
Infrared Thermography for Real-Time Assessment of the Effectiveness of Scoliosis Braces

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Background
3. Proposal
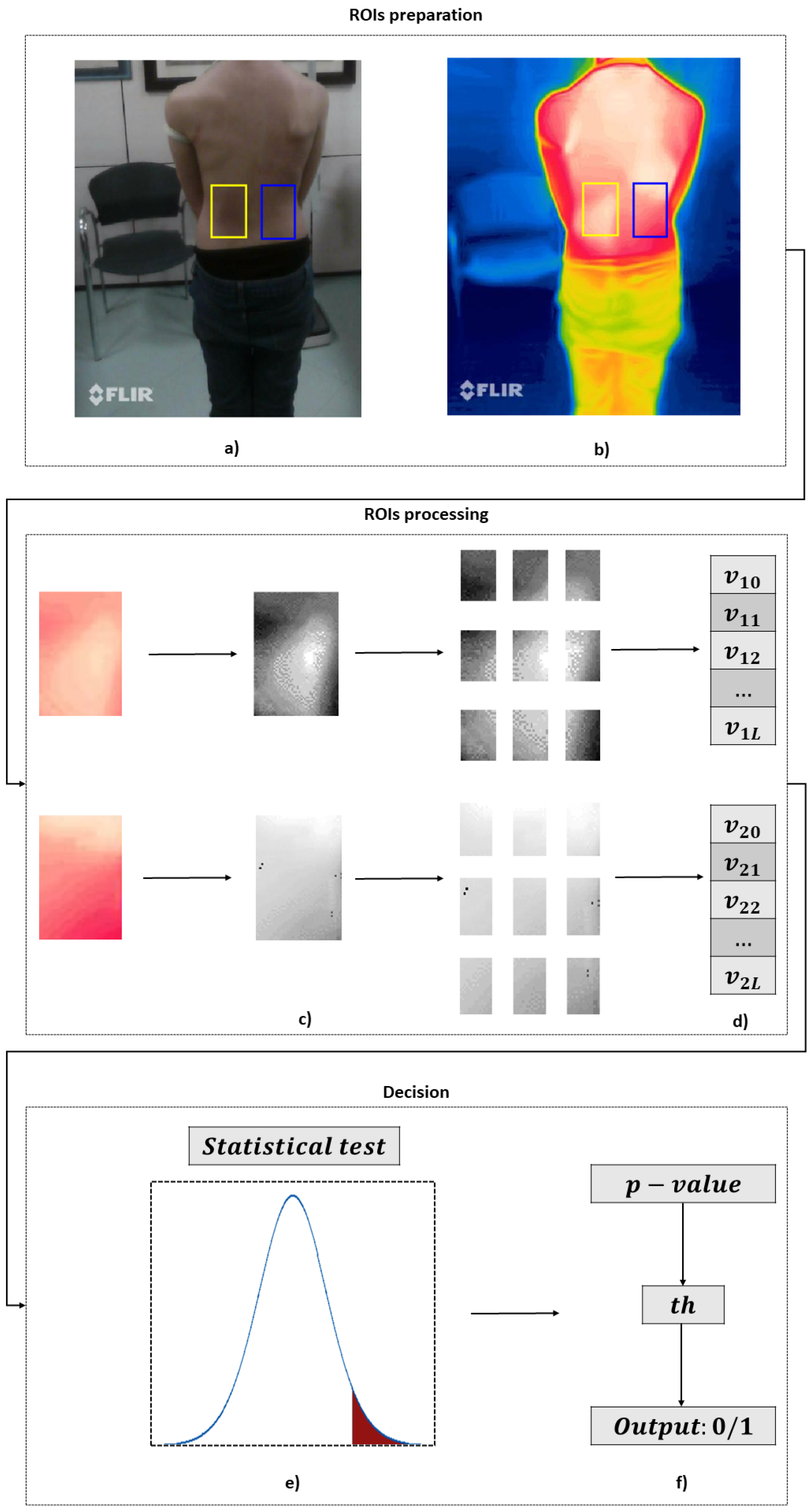
- The ROIs preparation module consists of three blocks.The first block, named Images Acquisition, captures the thermal and corresponding RGB images from the dorsum of the patient, immediately after removing the brace. It is noteworthy that the patient’s dorsum remains uncovered during this stage. To ensure that the bracing effect remains visible, it is recommended to wait no more than one minute between the patient removing the scoliosis corset and the start of image capturing. In fact, the duration of the corset’s pressure effect on skin temperature variation after its removal can be influenced by several factors, such as the duration of brace usage, the intensity of the applied pressure, the patient’s metabolism, sweating, and the ambient temperature. This effect may gradually dissipate within a few minutes or persist for an extended period ranging from several minutes to tens of minutes [49,50]. Hence, a waiting time of less than one minute can be considered a time to ensure adequate stability in the short term.In the second block, referred to as the Selection of the ROIs, the orthopedic specialist selects on his/her computer (with the help of cursors) two ROIs on the acquired RGB image: the first ROI corresponds to the area in which the thrust is exerted by the brace, whereas the second ROI is selected symmetrically to the first ROI with respect to the backbone. It should be pointed out that this selection is guided by the patient’s clinical history: the orthopedic specialist has access to the patient’s radiography, has knowledge of the diagnosis, knows the type of corset worn, and has the related prescription. As a result, he/she possesses the necessary information to identify the specific region of the back where the corset needs to exert its effect. Nevertheless, to avoid confirmation bias, the selection of the ROIs is not performed directly on the thermal image but rather on the RGB one.Finally, the third block (Mapping) is responsible for mapping the selected regions from the RGB image onto the thermal image.
