


Effect of Skin Pigmentation and Finger Choice on Accuracy of Oxygen Saturation Measurement in an IoT-Based Pulse Oximeter

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Related Work
3. Principle of Pulse Oximetry
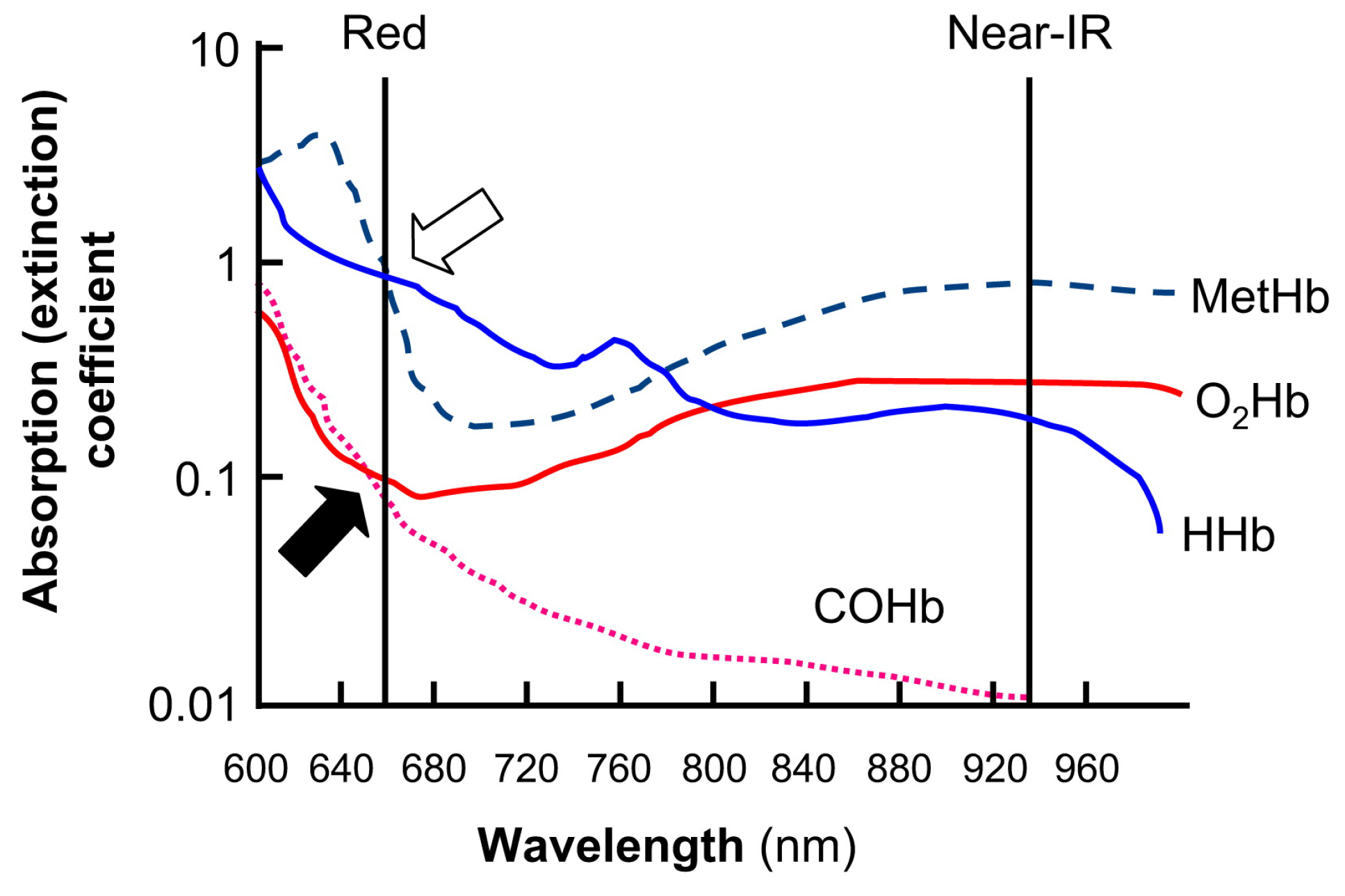
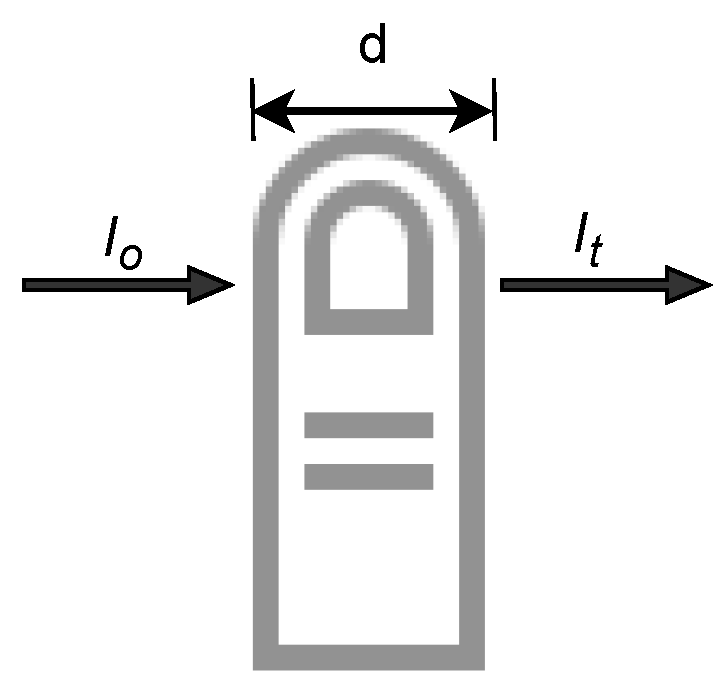
3.1. Relationship between Haemoglobin and Absorption of Light
3.2. Empirical Calibration of SpO2
3.3. Using RMS Value for Estimation of R-Value
4. Methods
4.1. System Design and Prototype
4.2. Ethics Approval
4.3. Recruitment of Volunteers
4.4. Study Protocol
4.5. Measurement Procedure
4.6. Finger Placement
4.7. Statistical Method
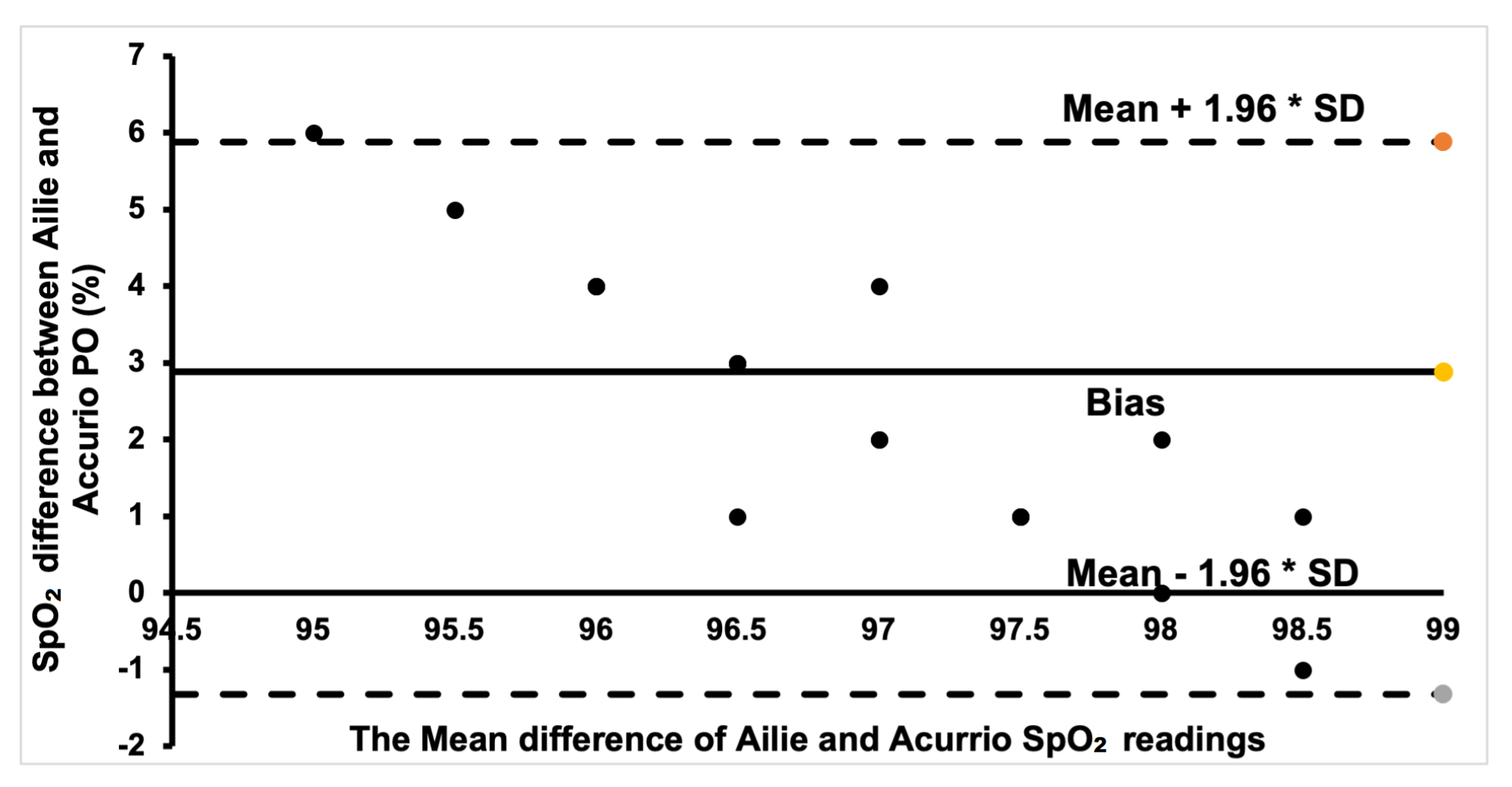
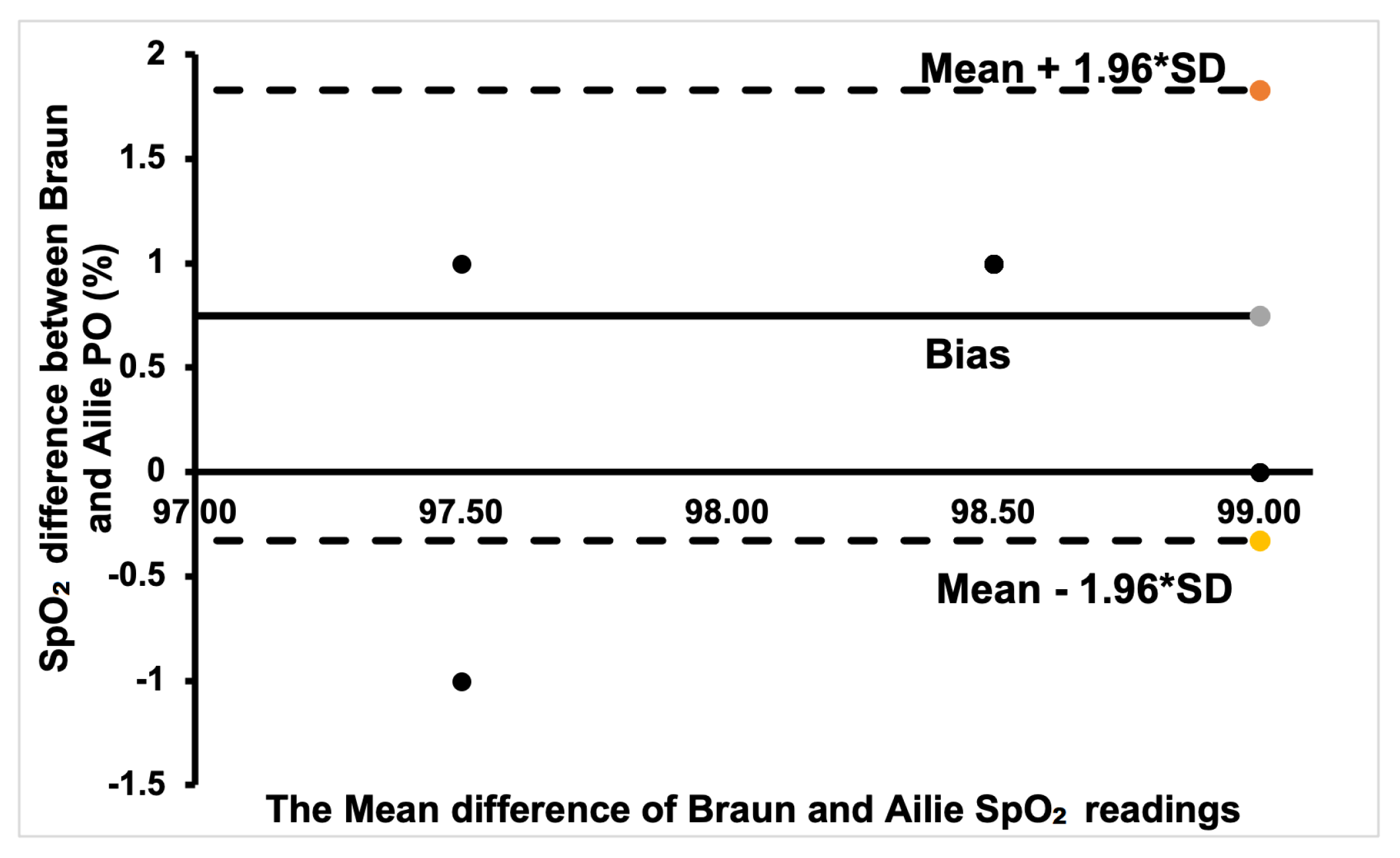
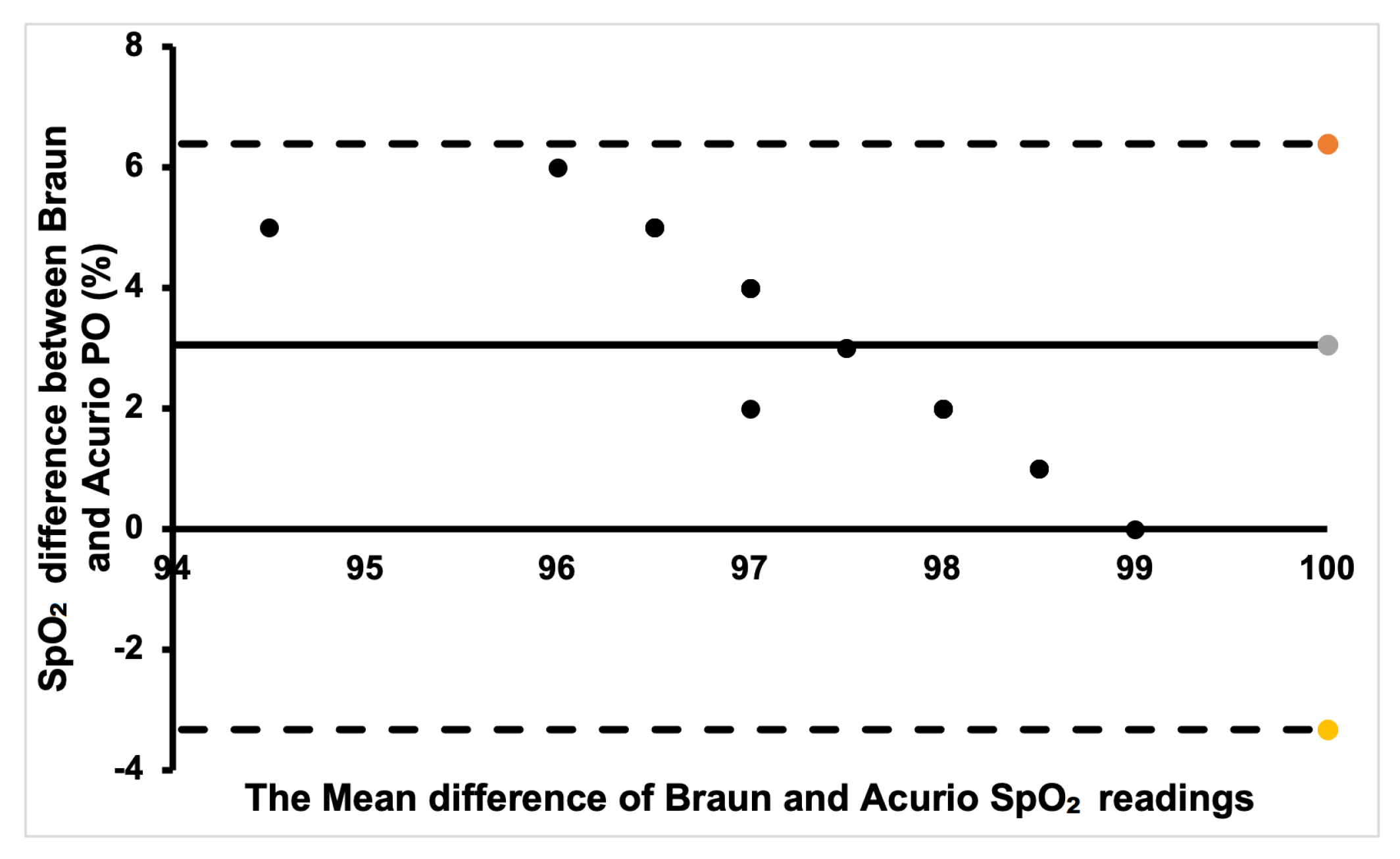
Bland–Altman Plot
- The average difference between predicted and commercial BP values;
- The upper limit of agreement, representing the 95% confidence interval for the average difference;
- The lower limit of agreement, representing the 95% confidence interval for the average difference.
5. Results and Discussion
5.1. Determining the Best Finger to Measure SpO2
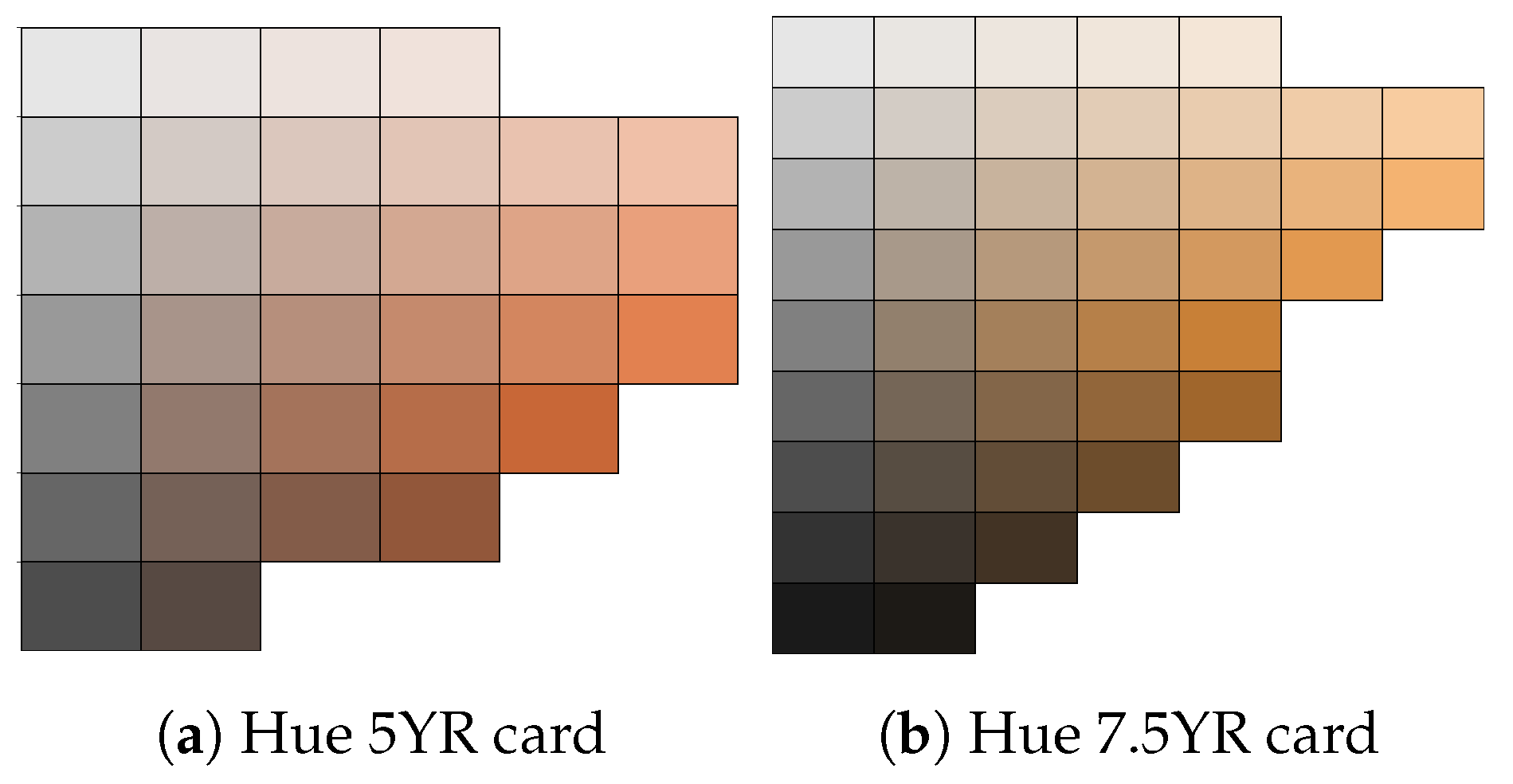
5.2. Comparison of Three Different Skin Colours
5.3. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ortega, R.; Hansen, C.J.; Elterman, K.; Woo, A. Pulse Oximetry. N. Engl. J. Med. 2011, 364, e33. [Google Scholar] [CrossRef]
