
Improvement in Quality of Life with Use of Ambient-Assisted Living: Clinical Trial with Older Persons in the Chilean Population



Abstract
1. Introduction
2. Use of Assisted Environments for Older Adults
3. Studies with Sensors in Older Adults
4. Materials and Methods
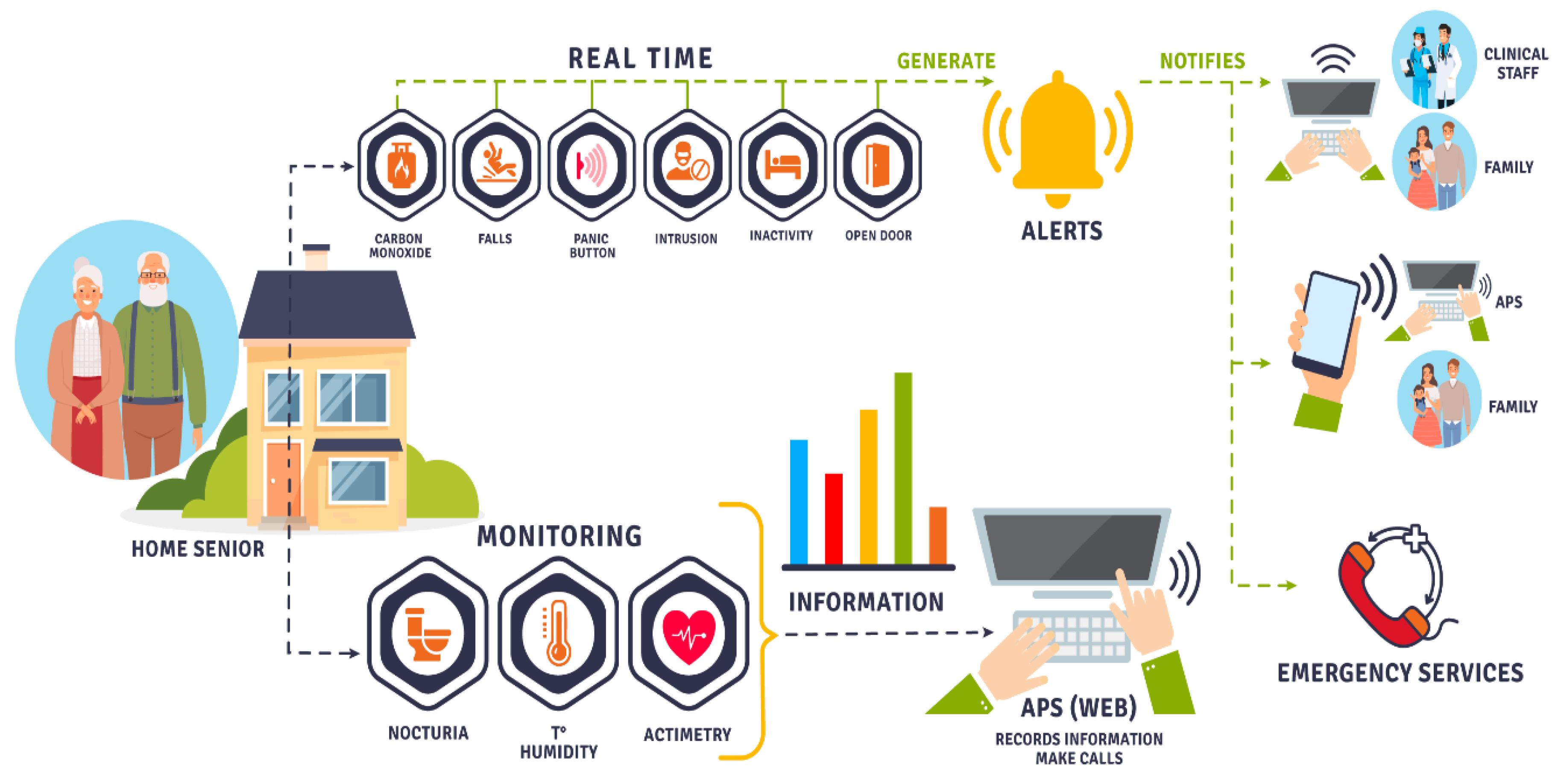
- Monitoring of environmental variables: MQ-9 sensor for gas detection. This sensor detects gas concentrations from 100 ppm to 10,000 ppm. DHT11 sensor to measure humidity and temperature. This sensor measures a temperature range from 0 °C to 50 °C with an accuracy of 0.2 °C and 20% to 90% relative humidity with 5% accuracy.
