

Using a Smartwatch to Record Precordial Electrocardiograms: A Validation Study

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. ECG Recordings
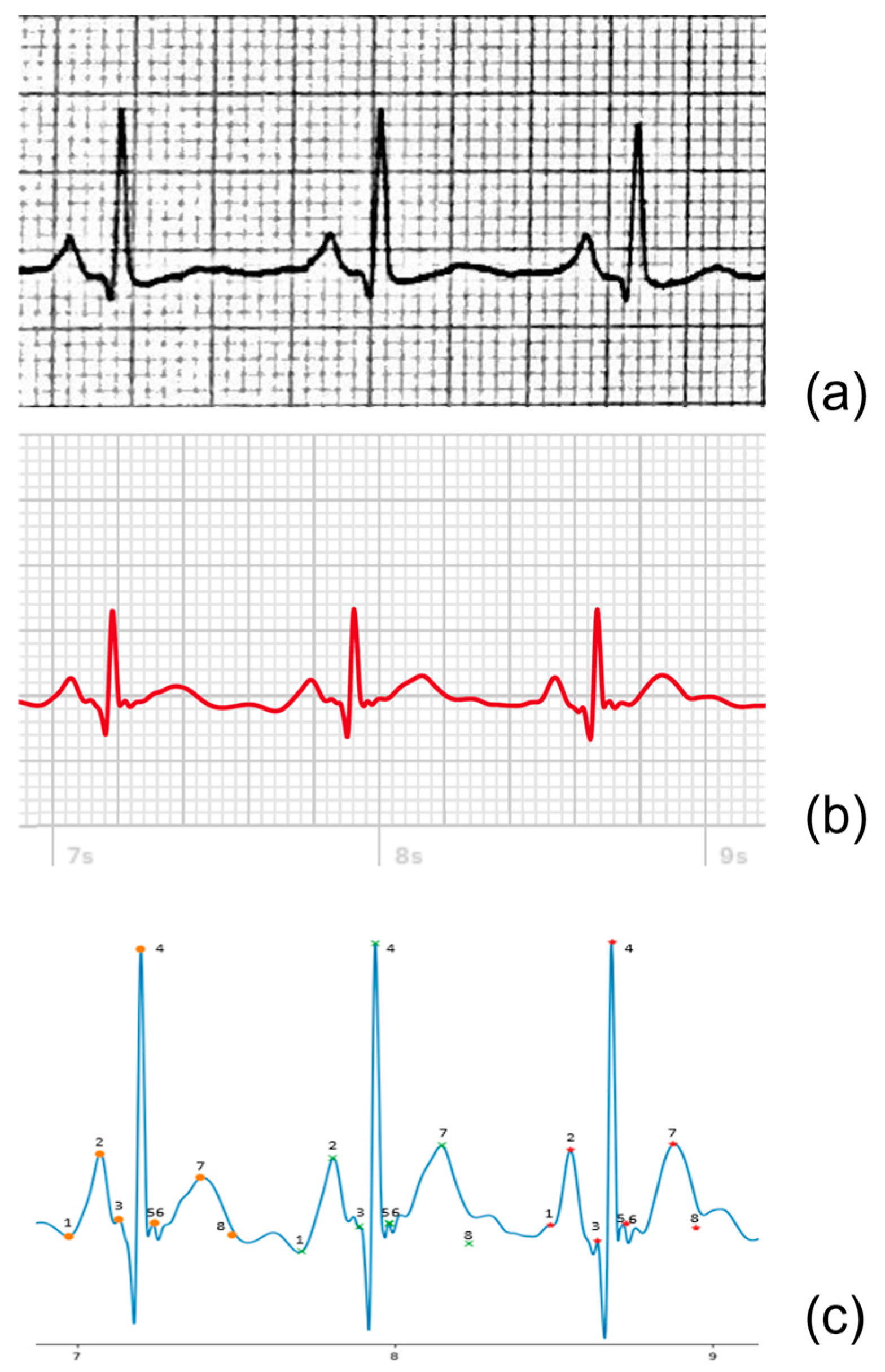
2.3. Data Processing
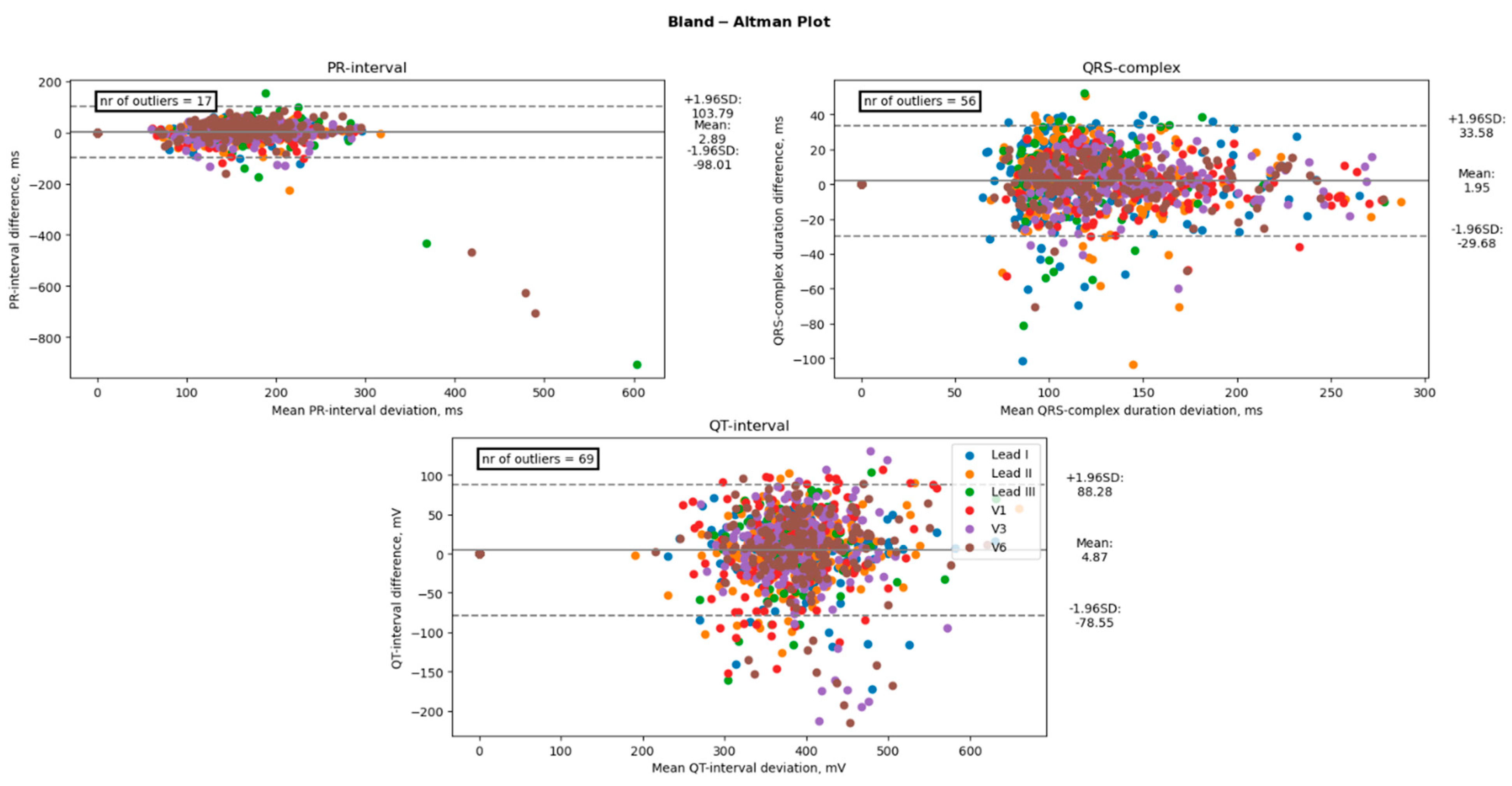
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Amplitude and Duration of ECG-Waves
4. Discussion
4.1. Main Findings
4.2. Previous Studies
4.3. Study Limitations
4.4. Future Clinical Perspective
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Strik, M.; Ploux, S.; Ramirez, F.D.; Abu-Alrub, S.; Jaîs, P.; Haïssaguerre, M.; Bordachar, P. Smartwatch-Based Detection of Cardiac Arrhythmias: Beyond the Differentiation between Sinus Rhythm and Atrial Fibrillation. Heart Rhythm 2021, 18, 1524–1532. [Google Scholar] [CrossRef]
- Manninger, M.; Zweiker, D.; Svennberg, E.; Chatzikyriakou, S.; Pavlovic, N.; Zaman, J.A.B.; Kircanski, B.; Lenarczyk, R.; Vanduynhoven, P.; Kosiuk, J.; et al. Current Perspectives on Wearable Rhythm Recordings for Clinical Decision-Making: The WEHRAbles 2 Survey. EP Eur. 2021, 23, 1106–1113. [Google Scholar] [CrossRef] [PubMed]
- Isakadze, N.; Martin, S.S. How Useful Is the Smartwatch ECG? Trends Cardiovasc. Med. 2020, 30, 442–448. [Google Scholar] [CrossRef]
- Boriani, G.; Schnabel, R.B.; Healey, J.S.; Lopes, R.D.; Verbiest-van Gurp, N.; Lobban, T.; Camm, J.A.; Freedman, B. Consumer-Led Screening for Atrial Fibrillation Using Consumer-Facing Wearables, Devices and Apps: A Survey of Health Care Professionals by AF-SCREEN International Collaboration. Eur. J. Intern. Med. 2020, 82, 97–104. [Google Scholar] [CrossRef]
- Ploux, S.; Strik, M.; Caillol, T.; Ramirez, F.D.; Abu-Alrub, S.; Marchand, H.; Buliard, S.; Haïssaguerre, M.; Bordachar, P. Beyond the Wrist: Using a Smartwatch Electrocardiogram to Detect Electrocardiographic Abnormalities. Arch. Cardiovasc. Dis. 2022, 115, 29–36. [Google Scholar] [CrossRef]
