


Test–Retest and Between–Device Reliability of Vmaxpro IMU at Hip and Ankle for Vertical Jump Measurement





Abstract
:1. Introduction
2. Materials and Methods
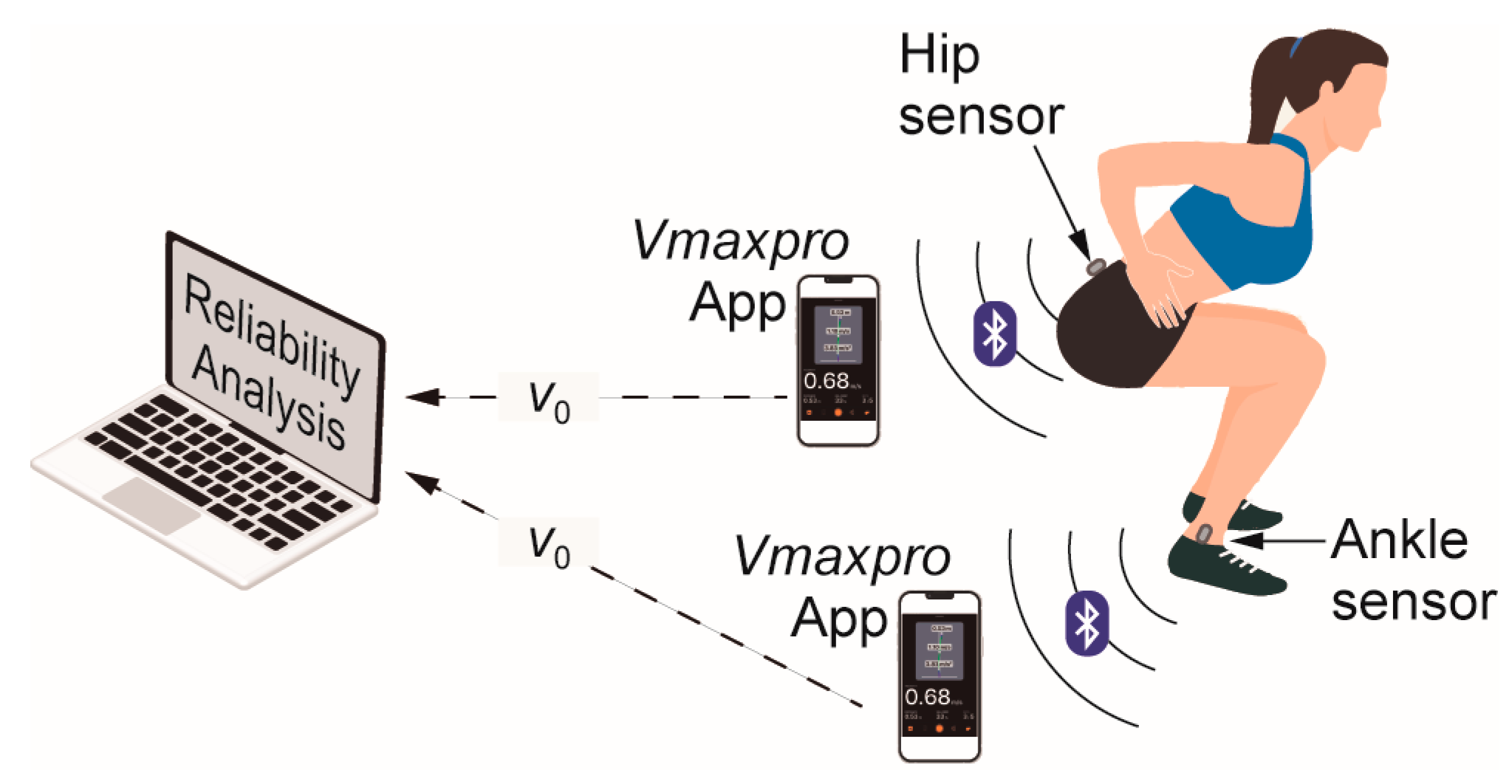
2.1. Study Design
2.2. Procedure
2.3. Participants
2.4. IMU-Based Vmaxpro
2.5. Statistical Analysis
3. Results
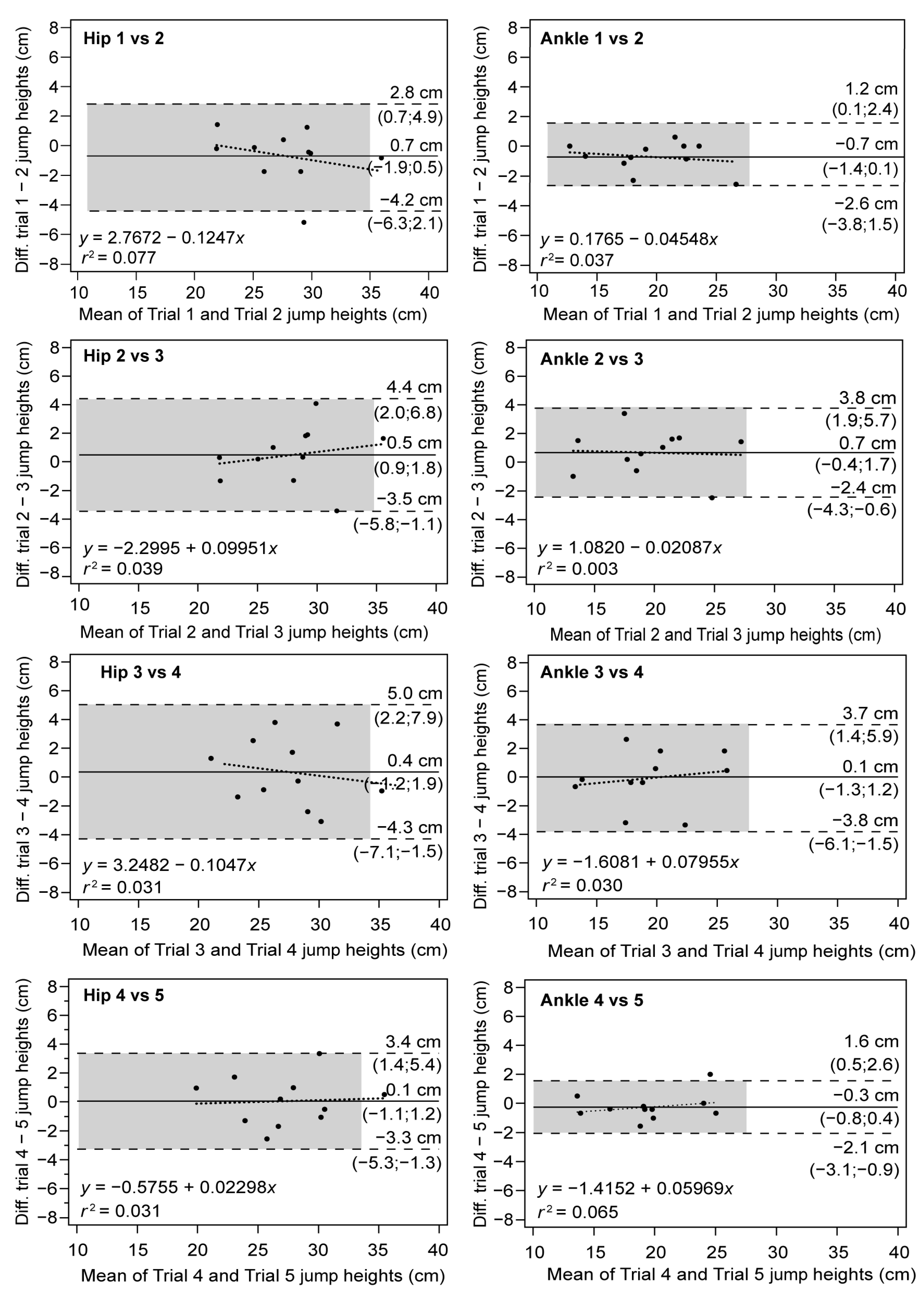
3.1. Intra-Session Test–Retest Reliability
3.2. Between-Session Test–Retest Reliability
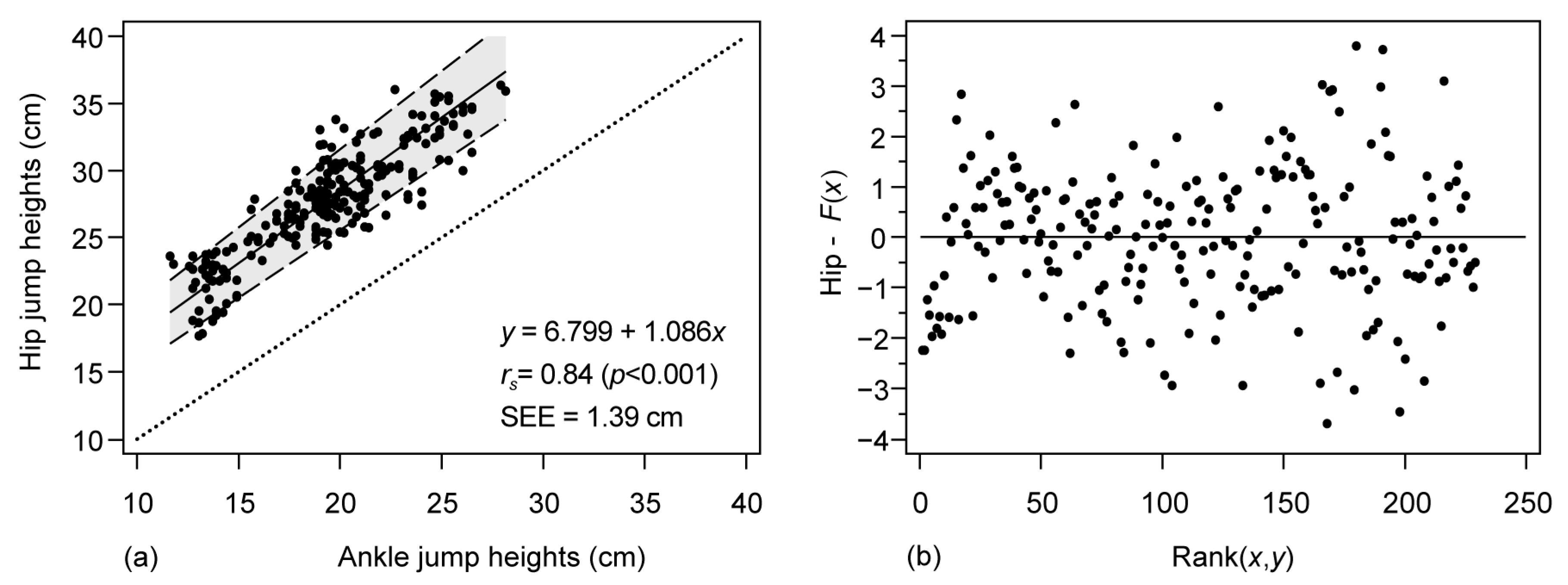
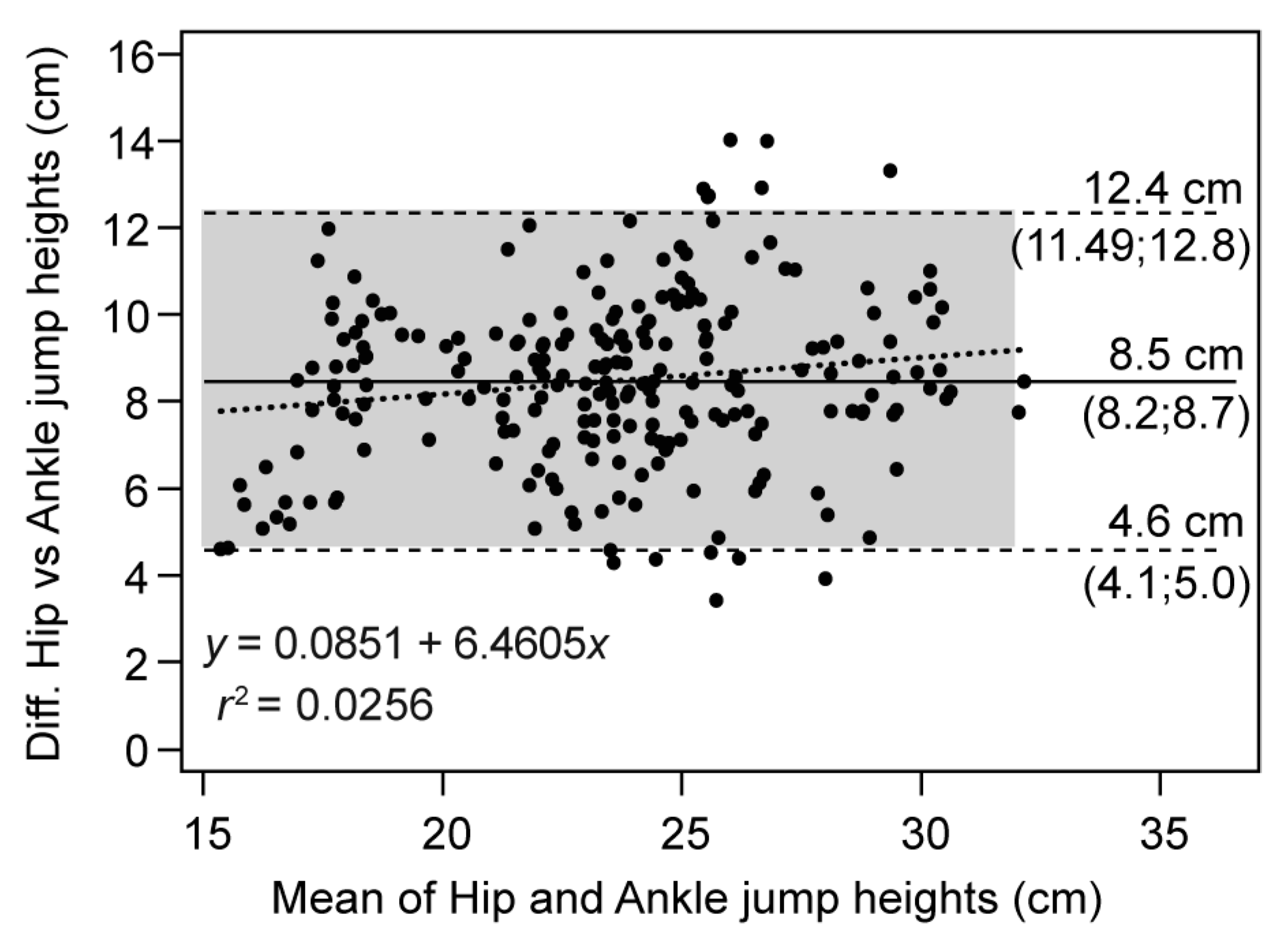
3.3. Between-Device Reliability (Vmaxpro in Hip vs. Vmaxpro in Ankle)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rantalainen, T.; Finni, T.; Walker, S. Jump Height from Inertial Recordings: A Tutorial for a Sports Scientist. Scand. J. Med. Sci. Sports 2020, 30, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Cronin, J.; Hansen, K. Strength and Power Predictors of Sports Speed. J. Strength Cond. Res. 2005, 19, 349–357. [Google Scholar] [PubMed]
