



Unobstructive Heartbeat Monitoring of Sleeping Infants and Young Children Using Sheet-Type PVDF Sensors

Abstract
:1. Introduction
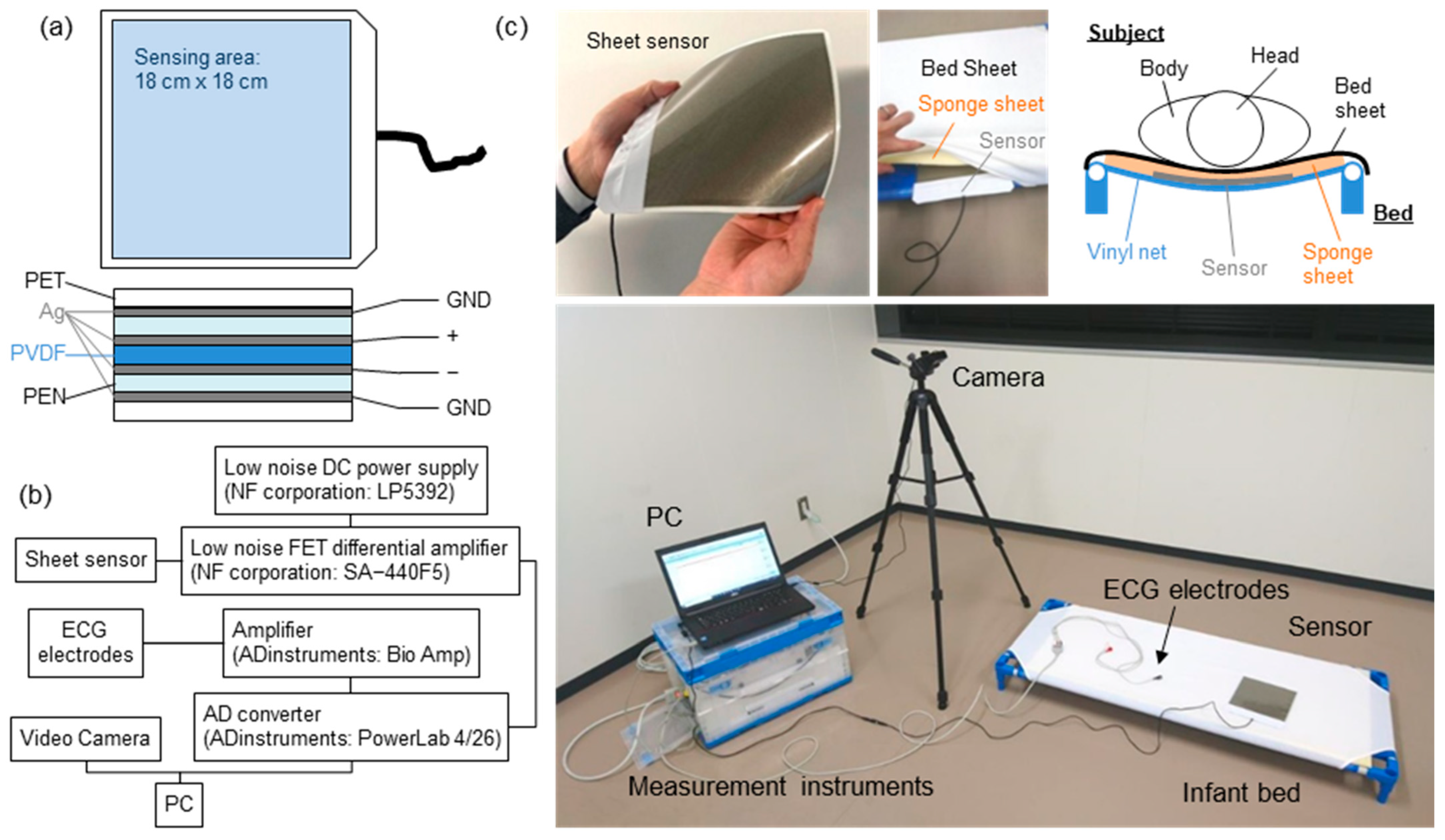
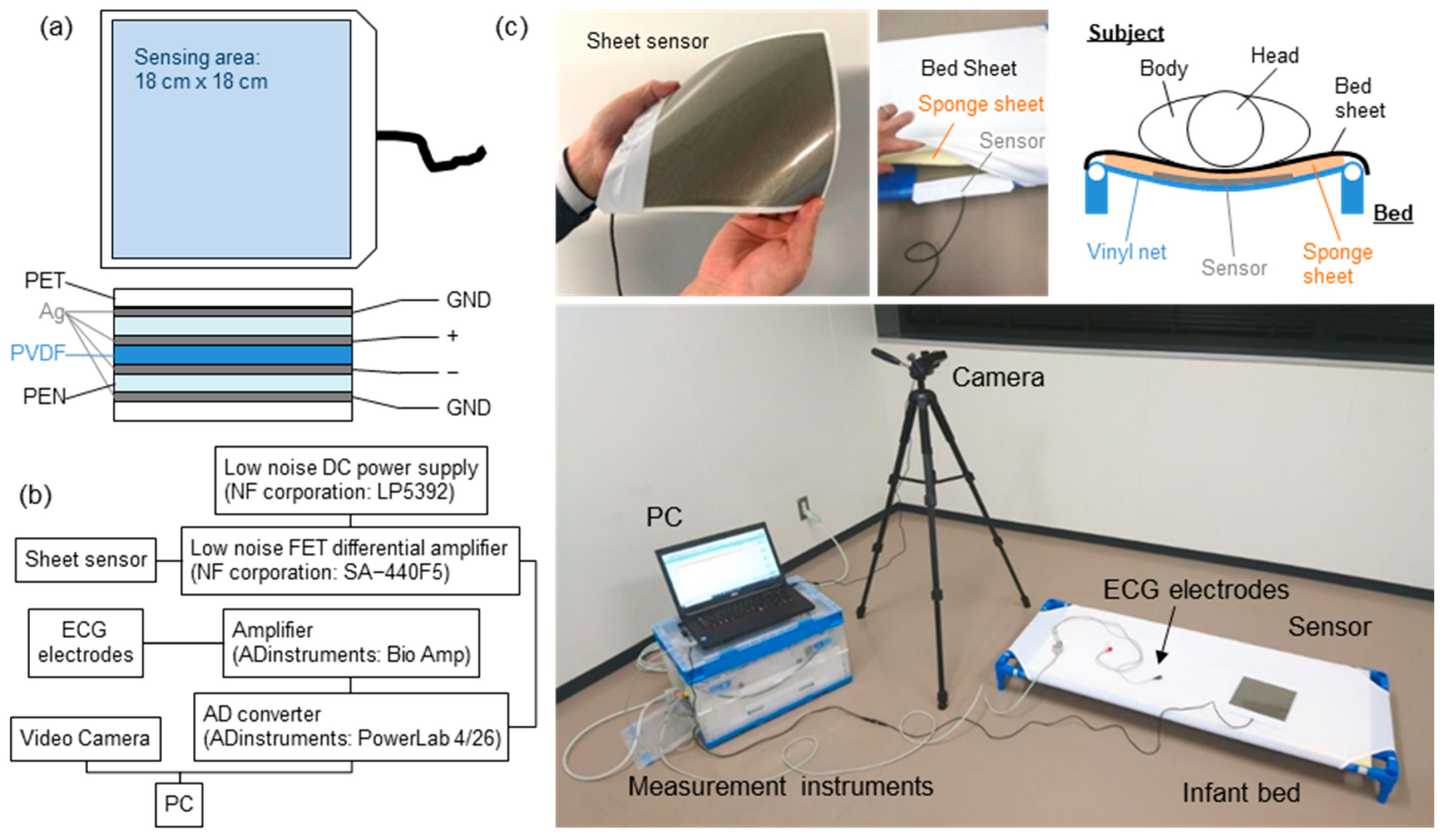
2. Materials and Methods
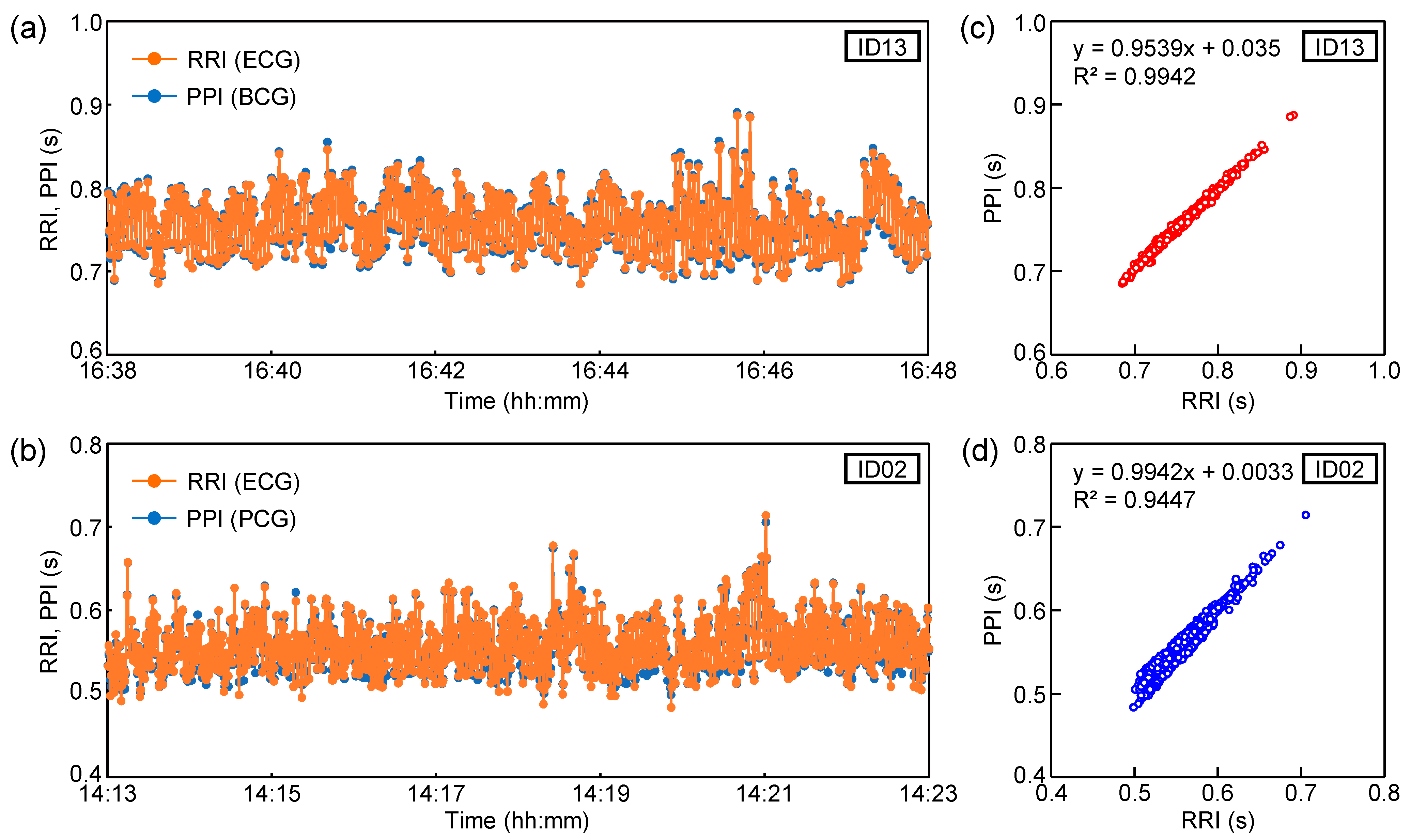
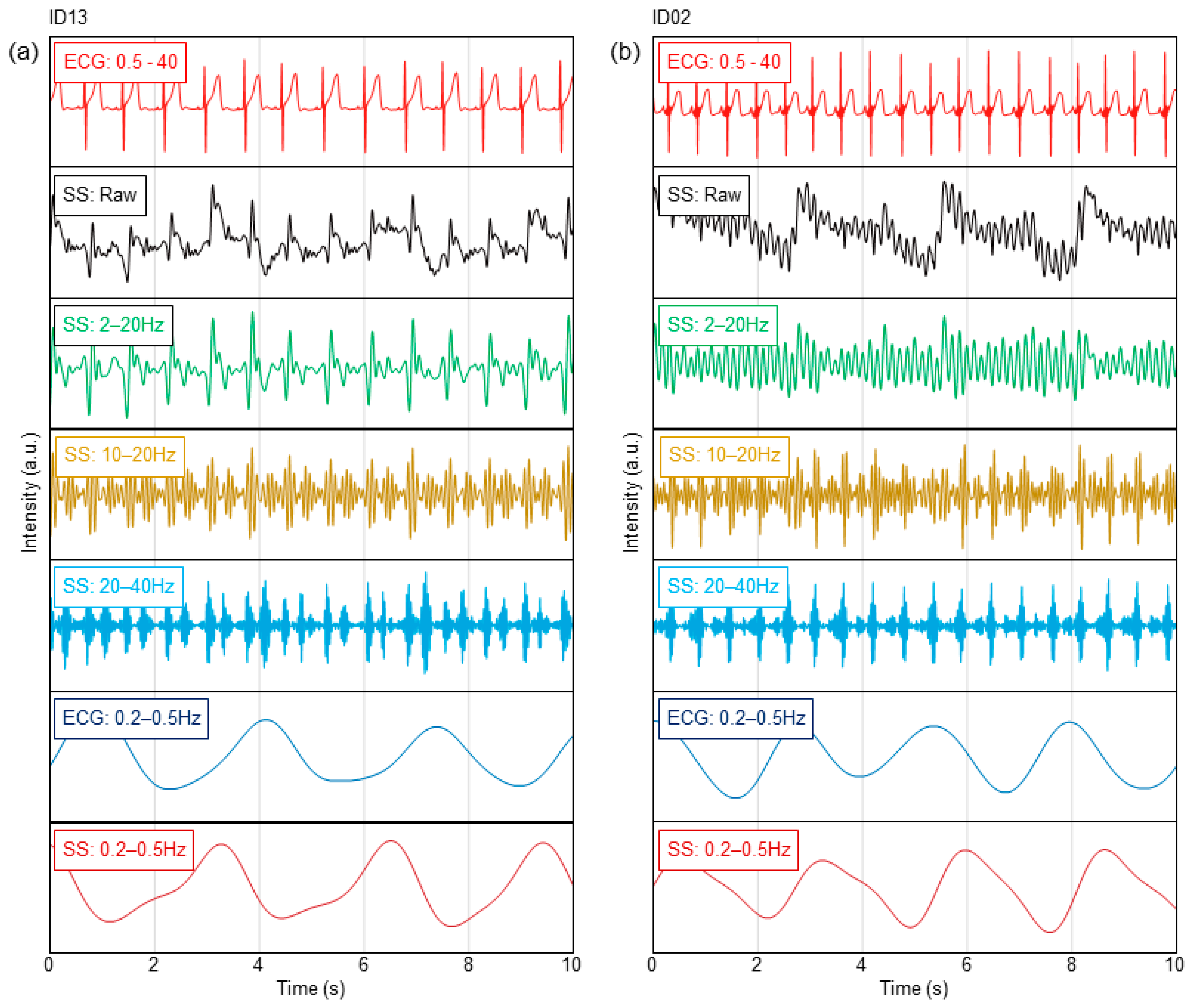
3. Results and Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rajala, S.; Lekkala, J. Film-type sensor materials PVDF and EMFi in measurement of cardiorespiratory signal—A review. IEEE Sens. J. 2012, 12, 439. [Google Scholar] [CrossRef]
- Ian, O.T.; Migeotte, P.-F.; Park, K.-S.; Etemadi, M.; Tavakolian, K.; Casanella, R.; Zanetti, J.; Tank, J.; Funtova, I.; Prisk, G.K.; et al. Ballistocardiography and seismocardiography: A review of recent advances. IEEE J. Biomed. Health Informat. 2015, 19, 1414. [Google Scholar]
- Sadek, I.; Biswas, J.; Abdulrazak, B. Ballistocardiogram signal processing: A review. Health Inf. Sci. Syst. 2019, 7, 10. [Google Scholar] [CrossRef] [PubMed]
- Saima, G.A.; Tassawar, I.; Anam, J.; Ehsan, U.M.; Nasira, K.; Sana, U.J.; Naeem, R. Sensing and Artificial Intelligent Maternal-Infant Health Care Systems: A Review. Sensors 2022, 22, 4362. [Google Scholar]
- Zheng, P.; Deedee, K.; Rong-Hao, L.; Xi, L.; Ward, C.; Hendrik, N.; Peter, A.; Carola, v.P. Continuous sensing and quantification of body motion in infants: A systematic review. Heliyon 2023, 9, e18234. [Google Scholar]
- Chow, P.; Nagendra, G.; Abisheganaden, J.; Wang, Y.T. A Novel approach to respiratory monitoring using an air-mattress system. Physiol. Meas. 2000, 21, 345. