
Mobile App Interventions for Parkinson’s Disease, Multiple Sclerosis and Stroke: A Systematic Literature Review


 , , ,
, , , 
 ,
,  , ,
, ,  , , ,
, , ,  , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Study Selection
2.3. Study Quality Assessment and Synthesis
3. Results
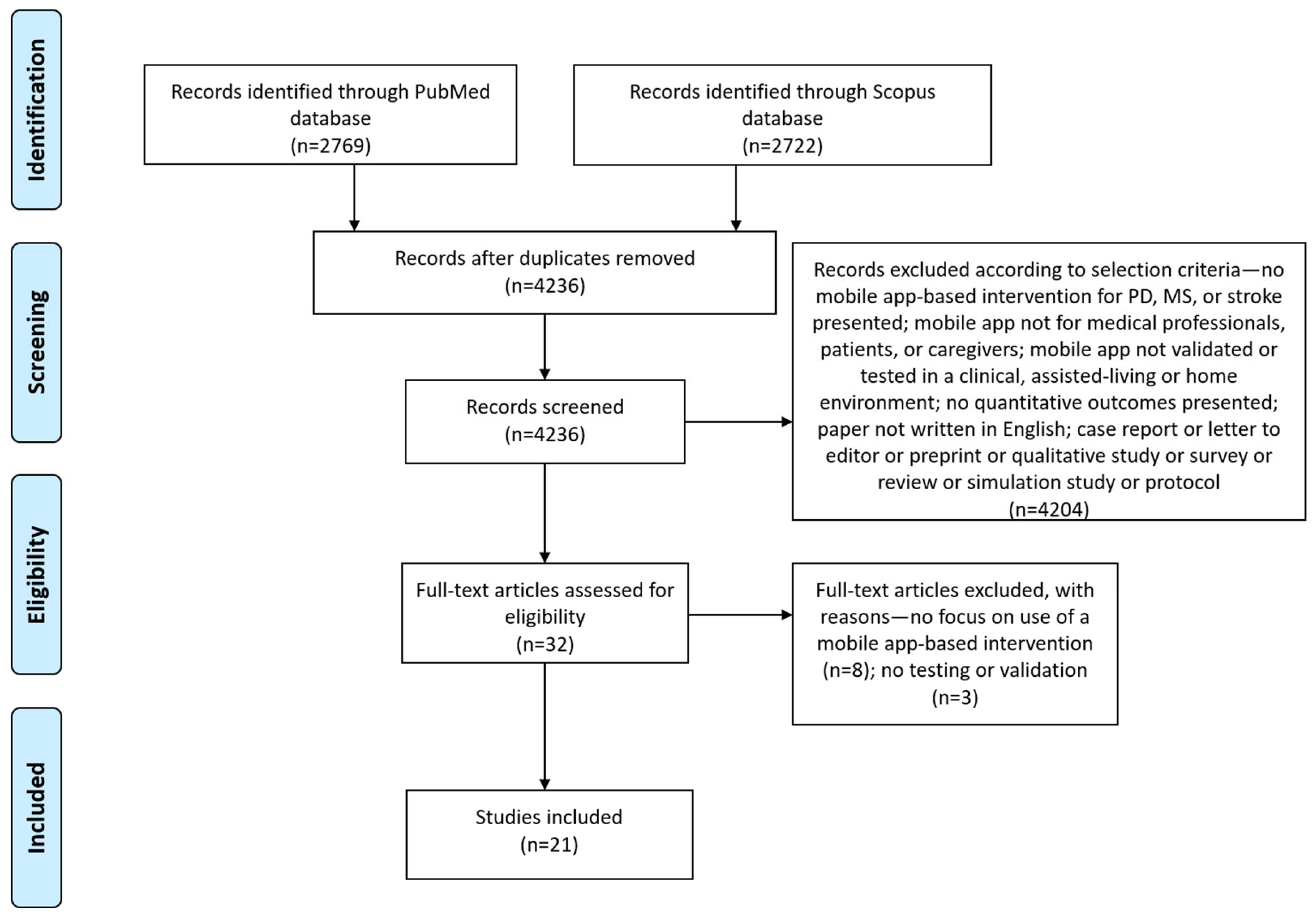
3.1. Screening Results
3.2. Study Quality Assessment
3.3. Mobile app Characteristics
3.4. Study Characteristics
3.5. Study Outcomes
3.6. Mobile App Interventions for CNSDs
3.6.1. Parkinson’s Disease
3.6.2. Multiple Sclerosis
3.6.3. Stroke
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Marras, C.; Beck, J.C.; Bower, J.H.; Roberts, E.; Ritz, B.; Ross, G.W.; Abbott, R.D.; Savica, R.; Van Den Eeden, S.K.; Willis, A.W.; et al. Prevalence of Parkinson’s Disease across North America. NPJ Park. Dis. 2018, 4, 21. [Google Scholar] [CrossRef] [PubMed]
- Gilmour, H.; Ramage-Morin, P.L.; Wong, S.L. Multiple Sclerosis: Prevalence and Impact. Health Rep. 2018, 29, 3–8. [Google Scholar] [PubMed]
- The GBD 2016 Lifetime Risk of Stroke Collaborators; Feigin, V.L.; Nguyen, G.; Cercy, K.; Johnson, C.O.; Alam, T.; Parmar, P.G.; Abajobir, A.A.; Abate, K.H.; Abd-Allah, F.; et al. Global, Regional, and Country-Specific Lifetime Risks of Stroke, 1990 and 2016. N. Engl. J. Med. 2018, 379, 2429–2437. [Google Scholar] [CrossRef] [PubMed]
- Ou, Z.; Pan, J.; Tang, S.; Duan, D.; Yu, D.; Nong, H.; Wang, Z. Global Trends in the Incidence, Prevalence, and Years Lived With Disability of Parkinson’s Disease in 204 Countries/Territories From 1990 to 2019. Front. Public Health 2021, 9, 1994. [Google Scholar] [CrossRef] [PubMed]
- Thayabaranathan, T.; Kim, J.; Cadilhac, D.A.; Thrift, A.G.; Donnan, G.A.; Howard, G.; Howard, V.J.; Rothwell, P.M.; Feigin, V.; Norrving, B.; et al. Global Stroke Statistics 2022. Int. J. Stroke 2022, 17, 946–956. [Google Scholar] [CrossRef]
- Stenager, E. A Global Perspective on the Burden of Multiple Sclerosis. Lancet Neurol. 2019, 18, 227–228. [Google Scholar] [CrossRef]
- Armstrong, M.J.; Okun, M.S. Diagnosis and Treatment of Parkinson Disease: A Review. JAMA—J. Am. Med. Assoc. 2020, 323, 548–560. [Google Scholar] [CrossRef]
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and Treatment of Multiple Sclerosis: A Review. JAMA—J. Am. Med. Assoc. 2021, 325, 765–779. [Google Scholar] [CrossRef]
- Feigin, V.L.; Brainin, M.; Norrving, B.; Martins, S.; Sacco, R.L.; Hacke, W.; Fisher, M.; Pandian, J.; Lindsay, P. World Stroke Organization (WSO): Global Stroke Fact Sheet 2022. Int. J. Stroke 2022, 17, 18–29. [Google Scholar] [CrossRef]
- Gorelick, P.B. The Global Burden of Stroke: Persistent and Disabling. Lancet Neurol. 2019, 18, 417–418. [Google Scholar] [CrossRef]
- Zhao, N.; Yang, Y.; Zhang, L.; Zhang, Q.; Balbuena, L.; Ungvari, G.S.; Zang, Y.; Xiang, Y. Quality of Life in Parkinson’s Disease: A Systematic Review and Meta-analysis of Comparative Studies. CNS Neurosci. Ther. 2021, 27, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Wills, O.C.; Probst, Y.C. Understanding Lifestyle Self-Management Regimens That Improve the Life Quality of People Living with Multiple Sclerosis: A Systematic Review and Meta-Analysis. Health Qual. Life Outcomes 2022, 20, 153. [Google Scholar] [CrossRef] [PubMed]
- González-Santos, J.; Rodríguez-Fernández, P.; Pardo-Hernández, R.; González-Bernal, J.J.; Fernández-Solana, J.; Santamaría-Peláez, M. A Cross-Sectional Study: Determining Factors of Functional Independence and Quality of Life of Patients One Month after Having Suffered a Stroke. Int. J. Environ. Res. Public Health 2023, 20, 995. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Lai, B.; Mehta, T.; Thirumalai, M.; Padalabalanarayanan, S.; Rimmer, J.H.; Motl, R.W. Exercise Training Guidelines for Multiple Sclerosis, Stroke, and Parkinson Disease: Rapid Review and Synthesis. Am. J. Phys. Med. Rehabil. 2019, 98, 613–621. [Google Scholar] [CrossRef]
- Elbers, R.G.; Rietberg, M.B.; Van Wegen, E.E.H.; Verhoef, J.; Kramer, S.F.; Terwee, C.B.; Kwakkel, G. Self-Report Fatigue Questionnaires in Multiple Sclerosis, Parkinson’s Disease and Stroke: A Systematic Review of Measurement Properties. Qual. Life Res. 2012, 21, 925–944. [Google Scholar] [CrossRef]