- Pálinkás, G.; Béres, B.; Tróznai, Z.; Utczás, K.; Petridis, L. The Relationship of Maximal Strength with the Force-Velocity Profile in Resistance Trained Women. Acta Polytech. Hung. 2021, 18, 173–185. [Google Scholar] [CrossRef]
- Washif, J.A.; Kok, L.-Y. Relationships between Vertical Jump Metrics and Sprint Performance, and Qualities That Distinguish Between Faster and Slower Sprinters. J. Sci. Sport Exerc. 2021, 4, 135–144. [Google Scholar] [CrossRef]
- Alba-Jiménez, C.; Moreno-Doutres, D.; Peña, J. Trends Assessing Neuromuscular Fatigue in Team Sports: A Narrative Review. Sports 2022, 10, 33. [Google Scholar] [CrossRef]
- Gathercole, R.J.; Sporer, B.C.; Stellingwerff, T.; Sleivert, G.G. Comparison of the Capacity of Different Jump and Sprint Field Tests to Detect Neuromuscular Fatigue. J. Strength Cond. Res. 2015, 29, 2522–2531. [Google Scholar] [CrossRef]
- McMahon, J.J.; Suchomel, T.J.; Lake, J.P.; Comfort, P. Understanding the Key Phases of the Countermovement Jump Force-Time Curve. Strength Cond. J. 2018, 40, 96–106. [Google Scholar] [CrossRef]
- Aragón, L.F. Evaluation of Four Vertical Jump Tests: Methodology, Reliability, Validity, and Accuracy. Meas. Phys. Educ. Exerc. Sci. 2000, 4, 215–228. [Google Scholar] [CrossRef]
- Villalon-Gasch, L.; Penichet-Tomás, A.; Jimenez-Olmedo, J.M.; Espina-agulló, J.J. Reliability of a Linear Sprint Test on Sand in Elite Female Beach Handball Players. J. Phys. Educ. Sport (JPES) 2022, 22, 1246–1251. [Google Scholar] [CrossRef]
- Olaya-Cuartero, J.; Cejuela, R. Influence of Biomechanical Parameters on Performance in Elite Triathletes along 29 Weeks of Training. Appl. Sci. 2021, 11, 1050. [Google Scholar] [CrossRef]
- Glatthorn, J.F.; Gouge, S.; Nussbaumer, S.; Stauffacher, S.; Impellizzeri, F.M.; Maffiuletti, N.A. Validity and Reliability of Optojump Photoelectric Cells for Estimating Vertical Jump Height. J. Strength Cond. Res. 2011, 25, 556–560. [Google Scholar] [CrossRef] [PubMed]
- Marković, S.; Dopsaj, M.; Tomažič, S.; Umek, A. Potential of IMU-Based Systems in Measuring Single Rapid Movement Variables in Females with Different Training Backgrounds and Specialization. Appl. Bionics Biomech. 2020, 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Fritschi, R.; Seiler, J.; Gross, M. Validity and Effects of Placement of Velocity-Based Training Devices. Sports 2021, 9, 123. [Google Scholar] [CrossRef] [PubMed]
- Olovsson Ståhl, E.; Öhrner, P. Concurrent Validity of an Inertial Sensor for Measuring Muscle Mechanical Properties. 2020. Available online: http://urn.kb.se/resolve?urn=urn:nbn:se:umu:diva-173423 (accessed on 30 January 2023).
