
Robust Arm Impedocardiography Signal Quality Enhancement Using Recursive Signal Averaging and Multi-Stage Wavelet Denoising Methods for Long-Term Cardiac Contractility Monitoring Armbands




Abstract
1. Introduction
2. Materials and Methods
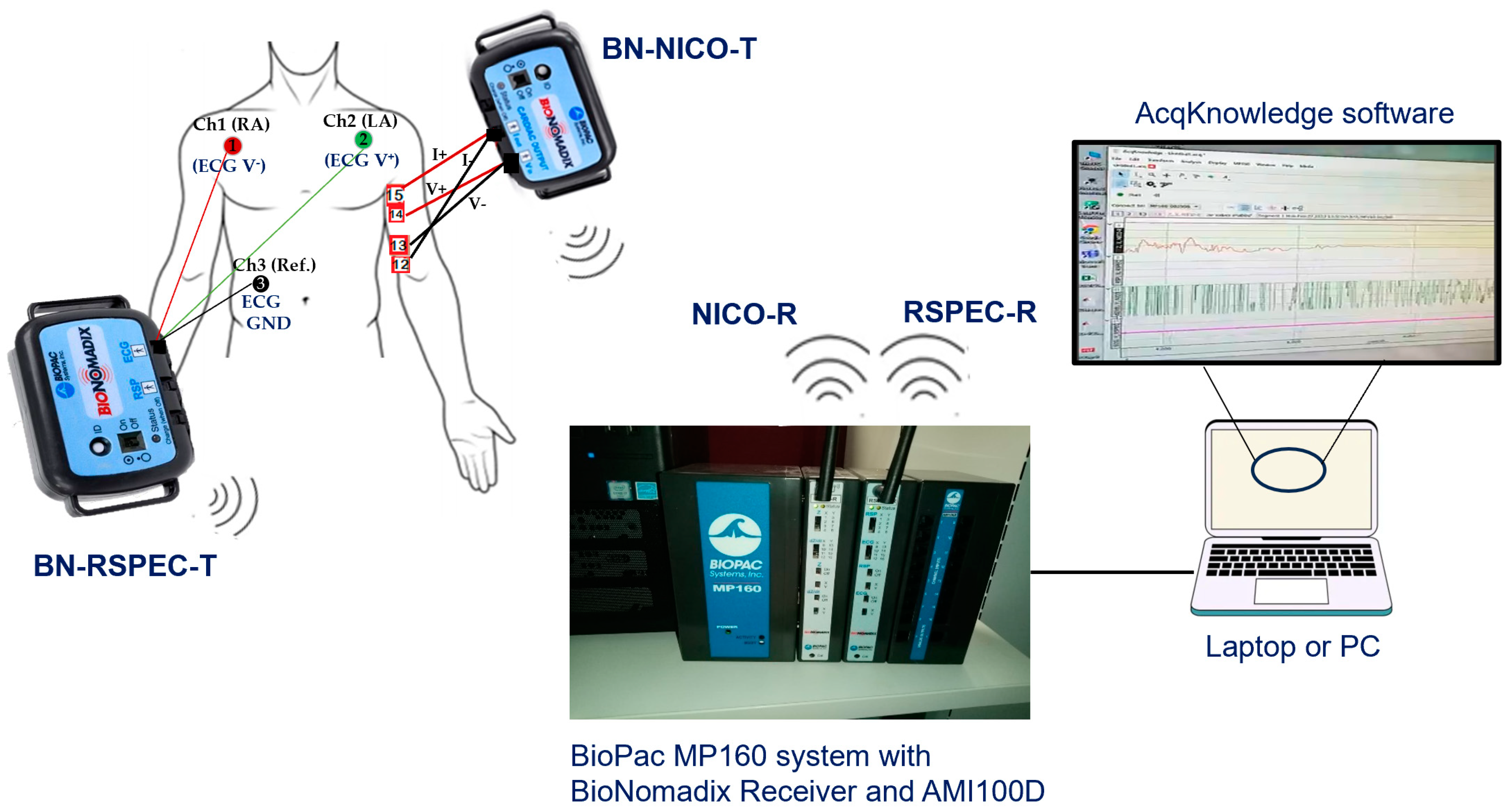
2.1. Data Acquisition and Sensor Systems
2.2. ICG and ECG Recording Modes and Analysis Tools
2.3. Arm ICG Electrode Location
2.4. ICG Pilot Study Data Set
2.5. ICG and ECG Prefiltering Stage with IIR Filters
2.6. Savitzky–Golay Prefiltering of the ICG Signals Stage
2.7. Beat-by-Beat Recursive Ensemble Averaging Denoising Process
2.7.1. Beat-by-Beat Segmentation Algorithm
2.7.2. ICG Ensemble Averaging Process
2.7.3. ICG Recursive Averaging BbyB Process
2.7.4. Selection of the Number of Beats Order (Nb) of the Rav Process
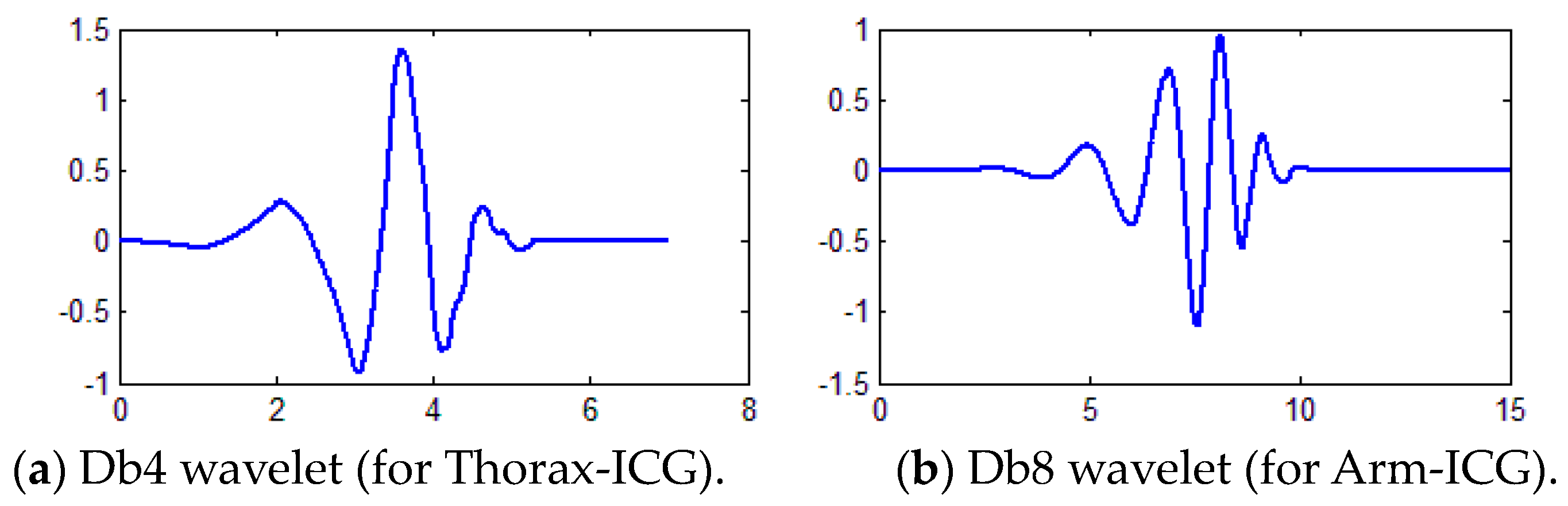
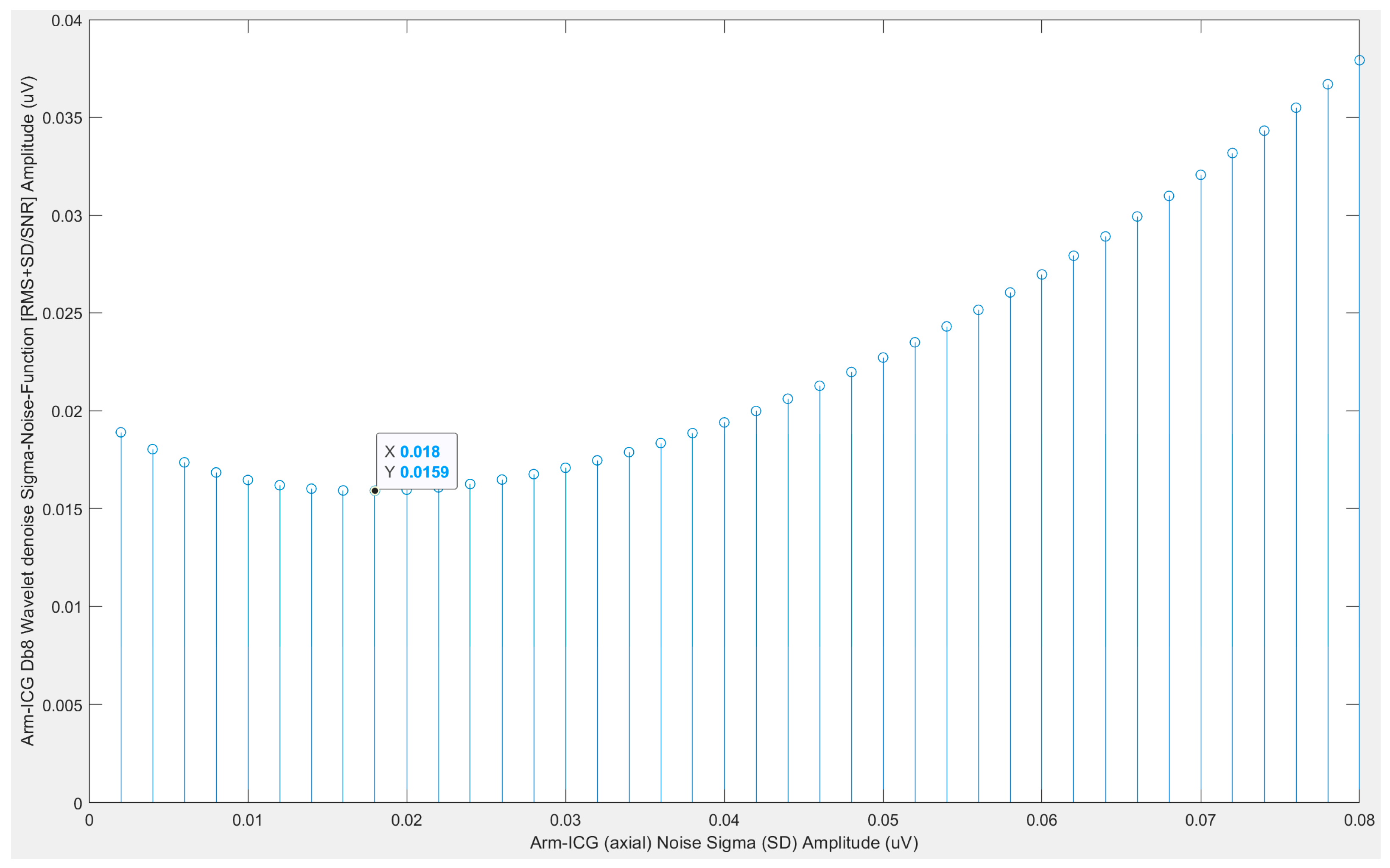
2.8. Beat-by-Beat Daubechies Wavelet Transform-Based Denoising of ICG Signals
2.9. ICG Beat-by-Beat Denoised ICG Waveform Quality Assessment and Inclusion Criteria
2.9.1. Pearson Correlation (p) BbyB with “Noiseless” SAICG Vector Reference
2.9.2. BbyB Residual Noise and SNR Metrics Based on the SAICG Signal-Vector
2.10. ICG Waveform Basic Features Metrics Definitions
- (A): For measuring the relative time delay (ms) of the ICG waveform main pulse with respect to the simultaneous ECG R-wave position, namely, (SFP(k) − 80), in a particular subject.
- (B): The ICG waveform main pulse peak amplitude (Ω/s).
- (C): The ICG main pulse width (ms) at mid-amplitude level (B/2).
- (VET): The ventricular ejection time (ms) used to derive the stroke volume (SV).
2.11. Functional Relationship between Arm-ICG and Thorax-ICG Features Metrics
- (D): The comparative metric of amplitude B values ratio (%) of Arm(B)/Thorax(B).
- (E): The time metrics difference (ms) of [Thorax(C) − Arm(C)].
- (F): The ICG pulse width time metric ratio [Thorax(C)/Arm(C)].
- (G): The ICG time metrics ratio [Thorax(VET)/Arm(VET)].
- (H): The ICG volume metric ratio [Thorax(SV)/Arm(SV)].