- Castellano-Aguilera, A.; Biviá-Roig, G.; Cuenca-Martínez, F.; Suso-Martí, L.; Calatayud, J.; Blanco-Díaz, M.; Casaña, J. Effectiveness of Virtual Reality on Balance and Risk of Falls in People with Multiple Sclerosis: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 14192. [Google Scholar] [CrossRef]
- Spanakis, M.; Xylouri, I.; Patelarou, E.; Patelarou, A. A Literature Review of High-Tech Physiotherapy Interventions in the Elderly with Neurological Disorders. Int. J. Environ. Res. Public Health 2022, 19, 9233. [Google Scholar] [CrossRef]
- da Fonseca, M.H.; Kovaleski, F.; Picinin, C.T.; Pedroso, B.; Rubbo, P. E-Health Practices and Technologies: A Systematic Review from 2014 to 2019. Healthcare 2021, 9, 1192. [Google Scholar] [CrossRef]
- Zasadzka, E.; Trzmiel, T.; Pieczyńska, A.; Hojan, K. Modern Technologies in the Rehabilitation of Patients with Multiple Sclerosis and Their Potential Application in Times of COVID-19. Medicina 2021, 57, 549. [Google Scholar] [CrossRef]
- Deb, R.; An, S.; Bhat, G.; Shill, H.; Ogras, U.Y. A Systematic Survey of Research Trends in Technology Usage for Parkinson’s Disease. Sensors 2022, 22, 5491. [Google Scholar] [CrossRef]
- Linares-del Rey, M.; Vela-Desojo, L.; Cano-de la Cuerda, R. Mobile Phone Applications in Parkinson’s Disease: A Systematic Review. Neurologia 2019, 34, 38–54. [Google Scholar] [CrossRef] [PubMed]
- Salimzadeh, Z.; Damanabi, S.; Kalankesh, L.R.; Ferdousi, R. Mobile Applications for Multiple Sclerosis: A Focus on Self-Management. Acta Inform. Med. 2019, 27, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Salgueiro, C.; Urrùtia, G.; Cabanas-Valdés, R. Available Apps for Stroke Telerehabilitation during Corona Virus Disease 2019 Confinement in Spain. Disabil. Rehabil. Assist. Technol. 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Adlakha, S.; Chhabra, D.; Shukla, P. Effectiveness of Gamification for the Rehabilitation of Neurodegenerative Disorders. Chaos Solitons Fractals 2020, 140, 110192. [Google Scholar] [CrossRef]
- Tăuţan, A.M.; Ionescu, B.; Santarnecchi, E. Artificial Intelligence in Neurodegenerative Diseases: A Review of Available Tools with a Focus on Machine Learning Techniques. Artif. Intell. Med. 2021, 117, 102081. [Google Scholar] [CrossRef]
- Triantafyllidis, A.K.; Velardo, C.; Salvi, D.; Shah, S.A.; Koutkias, V.G.; Tarassenko, L. A Survey of Mobile Phone Sensing, Self-Reporting and Social Sharing for Pervasive Healthcare. IEEE J. Biomed. Health Inform. 2017, 21, 218–227. [Google Scholar] [CrossRef]
- Langer, A.; Gassner, L.; Flotz, A.; Hasenauer, S.; Gruber, J.; Wizany, L.; Pokan, R.; Maetzler, W.; Zach, H. How COVID-19 Will Boost Remote Exercise-Based Treatment in Parkinson’s Disease: A Narrative Review. NPJ Park. Dis. 2021, 7, 1–9. [Google Scholar] [CrossRef]
- Chikersal, P.; Venkatesh, S.; Masown, K.; Walker, E.; Quraishi, D.; Dey, A.; Goel, M.; Xia, Z. Predicting Multiple Sclerosis Outcomes During the COVID-19 Stay-at-Home Period: Observational Study Using Passively Sensed Behaviors and Digital Phenotyping. JMIR Ment. Health 2022, 9, e38495. [Google Scholar] [CrossRef]
- Kondylakis, H.; Katehakis, D.G.; Kouroubali, A.; Logothetidis, F.; Triantafyllidis, A.; Kalamaras, I.; Votis, K.; Tzovaras, D. COVID-19 Mobile Apps: A Systematic Review of the Literature. J. Med. Internet Res. 2020, 22, e23170. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of Study Quality for Systematic Reviews: A Comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological Research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264. [Google Scholar] [CrossRef] [PubMed]
- Ellis, T.D.; Cavanaugh, J.T.; DeAngelis, T.; Hendron, K.; Thomas, C.A.; Saint-Hilaire, M.; Pencina, K.; Latham, N.K. Comparative Effectiveness of MHealth-Supported Exercise Compared With Exercise Alone for People With Parkinson Disease: Randomized Controlled Pilot Study. Phys. Ther. 2019, 99, 203–216. [Google Scholar] [CrossRef] [PubMed]