- Spaccarotella, C.A.M.; Migliarino, S.; Mongiardo, A.; Sabatino, J.; Santarpia, G.; De Rosa, S.; Curcio, A.; Indolfi, C. Measurement of the QT Interval Using the Apple Watch. Sci. Rep. 2021, 11, 10817. [Google Scholar] [CrossRef] [PubMed]
- Racine, H.P.; Strik, M.; van der Zande, J.; Alrub, S.A.; Caillol, T.; Haïssaguerre, M.; Ploux, S.; Bordachar, P. Role of Coexisting ECG Anomalies in the Accuracy of Smartwatch ECG Detection of Atrial Fibrillation. Can. J. Cardiol. 2022, 38, 1709–1712. [Google Scholar] [CrossRef]
- Abu-Alrub, S.; Strik, M.; Ramirez, F.D.; Moussaoui, N.; Racine, H.P.; Marchand, H.; Buliard, S.; Haïssaguerre, M.; Ploux, S.; Bordachar, P. Smartwatch Electrocardiograms for Automated and Manual Diagnosis of Atrial Fibrillation: A Comparative Analysis of Three Models. Front. Cardiovasc. Med. 2022, 9, 67. [Google Scholar] [CrossRef] [PubMed]
- Bansal, A.; Joshi, R. Portable Out-of-Hospital Electrocardiography: A Review of Current Technologies. J. Arrhythmia 2018, 34, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Avila, C.O. Novel Use of Apple Watch 4 to Obtain 3-Lead Electrocardiogram and Detect Cardiac Ischemia. Perm. J. 2019, 23. [Google Scholar] [CrossRef] [PubMed]
- Strik, M.; Ploux, S.; Weigel, D.; van der Zande, J.; Velraeds, A.; Racine, H.-P.; Ramirez, F.D.; Haïssaguerre, M.; Bordachar, P. The Use of Smartwatch Electrocardiogram beyond Arrhythmia Detection. Trends Cardiovasc. Med. 2023. [Google Scholar] [CrossRef]
- Leroux, J.; Strik, M.; Ramirez, F.D.; Racine, H.P.; Ploux, S.; Sacristan, B.; Chabaneix-Thomas, J.; Jalal, Z.; Thambo, J.B.; Bordachar, P. Feasibility and Diagnostic Value of Recording Smartwatch Electrocardiograms in Neonates and Children. J. Pediatr. 2022. [Google Scholar] [CrossRef] [PubMed]
- Behzadi, A.; Shamloo, A.S.; Mouratis, K.; Hindricks, G.; Arya, A.; Bollmann, A. Feasibility and Reliability of SmartWatch to Obtain 3-Lead Electrocardiogram Recordings. Sensors 2020, 20, 5074. [Google Scholar] [CrossRef]