- Chan, E.D.; Chan, M.M.; Chan, M.M. Pulse oximetry: Understanding its basic principles facilitates appreciation of its limitations. Respir. Med. 2013, 107, 789–799. [Google Scholar] [CrossRef]
- Allen, J.; Overbeck, K.; Nath, A.F.; Murray, A.; Stansby, G. A prospective comparison of bilateral photoplethysmography versus the ankle-brachial pressure index for detecting and quantifying lower limb peripheral arterial disease. J. Vasc. Surg. 2008, 47, 794–802. [Google Scholar] [CrossRef]
- Yelderman, M.; New, W. Evaluation of pulse oximetry. Anesthesiology 1983, 59, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Severinghaus, J.W.; Kelleher, J.F. Recent developments in pulse oximetry. Anesthesiology 1992, 76, 1018–1038. [Google Scholar]
- Hess, D.; Kacmarek, R. Techniques and devices for monitoring oxygenation: Oxygenation in the criticall ill patient. Respir. Care 1993, 38, 646–671. [Google Scholar]
- Elahi, S. COVID: Pulse Oxygen Monitors Work Less Well on Darker Skin, Experts Say. BBC News. 2022. Available online: https://www.bbc.com/news/health-58032842 (accessed on 4 July 2022).
- Hinkelbein, J.; Genzwuerker, H.V.; Sogl, R.; Fiedler, F. Effect of nail polish on oxygen saturation determined by pulse oximetry in critically ill patients. Resuscitation 2007, 72, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Ries, A.L.; Prewitt, L.M.; Johnson, J.J. Skin color and ear oximetry. Chest 1989, 96, 287–290. [Google Scholar] [CrossRef]
- Zeballos, R.J.; Weisman, I.M. Reliability of noninvasive oximetry in black subjects during exercise and hypoxia. Am. Rev. Respir. Dis. 1991, 144, 1240–1244. [Google Scholar] [CrossRef]
- Jubran, A.; Tobin, M.J. Reliability of pulse oximetry in titrating supplemental oxygen therapy in ventilator-dependent patients. Chest 1990, 97, 1420–1425. [Google Scholar] [CrossRef]
- Young, K. A Study of the Accuracy of Pulse Oximetry among Varying Skin Pigmentation Populations [Abstract]. Ph.D. Thesis, California State University, Long Beach, CA, USA, 1994. [Google Scholar]
- Coté, C.J.; Goldstein, E.A.; Fuchsman, W.H.; Hoaglin, D.C. The effect of nail polish on pulse oximetry. Anesth. Analg. 1988, 67, 683–686. [Google Scholar]
- Hakverdioğlu Yönt, G.; Akin Korhan, E.; Dizer, B. The effect of nail polish on pulse oximetry readings. Intensive Crit. Care Nurs. 2013, 30, 111–115. [Google Scholar] [CrossRef]
- Shi, C.; Goodall, M.; Dumville, J.; Hill, J.; Norman, G.; Hamer, O.; Clegg, A.; Watkins, C.L.; Georgiou, G.; Hodkinson, A.; et al. The accuracy of pulse oximetry in measuring oxygen saturation by levels of skin pigmentation: A systematic review and meta-analysis. BMC Med. 2022, 20, 267. [Google Scholar] [CrossRef] [PubMed]