2.12. ICG Signal Frames with Tukey Tapered Cosine Windowing
2.13. Removing Outliers
3. Results
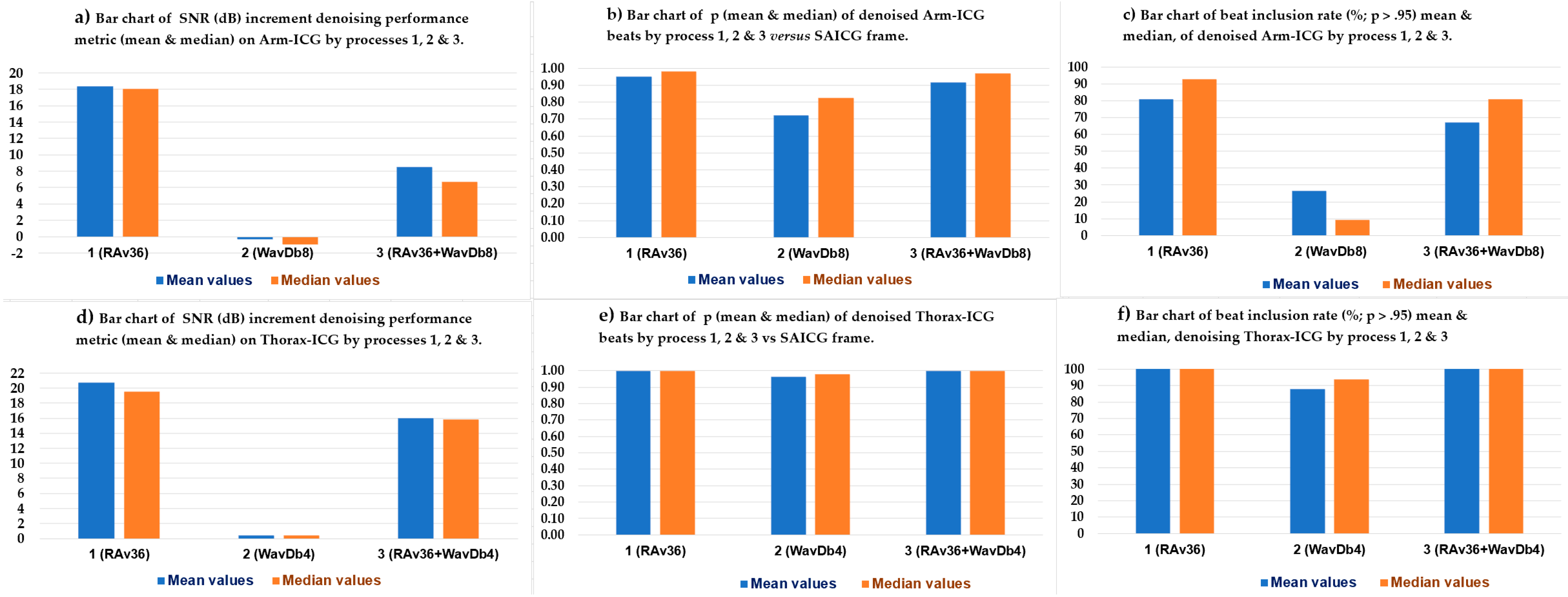
3.1. ICG Denoising Processes Performance
3.2. RAv36 Denoised ICG Waveform Features A, B, C and VET Metrics Assessment
3.2.1. Arm-ICG Mode Waveform Features A, B and C Metrics Assessment
3.2.2. Thorax-ICG Denoised Waveform Features A, B and C Metrics Assessment
3.2.3. Arm-ICG vs. Thorax-ICG Waveforms VET Timing Metric Assessment
3.2.4. Functional Relationship between Arm-ICG and Thorax-ICG: Metrics D, E, F, G & H
3.3. Functional Relationship Analysis of Measured SV Values on the Arm-ICG and on the Thorax-ICG
4. Discussion
- (a)
- Creating an effective real-time prefilter design approach for Arm-ICGs.
- (b)
- Developing a practical, robust, advanced and data-driven BbyB denoising process.
- (c)
- Establishing a compelling functional relationship with the conventional Thorax-ICG waveform feature metrics, which could be used to derive the cardiac SV from Arm-ICG recordings, with satisfactory accuracy and precision.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO), Cardiovascular Diseases (CADs). 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 14 May 2023).
- Wang, L.; Lu, Y.; Wang, H.; Gu, J.; Ma, Z.J.; Lian, Z.; Zhang, Z.; Krumholz, H.; Sun, N. Effectiveness of an impedance cardiography guided treatment strategy to improve blood pressure control in a real-world setting: Results from a pragmatic clinical trial. Open Heart 2021, 8, e001719. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, S.; Alhadidi, T.; Chabchoub, S.; Salah, R.B. Impedance cardiography: Recent applications and developments. BioMed Res. 2018, 29, 3542–3552. [Google Scholar] [CrossRef]
- Woltjer, H.H.; Bogaard, H.J.; De Vries, P.M.J.M. The technique of impedance cardiography: A review. Eur. Heart J. 1997, 18, 1396–1403. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, D.P. Impedance cardiography: Pulsatile blood flow and the biophysical and electrodynamic basis for the stroke volume equations. J. Electr. Bioimpedance 2009, 1, 2–17. [Google Scholar] [CrossRef]
- Aria, S.; Elfarri, Y.; Elvegård, M.; Gottfridsson, A.; Grønaas, H.S.; Harang, S.; Jansen, A.; Madland, T.E.R.; Martins, I.B.; Olstad, M.W.; et al. Measuring Blood Pulse Wave Velocity with Bioimpedance in Different Age Groups. Sensors 2019, 19, 850. [Google Scholar] [CrossRef]
- Escalona, O.J.; Abdul-Qayum, G.; Hilton, A.; Biglarbeigi, P.; McEneaney, D. February. Cardiac contractility assessment from arm impedance plethysmography (IPG). In IUPESM World Congress on Medical Physics and Biomedical Engineering; Springer: Berlin/Heidelberg, Germany, 2022. [Google Scholar]
- Bernstein, D.P.; Henry, I.C.; Lemmens, H.J.; Chaltas, J.L.; DeMaria, A.N.; Moon, J.B.; Kahn, A.M. Validation of stroke volume and cardiac output by electrical interroaubecof the brachial artery in normals: Assessment of strengths, limitations, and sources of error. J. Clin. Monit. Comput. 2015, 29, 789–800. [Google Scholar] [CrossRef]
- Wang, J.; Hu, W.; Kao, T.; Liu, C.; Lin, S. Development of forearm impedance plethysmography for the minimally invasive monitoring of cardiac pumping function. J. Biomed. Sci. Eng. 2011, 4, 122–129. [Google Scholar] [CrossRef]
- Saugel, B.; Cecconi, M.; Wagner, J.Y.; Reuter, D.A. Noninvasive continuous cardiac output monitoring in perioperative and intensive care medicine. Br. J. Anaesth. 2015, 114, 562–575. [Google Scholar] [CrossRef] [PubMed]
- Epperson, T.N.; Varacallo, M. Anatomy, shoulder and upper limb, brachial artery. In StatPearls; StatPearls Publishing: St. Petersburg, FL, USA, 2021. [Google Scholar]
- Bruss, Z.S.; Raja, A. Physiology, stroke volume. In StatPearls; StatPearls Publishing: St. Petersburg, FL, USA, 2022. [Google Scholar]
- Kubicek, W.G.; Karnegis, J.N.; Patterson, R.P.; A Witsoe, D.; Mattson, R.H. Development and evaluation of an impedance cardiac output system. Aerosp. Med. 1966, 37, 1208–1212. [Google Scholar]
