

Investigating Activity Recognition for Hemiparetic Stroke Patients Using Wearable Sensors: A Deep Learning Approach with Data Augmentation


Abstract
:1. Introduction
1.1. Motivation
1.2. Related Work
2. Materials and Methods
2.1. Experiments
2.1.1. Participants
2.1.2. Selection of Upper Extremity Movements
2.1.3. Experimental Environments
2.1.4. Sensors
2.1.5. Experimental Procedures
2.2. Data Analysis
2.2.1. Data Annotation and Exclusion
2.2.2. Preprocessing and Asymmetry Score
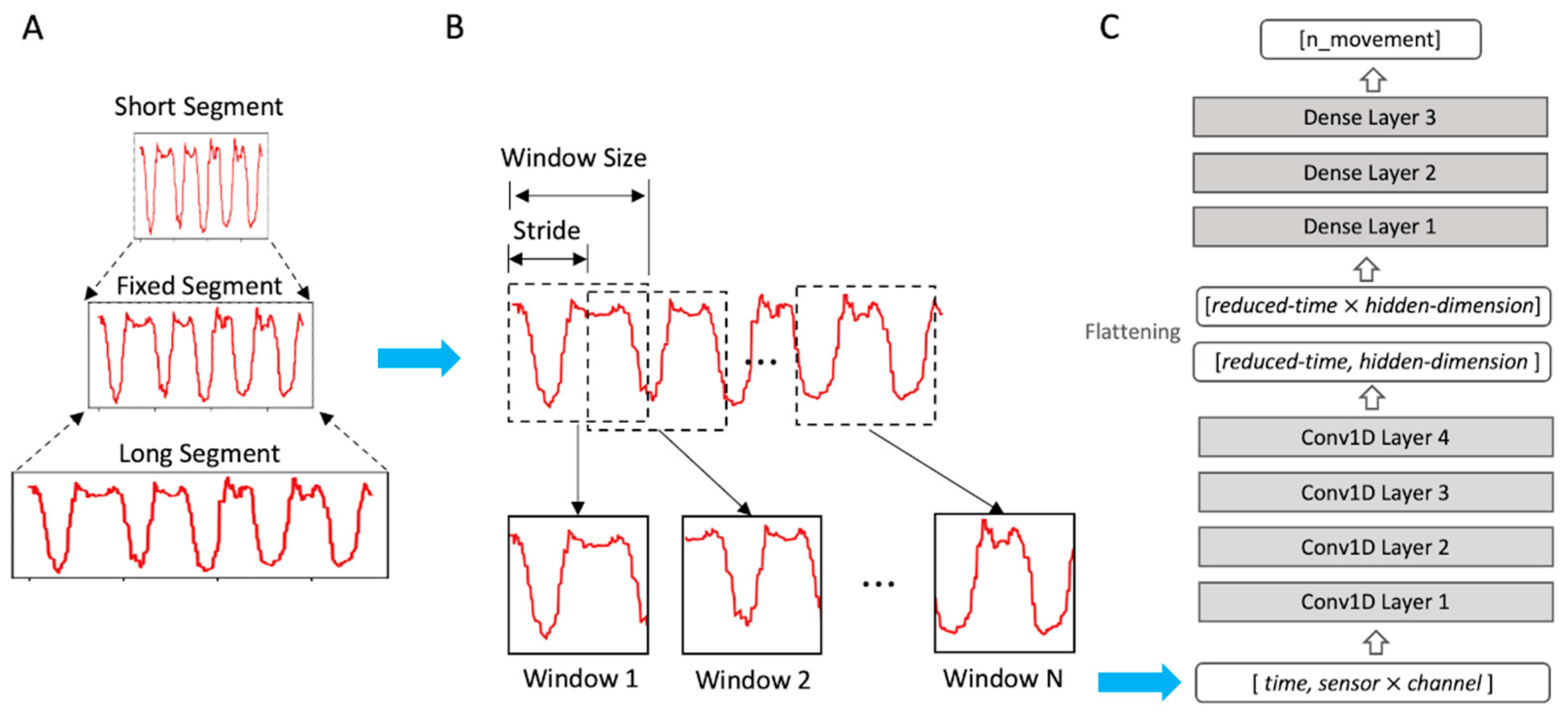
2.2.3. Linear Interpolation and Sliding Windows
2.2.4. Model
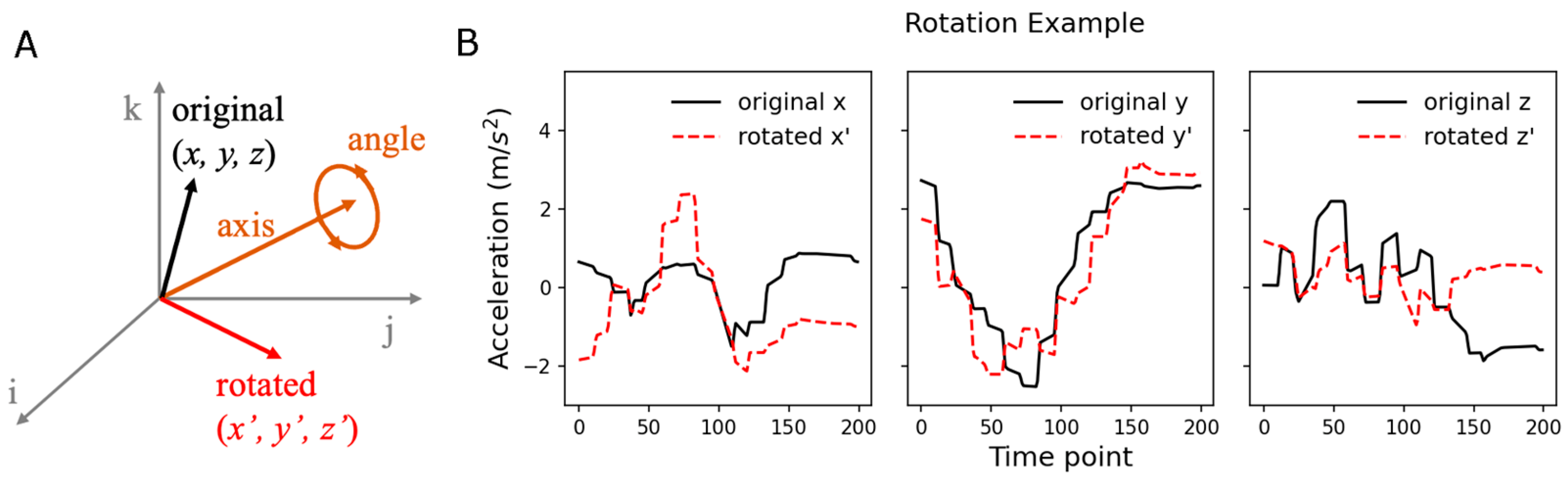
2.2.5. Data Augmentation
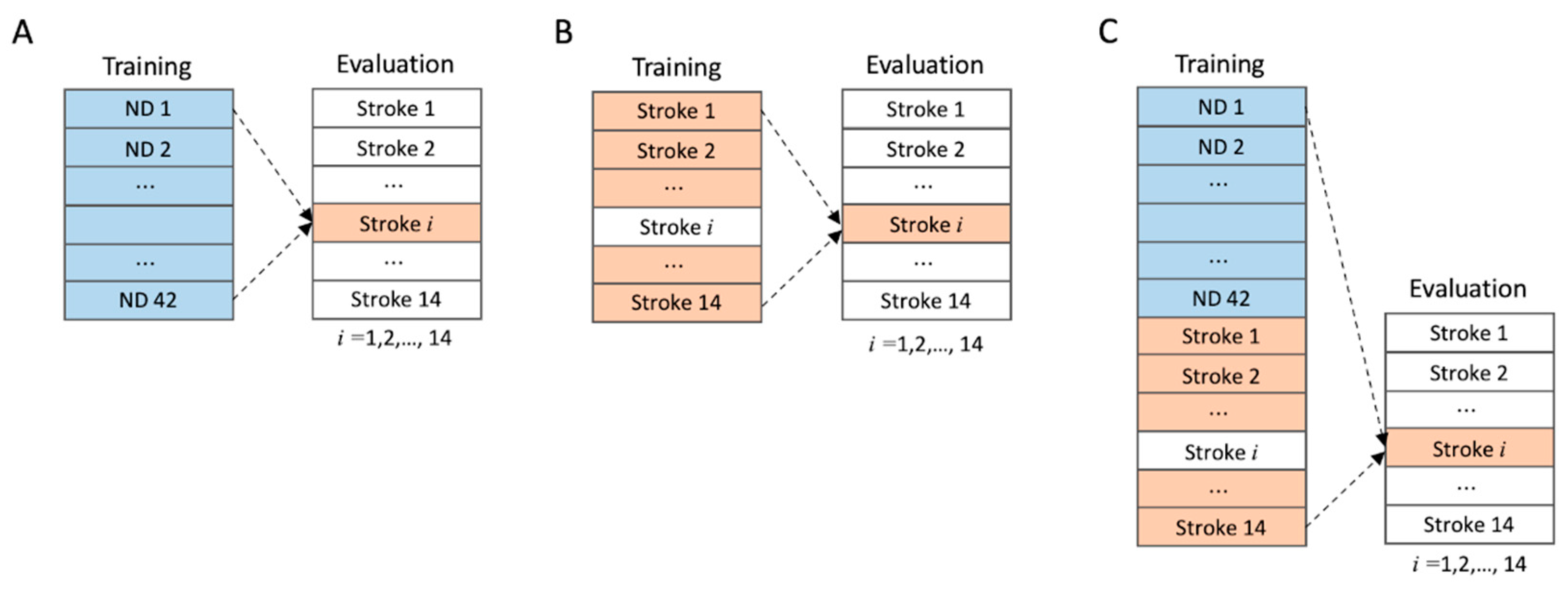
2.2.6. Training and Evaluation
2.2.7. Statistical Analysis
3. Results
3.1. Data Exploration
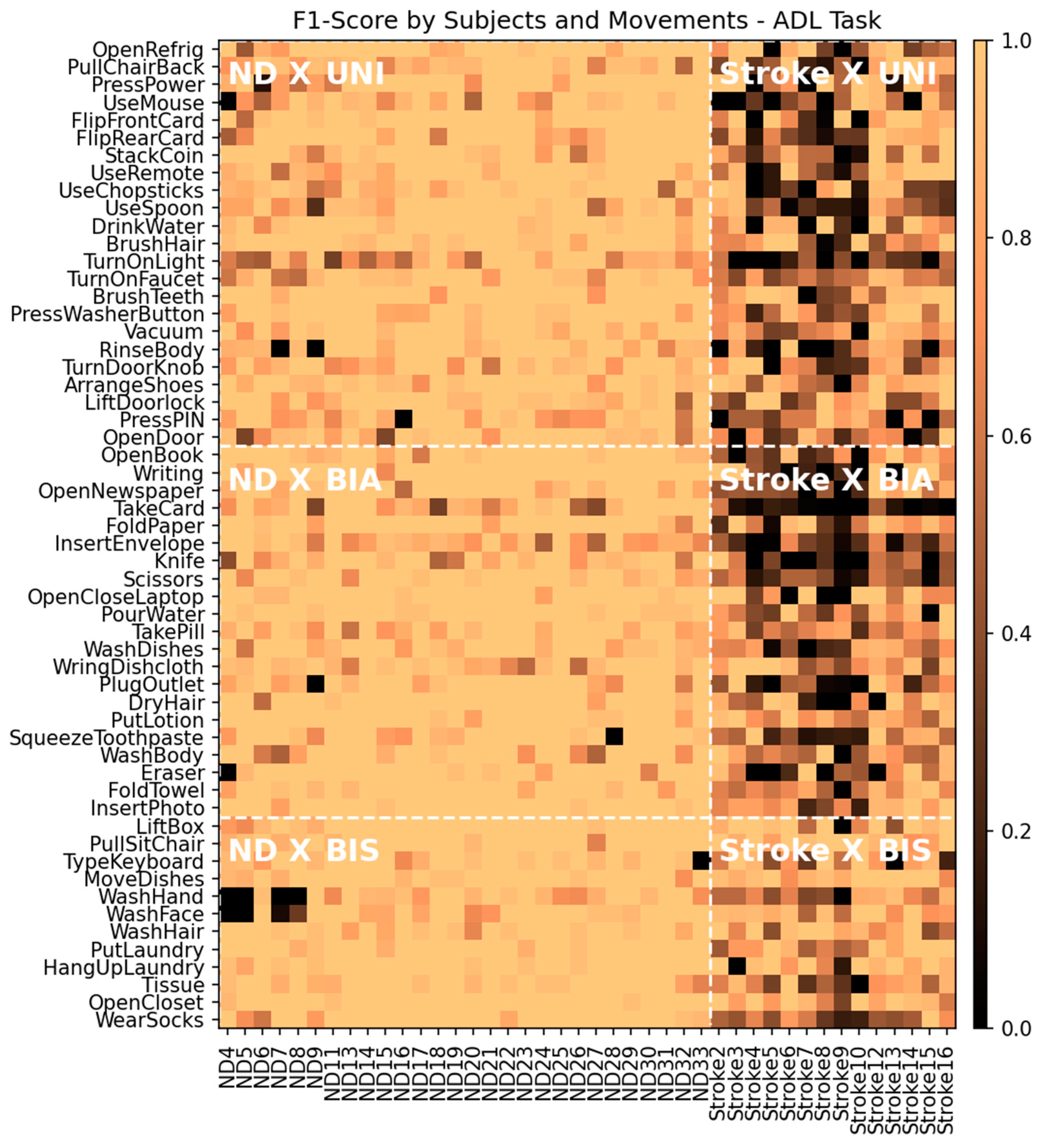
3.2. Training Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Taub, E.; Uswatte, G.; Mark, V.W.; Morris, D.M. The Learned Nonuse Phenomenon: Implications for Rehabilitation. Eur. Medicophys. 2006, 42, 241–255. [Google Scholar]
- Uswatte, G.; Taub, E.; Morris, D.; Light, K.; Thompson, P.A. The Motor Activity Log-28: Assessing Daily Use of the Hemiparetic Arm after Stroke. Neurology 2006, 67, 1189–1194. [Google Scholar] [CrossRef] [PubMed]
- Kwakkel, G.; Kollen, B.J.; Van der Grond, J.V.; Prevo, A.J.H. Probability of Regaining Dexterity in the Flaccid Upper Limb: Impact of Severity of Paresis and Time since Onset in Acute Stroke. Stroke 2003, 34, 2181–2186. [Google Scholar] [CrossRef] [PubMed]
- Haaland, K.Y.; Mutha, P.K.; Rinehart, J.K.; Daniels, M.; Cushnyr, B.; Adair, J.C. Relationship between Arm Usage and Instrumental Activities of Daily Living after Unilateral Stroke. Arch. Phys. Med. Rehabil. 2012, 93, 1957–1962. [Google Scholar] [CrossRef] [PubMed]
- Schweighofer, N.; Han, C.E.; Wolf, S.L.; Arbib, M.A.; Winstein, C.J. A Functional Threshold for Long-Term Use of Hand and Arm Function Can Be Determined: Predictions from a Computational Model and Supporting Data from the Extremity Constraint-Induced Therapy Evaluation (EXCITE) Trial. Phys. Ther. 2009, 89, 1327–1336. [Google Scholar] [CrossRef] [PubMed]