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Watanabe, T.; Watanabe, H.; Ando, H.; Ishikawa, T.; Kobayashi, K. Noninvasive measurement of heartbeat, respiration, snoring and body movements of a subject in bed via a pneumatic method. IEEE Trans. Biomed. Eng. 2006, 52, 2100. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-L.; Sun, Z.-T.; Chen, Y.-Y. Air-mattress system for ballistocardiogram-based heart rate and breathing rate estimation. Heliyon 2023, 9, e12717. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zhu, X.; Nemoto, T.; Kanemitsu, Y.; Kitamura, K.; Yamakoshi, K. Unconstrained detection of respiration rhythm and pulse rate with one under-pillow sensor during sleep. Med. Biol. Eng. Comput. 2005, 43, 306. [Google Scholar] [CrossRef]
- Abbas, A.K.; Heimann, K.; Jergus, K.; Orlikowsky, T.; Leonhardt, S. Neonatal non-contact respiratory monitoring based on real-time infrared thermography. Biomed. Eng. Online 2011, 10, 93. [Google Scholar] [CrossRef]
- Villarroel, M.; Chaichulee, S.; Jorge, J.; Davis, S.; Green, G.; Arteta, C.; Zisserman, A.; McCormick, K.; Watkinson, P.; Tarassenko, L. Non-contact physiological monitoring of preterm infants in the neonatal intensive care unit. npj Digit. Med. 2019, 2, 128. [Google Scholar] [CrossRef] [PubMed]
- Hagiyama, N.; Hirano, H.; Mito, A.; Soh, Z.; Fujita, E.; Ogura, Y.; Kaneko, S.; Nakamura, R.; Saeki, N.; Kawamoto, M.; et al. Unconstrained vital sign monitoring system using an aortic pulse wave sensor. Sci. Rep. 2020, 9, 17475. [Google Scholar] [CrossRef] [PubMed]
- Brink, M.; Muller, C.; Schierz, C. Contact-free measurement of heart rate, respiration rate, and body movements during sleep. Behav. Res. Methods. 2006, 38, 511. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.G.; Hong, K.H.; Kim, K.K.; Shin, J.H.; Lee, S.M.; Chung, G.S.; Beak, H.J.; Jeong, D.-U.; Park, K.S. Monitoring physiological signals using nonintrusive sensors installed in daily life equipment. Biomed. Eng. Lett. 2011, 1, 11. [Google Scholar] [CrossRef]