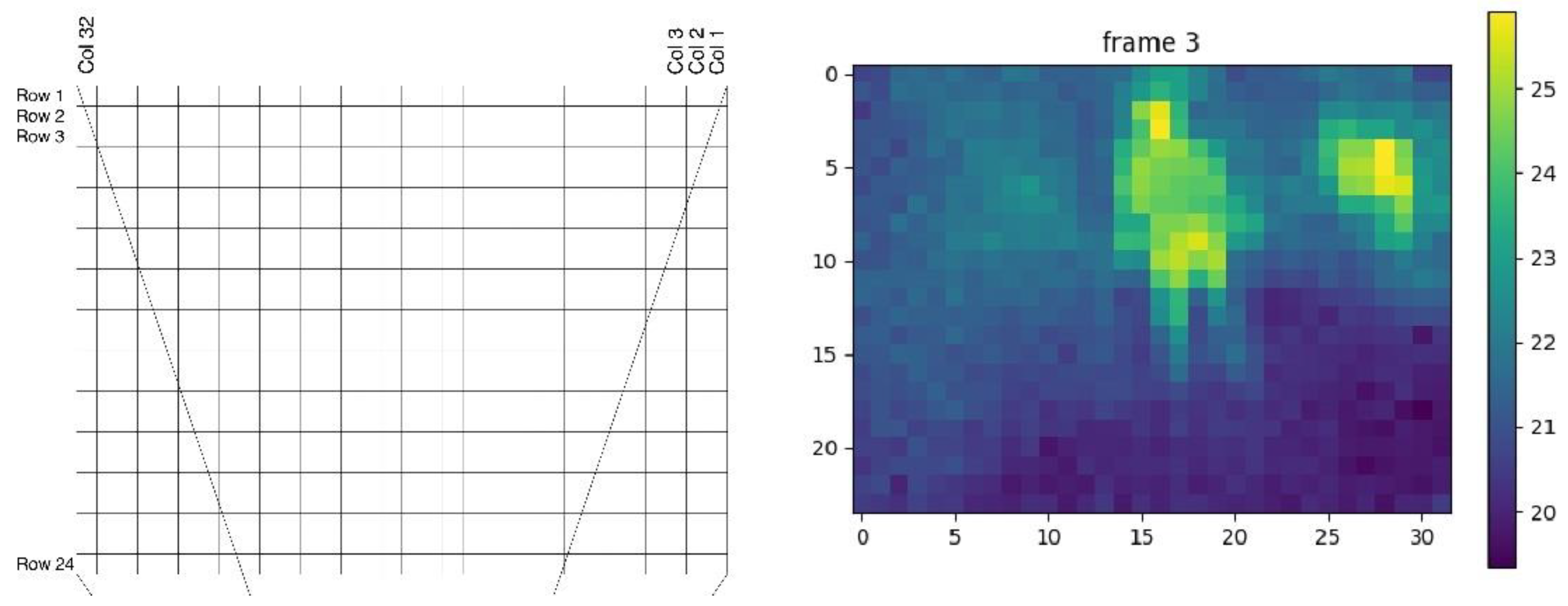
- Accident monitoring: Raspberry microcontroller with MLX90640 thermal sensor for fall detection. The sensor is a 32 × 24 pixel thermal infrared array that has a temperature range of −40 °C to 85 °C. The values are transmitted via I2C and received by the raspberry to be processed.
- Activity monitoring: To assess actimetry (or actigraphy) within the home. We used the Aeotec ZWA005 Trisensor, which has the ability to detect the presence and displacement of a person in a room through the measurement of movement, temperature and light. This sensor measures a temperature range of −15 to 50 °C with 1 °C accuracy, from 0 to 22,595 lux with 30 lux accuracy and a maximum of 7 m of motion sensitivity. It is also possible to monitor activity using the fall sensor (Raspberry + MLX90640), detecting presence and movement through heat variation in the room. The system also makes it possible to evaluate nocturia. For this, conductivity electrodes were used, which correspond to steel plates installed in the toilet and allow for the detection of urination events through the change in conductivity in the water.
