1. Introduction
Damage to the upper motor neurons can lead to gait deficits, spasticity, or even full loss of motor function. Transcutaneous spinal cord stimulation (tSCS) constitutes a promising, noninvasive therapy option for these patients. Several studies describe a decrease in spasticity and even enhancement of voluntary movement through tSCS in patients with spinal cord injury [
1,
2,
3,
4,
5,
6]. Moreover, recent investigations have shown similar results in patients with multiple sclerosis (MS) [
7,
8], reporting a reduction in spasticity as well as an increase in gait velocity and improvement of postural stability.
For tSCS application, an adhesive hydrogel electrode on the lumbar spinal cord and counter electrodes on the abdomen or iliac crest conduct current through the upper body [
5]. The objective is to target large- to medium-diameter afferent nerve fibers within the posterior roots, which are known to have enhancing effects on motor control and inhibiting effects on lower limb spasticity [
6,
9]. Prior to the application of tSCS therapy, a suitable electrode position along the spine and a therapy intensity need to be identified individually for each patient. To prevent discomfort or pain during the therapy in patients with intact body sensation, an electrode location at which a preferably low current activates afferent fibers is desired. Typically, a calibration procedure is conducted using double stimulation pulses of increasing intensity while recording the electromyogram (EMG) of posterior root muscles (PRMs) in the legs. The EMG responses evoked by the first stimulus and their suppression after the second stimulus indicate the recruitment of afferents [
10]. The placement of the back electrode can then be adjusted in a manual trial-and-error manner [
8] or in an automated process [
11]. In the latter, the EMG responses are classified according to the amplitude of the response to the first and suppression characteristics of the response to the second stimulation pulse. The use of EMG sensors involves time-consuming skin preparation with disinfection and abrasive paste, as well as electrode placement for several leg muscles. This procedure is usually required to take place in an expert environment to position the sensors and interpret the signals (in the case of a manual procedure). Thus, current calibration approaches are not suitable for home use and continue to hold great potential for simplification.
In this paper, we introduce a concept for simplification and automation of the calibration procedure. With this novel approach, we strive to simplify the measurement setup by using mechanomyography (MMG) instead of EMGs. Mechanomyography describes the recording of mechanical muscular activity by means of accelerometers, piezoelectric sensors, or condenser microphones [
12]. The applications range from fatigue detection [
13,
14] and examination of neuromuscular disorders [
15] to prosthetic control [
16]. Furthermore, previous studies have investigated MMG signals in the context of electrical evoked muscle contractions [
17,
18].
In our approach, we use an accelerometer-based sensor setup for activity recordings of PRMs. The accelerometers are integrated in inertial sensors, also known as inertial measurement units (IMUs) or wearables. We propose a new stimulation procedure that differs from the exclusively EMG-based tuning. In addition to double stimuli, we also apply single-pulse stimulation. We subtract the MMG response of the single stimulus from the response of the double stimulus to extract the acceleration caused by the second pulse of the double stimuli. Such a procedure is necessary because acceleration responses take much longer than EMG responses and therefore overlap in the recordings.
Calibration procedures with healthy individuals and MS patients were conducted while recording EMG and acceleration data from selected PRMs. For the first time, we deployed a machine learning (ML) approach on these data in order to automatically classify the recorded acceleration when considering the EMG classes as ground truth. Not only do IMUs simplify the process, as no skin preparation and electrode placement is necessary, but they are also associated with ecological and economical advantages, as the time savings and simplification during the preparation process decrease demand for expert knowledge and the personnel expenses. Moreover, disposable materials as EMG electrodes are avoided, which decreases the long-term costs and improves sustainability.
2. Materials and Methods