- Clapers, J.G.; Rocamora, A.S.; Casanella, R.; Areny, R.P. Towards the standardization of ballistocardiography systems for J-peak timing measurement. Measurement 2014, 58, 310. [Google Scholar] [CrossRef]
- Matsuo, K.; Mukai, T.; Guo, S. Unconstrained measurement of heart rate considering harmonics of respiratory signal using flexible tactile sensor sheet. J. Robot. Mechatron. 2021, 33, 826. [Google Scholar] [CrossRef]
- Nakamura, S.; Kamiyama, N.; Arita, Y.; Nakamura, T. Capacitively coupled electrode array sensors for body posture and ECG measurement during sleep. IEEE Access 2021, 9, 24363. [Google Scholar] [CrossRef]
- Wang, F.; Tanaka, M.; Chonan, S. Development of a PVDF piezopolymer sensor for unconstrained in-sleep cardiorespiratory monitoring. J. Intell. Mater. Syst. Struct. 2003, 14, 185. [Google Scholar] [CrossRef]
- Alamets, J.; Rauhala, E.; Huupponena, E.; Saastamoinen, A.; Varri, A.; Joutsen, A.; Hasan, J.; Himanenc, S.-L. Automatic detection of spiking events in EMFi sheet during sleep. Med. Eng. Phys. 2006, 28, 267. [Google Scholar] [CrossRef]
- Jingda, F.; Huang, W.; Jin, J.; Yanlei, W.; Xiang, Z.; Qijie, L.; Xuejun, J. Non-invasive monitoring of cardiac function through Ballistocardiogram: An algorithm integrating short-time Fourier transform and ensemble empirical mode decomposition. Front. Physiol. 2023, 14, 1201722. [Google Scholar]