- Nasarre, M.; Strik, M.; Ramirez, F.D.; Buliard, S.; Marchand, H.; Abu-Alrub, S.; Ploux, S.; Haïssaguerre, M.; Bordachar, P. Using a Smartwatch Electrocardiogram to Detect Abnormalities Associated with Sudden Cardiac Arrest in Young Adults. EP Eur. 2022, 24, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Carmen, A.M.; Alberto, P.; Serena, M.; Elisa, P.; Antonio, C.; Annalisa, M.; Sabato, S.; Salvatore, D.R.; Ciro, I. Multichannel Electrocardiograms Obtained by a Smartwatch for the Diagnosis of ST-Segment Changes. JAMA Cardiol. 2020, 5, 1176–1180. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding Bland Altman Analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Gil, M.Á.C. Standard and Precordial Leads Obtained with an Apple Watch. Ann. Intern. Med. 2020, 172, 436–437. [Google Scholar] [CrossRef]
- Kobel, M.; Kalden, P.; Michaelis, A.; Markel, F.; Mensch, S.; Weidenbach, M.; Riede, F.T.; Löffelbein, F.; Bollmann, A.; Shamloo, A.S.; et al. Accuracy of the Apple Watch IECG in Children With and Without Congenital Heart Disease. Pediatr. Cardiol. 2022, 43, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Strik, M.; Caillol, T.; Daniel Ramirez, F.; Abu-Alrub, S.; Marchand, H.; Welte, N.; Ritter, P.; Haïssaguerre, M.; Ploux, S.; Bordachar, P. Validating QT-Interval Measurement Using the Apple Watch ECG to Enable Remote Monitoring During the COVID-19 Pandemic. Circulation 2020, 142, 416–418. [Google Scholar] [CrossRef] [PubMed]
- Dasari, T.W.; Roe, M.T.; Chen, A.Y.; Peterson, E.D.; Giugliano, R.P.; Fonarow, G.C.; Saucedo, J.F. Impact of Time of Presentation on Process Performance and Outcomes in ST-Segment-Elevation Myocardial Infarction: A Report from the American Heart Association: Mission Lifeline Program. Circ. Cardiovasc. Qual. Outcomes 2014, 7, 656–663. [Google Scholar] [CrossRef]
- Pahlm, O.; Wagner, G.S. Proximal Placement of Limb Electrodes: A Potential Solution for Acquiring Standard Electrocardiogram Waveforms from Monitoring Electrode Positions. J. Electrocardiol. 2008, 41, 454–457. [Google Scholar] [CrossRef]
