

A Hybrid Protection Scheme for the Gait Analysis in Early Dementia Recognition



Abstract
:1. Introduction
- The proposal of a hybrid protection scheme that combines PHE and a cancelable biometric approach protects the patient’s gait feature and ensures their privacy.
- The adoption of a long short-term memory neural network architecture for the early recognition of dementia, having as input data the multivariate sequences of gait analysis.
- An ablation study on the performance of the proposed protection scheme.
- A comparative analysis between the proposed system and the other state-of-the-art early detection systems for early dementia recognition.
- An evaluation of the security and computational cost of the proposed hybrid protection scheme through security analysis, noninvertibility analysis, renewability analysis, and computational analysis.
2. Related Works
3. Proposed Method
3.1. Preprocessing and Feature Extraction
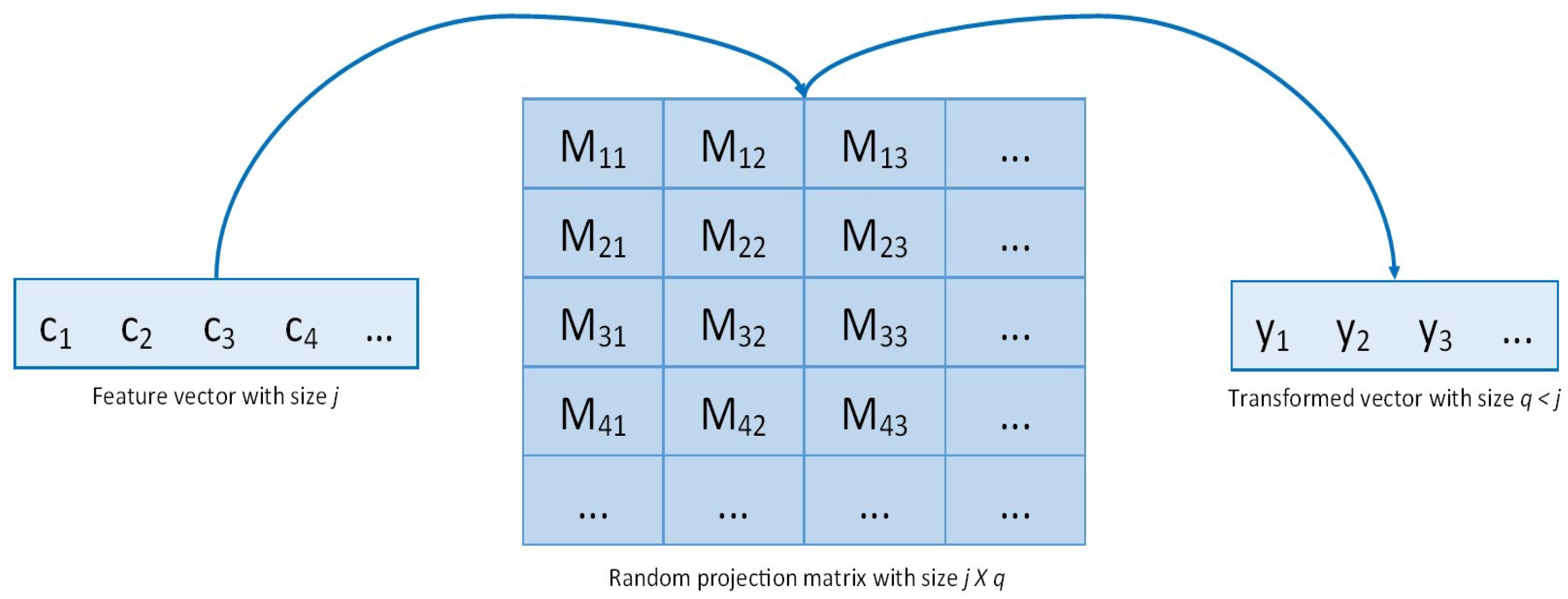
3.2. Hybrid Protection Scheme
4. Experimental Results and Analysis
4.1. LSTM Neural Network Architecture
4.2. Dataset
4.3. Results
4.4. Comparative Analysis
4.5. Paillier Cryptosystem Security Analysis
4.6. Noninvertibility Analysis
4.7. Renewability Analysis
4.8. Computational Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cicirelli, G.; Impedovo, D.; Dentamaro, V.; Marani, R.; Pirlo, G.; D’Orazio, T.R. Human Gait Analysis in Neurodegenerative Diseases: A Review. IEEE J. Biomed. Health Inform. 2022, 26, 229–242. [Google Scholar] [CrossRef] [PubMed]
- Dentamaro, V.; Impedovo, D.; Pirlo, G. Gait Analysis for Early Neurodegenerative Diseases Classification Through the Kinematic Theory of Rapid Human Movements. IEEE Access 2020, 8, 193966–193980. [Google Scholar] [CrossRef]
- Gao, H.-M.; Hong, J.-S. Why neurodegenerative diseases are progressive: Uncontrolled inflammation drives disease progression. Trends. Immunol. 2008, 29, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Simon, T.; Wei, S.-E.; Sheikh, Y. Realtime Multi-person 2D Pose Estimation Using Part Affinity Fields. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 1302–1310. [Google Scholar]
- Bertram, L.; Tanzi, R.E. The genetic epidemiology of neurodegenerative disease. J. Clin. Investig. 2005, 115, 1449–1457. [Google Scholar] [CrossRef] [PubMed]
- Dauer, W.; Przedborski, S. Parkinson’s Disease: Mechanisms and Models. Neuron 2003, 39, 889–909. [Google Scholar] [CrossRef] [PubMed]
- Ross, C.A.; Tabrizi, S.J. Huntington’s disease: From molecular pathogenesis to clinical treatment. Lancet Neurol. 2011, 10, 83–98. [Google Scholar] [CrossRef]