- Rago, V.; Brito, J.; Figueiredo, P.; Carvalho, T.; Fernandes, T.; Fonseca, P.; Rebelo, A. Countermovement Jump Analysis Using Different Portable Devices: Implications for Field Testing. Sports 2018, 6, 91. [Google Scholar] [CrossRef]
- Brooks, E.R.; Benson, A.C.; Bruce, L.M. Novel Technologies Found to Be Valid and Reliable for the Measurement of Vertical Jump Height with Jump-and-Reach Testing. J. Strength Cond. Res. 2018, 32, 2838–2845. [Google Scholar] [CrossRef]
- Spangler, R.; Rantalainen, T.; Gastin, P.B.; Wundersitz, D. Inertial Sensors Are a Valid Tool to Detect and Consistently Quantify Jumping. Int. J. Sports Med. 2018, 39, 802–808. [Google Scholar] [CrossRef]
- Rantalainen, T.; Gastin, P.B.; Spangler, R.; Wundersitz, D. Concurrent Validity and Reliability of Torso-Worn Inertial Measurement Unit for Jump Power and Height Estimation. J. Sports Sci. 2018, 36, 1937–1942. [Google Scholar] [CrossRef]
- Garnacho-Castaño, M.v.; Faundez-Zanuy, M.; Serra-Payá, N.; Maté-Muñoz, J.L.; López-Xarbau, J.; Vila-Blanch, M. Reliability and Validity of the Polar V800 Sports Watch for Estimating Vertical Jump Height. J. Sports Sci. Med. 2021, 20, 149–157. [Google Scholar] [CrossRef]
- Schleitzer, S.; Wirtz, S.; Julian, R.; Eils, E. Development and Evaluation of an Inertial Measurement Unit (IMU) System for Jump Detection and Jump Height Estimation in Beach Volleyball. Ger. J. Exerc. Sport Res. 2022, 52, 228–236. [Google Scholar] [CrossRef]
- Montalvo, S.; Gonzalez, M.P.; Dietze-Hermosa, M.S.; Eggleston, J.D.; Dorgo, S. Common Vertical Jump and Reactive Strength Index Measuring Devices: A Validity and Reliability Analysis. J. Strength Cond. Res. 2021, 35, 1234–1243. [Google Scholar] [CrossRef] [PubMed]
- Pino-Ortega, J.; García-Rubio, J.; Ibáñez, S.J. Validity and Reliability of the WIMU Inertial Device for the Assessment of the Vertical Jump. PeerJ 2018, 6, e4709. [Google Scholar] [CrossRef] [PubMed]
- Watkins, C.M.; Maunder, E.; van den Tillaar, R.; Oranchuk, D.J. Concurrent Validity and Reliability of Three Ultra-Portable Vertical Jump Assessment Technologies. Sensors 2020, 20, 7240. [Google Scholar] [CrossRef] [PubMed]
- Clemente, F.; Badicu, G.; Hasan, U.C.; Akyildiz, Z.; Pino-Ortega, J.; Silva, R.; Rico-González, M. Validity and Reliability of Inertial Measurement Units for Jump Height Estimations: A Systematic Review. Hum. Mov. 2022, 23, 1–20. [Google Scholar] [CrossRef]
- Read, M.M. The Effects of Varied Rest Interval Lengths on Depth Jump Performance; San Jose State University: San Jose, CA, USA, 1997; Volume 15. [Google Scholar]
- Mandic, R.; Jakovljevic, S.; Jaric, S. Effects of Countermovement Depth on Kinematic and Kinetic Patterns of Maximum Vertical Jumps. J. Electromyogr. Kinesiol. 2015, 25, 265–272. [Google Scholar] [CrossRef]
- Pérez-Castilla, A.; Rojas, F.J.; Gómez-Martínez, F.; García-Ramos, A. Vertical Jump Performance Is Affected by the Velocity and Depth of the Countermovement. Sports Biomech. 2019, 20, 1015–1030. [Google Scholar] [CrossRef]
- López, J.M.; López, J.L. Relevance of the Technique of Immobilizing Arms for the Kinetic Variables in the Countermovement Jump Test. Cult. Cienc. Y Deporte 2012, 7, 173–178. [Google Scholar] [CrossRef]
- Wade, L.; Lichtwark, G.A.; Farris, D.J. Comparisons of Laboratory-Based Methods to Calculate Jump Height and Improvements to the Field-Based Flight-Time Method. Scand. J. Med. Sci. Sports 2020, 30, 31–37. [Google Scholar] [CrossRef]
- McKay, A.K.A.; Stellingwerff, T.; Smith, E.S.; Martin, D.T.; Mujika, I.; Goosey-Tolfrey, V.L.; Sheppard, J.; Burke, L.M. Defining Training and Performance Caliber: A Participant Classification Framework. Int. J. Sports Physiol. Perform. 2022, 17, 317–331. [Google Scholar] [CrossRef]
- Held, S.; Rappelt, L.; Deutsch, J.-P.; Donath, L.; Jimenez-Olmedo, M. Valid and Reliable Barbell Velocity Estimation Using an Inertial Measurement Unit. Int. J. Environ. Res. Public Health 2021, 18, 9170. [Google Scholar] [CrossRef]
- Jimenez Olmedo, J.M.; Olaya-cuartero, J.; Villalon-gasch, L.; Penichet-tomás, A. Validity and Reliability of the VmaxPro IMU for Back Squat Exercise in Multipower Machine. J. Phys. Educ. Sport (JPES) 2022, 22, 2920–2926. [Google Scholar] [CrossRef]
- Linthorne, N.P. Analysis of Standing Vertical Jumps Using a Force Platform. Am. J. Phys. 2001, 69, 1198–1204. [Google Scholar] [CrossRef]
- Linnecke, T. How to Perform Jump Tests with Vmaxpro. Available online: https://vmaxpro.de/how-to-perform-jump-tests-with-vmaxpro/ (accessed on 19 September 2022).