- Grande-Fidalgo, A.; Calpe, J.; Redón, M.; Millán-Navarro, C.; Soria-Olivas, E. Lead Reconstruction Using Artificial Neural Networks for Ambulatory ECG Acquisition. Sensors 2021, 21, 5542. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.H.; Van Den Heever, D.J.; Swart, W. The Reconstruction of a 12-Lead Electrocardiogram from a Reduced Lead Set Using a Focus Time-Delay Neural Network. Acta Cardiol. Sin. 2021, 37, 47–57. [Google Scholar] [CrossRef]
- Heinzelmann, P.J.; Lugn, N.E.; Kvedar, J.C. Telemedicine in the Future. J. Telemed. Telecare 2005, 11, 384–390. [Google Scholar] [CrossRef]
- Leroux, J.; Strik, M.; Ramirez, F.D.; Ploux, S.; Sacristan, B.; Chabaneix-Thomas, J.; Jalal, Z.; Thambo, J.B.; Bordachar, P. Using a Smartwatch to Record an Electrocardiogram in the Pediatric Population. J. Electrocardiol. 2022, 71, 25–27. [Google Scholar] [CrossRef] [PubMed]
- Leroux, J.; Bordachar, P.; Strik, M.; Ramirez, F.D.; Ploux, S.; Chabaneix-Thomas, J.; Jalal, Z.; Thambo, J.B. Recording an ECG With a Smartwatch in Newborns and Young Children: Feasibility and Perspectives. Can. J. Cardiol. 2021, 37, 1877–1879. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables, Units | n |
|---|---|
| Age (year), mean ± SD | 46 (20.0) |
| Gender (% Female) | 19% |
| No ECG abnormalities | 67 |
| STEMI | 23 |
| NSTEMI | 13 |
| Pericarditis | 5 |
| Pre-excitation | 12 |
| Brugada | 6 |
| Long-QT | 4 |
| HCM | 4 |
| ARVC/D | 5 |
| Atrial fibrillation | 23 |
| Atrial flutter | 7 |
| Left bundle branch block | 10 |
| Right bundle branch block | 8 |
| Other patients with chest pain | 13 |
| Variables, Units | Lead | Mean 12-Leads | Mean AW | Bias | p-Value Bias | Lower LoA | CI_Lowerloa | Upper LoA | CI_Upperloa | Absolute Offset |
|---|---|---|---|---|---|---|---|---|---|---|
| P-wave (mV), mean | I | 0.062 | 0.064 | −0.002 | 0.095 | −0.035 | [−0.041 −0.030] | 0.031 | [0.025 0.037] | 0.012 |