- Niizeki, K.; Nishidate, I.; Uchida, K.; Kuwahara, M. Unconstrained cardiorespiratory and body movement monitoring system for home care. Med. Biol. Eng. Comput. 2005, 43, 716. [Google Scholar] [CrossRef]
- Karki, S.; Lekkala, J. Film-type transducer materials PVDF and EMFi in the measurement of heart and respiration rates. Annu. Int. Conf. Eng. Med. Biol. Soc. EMBS 2008, 2008, 530–533. [Google Scholar]
- Uchida, S.; Endo, T.; Suenaga, K.; Iwami, H.; Inoue, S.; Fujioka, E.; Imamura, A.; Atsumi, T.; Inagaki, Y.; Kamei, A. Sleep evaluation by a newly developed PVDF sensor non-contact sheet: A comparison with standard polysomnography and wrist actigraphy. Sleep Biol. Rhythm. 2011, 9, 178. [Google Scholar] [CrossRef]
- Vehkaoja, A.; Kontunen, A.; Lekkala, J. Effects of sensor type and sensor location on signal quality in bed mounted ballistocardiographic heart rate and respiration monitoring. Annu. Int. Conf. Eng. Med. Biol. Soc. EMBS 2015, 2015, 4383–4386. [Google Scholar]
- Xu, J.; Wang, Y.; Li, B.; Bian, L. Vital signs monitoring system based on piezoelectric film sensors. J. Phys. Conf. Ser. 2020, 1633, 012137. [Google Scholar] [CrossRef]
- Parchani, G.; Kumar, G.; Rao, R.; Udupa, K.; Saran, V. Efficacy of non-contact ballistocardiography system to determine heart rate variability. Ann. Neurosci. 2022, 29, 16. [Google Scholar] [CrossRef] [PubMed]
- Fang, F.J.; Yihan, Z.; Tianyi, L.; Yanbing, Z.; Ziyu, Z. Recent Research for Unobtrusive Atrial Fibrillation Detection Methods Based on Cardiac Dynamics Signals: A Survey. Sensors 2021, 21, 3814. [Google Scholar]
- Gang, S.; Ruidong, D.; Mingqi, Y.; Dan, H.; Biyong, Z. An elastic manifold learning approach to beat-to-beat interval estimation with ballistocardiography signals. Adv. Eng. Inform. 2020, 44, 101051. [Google Scholar]