The presented approach involved several steps, which we describe extensively in the subsections following this summary. The investigation starts with EMG and IMU sensor data acquisition from the leg muscles during a tSCS calibration procedure on healthy subjects and MS patients. Subsequently, the recorded EMG and acceleration data were passed through a preprocessing pipeline. Here, we cleaned and filtered the data. In addition, the EMG signals were separated into different classes depending on the EMG’s amplitude characteristics. These class labels describe the occurrence or absence of a muscular response after a tSCS stimulus and were considered as ground truth for the subsequent machine learning approach. With this approach, we want to investigate whether muscular responses visible in acceleration signals can be classified in accordance with the EMG-based class labels. For that, we extracted characteristics (features) in the time and frequency domain from all muscular responses after a tSCS stimulus in the acceleration signals. Additionally, the metadata of each participant (e.g., age, height) as well as stimulation properties were added to this feature table. By grouping these extracted features, we generated two different feature sets. After that, three machine learning algorithms were trained and tested using the previously generated feature sets and the ground truth class labels. We trained and tested all algorithms on three datasets: only patient data, only data from healthy subjects, and a mixed dataset consisting of both groups. The output of the different algorithms includes class labels for each recorded acceleration signal. By comparing the ground truth labels and the output, we can estimate the accuracy of each algorithm. During a calibration procedure, the detected response classes provide information on each subject’s individual optimal therapy intensity and electrode position. To evaluate the performance of the classification algorithms in the context of the application, we determined these parameters from the ground truth class labels as well as from the class labels returned by the machine learning algorithms. All steps are subsequently described in more detail.
2.1. Data Acquisition Protocol
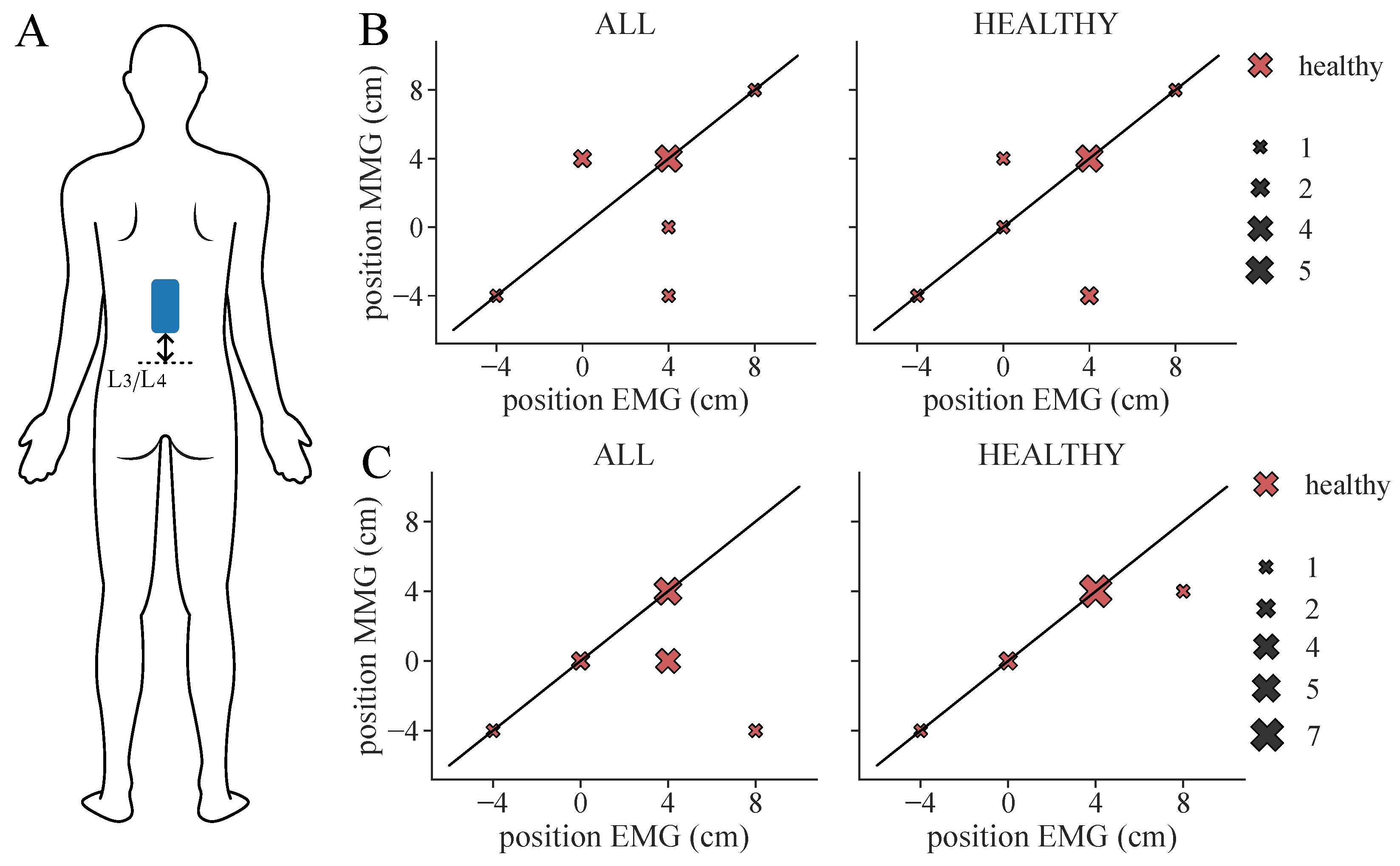
A tSCS calibration process was conducted on 11 healthy volunteers (female: 4, male: 7, age: 34.2 ± 6.9 years) and 11 MS patients (female: 6, male: 5, age: 55.9 ± 9.2 years). Individual participant characteristics are shown in
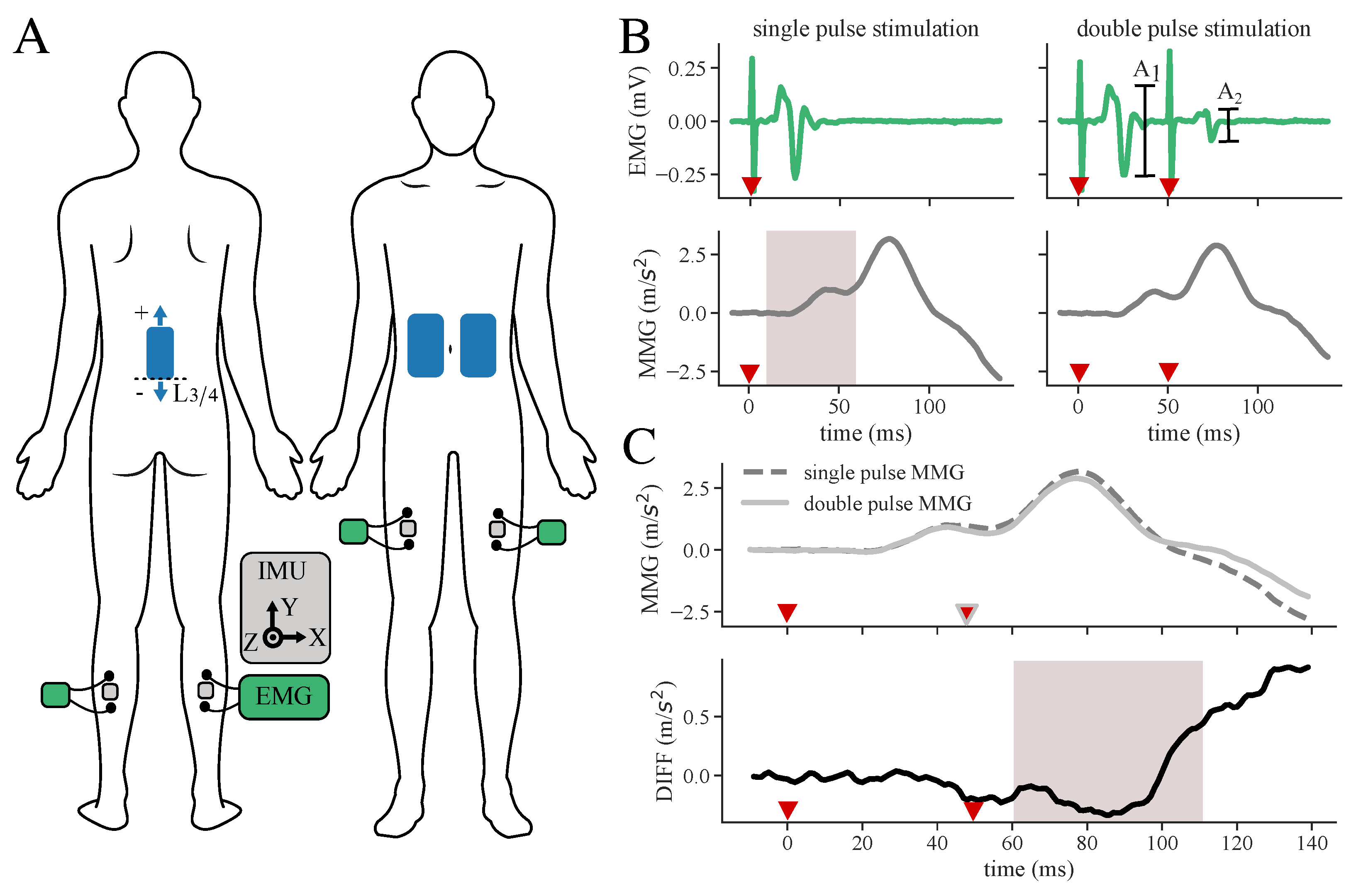
Table 1. Each healthy subject underwent several calibration sessions with varying back electrode positions. The patient dataset consists of two data recordings recorded on two different days for each individual patient, to whom only one electrode position was applied per recording day. These data originate from an ongoing study, which examines the immediate effect of tSCS on gait and spasticity in MS patients. As the tuning process is not the primary focus in this study, and we strive to keep the demands of the individual patient at a low level, the number of electrode positions is minimal. However, to still investigate the electrode positions, data from several positions were recorded within the healthy cohort. In order to place a 5 × 10 cm hydrogel stimulation electrode (axion GmbH, Leonberg, Germany) on the spine, the intervertebral space L3/L4 was identified through palpation. After disinfecting the skin, the back electrode was placed on the spine. For the healthy participants, it was placed successively at three different positions: with the lower edge of the electrode 4 cm caudal to L3/L4, on L3/L4, and 4 cm cranial to L3/L4. For the subjects S4 and S10, an additional fourth calibration session with the electrode located 8 cm cranial to L3/L4 was conducted. We chose an additional, even more cranial, position due to lack of reflex activity in the quadriceps muscle, indicating that the three previously recorded positions would not be ideal for a potential therapy application. Regarding the MS patient group, only one electrode position was tested per recording day, varying from 0–4.5 cm cranial to L3/L4. Two interconnected counter electrodes of size 12 × 7 cm (axion GmbH, Leonberg, Germany) were positioned on the abdomen (cf.
Figure 1A).
During one calibration session, three double (inter-pulse interval of 50 ms) and three single biphasic pulses (1 ms per phase) were applied with 5 s in between the stimulation incidences with the RehaMove3 stimulator (Hasomed GmbH, Magdeburg, Germany). This stimulation pattern was repeated with increasing stimulation intensities using an increment of 5 mA and starting at an intensity of 5 mA. The examiner terminated the calibration process when reaching the subject’s discomfort level.
Electrical and mechanical muscular responses of the quadriceps (Q), specifically the rectus femoris muscle, and triceps surae (TS) were bilaterally recorded by means of synchronized EMG sensors and IMUs (MuscleLab, Ergotest Innovation AS, Stathelle, Norway). The sample rates were 1 kHz for the EMG and 0.5 kHz for the IMU, respectively. Before the EMG electrode placement, the examiner prepared the skin using disinfection and abrasive paste. The IMUs were placed in between the electrodes of the EMG sensors (Hydrogel Kendall H124SG, Covidien LLC, Mansfield, OH, USA) using elastic straps to ensure that signals of the same muscles were acquired. The complete electrode and sensor setup is shown in
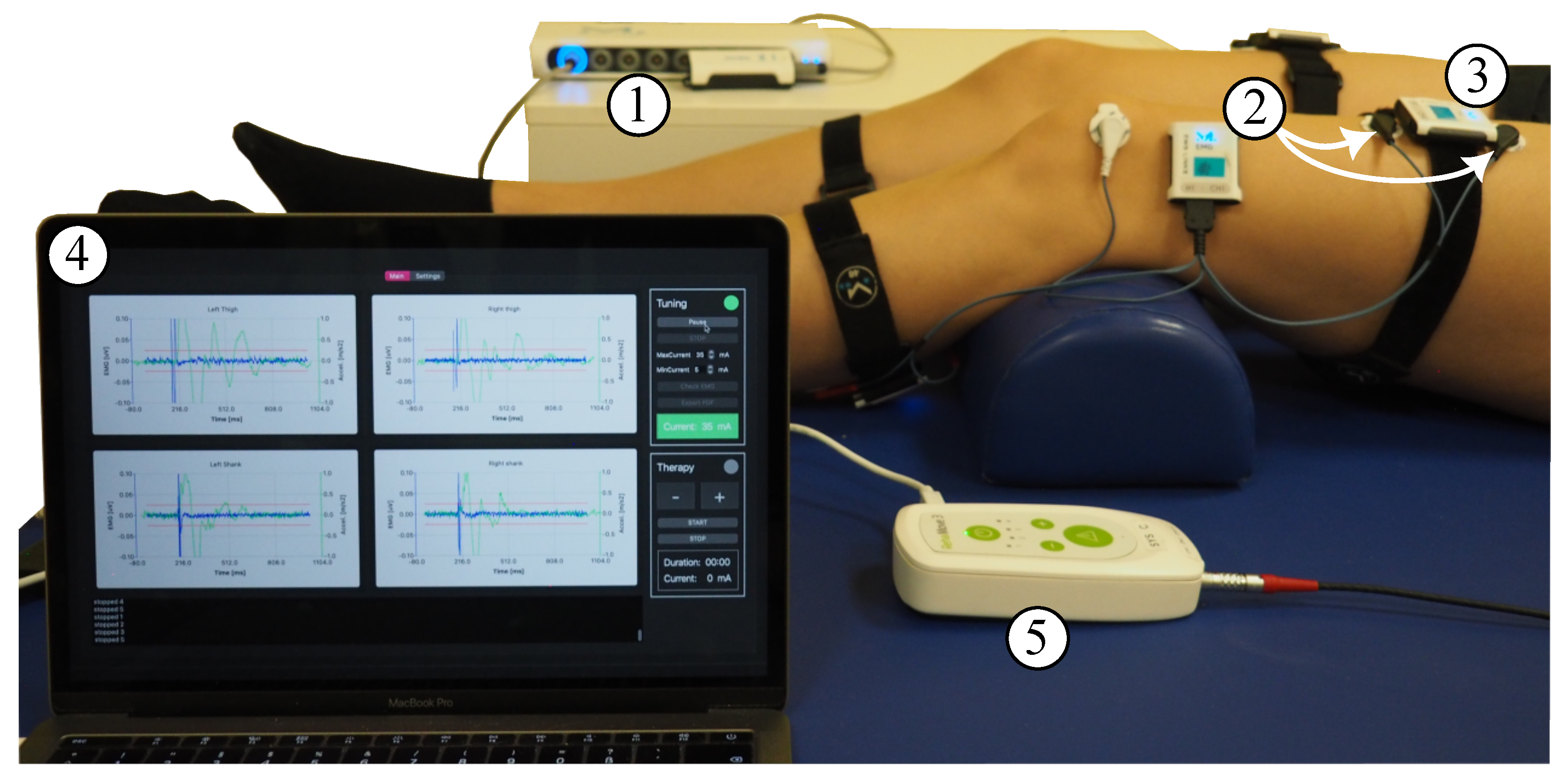
Figure 1A. The stimulation and data acquisition during the calibration process were controlled via a customized QT-user interface (QT version 6.3.0 for macOS) programmed in C++11.