- Courel-Ibáñez, J.; Martínez-Cava, A.; Morán-Navarro, R.; Escribano-Peñas, P.; Chavarren-Cabrero, J.; González-Badillo, J.J.; Pallarés, J.G. Reproducibility and Repeatability of Five Different Technologies for Bar Velocity Measurement in Resistance Training. Ann. Biomed. Eng. 2019, 47, 1523–1538. [Google Scholar] [CrossRef] [PubMed]
- Shrout, P.E.; Fleiss, J.L. Intraclass Correlations: Uses in Assessing Rater Reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Hedayat, A.S.; Sinha, B.; Yang, M. Statistical Methods in Assessing Agreement: Models, Issues, and Tools. J. Am. Stat. Assoc. 2002, 97, 257–270. [Google Scholar] [CrossRef]
- Lake, J.; Augustus, S.; Austin, K.; Mundy, P.; McMahon, J.; Comfort, P.; Haff, G. The Validity of the Push Band 2.0 during Vertical Jump Performance. Sports 2018, 6, 140. [Google Scholar] [CrossRef]
- Passing, H.; Bablok, W. Comparison of Several Regression Procedures for Method Comparison Studies and Determination of Sample Sizes. Application of Linear Regression Procedures for Method Comparison Studies in Clinical Chemistry, Part II. Clin. Chem. Lab. Med. 1984, 22, 431–445. [Google Scholar] [CrossRef]
- Portney, L.G. Foundations of Clinical Research: Applications to Evidence-Based Practice, 4th ed.; Dean Emerita MGH Institute of Health Professions School of Health and Rehabilitation Sciences Boston, M., F.A. Davis Company, Eds.; F.A. Davis Company: Philadelphia, PA, USA, 2020; ISBN 9780803661134. [Google Scholar]
- Atkinson, G.; Nevill, A.M. Statistical Methods for Assessing Measurement Error (Reliability) in Variables Relevant to Sports Medicine. Sport. Med. 1998, 26, 217–238. [Google Scholar] [CrossRef]
- Montoro-Bombú, R.; Field, A.; Santos, A.C.; Rama, L. Validity and Reliability of the Output Sport Device for Assessing Drop Jump Performance. Front. Bioeng. Biotechnol. 2022, 10, 1015526. [Google Scholar] [CrossRef]
- Hopkins, W.G. Measures of Reliability in Sports Medicine and Science. Sport. Med. 2000, 30, 1–15. [Google Scholar] [CrossRef]
- Bernards, J.R.; Sato, K.; Haff, G.G.; Bazyler, C.D. Current Research and Statistical Practices in Sport Science and a Need for Change. Sports 2017, 5, 87. [Google Scholar] [CrossRef]
- Pueo, B.; Lopez, J.J.; Mossi, J.M.; Colomer, A.; Jimenez-Olmedo, J.M. Video-Based System for Automatic Measurement of Barbell Velocity in Back Squat. Sensors 2021, 21, 925. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, A.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sports Exerc. 2009, 41, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.H.; Fraser, C.G. Strategies to Set Global Analytical Quality Specifications in Laboratory Medicine: 10 Years on from the Stockholm Consensus Conference. Accredit. Qual. Assur. 2010, 15, 323–330. [Google Scholar] [CrossRef]
- Stöckl, D.; Rodríguez Cabaleiro, D.; van Uytfanghe, K.; Thienpont, L.M. Interpreting Method Comparison Studies by Use of the Bland-Altman Plot: Reflecting the Importance of Sample Size by Incorporating Confidence Limits and Predefined Error Limits in the Graphic. Clin. Chem. 2004, 50, 2216–2218. [Google Scholar] [CrossRef]
- Bartlett, J.W.; Frost, C. Reliability, Repeatability and Reproducibility: Analysis of Measurement Errors in Continuous Variables. Ultrasound Obstet. Gynecol. 2008, 31, 466–475. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G. A Spreadsheet to Compare Means of Two Groups. Sportscience 2015, 19, 36–44. [Google Scholar]