- The ROIs processing module is divided into three blocks.The first block, named Grayscale Conversion, handles the conversion of the thermal ROIs from the RGB color space to grayscale, where white is associated with the maximum temperature value and black is associated with the minimum temperature value. Consequently, each ROI undergoes a transformation from three dimensions (red, green, and blue channels) to one dimension (grayscale) to save computational effort.Then, in the ROIs Partitioning block, each ROI converted to grayscale is divided by performing both horizontal and vertical slicing. As a result, each ROI is segmented into subregions, where N represents the number of horizontal slices and M represents the number of vertical slices.In this way, the last block, called Partitions Averaging, performs an average assessment on each of the subregions within the partitioned grayscale ROIs. This process generates two vectors, each with dimensions [, 1], corresponding to the averaged values of the temperature of each ROI subregion.
- These two vectors are compared through the Decision module.In particular, a Statistical Test is performed between the two vectors to evaluate whether there is a statistically significant difference between the means of the two groups represented by the vectors. The output of this test is the p-value, which indicates the probability of obtaining test results at least as extreme as the result actually observed, under the assumption that the null hypothesis is correct. In this context, the null hypothesis implies no significant difference between the two vectors, suggesting inadequate scoliosis brace pressure. For this reason, the lower the p-value, the lower the probability of erroneously rejecting the null hypothesis. The utilization of a statistically derived score affords independence from absolute temperature (and consequently, pressure) values measured on the patient’s back, which significantly vary among different patients and corsets, given the anatomical distinctions inherent to each individual. As a matter of fact, typical pressure values range from 7 to 10 kPa [51], but these values are subject to significant variability, both inter-subject and intra-subject.The resulting p-value is compared with a Threshold to associate it with an Output that can indicate whether the scoliosis brace is functioning adequately. More specifically, if the obtained p-value is found to be lower than the threshold value, and if the average temperature of ROI #1 (region where brace pressure is assumed to be) is greater than that of ROI #2 (region where brace pressure is not assumed to be), the pressure of the scoliosis corset is indicated as adequate. Conversely, if the p-value exceeds the threshold value, it is indicated as inadequate. The identification of this threshold can follow an a priori model, which is based on prior information, or models based on learning from newly acquired data.