- Salah, I.B.; Ouni, K. Denoising of the impedance cardiographie signal (ICG) for a best detection of the characteristic points. In Proceedings of the 2017 2nd International Conference on Bio-Engineering for Smart Technologies (BioSMART), Paris, France, 30 August–1 September 2017; pp. 1–4. [Google Scholar] [CrossRef]
- DeMarzo, A.P. Clinical Use of Impedance Cardiography for Hemodynamic Assessment of Early Cardiovascular Disease and Management of Hypertension. High Blood Press. Cardiovasc. Prev. 2020, 27, 203–213. [Google Scholar] [CrossRef]
- Metshein, M.; Gautier, A.; Larras, B.; Frappe, A.; John, D.; Cardiff, B.; Annus, P.; Land, R.; Martens, O. Study of Electrode Locations for Joint Acquisition of Impedance- and Electro-cardiography Signals. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2021, 2021, 7264. [Google Scholar] [CrossRef]
- Chabchoub, S.; Mansouri, S.; Ben Salah, R. Impedance cardiography signal denoising using discrete wavelet transform. Australas. Phys. Eng. Sci. Med. 2016, 39, 655–663. [Google Scholar] [CrossRef] [PubMed]
- AlHinai, N. Chapter 1—Introduction to biomedical signal processing and artificial intelligence. In Biomedical Signal Processing and Artificial Intelligence in Healthcare; Zgallai, W., Ed.; Academic Press: Cambridge, MA, USA, 2020. [Google Scholar] [CrossRef]
- De Oliveira, M.A.; Araujo, N.V.S.; Da Silva, R.N.; Da Silva, T.I.; Epaarachchi, J. Use of Savitzky–Golay Filter for Performances Improvement of SHM Systems Based on Neural Networks and Distributed PZT Sensors. Sensors 2018, 18, 152. [Google Scholar] [CrossRef] [PubMed]
- Savitzky, A.; Golay, M.J.E. Smoothing and Differentiation of Data by Simplified Least Squares Procedures. Anal. Chem. 1964, 36, 1627–1639. [Google Scholar] [CrossRef]
- Huang, H.; Hu, S.; Sun, Y. A Discrete Curvature Estimation Based Low-Distortion Adaptive Savitzky–Golay Filter for ECG Denoising. Sensors 2019, 19, 1617. [Google Scholar] [CrossRef] [PubMed]
- Escalona, O.J.; Magwood, S.; Hilton, A.; McCallan, N. Feasibility of Wearable Armband Bipolar ECG Lead-1 for Long-term HRV Monitoring by Combined Signal Averaging and 2-stage Wavelet Denoising. In Proceedings of the 2022 Computing in Cardiology (CinC), Tampere, Finland, 4–7 September 2022; Volume 49. [Google Scholar] [CrossRef]
- Escalona, O.; Mukhtar, S.; McEneaney, D.; Finlay, D. Armband sensors location assessment for left Arm-ECG bipolar leads waveform components discovery tendencies around the MUAC line. Sensors 2022, 22, 7240. [Google Scholar] [CrossRef]
- Escalona, O.J.; Mitchell, R.; Balderson, D.; Harron, D. A fast and reliable QRS alignment technique for high-frequency analysis of the signal-averaged ECG. Med. Biol. Eng. Comput. 1993, 3, S137–S146. [Google Scholar] [CrossRef]
- Escalona, O.J.; Lynn, W.D.; Perpiñan, G.; McFrederick, L.; McEneaney, D.J. Data-driven ECG denoising techniques for characterising bipolar lead sets along the left arm in wearable long-term heart rhythm monitoring. Electronics 2017, 6, 84. [Google Scholar] [CrossRef]
- Villegas, A.; McEneaney, D.; Escalona, O. Arm-ECG Wireless Sensor System for Wearable Long-Term Surveillance of Heart Arrhythmias. Electronics 2018, 8, 1300. [Google Scholar] [CrossRef]
- Vizcaya, P.; Perpiñan, G.; McEneaney, D.; Escalona, O.J. Standard ECG lead I prospective estimation study from far-field bipolar leads on the left upper arm: A neural network approach. Biomed. Signal Process. Control 2019, 51, 171–180. [Google Scholar] [CrossRef]
- McCallan, N.; Finlay, D.; Biglarbeigi, P.; Perpinan, G.; Jenning, M.; Ng, K.Y.; McLaughlin, J.; Escalona, O.J. Wearable Technology: Signal Recovery of Electrocardiogram from Short Spaced Leads in the Far-Field Using Discrete Wavelet Transform Based Techniques. In Proceedings of the 2019 Computing in Cardiology (CinC), Singapore, 8–11 September 2019; Volume 46, p. 1. [Google Scholar]
