
A Single-Sensor Approach to Quantify Gait in Patients with Hereditary Spastic Paraplegia

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Walking Protocol
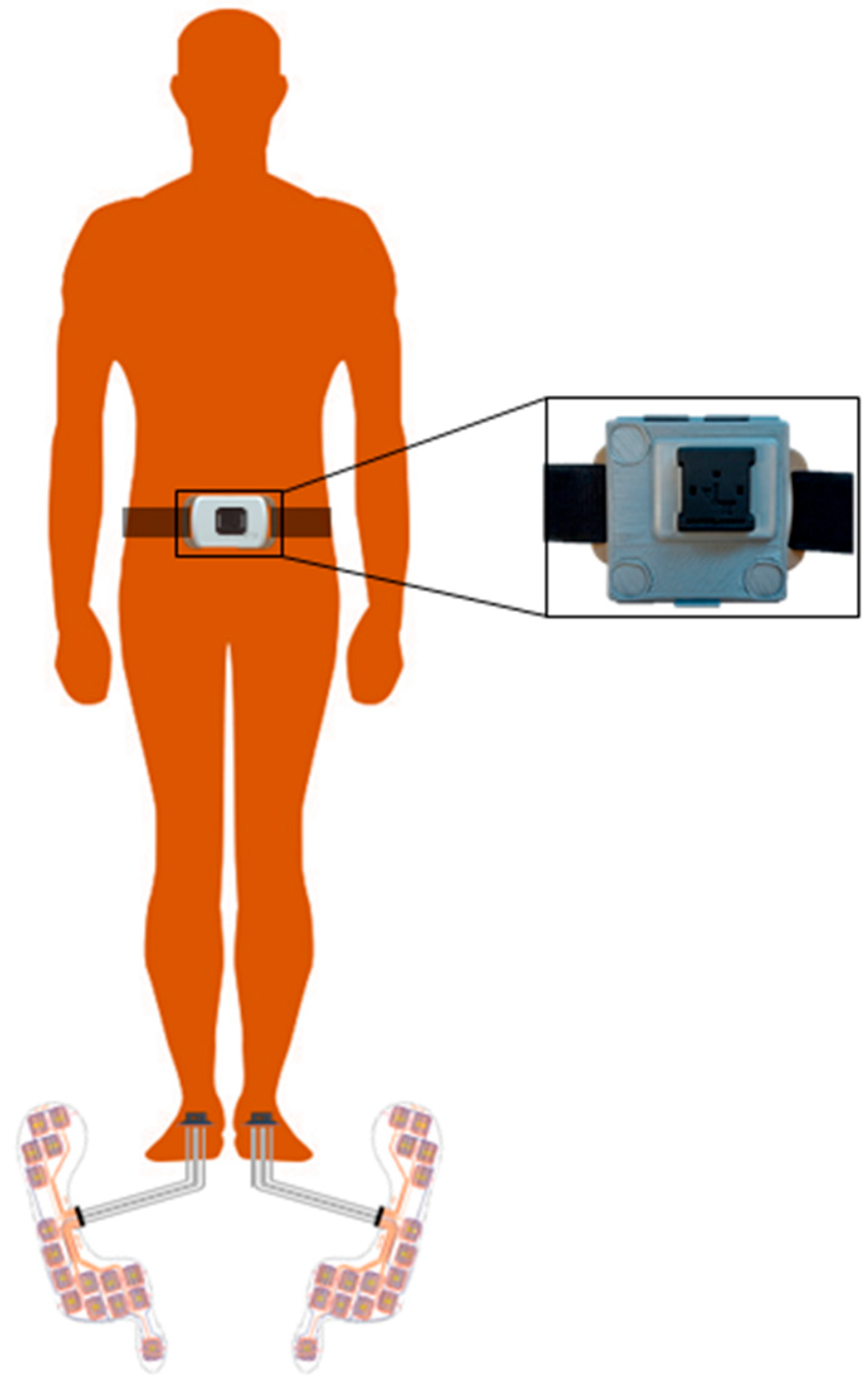
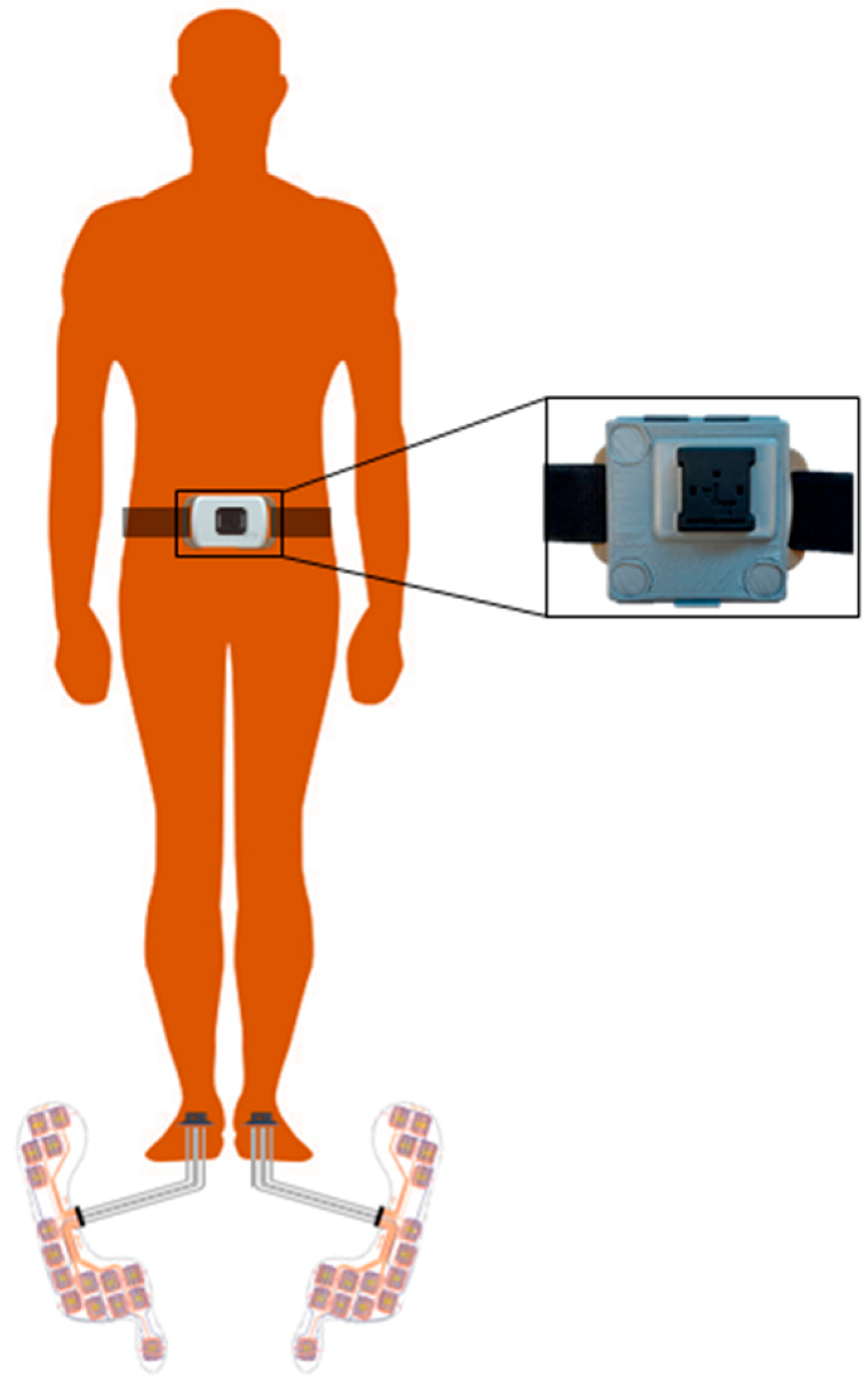
2.3. Measurement Systems
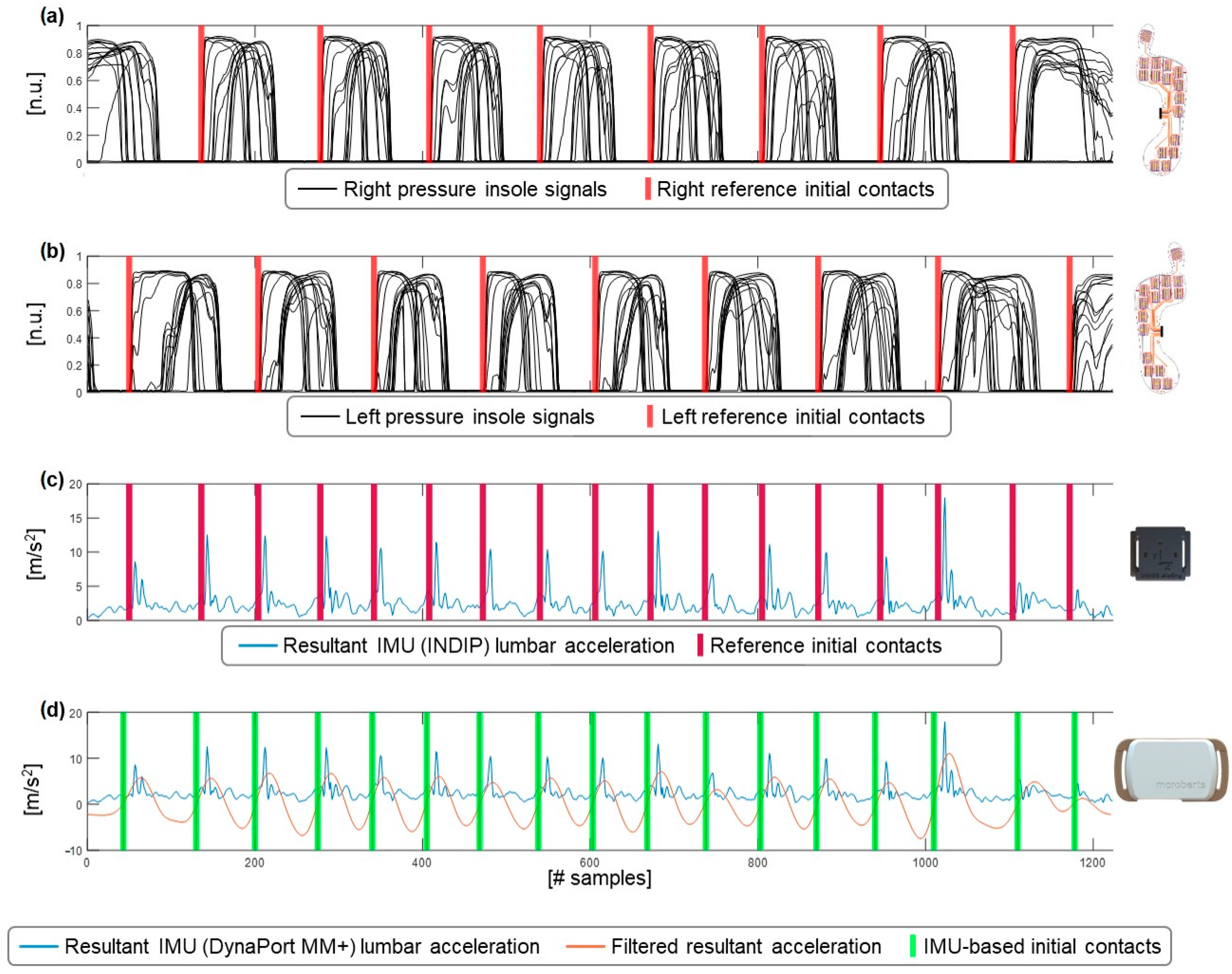
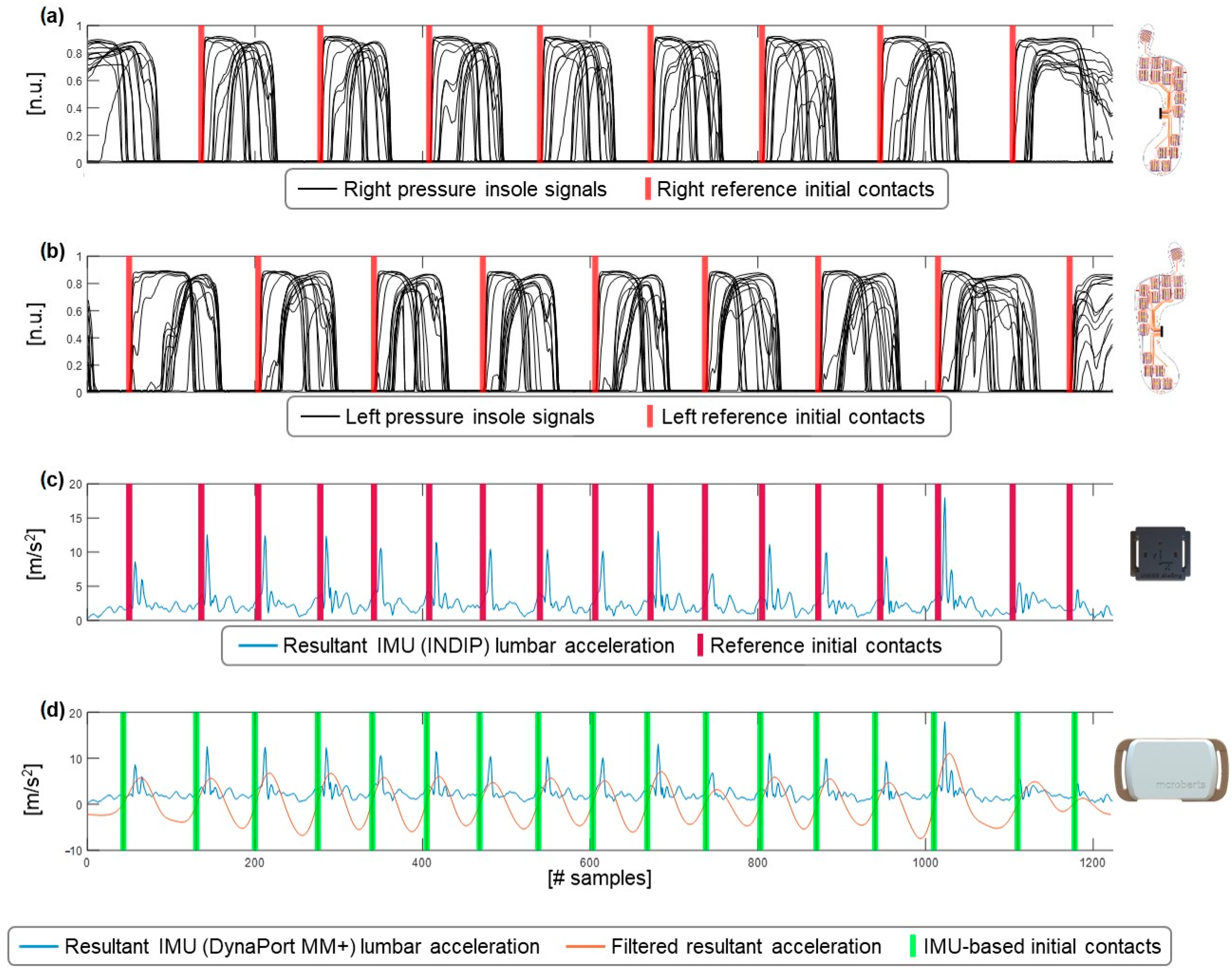
2.4. Data Processing
2.5. Statistical Analysis
2.5.1. Performance Metrics Based on Initial Contact Detection
2.5.2. Accuracy
2.5.3. Reliability
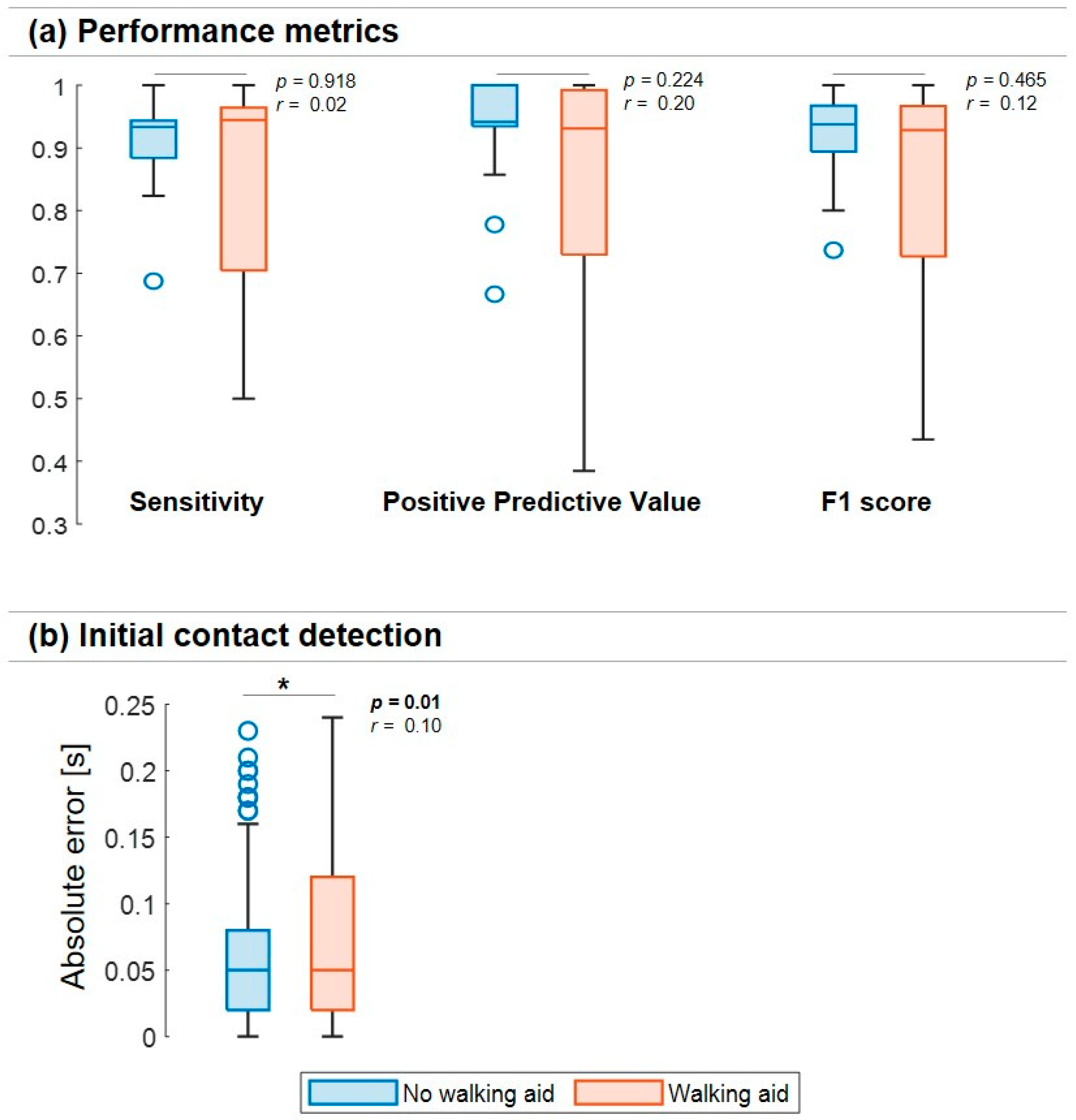
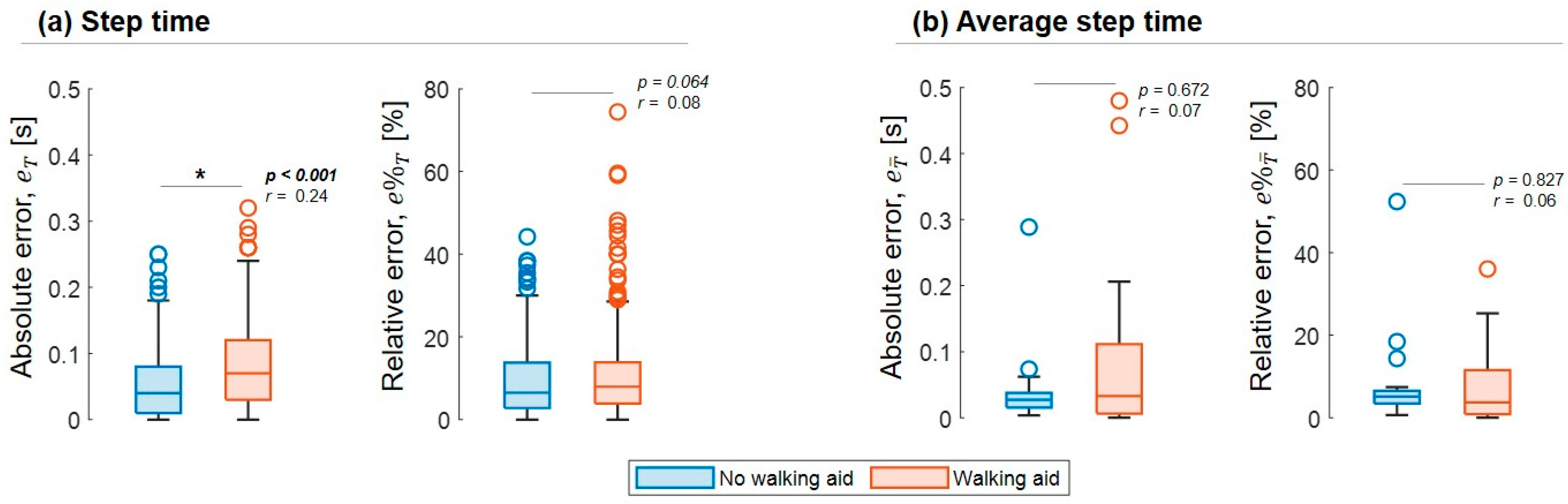
2.5.4. Effect of Using Walking Aids
3. Results
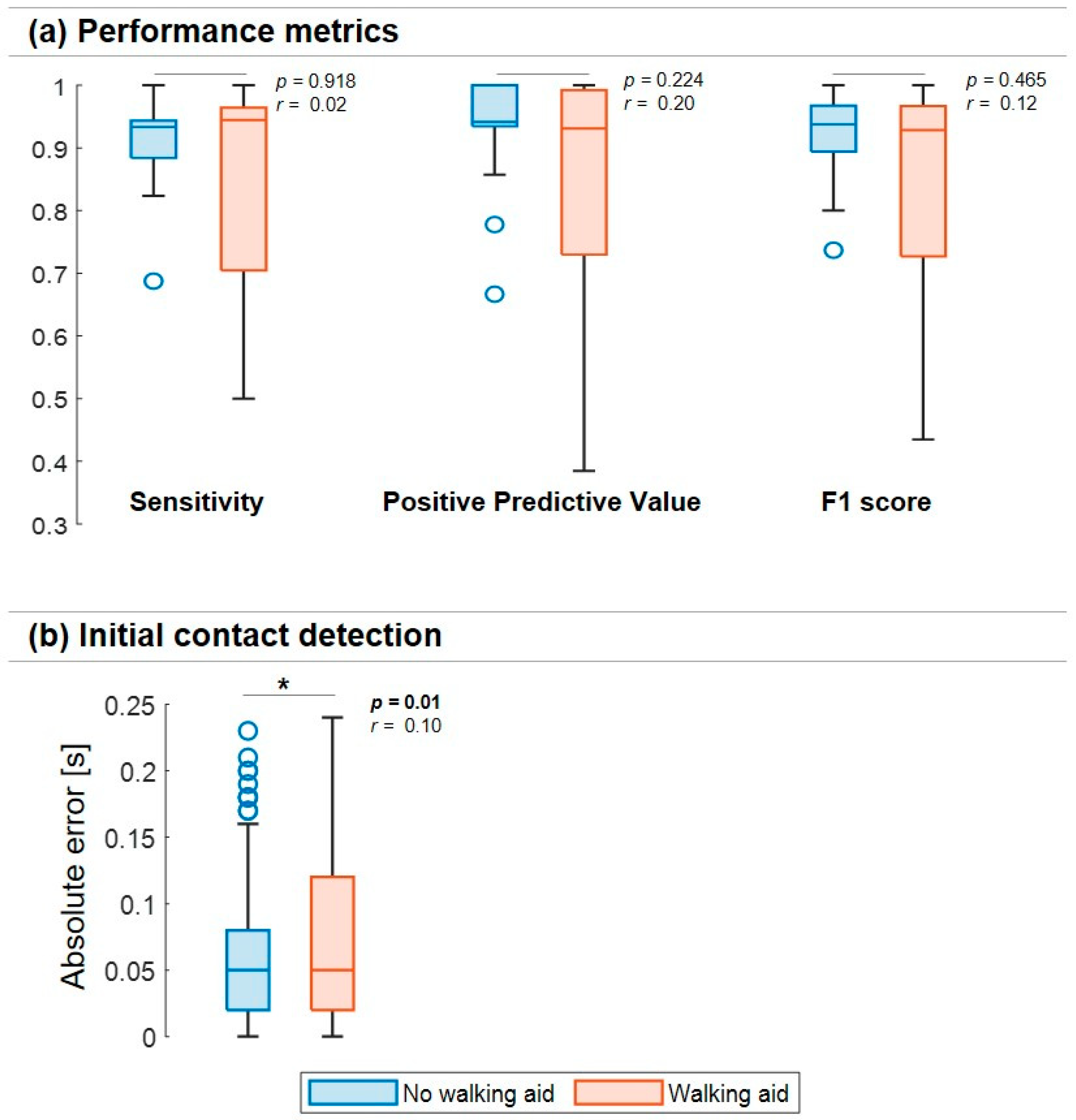
3.1. Initial Contact Detection—Performance Metrics
3.2. Initial Contact Detection—Accuracy
3.3. Initial Contact Detection—Reliability
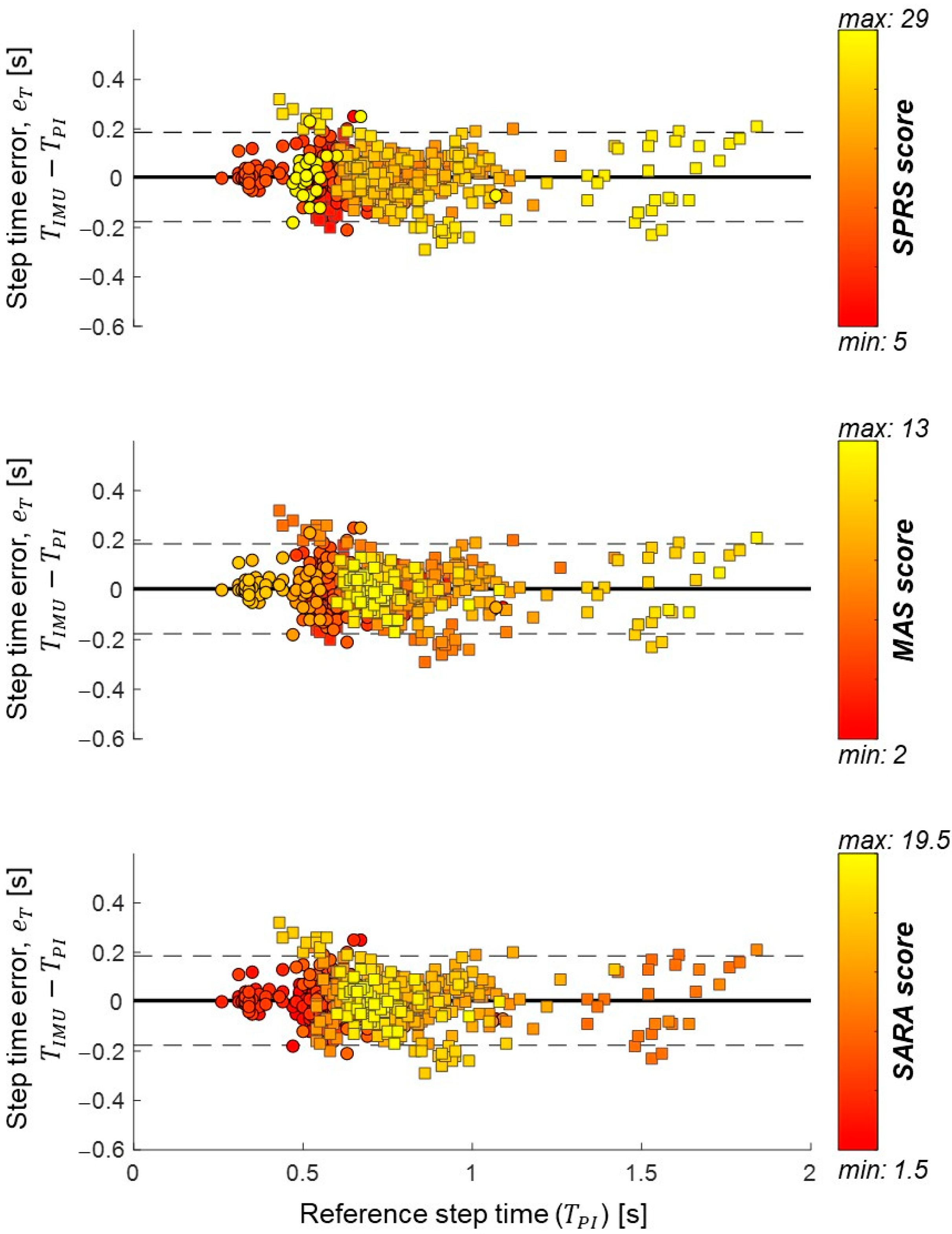
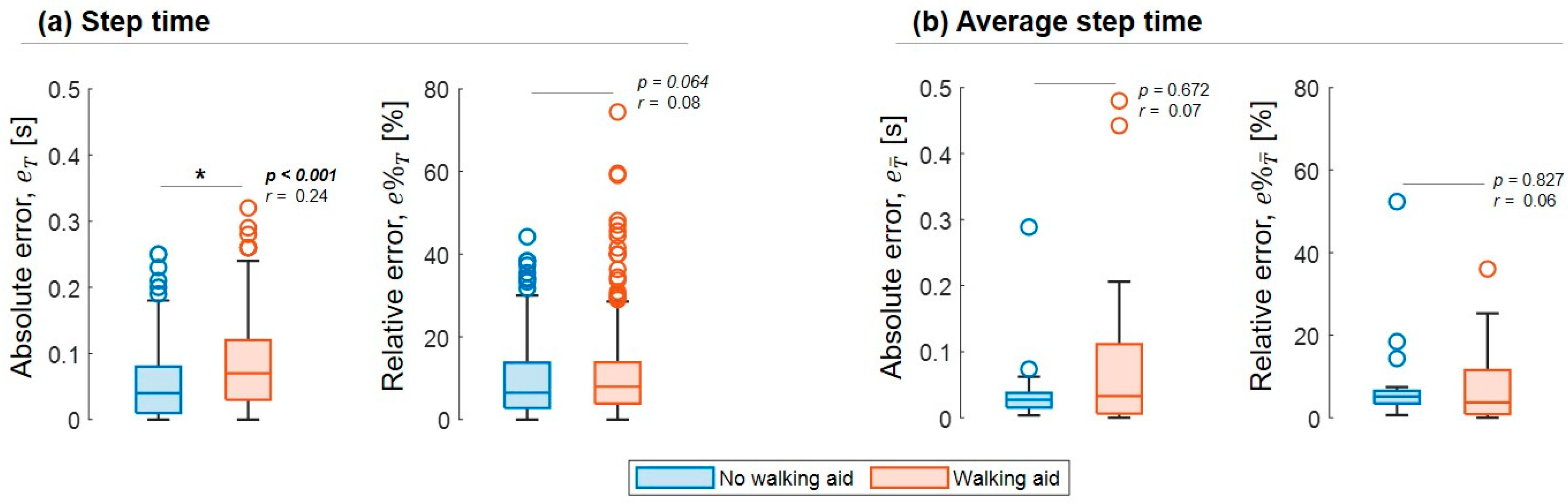
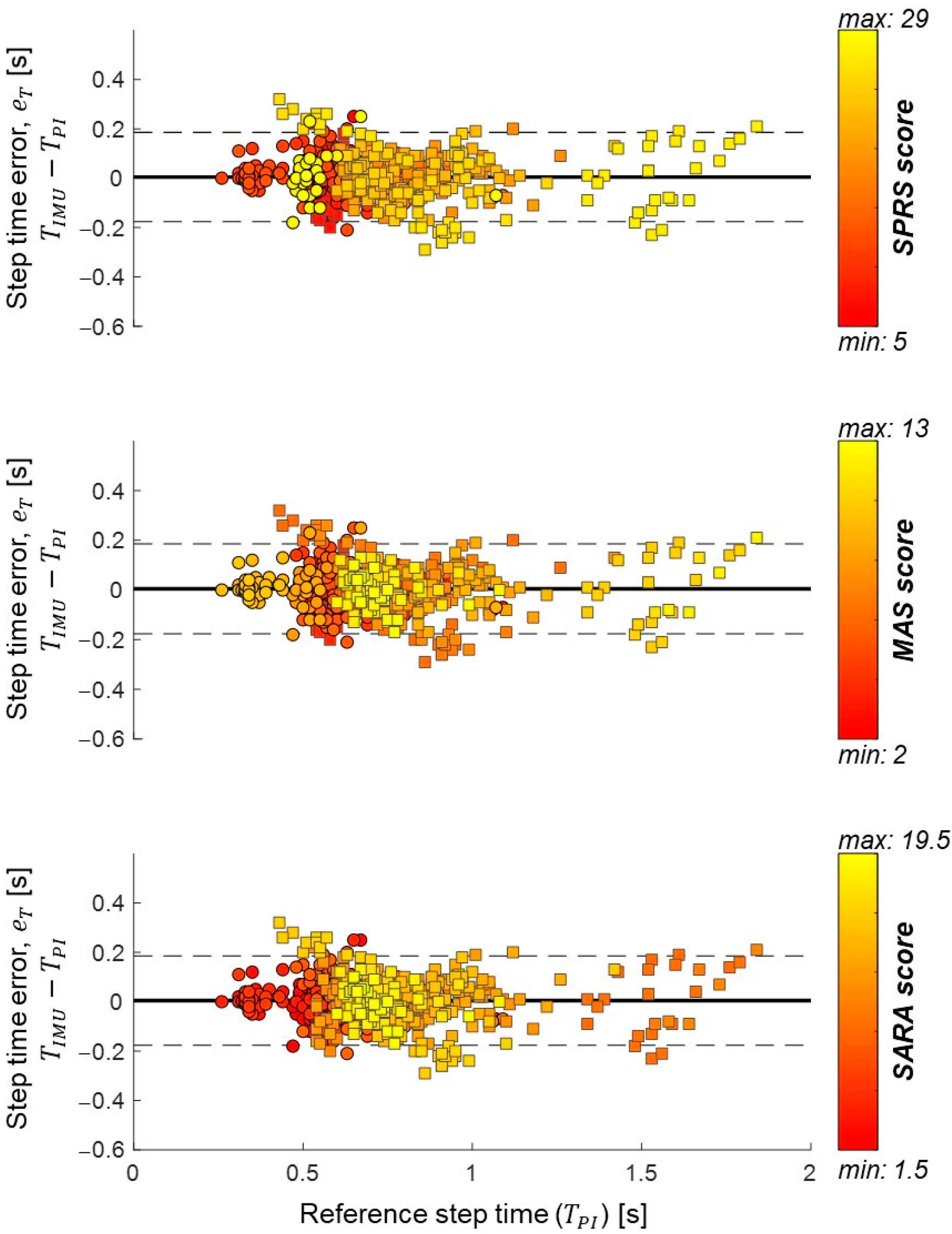
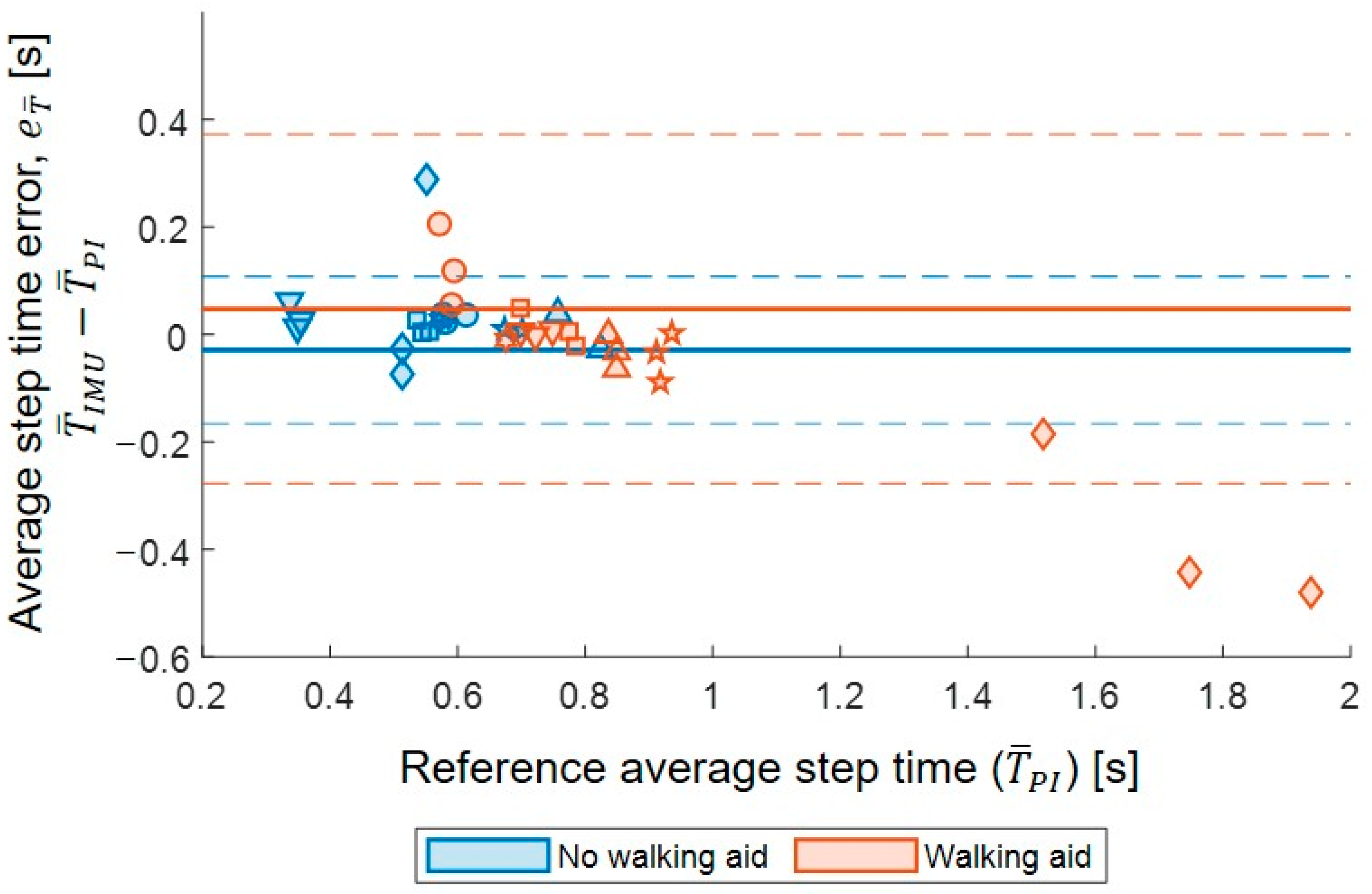
3.4. Step Time Accuracy
3.5. Step Time Reliability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Depienne, C.; Stevanin, G.; Brice, A.; Durr, A. Hereditary spastic paraplegias: An update. Curr. Opin. Neurol. 2007, 20, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.I.; Braatz, F.; Metaxiotis, D.; Armbrust, P.; Dreher, T.; Doderlein, L.; Mikut, R. Gait analysis may help to distinguish hereditary spastic paraplegia from cerebral palsy. Gait Posture 2011, 33, 556–561. [Google Scholar] [CrossRef]