- Hidaka, Y.; Han, C.E.; Wolf, S.L.; Winstein, C.J.; Schweighofer, N. Use It and Improve It or Lose It: Interactions between Arm Function and Use in Humans Post-Stroke. PLoS Comput. Biol. 2012, 8, e1002343. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.K.; Shawen, N.; Mummidisetty, C.K.; Kaur, S.; Bo, X.; Poellabauer, C.; Kording, K.; Jayaraman, A. Activity Recognition for Persons with Stroke Using Mobile Phone Technology: Toward Improved Performance in a Home Setting. J. Med. Internet Res. 2017, 19, e184. [Google Scholar] [CrossRef]
- Lee, S.I.; Adans-Dester, C.P.; Grimaldi, M.; Dowling, A.V.; Horak, P.C.; Black-Schaffer, R.M.; Bonato, P.; Gwin, J.T. Enabling Stroke Rehabilitation in Home and Community Settings: A Wearable Sensor-Based Approach for Upper-Limb Motor Training. IEEE J. Transl. Eng. Health Med. 2018, 6, 2100411. [Google Scholar] [CrossRef]
- Uswatte, G.; Miltner, W.H.R.; Foo, B.; Varma, M.; Moran, S.; Taub, E. Objective Measurement of Functional Upper-Extremity Movement Using Accelerometer Recordings Transformed with a Threshold Filter. Stroke 2000, 31, 662–667. [Google Scholar] [CrossRef]
- Parnandi, A.; Wade, E.; Mataric, M. Functional Score Estimation of Post-Stroke Assessment Test from Wearable Inertial Sensor Data. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Buenos Aires, Argentina, 31 August–4 September 2010; pp. 86–89. [Google Scholar]
- Chen, Y.-A.; Lewthwaite, R.; Schweighofer, N.; Monterosso, J.R.; Fisher, B.E.; Winstein, C. The Essential Role of Social Context and Self-Efficacy in Daily Paretic Arm/Hand Use after Stroke: An Ecological Momentary Assessment Study with Accelerometry. Arch. Phys. Med. Rehabil. 2022, 104, 390–402. [Google Scholar] [CrossRef]
- Lucas, A.; Hermiz, J.; Labuzetta, J.; Arabadzhi, Y.; Karanjia, N.; Gilja, V. Use of Accelerometry for Long Term Monitoring of Stroke Patients. IEEE J. Transl. Eng. Health Med. 2019, 7, 2100310. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Shao, J.; Xu, X.S.; Shen, H.T. Max-Margin Adaptive Model for Complex Video Pattern Recognition. Multimed. Tools Appl. 2015, 74, 505–521. [Google Scholar] [CrossRef]