- Perpiñan, G.; McEneaney, D.J.; Escalona, O.J. Denoising Performance of Discrete Wavelet Transform and Empirical Mode Decomposition Based Techniques on Monitoring Cardia” Electrograms from the Left-Arm. In Proceedings of the 2019 Computing in Cardiology (CinC), Singapore, 8–11 September 2019; Volume 46, pp. 1–4. [Google Scholar] [CrossRef]
- Ali Sheikh, S.A.; Shah, A.; Levantsevych, O.; Soudan, M.; Alkhalaf, J.; Bahrami Rad, A.; Inan, O.T.; Clifford, G.D. An open-source automated algorithm for removal of noisy beats for accurate impedance cardiogram analysis. Physiol. Meas. 2020, 41, 075002. [Google Scholar] [CrossRef] [PubMed]
- Benabdallah, H.; Kerai, S. Respiratory and motion artefacts removal from ICG signal using denoising techniques for hemodynamic parameters monitoring. Traitement Signal 2021, 38, 919–928. [Google Scholar] [CrossRef]
- Lema-Condo, E.L.; Bueno-Palomeque, F.L.; Castro-Villalobos, S.E.; Ordoñez Morales, E.F.; Serpa-Andrade, L.J. Comparison of wavelet transform symlets (2-10) and daubechies (2-10) for an electro ncephalographic signal analysis. In Proceedings of the 2017 IEEE XXIV International Conference on Electronics, Electrical Engineering and Computing (INTERCON), Cusco, Peru, 15–18 August 2017. [Google Scholar] [CrossRef]
- Sebastian, T.; Pandey, P.C.; Naidu, S.M.M.; Pandey, V.K. Wavelet based denoising for suppression of respiratory and motion artifacts in impedance cardiography. In Proceedings of the 2011 Computing in Cardiology, Hangzhou, China, 18–21 September 2011; Volume 38, pp. 501–504. [Google Scholar]
- Lázaro, J.; Reljin, N.; Hossain, M.B.; Noh, Y.; Laguna, P.; Chon, K.H. Wearable Armband Device for Daily Life Electrocardiogram Monitoring. IEEE Trans. Biomed. Eng. 2020, 67, 3464–3473. [Google Scholar] [CrossRef] [PubMed]
- Daud, S.N.S.S.; Sudriman, R.; Mahmood, R.N.H.; Omar, C. Denoising Semi-simulated EEG Signal Contaminated Ocular Noise using Various Wavelet Filters. In Proceedings of the 2022 13th International Conference on Information and Communication Systems (ICICS), Irbid, Jordan, 21–23 June 2022; pp. 452–457. [Google Scholar] [CrossRef]
- Elamvazuthi, I.; Ling, G.A.; Nurhanim, K.A.R.K.; Vasant, P.; Parasuraman, S. Surface electromyography (sEMG) feature extraction based on Daubechies wavelets. In Proceedings of the 2013 IEEE 8th Conference on Industrial Electronics and Applications (ICIEA), Melbourne, VIC, Australia, 19–21 June 2013; pp. 1492–1495. [Google Scholar] [CrossRef]
- Schmid, M.; Rath, D.; Diebold, U. Why and how Savitzky–Golay filters should be replaced. ACS Meas. Sci. Au 2022, 2, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Escalona, O.J.; Mendoza, M.; Villegas, G.; Navarro, C. Real-time system for high-resolution ECG diagnosis based on 3D late potential fractal dimension estimation. In Proceedings of the 2011 Computing in Cardiology, Hangzhou, China, 18–21 September 2011; Volume 38, pp. 789–792. [Google Scholar]
- Bloomfield, P. Fourier Analysis of Time Series: An Introduction; Wiley-Interscience: New York, NY, USA, 2000. [Google Scholar]
- Detect and Remove Outliers in Data—MATLAB Rmoutliers—MathWorks United Kingdom. Available online: https://uk.mathworks.com/help/matlab/ref/rmoutliers.html (accessed on 14 May 2023).
- Escalona, O.J.; Mendoza, M. Electrocardiographic waveforms fitness check device technique for sudden cardiac death risk screening. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 3453–3556. [Google Scholar] [CrossRef]
- Wang, Z.; Zhu, J.; Yan, T.; Yang, L. A new modified wavelet-based ECG denoising. Comput. Assist. Surg. Abingdon Engl. 2019, 24, 174–183. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean | SD | Median | IQR |
|---|---|---|---|---|
| Age (y): both genders | 38.60 | 14.45 | 39.00 | 23.00 |
| Age (y): females (46.7%) | 27.57 | 6.73 | 25.00 | 6.00 |
| Age (y): males (53.3%) | 48.25 | 12.28 | 48.50 | 17.75 |
| Height (cm) | 167.27 | 8.52 | 168.50 | 10.75 |
| Weight (kg) | 70.13 | 8.75 | 70.00 | 14.50 |
| BMI (kg/m2) | 25.21 | 3.85 | 24.65 | 5.91 |
| Waist measure (cm): around | 86.37 | 12.83 | 84.00 | 20.00 |
| Chest measure (cm): around at axilla level (cm) | 93.30 | 7.97 | 94.00 | 11.75 |