- Bickler, P.E.; Feiner, J.R.; Severinghaus, J.W. Effects of skin pigmentation on pulse oximeter accuracy at low saturation. Anesthesiology 2005, 102, 715–719. [Google Scholar] [CrossRef]
- Adler, J.N.; Hughes, L.A.; Vivilecchia, R.; Camargo, C.A., Jr. Effect of skin pigmentation on pulse oximetry accuracy in the emergency department. Acad. Emerg. Med. 1998, 5, 965–970. [Google Scholar] [CrossRef]
- Holder, A.L.; Wong, A.K.I. The Big Consequences of Small Discrepancies: Why Racial Differences in Pulse Oximetry Errors Matter. Crit. Care Med. 2022, 50, 335–337. [Google Scholar] [CrossRef]
- Wong, A.K.I.; Charpignon, M.; Kim, H.; Josef, C.; de Hond, A.A.H.; Fojas, J.J.; Tabaie, A.; Liu, X.; Mireles-Cabodevila, E.; Carvalho, L.; et al. Analysis of Discrepancies Between Pulse Oximetry and Arterial Oxygen Saturation Measurements by Race and Ethnicity and Association with Organ Dysfunction and Mortality. JAMA Netw. Open 2021, 4, e2131674. [Google Scholar] [CrossRef]
- Mahgoub, M.T.A.; Khalifa, O.O.; Sidek, K.A.; Khan, S. Health monitoring system using Pulse Oximeter with remote alert. In Proceedings of the 2015 International Conference on Computing, Control, Networking, Electronics and Embedded Systems Engineering (ICCNEEE), Khartoum, Sudan, 7–9 September 2015; pp. 357–361. [Google Scholar]