5. Results
5.1. Actimetry
5.2. Impact on Behavior Pattern
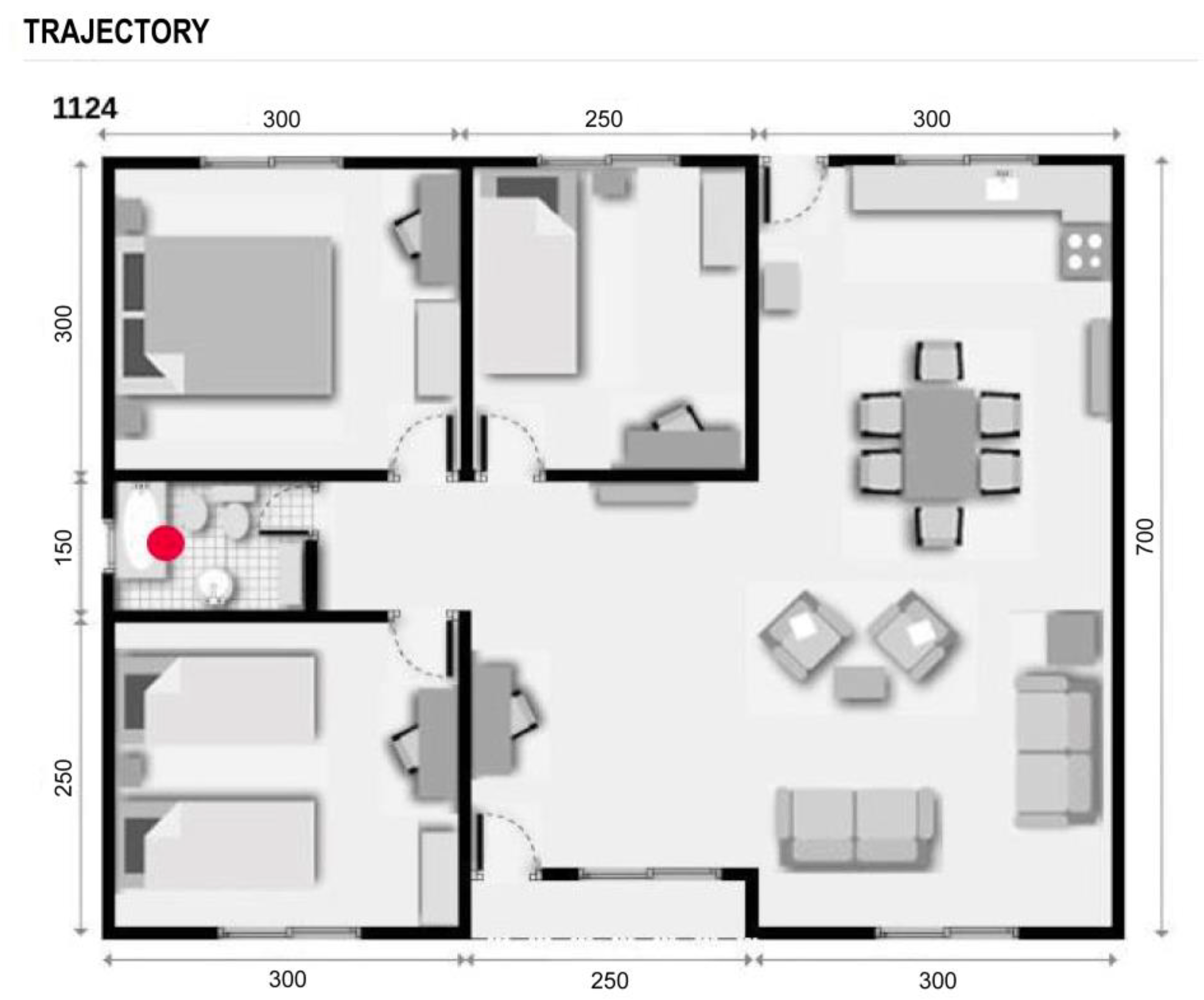
5.2.1. Positioning and Trajectories
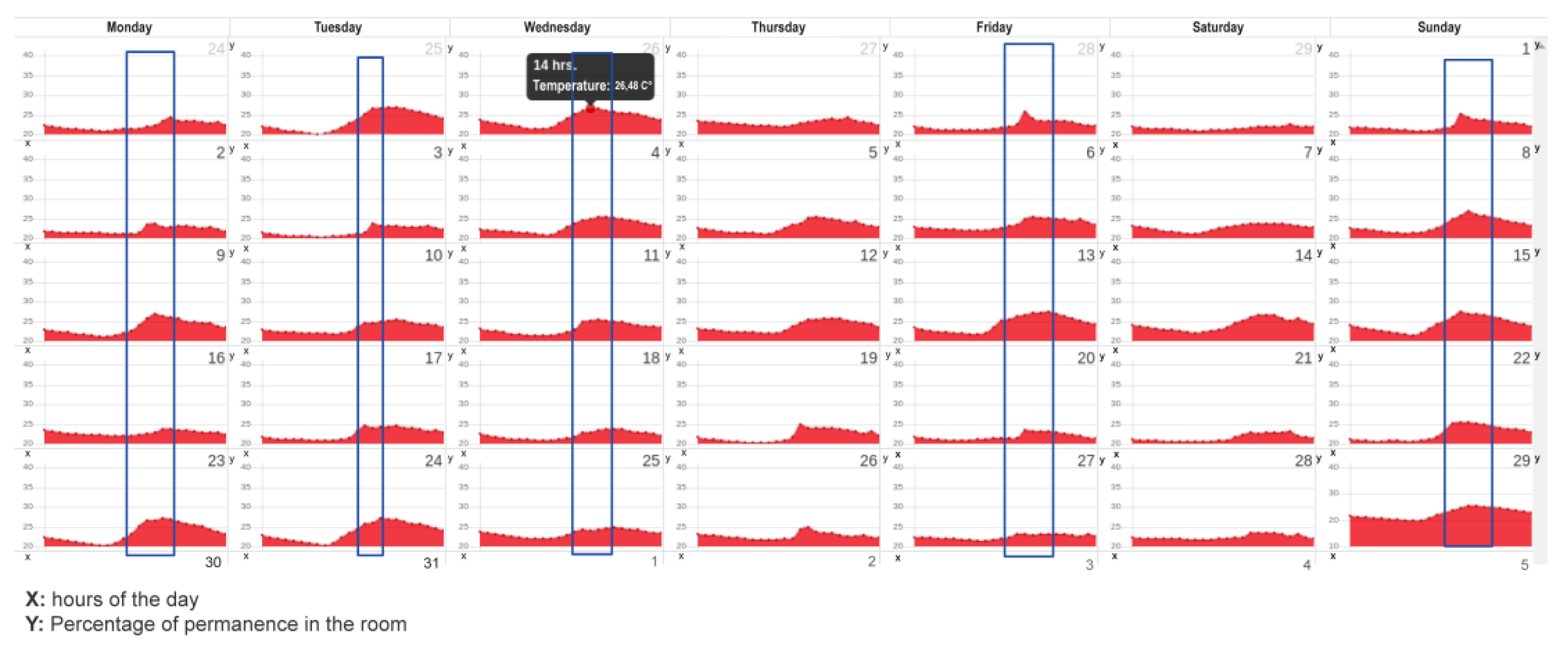
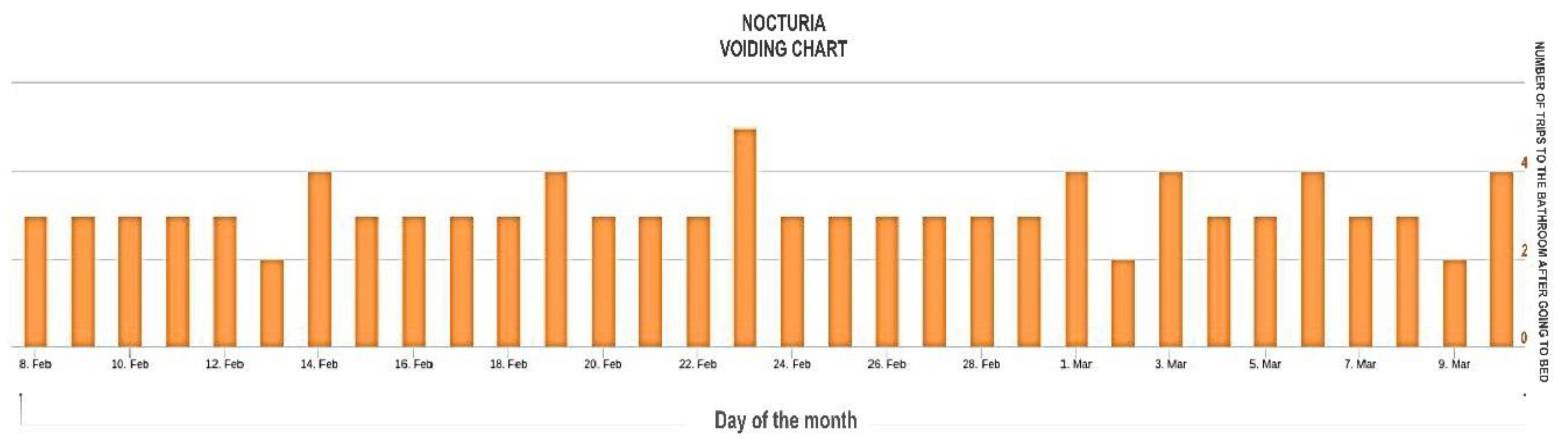
5.2.2. Night Activity
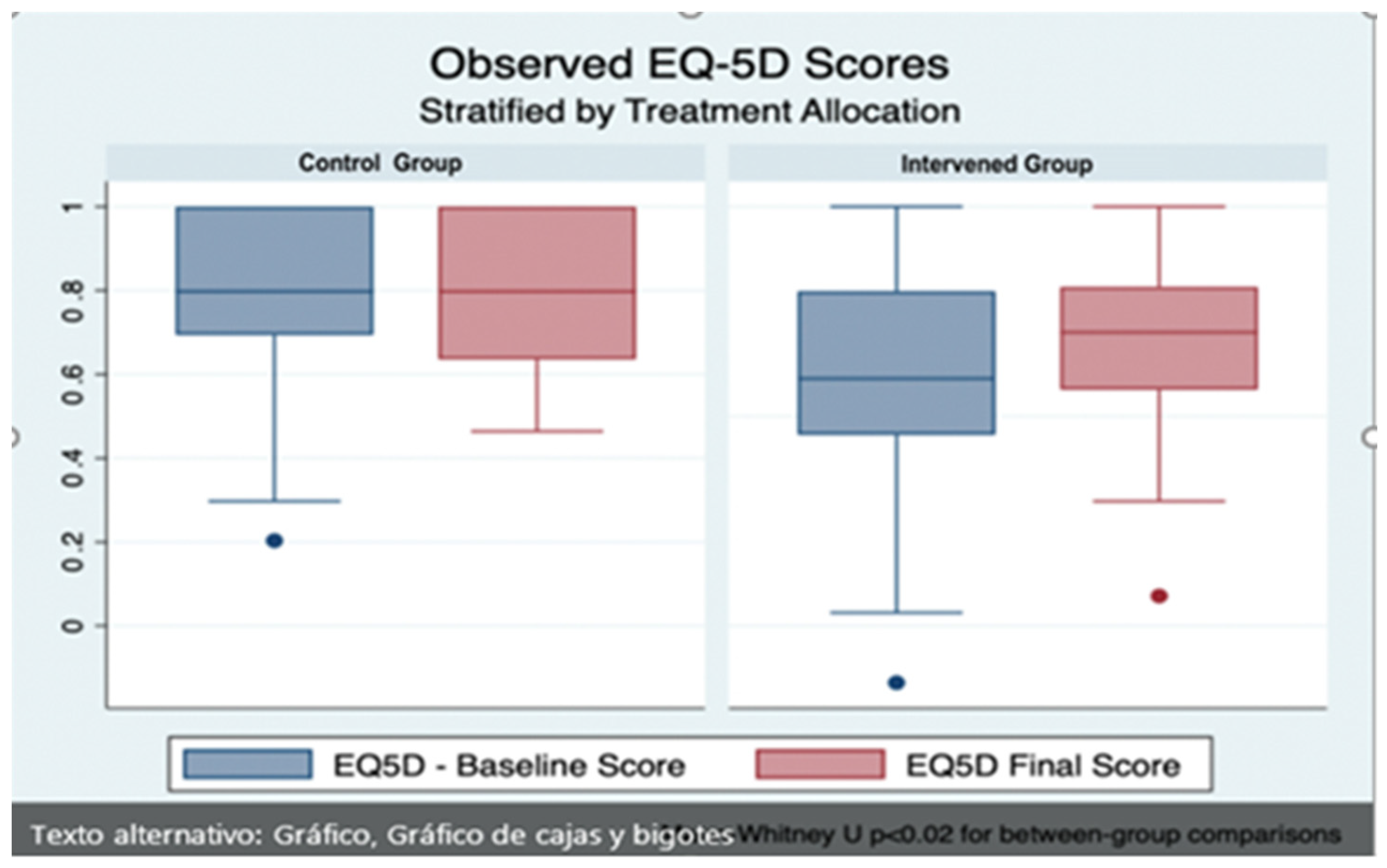
5.3. Impact of the Intervention on Quality of Life
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Engineer, A.; Sternberg, E.; Najafi, B. Designing interiors to mitigate physical and cognitive deficits related to aging and to promote longevity in older adults: A review. Gerontology 2018, 64, 612–622. [Google Scholar] [CrossRef]
- United Nations; ECLAC. Human Rights of the Elderly in Chile in Times of Pandemic: Promotion Actions from the National Service of the Elderly (SENAMA). Internet December 2021. Available online: https://bit.ly/3byyvfs (accessed on 20 June 2022).