4. Experimental Validation
4.1. Experimental Setup
4.2. Experimental Study
4.3. Performance Evaluation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Trobisch, P.; Suess, O.; Schwab, F. Idiopathic scoliosis. Dtsch. Ärztebl. Int. 2010, 107, 875. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Aulisa, A.G.; Cerny, P.; de Mauroy, J.C.; McAviney, J.; Mills, A.; Donzelli, S.; Grivas, T.B.; Hresko, M.T.; Kotwicki, T.; et al. The classification of scoliosis braces developed by SOSORT with SRS, ISPO, and POSNA and approved by ESPRM. Eur. Spine J. 2022, 31, 980–989. [Google Scholar] [CrossRef] [PubMed]
- Janicki, J.A.; Alman, B. Scoliosis: Review of diagnosis and treatment. Paediatr. Child Health 2007, 12, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Zaina, F.; De Mauroy, J.; Grivas, T.; Hresko, M.; Kotwizki, T.; Maruyama, T.; Price, N.; Rigo, M.; Stikeleather, L.; Wynne, J.; et al. Bracing for scoliosis in 2014: State of the art. Eur. J. Phys. Rehabil. Med. 2014, 50, 93–110. [Google Scholar] [PubMed]
- Carman, D.; Browne, R.; Birch, J. Measurement of scoliosis and kyphosis radiographs. Intraobserver and interobserver variation. JBJS 1990, 72, 328–333. [Google Scholar] [CrossRef]
- Horng, M.H.; Kuok, C.P.; Fu, M.J.; Lin, C.J.; Sun, Y.N. Cobb angle measurement of spine from X-ray images using convolutional neural network. Comput. Math. Methods Med. 2019, 2019, 6357171. [Google Scholar] [CrossRef]
- Weinstein, S.L.; Dolan, L.A.; Cheng, J.C.; Danielsson, A.; Morcuende, J.A. Adolescent idiopathic scoliosis. Lancet 2008, 371, 1527–1537. [Google Scholar] [CrossRef]
- Rigo, M.D.; Villagrasa, M.; Gallo, D. A specific scoliosis classification correlating with brace treatment: Description and reliability. Scoliosis 2010, 5, 1. [Google Scholar] [CrossRef]
- Tsiligiannis, T.; Grivas, T. Pulmonary function in children with idiopathic scoliosis. Scoliosis 2012, 7, 7. [Google Scholar] [CrossRef]
- Bignardi, C. Usefulness of Measuring the Pressure Exerted by Orthopedic Braces. Int. J. Eng. Res. Technol. 2019, 12, 2903–2909. [Google Scholar]
- Negrini, S.; Donzelli, S.; Aulisa, A.G.; Czaprowski, D.; Schreiber, S.; de Mauroy, J.C.; Diers, H.; Grivas, T.B.; Knott, P.; Kotwicki, T.; et al. 2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018, 13, 1–48. [Google Scholar] [CrossRef] [PubMed]
- Richards, B.S.; Bernstein, R.M.; D’Amato, C.R.; Thompson, G.H. Standardization of criteria for adolescent idiopathic scoliosis brace studies: SRS Committee on Bracing and Nonoperative Management. Spine 2005, 30, 2068–2075. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Di Felice, F.; Negrini, F.; Rebagliati, G.; Zaina, F.; Donzelli, S. Predicting final results of brace treatment of adolescents with idiopathic scoliosis: First out-of-brace radiograph is better than in-brace radiograph—SOSORT 2020 award winner. Eur. Spine J. 2022, 31, 3519–3526. [Google Scholar] [CrossRef] [PubMed]
- Grazioso, S.; Selvaggio, M.; Di Gironimo, G.; Ruggiero, R. INBODY: Instant Photogrammetric 3D Body Scanner. In Proceedings of the 7th International Conference on 3D Body Scanning Technologies, Lugano, Switzerland, 30 November–1 December 2016; pp. 296–301. [Google Scholar]