- Cimolin, V.; Piccinini, L.; D’Angelo, M.G.; Turconi, A.C.; Berti, M.; Crivellini, M.; Albertini, G.; Galli, M. Are patients with hereditary spastic paraplegia different from patients with spastic diplegia during walking? Gait evaluation using 3D gait analysis. Funct. Neurol. 2007, 22, 23–28. [Google Scholar] [PubMed]
- Klebe, S.; Stolze, H.; Kopper, F.; Lorenz, D.; Wenzelburger, R.; Volkmann, J.; Porschke, H.; Deuschl, G. Gait analysis of sporadic and hereditary spastic paraplegia. J. Neurol. 2004, 251, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Martino, G.; Ivanenko, Y.; Serrao, M.; Ranavolo, A.; Draicchio, F.; Casali, C.; Lacquaniti, F. Locomotor coordination in patients with Hereditary Spastic Paraplegia. J. Electromyogr. Kinesiol. 2019, 45, 61–69. [Google Scholar] [CrossRef]
- Regensburger, M.; Spatz, I.T.; Ollenschlager, M.; Martindale, C.F.; Lindeburg, P.; Kohl, Z.; Eskofier, B.; Klucken, J.; Schule, R.; Klebe, S.; et al. Inertial Gait Sensors to Measure Mobility and Functioning in Hereditary Spastic Paraplegia: A Cross-Sectional Multicenter Clinical Study. Neurology 2022, 99, e1079–e1089. [Google Scholar] [CrossRef]
- Martindale, C.F.; Roth, N.; Gasner, H.; Jensen, D.; Kohl, Z.; Eskofier, B.M. Mobile Gait Analysis using Personalised Hidden Markov Models for Hereditary Spastic Paraplegia Patients. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 17–21 July 2018; Volume 2018, pp. 5430–5433. [Google Scholar] [CrossRef]