| II | 0.081 | 0.083 | −0.002 | 0.090 | −0.033 | [−0.038 −0.027] | 0.028 | [0.023 0.034] | 0.011 | |
| III | 0.048 | 0.052 | −0.004 | 0.103 | −0.050 | [−0.058 −0.042] | 0.042 | [0.034 0.050] | 0.018 | |
| V1 | 0.034 | 0.034 | −0.001 | 0.851 | −0.082 | [−0.097 −0.068] | 0.081 | [0.067 0.095] | 0.032 | |
| V3 | 0.084 | 0.079 | 0.005 | 0.130 | −0.087 | [−0.103 −0.071] | 0.098 | [0.081 0.114] | 0.033 | |
| V6 | 0.095 | 0.092 | 0.002 | 0.122 | −0.039 | [−0.046 −0.032] | 0.044 | [0.036 0.051] | 0.016 | |
| R-wave (mV), mean | I | 0.763 | 0.755 | 0.009 | 0.534 | −0.364 | [−0.429 −0.298] | 0.381 | [0.316 0.446] | 0.138 |
| II | 0.481 | 0.494 | −0.013 | 0.528 | −0.560 | [−0.656 −0.464] | 0.533 | [0.437 0.629] | 0.208 | |
| III | −0.187 | −0.236 | 0.049 | 0.209 | −0.683 | [−0.811 −0.555] | 0.781 | [0.652 0.909] | 0.232 | |
| V1 | −0.400 | −0.494 | 0.094 | 1.47 × 10−6 | −0.382 | [−0.466 −0.299] | 0.571 | [0.487 0.654] | 0.201 | |
| V3 | −0.158 | −0.307 | 0.149 | 8.61 × 10−7 | −0.630 | [−0.766 −0.493] | 0.928 | [0.792 1.065] | 0.332 | |
| V6 | 1.347 | 1.218 | 0.129 | 1.19 × 10−6 | −0.562 | [−0.683 −0.441] | 0.820 | [0.698 0.941] | 0.296 | |
| T-wave (mV), mean | I | 0.124 | 0.129 | −0.005 | 0.479 | −0.196 | [−0.230 −0.163] | 0.186 | [0.153 0.220] | 0.069 |
| II | 0.162 | 0.169 | −0.007 | 0.085 | −0.107 | [−0.125 −0.090] | 0.094 | [0.076 0.112] | 0.038 | |
| III | 0.061 | 0.079 | −0.018 | 0.081 | −0.210 | [−0.243 −0.176] | 0.174 | [0.141 0.207] | 0.074 | |
| V1 | 0.117 | 0.107 | 0.010 | 0.265 | −0.219 | [−0.259 −0.179] | 0.239 | [0.200 0.280] | 0.087 | |
| V3 | 0.384 | 0.397 | −0.013 | 0.505 | −0.523 | [−0.612 −0.433] | 0.497 | [0.408 0.587] | 0.182 | |
| V6 | 0.295 | 0.285 | 0.010 | 0.131 | −0.175 | [−0.208 −0.143] | 0.196 | [0.164 0.230] | 0.069 | |
| ST- segment (mV), mean | I | −0.009 | −0.004 | −0.005 | 0.065 | −0.077 | [−0.090 −0.065] | 0.067 | [0.055 0.080] | 0.026 |