- Wanga, F.; Zoub, Y.; Tanaka, M.; Matsuda, T.; Chonan, S. Unconstrained cardiorespiratory monitor for premature infants. Int. J. Appl. Electromagn. Mech. 2007, 25, 469. [Google Scholar] [CrossRef]
- Rajala, S.; Lekkala, J. Infant respiration and heart rate monitoring with EMFI sensor. In Proceedings of the XXI IMEKO World Congress “Measurement in Research and Industry”, Prague, Czech Republic, 30 August–4 September 2015. [Google Scholar]
- Lee, W.K.; Yoon, H.; Han, C.; Joo, K.M.; Park, K.S. Physiological signal monitoring bed for infants based on load-cell sensors. Sensors 2016, 16, 409. [Google Scholar] [CrossRef]
- Joshi, R.; Bierling, B.L.; Long, X.; Weijers, J.; Feijs, L.; Pul, C.V.; Andriessen, P. A ballistographic approach for continuous and non-obtrusive monitoring of movement in neonotes. IEEE J. Transl. Eng. Health Med. 2018, 6, 2700809. [Google Scholar] [CrossRef]
- Bifulco, P.; Gargiulo, G.; Angelo, G.; Liccardo, A.; Romano, M.; Clemente, F.; Cesarelli, M. Monitoring of respiration, seismocardiogram and heart sounds by a PVDF piezo film sensor. In Proceedings of the 20th IMEKO TC4 Symposium on Measurements of Electrical Quantities, Benevento, Italy, 15–17 September 2014; p. 786. [Google Scholar]
- Lee, W.K.; Chung, G.S.; Beak, H.J.; Park, K.S. Heart sounds measurement using PVDF film sensor and their comparison with RR intervals of ECG signals. In Proceedings of the 2012 IEEE-EMBS International Conference on Biomedical and Health Informatics, Hong Kong, China, 5–7 January 2012; pp. 864–866. [Google Scholar]
- Niccolò, M.; Federico, C.; Guido, M.; Paolo, C. A Unified Methodology for Heartbeats Detection in Seismocardiogram and Ballistocardiogram Signals. Computers 2020, 9, 41. [Google Scholar]