- Ginis, P.; Nieuwboer, A.; Dorfman, M.; Ferrari, A.; Gazit, E.; Canning, C.G.; Rocchi, L.; Chiari, L.; Hausdorff, J.M.; Mirelman, A. Feasibility and Effects of Home-Based Smartphone-Delivered Automated Feedback Training for Gait in People with Parkinson’s Disease: A Pilot Randomized Controlled Trial. Park. Relat. Disord. 2016, 22, 28–34. [Google Scholar] [CrossRef]
- Landers, M.R.; Ellis, T.D. A Mobile App Specifically Designed to Facilitate Exercise in Parkinson Disease: Single-Cohort Pilot Study on Feasibility, Safety, and Signal of Efficacy. JMIR mHealth uHealth 2020, 8, e18985. [Google Scholar] [CrossRef] [PubMed]
- Golan, D.; Sagiv, S.; Glass-Marmor, L.; Miller, A. Mobile Phone-Based e-Diary for Assessment and Enhancement of Medications Adherence among Patients with Multiple Sclerosis. Mult. Scler. J.—Exp. Transl. Clin. 2020, 6, 2055217320939309. [Google Scholar] [CrossRef]
- Nasseri, N.N.; Ghezelbash, E.; Zhai, Y.; Patra, S.; Riemann-Lorenz, K.; Heesen, C.; Rahn, A.C.; Stellmann, J.-P. Feasibility of a Smartphone App to Enhance Physical Activity in Progressive MS: A Pilot Randomized Controlled Pilot Trial over Three Months. PeerJ 2020, 8, e9303. [Google Scholar] [CrossRef]
- Pedullà, L.; Brichetto, G.; Tacchino, A.; Vassallo, C.; Zaratin, P.; Battaglia, M.A.; Bonzano, L.; Bove, M. Adaptive vs. Non-Adaptive Cognitive Training by Means of a Personalized App: A Randomized Trial in People with Multiple Sclerosis. J. Neuroeng. Rehabil. 2016, 13, 88. [Google Scholar] [CrossRef]
- Van Geel, F.; Geurts, E.; Abasıyanık, Z.; Coninx, K.; Feys, P. Feasibility Study of a 10-Week Community-Based Program Using the WalkWithMe Application on Physical Activity, Walking, Fatigue and Cognition in Persons with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2020, 42, 102067. [Google Scholar] [CrossRef]
- Burgos, P.I.; Lara, O.; Lavado, A.; Rojas-Sepúlveda, I.; Delgado, C.; Bravo, E.; Kamisato, C.; Torres, J.; Castañeda, V.; Cerda, M. Exergames and Telerehabilitation on Smartphones to Improve Balance in Stroke Patients. Brain Sci. 2020, 10, 773. [Google Scholar] [CrossRef]
- Chae, S.H.; Kim, Y.; Lee, K.-S.; Park, H.-S. Development and Clinical Evaluation of a Web-Based Upper Limb Home Rehabilitation System Using a Smartwatch and Machine Learning Model for Chronic Stroke Survivors: Prospective Comparative Study. JMIR mHealth uHealth 2020, 8, e17216. [Google Scholar] [CrossRef]
- Choi, Y.-H.; Ku, J.; Lim, H.; Kim, Y.H.; Paik, N.-J. Mobile Game-Based Virtual Reality Rehabilitation Program for Upper Limb Dysfunction after Ischemic Stroke. Restor. Neurol. Neurosci. 2016, 34, 455–463. [Google Scholar] [CrossRef]
- Chung, B.P.H.; Chiang, W.K.H.; Lau, H.; Lau, T.F.O.; Lai, C.W.K.; Sit, C.S.Y.; Chan, K.Y.; Yeung, C.Y.; Lo, T.M.; Hui, E.; et al. Pilot study on comparisons between the effectiveness of mobile video-guided and paper-based home exercise programs on improving exercise adherence, self-efficacy for exercise and functional outcomes of patients with stroke with 3-month follow-up: A single-blind randomized controlled trial. Hong Kong Physiother. J. 2020, 40, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Grau-Pellicer, M.; Lalanza, J.F.; Jovell-Fernández, E.; Capdevila, L. Impact of MHealth Technology on Adherence to Healthy PA after Stroke: A Randomized Study. Top. Stroke Rehabil. 2020, 27, 354–368. [Google Scholar] [CrossRef]
- Ifejika, N.L.; Bhadane, M.; Cai, C.C.; Noser, E.A.; Grotta, J.C.; Savitz, S.I. Use of a Smartphone-Based Mobile App for Weight Management in Obese Minority Stroke Survivors: Pilot Randomized Controlled Trial with Open Blinded End Point. JMIR mHealth uHealth 2020, 8, e17816. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.-N.; Shen, H.-N.; Lin, C.-Y.; Elwyn, G.; Huang, S.-C.; Wu, T.-F.; Hou, W.-H. Does a Mobile App Improve Patients’ Knowledge of Stroke Risk Factors and Health-Related Quality of Life in Patients with Stroke? A Randomized Controlled Trial. BMC Med. Inform. Decis. Mak. 2019, 19, 282–289. [Google Scholar] [CrossRef]
- Langan, J.; Bhattacharjya, S.; Subryan, H.; Xu, W.; Chen, B.; Li, Z.; Cavuoto, L. In-Home Rehabilitation Using a Smartphone App Coupled With 3D Printed Functional Objects: Single-Subject Design Study. JMIR mHealth uHealth 2020, 8, e19582. [Google Scholar] [CrossRef]