Figure 2 shows the full measurement and stimulation equipment.
2.2. Preprocessing
To classify the EMG responses according to the response amplitude characteristics, the recorded EMG signals during double-pulse stimulation pass through a data processing pipeline implemented in Python 3.9 and adapted from our previously published algorithm for EMG-based analysis [
11]. Firstly, the stimulation artifacts are detected in the EMG to synchronize the sensor acquisition precisely with the stimulation. An artifact is marked if the double derivative of the EMG signal is greater than a threshold. Subsequently, the EMG signals are cropped to a common time window, starting 10 ms before the first stimulus and ending 400 ms after the first stimulus. The cropping is followed by a 50 Hz anti-humming [
19] and a sliding-median filter with a kernel size of 31 samples. The latter serves as a high-pass filter without applying a ringing effect on the signal. Finally, a similarity check among the three repetitions is conducted with connectivity matrices. Only repetitions with a sufficiently high coefficient of determination between them are averaged. If none of the repetitions are similar, the corresponding signal is marked as faulty. The averaged signals can then be classified according to the characteristics of the peak-to-peak response of the first (
) and the suppression (
S) of the second pulse (
) [
11], with
S:
The EMG responses of each muscle and each applied intensity can subsequently be categorized in a 2-class (distinguishing between response and no response) or 3-class (distinguishing between reflex response, direct muscular response, and no response) manner, as shown in
Table 2. Note that
• class 1 of the 2-class classification is equivalent to (
• class 1 ∩
• class 2) of the 3-class classification. The classes assigned to the EMG responses are considered ground truth for the supervised classification routine. By analyzing the distribution of classes in the four muscles along the applied stimulation intensity and the different electrode positions, a suitable stimulation amplitude and electrode location can be chosen.
Regarding the MMG data, only the acceleration in the z-direction corresponding to the axis orthogonal to the skin is considered for the feature extraction. For preprocessing of the MMG responses of double as well as single pulses, the timestamps of the stimulation artifacts found in the EMG signal are used to crop the signal accordingly to the cropped EMG. Subsequently, the average of the first 10 ms is subtracted from the signal as a non-dynamic gravity filter. The similarity check of the three repetitions is conducted again using connectivity matrices. Analogous repetitions are averaged. As shown in
Figure 1B, the mechanical muscular responses in the acceleration signal are much longer than the electrical muscle activity of the EMG, and the responses to the first and second impulse overlap. To separate the responses on the first and second pulse of a double stimulus, we applied the following procedure: the response to the first stimulus is directly measured by applying just a single pulse. We then subtract this response from the response of a double-pulse stimulation. The resulting signal (DIFF) represents the response to the second stimulus of a double pulse and enables direct assessment of the response suppression
S (cf.
Figure 1C). Finally, the averaged single- and double-pulse responses as well as the DIFF signal are used to extract features.
2.3. Data Distribution
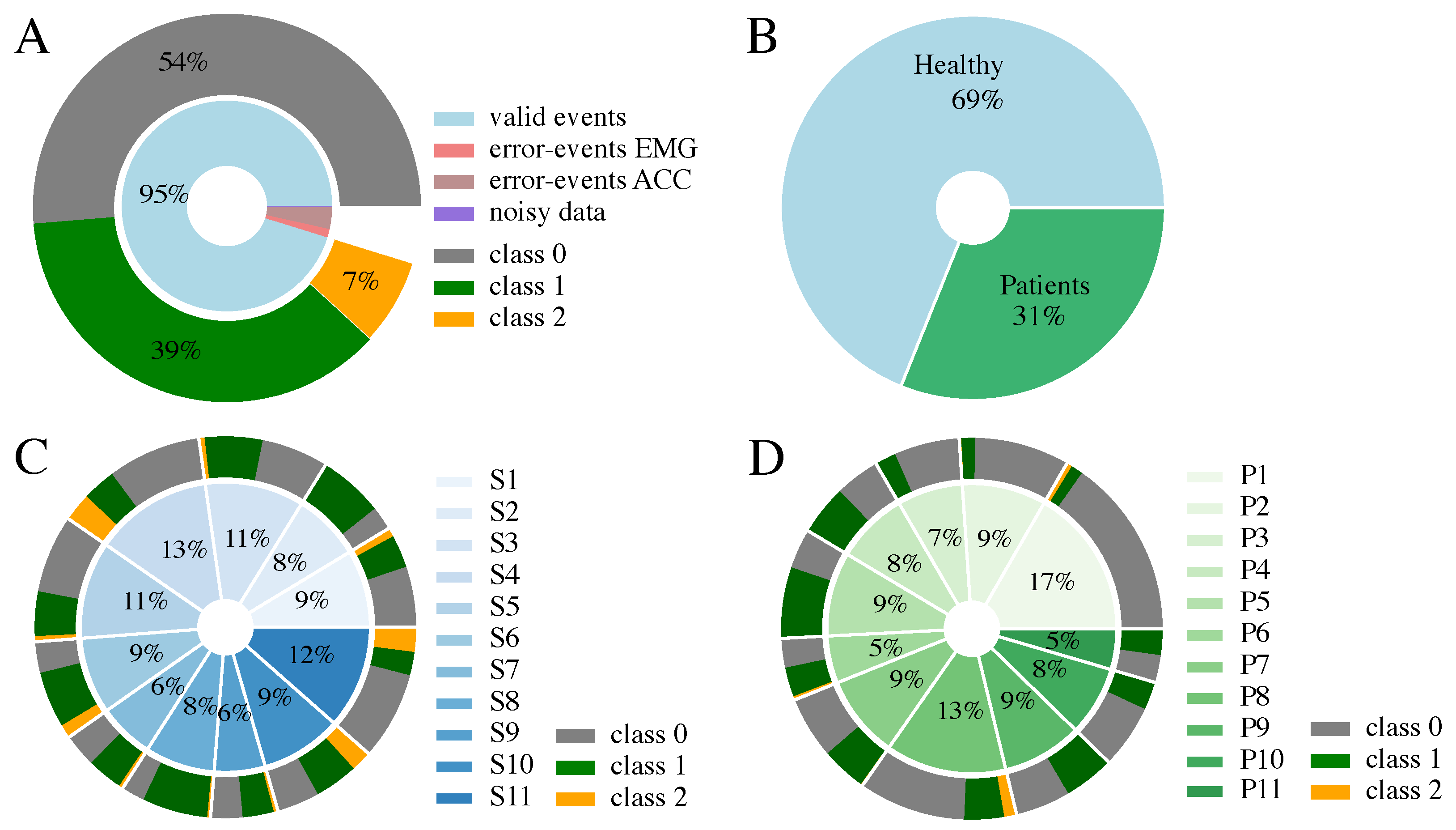
The full dataset used for this classification approach consists of 2196 events. An event comprises an averaged EMG and MMG muscle response to a single-pulse and double-pulse stimulation for a certain muscle at a specific application current and electrode position. The composition of the data is shown in
Figure 3. In total, 5% of the data events had to be excluded from the set for the ML-based classification due to errors during the similarity check in the preprocessing pipeline of the EMG and MMG signal, as none of the repetitions were marked as similar. These errors may occur due to movement of the subject during data acquisition, due to occurrence of spontaneous rhythmic muscle twitches, or due to failure of the stimulation artifact detection in the EMG signal. Less than 1% was excluded because of noise in the averaged EMG signal, also resulting from spontaneous muscular activity differing in the three repetitions. The remaining data exhibit an uneven distribution of the ground truth classification. Class 0 is dominant, with 54% of the data belonging to this class, followed by class 1 with 39%, and class 2 with only 7% of all events. As the maximum current applied during the tuning process varies among the participants, the proportion that the individual subjects contributes to the dataset ranges from 6–13% for the healthy participants and 5–17% for the patients.