- Ministry of Social Development. Older Adults Synthesis of Results. Casen 2017. Available online: https://bit.ly/3NvWRne (accessed on 20 June 2022).
- Association of Municipalities of Chile (AMUCH). Chile Will Become the Second Country in Latin America with the Highest Percentage of Older Adults. Internet March 2017. Available online: https://bit.ly/3jOqELS (accessed on 20 June 2022).
- United Nations; ECLAC. Ageing, Older People and the 2030 Agenda for Sustainable Development Regional and Human Rights Perspective. 2018. Available online: https://bit.ly/2CYprgl (accessed on 20 June 2022).
- Chile and its Elders. Results of the V National Survey of Quality of Life in Old Age 2019. Pontificia Universidad Católica de Chile and Caja Los Andes. 2020. Available online: https://bit.ly/3vXjWrQ (accessed on 30 June 2022).
- Library of Congress. The Andes. Communal Report 2020. Available online: https://bit.ly/3mvvJe5 (accessed on 1 July 2022).
- World Health Organization (WHO). Decade of Healthy Aging (2020–2030). Available online: https://bit.ly/3CvQrQy (accessed on 15 September 2021).
- Rodrigo, T.-C.; Cristian, C.; Jordi, V.; Roberto, V.-U.; Marcelo, C.-C.; Diego, V. Evaluation of physical activity in patients with chronic obstructive pulmonary disease. Rev. Médica De Chile 2017, 145, 1588–1596. [Google Scholar] [CrossRef]
- National Health Survey 2016–2017. First Results. Available online: https://bit.ly/3jQO43c (accessed on 15 September 2022).
- National Service for the Elderly (SENAMA). SENAMA Promotes the Physical Exercise of Quarantined Seniors through Innovative Multifunctional Exercise Program 2020. Available online: https://bit.ly/3vWXJKJ (accessed on 1 July 2022).
- World Health Organization. Falls. Available online: https://bit.ly/2KYMWrX (accessed on 30 June 2022).
- Ginarte, M.; Santiesteban, R. Importance of Physical Exercise In the Health of the Elderly. Cuba. J. Phys. Med. Rehabil. 2012, 4, 125–134. Available online: https://bit.ly/3EumalM (accessed on 1 July 2022).
- Falck, R.; Davis, J.; Khan, K.; Handy, T.; Liu-Ambrose, T. A wrinkle in measuring time uses for cognitive health: How should we measure physical activity, sedentary behavior and sleep? Am. J. Lifestyle Med. 2021, 15598276211031495. [Google Scholar] [CrossRef]
- SENAMA. Condominium Program of Sheltered Housing. 2022. Available online: http://www.senama.gob.cl/storage/docs/Guia_CVT_2019.pdf (accessed on 20 June 2022).
- World Health Organization. The Global Embrace. WHO Campaign for Active Ageing. 2001. Available online: https://bit.ly/3BtwYyB (accessed on 30 June 2022).
- World Health Organization. Frequently Asked Questions. Available online: https://bit.ly/3pexGMt (accessed on 1 July 2022).
- Gallardo-Peralta, L.; Jorquera, I.; Morán, M.; Quiroz, B. Gender Differences in Health and Quality of Life in Older People in Northern Chile. Polis. Rev. Latinoam. 2018, 49. Available online: https://bit.ly/3bKkbRo (accessed on 1 July 2022).