- Bonci, T.; Keogh, A.; Del Din, S.; Scott, K.; Mazza, C.; on Behalf of the Mobilise-D Consortium. An Objective Methodology for the Selection of a Device for Continuous Mobility Assessment. Sensors 2020, 20, 6509. [Google Scholar] [CrossRef]
- McCamley, J.; Donati, M.; Grimpampi, E.; Mazza, C. An enhanced estimate of initial contact and final contact instants of time using lower trunk inertial sensor data. Gait Posture 2012, 36, 316–318. [Google Scholar] [CrossRef]
- Zijlstra, W.; Hof, A.L. Assessment of spatio-temporal gait parameters from trunk accelerations during human walking. Gait Posture 2003, 18, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, R.C.; Lopez, A.M.; Rodriguez-Uria, J.; Alvarez, D.; Alvarez, J.C. Real-time gait event detection for normal subjects from lower trunk accelerations. Gait Posture 2010, 31, 322–325. [Google Scholar] [CrossRef]
- Soltani, A.; Aminian, K.; Mazza, C.; Cereatti, A.; Palmerini, L.; Bonci, T.; Paraschiv-Ionescu, A. Algorithms for Walking Speed Estimation Using a Lower-Back-Worn Inertial Sensor: A Cross-Validation on Speed Ranges. IEEE Trans. Neural. Syst. Rehabil. Eng. 2021, 29, 1955–1964. [Google Scholar] [CrossRef]
- Mobbs, R.J.; Perring, J.; Raj, S.M.; Maharaj, M.; Yoong, N.K.M.; Sy, L.W.; Fonseka, R.D.; Natarajan, P.; Choy, W.J. Gait metrics analysis utilizing single-point inertial measurement units: A systematic review. Mhealth 2022, 8, 9. [Google Scholar] [CrossRef]