- Paniz, B.; Jeremy, R.; Amin, H.; Cyril, T.; Olivier, D.; Philippe, V.D.B. Investigating Cardiorespiratory Interaction Using Ballistocardiography and Seismocardiography—A Narrative Review. Sensors 2022, 22, 9565. [Google Scholar]
- Jiena, H.; Yitao, Z.; Shaolong, Z.; Xingguang, G.; Yunfeng, W.; Chuanglu, C.; Haiying, Z. Respiration Signal Extraction from Pulse Wave Collected by PVDF Sensor. IEEE Access. 2020, 8, 149878. [Google Scholar]
- Kim, C.-S.; Ober, S.L.; McMurtry, M.S.; Finegan, B.A.; Inan, O.T.; Mukkamala, R.; Hahn, J.-O. Ballistocardiogram: Mechanism and potential for unobtrusive cardiovascular health monitoring. Sci. Rep. 2015, 6, 31297. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject No. | Gender | Age/Months | Height (cm) | Weight (kg) | ECG | Awakening | Measurement Duration (min) |
|---|---|---|---|---|---|---|---|
| ID01 | Male | 0/7 | 68 | 7.6 | With | Spontaneously | 33 |
| ID02 | Male | 0/11 | - | 7.9 | With | Spontaneously | 29 |
| ID03 | Female | 0/11 | 62.2 | 8.5 | Without | Spontaneously | 19 |
| ID04 | Male | 1/8 | 84 | 13 | With | Forced | 31 |
| ID05 | Male | 0/11 | 70 | 9 | Without | Forced | 64 |
| ID06 | Female | 2/6 | 96 | 12.5 | Without | Forced | 68 |
| ID07 | Female | 0/7 | - | 7 | Without | Spontaneously | 54 |
| ID08 | Female | 4/11 | 105 | 17.5 | Without | Forced | 65 |
| ID09 | Male | 3/3 | 95 | 15.7 | With | Forced | 53 |
| ID10 | Male | 0/10 | 75 | 10 | Without | Spontaneously | 22 |
| ID11 | Female | 1/2 | 72 | 10.5 | With | Forced | 35 |
| ID12 | Female | 1/6 | 77 | 9.5 | With | Spontaneously | 31 |
| ID13 | Female | 5/8 | 104 | 16 | With | Forced | 56 |
