

Physical Frailty Prediction Using Cane Usage Characteristics during Walking


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
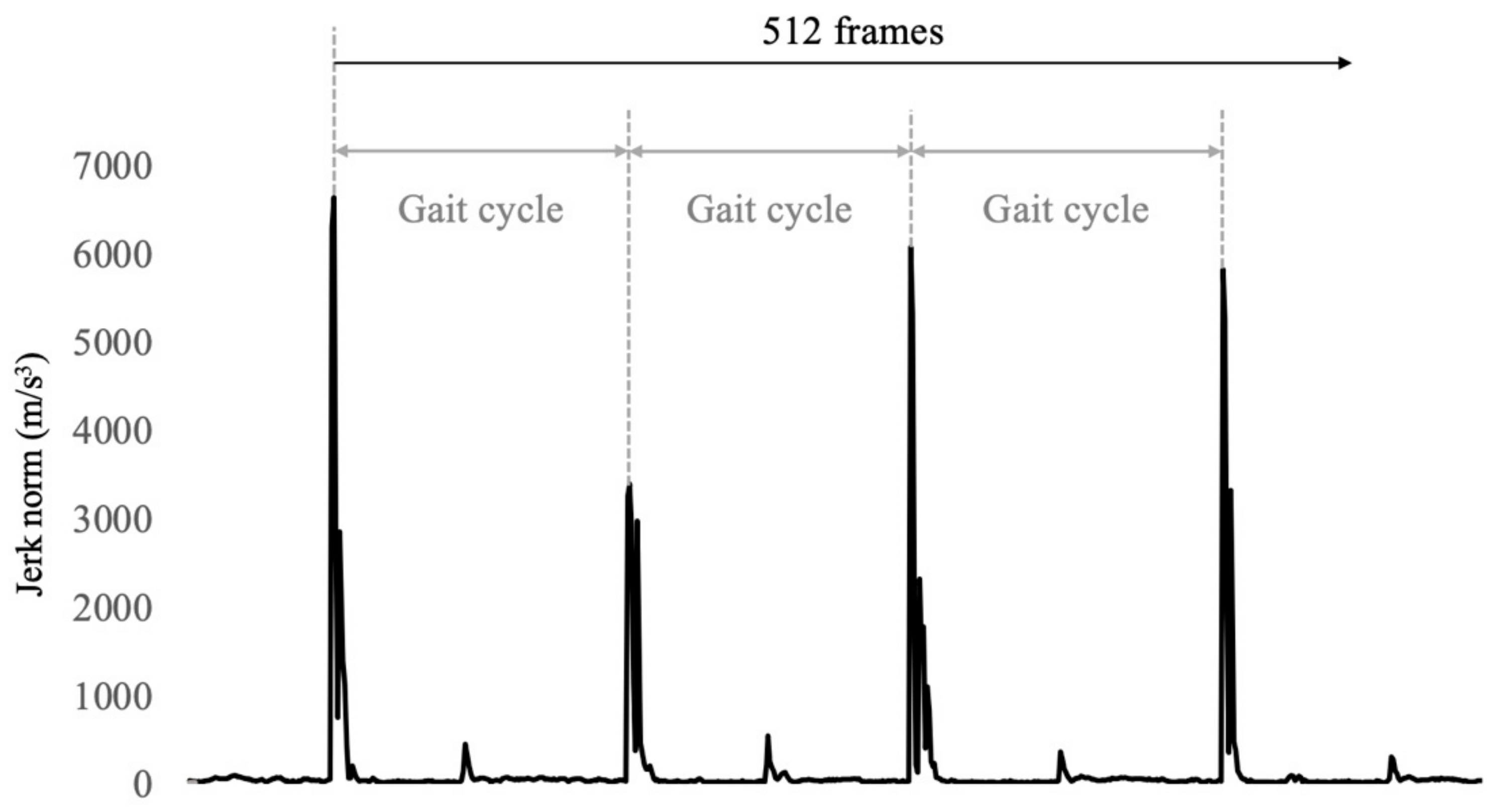
2.3. Data Analysis
2.4. Frailty Assessment
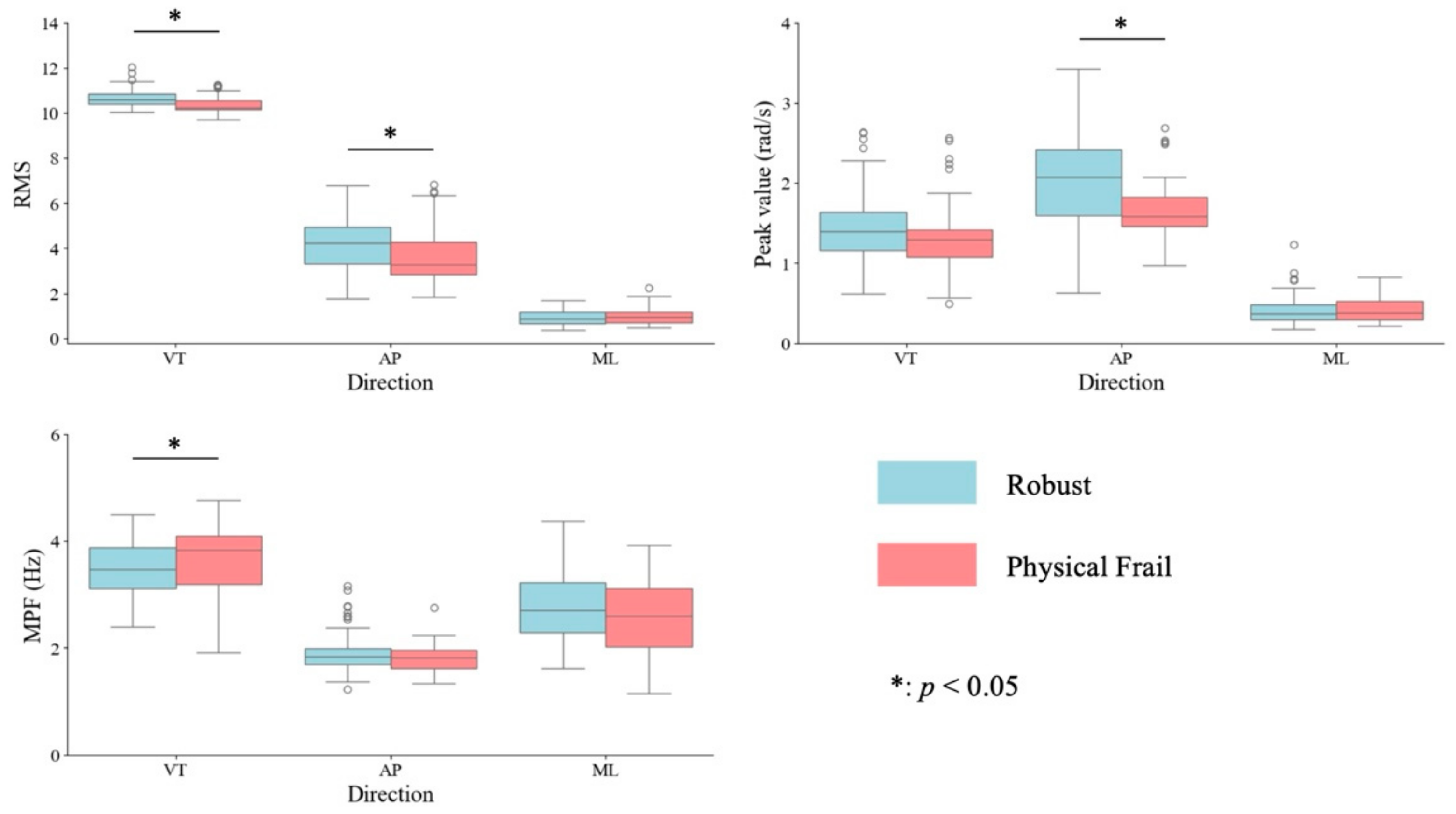
2.5. Statistical Analysis
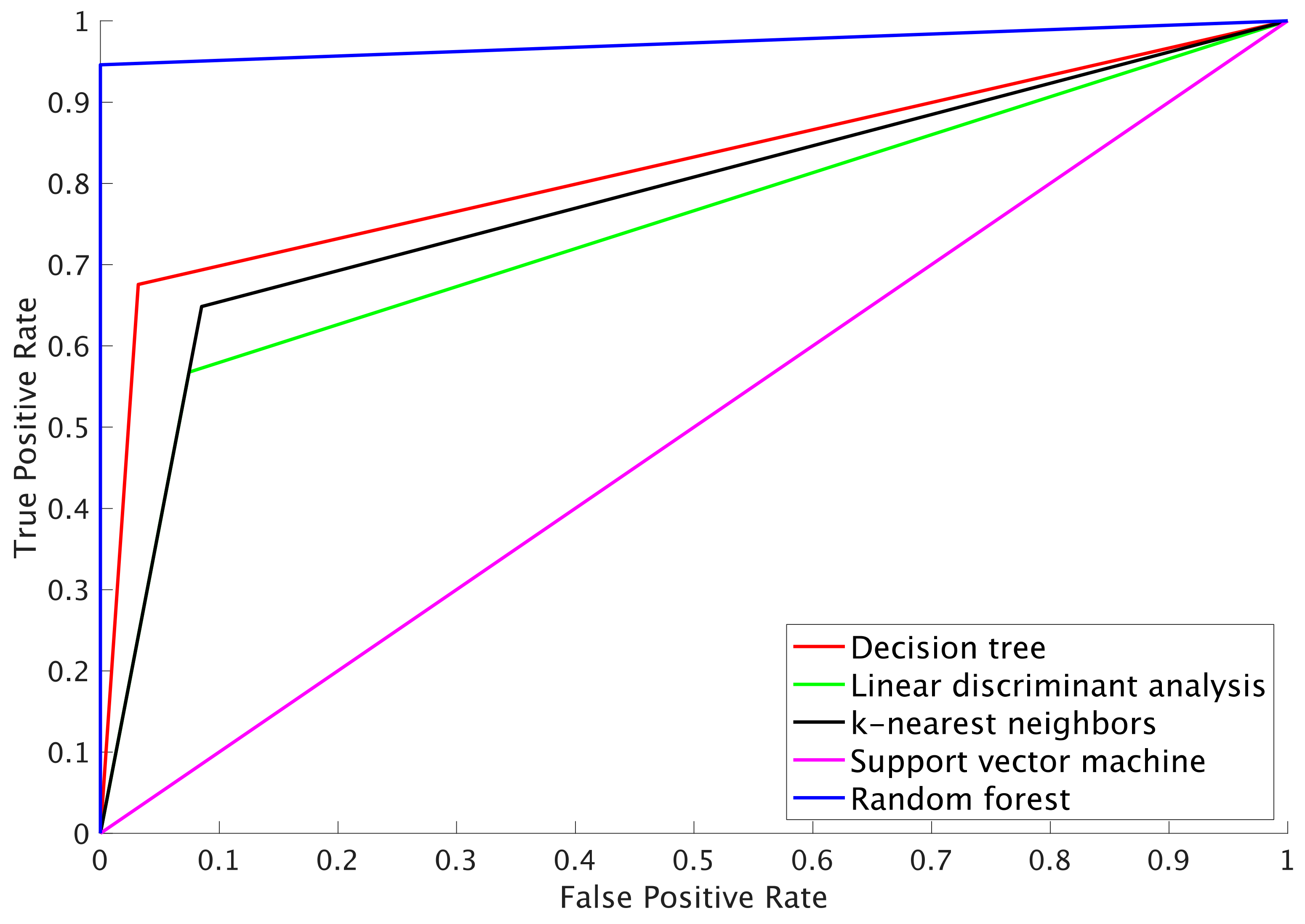
- DT: A simple and highly interpretable model that allows for a visual understanding of feature importance. In this study, the number of splits was set to 5.
- LDA: Used to evaluate whether the data are linearly separable. LDA is computationally efficient and effective when strong linear relationships are present.
- k-NN: A non-parametric method that is well suited to capturing local patterns in the data. It directly leverages similarities between different physical frailty states. The datasets were normalized to z-scores for this model.
- SVM: Capable of handling non-linear data and effective in classifying high-dimensional data. Using a Gaussian kernel, it can effectively classify data with complex boundaries. The datasets were normalized to z-scores for this model as well.
- RF: An ensemble learning method that helps prevent overfitting and offers high classification performance. It also enables the evaluation of feature importance. In this study, the ensemble method was performed using the following parameters: LogitBoost as the method, 243 learning cycles, and a learning rate of 0.59256. This ensemble model combines multiple weak learners to improve classification performance.
3. Results
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Annual Report on the Ageing Society. Available online: https://www8.cao.go.jp/kourei/whitepaper/index-w.html (accessed on 20 May 2024).