- Negrini, S.; Grivas, T.B.; Kotwicki, T.; Rigo, M.; Zaina, F.; International Society on Scoliosis Orthopaedic and Rehabilitation Treatment. Guidelines on “Standards of management of idiopathic scoliosis with corrective braces in everyday clinics and in clinical research”: SOSORT Consensus 2008. Scoliosis 2009, 4, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Knott, P.; Pappo, E.; Cameron, M.; deMauroy, J.C.; Rivard, C.; Kotwicki, T.; Zaina, F.; Wynne, J.; Stikeleather, L.; Bettany-Saltikov, J.; et al. SOSORT 2012 consensus paper: Reducing x-ray exposure in pediatric patients with scoliosis. Scoliosis 2014, 9, 4. [Google Scholar] [CrossRef]
- Daruwalla, J.; Balasubramaniam, P. Moiré topography in scoliosis. Its accuracy in detecting the site and size of the curve. J. Bone Jt. Surg. Br. Vol. 1985, 67, 211–213. [Google Scholar] [CrossRef]
- Sudo, H.; Kokabu, T.; Abe, Y.; Iwata, A.; Yamada, K.; Ito, Y.M.; Iwasaki, N.; Kanai, S. Automated noninvasive detection of idiopathic scoliosis in children and adolescents: A principle validation study. Sci. Rep. 2018, 8, 17714. [Google Scholar] [CrossRef]
- Gaussorgues, G.; Chomet, S. Infrared Thermography; Springer Science & Business Media: Berlin/Heidelberg, Germany, 1993; Volume 5. [Google Scholar]
- Meola, C.; Carlomagno, G.M. Recent advances in the use of infrared thermography. Meas. Sci. Technol. 2004, 15, R27. [Google Scholar] [CrossRef]
- Bernard, V.; Staffa, E.; Mornstein, V.; Bourek, A. Infrared camera assessment of skin surface temperature—Effect of emissivity. Phys. Medica 2013, 29, 583–591. [Google Scholar] [CrossRef]
- Jones, B.F.; Plassmann, P. Digital infrared thermal imaging of human skin. IEEE Eng. Med. Biol. Mag. 2002, 21, 41–48. [Google Scholar] [CrossRef]
- Osornio-Rios, R.A.; Antonino-Daviu, J.A.; de Jesus Romero-Troncoso, R. Recent industrial applications of infrared thermography: A review. IEEE Trans. Ind. Inf. 2018, 15, 615–625. [Google Scholar] [CrossRef]
- Chrysochoos, A. Infrared thermography applied to the analysis of material behavior: A brief overview. Quant. InfraRed Thermogr. J. 2012, 9, 193–208. [Google Scholar] [CrossRef]
- Ishimwe, R.; Abutaleb, K.; Ahmed, F. Applications of thermal imaging in agriculture—A review. Adv. Remote Sens. 2014, 3, 128. [Google Scholar] [CrossRef]
- Rekant, S.I.; Lyons, M.A.; Pacheco, J.M.; Arzt, J.; Rodriguez, L.L. Veterinary applications of infrared thermography. Am. J. Vet. Res. 2016, 77, 98–107. [Google Scholar] [CrossRef] [PubMed]
- McBride, A.; Bargmann, S.; Pond, D.; Limbert, G. Thermoelastic modelling of the skin at finite deformations. J. Therm. Biol. 2016, 62, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Faust, O.; Acharya, U.R.; Ng, E.; Hong, T.J.; Yu, W. Application of infrared thermography in computer aided diagnosis. Infrared Phys. Technol. 2014, 66, 160–175. [Google Scholar] [CrossRef]
- Angrisani, L.; Arpaia, P.; De Benedetto, E.; Duraccio, L.; Lo Regio, F.; Tedesco, A. Wearable Brain-Computer Interfaces based on Steady-State Visually Evoked Potentials and Augmented Reality: A Review. IEEE Sens. J. 2023, 23, 16501–16514. [Google Scholar] [CrossRef]
- Georgios, L.; Kerstin, S.; Theofylaktos, A. Internet of things in the context of industry 4.0: An overview. Int. J. Entrep. Knowl. 2019, 7, 4–19. [Google Scholar]