| Thorax L distance (cm): for estimating SV | 39.07 | 6.91 | 36.00 | 12.00 |
| Thorax Zo impedance (Ω): for estimating SV | 50.71 | 9.13 | 55.50 | 14.70 |
| Arm circumference (cm): MUAC | 8.75 | 3.85 | 12.83 | 7.97 |
| Arm L distance (cm): for estimating SV | 16.47 | 3.66 | 16.00 | 3.50 |
| Arm Zo impedance (Ω): for estimating SV | 83.30 | 23.19 | 91.70 | 38.85 |
| Thorax-ICG Cases | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Mean | SD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| VET (ms) | 257 | 244 | 252 | 261 | 259 | 256 | 203 | 250 | 258 | 243 | 248.3 | 16.1 |
| RecAv(#) Process (# = Beats) | Chest-ECG SNR Mean Value (N = 9) | Chest-ECG SNR Mean Value (dB) | Arm-ECG SNR Mean Value (N = 9) | Arm-ECG SNR Mean Value (dB) | SNRdiff (dB): Thorax-Arm (SNRdB) |
|---|---|---|---|---|---|
| RecAv(16) | 106.3 | 40.5 | 13.1 | 22.3 | 18.2 |
| RecAv(32) | 194.4 | 45.8 | 39.4 | 31.9 | 13.9 |
| RecAv(64) | 256.0 | 48.2 | 64.4 | 36.2 | 12.0 |
| Case # → | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Thorax-ICG Db4 σoptim (µV) | 16 | 20 | 10 | 7.0 | 55 | 14 | 18 | 7.0 | 5.0 | 22 | 28 | 10 | 9.0 | 24 | 12 |
| Arm-ICG Db8 σoptim (µV) | 36 | 20 | 60 | 18 | 16 | 85 | 24 | 60 | 9.0 | 25 | 60 | 55 | 45 | 54 | 6.5 |
| Performance Metric on ICG | RAv36 | WavDb4/8 | RAv36 + WavDb4/8 |
|---|---|---|---|
| SNRincre-dB mean (±SD): Thorax-ICG, all beats | 20.72 (±4.69) | 0.42 (±0.89) | 16.03 (±4.38) |
| SNRincre-dB mean (±SD): Arm-ICG, all beats | 18.36 (±4.59) | −0.32 (±1.47) | 8.54 (±6.91) |
| SNRincre-dB median (IQR): Thorax-ICG, all beats | 19.56 (4.61) | 0.42 (0.71) | 15.84 (5.81) |
| SNRincre-dB median (IQR): Arm-ICG, all beats | 18.06 (6.61) | −0.94 (1.44) | 6.71 (8.08) |
| p mean (±SD): Thorax-ICG, all beats | 0.998 (±0.0018) | 0.963 (±0.0330) | 0.998 (±0.0022) |
| p mean (±SD): Arm-ICG, all beats | 0.952 (±0.0607) | 0.721 (±0.206) | 0.919 (±0.1050) |
| p median (IQR): Thorax-ICG all beats | 0.999 (0.0016) | 0.978 (0.0359) | 0.998 (0.0019) |
| p median (IQR): Arm-ICG all beats | 0.982 (0.0387) | 0.824 (0.318) | 0.9701 (0.0845) |
| BIR% mean (±SD): Thorax-ICG (BbyB) | 100.0 (±0.0) | 88.01 (±13.06) | 100.0 (±0.00) |
| BIR% mean (±SD): Arm-ICG (BbyB) | 80.89 (±24.17) | 26.69 (±29.95) | 67.31 (±32.95) |
| BIR% median (IQR): Thorax-ICG (BbyB) | 100.0 (0.0) | 93.62 (10.92) | 100.0 (0.00) |
| BIR% median (IQR): Arm-ICG (BbyB) | 92.86 (25.59) | 9.46 (42.13) | 81.12 (47.66) |
| Case # | IncBt Count (p > 0.95) | p IncBt Mean | IncBt BIR% (%) | A Mean (ms) | A SD (ms) | A Medn (ms) | A IQR (ms) | A ER% (%) | B Mean (Ω/s) | B SD (Ω/s) | B Medn (Ω/s) | B IQR (Ω/s) | B ER% (%) | C Mean (ms) | C SD (ms) | C Medn (ms) | C IQR (ms) | C ER% (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 462 | 0.991 | 93.5 | 466 | 3.21 | 466 | 3.50 | 0.520 | 0.483 | 0.052 | 0.472 | 0.068 | 8.49 | 88.9 | 3.43 | 89.0 | 5.00 | 3.03 |
| 2 | 120 | 0.968 | 20.9 | 469 | 5.48 | 470 | 8.50 | 1.082 | 0.214 | 0.046 | 0.210 | 0.087 | 19.0 | 81.2 | 8.31 | 78.5 | 9.13 | 7.77 |
| 3 | 393 | 0.984 | 64.5 | 511 | 7.93 | 509 | 10.5 | 1.351 | 0.151 | 0.026 | 0.150 | 0.024 | 14.2 | 96.3 | 6.00 | 96.0 | 7.00 | 4.71 |
| 4 | 639 | 0.992 | 100 | 514 | 5.79 | 517 | 9.50 | 0.957 | 0.199 | 0.024 | 0.200 | 0.032 | 9.90 | 104.8 | 5.78 | 104.0 | 10.0 | 4.55 |
| 5 | 386 | 0.988 | 92.1 | 514 | 4.13 | 515 | 4.00 | 0.597 | 0.521 | 0.069 | 0.511 | 0.120 | 10.8 | 92.3 | 4.61 | 91.5 | 4.50 | 3.48 |
| 6 | 272 | 0.968 | 50.9 | 475 | 6.54 | 475 | 11.0 | 1.437 | 0.208 | 0.067 | 0.182 | 0.109 | 24.1 | 89.3 | 7.08 | 89.8 | 10.5 | 6.20 |
| 7 | 394 | 0.986 | 91.8 | 486 | 4.31 | 487 | 6.00 | 0.709 | 0.264 | 0.023 | 0.266 | 0.029 | 6.64 | 92.6 | 3.25 | 93.0 | 3.50 | 2.73 |
| 8 | 188 | 0.972 | 46.5 | 449 | 6.37 | 449 | 10.5 | 1.206 | 0.181 | 0.037 | 0.185 | 0.051 | 18.1 | 77.8 | 4.68 | 76.8 | 5.50 | 4.60 |
| 9 | 542 | 0.993 | 98.7 | 468 | 4.12 | 469 | 5.00 | 0.682 | 0.199 | 0.021 | 0.192 | 0.035 | 8.88 | 90.4 | 3.01 | 90.0 | 4.50 | 2.83 |
