.54 | |||
| P50 * | 78.13 | |||
| Procedure Assessment | Saline | Wire | p Value |
|---|---|---|---|
| Analyzed patients | 160 | 159 | |
| Navigation and localization success | |||
| T1 | 58 (36.3) | 76 (47.8) | |
| T2 | 89 (55.6) | 69 (43.4) | |
| T3 | 13 (8.1) | 14 (8.8) | 0.083 |
| Analyzed patients | 160 | 159 | |
| Supplementary actions | |||
| None | 147 (91.9) | 145 (91.2) | |
| Repositioning | 3 (1.9) | 6 (3.8) | |
| Recut | 10 (6.2) | 8 (5.0) | 0.522 |
| Analyzed patients (T1-T2 classes) | 147 | 145 | |
| DCAJ distance | |||
| Absolute distance (cm) | 1.36 ± 0.86 | 1.12 ± 0.80 | 0.012 |
| 95% CI | 1.22–1.50 | 0.98–1.25 | |
| range | 0 to 3 | 0 to 2.9 | |
| Analyzed patients (T1-T2 classes) | 143 | 142 | |
| Pull-out distance | |||
| Distance (mm) | 17.5 ± 9.51 | 15.81 ± 7.55 | 0.207 |
| 95% CI | 0.107–0.386 | −0.08–0.181 | |
| range | 5–50 | 5–40 | |
| Combined | 16.6 ± 8.6 | ||
| Assessment | Saline (n = 147) | Wire (n = 145) | p Value |
|---|---|---|---|
| Hemostasis | |||
| Direct | 74 (50.3) | 120 (82.8) | |
| Delayed | 73 (49.7) | 25 (17.2) | <0.001 |
| Extracorporeal catheter section, before recut (first insertion) | |||
| E1 | 147 (100) | 40 (27.6) | |
| E2 | 0 (0) | 56 (38.6) | |
| E3 | 0 (0) | 49 (33.8) | <0.001 |
| Absolute length (cm) | 0.01 ± 0.116 | 4.36 ± 2.45 | <0.001 |
| 95% CI | −0.005–0.03 | 3.96–4.76 | |
| range | 0–1 | 0–11 | |
| Extracorporeal catheter section, after recut | |||
| E1 | 147 (100) | 116 (80) | |
| E2 | 0 (0) | 29 (20) | <0.001 |
| Absolute length (cm) | 0.01 ± 0.12 | 1.61 ± 1.00 | <0.001 |
| 95% CI | −0.005–0.03 | 1.44–1.77 | |
| range | 0–1 | 0–4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gullo, G.; Frossard, P.; Colin, A.; Qanadli, S.D. Comparison of ECG Saline-Conduction Technique and ECG Wire-Based Technique for Peripherally Inserted Central Catheter Insertion: A Randomized Controlled Trial. Sensors 2024, 24, 894. https://doi.org/10.3390/s24030894
Gullo G, Frossard P, Colin A, Qanadli SD. Comparison of ECG Saline-Conduction Technique and ECG Wire-Based Technique for Peripherally Inserted Central Catheter Insertion: A Randomized Controlled Trial. Sensors. 2024; 24(3):894. https://doi.org/10.3390/s24030894
Chicago/Turabian StyleGullo, Giuseppe, Pierre Frossard, Anaïs Colin, and Salah Dine Qanadli. 2024. "Comparison of ECG Saline-Conduction Technique and ECG Wire-Based Technique for Peripherally Inserted Central Catheter Insertion: A Randomized Controlled Trial" Sensors 24, no. 3: 894. https://doi.org/10.3390/s24030894
APA StyleGullo, G., Frossard, P., Colin, A., & Qanadli, S. D. (2024). Comparison of ECG Saline-Conduction Technique and ECG Wire-Based Technique for Peripherally Inserted Central Catheter Insertion: A Randomized Controlled Trial. Sensors, 24(3), 894. https://doi.org/10.3390/s24030894