- Chugh, S.; Kaur, J. Low cost calibration free Pulse oximeter. In Proceedings of the 2015 Annual IEEE India Conference (INDICON), New Delhi, India, 17–20 December 2015; pp. 1–5. [Google Scholar]
- Naeem, Z.H.; Youseffi, M.; Sefat, F.; Khaghani, S.A.; Raja, T.I.; Patel, A.; Javid, F.; Jamil, M.M.A.; Wahab, M.H.A. Design and Development of a Low Cost Pulse Oximeter. J. Phys. Conf. Ser. 2021, 1793, 012068. [Google Scholar] [CrossRef]
- Al Rasyid, M.U.H.; Lee, B.H.; Sudarsono, A. Implementation of body temperature and pulseoximeter sensors for wireless body area network. Sens. Mater. 2015, 27, 727–732. [Google Scholar]
- Nwibor, C.; Haxha, S.; Ali, M.M.; Sakel, M.; Haxha, A.R.; Saunders, K.; Nabakooza, S. Remote Health Monitoring System for the Estimation of Blood Pressure, Heart Rate, and Blood Oxygen Saturation Level. IEEE Sens. J. 2023, 23, 5401–5411. [Google Scholar] [CrossRef]
- HomeCare Magazine. Understanding SpO2 and Normal Oxygen Levels. 2022. Available online: https://www.homecaremag.com/understanding-SpO2-and-normal-oxygen-levels#:~:text=SpO2%2C%20also%20known%20as%20oxygen,will%20not%20function%20as%20efficiently (accessed on 2 February 2022).