- Gattulli, V.; Impedovo, D.; Pirlo, G.; Semeraro, G. Early Dementia Identification: On the Use of Random Handwriting Strokes. In Intertwining Graphonomics with Human Movements. IGS 2022. Lecture Notes in Computer Science; Carmona-Duarte, C., Diaz, M., Ferrer, M.A., Morales, A., Eds.; Springer: Cham, Switzerland, 2022; Volume 13424, pp. 285–300. [Google Scholar] [CrossRef]
- Pirker, W.; Katzenschlager, R. Gait disorders in adults and the elderly. Wien. Klin. Wochenschr. 2017, 129, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Alharthi, A.S.; Yunas, S.U.; Ozanyan, K.B. Deep Learning for Monitoring of Human Gait: A Review. IEEE Sens. J. 2019, 19, 9575–9591. [Google Scholar] [CrossRef]
- Kwon, H.; Clifford, G.D.; Genias, I.; Bernhard, D.; Esper, C.D.; Factor, S.A.; McKay, J.L. An Explainable Spatial-Temporal Graphical Convolutional Network to Score Freezing of Gait in Parkinsonian Patients. Sensors 2023, 23, 1766. [Google Scholar] [CrossRef]
- Ghoraani, B.; Boettcher, L.N.; Hssayeni, M.D.; Rosenfeld, A.; Tolea, M.I.; Galvin, J.E. Detection of mild cognitive impairment and Alzheimer’s disease using dual-task gait assessments and machine learning. Biomed. Signal Process. Control 2021, 64, 102249. [Google Scholar] [CrossRef]
- Erdaş, Ç.B.; Sümer, E.; Kibaroğlu, S. CNN-based severity prediction of neurodegenerative diseases using gait data. Digit. Health 2022, 8, 20552076221075147. [Google Scholar] [CrossRef]
- Giannakopoulou, K.M.; Roussaki, I.; Demestichas, K. Internet of Things Technologies and Machine Learning Methods for Parkinson’s Disease Diagnosis, Monitoring and Management: A Systematic Review. Sensors 2022, 22, 1799. [Google Scholar] [CrossRef] [PubMed]
- Qayyum, A.; Qadir, J.; Bilal, M.; Al-Fuqaha, A. Secure and Robust Machine Learning for Healthcare: A Survey. IEEE Rev. Biomed. Eng. 2021, 14, 156–180. [Google Scholar] [CrossRef] [PubMed]
- Shafahi, A.; Huang, W.R.; Najibi, M.; Suciu, O.; Studer, C.; Dumitras, T.; Goldstein, T. Poison Frogs! Targeted Clean-Label Poisoning Attacks on Neural Networks. arXiv 2018, arXiv:abs/1804.00792. [Google Scholar]
- Finlayson, S.G.; Kohane, I.S.; Beam, A. Adversarial At-tacks Against Medical Deep Learning Systems. arXiv 2018, arXiv:abs/1804.05296. [Google Scholar]
- Dentamaro, V.; Giglio, P.; Impedovo, D.; Moretti, L.; Pirlo, G. AUCO ResNet: An end-to-end network for Covid-19 pre-screening from cough and breath. Pattern Recognit. 2022, 127, 108656. [Google Scholar] [CrossRef] [PubMed]
- Al-Rubaie, M.; Chang, J.M. Privacy-Preserving Machine Learning: Threats and Solutions. IEEE Secur. Priv. 2019, 17, 49–58. [Google Scholar] [CrossRef]
- Kaur, H.; Khanna, P. Privacy preserving remote multi-server biometric authentication using cancelable biometrics and secret sharing. Future Gener. Comput. Syst. 2020, 102, 30–41. [Google Scholar] [CrossRef]