- Del Din, S.; Godfrey, A.; Mazzà, C.; Lord, S.; Rochester, L. Free-living monitoring of Parkinson’s disease: Lessons from the field. In Movement Disorders; Wiley Online Library: Hoboken, NJ, USA, 2016; Volume 31, pp. 1293–1313. [Google Scholar]
- Mazzà, C.; Alcock, L.; Aminian, K.; Becker, C.; Bertuletti, S.; Bonci, T.; Brown, P.; Brozgol, M.; Buckley, E.; Carsin, A.E.; et al. Technical validation of real-world monitoring of gait: A multicentric observational study. BMJ Open 2021, 11, e050785. [Google Scholar] [CrossRef]
- Micó-Amigo, M.E.; Bonci, T.; Paraschiv-Ionescu, A.; Ullrich, M.; Kirk, C.; Soltani, A.; Küderle, A.; Gazit, E.; Salis, F.; Alcock, L. Assessing real-world gait with digital technology? Validation, insights and recommendations from the Mobilise-D consortium. J. Neuroeng. Rehabil. 2022, 20, 1–26. [Google Scholar] [CrossRef]
- Paraschiv-Ionescu, A.; Soltani, A.; Aminian, K. Real-world speed estimation using single trunk IMU: Methodological challenges for impaired gait patterns. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; Volume 2020, pp. 4596–4599. [Google Scholar] [CrossRef]
- Salis, F.; Bertuletti, S.; Scott, K.; Caruso, M.; Bonci, T.; Buckley, E.; Croce, U.D.; Mazza, C.; Cereatti, A. A wearable multi-sensor system for real world gait analysis. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, 26–30 July 2021; Volume 2021, pp. 7020–7023. [Google Scholar] [CrossRef]
- Salis, F.; Bertuletti, S.; Bonci, T.; Caruso, M.; Scott, K.; Alcock, L.; Buckley, E.; Gazit, E.; Hansen, C.; Schwickert, L.; et al. A multi-sensor wearable system for the assessment of diseased gait in real-world conditions. Front. Bioeng. Biotechnol. 2023, 11, 1143248. [Google Scholar] [CrossRef]