- Watanabe, D.; Yoshida, T.; Watanabe, Y.; Yamada, Y.; Miyachi, M.; Kimura, M. Validation of the Kihon Checklist and the frailty screening index for frailty defined by the phenotype model in older Japanese adults. BMC Geriatr. 2022, 22, 478. [Google Scholar] [CrossRef] [PubMed]
- Satake, S.; Shimokata, H.; Senda, K.; Kondo, I.; Toba, K. Validity of total Kihon Checklist score for predicting the incidence of 3-year dependency and mortality in a community-dwelling older population. J. Am. Med. Dir. Assoc. 2017, 18, 552.e1–552.e6. [Google Scholar] [CrossRef] [PubMed]
- Hirashiki, A.; Shimizu, A.; Suzuki, N.; Nomoto, K.; Kokubo, M.; Hashimoto, K.; Sato, K.; Kondo, I.; Murohara, T.; Arai, H. Composite biomarkers for assessing frailty status in stable older adults with cardiovascular disease. Circ. Rep. 2022, 4, 123–130. [Google Scholar] [CrossRef]
- Arai, H.; Satake, S. English translation of the Kihon Checklist. Geriatr. Gerontol. Int. 2015, 15, 518–519. [Google Scholar] [CrossRef] [PubMed]
- Satake, S.; Senda, K.; Hong, Y.J.; Miura, H.; Endo, H.; Sakurai, T.; Kondo, I.; Toba, K. Validity of the Kihon Checklist for assessing frailty status. Geriatr. Gerontol. Int. 2016, 16, 709–715. [Google Scholar] [CrossRef]
- Fan, S.; Ye, J.; Xu, Q.; Peng, R.; Hu, B.; Pei, Z.; Yang, Z.; Xu, F. Digital health technology combining wearable gait sensors and machine learning improve the accuracy in prediction of frailty. Front. Public Health 2023, 11, 1169083. [Google Scholar] [CrossRef]
- Dang, D.C.; Suh, Y.S. Walking distance estimation using walking canes with inertial sensors. Sensors 2018, 18, 230. [Google Scholar] [CrossRef]
- Gill, S.; Seth, N.; Scheme, E. A multi-sensor matched filter approach to robust segmentation of assisted gait. Sensors 2018, 18, 2970. [Google Scholar] [CrossRef]
- Nohara, R.; Toda, H.; Tada, M.; Fujita, K. Relationship between walking ability and cane movement detectable by inertial sensors. Trans. Jpn. Soc. Med. Biol. Eng. 2021, 59, 14–23. [Google Scholar]
- Ribeiro, N.F.; Mouta, P.; Santos, C.P. Two kinematic data-based approaches for cane event detection. J. Ambient. Intell. Humaniz. Comput. 2023, 14, 567–579. [Google Scholar] [CrossRef]
- Gill, S.; Seth, N.; Scheme, E. A multi-sensor cane can detect changes in gait caused by simulated gait abnormalities and walking terrains. Sensors 2020, 20, 631. [Google Scholar] [CrossRef]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait speed and survival in older adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. Bull. World Health Organ. 2001, 79, 373. [Google Scholar]
- Antonsson, E.K.; Mann, R.W. The frequency content of gait. J. Biomech. 1985, 18, 39–47. [Google Scholar] [CrossRef]
- Sewo Sampaio, P.Y.; Sampaio, R.A.C.; Yamada, M.; Arai, H. Systematic review of the Kihon Checklist: Is it a reliable assessment of frailty? Geriatr. Gerontol. Int. 2016, 16, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, S.S.; Wilk, M.B. An analysis of variance test for normality (complete samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Mann, H.B.; Whitney, D.R. On a test of whether one of two random variables is stochastically larger than the other. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013. [Google Scholar]
- Imura, T.; Toda, H.; Iwamoto, Y.; Inagawa, T.; Imada, N.; Tanaka, R.; Inoue, Y.; Araki, H.; Araki, O. Comparison of supervised machine learning algorithms for classifying home discharge possibility in convalescent stroke patients: A secondary analysis. J. Stroke Cerebrovasc. Dis. 2021, 30, 106011. [Google Scholar] [CrossRef]
- Kawai, H.; Obuchi, S.; Ejiri, M.; Ito, K. Association between daily life walking speed and frailty measured by a smartphone application: A cross-sectional study. BMJ Open 2023, 13, e065098. [Google Scholar] [CrossRef]
- Nilsson, J.; Thorstensson, A. Ground reaction forces at different speeds of human walking and running. Acta Physiol. Scand. 1989, 136, 217–227. [Google Scholar] [CrossRef]
