

Quantification of Comfort for the Development of Binding Parts in a Standing Rehabilitation Robot


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Questionnaire
- Can you withstand that pressure for over an hour?
- Can you do your daily activities while maintaining that pressure?
- Are there any restrictions on movement?
2.3. Equipments
2.3.1. A Pneumatic Cuff and a Compression Device
2.3.2. Pressure Sensor
2.3.3. Near-Infrared Spectroscopy (NIRS)
2.3.4. Temperature Sensor
2.4. Experimental Protocol
2.4.1. Experiment 1: Measurement of Pressure and Comfort for Each Binding Part
2.4.2. Experiment 2: Measurement of Comfort and Physiological Changes in the Thigh
2.5. Statistical Analysis
3. Results
3.1. Comfort and Interface Pressure at Binding Parts
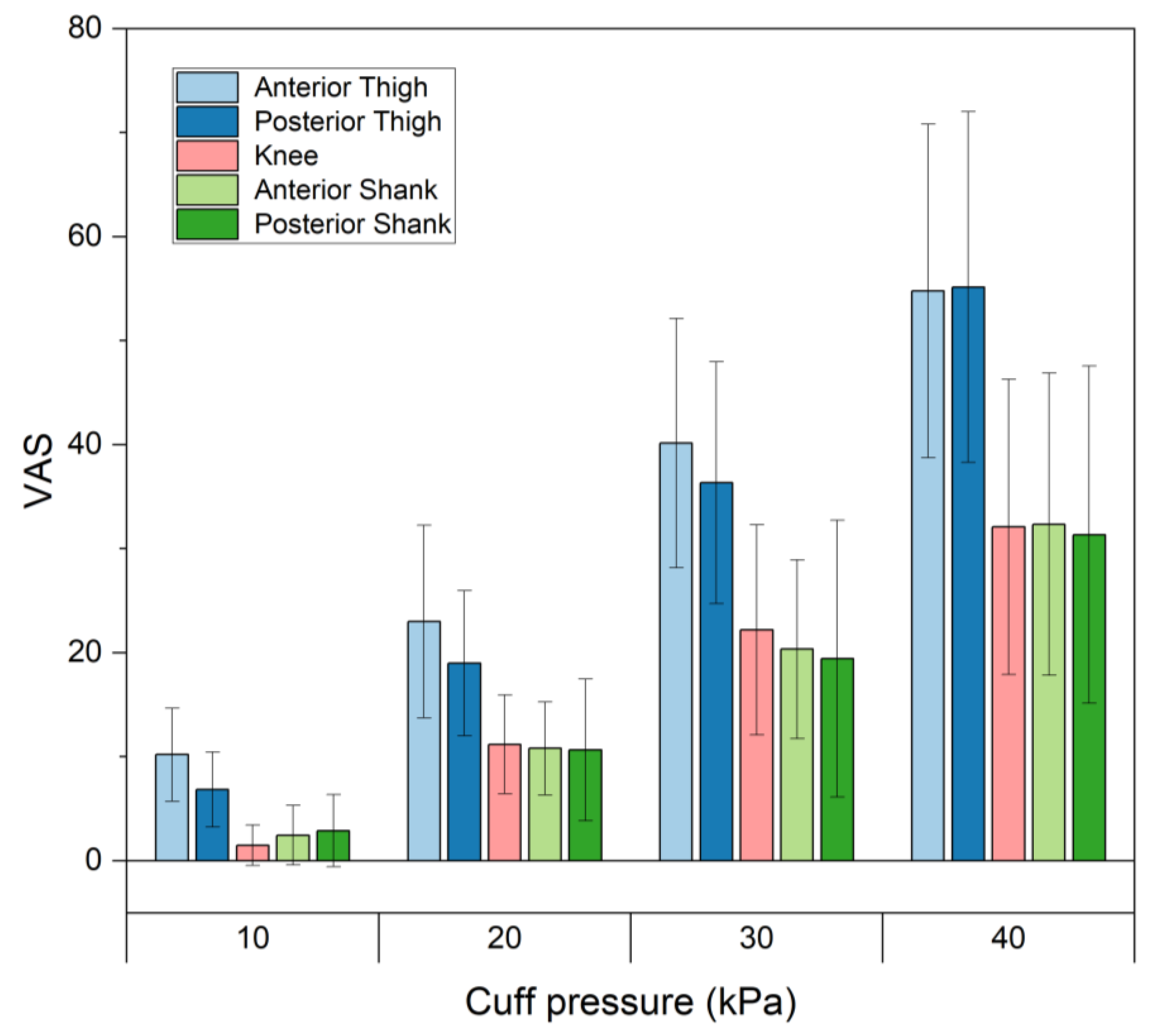
3.1.1. VAS
3.1.2. Masking of Interface Pressure Distributions
3.2. Comfort and Physiological Changes in the Thigh
3.2.1. Questionnaire
3.2.2. Interface Pressure
3.2.3. Tissue Oxygen Saturation (StO2)
3.2.4. Skin Temperature
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tamez-Duque, J.; Cobian-Ugalde, R.; Kilicarslan, A.; Venkatakrishnan, A.; Soto, R.; Contreras-Vidal, J.L. Real-Time Strap Pressure Sensor System for Powered Exoskeletons. Sensors 2015, 15, 4550–4563. [Google Scholar] [CrossRef]
- Rathore, A.; Wilcox, M.; Ramirez, D.Z.M.; Loureiro, R.; Carlson, T. Quantifying the human-robot interaction forces between a lower limb exoskeleton and healthy users. In Proceedings of the 38th Annual International Conference of the IEEE Engi-neering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 586–589. [Google Scholar]
- Pons, J.L. Rehabilitation Exoskeletal Robotics. IEEE Eng. Med. Biol. Mag. 2010, 29, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Benson, I.; Hart, K.; Tussler, D.; Van Middendorp, J.J. Lower-limb exoskeletons for individuals with chronic spinal cord injury: Findings from a feasibility study. Clin. Rehabil. 2015, 30, 73–84. [Google Scholar] [CrossRef]
- Groah, S.L.; Schladen, M.; Pineda, C.G.; Hsieh, C.-H.J. Prevention of Pressure Ulcers Among People With Spinal Cord Injury: A Systematic Review. PMR 2014, 7, 613–636. [Google Scholar] [CrossRef] [PubMed]
- Meyer, J.T.; Schrade, S.O.; Lambercy, O.; Gassert, R. User-centered Design and Evaluation of Physical Interfaces for an Exoskeleton for Paraplegic Users. In Proceedings of the 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), Toroto, ON, Canada, 24–28 June 2019; pp. 1159–1166. [Google Scholar]