- Hamme, T.; Garofalo, G.; Rúa, E.A.; Preuveneers, D.; Joosen, W. A Systematic Comparison of Age and Gender Prediction on IMU Sensor-Based Gait Traces. Sensors 2019, 19, 2945. [Google Scholar] [CrossRef]
- Podschwadt, R.; Takabi, D.; Hu, P.; Rafiei, M.H.; Cai, Z. A Survey of Deep Learning Architectures for Privacy-Preserving Machine Learning With Fully Homomorphic Encryption. IEEE Access 2022, 10, 117477–117500. [Google Scholar] [CrossRef]
- ISO/IEC 24745:2022; Information Security, Cybersecurity and Privacy Protection—Biometric Information Protection. Available online: https://www.iso.org/standard/75302.html (accessed on 16 January 2023).
- Zhou, Y.; Song, L.; Liu, Y.; Vijayakumar, P.; Gupta, B.B.; Alhalabi, W.; Alsharif, H. A privacy-preserving logistic regression-based diagnosis scheme for digital healthcare. Future Gener. Comput. Syst. 2023, 144, 63–73. [Google Scholar] [CrossRef]
- Tieu, N.-D.T.; Nguyen, H.H.; Nguyen-Son, H.-Q.; Yamagishi, J.; Echizen, I. Spatio-temporal generative adversarial network for gait anonymization. J. Inf. Secur. Appl. 2019, 46, 307–319. [Google Scholar] [CrossRef]
- Guo, X.; Lin, H.; Wu, Y.; Peng, M. A new data clustering strategy for enhancing mutual privacy in healthcare IoT systems. Future Gener. Comput. Syst. 2020, 113, 407–417. [Google Scholar] [CrossRef]
- Deng, G.; Tang, M.; Xi, Y.; Zhang, M. Privacy-Preserving Online Medical Prediagnosis Training Model Based on Soft-Margin SVM. IEEE Trans. Serv. Comput. 2022, 16, 2072–2084. [Google Scholar] [CrossRef]
- Chen, Y.; Mao, Q.; Wang, B.; Duan, P.; Zhang, B.; Hong, Z. Privacy-Preserving Multi-Class Support Vector Machine Model on Medical Diagnosis. IEEE J. Biomed. Health Inform. 2022, 26, 3342–3353. [Google Scholar] [CrossRef]
- Xie, B.; Xiang, T.; Liao, X.; Wu, J. Achieving Privacy-Preserving Online Diagnosis With Outsourced SVM in Internet of Medical Things Environment. IEEE Trans. Dependable Secur. Comput. 2022, 19, 4113–4126. [Google Scholar] [CrossRef]
- Behera, S.; Rekha, B.; Pandey, P.; Vidya, B.; Prathuri, J.R. Preserving the Privacy of Medical Data using Homomorphic Encryption and Prediction of Heart Disease using K-Nearest Neighbor. In Proceedings of the IEEE International Conference on Data Science and Information System, ICDSIS 2022, Malnad College of Engineering, Hassan, Karnataka, India, 29–30 July 2022. [Google Scholar] [CrossRef]
- Bost, R.; Popa, R.A.; Tu, S.; Goldwasser, S. Machine Learning Classification over Encrypted Data. In Proceedings of the Network and Distributed System Security (NDSS) Symposium, San Diego, CA, USA, 8–11 February 2015; Available online: https://www.ndss-symposium.org/wp-content/uploads/2017/09/04_1_2.pdf (accessed on 1 October 2023).