- Salis, F.; Bertuletti, S.; Bonci, T.; Della Croce, U.; Mazza, C.; Cereatti, A. A method for gait events detection based on low spatial resolution pressure insoles data. J. Biomech. 2021, 127, 110687. [Google Scholar] [CrossRef]
- Paraschiv-Ionescu, A.; Newman, C.J.; Carcreff, L.; Gerber, C.N.; Armand, S.; Aminian, K. Locomotion and cadence detection using a single trunk-fixed accelerometer: Validity for children with cerebral palsy in daily life-like conditions. J. Neuroeng. Rehabil. 2019, 16, 24. [Google Scholar] [CrossRef] [Green Version]
- Tietsch, M.; Muaremi, A.; Clay, I.; Kluge, F.; Hoefling, H.; Ullrich, M.; Kuderle, A.; Eskofier, B.M.; Muller, A. Robust Step Detection from Different Waist-Worn Sensor Positions: Implications for Clinical Studies. Digit. Biomark. 2020, 4 (Suppl. S1), 50–58. [Google Scholar] [CrossRef]
- Walther, B.A.; Moore, J.L. The concepts a literature with of species richness the performance estimators, of estimator review performance precision. Ecography 2005, 28, 815–829. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Field, A.P. Intraclass Correlation. In Wiley StatsRef: Statistics Reference Online; Wikipedia: San Francisco, CA, USA, 2023. [Google Scholar] [CrossRef]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGraw, K.O.; Wong, S. Forming inferences about some intraclass correlations coefficients: Correction. Psychol. Methods 1996, 1, 390. [Google Scholar] [CrossRef]