- Sanchez-Villamañan, M.D.C.; Gonzalez-Vargas, J.; Torricelli, D.; Moreno, J.C.; Pons, J.L. Compliant lower limb exoskeletons: A comprehensive review on mechanical design principles. J. Neuroeng. Rehabil. 2019, 16, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Yandell, M.B.; Quinlivan, B.T.; Popov, D.; Walsh, C.; Zelik, K.E. Physical interface dynamics alter how robotic exosuits augment human movement: Implications for optimizing wearable assistive devices. J. Neuroeng. Rehabil. 2017, 14, 1–11. [Google Scholar] [CrossRef]
- Merskey, N.; Bogduk, N. (Eds.) Classification of Chronic Pain. Task Force on Taxonomy, 2nd ed.; IASP Press: Washington, DC, USA, 1994. [Google Scholar]
- Daly, W.C.; Voo, L.; Rosenbaum-Chou, T.; Arabian, A.P.; Boone, D.P. Socket Pressure and Discomfort in Upper-Limb Prostheses. JPO J. Prosthetics Orthot. 2014, 26, 99–106. [Google Scholar] [CrossRef]
- Li, W.; Mo, R.; Yu, S.; Chu, J.; Hu, Y.; Wang, L. The effects of the seat cushion contour and the sitting posture on surface pressure distribution and comfort during seated work. Int. J. Occup. Med. Environ. Health 2020, 33, 675–689. [Google Scholar] [CrossRef] [PubMed]
- Harms-Ringdahl, K.; Carlsson, A.M.; Ekholm, J.; Raustorp, A.; Svensson, T.; Toresson, H.-G. Pain assessment with different intensity scales in response to loading of joint structures. Pain 1986, 27, 401–411. [Google Scholar] [CrossRef]
- Chaffin, D.B. Localized muscle fatigue—Definition and measurement. J. Occup. Environ. Med. 1973, 15, 346–354. [Google Scholar]
- Wiker, S.F.; Chaffin, D.B.; Langolf, G.D. Shoulder posture and localized muscle fatigue and discomfort. Ergonomics 1989, 32, 211–237. [Google Scholar] [CrossRef] [PubMed]
- Kermavnar, T.; Power, V.; de Eyto, A.; O’Sullivan, L.W. Computerized Cuff Pressure Algometry as Guidance for Circumferential Tissue Compression for Wearable Soft Robotic Applications: A Systematic Review. Soft Robot. 2018, 5, 1–16. [Google Scholar] [CrossRef]
- Pons, J.L.; Rocon, E.; Ruiz, A.F.; Raya, R.; Schiele, A. Wearable Robots: Biomechatronic Exoskeletons; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- Yandell, M.B.; Ziemnicki, D.M.; McDonald, K.A.; Zelik, K.E. Characterizing the comfort limits of forces applied to the shoulders, thigh and shank to inform exosuit design. PLOS ONE 2020, 15, e0228536. [Google Scholar] [CrossRef] [PubMed]
- Kermavnar, T.; O’Sullivan, K.J.; De Eyto, A.; O’Sullivan, L.W. Discomfort/Pain and Tissue Oxygenation at the Lower Limb During Circumferential Compression: Application to Soft Exoskeleton Design. Hum. Factors J. Hum. Factors Ergon. Soc. 2020, 62, 475–488. [Google Scholar] [CrossRef] [PubMed]