2.4. Feature Extraction
We conceived a list of features in the time and frequency domain to assess mechanical muscle activity characteristics from the MMG. For each evaluated electrode position and stimulation current, these features were extracted for all investigated muscles. Features can be sorted into different categories and serve as input to the supervised classification approaches:
meta: subject’s metadata, e.g., age, height (four features);
stim: stimulation parameters: current and electrode position (two features);
MMG data: sensor data information from MMG (30 features).
The full list of features is displayed in
Table 3. The amplitude features, such as MMG single median or MMG DIFF rms, are determined on a window basis from the MMG signals. For the thigh muscles (quadriceps), we chose a window of 10–60 ms after the first stimulation pulse (winA1) for features extracted from the MMG single-pulse response, starting before the onset of the MMG response and ending before the onset of possible muscle response to stimulus two in the double-pulse data. The corresponding window of 10–60 ms after the second stimulus (winDIFF) is selected for amplitude feature extraction from DIFF. For the calf muscles (triceps surae), we shifted both windows, winA1 and winDiff, 5 ms to the right, as the response onset is delayed compared to the thigh muscles. The features 35 and 36 in
Table 3 are extracted from the second sensor of the same leg and not from the sensor from which all other MMG data features are determined. These two features were chosen as an approach to perceive possible crosstalk of other muscle activation. To simplify and automate the application of tSCS therapy, we created machine learning approaches using MMG signals and corresponding EMGs recorded from PRMs during double and single tSCS pulses. The EMG responses could easily be sorted into classes based on the amplitudes of first and second pulse responses. These classes were taken as ground truth for the supervised classification algorithms. For the ML-based classification approaches, two combinations of different feature categories were considered. MMG data & meta (SET-OBSERVE), as an observation approach as well as a combination of meta & stim (SET-PREDICT), act as a sensor-less prediction approach without any features extracted from MMG.
2.5. ML-Based Classification Approach
We investigated three standard ML approaches to classify the data. The Random Forest (RF) Classifier, the Support Vector Machine (SVM) classifier, as well as Linear Discriminant Analysis (LDA) were considered as possible solutions to the classification problem. The algorithms were applied in a leave-one-subject-out (LOSO) cross-validation loop using the python package scikit-learn (1.3.2). Thus, the dataset of each subject serves as test data for a model trained with the data of the remaining subjects. The balanced accuracy score for imbalanced datasets embedded in the sklearn package was chosen as a measure to validate the classification and avoid overestimating the model performance. To investigate the impact of the different subject groups on the classifiers, three datasets serve as an input for all models: the whole dataset including patients as well as healthy subjects (ALL), only data of healthy subjects (HEALTHY), and only data of patients (PATIENTS). Due to the lack of direct muscle responses (
• class 2), especially in the patient dataset (cf.
Figure 3D), all machine learning models were implemented as a 3-class classification problem as well as a 2-class classification problem (cf.
Table 2).
Hyperparameter optimization for the three classifiers was implemented as a random search with 50 iterations.
Table 4 shows the optimized parameters. The hyperparameter cross-validation was again realized in a LOSO manner. However, in the hyperparameter LOSO loop, only the training data, which consist of n
subjects, was considered. The hyperparameters were chosen according to the maximum mean balanced accuracy achieved among the LOSO cross-validation sets. Note that the hyperparameters were solely extracted for the 3-class classification problem. The parameters for the 2-class classification were chosen accordingly. The class weights were set to a balanced state according to the class distribution of the respective dataset for all classifiers.
The classification models and their results for the different datasets (ALL, HEALTHY, PATIENTS), the two feature sets (SET-OBSERVE, SET-PREDICT), the 2-class and 3-class classification, and the three classifiers (SVM, RF, LDA) were documented by means of the python package mlflow (2.8.1). Consequently, 36 different combinations of dataset, feature set, number of classes, and classifier were investigated.
2.6. Identification of Stimulation Parameters
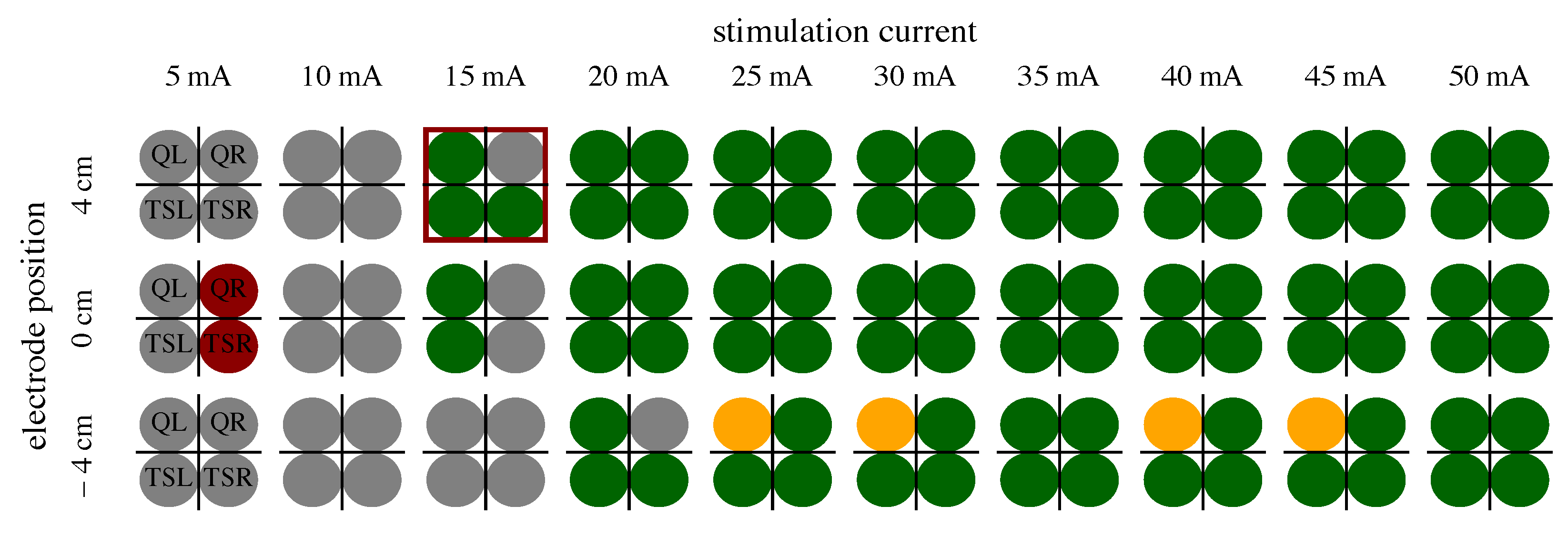
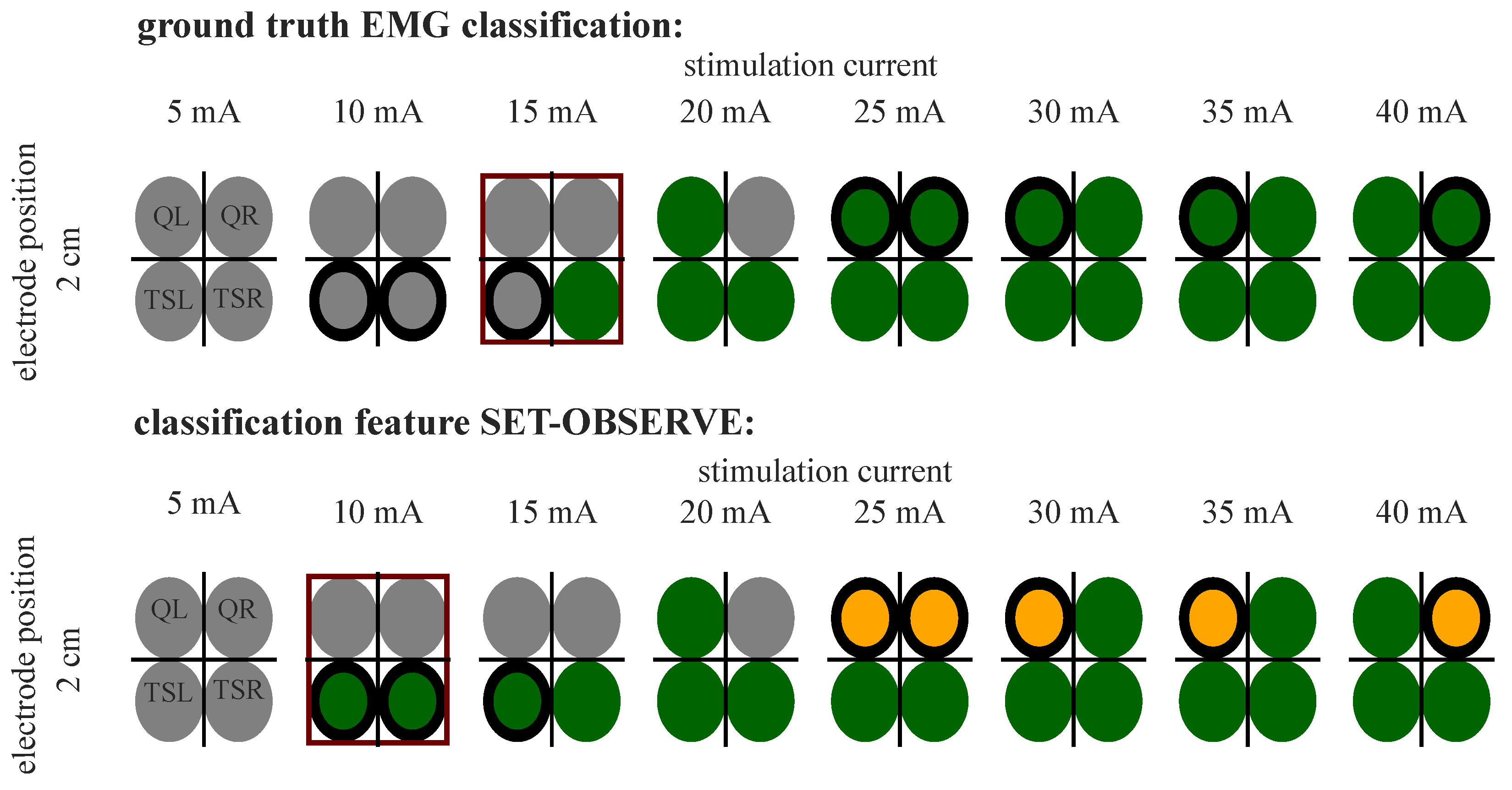
To find a suitable therapy current and electrode position, the assigned class distribution in the four muscles along the applied stimulation intensity is analyzed for each individual. An example of the class distribution extracted from EMG data with the proposed position and therapy current is presented in
Figure 4. For extracting the parameter pair (position, current), the following nested search is applied to each individual subject [