- Holland, K. Is My Blood Oxygen Level Normal? 2022. Available online: https://www.healthline.com/health/normal-blood-oxygen-level#:~:text=Normal%3A%20A%20normal%20ABG%20oxygen,between%2095%20and%20100%20percent (accessed on 23 March 2022).
- Shi, C.; Goodall, M.; Dumville, J.; Hill, J.; Norman, G.; Hamer, O.; Clegg, A.; Watkins, C.L.; Georgiou, G.; Hodkinson, A.; et al. The effects of skin pigmentation on the accuracy of pulse oximetry in measuring oxygen saturation: A systematic review and meta-analysis. medRxiv 2022. [Google Scholar] [CrossRef]
- Al-Halawani, R.; Charlton, P.H.; Qassem, M.; Kyriacou, P.A. A review of the effect of skin pigmentation on pulse oximeter accuracy. Physiol. Meas. 2023, 44, 05TR01. [Google Scholar] [CrossRef]
- Cabanas, A.M.; Fuentes-Guajardo, M.; Latorre, K.; León, D.; Martín-Escudero, P. Skin Pigmentation Influence on Pulse Oximetry Accuracy: A Systematic Review and Bibliometric Analysis. Sensors 2022, 22, 3402. [Google Scholar] [CrossRef]
- Elgendi, M. On the analysis of fingertip photoplethysmogram signals. Curr. Cardiol. Rev. 2012, 8, 14–25. [Google Scholar] [CrossRef]
- Visualdictionaryonline.com. HUMAN BEING:: SENSE ORGANS:: TOUCH:: FINGER Image—Visual Dictionary Online. 2022. Available online: http://www.visualdictionaryonline.com/human-being/sense-organs/touch/finger.php (accessed on 18 September 2018).
- Wang, C.; Li, Z.; Wei, X. Monitoring heart and respiratory rates at radial artery based on PPG. Optik 2013, 124, 3954–3956. [Google Scholar] [CrossRef]
- Tremper, K.K.; Barker, S.J. Pulse oximetry. Anesthesiology 1989, 70, 98–108. [Google Scholar] [CrossRef]
- Sinex, J.E. Pulse oximetry: Principles and limitations. Am. J. Emerg. Med. 1999, 17, 59–66. [Google Scholar] [CrossRef]
- Shi, P. Photoplethysmography in Noninvasive Cardiovascular Assessment. Ph.D. Thesis, Loughborough University, Loughborough, UK, 2009. [Google Scholar]
- Baker, W.B.; Parthasarathy, A.B.; Busch, D.R.; Mesquita, R.C.; Greenberg, J.H.; Yodh, A.G. Modified Beer-Lambert law for blood flow. Biomed. Opt. Express 2014, 5, 4053–4075. [Google Scholar] [CrossRef]
- Ralston, A.C.; Webb, R.K.; Runciman, W.B. Potential errors in pulse oximetry. III: Effects of interferences, dyes, dyshaemoglobins and other pigments. Anaesthesia 1991, 46, 291–295. [Google Scholar] [CrossRef]
- Hampson, N.B.; Scott, K.L.; Zmaeff, J.L. Carboxyhemoglobin measurement by hospitals: Implications for the diagnosis of carbon monoxide poisoning. J. Emerg. Med. 2006, 31, 13–16. [Google Scholar] [CrossRef]
- Haxha, S.; Jhoja, J. Optical Based Noninvasive Glucose Monitoring Sensor Prototype. IEEE Photonics J. 2016, 8, 6805911. [Google Scholar] [CrossRef]
- Solà, J.; Castoldi, S.; Chételat, O.; Correvon, M.; Dasen, S.; Droz, S.; Jacob, N.; Kormann, R.; Neumann, V.; Perrenoud, A.; et al. SpO2 sensor embedded in a finger ring: Design and implementation. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2006, 2006, 4295–4298. [Google Scholar]
- Zhang, Q.; Xi, S.; Xing, B. Design of noninvasive blood oxygen measurement system based on S3C2440A. Appl. Electron. Tech. 2013, 6, 67–69+73. [Google Scholar]