- MacEira-Elvira, P.; Popa, T.; Schmid, A.C.; Hummel, F.C. Wearable Technology in Stroke Rehabilitation: Towards Improved Diagnosis and Treatment of Upper-Limb Motor Impairment. J. Neuroeng. Rehabil. 2019, 16, 142. [Google Scholar] [CrossRef] [PubMed]
- Bulling, A.; Blanke, U.; Schiele, B. A Tutorial on Human Activity Recognition Using Body-Worn Inertial Sensors. ACM Comput. Surv. 2014, 46, 1–33. [Google Scholar] [CrossRef]
- Adans-Dester, C.; Hankov, N.; O’Brien, A.; Vergara-Diaz, G.; Black-Schaffer, R.; Zafonte, R.; Dy, J.; Lee, S.I.; Bonato, P. Enabling Precision Rehabilitation Interventions Using Wearable Sensors and Machine Learning to Track Motor Recovery. NPJ Digit. Med. 2020, 3, 121. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.K.M.; Leo, K.-H.; Sanel, S.; Chew, E.; Zhao, L. Triaxial Rehabilitative Data Analysis Incorporating Matching Pursuit. In Proceedings of the 2017 25th European Signal Processing Conference (EUSIPCO), Kos, Greece, 28 August–2 September 2017. [Google Scholar]
- Formstone, L.; Huo, W.; Wilson, S.; McGregor, A.; Bentley, P.; Vaidyanathan, R. Quantification of Motor Function Post-Stroke Using Novel Combination of Wearable Inertial and Mechanomyographic Sensors. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 1158–1167. [Google Scholar] [CrossRef] [PubMed]
- Panwar, M.; Biswas, D.; Bajaj, H.; Jobges, M.; Turk, R.; Maharatna, K.; Acharyya, A. Rehab-Net: Deep Learning Framework for Arm Movement Classification Using Wearable Sensors for Stroke Rehabilitation. IEEE Trans. Biomed. Eng. 2019, 66, 3026–3037. [Google Scholar] [CrossRef] [PubMed]
- Kaku, A.; Parnandi, A.; Venkatesan, A.; Pandit, N.; Schambra, H.; Fernandez-Granda, C. Towards Data-Driven Stroke Rehabilitation via Wearable Sensors and Deep Learning. In Proceedings of the 5th Machine Learning for Healthcare Conference, Virtual, 7–8 August 2020; Volume 126, pp. 143–171. [Google Scholar]
- Boukhennoufa, I.; Zhai, X.; Utti, V.; Jackson, J.; McDonald-Maier, K.D. A Comprehensive Evaluation of State-of-the-Art Time-Series Deep Learning Models for Activity-Recognition in Post-Stroke Rehabilitation Assessment. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBS), Virtual, 1 November–5 November 2021; Institute of Electrical and Electronics Engineers Inc.: New York, NY, USA, 2021; pp. 2242–2247. [Google Scholar]