- Podschwadt, R.; Takabi, D. Non-interactive Privacy Pre-serving Recurrent Neural Network Prediction with Homo-morphic Encryption. In Proceedings of the IEEE International Conference on Cloud Computing, CLOUD, Chicago, IL, USA, 5–10 September 2021; pp. 65–70. [Google Scholar] [CrossRef]
- Yang, W.; Wang, S.; Shahzad, M.; Zhou, W. A cancelable biometric authentication system based on feature-adaptive random projection. J. Inf. Secur. Appl. 2021, 58, 102704. [Google Scholar] [CrossRef]
- Chen, S.; Lach, J.; Lo, B.; Yang, G.-Z. Toward Pervasive Gait Analysis With Wearable Sensors: A Systematic Review. IEEE J. Biomed. Health Inform. 2016, 20, 1521–1537. [Google Scholar] [CrossRef]
- Shahreza, H.O.; Rathgeb, C.; Osorio-Roig, D.; Hahn, V.K.; Marcel, S.; Busch, C. Hybrid Protection of Biometric Tem-plates by Combining Homomorphic Encryption and Cancel-able Biometrics. In Proceedings of the 2022 IEEE International Joint Conference on Biometrics, IJCB 2022, Abu Dhabi, United Arab Emirates, 10–13 October 2022. [Google Scholar] [CrossRef]
- De Groote, F.; De Laet, T.; Jonkers, I.; Schutter, J. Kalman smoothing improves the estimation of joint kinematics and kinetics in marker-based human gait analysis. J. Biomech. 2008, 41, 3390–3398. [Google Scholar] [CrossRef]
- Lukšys, D.; Jatužis, D.; Jonaitis, G.; Griškevičius, J. Application of continuous relative phase analysis for differentiation of gait in neurodegenerative disease. Biomed. Signal Process. Control 2021, 67, 102558. [Google Scholar] [CrossRef]