| 10 | 455 | 0.984 | 93.1 | 513 | 5.33 | 513 | 10.0 | 0.948 | 0.352 | 0.024 | 0.346 | 0.034 | 5.40 | 88.0 | 2.52 | 87.5 | 2.50 | 2.28 |
| 11 | 400 | 0.980 | 76.3 | 479 | 4.74 | 479 | 7.00 | 0.809 | 0.186 | 0.024 | 0.183 | 0.032 | 10.3 | 91.6 | 6.67 | 90.0 | 9.00 | 5.91 |
| 12 | 444 | 0.986 | 93.7 | 495 | 3.48 | 496 | 5.50 | 0.608 | 0.265 | 0.019 | 0.267 | 0.023 | 6.17 | 77.2 | 2.63 | 77.5 | 4.00 | 2.94 |
| 13 | 624 | 0.994 | 100 | 505 | 3.47 | 505 | 4.50 | 0.536 | 0.255 | 0.025 | 0.254 | 0.034 | 8.02 | 85.8 | 2.45 | 85.5 | 3.50 | 2.23 |
| 14 | 486 | 0.984 | 98.4 | 480 | 4.54 | 480 | 5.00 | 0.695 | 0.149 | 0.028 | 0.146 | 0.035 | 14.7 | 84.5 | 5.13 | 84.8 | 8.50 | 5.22 |
| 15 | 468 | 0.998 | 92.9 | 463 | 2.26 | 463 | 3.00 | 0.388 | 0.397 | 0.008 | 0.397 | 0.010 | 1.83 | 90.5 | 1.48 | 90.5 | 2.00 | 1.40 |
| Mean | --> | 0.98 | 80.9 | 485.8 | 4.78 | 486 | 6.90 | 0.83 | 0.27 | 0.03 | 0.26 | 0.05 | 11.1 | 88.7 | 4.47 | 88.3 | 5.94 | 3.99 |
| Case # | IncBt Count (p > 0.95) | p IncBt Mean | IncBt BIR% (%) | A Mean (ms) | A SD (ms) | A Medn (ms) | A IQR (ms) | A ER% (%) | B Mean (Ω/s) | B SD (Ω/s) | B Medn (Ω/s) | B IQR (Ω/s) | B ER% (%) | C Mean (ms) | C SD (ms) | C Medn (ms) | C IQR (ms) | C ER% (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 494 | 0.999 | 100 | 436 | 1.32 | 436 | 1.50 | 0.25 | 1.24 | 0.027 | 1.24 | 0.034 | 1.66 | 110 | 1.98 | 110 | 2.50 | 1.42 |
| 2 | 619 | 0.997 | 100 | 428 | 2.82 | 429 | 3.00 | 0.25 | 2.05 | 0.182 | 2.08 | 0.138 | 5.66 | 109 | 3.61 | 110 | 3.00 | 2.17 |
| 3 | 612 | 0.997 | 100 | 478 | 3.25 | 479 | 3.50 | 0.49 | 1.86 | 0.083 | 1.85 | 0.138 | 3.82 | 110 | 1.73 | 111 | 1.50 | 1.12 |
| 4 | 634 | 0.999 | 100 | 486 | 1.86 | 486 | 2.00 | 0.31 | 1.72 | 0.022 | 1.72 | 0.030 | 1.04 | 113 | 1.36 | 114 | 1.50 | 0.89 |
| 5 | 434 | 0.997 | 100 | 469 | 2.84 | 469 | 3.50 | 0.48 | 2.85 | 0.229 | 2.91 | 0.322 | 6.93 | 112 | 4.01 | 111 | 3.50 | 2.34 |
| 6 | 544 | 0.995 | 100 | 465 | 4.18 | 466 | 5.00 | 0.70 | 0.91 | 0.107 | 0.91 | 0.088 | 7.39 | 117 | 5.23 | 117 | 5.63 | 3.30 |
| 7 | 319 | 0.999 | 100 | 460 | 2.09 | 460 | 3.00 | 0.37 | 1.35 | 0.054 | 1.36 | 0.072 | 3.14 | 110 | 1.49 | 110 | 2.50 | 1.08 |
| 8 | 419 | 10.00 | 100 | 451 | 1.13 | 451 | 1.00 | 0.19 | 1.47 | 0.038 | 1.45 | 0.065 | 2.24 | 115 | 0.67 | 116 | 1.00 | 0.46 |
| 9 | 539 | 0.999 | 100 | 443 | 2.85 | 443 | 3.50 | 0.49 | 1.18 | 0.044 | 1.18 | 0.077 | 3.18 | 128 | 3.60 | 127 | 5.00 | 2.29 |
| 10 | 444 | 0.998 | 100 | 468 | 2.18 | 468 | 2.50 | 0.41 | 2.10 | 0.028 | 2.10 | 0.039 | 1.10 | 104 | 2.30 | 104 | 3.00 | 1.74 |
| 11 | 554 | 0.999 | 100 | 423 | 1.39 | 424 | 1.50 | 0.24 | 1.36 | 0.091 | 1.33 | 0.107 | 5.50 | 99 | 1.81 | 99 | 2.38 | 1.40 |
| 12 | 484 | 0.998 | 100 | 473 | 2.33 | 473 | 3.00 | 0.39 | 2.50 | 0.055 | 2.49 | 0.044 | 1.57 | 109 | 0.97 | 109 | 1.00 | 0.70 |
| 13 | 564 | 0.999 | 100 | 468 | 1.52 | 469 | 2.50 | 0.27 | 1.46 | 0.100 | 1.42 | 0.138 | 5.67 | 110 | 2.32 | 109 | 3.50 | 1.75 |
| 14 | 504 | 0.993 | 100 | 470 | 5.40 | 470 | 7.00 | 0.92 | 0.68 | 0.052 | 0.68 | 0.061 | 5.90 | 141 | 5.84 | 141 | 8.50 | 3.43 |
| 15 | 452 | 0.999 | 100 | 452 | 1.83 | 452 | 3.00 | 0.34 | 1.84 | 0.053 | 1.85 | 0.080 | 2.51 | 109 | 1.12 | 109 | 1.50 | 0.78 |
| Mean | --> | 0.998 | 100 | 458 | 2.47 | 458 | 3.03 | 0.41 | 1.64 | 0.08 | 1.64 | 0.10 | 3.82 | 113 | 2.54 | 113 | 3.07 | 1.66 |
| Case # → | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | Mean | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Arm-ICG | BIR% at p > 0.95 (%) | 93.5 | 20.9 | 64.5 | 100 | 92.1 | 50.9 | 91.8 | 46.5 | 98.7 | 93.0 | 76.3 | 93.7 | 100 | 98.4 | 92.9 | 80.9 |
| SNRincre-dB mean (dB) | 19.0 | 23.3 | 26.1 | 18.1 | 16.7 | 13.4 | 15.8 | 17.4 | 12.6 | 10.4 | 22.1 | 19.8 | 24.5 | 21.7 | 14.7 | 18.4 | |
| VET mean (ms) | 194 | 227 | 202 | 217 | 192 | 200 | 206 | 186 | 200 | 190 | 185 | 173 | 187 | 195 | 224 | 198 | |
| VET SD (ms) | 18.5 | 22.3 | 9.73 | 7.79 | 10.4 | 15.5 | 17.7 | 16.1 | 11.3 | 10.7 | 17.9 | 22.2 | 12.6 | 13.2 | 7.30 | 14.2 | |