| ID14 | Female | 3/2 | 96 | 14.5 | With | Forced | 52 |
| ID15 | Male | 0/11 | 72.8 | 9.2 | With | Spontaneously | 29 |
| ID16 | Male | 5/2 | 110 | 19 | Without | Spontaneously | 34 |
| ID17 | Female | 0/5 | 65 | 6.7 | With | Spontaneously | 22 |
| ID18 | Female | 1/7 | - | 8.2 | With | Forced | 58 |
| ID19 | Male | 3/11 | 93.7 | 13 | With | Forced | 60 |
| ID20 | Female | 0/8 | 67 | 8.9 | With | Forced | 24 |
| ID21 | Male | 0/3 | 57 | 4.7 | With | Spontaneously | 7 |
| ID22 | Male | 1/10 | 78 | 9.6 | With | Forced | 42 |
| ID23 | Female | 1/8 | 84.4 | 10 | With | Spontaneously | 54 |
| ID24 | Male | 0/9 | 71 | 8.7 | With | Spontaneously | 28 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumaki, D.; Motoshima, Y.; Higuchi, F.; Sato, K.; Sekine, T.; Tokito, S. Unobstructive Heartbeat Monitoring of Sleeping Infants and Young Children Using Sheet-Type PVDF Sensors. Sensors 2023, 23, 9252. https://doi.org/10.3390/s23229252
Kumaki D, Motoshima Y, Higuchi F, Sato K, Sekine T, Tokito S. Unobstructive Heartbeat Monitoring of Sleeping Infants and Young Children Using Sheet-Type PVDF Sensors. Sensors. 2023; 23(22):9252. https://doi.org/10.3390/s23229252
Chicago/Turabian StyleKumaki, Daisuke, Yuko Motoshima, Fujio Higuchi, Katsuhiro Sato, Tomohito Sekine, and Shizuo Tokito. 2023. "Unobstructive Heartbeat Monitoring of Sleeping Infants and Young Children Using Sheet-Type PVDF Sensors" Sensors 23, no. 22: 9252. https://doi.org/10.3390/s23229252
APA StyleKumaki, D., Motoshima, Y., Higuchi, F., Sato, K., Sekine, T., & Tokito, S. (2023). Unobstructive Heartbeat Monitoring of Sleeping Infants and Young Children Using Sheet-Type PVDF Sensors. Sensors, 23(22), 9252. https://doi.org/10.3390/s23229252