- Hayashi, S.; Kawanishi, K.; Ujike, I.; Chun, P.J. Development of Cloud Computing System for Concrete Structure Inspection by Deep Learning Based Infrared Thermography Method. In Proceedings of the ISARC 2020, International Symposium on Automation and Robotics in Construction, Kitakyshu, Japan, 27–28 October 2020; IAARC Publications: Lille, France, 2020; Volume 37, pp. 927–934. [Google Scholar]
- Papež, B.J.; Palfy, M.; Turk, Z. Infrared thermography based on artificial intelligence for carpal tunnel syndrome diagnosis. J. Int. Med. Res. 2008, 36, 1363–1370. [Google Scholar] [CrossRef]
- Apicella, A.; Arpaia, P.; De Benedetto, E.; Donato, N.; Duraccio, L.; Giugliano, S.; Prevete, R. Employment of Domain Adaptation techniques in SSVEP-based Brain-Computer Interfaces. IEEE Access 2023, 11, 36147–36157. [Google Scholar] [CrossRef]
- Germi, J.; Mensah-Brown, K.; Chen, H.; Schuster, J. Use of smartphone-integrated infrared thermography to monitor sympathetic dysfunction as a surgical complication. Interdiscip. Neurosurg. 2022, 28, 101475. [Google Scholar] [CrossRef]
- Romanò, C.; Logoluso, N.; Dell’Oro, F.; Elia, A.; Drago, L. Telethermographic findings after uncomplicated and septic total knee replacement. Knee 2012, 19, 193–197. [Google Scholar] [CrossRef]
- Kawali, A.A. Thermography in ocular inflammation. Indian J. Radiol. Imaging 2013, 23, 281–283. [Google Scholar] [CrossRef]
- Scheidt, S.; Rüwald, J.; Schildberg, F.A.; Mahlein, A.K.; Seuser, A.; Wirtz, D.C.; Jacobs, C. A systematic review on the value of infrared thermography in the early detection of periprosthetic joint infections. Z. Orthop. Unf. 2020, 158, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Park, D.; Kim, B.H.; Lee, S.E.; Kim, D.Y.; Eom, Y.S.; Cho, J.M.; Yang, J.W.; Kim, M.; Kwon, H.D.; Lee, J.W. Application of digital infrared thermography for carpal tunnel syndrome evaluation. Sci. Rep. 2021, 11, 21963. [Google Scholar] [CrossRef]
- Bagavathiappan, S.; Philip, J.; Jayakumar, T.; Raj, B.; Rao, P.N.S.; Varalakshmi, M.; Mohan, V. Correlation between plantar foot temperature and diabetic neuropathy: A case study by using an infrared thermal imaging technique. J. Diabetes Sci. Technol. 2010, 4, 1386–1392. [Google Scholar] [CrossRef]
- Tan, J.H.; Ng, E.; Acharya, U.R.; Chee, C. Infrared thermography on ocular surface temperature: A review. Infrared Phys. Technol. 2009, 52, 97–108. [Google Scholar] [CrossRef]
- Luximon, A.; Chao, H.; Goonetilleke, R.S.; Luximon, Y. Theory and applications of InfraRed and thermal image analysis in ergonomics research. Front. Comput. Sci. 2022, 4, 990290. [Google Scholar] [CrossRef]
- Marzano-Felisatti, J.M.; Martinez-Amaya, A.; Priego-Quesada, J.I. Preliminary Analysis of Skin Temperature Asymmetries in Elite Young Tennis Players. Appl. Sci. 2023, 13, 628. [Google Scholar] [CrossRef]
- Gómez-Carmona, P.; Fernández-Cuevas, I.; Sillero-Quintana, M.; Arnaiz-Lastras, J.; Navandar, A. Infrared thermography protocol on reducing the incidence of soccer injuries. J. Sport Rehabil. 2020, 29, 1222–1227. [Google Scholar] [CrossRef]
- Lubkowska, A.; Gajewska, E. Temperature distribution of selected body surfaces in scoliosis based on static infrared thermography. Int. J. Environ. Res. Public Health 2020, 17, 8913. [Google Scholar] [CrossRef] [PubMed]
- Kwok, G.; Yip, J.; Yick, K.L.; Cheung, M.C.; Tse, C.Y.; Ng, S.P.; Luximon, A. Postural screening for adolescent idiopathic scoliosis with infrared thermography. Sci. Rep. 2017, 7, 14431. [Google Scholar] [CrossRef] [PubMed]