- Dentamaro, V.; Impedovo, D.; Pirlo, G. Fall Detection by Human Pose Estimation and Kinematic Theory. In Proceedings of the 2020 25th International Conference on Pattern Recognition (ICPR), Milan, Italy, 10–15 January 2021; pp. 2328–2335. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-Learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Johnson, W.B.; Lindenstrauss, J.; Schechtman, G. Exten-sions of lipschitz maps into Banach spaces. Isr. J. Math. 1986, 54, 129–138. [Google Scholar] [CrossRef]
- Bingham, E.; Mannila, H. Random projection in dimensionality reduction: Applications to image and text data. In Proceedings of the Seventh ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 26–29 August 2001; pp. 245–250. [Google Scholar] [CrossRef]
- Zou, F.; Shen, L.; Jie, Z.; Zhang, W.; Liu, W. A Sufficient Condition for Convergences of Adam and RMSPro. In Proceedings of the 2019 IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Long Beach, CA, USA, 15–20 June 2019; pp. 1119–11127. [Google Scholar] [CrossRef]
- Cheriet, M.; Dentamaro, V.; Hamdan, M.; Impedovo, D.; Pirlo, G. Multi-speed transformer network for neurodegenerative disease assessment and activity recognition. Comput. Methods Programs Biomed. 2023, 230, 107344. [Google Scholar] [CrossRef] [PubMed]
- Will, M.A.; Ko, R.K.L. A guide to homomorphic encryption. In The Cloud Security Ecosystem: Technical, Legal, Business and Management Issues; Elsevier: Waltham, MA, USA, 2015; pp. 101–127. [Google Scholar] [CrossRef]
- Steeb, W.-H. Problems and Solutions in Introductory and Advanced Matrix Calculus; World Scientific Publishing Co. Pte Ltd.: Singapore, 2006; 252p. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Feature | Description |
|---|---|---|
| Temporal space | Displacement | |
| Displacement x | ||
| Displacement y | ||
| Velocity | ||
| Velocity x | ||
| Velocity y | ||
| Acceleration | ||
| Acceleration x | ||
| Acceleration y | ||
| Tangent angle | ||