- Kiranyaz, S.; Avci, O.; Abdeljaber, O.; Ince, T.; Gabbouj, M.; Inman, D.J. 1D Convolutional Neural Networks and Applications: A Survey. Mech. Syst. Signal Process. 2021, 151, 107398. [Google Scholar] [CrossRef]
- Hochreiter, S.; Schmidhuber, J. Long Short-Term Memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef]
- Cho, K.; Van Merriënboer, B.; Gulcehre, C.; Bahdanau, D.; Bougares, F.; Schwenk, H.; Bengio, Y. Learning Phrase Representations Using RNN Encoder-Decoder for Statistical Machine Translation. arXiv 2014, arXiv:1406.1078. [Google Scholar]
- Zhang, S.; Li, Y.; Zhang, S.; Shahabi, F.; Xia, S.; Deng, Y.; Alshurafa, N. Deep Learning in Human Activity Recognition with Wearable Sensors: A Review on Advances. Sensors 2022, 22, 1476. [Google Scholar] [CrossRef] [PubMed]
- Rose, D.K.; Winstein, C.J. Bimanual Training After Stroke: Are Two Hands Better Than One? Top. Stroke Rehabil. 2004, 11, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Desrosiers, J.; Bourbonnais, D.; Corriveau, H.; Gosselin, S.; Bravo, G. Effectiveness of Unilateral and Symmetrical Bilateral Task Training for Arm during the Subacute Phase after Stroke: A Randomized Controlled Trial. Clin. Rehabil. 2005, 19, 581–593. [Google Scholar] [CrossRef] [PubMed]
- Van Delden, A.; Peper, C.; Beek, P.; Kwakkel, G. Unilateral versus Bilateral Upper Limb Exercise Therapy after Stroke: A Systematic Review. J. Rehabil. Med. 2012, 44, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.R.; Klaesner, J.W.; Lang, C.E. Quantifying Real-World Upper-Limb Activity in Nondisabled Adults and Adults with Chronic Stroke. Neurorehabilit. Neural Repair 2015, 29, 969–978. [Google Scholar] [CrossRef] [PubMed]
- Um, T.T.; Pfister, F.M.J.; Pichler, D.; Endo, S.; Lang, M.; Hirche, S.; Fietzek, U.; Kulic, D. Data Augmentation of Wearable Sensor Data for Parkinson’s Disease Monitoring Using Convolutional Neural Networks. In Proceedings of the 19th ACM International Conference on Multimodal Interaction(ICMI 2017), Glasgow, Scotland, 13–17 November 2017; Association for Computing Machinery, Inc.: New York, NY, USA, 2017; Volume 2017, pp. 216–220. [Google Scholar]