| II | −0.001 | 0.000 | −0.001 | 0.781 | −0.092 | [−0.107 −0.076] | 0.090 | [0.074 0.105] | 0.031 | |
| III | 0.008 | 0.008 | 0.000 | 0.967 | −0.120 | [−0.141 −0.099] | 0.120 | [0.099 0.141] | 0.039 | |
| V1 | 0.040 | 0.035 | 0.005 | 0.088 | −0.065 | [−0.077 −0.052] | 0.074 | [0.062 0.086] | 0.026 | |
| V3 | 0.057 | 0.051 | 0.006 | 0.087 | −0.088 | [−0.104 −0.071] | 0.100 | [0.083 0.116] | 0.037 | |
| V6 | 0.000 | 0.000 | 0.000 | 0.959 | −0.127 | [−0.149 −0.104] | 0.127 | [0.105 0.150] | 0.039 |
| Variables, Units | Lead | Mean 12-Leads | Mean AW | Bias | p-Value Bias | Lower LoA | CI_Lowerloa | Upper LoA | CI_Upperloa | Absolute Offset |
|---|---|---|---|---|---|---|---|---|---|---|
| PR-interval (msec), mean | I | 153.6 | 149.8 | 3.8 | 0.1 | −52.0 | [−61.7 −42.2] | 59.6 | [49.8 69.4] | 21.0 |
| II | 148.4 | 144.5 | 3.9 | 0.1 | −54.3 | [−64.5 −44.1] | 62.1 | [51.9 72.3] | 18.8 | |
| III | 79.1 | 78.1 | 0.9 | 0.9 | −151.3 | [−178.0 −124.6] | 153.2 | [126.5 179.9] | 22.5 | |
| V1 | 139.9 | 136.6 | 3.3 | 0.1 | −49.9 | [−59.2 −40.6] | 56.5 | [47.1 65.8] | 18.2 | |
| V3 | 157.8 | 155.5 | 2.3 | 0.3 | −55.0 | [−65.1 −45.0] | 59.6 | [49.5 69.6] | 20.4 | |
| V6 | 162.5 | 159.3 | 3.2 | 0.6 | −155.8 | [−183.7 −127.9] | 162.1 | [134.3 190.0] | 32.5 | |
| QRS-complex (msec), mean | I | 116.8 | 113.9 | 2.8 | 0.1 | −39.5 | [−47.0 −32.1] | 45.2 | [37.8 52.6] | 16.9 |
| II | 111.1 | 108.5 | 2.6 | 0.1 | −36.4 | [−43.3 −29.6] | 41.7 | [34.8 48.6] | 14.8 | |
| III | 55.8 | 53.8 | 2.0 | 0.1 | −26.8 | [−31.8 −21.7] | 30.7 | [25.7 35.8] | 7.4 | |
| V1 | 122.4 | 121.0 | 1.4 | 0.1 | −24.6 | [−29.1 −20.0] | 27.4 | [22.9 32.0] | 9.5 | |
| V3 | 134.0 | 132.5 | 1.5 | 0.1 | −23.8 | [−28.2 −19.4] | 26.8 | [22.4 31.3] | 9.5 | |
| V6 | 124.9 | 123.6 | 1.3 | 0.1 | −21.8 | [−25.8 −17.7] | 24.4 | [20.3 28.4] | 8.5 | |
| QT-interval (msec), mean | I | 371.1 | 367.1 | 4.0 | 0.1 | −67.1 | [−79.5 −54.6] | 75.1 | [62.7 87.6] | 25.9 |
| II | 334.3 | 330.0 | 4.3 | 0.1 | −67.7 | [−80.3 −55.1] | 76.4 | [63.8 89.0] | 26.5 | |