| Sigma–lognormal features | Lognormal stroke number | Number of lognormal strokes |
| D parameter | D parameter for all lognormal strokes | |
| parameter | parameter for all lognormal strokes | |
| parameter | parameter for all lognormal strokes | |
| parameter | parameter for all lognormal strokes | |
| Corners | Nose–neck–hip | Angle between nose, neck, and hip |
| Neck–hip–knee | Angle between neck, hip, and knee | |
| Shoulder–elbow–wrist | Angle between shoulder, elbow, and wrist | |
| Hip–knee–ankle | Angle between hip, knee, and ankle | |
| Right knee–hip–left knee | Angle between right knee, hip, and left knee |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Patients | |
| Adults aged 65 to 90 years | Refusal to give informed consent |
| Diagnosis of mild to severe dementia | Any condition that would limit the ability of the patient to participate in the study |
| Gender-inclusive: 6 men and 14 women | Patients who did not complete all the required walking tasks |
| Healthy controls | |
| Adults aged 30 to 75 years | Refusal to give informed consent |
| No dementia diagnosis | Subject who did not complete all the required walking tasks |
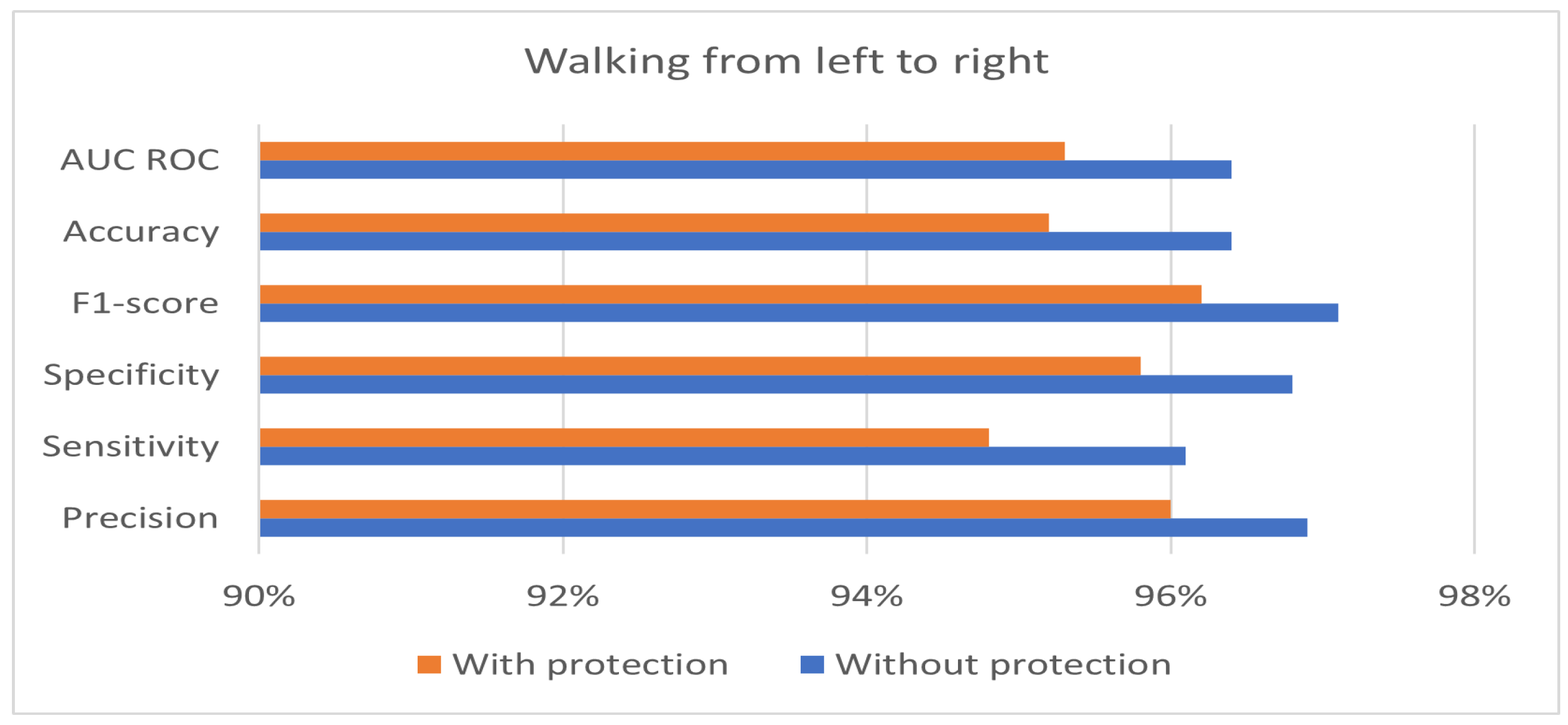
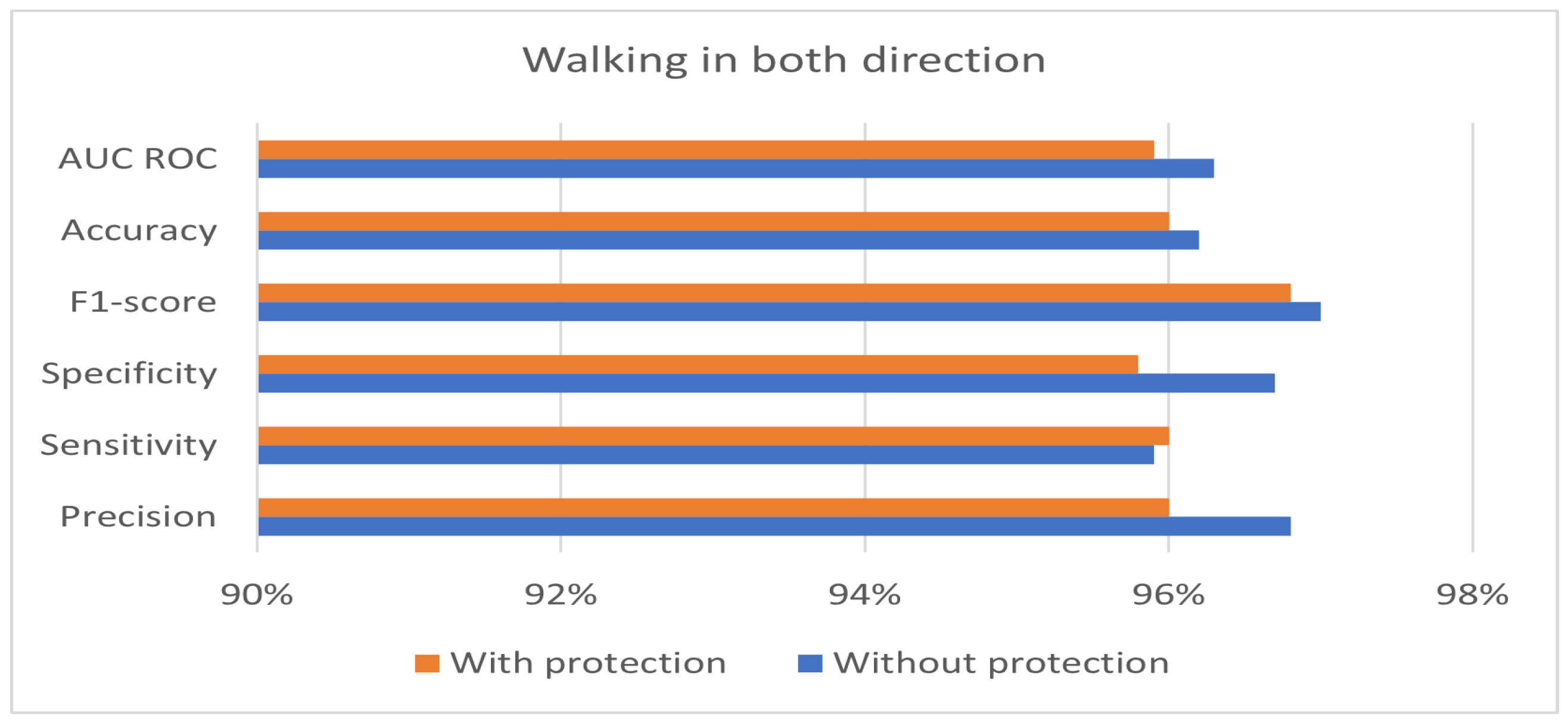
| Score | Walking from Left to Right | Walking from Right to Left | Walking in Both Directions |
|---|---|---|---|
| Precision | 96.9% | 97.3% | 96.8% |
| Sensitivity | 96.1% | 96.7% | 95.9% |
| Specificity | 96.8% | 97.2% | 96.7% |
| F1-score | 97.1% | 97.5% | 97.0% |
| Accuracy | 96.4% | 96.8% | 96.2% |
| AUC ROC | 96.4% | 96.9% | 96.3% |
| Score | Walking from Left to Right | Walking from Right to Left | Walking in Both Directions |
|---|---|---|---|
| Precision | 96.0% | 96.7% | 96.0% |