- Paul, L.; Wyke, S.; Brewster, S.; Sattar, N.; Gill, J.M.R.; Alexander, G.; Rafferty, D.; McFadyen, A.K.; Ramsay, A.; Dybus, A. Increasing Physical Activity in Stroke Survivors Using STARFISH, an Interactive Mobile Phone Application: A Pilot Study. Top. Stroke Rehabil. 2016, 23, 170–177. [Google Scholar] [CrossRef]
- Requena, M.; Montiel, E.; Baladas, M.; Muchada, M.; Boned, S.; López, R.; Rodríguez-Villatoro, N.; Juega, J.; García-Tornel, Á.; Rodríguez-Luna, D.; et al. Farmalarm: Application for Mobile Devices Improves Risk Factor Control after Stroke. Stroke 2019, 50, 1819–1824. [Google Scholar] [CrossRef] [PubMed]
- Sarfo, F.S.; Adusei, N.; Ampofo, M.; Kpeme, F.K.; Ovbiagele, B. Pilot Trial of a Tele-Rehab Intervention to Improve Outcomes after Stroke in Ghana: A Feasibility and User Satisfaction Study. J. Neurol. Sci. 2018, 387, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Sawant, N.; Bose, M.; Parab, S. Dexteria App. Therapy versus Conventional Hand Therapy in Stroke. J. Enabling Technol. 2020, 14, 221–231. [Google Scholar] [CrossRef]
- Verna, V.; De Bartolo, D.; Iosa, M.; Fadda, L.; Pinto, G.; Caltagirone, C.; De Angelis, S.; Tramontano, M. Te.M.P.O., an App for Using Temporal Musical Mismatch in Post-Stroke Neurorehabilitation: A Preliminary Randomized Controlled Study. NeuroRehabilitation 2020, 47, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Qian, X.; Yuan, M.; Wang, C. Effects of Mobile Phone App-Based Continuing Nursing Care on Self-Efficacy, Quality of Life, and Motor Function of Stroke Patients in the Community. Acta Neurol. Belg. 2021, 123, 107–114. [Google Scholar] [CrossRef]
- Avan, A.; Hachinski, V. Stroke and Dementia, Leading Causes of Neurological Disability and Death, Potential for Prevention. Alzheimer’s Dement. 2021, 17, 1072–1076. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Nichols, E.; Alam, T.; Bannick, M.S.; Beghi, E.; Blake, N.; Culpepper, W.J.; Dorsey, E.R.; Elbaz, A.; Ellenbogen, R.G.; et al. Global, Regional, and National Burden of Neurological Disorders, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef]
- Brooks, S.K.; Weston, D.; Greenberg, N. Social and Psychological Impact of the COVID-19 Pandemic on People with Parkinson’s Disease: A Scoping Review. Public Health 2021, 199, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Freiman, J.A.; Chalmers, T.C.; Smith, H.A.; Kuebler, R.R. The Importance of Beta, the Type II Error, and Sample Size in the Design and Interpretation of the Randomized Controlled Trial. In Medical Uses of Statistics; CRC Press: Boca Raton, FL, USA, 2019; pp. 357–389. [Google Scholar]
- Toerien, M.; Brookes, S.T.; Metcalfe, C.; de Salis, I.; Tomlin, Z.; Peters, T.J.; Sterne, J.; Donovan, J.L. A Review of Reporting of Participant Recruitment and Retention in RCTs in Six Major Journals. Trials 2009, 10, 52. [Google Scholar] [CrossRef]
- Crotty, G.F.; Schwarzschild, M.A. Chasing Protection in Parkinson’s Disease: Does Exercise Reduce Risk and Progression? Front. Aging Neurosci. 2020, 12, 186. [Google Scholar] [CrossRef]
- Timmers, T.; Janssen, L.; Kool, R.B.; Kremer, J.A.M. Educating Patients by Providing Timely Information Using Smartphone and Tablet Apps: Systematic Review. J. Med. Internet Res. 2020, 22, e17342. [Google Scholar] [CrossRef]
- Payne, H.E.; Lister, C.; West, J.H.; Bernhardt, J.M. Behavioral Functionality of Mobile Apps in Health Interventions: A Systematic Review of the Literature. JMIR mHealth uHealth 2015, 3, e3335. [Google Scholar] [CrossRef]
- Omberg, L.; Chaibub Neto, E.; Perumal, T.M.; Pratap, A.; Tediarjo, A.; Adams, J.; Bloem, B.R.; Bot, B.M.; Elson, M.; Goldman, S.M.; et al. Remote Smartphone Monitoring of Parkinson’s Disease and Individual Response to Therapy. Nat. Biotechnol. 2022, 40, 480–487. [Google Scholar] [CrossRef]
- Fröhlich, H.; Bontridder, N.; Petrovska-Delacréta, D.; Glaab, E.; Kluge, F.; El Yacoubi, M.; Marín Valero, M.; Corvol, J.-C.; Eskofier, B.; Van Gyseghem, J.-M.; et al. Leveraging the Potential of Digital Technology for Better Individualized Treatment of Parkinson’s Disease. Front. Neurol. 2022, 13, 788427. [Google Scholar] [CrossRef] [PubMed]