- Kressig, R.W.; Gregor, R.J.; Oliver, A.; Waddell, D.; Smith, W.; O’Grady, M.; Curns, A.T.; Kutner, M.; Wolf, S.L. Temporal and spatial features of gait in older adults transitioning to frailty. Gait Posture 2004, 20, 30–35. [Google Scholar] [CrossRef]
- Espy, D.D.; Yang, F.; Bhatt, T.; Pai, Y.C. Independent influence of gait speed and step length on stability and fall risk. Gait Posture 2010, 32, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Stoffregen, T.A.; Pauelsen, M.; Jafari, H.; Strandkvist, V.; Nyberg, L.; Gustafsson, T.; Vikman, I.; Röijezon, U. Frequency domain shows: Fall-related concerns and sensorimotor decline explain inability to adjust postural control strategy in older adults. PLoS ONE 2020, 15, e0242608. [Google Scholar]
- Anzai, E.; Ren, D.; Cazenille, L.; Aubert-Kato, N.; Tripette, J.; Ohta, Y. Random forest algorithms to classify frailty and falling history in seniors using plantar pressure measurement insoles: A large-scale feasibility study. BMC Geriatr. 2022, 22, 746. [Google Scholar]
- Kraus, M.; Saller, M.M.; Baumbach, S.F.; Neuerburg, C.; Stumpf, U.C.; Böcker, W.; Keppler, A.M. Prediction of physical frailty in orthogeriatric patients using sensor insole-based gait analysis and machine learning algorithms: Cross-sectional study. JMIR Med. Inform. 2022, 10, e32724. [Google Scholar] [CrossRef]
- Park, C.; Mishra, R.; Sharafkhaneh, A.; Bryant, M.S.; Nguyen, C.; Torres, I.; Naik, A.D.; Najafi, B. Digital biomarker representing frailty phenotypes: The use of machine learning and sensor-based sit-to-stand test. Sensors 2021, 21, 3258. [Google Scholar] [CrossRef]
- Mandrekar, J.N. Receiver operating characteristic curve in diagnostic test assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef]
- Wade, J.W.; Boyles, R.; Flemming, P.; Sarkar, A.; De Riesthal, M.; Withrow, T.J.; Sarkar, N. Feasibility of automated mobility assessment of older adults via an instrumented cane. IEEE J. Biomed. Health Inform. 2019, 23, 1631–1638. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Physical Frail | Robust | p-Value | |
|---|---|---|---|---|
| Age (years) | 81.0 (7.5) | 85.0 (9.0) | 80.0 (7.5) | 0.063 |
| Sex, n (%) | ||||
| Male | 13 (28.2) | 4 (26.6) | 9 (30.0) | |
| Female | 32 (71.8) | 11 (73.4) | 21 (70.0) | |
| Height (m) | 1.53 (0.17) | 1.52(0.07) | 1.53 (0.12) | 0.238 |
| Weight (kg) | 50.5 (11.6) | 48.4 (20.6) | 51.0 (10.6) | 0.887 |
| BMI (kg/m2) | 22.3 (3.8) | 22.4 (3.7) | 22.5 (3.4) | 0.198 |
| Decision Tree | Linear Discriminant Analysis | k-Nearest Neighbors | Support Vector Machine | Random Forest | |
|---|---|---|---|---|---|
| Accuracy (%) | 78.6 | 73.3 | 73.3 | 71.8 | 76.3 |
| Precision (%) | 96.7 | 92.1 | 90.6 | 100 | 99 |
| Recall (%) | 87.5 | 82.8 | 88.9 | 71.8 | 97.8 |
| F1 score | 91.8 | 87.0 | 89.7 | 83.6 | 98.3 |
| AUC 1 | 0.81 | 0.72 | 0.81 | 0.5 | 0.96 |
| Decision Tree | Linear Discriminant Analysis | k-Nearest Neighbors | Support Vector Machine | Random Forest | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Actual | Actual | Actual | Actual | Actual | |||||||
| True | Negative | True | Negative | True | Negative | True | Negative | True | Negative | ||
| Predicted | True | 90.9 | 13.0 | 86.6 | 18.0 | 85.2 | 10.6 | 94.0 | 37.0 | 93.1 | 2.2 |
| Negative | 3.1 | 24.0 | 7.4 | 19.0 | 8.8 | 26.4 | 0.0 | 0.0 | 0.9 | 34.8 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toda, H.; Chin, T. Physical Frailty Prediction Using Cane Usage Characteristics during Walking. Sensors 2024, 24, 6910. https://doi.org/10.3390/s24216910
Toda H, Chin T. Physical Frailty Prediction Using Cane Usage Characteristics during Walking. Sensors. 2024; 24(21):6910. https://doi.org/10.3390/s24216910
Chicago/Turabian StyleToda, Haruki, and Takaaki Chin. 2024. "Physical Frailty Prediction Using Cane Usage Characteristics during Walking" Sensors 24, no. 21: 6910. https://doi.org/10.3390/s24216910
APA StyleToda, H., & Chin, T. (2024). Physical Frailty Prediction Using Cane Usage Characteristics during Walking. Sensors, 24(21), 6910. https://doi.org/10.3390/s24216910