| Sensitivity | 94.8% | 97.4% | 96.0% |
| Specificity | 95.8% | 96.5% | 95.8% |
| F1-score | 96.2% | 97.7% | 96.8% |
| Accuracy | 95.2% | 97.0% | 96.0% |
| AUC ROC | 95.3% | 97.0% | 95.9% |
| Score | Walking from Left to Right | Walking from Right to Left | Walking in Both Directions |
|---|---|---|---|
| Precision | 0.9% | 0.6% | 0.8% |
| Sensitivity | 1.3% | −0.7% | −0.1% |
| Specificity | 1.0% | 0.7% | 0.9% |
| F1-score | 0.9% | −0.2% | 0.2% |
| Accuracy | 1.2% | −0.2% | 0.2% |
| AUC ROC | 1.1% | −0.1% | 0.4% |
| Work | Prec. | Sens. | Spec. | F1 | Acc. | AUC |
|---|---|---|---|---|---|---|
| [2] | 97.7% | 96.9% | 97.1% | 96.7% | 96.9% | 96.9% |
| [43] | 95.9% | 95.3% | 95.7% | 95.5% | 95.5% | 96.1% |
| Proposed system | 96.7% | 97.4% | 96.5% | 97.7% | 97.0% | 97.0% |
| Phase | Running Time (s) |
|---|---|
| Encryption | 3.322 |
| Random projection | 53.899 |
| Decryption | 0.0389 |
| Total | 57.259 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castro, F.; Impedovo, D.; Pirlo, G. A Hybrid Protection Scheme for the Gait Analysis in Early Dementia Recognition. Sensors 2024, 24, 24. https://doi.org/10.3390/s24010024
Castro F, Impedovo D, Pirlo G. A Hybrid Protection Scheme for the Gait Analysis in Early Dementia Recognition. Sensors. 2024; 24(1):24. https://doi.org/10.3390/s24010024
Chicago/Turabian StyleCastro, Francesco, Donato Impedovo, and Giuseppe Pirlo. 2024. "A Hybrid Protection Scheme for the Gait Analysis in Early Dementia Recognition" Sensors 24, no. 1: 24. https://doi.org/10.3390/s24010024
APA StyleCastro, F., Impedovo, D., & Pirlo, G. (2024). A Hybrid Protection Scheme for the Gait Analysis in Early Dementia Recognition. Sensors, 24(1), 24. https://doi.org/10.3390/s24010024