11]:
At least two • class 1 labels in one current among all muscles present in the respective electrode position;
Largest number of class 1 labels per current;
Smallest current difference between onset of leg response and presence of maximum number of class 1 labels;
Lowest stimulation current;
Largest sum of all class 1 labels in the respective position.
We chose a sub-motor-threshold therapy current of 90% of the intensity, where the first reflex occurred [
8,
11]. By extracting the therapy parameters for both EMG and SET-OBSERVE and SET-PREDICT classifications, the ML-based classification approach and its accuracy can be assessed in the context of tSCS application. Note that, for the patients, only the stimulation current is determined, as only one electrode position is available in the datasets.
4. Discussion
To simplify and automate the application of tSCS therapy, we deployed machine learning approaches to classify a sensor-based feature set containing MMG data characteristics from PRMs to double and single tSCS pulses using the corresponding EMG classes as ground truth. Additionally, a feature set without any sensor information containing only metadata and stimulation information was determined and classified. Through the ML-based class distributions, we identified suitable therapy parameters for each subject and compared these with the ground truth parameters extracted from the EMG classes.
The results show better classification accuracy for the feature set SET-OBSERVE, which includes MMG data, implying the importance of sensory observations to target individual therapy parameters. However, the classifiers for the 3-class classification performed only moderately well for the separation between class 1 (•, reflex response) and class 2 (•, direct muscular response). Thus, the similarity between these classes regarding the MMG in the 3-class classification problem is very high, making a separation challenging. We suspect two reasons for this, as follows.
Firstly, the suppression (
1) that is important for the 3-class EMG classification cannot be determined directly from MMG due to the non-linear summation of the forces and, therefore, the accelerations, in the case of sequential induced muscle twitches. With the same muscle activation, and accordingly the same EMG response to the first and second impulse (no suppression), the increase in force or acceleration due to the second impulse can be greater than the response to the first impulse [
20,
21]. This means that the amplitude of the acceleration in the DIFF signal would be increased compared to the response of the first impulse, despite the same EMG activity. Another problem is that these non-linear effects are strongly dependent on the muscle fiber type [
22], and the composition of muscle fiber types can vary among patients. To reduce these non-linear force summations after the sequential muscle twitches, we could apply longer inter-pulse intervals between the double stimulation pulses. However, this would directly influence the suppression effect in the EMG signals, especially for patients with SCI [
10]. As we need the post-activation suppression information to distinguish between reflex response and direct muscular response in the ground truth data, lengthening the inter-pulse interval would not be beneficial for therapy parameter identification.
The second reason for inaccuracies when distinguishing between reflex response and muscular response could be crosstalk in the acceleration signals due to movement of joints or contraction of other leg muscles. To provide knowledge on the activity of the other recorded leg muscle to the algorithm, we added two amplitude features of these muscles to the feature set SET-OBSERVE. This was done as a simple attempt to internally track and catch crosstalk. As we fastened the IMUs with elastic straps over the muscle belly, contractions from muscles with direct contact to the strap could disturb the sensor signals further. However, lower limb muscles that were not recorded during the calibration process are part of the PRMs, such as the hamstring or tibialis anterior muscle [
23]. Hence, activity in these muscles can still indicate activation of afferent nerves accountable for spasticity reduction and therefore lead to suitable therapy parameters. Nonetheless, as these muscles were not part of our datasets, this assumption is not verifiable and would have to be examined in further investigations. Crosstalk of joint movement resulting from the muscle contractions due to the tSCS pulses is also a possible signal disturbance. There is a considerable delay between a contraction of a distant muscle and a perceptible movement at the sensor. Keeping the measurement interval close to the stimuli should guarantee that only local contraction forces and corresponding accelerations are sensed. If crosstalk is present, then crosstalk from antagonistic muscles across the strap is more likely than from muscles further away, which can only act on the sensor via joint or leg movements with a greater time delay. To avoid big influences of superposition because of different acceleration sources, we chose the windows winA1 and winDIFF to be very close to the pulse artifact and, therefore, to the reflex or muscle activation time stamp.