- Winstein, C.; Kim, B.; Kim, S.; Martinez, C.; Schweighofer, N. Dosage Matters: A Phase IIb Randomized Controlled Trial of Motor Therapy in the Chronic Phase after Stroke. Stroke 2019, 50, 1831–1837. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, R.C. The Assessment and Analysis of Handedness: The Edinburgh Inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The Post-Stroke Hemiplegic Patient. 1. a Method for Evaluation of Physical Performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [CrossRef]
- Chen, S.; Wolf, S.L.; Zhang, Q.; Thompson, P.A.; Winstein, C.J. Minimal Detectable Change of the Actual Amount of Use Test and the Motor Activity Log: The EXCITE Trial. Neurorehabil. Neural Repair 2012, 26, 507–514. [Google Scholar] [CrossRef]
- Winstein, C.J.; Wolf, S.L.; Dromerick, A.W.; Lane, C.J.; Nelsen, M.A.; Lewthwaite, R.; Cen, S.Y.; Azen, S.P. Effect of a Task-Oriented Rehabilitation Program on Upper Extremity Recovery Following Motor Stroke: The ICARE Randomized Clinical Trial. JAMA 2016, 315, 571–581. [Google Scholar] [CrossRef]
- Wolf, S.L.; Catlin, P.A.; Ellis, M.; Archer, A.L.; Morgan, B.; Piacentino, A. Assessing Wolf Motor Function Test as Outcome Measure for Research in Patients After Stroke. Stroke 2001, 32, 1635–1639. [Google Scholar] [CrossRef] [PubMed]
- Ashford, S.; Slade, M.; Malaprade, F.; Turner-Stokes, L. Evaluation of Functional Outcome Measures for the Hemiparetic Upper Limb: A Systematic Review. J. Rehabil. Med. 2008, 40, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Costenoble, A.; Knoop, V.; Vermeiren, S.; Vella, R.A.; Debain, A.; Rossi, G.; Bautmans, I.; Verté, D.; Gorus, E.; De Vriendt, P. A Comprehensive Overview of Activities of Daily Living in Existing Frailty Instruments: A Systematic Literature Search. Gerontologist 2021, 61, e12–e22. [Google Scholar] [CrossRef] [PubMed]
- Lecun, Y.; Bottou, L.; Bengio, Y.; Haffner, P. Gradient-Based Learning Applied to Document Recognition. Proc. IEEE 1998, 86, 2278–2324. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet Classification with Deep Convolutional Neural Networks. Commun. ACM 2017, 60, 84–90. [Google Scholar] [CrossRef]