- Bouten, C.V.; Oomens, C.W.; Baaijens, F.P.; Bader, D.L. The etiology of pressure ulcers: Skin deep or muscle bound? Arch. Phys. Med. Rehabil. 2003, 84, 616–619. [Google Scholar] [CrossRef] [PubMed]
- Agam, L.; Gefen, A. Pressure ulcers and deep tissue injury: A bioengineering perspective. J. Wound Care 2007, 16, 336–342. [Google Scholar] [CrossRef]
- Stekelenburg, A.; Gawlitta, D.; Bader, D.L.; Oomens, C.W. Deep Tissue Injury: How Deep is Our Understanding? Arch. Phys. Med. Rehabil. 2008, 89, 1410–1413. [Google Scholar] [CrossRef]
- Reenalda, J.; Jannink, M.; Nederhand, M.; Ijzerman, M. Clinical Use of Interface Pressure to Predict Pressure Ulcer Development: A Systematic Review. Assist. Technol. 2009, 21, 76–85. [Google Scholar] [CrossRef]
- Oomens, C.; Loerakker, S.; Bader, D. The importance of internal strain as opposed to interface pressure in the prevention of pressure related deep tissue injury. J. Tissue Viability 2010, 19, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Sangeorzan, B.J.; Harrington, R.M.; Wyss, C.R.; Czerniecki, J.M.; Iii, F.A.M. Circulatory and mechanical response of skin to loading. J. Orthop. Res. 1989, 7, 425–431. [Google Scholar] [CrossRef]
- Bader, D. The recovery characteristics of soft tissues following repeated loading. J. Rehabil. Res. Dev. 1990, 27, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Makhsous, M.; Lin, F.; Hanawalt, D.; Kruger, S.L.; LaMantia, A. The Effect of Chair Designs on Sitting Pressure Distribution and Tissue Perfusion. Hum. Factors J. Hum. Factors Ergon. Soc. 2012, 54, 1066–1074. [Google Scholar] [CrossRef] [PubMed]
- Mak, A.F.; Zhang, M.; Tam, E.W. Biomechanics of Pressure Ulcer in Body Tissues Interacting with External Forces during Locomotion. Annu. Rev. Biomed. Eng. 2010, 12, 29–53. [Google Scholar] [CrossRef]
- Kermavnar, T.; O’Sullivan, K.J.; Casey, V.; de Eyto, A.; O’Sullivan, L.W. Circumferential tissue compression at the lower limb during walking, and its effect on discomfort, pain and tissue oxygenation: Application to soft exoskeleton design. Appl. Ergon 2020, 86, 103093. [Google Scholar] [CrossRef]
- Reinhardt, L.; Siebert, T.; Leichsenring, K.; Blickhan, R.; Böl, M. Intermuscular pressure between synergistic muscles correlates with muscle force. J. Exp. Biol. 2016, 219, 2311–2319. [Google Scholar] [CrossRef] [PubMed]
- Ohnhaus, E.E.; Adler, R. Methodological problems in the measurement of pain: A comparison between the verbal rating scale and the visual analogue scale. Pain 1975, 1, 379–384. [Google Scholar] [CrossRef]