| VET median (ms) | 191 | 229 | 202 | 218 | 192 | 201 | 207 | 182 | 198 | 190 | 182 | 168 | 186 | 194 | 225 | 198 | |
| VET IQR (ms) | 14.0 | 17.3 | 11.5 | 12.5 | 14.4 | 17.6 | 19.3 | 16.5 | 17.5 | 8.50 | 14.5 | 12.8 | 9.50 | 16.8 | 11.0 | 14.2 | |
| VET ER% (%) | 6.03 | 6.87 | 3.65 | 3.00 | 4.36 | 6.78 | 7.49 | 6.22 | 4.60 | 4.22 | 6.15 | 6.76 | 3.63 | 5.35 | 3.25 | 5.2 | |
| VET/C (ratio) | 2.19 | 2.79 | 2.10 | 2.07 | 2.08 | 2.24 | 2.22 | 2.39 | 2.21 | 2.16 | 2.02 | 2.24 | 2.18 | 2.31 | 2.47 | 2.24 | |
| Base imp. Zo mean (Ω) | 76.4 | 60.2 | 93.6 | 46.7 | 116 | 91.7 | 54.9 | 54.5 | 57.9 | 113 | 109 | 97.1 | 92.3 | 98.7 | 87.3 | 83.3 | |
| LARM (cm) | 10.0 | 18.0 | 15.0 | 12.0 | 16.0 | 16.0 | 12.0 | 19.0 | 17.0 | 17.0 | 15.0 | 20.0 | 19.0 | 19.0 | 25.0 | 16.7 | |
| SV (cm3) | 0.24 | 0.65 | 0.12 | 0.43 | 0.29 | 0.19 | 0.39 | 0.61 | 0.51 | 0.23 | 0.10 | 0.29 | 0.30 | 0.16 | 1.09 | 0.37 | |
| Thorax-ICG | BIR% at p > 0.95 (%) | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| SNRincre-dB mean (dB) | 21.1 | 19.6 | 12.7 | 28.5 | 16.0 | 18.3 | 21.5 | 23.9 | 17.0 | 28.9 | 19.6 | 27.6 | 17.9 | 19.4 | 18.9 | 20.7 | |
| VET mean (ms) | 291 | 273 | 257 | 244 | 252 | 261 | 259 | 276 | 288 | 256 | 203 | 250 | 258 | 292 | 243 | 260 | |
| VET SD (ms) | 1.22 | 8.53 | 6.45 | 3.39 | 3.48 | 10.92 | 3.03 | 2.24 | 4.42 | 1.30 | 2.19 | 2.78 | 5.29 | 12.97 | 2.85 | 4.74 | |
| VET median (ms) | 291 | 274 | 259 | 244 | 252 | 262 | 259 | 277 | 288 | 256 | 204 | 250 | 259 | 297 | 244 | 261 | |
| VET IQR (ms) | 1.50 | 2.50 | 4.50 | 4.00 | 4.50 | 10.0 | 5.00 | 3.50 | 7.50 | 1.50 | 3.50 | 3.00 | 6.00 | 10.5 | 3.50 | 4.73 | |
| VET ER% (%) | 0.31 | 1.68 | 1.73 | 1.06 | 1.11 | 2.84 | 1.01 | 0.72 | 1.35 | 0.42 | 0.88 | 0.83 | 1.65 | 2.31 | 0.91 | 1.25 | |
| VET/C (ratio) | 2.64 | 2.49 | 2.32 | 2.15 | 2.25 | 2.22 | 2.35 | 2.39 | 2.25 | 2.46 | 2.05 | 2.30 | 2.36 | 2.08 | 2.24 | 2.30 | |
| Base imp. Zo mean (Ω) | 56.0 | 56.6 | 60.7 | 42.9 | 56.9 | 57.8 | 38.9 | 38.8 | 37.6 | 55.5 | 66.2 | 46.4 | 56.0 | 49.1 | 41.2 | 50.7 | |
| LTHORX (cm) | 35.0 | 36.0 | 32.0 | 36.0 | 38.0 | 32.0 | 36.0 | 31.0 | 49.0 | 32.0 | 47.0 | 39.0 | 44.0 | 48.0 | 51.0 | 39.1 | |
| SV (cm3) | 21.1 | 33.8 | 19.9 | 44.4 | 48.0 | 10.9 | 44.9 | 74.7 | 86.7 | 26.8 | 21.0 | 66.2 | 35.0 | 28.5 | 103 | 44.3 |
| Comparative Metric | Mean | SD | Median | IQR |
|---|---|---|---|---|
| D = [Arm(B)/Thorax(B)] (%) | 17.4 | 7.51 | 16.8 | 8.63 |
| E= [Thorax(C) − Arm(C)] (ms) | 24.4 | 12.7 | 21.3 | 12.9 |
| F= [Thorax( C)/Arm(C)] (ratio) | 1.28 | 0.16 | 1.24 | 0.19 |
| G= [Thorax(VET)/Arm(VET)] (ratio) | 1.32 | 0.14 | 1.31 | 0.21 |
| H = [Thorax(SV)/Arm(SV)] (ratio) | 132.8 | 52.8 | 118.7 | 70.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Escalona, O.; Cullen, N.; Weli, I.; McCallan, N.; Ng, K.Y.; Finlay, D. Robust Arm Impedocardiography Signal Quality Enhancement Using Recursive Signal Averaging and Multi-Stage Wavelet Denoising Methods for Long-Term Cardiac Contractility Monitoring Armbands. Sensors 2023, 23, 5892. https://doi.org/10.3390/s23135892
Escalona O, Cullen N, Weli I, McCallan N, Ng KY, Finlay D. Robust Arm Impedocardiography Signal Quality Enhancement Using Recursive Signal Averaging and Multi-Stage Wavelet Denoising Methods for Long-Term Cardiac Contractility Monitoring Armbands. Sensors. 2023; 23(13):5892. https://doi.org/10.3390/s23135892
Chicago/Turabian StyleEscalona, Omar, Nicole Cullen, Idongesit Weli, Niamh McCallan, Kok Yew Ng, and Dewar Finlay. 2023. "Robust Arm Impedocardiography Signal Quality Enhancement Using Recursive Signal Averaging and Multi-Stage Wavelet Denoising Methods for Long-Term Cardiac Contractility Monitoring Armbands" Sensors 23, no. 13: 5892. https://doi.org/10.3390/s23135892
APA StyleEscalona, O., Cullen, N., Weli, I., McCallan, N., Ng, K. Y., & Finlay, D. (2023). Robust Arm Impedocardiography Signal Quality Enhancement Using Recursive Signal Averaging and Multi-Stage Wavelet Denoising Methods for Long-Term Cardiac Contractility Monitoring Armbands. Sensors, 23(13), 5892. https://doi.org/10.3390/s23135892