- Le, Q.V.; Jaitly, N.; Hinton, G.E. A Simple Way to Initialize Recurrent Networks of Rectified Linear Units. arXiv 2015, arXiv:1504.00941. [Google Scholar] [CrossRef]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A Simple Way to Prevent Neural Networks from Overfitting. J. Mach. Learn. Res. 2014, 5, 1929–1958. [Google Scholar]
- Shorten, C.; Khoshgoftaar, T.M. A Survey on Image Data Augmentation for Deep Learning. J. Big Data 2019, 6, 60. [Google Scholar] [CrossRef]
- Loshchilov, I.; Hutter, F. Decoupled Weight Decay Regularization. arXiv 2017, arXiv:1711.05101. [Google Scholar]
- Raudenbush, S.W.; Bryk, A.S. Hierarchical Linear Models: Applications and Data Analysis Methods (Vol. 1), 2nd ed.; SAGE Publications: London, UK, 2001. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; The R Foundation: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Bochniewicz, E.M.; Emmer, G.; McLeod, A.; Barth, J.; Dromerick, A.W.; Lum, P. Measuring Functional Arm Movement after Stroke Using a Single Wrist-Worn Sensor and Machine Learning. J. Stroke Cerebrovasc. Dis. 2017, 26, 2880–2887. [Google Scholar] [CrossRef]
- Chen, P.W.; Baune, N.A.; Zwir, I.; Wang, J.; Swamidass, V.; Wong, A.W.K. Measuring Activities of Daily Living in Stroke Patients with Motion Machine Learning Algorithms: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 1634. [Google Scholar] [CrossRef] [PubMed]
- Miao, S.; Shen, C.; Feng, X.; Zhu, Q.; Shorfuzzaman, M.; Lv, Z. Upper Limb Rehabilitation System for Stroke Survivors Based on Multi-Modal Sensors and Machine Learning. IEEE Access 2021, 9, 30283–30291. [Google Scholar] [CrossRef]
- Boukhennoufa, I.; Zhai, X.; Utti, V.; Jackson, J.; McDonald-Maier, K.D. Wearable Sensors and Machine Learning in Post-Stroke Rehabilitation Assessment: A Systematic Review. Biomed. Signal Process. Control 2022, 71, 103197. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Handedness (R a/L b) | Affected Side (R/L) | Gender (F/M) | Age (Years) | Stroke Onset (Months) | FMA-UE c | MMSE-K d | EHI e |
|---|---|---|---|---|---|---|---|---|
| Stroke1 | R | R | M | 68 | 19 | 56 | 28 | 90 |
| Stroke2 | R | R | F | 86 | 44 | 58 | 30 | 100 |
| Stroke3 | R | R | M | 73 | 13 | 42 | 27 | 70 |