| III | 183.0 | 178.8 | 4.2 | 0.1 | −60.0 | [−71.2 −48.7] | 68.3 | [57.1 79.6] | 18.1 | |
| V1 | 324.0 | 318.5 | 5.5 | 0.1 | −86.6 | [−102.7 −70.4] | 97.6 | [81.5 113.8] | 35.4 | |
| V3 | 367.5 | 362.3 | 5.2 | 0.1 | −93.9 | [−111.3 −76.5] | 104.2 | [86.9 121.7] | 34.9 | |
| V6 | 377.0 | 371.1 | 5.9 | 0.1 | −89.3 | [−106.0 −72.6] | 101.2 | [84.5 117.8] | 33.3 |
| Slope | Intercept | R-Squared | p-Value | |
|---|---|---|---|---|
| P-wave | 0.84 | 0.01 | 0.67 | <0.05 |
| R-wave | 0.99 | −0.07 | 0.90 | <0.05 |
| T-wave | 0.89 | 0.02 | 0.76 | <0.05 |
| ST-segment | 0.67 | 0.00 | 0.60 | <0.05 |
| PR-interval | 0.90 | 11.57 | 0.64 | <0.05 |
| QRS-complex | 0.96 | 2.18 | 0.93 | <0.05 |
| QT-interval | 0.95 | 12.51 | 0.92 | <0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Zande, J.; Strik, M.; Dubois, R.; Ploux, S.; Alrub, S.A.; Caillol, T.; Nasarre, M.; Donker, D.W.; Oppersma, E.; Bordachar, P. Using a Smartwatch to Record Precordial Electrocardiograms: A Validation Study. Sensors 2023, 23, 2555. https://doi.org/10.3390/s23052555
van der Zande J, Strik M, Dubois R, Ploux S, Alrub SA, Caillol T, Nasarre M, Donker DW, Oppersma E, Bordachar P. Using a Smartwatch to Record Precordial Electrocardiograms: A Validation Study. Sensors. 2023; 23(5):2555. https://doi.org/10.3390/s23052555
Chicago/Turabian Stylevan der Zande, Joske, Marc Strik, Rémi Dubois, Sylvain Ploux, Saer Abu Alrub, Théo Caillol, Mathieu Nasarre, Dirk W. Donker, Eline Oppersma, and Pierre Bordachar. 2023. "Using a Smartwatch to Record Precordial Electrocardiograms: A Validation Study" Sensors 23, no. 5: 2555. https://doi.org/10.3390/s23052555
APA Stylevan der Zande, J., Strik, M., Dubois, R., Ploux, S., Alrub, S. A., Caillol, T., Nasarre, M., Donker, D. W., Oppersma, E., & Bordachar, P. (2023). Using a Smartwatch to Record Precordial Electrocardiograms: A Validation Study. Sensors, 23(5), 2555. https://doi.org/10.3390/s23052555