- Chan, Z.Y.S.; Zhang, J.H.; Au, I.P.H.; An, W.W.; Shum, G.L.K.; Ng, G.Y.F.; Cheung, R.T.H. Gait Retraining for the Reduction of Injury Occurrence in Novice Distance Runners: 1-Year Follow-up of a Randomized Controlled Trial. Am. J. Sport. Med. 2018, 46, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. CHAPTER 3—The Significance of a Product Moment rs. In Statistical Power Analysis for the Behavioral Sciences; Cohen, J., Ed.; Academic Press: Cambridge, MA, USA, 1977; pp. 75–107. [Google Scholar] [CrossRef]
- Martindale, C.F.; Roth, N.; Gasner, H.; List, J.; Regensburger, M.; Eskofier, B.M.; Kohl, Z. Technical Validation of an Automated Mobile Gait Analysis System for Hereditary Spastic Paraplegia Patients. IEEE J. Biomed. Health Inf. 2020, 24, 1490–1499. [Google Scholar] [CrossRef]
- Mico-Amigo, M.E.; Kingma, I.; Ainsworth, E.; Walgaard, S.; Niessen, M.; van Lummel, R.C.; van Dieen, J.H. A novel accelerometry-based algorithm for the detection of step durations over short episodes of gait in healthy elderly. J. Neuroeng. Rehabil. 2016, 13, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trojaniello, D.; Ravaschio, A.; Hausdorff, J.M.; Cereatti, A. Comparative assessment of different methods for the estimation of gait temporal parameters using a single inertial sensor: Application to elderly, post-stroke, Parkinson’s disease and Huntington’s disease subjects. Gait Posture 2015, 42, 310–316. [Google Scholar] [CrossRef]