- Buchheit, M.; Lacome, M.; Cholley, Y.; Simpson, B.M. Neuromuscular Responses to Conditioned Soccer Sessions Assessed via GPS-Embedded Accelerometers: Insights into Tactical Periodization. Int. J. Sports Physiol. Perform. 2018, 13, 577–583. [Google Scholar] [CrossRef]
- Pérez-Castilla, A.; Fernandes, J.F.T.; Rojas, F.J.; García-Ramos, A. Reliability and Magnitude of Countermovement Jump Performance Variables: Influence of the Take-off Threshold. Meas. Phys. Educ. Exerc. Sci. 2021, 25, 227–235. [Google Scholar] [CrossRef]
- Weenk, D.; Stevens, A.G.; Koning, B.; Van Bernhard, B.-J.; Hermanus, J.H.; Veltink, P.H. A Feasibility Study in Measuring Soft Tissue Artifacts on the Upper Leg Using Inertial and Magnetic Sensors. In Proceedings of the 4th Dutch Bio-Medical Engineering Conference sensors, Egmond aan Zee, The Netherlands, 24–25 January 2013; p. 154. [Google Scholar]
- Claudino, J.G.; Cronin, J.; Mezêncio, B.; McMaster, D.T.; McGuigan, M.; Tricoli, V.; Amadio, A.C.; Serrão, J.C. The Countermovement Jump to Monitor Neuromuscular Status: A Meta-Analysis. J. Sci. Med. Sport 2017, 20, 397–402. [Google Scholar] [CrossRef]
- Pueo, B.; Hopkins, W.; Penichet-Tomas, A.; Jimenez-Olmedo, J. Accuracy of Flight Time and Countermovement-Jump Height Estimated from Videos at Different Frame Rates with MyJump. Biol. Sport 2023, 40, 595–601. [Google Scholar] [CrossRef]
- García-Pinillos, F.; Roche-Seruendo, L.E.; Marcén-Cinca, N.; Marco-Contreras, L.A.; Latorre-Román, P.A. Absolute Reliability and Concurrent Validity of the Stryd System for the Assessment of Running Stride Kinematics at Different Velocities. J. Strength Cond. Res. 2021, 35, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Gindre, C.; Lussiana, T.; Hebert-Losier, K.; Morin, J.B. Reliability and Validity of the Myotest ® for Measuring Running Stride Kinematics. J. Sports Sci. 2015, 34, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Al-Amri, M.; Nicholas, K.; Button, K.; Sparkes, V.; Sheeran, L.; Davies, J. Inertial Measurement Units for Clinical Movement Analysis: Reliability and Concurrent Validity. Sensors 2018, 18, 719. [Google Scholar] [CrossRef] [PubMed]
- Althouse, D. Effects of IMU Sensor Location and Number on the Validity of Vertical Acceleration Time-Series Data in Countermovement Jumping. All Graduate Plan B and other Reports. 2022. Available online: https://digitalcommons.usu.edu/gradreports/1657/ (accessed on 30 January 2023).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 11 | Mean | SD |
|---|---|---|
| Age (years) | 23.10 | 3.10 |
| Height (m) | 1.73 | 0.05 |
| Body mass (kg) | 64.0 | 7.80 |
| Fat percentage (%) | 17.30 | 2.70 |
| BMI (kg/m2) | 21.30 | 1.90 |
| Training experience (years) | 9.30 | 1.80 |
| Device | Total (cm) | Session 1 (cm) | Session 2 (cm) | Mean Diff. between Sessions (cm) | ES (g) |
|---|---|---|---|---|---|
| Vmaxpro Hip | 27.9 | 27.1 | 27.7 | −0.1 | 0.04 (Trivial) |
| (CI 95%) | (27.1 to 28.65) | (27.2 to 28.6) | (26.9 to 28.5) | (−0.7 to 0.3) | (−0.22 to 0.31) |
| Vmaxpro Ankle | 19.3 | 19.5 | 19.4 | −0.39 | 0.07 (Trivial) |
| (CI 95%) | (18.8 to 19.8) | (18.8 to 20.2) | (18.8 to 19.9) | (−0.9 to 0.1) | (−0.19 to 0.34) |
| Mean diff. between devices (cm) | −8.5 * | −8.4 * | −8.5 * | – | – |
| (CI 95%) | (−8.7 to −8.2) | (−8.8 to −7.9) | (−8.8 to −8.1) | – | – |
| ES (g) | −2.2 (Large) | −2.2 (Large) | −2.2 (Large) | – | – |
| (CI 95%) | (−2.5 to −1.8) | (−2.5 to −1.9) | −2.5 to −1.9) | – | – |