- Triantafyllidis, A.; Kondylakis, H.; Votis, K.; Tzovaras, D.; Maglaveras, N.; Rahimi, K. Features, Outcomes, and Challenges in Mobile Health Interventions for Patients Living with Chronic Diseases: A Review of Systematic Reviews. Int. J. Med. Inform. 2019, 132, 103984. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Freeman, B.; Li, M. Can Mobile Phone Apps Influence People’s Health Behavior Change? An Evidence Review. J. Med. Internet Res. 2016, 18, e5692. [Google Scholar] [CrossRef]
- Nussbaum, R.; Kelly, C.; Quinby, E.; Mac, A.; Parmanto, B.; Dicianno, B.E. Systematic Review of Mobile Health Applications in Rehabilitation. Arch. Phys. Med. Rehabil. 2019, 100, 115–127. [Google Scholar] [CrossRef]
- Szeto, S.G.; Wan, H.; Alavinia, M.; Dukelow, S.; MacNeill, H. Effect of Mobile Application Types on Stroke Rehabilitation: A Systematic Review. J. Neuroeng. Rehabil. 2023, 20, 12. [Google Scholar] [CrossRef]
- Kao, C.K.; Liebovitz, D.M. Consumer Mobile Health Apps: Current State, Barriers, and Future Directions. PM&R 2017, 9, S106–S115. [Google Scholar]
- Noorbergen, T.J.; Adam, M.T.P.; Teubner, T.; Collins, C.E. Using Co-Design in Mobile Health System Development: A Qualitative Study with Experts in Co-Design and Mobile Health System Development. JMIR mHealth uHealth 2021, 9, e27896. [Google Scholar] [CrossRef]
- Harrington, C.N.; Wilcox, L.; Connelly, K.; Rogers, W.; Sanford, J. Designing Health and Fitness Apps with Older Adults: Examining the Value of Experience-Based Co-Design. In Proceedings of the 12th EAI International Conference on Pervasive Computing Technologies for Healthcare, New York, NY, USA, 21–24 May 2018; pp. 15–24. [Google Scholar]
- Sanz, M.F.; Acha, B.V.; García, M.F. Co-Design for People-Centred Care Digital Solutions: A Literature Review. Int. J. Integr. Care 2021, 21, 16. [Google Scholar] [CrossRef]
- Scholz, M.; Haase, R.; Schriefer, D.; Voigt, I.; Ziemssen, T. Electronic Health Interventions in the Case of Multiple Sclerosis: From Theory to Practice. Brain Sci. 2021, 11, 180. [Google Scholar] [CrossRef]
- Wang, S.; Bolling, K.; Mao, W.; Reichstadt, J.; Jeste, D.; Kim, H.-C.; Nebeker, C. Technology to Support Aging in Place: Older Adults’ Perspectives. Healthcare 2019, 7, 60. [Google Scholar] [CrossRef]


{kind=link}
| Authors | SB | SD | CF | BL | DC | WD | GR |
|---|---|---|---|---|---|---|---|
| Ellis et al., 2019 [32] | M | S | M | M | M | S | S |
| Ginis et al., 2016 [33] | W | S | W | W | S | S | W |
| Landers et al., 2020 [34] | W | M | W | M | M | W | W |
| Golan et al., 2020 [35] | S | S | M | M | M | S | S |
| Nasseri et al., 2020 [36] | M | S | M | M | S | S | S |
| Pedullà et al., 2016 [37] | M | S | S | S | S | S | S |
| Van Geel et al., 2020 [38] | M | M | W | M | S | M | M |
| Burgos et al., 2020 [39] | M | S | W | M | S | W | W |
| Chae et al., 2020 [40] | M | M | S | M | M | M | S |
| Choi et al., 2016 [41] | W | S | W | S | S | S | W |
| Chung et al., 2020 [42] | M | S | S | S | W | S | M |
| Grau-Pellicer et al., 2020 [43] | W | S | S | W | S | S | W |
| Ifejika et al., 2020 [44] | M | S | S | S | S | M | S |
| Kang et al., 2019 [45] | M | S | S | M | S | M | S |
| Langan et al., 2020 [46] | W | M | W | M | S | S | W |
| Paul et al., 2016 [47] | M | S | W | W | S | S | W |
| Requena et al., 2019 [48] | W | M | M | M | M | W | W |
| Sarfo et al., 2018 [49] | M | M | W | M | S | S | M |
| Sawant et al., 2020 [50] | W | W | W | M | S | S | W |
| Verna et al., 2020 [51] | M | S | S | M | S | S | S |
| Xu et al., 2021 [52] | W | W | S | M | M | W | W |
| Authors | App Name | Available Commercially | Target Disease(s) | App Type |
|---|---|---|---|---|
| Ellis et al., 2019 [32] | Wellpepper | Yes | Parkinson’s | Exercise/ Physical activity |
| Ginis et al., 2016 [33] | FOG-cue app (Inertial measurement units combined with a smartphone application (CuPiD-system)) | No data | Parkinson’s | Physical rehabilitation |