- Redaelli, D.F.; Abbate, V.; Storm, F.A.; Ronca, A.; Sorrentino, A.; De Capitani, C.; Biffi, E.; Ambrosio, L.; Colombo, G.; Fraschini, P. 3D printing orthopedic scoliosis braces: A test comparing FDM with thermoforming. Int. J. Adv. Manuf. Technol. 2020, 111, 1707–1720. [Google Scholar] [CrossRef]
- Shen, W.; Zhang, J.; Yang, F. Modeling and numerical simulation of bioheat transfer and biomechanics in soft tissue. Math. Comput. Model. 2005, 41, 1251–1265. [Google Scholar] [CrossRef]
- Dulieu-Barton, J. Introduction to thermoelastic stress analysis. Strain 1999, 35, 35–39. [Google Scholar] [CrossRef]
- Gulyaev, Y.V.; Markov, A.; Koreneva, L.; Zakharov, P. Dynamical infrared thermography in humans. IEEE Eng. Med. Biol. Mag. 1995, 14, 766–771. [Google Scholar] [CrossRef]
- Hart, J.; Owens, E.F., Jr. Stability of paraspinal thermal patterns during acclimation. J. Manip. Physiol. Ther. 2004, 27, 109–117. [Google Scholar] [CrossRef]
- Pham, V.; Houilliez, A.; Schill, A.; Carpentier, A.; Herbaux, B.; Thevenon, A. Study of the pressures applied by a Chêneau brace for correction of adolescent idiopathic scoliosis. Prosthetics Orthot. Int. 2008, 32, 345–355. [Google Scholar] [CrossRef]
- FLIR ONE Pro—iOS. Available online: https://www.flir.it/products/flir-one-pro/?vertical=condition+monitoring&segment=solutions (accessed on 8 July 2023).
- Mitsiaki, I.; Thirios, A.; Panagouli, E.; Bacopoulou, F.; Pasparakis, D.; Psaltopoulou, T.; Sergentanis, T.N.; Tsitsika, A. Adolescent idiopathic scoliosis and mental health disorders: A narrative review of the literature. Children 2022, 9, 597. [Google Scholar] [CrossRef]
- JCGM 100:2008; Guide to the Expression of Uncertainty in Measurement. JCGM: Daly City, CA, USA, 2008; Volume 101, p. 2008.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metric | Set #1 | Set #2 | Set #3 | Set #4 | Set #5 | Set #6 | Set #7 | Set #8 | Set #9 | Set #10 | Mean |
|---|---|---|---|---|---|---|---|---|---|---|---|
| A (%) | 70.0 | 55.0 | 65.0 | 75.0 | 65.0 | 70.0 | 60.0 | 65.0 | 65.0 | 65.0 | 65.5 |
| u (%) | 10.5 | 11.4 | 10.9 | 9.9 | 10.9 | 10.5 | 11.2 | 10.9 | 10.9 | 10.9 | 3.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angrisani, L.; De Benedetto, E.; Duraccio, L.; Lo Regio, F.; Ruggiero, R.; Tedesco, A. Infrared Thermography for Real-Time Assessment of the Effectiveness of Scoliosis Braces. Sensors 2023, 23, 8037. https://doi.org/10.3390/s23198037
Angrisani L, De Benedetto E, Duraccio L, Lo Regio F, Ruggiero R, Tedesco A. Infrared Thermography for Real-Time Assessment of the Effectiveness of Scoliosis Braces. Sensors. 2023; 23(19):8037. https://doi.org/10.3390/s23198037
Chicago/Turabian StyleAngrisani, Leopoldo, Egidio De Benedetto, Luigi Duraccio, Fabrizio Lo Regio, Roberto Ruggiero, and Annarita Tedesco. 2023. "Infrared Thermography for Real-Time Assessment of the Effectiveness of Scoliosis Braces" Sensors 23, no. 19: 8037. https://doi.org/10.3390/s23198037
APA StyleAngrisani, L., De Benedetto, E., Duraccio, L., Lo Regio, F., Ruggiero, R., & Tedesco, A. (2023). Infrared Thermography for Real-Time Assessment of the Effectiveness of Scoliosis Braces. Sensors, 23(19), 8037. https://doi.org/10.3390/s23198037