- Mueller, M.J.; Zou, D.; Lott, D.J. “Pressure Gradient” as an Indicator of Plantar Skin Injury. Diabetes Care 2005, 28, 2908–2912. [Google Scholar] [CrossRef]
- Lyder, C.H. Pressure Ulcer Prevention and Management. JAMA 2003, 289, 223–226. [Google Scholar] [CrossRef]
- Partsch, B.; Partsch, H. Calf compression pressure required to achieve venous closure from supine to standing positions. J. Vasc. Surg. 2005, 42, 734–738. [Google Scholar] [CrossRef]
- Rastel, D.; Lun, B. Lower Limb Deep Vein Diameters Beneath Medical Compression Stockings in the Standing Position. Eur. J. Vasc. Endovasc. Surg. 2018, 57, 276–282. [Google Scholar] [CrossRef]
- Ring, E.F.J.; Ammer, K. Infrared thermal imaging in medicine. Physiol. Meas. 2012, 33, R33–R46. [Google Scholar] [CrossRef] [PubMed]
- Hom, C.; Vasquez, P.; Pozos, R.S. Peripheral skin temperature effects on muscle oxygen levels. J. Therm. Biol. 2004, 29, 785–789. [Google Scholar] [CrossRef]
- Kaplan, L.J.; McPartland, K.; Santora, T.A.; Trooskin, S.Z. Start with a Subjective Assessment of Skin Temperature to Identify Hypoperfusion in Intensive Care Unit Patients. J. Trauma Inj. Infect. Crit. Care 2001, 50, 620–628. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cuff Pressure (kPa) | Interface Pressure for Each Mask (kPa) | ||||
|---|---|---|---|---|---|
| Whole | Medial | Center | Lateral | ||
| Anterior Thigh | 10 | 7.9 0.9 | 7.8 1.2 | 8.0 1.6 | 8.2 1.2 |
| 20 | 18.1 0.8 | 18.5 1.8 | 18.3 2.2 | 18.2 1.7 | |
| 30 | 28.1 1.1 | 28.9 2.5 | 29.1 3.5 | 28.1 2.1 | |
| 40 | 37.5 1.4 | 39.2 2.9 | 38.2 3.2 | 37.5 2.6 | |
| Posterior Thigh | 10 | 8.1 0.8 | 8.1 0.8 | 8.4 1.5 | 7.9 1.1 |
| 20 | 17.9 0.8 | 17.6 1.6 | 18.5 2.0 | 17.8 1.7 | |
| 30 | 28.1 1.0 | 27.3 2.2 | 29.2 3.1 | 28.3 2.1 | |
| 40 | 38.1 1.3 | 36.9 2.6 | 39.5 3.7 | 28.3 3.3 | |
| Knee | 10 | 7.8 0.9 | 8.0 1.0 | 8.0 1.4 | 7.6 1.0 |
| 20 | 18.8 1.3 | 19.3 1.7 | 18.8 2.4 | 18.9 1.4 | |
| 30 | 29.7 1.5 | 30.3 1.9 | 29.8 3.1 | 29.7 2.0 | |
| 40 | 40.2 1.6 | 40.7 2.2 | 40.5 3.3 | 40.1 2.0 | |
| Anterior Shank | 10 | 7.3 0.7 | 7.3 0.9 | 7.0 1.0 | 7.6 0.8 |
| 20 | 17.4 1.2 | 18.0 1.7 | 16.3 1.5 | 18.1 1.2 | |
| 30 | 27.4 1.3 | 28.6 2.2 | 25.8 1.8 | 28.5 1.2 | |
| 40 | 37.6 1.5 | 39.0 2.5 | 35.9 2.3 | 38.9 1.3 | |
| Posterior Shank | 10 | 7.3 0.7 | 7.5 1.0 | 7.4 1.0 | 7.3 0.7 |
| 20 | 17.3 0.8 | 17.6 1.9 | 17.3 1.9 | 17.5 1.6 | |
| 30 | 27.5 1.7 | 28.0 3.0 | 27.7 2.6 | 28.2 2.6 | |
| 40 | 38.2 1.5 | 38.5 3.8 | 38.3 3.0 | 38.9 3.1 | |
| Cuff Pressure (kPa) | ||||
|---|---|---|---|---|
| 10 | 13.3 | 16.7 | 20 | |
| VAS | 15.2 ± 7.1 | 28.0 ± 11.2 | 42.4 ± 12.9 | 51.4 ± 13.7 |