- Polhemus, A.; Ortiz, L.D.; Brittain, G.; Chynkiamis, N.; Salis, F.; Gassner, H.; Gross, M.; Kirk, C.; Rossanigo, R.; Taraldsen, K.; et al. Walking on common ground: A cross-disciplinary scoping review on the clinical utility of digital mobility outcomes. NPJ Digit. Med. 2021, 4, 149. [Google Scholar] [CrossRef]
- Gassner, H.; List, J.; Martindale, C.F.; Regensburger, M.; Klucken, J.; Winkler, J.; Kohl, Z. Functional gait measures correlate to fear of falling, and quality of life in patients with Hereditary Spastic Paraplegia: A cross-sectional study. Clin. Neurol. Neurosurg. 2021, 209, 106888. [Google Scholar] [CrossRef]
- Serrao, M.; Rinaldi, M.; Ranavolo, A.; Lacquaniti, F.; Martino, G.; Leonardi, L.; Conte, C.; Varrecchia, T.; Draicchio, F.; Coppola, G.; et al. Gait Patterns in Patients with Hereditary Spastic Paraparesis. PLoS ONE 2016, 11, e0164623. [Google Scholar] [CrossRef]
- van Vugt, Y.; Stinear, J.; Claire Davies, T.; Zhang, Y. Postural stability during gait for adults with hereditary spastic paraparesis. J. Biomech. 2019, 88, 12–17. [Google Scholar] [CrossRef]
- van de Venis, L.; Weerdesteyn, V.; Konijnenburg, A.; van de Warrenburg, B.P.C.; Geurts, A.C.H.; Nonnekes, J. Increased trunk movements in people with hereditary spastic paraplegia: Do these involve balance correcting strategies? J. Neurol. 2022, 269, 4264–4269. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Mean ± SD/Median (Quartile 1, Quartile 3) |
|---|---|
| Age (years) | 54 ± 15 |
| Height (cm) | 177 ± 7 |