| Landers et al., 2020 [34] | 9zest Parkinson’s Therapy | Yes | Parkinson’s | Exercise/Physical activity |
| Golan et al., 2020 [35] | MyMS&Me | No data | Multiple Sclerosis | Treatment adherence support |
| Nasseri et al., 2020 [36] | N/A | No data | Multiple Sclerosis | Exercise/Physical activity |
| Pedullà et al., 2016 [37] | COGNI-TRAcK | No data | Multiple Sclerosis | Cognitive training |
| Van Geel et al., 2020 [38] | WalkWithMe | No data | Multiple Sclerosis | Exercise/Physical activity |
| Burgos et al., 2020 [39] | No data | No data | Stroke | Physical rehabilitation |
| Chae et al., 2020 [40] | N/A | No data | Stroke | Physical rehabilitation |
| Choi et al., 2016 [41] | MoU-Rehab | No data | Stroke | Physical rehabilitation |
| Chung et al., 2020 [42] | N/A | No data | Stroke | Exercise/Physical activity |
| Grau-Pellicer et al., 2020 [43] | Fitlab | Yes | Stroke | Exercise/Physical activity |
| Ifejika et al., 2020 [44] | Lose it! | Free mobile app | Stroke | Diet |
| Kang et al., 2019 [45] | SHEMA | No data | Stroke | Health education |
| Langan et al., 2020 [46] | mRehab | No data | Stroke | Physical rehabilitation |
| Paul et al., 2016 [47] | STARFISH | No data | Stroke | Exercise/Physical activity |
| Requena et al., 2019 [48] | Farmalarm | No data | Stroke | Health education/Treatment adherence support |
| Sarfo et al., 2018 [49] | 9zest Stroke Rehab App | Yes | Stroke | Exercise/Physical activity |
| Sawant et al., 2020 [50] | Dexteria | Yes | Stroke | Physical rehabilitation |
| Verna et al., 2020 [51] | Te.M.P.O. | No data | Stroke | Cognitive training |
| Xu et al., 2021 [52] | Rehabilitation Guardian | No data | Stroke | Health education |
| Authors | Intervention | Main Features | Study Design | Study Duration | Study Sample | Outcome Measures | Statistically Significant Outcomes (Yes/No) |
|---|---|---|---|---|---|---|---|
| Ellis et al., 2019 [32] | Exercise program | Remote monitoring, reminders, communication with care team, plan adaptation | RCT | 12 months | 51 patients, mean age 64.1 (9.5) years | Physical activity, health-related quality of life, walking capacity, adherence, safety, acceptability | No—No difference in physical activity between the two groups |
| Ginis et al., 2016 [33] | Gait training and freezing of gait (FOG) detection | Detection of FOG, exercises to improve gait, continuous cueing while walking | RCT | 6 weeks + 4 weeks follow-up | 40 patients (age not reported) | Gait speed under usual and dual-task (DT) conditions. Secondary outcomes: balance and movement scales, quality of life, Parkinson’s global status | Yes—Intervention group improved more in terms of balance and quality of life |
| Landers et al., 2020 [34] | Physical exercise program | Customized exercise program, calibrated to the user’s level of functioning using a proprietary algorithm to select exercises | Prospective, single-cohort study | 12 weeks | 28 participants, mean age 62.1 (9.6) years | Movement measures: 30 s sit-to-stand (STS), timed up and go (TUG); Parkinson’s Disease Questionnaire 8 (PDQ8) | Yes—Improvement in all measures |
| Golan et al., 2020 [35] | E-diary for assessment and enhancement of medication adherence | Medication reminders, self-reports | RCT | 12 months | 117 patients: 62 in intervention, mean age 40.3 (11.4) years; 55 in control, mean age 42.3 (13.9) years | Adherence to physical activity | No—Similar adherence for the intervention and control groups |
| Nasseri et al., 2020 [36] | Promotion of physical activity through texts, images, video | Multimedia content for physical activity promotion, statistics on performed physical activity | RCT | 3 months | 38 patients, mean age 51 years | Physical activity | No—No difference between the two groups was found |
| Pedullà et al., 2016 [37] | Cognitive exercises through mobile app with automatic exercise level adaptation | Working memory-based exercises in mobile app | RCT | 8 weeks | 28 patients, mean age 47.5 (9.3) years | Neuropsychological assessment, adherence | Yes—Improved cognition in the intervention group |