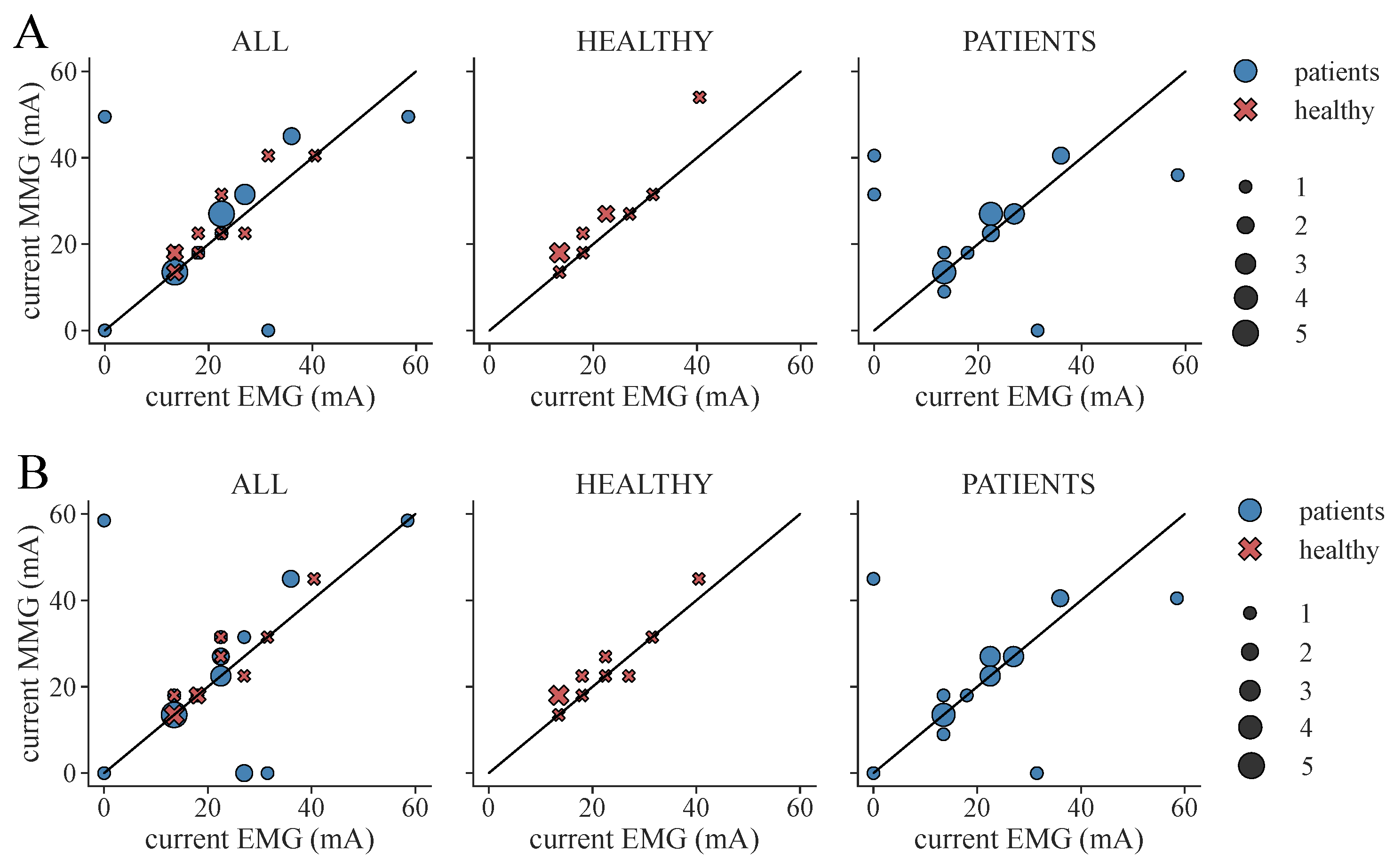
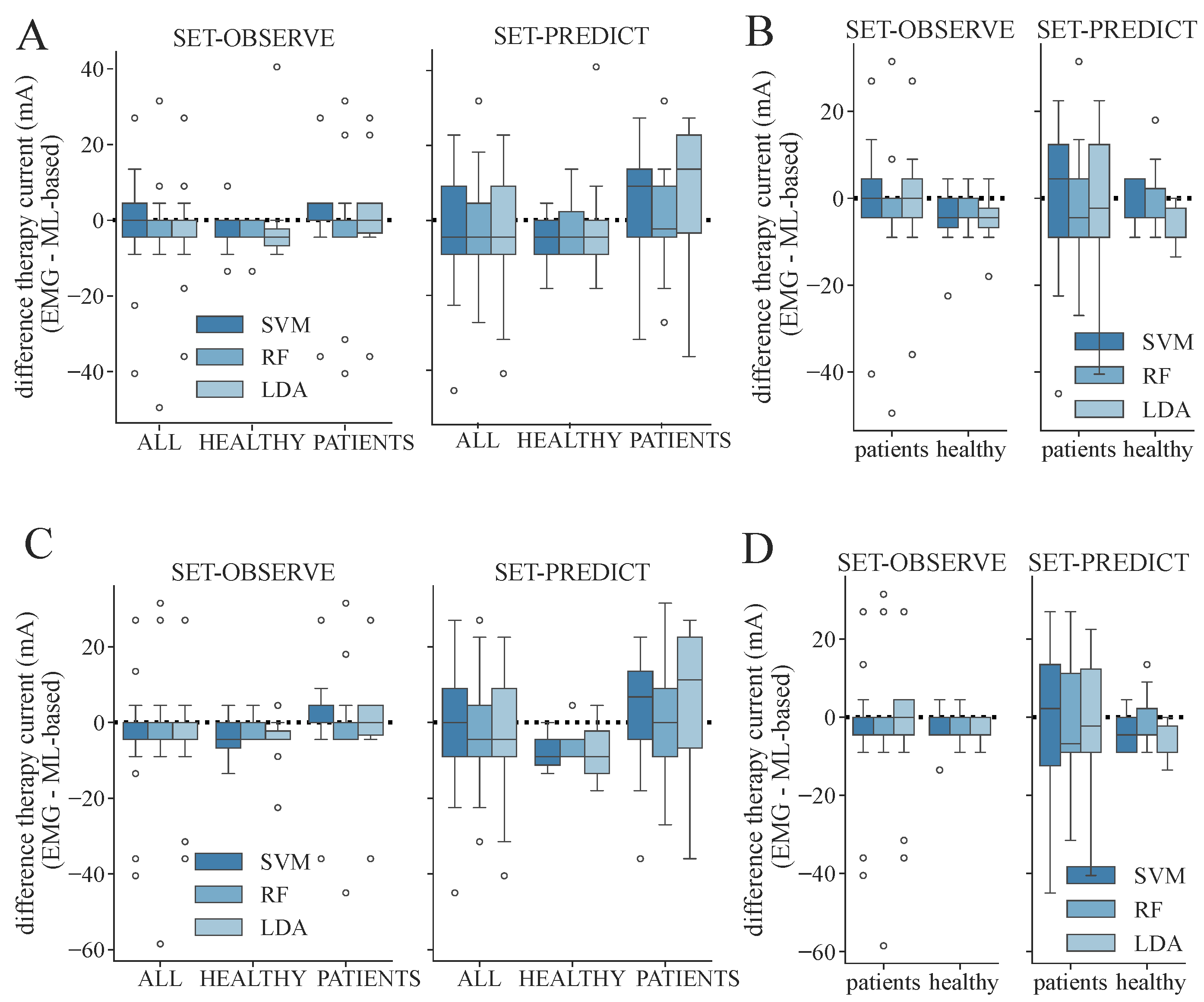
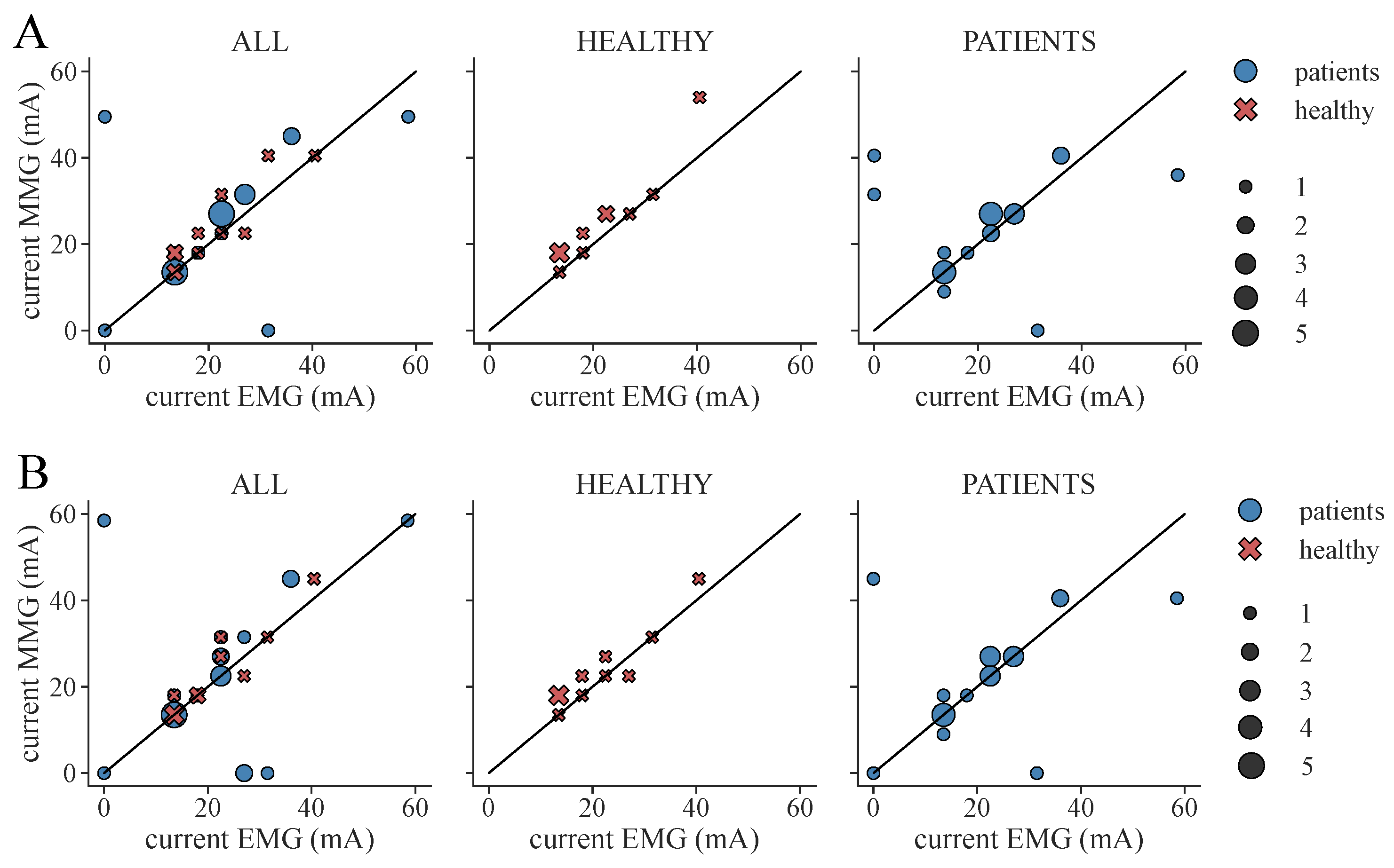
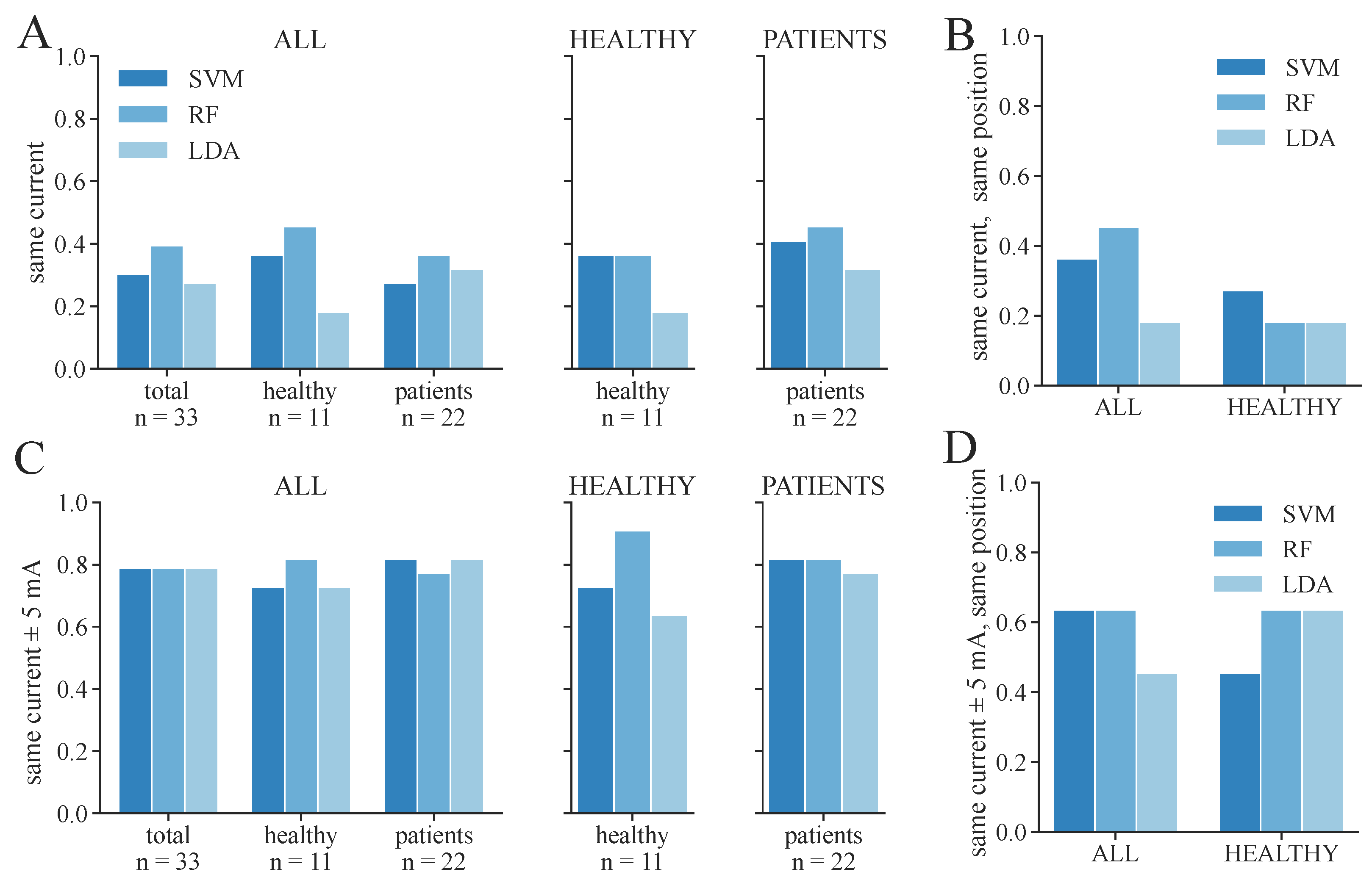
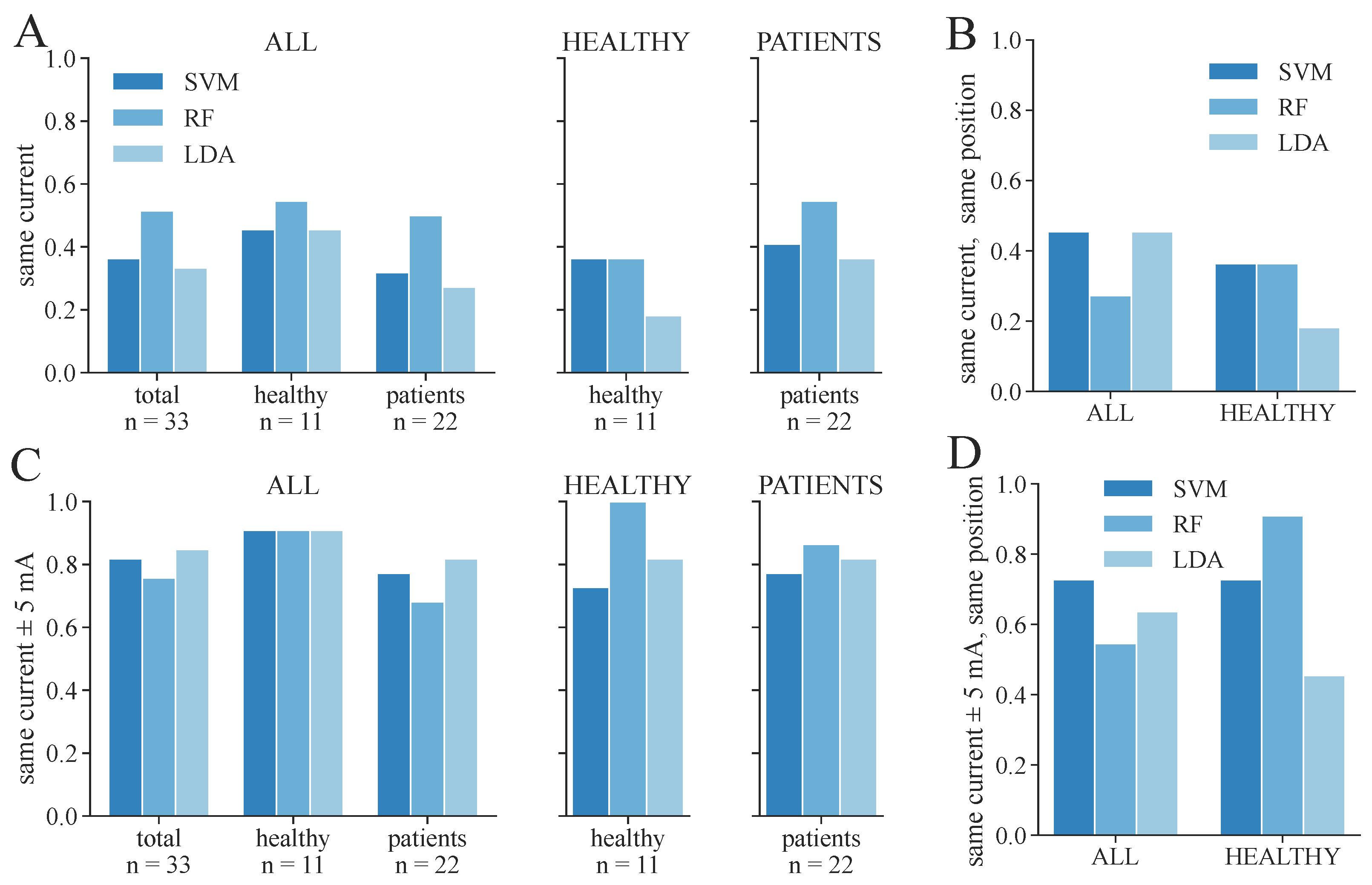
After the ML-based classification, we further identified individual therapy parameters for each subject from the classification results. The therapy current extracted from ground truth and from ML-based classification corresponded in only a fraction of the subjects. However, most of the determined currents varied around the optimal value. These fluctuations between ground truth and predicted therapy current result from inaccuracies of the classifiers, especially around the applied pulse amplitude at which the first muscle reactions occur. These inaccuracies also transfer to the choice of the electrode position in healthy subjects. However, a position that was not labeled as optimal through the ground truth classification can still be potentially suitable for tSCS when an adapted higher current is applied. Nonetheless, we strive for the most tolerable stimulation for the subject, which we assume can be extracted from the EMG data acquired at different electrode positions. Overall, the presented algorithms show good results for both therapy current and position identification. In order to successfully use MMG for personalized tSCS tuning, synchronized stimulation and IMU recording would be required, as no artifacts are visible in the acceleration signals.