| Stroke4 | R | R | M | 73 | 14 | 44 | 30 | 100 |
| Stroke5 | R | L | M | 63 | 26 | 59 | 29 | 100 |
| Stroke6 | R | L | M | 69 | 12 | 51 | 30 | 100 |
| Stroke7 | R | L | M | 63 | 44 | 35 | 26 | 70 |
| Stroke8 | R | R | M | 76 | 3 | 33 | 25 | 100 |
| Stroke9 | R | L | M | 59 | 78 | 43 | 28 | 80 |
| Stroke10 | R | L | F | 34 | 13 | 54 | 30 | 100 |
| Stroke11 | R | R | F | 54 | 28 | 63 | 30 | 100 |
| Stroke12 | R | R | F | 61 | 49 | 56 | 30 | 100 |
| Stroke13 | R | R | M | 61 | 29 | 55 | 30 | 100 |
| Stroke14 | R | L | M | 52 | 10 | 66 | 30 | 100 |
| Stroke15 | R | R | M | 65 | 21 | 44 | 30 | 100 |
| Task | Movement Type | Example Movements |
|---|---|---|
| ROM | ||
| UNI a | Shoulder flexion/extension, external/internal rotation, abduction/adduction | |
| Elbow and wrist flexion/extension | ||
| Forearm supination/pronation | ||
| Scaption, reaching forward, Ggrasping | ||
| ADL | ||
| UNI | Open the door, turn on the light, brush one’s hair | |
| BIA b | Put in envelope, fold a towel, open the laptop | |
| BIS c | Lift the box up, wash one’s face, type on a keyboard | |
| Task | Mean | STD a | Min b | Median | Max c |
|---|---|---|---|---|---|
| ROM | 1016 | 492 | 240 | 912 | 3715 |
| ADL | 4229 | 3072 | 262 | 3415 | 25,401 |
| Task | UNI a | BIA b | BIS c |
|---|---|---|---|
| ROM | 4.71 ± 0.80 d | – | – |
| ADL | 2.88 ± 0.92 | 0.51 ± 0.30 | 0.22 ± 0.09 |
| Task | Training Groups | |||
|---|---|---|---|---|
| ND (Split a) | Stroke (LOSO-CV b) | ND + Stroke (LOSO-CV) | ||
| ROM | ||||
| Original data | 0.553 ± 0.238 c | 0.676 ± 0.105 | 0.721 ± 0.168 | |
| Augmented data | 0.627 ± 0.176 | 0.709 ± 0.102 | 0.747 ± 0.126 | |
| ADL | ||||
| Original data | 0.454 ± 0.162 | 0.526 ± 0.123 | 0.603 ± 0.137 | |
| Augmented data | 0.512 ± 0.123 | 0.631 ± 0.096 | 0.681 ± 0.119 | |
| Task | Evaluation Groups | |||
|---|---|---|---|---|
| ND | Stroke | |||
| (mean ± std) | (min/max) a | (mean ± std) | (min/max) | |
| ROM | 0.913 ± 0.076 | 0.575 (ND32)/0.980 (ND8) | 0.721 ± 0.168 | 0.465 (Stroke8)/ 0.939 (Stroke12) |
| ADL | 0.929 ± 0.042 | 0.829 (ND4)/ 0.980 (ND22) | 0.603 ± 0.137 | 0.359 (Stroke9)/ 0.817 (Stroke12) |
| Movement Types | Evaluation Groups | |
|---|---|---|