| Likert scale (1: strongly disagree, 7: strongly agree) | ||||
| Can you withstand for over an hour? | 6.7 ± 0.9 | 5.7 ± 1.3 | 4.1 ± 1.4 | 2.9 ± 1.6 |
| Can you do your daily activities while maintaining the pressure? | 5.9 ± 1.0 | 4.9 ± 1.3 | 3.8 ± 1.3 | 2.5 ± 1.7 |
| Are there any restrictions on movement? | 1.6 ± 0.7 | 2.7 ± 0.9 | 3.7 ± 0.8 | 4.6 ± 1.1 |
| Cuff Pressure (kPa) | ||||
|---|---|---|---|---|
| 10 | 13.3 | 16.7 | 20 | |
| Maximum pressure (kPa) | 12.0 ± 2.2 | 19.0 ± 3.9 | 24.5 ± 4.3 | 31.6 ± 5.8 |
| Pressure gradient (kPa/mm) | 0.8 ± 0.3 | 1.2 ± 0.5 | 1.5 ± 0.6 | 2.1 ± 0.8 |
| Skin temperature on the compressed leg (right) (°C) | 32.2 ± 1.0 | 33.6 ± 0.8 | 33.8 ± 0.8 | 33.9 ± 0.8 |
| Skin temperature on the unpressurized leg (left) (°C) | 31.6 ± 0.7 | 32.6 ± 0.8 | 32.9 ± 0.6 | 32.8 ± 0.8 |
| Temperature change on the compressed leg (right) (°C) | 0.5 ± 0.3 | 0.2 ± 0.3 | 0.1 ± 0.3 | 0.0 ± 0.3 |
| Temperature change on the unpressurized leg (left) (°C) | 0.4 ± 0.1 | 0.1 ± 0.1 | 0.0 ± 0.2 | 0.0 ± 0.2 |
| Cuff Pressure (kPa) | |||||
|---|---|---|---|---|---|
| 10 | 13.3 | 16.7 | 20 | ||
| StO2 (%) | 111.9 ± 6.7 | 110.9 ± 5.9 | 107.5 ± 9.6 | 92.2 ± 16.9 | |
| Increase group | Number of subjects | 14 | 14 | 13 | 6 |
| StO2 (%) | 113.0 ± 5.6 | 112.3 ± 5.1 | 112.1 ± 5.1 | 110.9 ± 5.3 | |
| Decreased group | Number of subjects | 1 | 1 | 2 | 9 |
| StO2 (%) | 97.2 | 99.8 | 89.0 ± 7.5 | 84.7 ± 13.4 | |
| Subject | StO2 | Skin Temperature |
|---|---|---|
| #1 | −0.966 | −0.527 |
| #2 | −0.844 | 0.986 |
| #3 | −0.907 | 0.897 |
| #4 | −0.921 | 0.580 |
| #5 | −0.354 | 0.346 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nam, Y.; Yang, S.; Kim, J.; Koo, B.; Song, S.; Kim, Y. Quantification of Comfort for the Development of Binding Parts in a Standing Rehabilitation Robot. Sensors 2023, 23, 2206. https://doi.org/10.3390/s23042206
Nam Y, Yang S, Kim J, Koo B, Song S, Kim Y. Quantification of Comfort for the Development of Binding Parts in a Standing Rehabilitation Robot. Sensors. 2023; 23(4):2206. https://doi.org/10.3390/s23042206
Chicago/Turabian StyleNam, Yejin, Sumin Yang, Jongman Kim, Bummo Koo, Sunghyuk Song, and Youngho Kim. 2023. "Quantification of Comfort for the Development of Binding Parts in a Standing Rehabilitation Robot" Sensors 23, no. 4: 2206. https://doi.org/10.3390/s23042206
APA StyleNam, Y., Yang, S., Kim, J., Koo, B., Song, S., & Kim, Y. (2023). Quantification of Comfort for the Development of Binding Parts in a Standing Rehabilitation Robot. Sensors, 23(4), 2206. https://doi.org/10.3390/s23042206