| Van Geel et al., 2020 [38] | Support in physical activity (walking) | Tracking of walking activities, verbal feedback through a virtual coach to reach goals | Cohort study | 7 months | 19 patients, mean age 42.5 years | Physical activity. Secondary outcomes: cognition, fatigue, health related quality of life. | Yes—Improvements in physical activity, cognition and fatigue |
| Burgos et al., 2020 [39] | Improvement of balance of stroke patients | Exergames | RCT | 4 weeks | 10 stroke patients, mean age 61.3 (8.3) years | Berg balance scale, Mini-BESTest, and Barthel scale | Yes—Improvements compared to control group in Berg balance scale and Barthel scale |
| Chae et al., 2020 [40] | Improvement of upper limb function (through a smartphone collecting and providing feedback on exercise data) | Exercise recognition and sharing of exercise data with therapists | Prospective comparative study | 18 weeks | 33 chronic stroke survivors: intervention, mean age 58.3 (9.3) years; control, mean age 64.5 (9.6) years | Wolf Motor function test (WMFT), Fugl–Meyer assessment of upper extremity, grip power test, Beck depression inventory, and range of motion (ROM) assessment | Yes—Improvements of WMFT and ROM compared to control group |
| Choi et al., 2016 [41] | Upper extremity rehabilitation program | Μobile game-based virtual reality rehabilitation program | RCT | 10 sessions of daily therapy, 5 days per week for 2 weeks | 24 patients with ischemic stroke: intervention, mean age 61.0 (15.2) years; control, mean age 72.1 (9.9) years | Fugl–Meyer assessment of the upper extremity (FMA-UE), Brunnstrom stage (B-stage) for the arm and the hand, manual muscle testing (MMT), modified Barthel index, EuroQol-5 dimension, and Beck depression inventory | Yes—Greater improvement in FMA-UE, B-stage, and MMT |
| Chung et al., 2020 [42] | Exercise program | Videos to perform exercise | RCT | 90 days | 56 stroke patients, mean age 69.8 (14.9) years | Exercise adherence | Yes—Improvement of exercise adherence compared to control group |
| Grau-Pellicer et al., 2020 [43] | Improvement of physical activity through feedback and visualization methods | Visualization of results and communication with supervisors | RCT | 8 weeks | 41 chronic stroke survivors: intervention, mean age 62.96 (11.87) years; control, mean age 68.53 (11.53) years | Adherence to physical activity | Yes—Community ambulation increased more, and sitting time was reduced in the intervention group |
| Ifejika et al., 2020 [44] | Weight loss intervention | Recording of meals, compliance notifications, reminder messages | RCT | 6 months | 36 obese African American or Hispanic patients, mean age 54.1 (9.4) years | Reduction in total body weight | No—No significant difference compared to keeping a food journal in paper |
| Kang et al., 2019 [45] | Educational intervention to improve stroke knowledge | Educational content | RCT | 30 days | 76 stroke patients: intervention, mean age 50.47 (10.82) years; control, mean age 52.33 (11.03) years | Stroke knowledge, health-related quality of life | No- No differences compared to control group |
| Langan et al., 2020 [46] | Improvement of upper limb mobility through the conduction of daily living activities | Guidance for practice of activities of daily living | Single-subject experimental study | 6 weeks | 16 participants, 37–78 years old | Changes in clinical assessments | Yes—Improvements in functional performance and hand dexterity |
| Paul et al., 2016 [47] | Support in physical activity (walking) through gamification with individual and group goals and rewards | Gamification, goals and rewards through visual representations | Experimental study | 6 weeks | 23 patients (12 women; age: 56.0 ± 10.0 years, time since stroke: 4.2 ± 4.0 years). 15 intervention/8 control | Physical activity, sedentary time. Secondary outcomes: heart rate, blood pressure, body mass index, fatigue severity scale, instrumental activity of daily living scale, ten-meter walk test, stroke-specific quality of life scale, and psychological general well-being index | Yes—Average daily step count increased in the intervention vs. control group |