| Hip | Ankle | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 2–1 | 3–2 | 4–3 | 5–4 | Mean | 2–1 | 3–2 | 4–3 | 5–4 | Mean | |
| Mean change (cm) | 0.70 | −0.48 | −0.37 | −0.05 | – | 0.71 | −0.67 | 0.07 | 0.25 | – |
| CI-95% lower | −0.51 | −1.83 | −1.97 | −1.19 | – | 0.05 | −1.74 | −1.21 | −0.37 | – |
| CI-95% upper | 1.91 | 0.87 | 1.23 | 1.09 | – | 1.38 | 0.39 | 1.35 | 0.87 | – |
| ICC | 0.92 | 0.90 | 0.86 | 0.93 | 0.91 | 0.98 | 0.95 | 0.92 | 0.96 | 0.96 |
| CI-95% lower | 0.72 | 0.65 | 0.53 | 0.75 | 0.80 | 0.92 | 0.82 | 0.73 | 0.89 | 0.89 |
| CI-95% upper | 0.98 | 0.97 | 0.96 | 0.98 | 0.97 | 0.99 | 0.99 | 0.98 | 0.99 | 0.99 |
| CCC | 0.89 | 0.88 | 0.83 | 0.92 | 0.88 | 0.96 | 0.92 | 0.89 | 0.97 | 0.93 |
| CI-95% lower | 0.66 | 0.62 | 0.51 | 0.92 | 0.68 | 0.86 | 0.74 | 0.67 | 0.90 | 0.79 |
| CI-95% upper | 0.96 | 0.99 | 0.99 | 0.99 | 0.98 | 0.98 | 0.93 | 0.99 | 0.99 | 0.97 |
| ρ (precision) | 0.91 | 0.89 | 0.83 | 0.84 | 0.90 | 0.97 | 0.93 | 0.91 | 0.97 | 0.95 |
| Cb (accuracy) | 0.98 | 0.99 | 0.97 | 0.99 | 0.99 | 0.98 | 0.99 | 0.98 | 0.99 | 0.98 |
| SEM (cm) | 0.70 | 1.12 | 1.35 | 0.65 | 1.41 | 1.19 | 1.29 | 1.08 | 1.15 | 1.00 |
| CI-95% lower | 0.49 | 0.78 | 0.94 | 0.46 | 1.13 | 0.90 | 0.97 | 0.82 | 0.87 | 0.80 |
| CI-95% upper | 1.22 | 1.97 | 2.37 | 1.14 | 1.88 | 1.80 | 1.95 | 1.64 | 1.74 | 1.33 |
| SEMstd | 0.32 | 0.36 | 0.44 | 0.29 | 0.34 | 0.17 | 0.27 | 0.34 | 0.17 | 0.24 |
| CI-95% lower | 0.23 | 0.25 | 0.31 | 0.20 | 0.27 | 0.12 | 0.19 | 0.24 | 0.12 | 0.19 |
| CI-95% upper | 0.57 | 0.63 | 0.77 | 0.51 | 0.45 | 0.30 | 0.47 | 0.59 | 0.29 | 0.32 |
| CV (%) | 4.64 | 5.04 | 6.08 | 4.64 | 5.10 | 3.63 | 5.62 | 7.00 | 3.63 | 5.13 |
| SWC (cm) | 0.36 | 0.40 | 0.48 | 0.34 | 0.40 | 0.20 | 0.32 | 0.38 | 0.18 | 0.28 |
| CI-95% lower | 0.25 | 0.28 | 0.33 | 0.24 | 0.32 | 0.14 | 0.22 | 0.27 | 0.13 | 0.23 |
| CI-95% upper | 0.63 | 0.71 | 0.84 | 0.60 | 0.53 | 0.35 | 0.56 | 0.67 | 0.32 | 0.38 |
| Ankle vs. Hip Devices | 95% CI | |
|---|---|---|
| Paired differences (cm) | −8.50 * | −8.7 to −8.2 |
| ES (paired) | −2.2 | −2.5 to −1.8 |
| ICC | 0.77 | 0.74 to 0.82 |
| CCC | 0.25 | 0.21 to 0.29 |
| ρ (precision) | 0.87 | – |
| Cb (accuracy) | 0.29 | – |
| SEM (cm) | 1.47 | 1.33 to 1.66 |
| SEMstd | 0.39 | 0.35 to 0.44 |
| CVhip (%) | 14.5 | – |
| CVankle (%) | 19.2 | – |
| SWC (cm) | 0.42 | 0.37 to 0.47 |
| SNR | 0.28 | 0.26 to 0.30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villalon-Gasch, L.; Jimenez-Olmedo, J.M.; Olaya-Cuartero, J.; Pueo, B. Test–Retest and Between–Device Reliability of Vmaxpro IMU at Hip and Ankle for Vertical Jump Measurement. Sensors 2023, 23, 2068. https://doi.org/10.3390/s23042068
Villalon-Gasch L, Jimenez-Olmedo JM, Olaya-Cuartero J, Pueo B. Test–Retest and Between–Device Reliability of Vmaxpro IMU at Hip and Ankle for Vertical Jump Measurement. Sensors. 2023; 23(4):2068. https://doi.org/10.3390/s23042068
Chicago/Turabian StyleVillalon-Gasch, Lamberto, Jose M. Jimenez-Olmedo, Javier Olaya-Cuartero, and Basilio Pueo. 2023. "Test–Retest and Between–Device Reliability of Vmaxpro IMU at Hip and Ankle for Vertical Jump Measurement" Sensors 23, no. 4: 2068. https://doi.org/10.3390/s23042068
APA StyleVillalon-Gasch, L., Jimenez-Olmedo, J. M., Olaya-Cuartero, J., & Pueo, B. (2023). Test–Retest and Between–Device Reliability of Vmaxpro IMU at Hip and Ankle for Vertical Jump Measurement. Sensors, 23(4), 2068. https://doi.org/10.3390/s23042068