- Zhi, W.; Feng, L.L. Study on multiParameter monitoring instrument based on embedded system. Appl. Electron. Tech. 2009, 11, 71–74+78. [Google Scholar]
- Nitzan, M.; Romem, A.; Koppel, R. Pulse oximetry: Fundamentals and technology update. Med. Devices 2014, 7, 231–239. [Google Scholar] [CrossRef]
- Zonios, G.; Iyer, V.K.; Shankar, U.S. Adaptive Calibration for Pulse Oximetry. U.S. Patent 6,839,580, 4 January 2005. [Google Scholar]
- Rusch, T.L.; Sankar, R.; Scharf, J.E. Signal processing methods for pulse oximetry. Comput. Biol. Med. 1996, 26, 143–159. [Google Scholar] [CrossRef]
- Salyer, J.W. Neonatal and pediatric pulse oximetry. Respir. Care 2003, 48, 386–396; discussion 397–398. [Google Scholar]
- Reddy, K.A.; George, B.; Mohan, N.M.; Kumar, V.J. A Novel Calibration-Free Method of Measurement of Oxygen Saturation in Arterial Blood. IEEE Trans. Instrum. Meas. 2009, 58, 1699–1705. [Google Scholar] [CrossRef]
- Flewelling, R. Noninvasive Optical Monitoring. In The Biomedical Engineering HandBook, 2nd ed.; Bronzino, E.J.D., Ed.; CRC Press: Boca Raton, FL, USA, 2000; Chapter 86. [Google Scholar]
- Mendelson, Y.; Kent, J. Variations in optical absorption spectra of adult and fetal haemoglobins and its effect on pulse oximetry. IEEE Trans. Biomed. Eng. 1989, 36, 844–848. [Google Scholar] [CrossRef]
- Oak, S.; Aroul, P. How to Design Peripheral Oxygen Saturation (SpO2) and Optical Heart Rate Monitoring (OHRM) Systems Using AFE4403. Application Report SLAA655. 2015. Available online: https://www.ti.com/lit/pdf/slaa655 (accessed on 17 May 2024).
- Szczepaaski, A.; Saeed, K. A Mobile Device System for Early Warning of ECG Anomalies. Sensors 2014, 14, 11031–11044. [Google Scholar] [CrossRef]
- Munsell, A.H. Atlas of the Munsell Color System; Wadsworth, Howland Co., Inc., Printers: Boston, MA, USA, 1915. [Google Scholar]
- Munsell Color System; Color Matching from Munsell Color Company. Munsell Color Notation and Color Test; Dimensions of Color Munsell Color System. 2022. Available online: https://munsell.com/about-munsell-color/how-color-notation-works (accessed on 4 July 2022).
- Zanca, J. Exploring Methods to Improve Pressure Ulcer Detection: Spectroscopic Assessment of the Blanch Response. Doctoral Dissertation, University of Pittsburgh, Pittsburgh, PA, USA, 2006. [Google Scholar]
- Muddy Colors. Thinking about Skin Tones, Chroma and Munsell. 2022. Available online: https://www.muddycolors.com/2019/07/thinking-about-skin-tones-chroma-and-munsell (accessed on 5 July 2022).
- Acurio AS-302 OLED Medical Fingertip Pulse Oximeter with FDA CE ISO Approval. 2022. Available online: https://www.medicalexpo.com/prod/shenzhen-acurio-instruments/product-301658-1127997.html (accessed on 5 July 2022).
- Braunhealthcare.com. Braun Pulse Oximeter. 2022. Available online: https://www.iacl.ie/pulse-oximeters/braun-pulse-oximeter.4100.html (accessed on 5 July 2022).
- Amazon.co.uk. 2022. Available online: https://www.amazon.co.uk/AILE-Oximeter-Approved-Monitor-Oximeter-Monitor/dp/B08TTYG32S (accessed on 5 July 2022).
- Zach, V. What Is a Bland-Altman Plot? (Definition & Example). Statology. Available online: https://www.statology.org/bland-altman-plot (accessed on 3 September 2022).