| Body mass (kg) | 83 ± 17 |
| Spastic Paraplegia Rating Scale (SPRS) | 19.5 (14.8, 22.0) * |
| Modified Ashworth Scale (MAS) | 8.0 (6.0, 12.0) |
| Scale for the Assessment and Rating of Ataxia (SARA) | 10.0 (2.0, 11.8) |
| Gender | 3 females, 10 males |
| SPG mutation | SPG4: 3 patients SPG7: 9 patients Other: 1 patient |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Gelder, L.M.A.; Bonci, T.; Buckley, E.E.; Price, K.; Salis, F.; Hadjivassiliou, M.; Mazzà, C.; Hewamadduma, C. A Single-Sensor Approach to Quantify Gait in Patients with Hereditary Spastic Paraplegia. Sensors 2023, 23, 6563. https://doi.org/10.3390/s23146563
van Gelder LMA, Bonci T, Buckley EE, Price K, Salis F, Hadjivassiliou M, Mazzà C, Hewamadduma C. A Single-Sensor Approach to Quantify Gait in Patients with Hereditary Spastic Paraplegia. Sensors. 2023; 23(14):6563. https://doi.org/10.3390/s23146563
Chicago/Turabian Stylevan Gelder, Linda M. A., Tecla Bonci, Ellen E. Buckley, Kathryn Price, Francesca Salis, Marios Hadjivassiliou, Claudia Mazzà, and Channa Hewamadduma. 2023. "A Single-Sensor Approach to Quantify Gait in Patients with Hereditary Spastic Paraplegia" Sensors 23, no. 14: 6563. https://doi.org/10.3390/s23146563
APA Stylevan Gelder, L. M. A., Bonci, T., Buckley, E. E., Price, K., Salis, F., Hadjivassiliou, M., Mazzà, C., & Hewamadduma, C. (2023). A Single-Sensor Approach to Quantify Gait in Patients with Hereditary Spastic Paraplegia. Sensors, 23(14), 6563. https://doi.org/10.3390/s23146563