In this paper, we investigated both 3-class classification as well as a simplified 2-class classification. The latter generally produced higher balanced accuracy values and more accurate stimulation parameters. Thus, we pose the question of whether a 2-class classification would be precise enough to activate afferents and, hence, achieve a therapeutic effect after tSCS therapy. Referring to the data we collected in this and in previous investigations, we observe that if a rather big electrode of 5 × 10 cm is placed over the upper lumbar spine, class 1 (reflex) responses will be most probably elicited before class 2 (direct muscular) responses occur. This corresponds with the recruitment order of different nerve fiber types. Large-diameter proprioceptive sensory nerves have the lowest activation threshold and are therefore recruited at lower stimulation intensities than motor fibers [
24,
25]. To conclude, since we strive for therapy currents at sub-motor level and since the first responses visible during the calibration procedures are most likely reflex responses elicited by afferents, a 2-class classification would presumably be sufficient. However, whether that is true for all groups of patients that would profit from tSCS cannot be confirmed and would have to be determined in further investigations.
The newly introduced method with single- and double-pulse stimulation was intended to improve the classification of muscle and reflex responses in the MMG. However, a disadvantage of this approach is the double time compared to the EMG-based approach, which only includes double stimuli. Given the good performance of tSCS-tuning based on 2-class classification, the question arises whether the inclusion of single-pulse data, i.e., the calculated differences and the corresponding features, is necessary to sufficiently detect any stimulus-induced activity in the MMG data. This open question will be pursued in the future.
For our investigations, we included patient tuning data as well as data from healthy subjects. Due to the limited quantity of our patient dataset, a machine learning approach using exclusively the available patient data would have been unsatisfying. Therefore, we included the larger healthy dataset in order to be able to investigate the performance of our method with several electrode positions. However, our results indicate that the accuracy of the therapy parameter choice is slightly higher for the patient cohort if we train the model solely on the PATIENT dataset instead of on the mixed ALL dataset (cf.
Figure 10A and
Figure 11A). This could imply that training an individual model for patients with a common medical condition is beneficial. Another patient group that was not investigated in the paper but would profit from a simplified tSCS tuning process is the group of patients with spinal cord injuries. Hence, this cohort should be included in future studies.
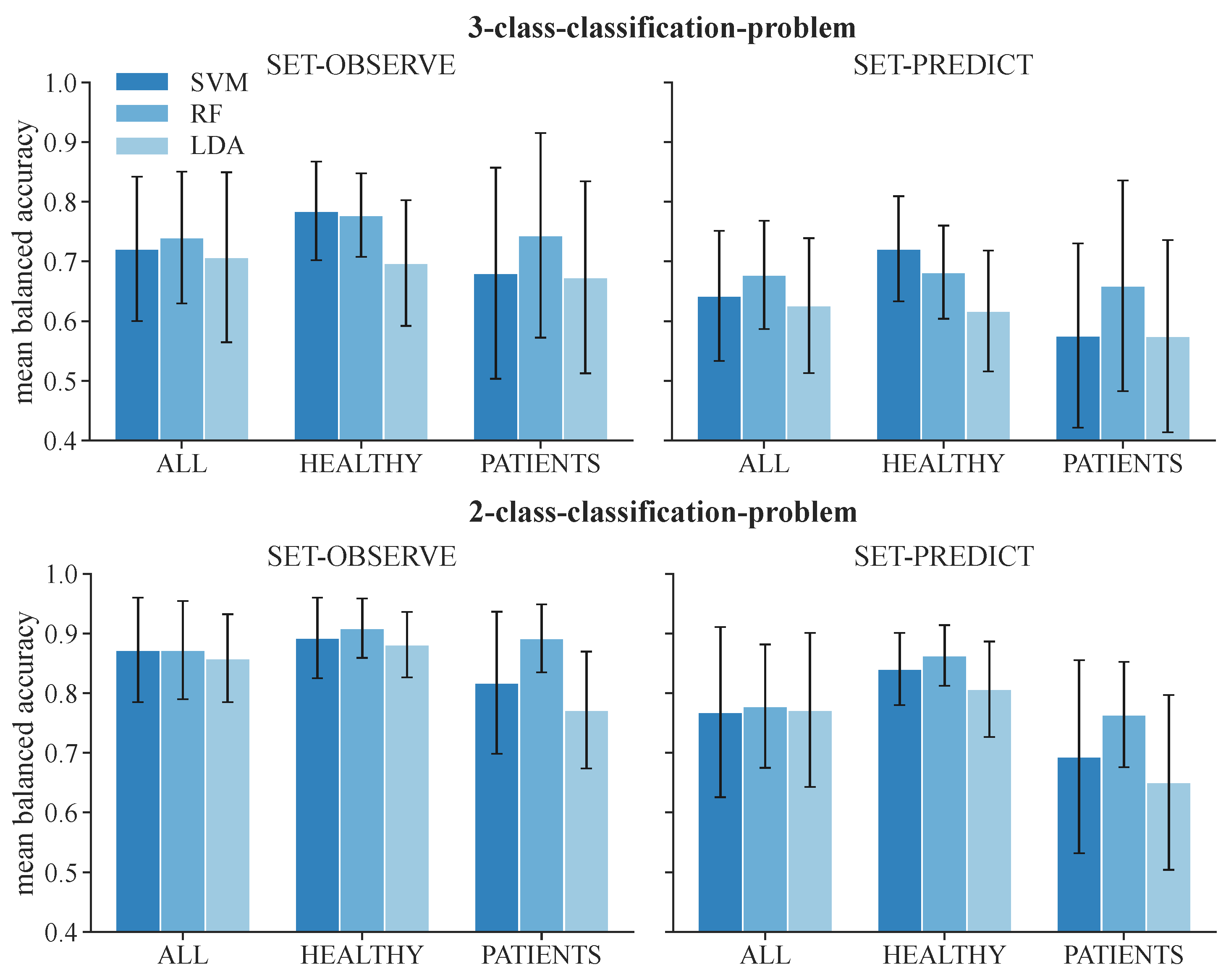
Another disparity in the results of the different subject groups is the larger standard deviation of the balanced accuracy among the MS patient group (cf.
Figure 5, dataset PATIENTS) compared to the mixed dataset (ALL) and healthy dataset (HEALTHY). A reason for that could be the difference in composition of the two datasets (cf.
Figure 3). The total number of events for the patients accounts for only one-third of the overall dataset. Additionally, the proportions of class 1 and class 2 events are smaller in the patient data. Therefore, the transition phase from no response (class 0) to response (class 1 and class 2) during the individual tuning of a patient takes up a larger proportion of the PATIENT dataset. However, in this transition phase, more natural inaccuracies in the classification approaches occur due to the small amplitudes of the responses. The smaller quantity of events and higher proportion of the transition phase could explain the larger standard deviation of the balanced accuracies. Another reason could be the disparity in severity and location of neurological defects among the MS patients, which causes a limited comparability between them. Thus, the LOSO cross-validation performance can vary considerably within the patient group. To conclude, to further improve the performance and reliability of our models, larger datasets from MS patients would be beneficial. Additional models for other patient groups, such as SCI, can be trained when the corresponding data are available.
For MMG, two sensor technologies are commonly used: piezoelectric contact (PEC) and accelerometer (ACC). In [
26], the frequency responses of PEC and ACC have been experimentally determined. Results for the sensors without housing restrictions show that the PEC transducer resembled that of the double integral over time of the ACC transducer signal, acting as a displacement meter of muscle vibration. As it correlates better with muscle force, we selected ACC as the sensor technology. However, study [
26] indicates the negative influence of housing restrictions on the measurements. We used a medically certified system with synchronous EMG and acceleration recording, as this was mandatory for our investigation. The inertial sensors with accelerometer have a dimension of 41 × 47 mm and a mass of 20 g. These physical quantities result from the use of rechargeable batteries for enabling wireless data transmission. The latter increases the usability of the system. Latencies in data transmission are not critical, as data from the sensors are transmitted with synchronized time stamps batch-wise to the laptop after each applied single or double pulse. Upon receiving the data, non-causal data processing is performed. The sensor size and mass (inertia) might negatively impact the detection of muscle responses as they dampen vibration. Possible advantages of smaller and lighter sensors and different mounting approaches need to be investigated in the future.
As we only looked at a small number of classifiers, there might be other algorithms that reach a similar or even better performance. We chose classifiers that are suitable for multi-class classification and tried to include linear (LDA) as well as non-linear algorithms (RF and SVM with radial basis function kernel) that vary in their computational complexity. Despite their differences, the performance of the chosen classifiers is similar. Hence, we expect that other classifier types would perform comparably. With the choice of our classifiers and their performances, we conclude that machine learning-based classification algorithms are generally suitable for this application.
Recent publications have determined that selective tSCS targets specific muscle groups for patients with SCI [
27,
28]. In this application, finding the accurate electrode position is more essential than in the calibration procedure that we proposed in this paper, as smaller electrodes or electrode arrays are used to selectively activate muscles. Hence, applying the proposed algorithm to these datasets would be another opportunity to investigate its performance in the context of a more advanced application.


 ,
, 











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}