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef]
- Mizukoshi, K.; Shibasaki, M.; Amaya, F.; Mizobe, T.; Tanaka, Y. Which Finger Do You Attach Pulse Oximetry To? Index Finger or Not? Eur. J. Anaesthesiol. 2009, 26 (Suppl. S45), 3AP1–3AP5. [Google Scholar]
- Basaranoglu, G.; Bakan, M.; Umutoglu, T.; Zengin, S.U.; Idin, K.; Salihoglu, Z. Comparison of SpO2 values from different fingers of the hands. SpringerPlus 2015, 4, 561. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | 25–60 yrs |
| Gender (Female/Male) | 5/15 |
| Skin: | |
| White | 7 |
| Brown | 7 |
| Black | 6 |
| Right thumb | R1 | Left thumb | L1 |
| Right index | R2 | Left index | L2 |
| Right middle | R3 | Left middle | L3 |
| Right ring | R4 | Left ring | L4 |
| Right little | R5 | Left little | L5 |
| Finger | SpO2 (Mean ± 1.96 × SD) | R1 | R2 | R3 | R4 | R5 | L1 | L2 | L3 | L4 | L5 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| R1 | 97.95 ± 0.94 | - | |||||||||
| R2 | 97.90 ± 0.64 | NS | - | ||||||||
| R3 | 98.05 ± 0.69 | NS | NS | - | |||||||
| R4 | 97.80 ± 1.15 | NS | NS | NS | - | ||||||
| R5 | 98.10 ± 0.64 | NS | NS | NS | NS | - | |||||
| L1 | 97.40 ± 1.90 | NS | NS | NS | NS | NS | - | ||||
| L2 | 97.60 ± 1.10 | NS | NS | NS | NS | NS | NS | - | |||
| L3 | 97.75 ± 1.25 | NS | NS | NS | NS | NS | NS | NS | - | ||
| L4 | 98.10 ± 0.45 | NS | NS | NS | NS | NS | NS | NS | NS | - | |
| L5 | 97.70 ± 0.66 | NS | NS | NS | NS | NS | NS | NS | NS | NS |
| Finger | SpO2 (Mean ± 1.96 × SD) | R1 | R2 | R3 | R4 | R5 | L1 | L2 | L3 | L4 | L5 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| R1 | 95.80 ± 1.85 | - | |||||||||
| R2 | 95.65 ± 2.13 | NS | - | ||||||||
| R3 | 94.8 ± 6.24 | NS | NS | - | |||||||
| R4 | 96.80 ± 2.25 | NS | NS | NS | - | ||||||
| R5 | 96.25 ± 3.13 | NS | NS | NS | NS | - | |||||
| L1 | 95.35 ± 2.83 | NS | NS | NS | NS | NS | - | ||||
| L2 | 95.90 ± 3.73 | NS | NS | NS | NS | NS | NS | - | |||
| L3 | 95.45 ± 3.35 | NS | NS | NS | NS | NS | NS | NS | - | ||
| L4 | 96.70 ± 2.23 | NS | NS | NS | NS | NS | NS | NS | NS | - | |
| L5 | 96.20 ± 3.16 | NS | NS | NS | NS | NS | NS | NS | NS | NS |
| Finger | SpO2 (Mean ± 1.96 × SD) | R1 | R2 | R3 | R4 | R5 | L1 | L2 | L3 | L4 | L5 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| R1 | 96.75 ± 3.63 | - | |||||||||
| R2 | 98.40 ± 0.94 | NS | - | ||||||||
| R3 | 98.40 ± 1.10 | NS | NS | - | |||||||
| R4 | 98.50 ± 1.19 | NS | NS | NS | - | ||||||
| R5 | 98.5 ± 1.40 | NS | NS | NS | NS | - | |||||
| L1 | 97.95 ± 1.79 | NS | NS | NS | NS | NS | - | ||||
| L2 | 98.35 ± 1.27 | NS | NS | NS | NS | NS | NS | - | |||
| L3 | 98.85 ± 0.49 | NS | NS | NS | NS | NS | NS | NS | - | ||
| L4 | 98.50 ± 1.00 | NS | NS | NS | NS | NS | NS | NS | NS | - | |
| L5 | 98.7 ± 0.73 | NS | NS | NS | NS | NS | NS | NS | NS | NS |
| Commercial Oximeter | Skin | SpO2 (Mean ± 1.96 × SD) | White | Brown | Black |
|---|---|---|---|---|---|
| Ailie | White | 98.00 ± 0.53 | - | ||
| Brown | 98.14 ± 0.38 | NS | - | ||
| Black | 98.14 ± 0.38 | NS | NS | - | |
| Acurio | White | 96.00 ± 1.35 | - | ||
| Brown | 94.00 ± 1.77 | NS | - | ||
| Black | 97.00 ± 2.36 | NS | NS | ||
| Braun | White | 99.00 ± 0.38 | - | ||
| Brown | 99.00 ± 0.00 | NS | - | ||
| Black | 97.00 ± 0.98 | NS | NS | - | |
| Custom | White | 99.29 ± 1.11 | - | ||
| Brown | 99.86 ± 0.38 | NS | - | ||
| Black | 99.29 ± 0.49 | NS | NS | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haxha, S.; Nwibor, C.; Ali, M.; Sakel, M.; Saunders, K.; Dyo, V.; Nabakooza, S. Effect of Skin Pigmentation and Finger Choice on Accuracy of Oxygen Saturation Measurement in an IoT-Based Pulse Oximeter. Sensors 2024, 24, 3301. https://doi.org/10.3390/s24113301
Haxha S, Nwibor C, Ali M, Sakel M, Saunders K, Dyo V, Nabakooza S. Effect of Skin Pigmentation and Finger Choice on Accuracy of Oxygen Saturation Measurement in an IoT-Based Pulse Oximeter. Sensors. 2024; 24(11):3301. https://doi.org/10.3390/s24113301
Chicago/Turabian StyleHaxha, Shyqyri, Chike Nwibor, Mian Ali, Mohamed Sakel, Karen Saunders, Vladimir Dyo, and Shakira Nabakooza. 2024. "Effect of Skin Pigmentation and Finger Choice on Accuracy of Oxygen Saturation Measurement in an IoT-Based Pulse Oximeter" Sensors 24, no. 11: 3301. https://doi.org/10.3390/s24113301
APA StyleHaxha, S., Nwibor, C., Ali, M., Sakel, M., Saunders, K., Dyo, V., & Nabakooza, S. (2024). Effect of Skin Pigmentation and Finger Choice on Accuracy of Oxygen Saturation Measurement in an IoT-Based Pulse Oximeter. Sensors, 24(11), 3301. https://doi.org/10.3390/s24113301