| ND | Stroke | |
| UNI | 0.918 ± 0.151 a | 0.581 ± 0.342 |
| BIA | 0.936 ± 0.134 | 0.541 ± 0.336 |
| BIS | 0.938 ± 0.167 | 0.757 ± 0.266 |
| Task | True a | Inference b | Proportion c |
|---|---|---|---|
| ROM | |||
| FrontWrstExt (UNI) | WrstExt (UNI) | 0.33 | |
| Scaption90 (UNI) | ShAbd90 (UNI) | 0.29 | |
| SupPro (UNI) | FrontSupPro (UNI) | 0.24 | |
| ShRot (UNI) | ShHorAdd (UNI) | 0.22 | |
| ShHorAdd (UNI) | ShRot (UNI) | 0.20 | |
| FrontWrstFlex (UNI) | WrstFlex (UNI) | 0.19 | |
| ShFlex90 (UNI) | ShAbd90 (UNI) | 0.18 | |
| ShFlex90 (UNI) | Scaption90 (UNI) | 0.17 | |
| FrontSupPro (UNI) | SupPro (UNI) | 0.15 | |
| ADL | |||
| UseRemote (UNI) | Scissors (BIA) | 0.32 | |
| Eraser (BIA) | Knife (BIA) | 0.31 | |
| RinseBody (UNI) | WashBody (BIA) | 0.27 | |
| PressPIN (UNI) | LiftDoorlock (UNI) | 0.25 | |
| TurnOnLight (UNI) | LiftDoorlock (UNI) | 0.20 | |
| OpenNewspaper (BIA) | WearSocks (BIS) | 0.20 | |
| FoldTowel (BIA) | WearSocks (BIS) | 0.20 | |
| TurnOnLight (UNI) | PressPIN (UNI) | 0.20 | |
| WringDishcloth (BIA) | WashHand (BIS) | 0.19 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, Y.; Choi, S.-A.; Shin, Y.; Jeong, Y.; Lim, J.; Kim, S. Investigating Activity Recognition for Hemiparetic Stroke Patients Using Wearable Sensors: A Deep Learning Approach with Data Augmentation. Sensors 2024, 24, 210. https://doi.org/10.3390/s24010210
Oh Y, Choi S-A, Shin Y, Jeong Y, Lim J, Kim S. Investigating Activity Recognition for Hemiparetic Stroke Patients Using Wearable Sensors: A Deep Learning Approach with Data Augmentation. Sensors. 2024; 24(1):210. https://doi.org/10.3390/s24010210
Chicago/Turabian StyleOh, Youngmin, Sol-A Choi, Yumi Shin, Yeonwoo Jeong, Jongkuk Lim, and Sujin Kim. 2024. "Investigating Activity Recognition for Hemiparetic Stroke Patients Using Wearable Sensors: A Deep Learning Approach with Data Augmentation" Sensors 24, no. 1: 210. https://doi.org/10.3390/s24010210
APA StyleOh, Y., Choi, S.-A., Shin, Y., Jeong, Y., Lim, J., & Kim, S. (2024). Investigating Activity Recognition for Hemiparetic Stroke Patients Using Wearable Sensors: A Deep Learning Approach with Data Augmentation. Sensors, 24(1), 210. https://doi.org/10.3390/s24010210