| Requena et al., 2019 [48] | Stroke awareness via mobile app for control of vascular risk factors: hypertension, diabetes, cholesterol, smoking | Medication alerts and compliance control, chat communication with medical staff, didactic video, exercise monitoring | 2-arm open-label nonrandomized study | 4 weeks | 159 stroke patients, mean age 58.4 (11.4) years | Under control risk factors | Yes—4 out of 4 risk factors under control was higher in intervention group |
| Sarfo et al., 2018 [49] | Physical exercise program | Standardized rehabilitation program | Single-site, single-arm, observational prospective pilot study | 12 weeks. 5 day-a-week exercise program | 20 stroke survivors, mean age 54.6 (10.2) years | stroke levity scale (SLS), modified Rankin score, Barthel’s index of activities of daily living, national institute of health stroke scale, Montreal cognitive assessment (MoCA), fatigue severity scale, visual analogue scale for pain, feasibility outcomes | Yes—Improvement in SLS, and MoCA scores. Excellent participant satisfaction |
| Sawant et al., 2020 [50] | App-based hand therapy | Hand training: tap, pinch and scribble | Experimental study | 30 days | 39 participants in 3 groups (13 participants per group): (A) conventional hand therapy, mean age 50.2 (8.1) years, (B) app therapy, mean age 52.7 (8.8) years, (C) conventional therapy along with app therapy, mean age 53.6 (6.2) years | Hand function | Yes—All three groups improved on hand function post-treatment. Group C (combined therapy) displayed the largest improvement |
| Verna et al., 2020 [51] | Cognitive exercise using variations of music tone during the listening of a sequence of different music themes | Music listening | RCT | 4 weeks | 30 inpatients, mean age 57.53 (13.33) years. | disability rating scale (DRS), the modified Barthel index (MBI), stroke-specific quality of life scale (SSQoL) | Yes—Significant differences in effectiveness were found in the between-subject analysis of SSQoL and DRS scores |
| Xu et al., 2021 [52] | App-based continuing nursing care to support the self-efficacy, quality of life, and motor function of stroke patients in the community | Patient diary, communication between patient and care team | Experimental study | 3 months | 101 stroke patients: intervention, mean age 68.52 (3.15) years; control, mean age 68.68 (3.18) years | Changes in physiological indicators, motor function, self-efficacy, quality of life, and satisfaction toward nursing | Yes—Improvements in all outcomes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Triantafyllidis, A.; Segkouli, S.; Zygouris, S.; Michailidou, C.; Avgerinakis, K.; Fappa, E.; Vassiliades, S.; Bougea, A.; Papagiannakis, N.; Katakis, I.; et al. Mobile App Interventions for Parkinson’s Disease, Multiple Sclerosis and Stroke: A Systematic Literature Review. Sensors 2023, 23, 3396. https://doi.org/10.3390/s23073396
Triantafyllidis A, Segkouli S, Zygouris S, Michailidou C, Avgerinakis K, Fappa E, Vassiliades S, Bougea A, Papagiannakis N, Katakis I, et al. Mobile App Interventions for Parkinson’s Disease, Multiple Sclerosis and Stroke: A Systematic Literature Review. Sensors. 2023; 23(7):3396. https://doi.org/10.3390/s23073396
Chicago/Turabian StyleTriantafyllidis, Andreas, Sofia Segkouli, Stelios Zygouris, Christina Michailidou, Konstantinos Avgerinakis, Evangelia Fappa, Sophia Vassiliades, Anastasia Bougea, Nikos Papagiannakis, Ioannis Katakis, and et al. 2023. "Mobile App Interventions for Parkinson’s Disease, Multiple Sclerosis and Stroke: A Systematic Literature Review" Sensors 23, no. 7: 3396. https://doi.org/10.3390/s23073396
APA StyleTriantafyllidis, A., Segkouli, S., Zygouris, S., Michailidou, C., Avgerinakis, K., Fappa, E., Vassiliades, S., Bougea, A., Papagiannakis, N., Katakis, I., Mathioudis, E., Sorici, A., Bajenaru, L., Tageo, V., Camonita, F., Magga-Nteve, C., Vrochidis, S., Pedullà, L., Brichetto, G., ... Tzovaras, D. (2023). Mobile App Interventions for Parkinson’s Disease, Multiple Sclerosis and Stroke: A Systematic Literature Review. Sensors, 23(7), 3396. https://doi.org/10.3390/s23073396