- Silva, S.; Martins, H.; Valente, A.; Soares, S. A bluetooth approach to diabetes sensing on ambient assisted living systems. Procedia Comput. Sci. 2012, 14, 181–188. [Google Scholar] [CrossRef]
- Aminoff, M.J.; Daroff, R.B. Encyclopedia of the Neurological Sciences, 2nd ed.; J. Krishna, S., Mashaqi, A., Eds.; Academic Press: Cambridge, MA, USA, 2014; pp. 36–40. ISBN 9780123851581. [Google Scholar] [CrossRef]
- Ochoa-Vázquez, J.; Cruz-Ortiz, M.; del Carmen Pérez-Rodríguez, M.; Cuevas-Guerrero, C.E. Aging: A look at the demographic transition and its implications for health care. Rev. De Enfermería 2018, 26, 273–280. Available online: https://bit.ly/3XyODBe (accessed on 20 June 2022).
- Padial Espinosa, M.; Pinzón Pulido, S.; Espinosa Almendro, J.M.; Kalache, A.; Garrido Peña, F. Longevidad y revolución digital. Contribución de las tecnologías de la información y de la comunicación al envejecimiento saludable. Gerokomos 2020, 31, 6–14. Available online: https://bit.ly/3gDwstt (accessed on 30 June 2022).
- Ramos, R.G.; Domingo, J.D.; Zalama, E.; Gómez-García-Bermejo, J.; López, J. SDHAR-HOME: A sensor dataset for human activity recognition at home. Sensors 2022, 22, 8109. [Google Scholar] [CrossRef]
- Chua, S.; Foo, L.K.; Hans, W.; Guesgen, S.M. Incremental learning of human activities in smart homes. Sensors 2022, 22, 8458. [Google Scholar] [CrossRef]
- Momin, S.; Sufian, A.; Barman, D.; Dutta, P.; Dong, M.; Leo, M. In-home older adults’ activity pattern monitoring using depth sensors: A review. Sensors 2022, 22, 9067. [Google Scholar] [CrossRef]
- Pirzada, P.; Wilde, A.; Doerty, H.; Harris-Britill, D. Ethics and acceptance of smart homes for older adults. Inform. Health Soc. Care 2022, 47, 10–37. [Google Scholar] [CrossRef]
- Haddad, Y.K.; Bergen, G.; Florence, C. Estimating the economic burden related to older adult falls by state. J. Public Health Manag. Pract. 2019, 25, E17–E24. [Google Scholar] [CrossRef]
- Patel, M.; Pavic, A.; Goodwin, V. Wearable inertial sensors to measure gait and posture characteristic differences in older adult fallers and non-fallers: A scoping review. Gait Posture 2020, 76, 110–112. [Google Scholar] [CrossRef]
- González-Olguín, A.; Ramos, D.; Higueras, F.; Martínez, L.; Taramasco Robles, D. Classification of center of mass acceleration patterns in older people with knee osteoartritis and fear of falling. Int. J. Environ. Res. Public Health 2002, 19, 12890. [Google Scholar] [CrossRef]
- Demongeot, J.G.; Elena, A.; Jelassi, M.; Miled, S.B.; Bellamine, S.; Taramasco, C. Smart Homes and Sensors for Surveillance and Preventive Education at Home: Example of Obesity. Information 2016, 7, 50. [Google Scholar] [CrossRef]
- Taramasco, C.; Rodenas, F.; Martinez, P.; Fuentes RMunoz, R.; Olivares, R.; de Alburquerque, V.; Demongeot, J.G. A novel monitoring system for fall detection in older people. IEEE Access 2018, 6, 43563–43574. [Google Scholar] [CrossRef]
- Taramasco, C.; Rodenas, T.; Martinez, F.; Fuentes, P.; Muñoz, R.; Olivares, R.; de Alburquerque, V.; Demongeot, J.G. A Novel Low-Cost Sensor Prototype for Nocturia Monitoring in Older People. IEEE Access 2018, 6, 52500–52509. [Google Scholar] [CrossRef]
- Riquelme, F.; Espinoza, C.; Rodenas, T.; Minonzio, J.G.; Taramasco, C. eHomeSeniors Dataset: An Infrared Thermal Sensor Dataset for Automatic Fall Detection Research. Sensors 2019, 19, 4565. [Google Scholar] [CrossRef]
- Taramasco, C.; Lazo, Y.; Rodenas, T.; Fuentes, P.; Martínez, F.; Demongeot, J. System design for emergency alert triggered by falls using convolutional neural networks. J. Med. Syst. 2020, 44, 1–13. [Google Scholar] [CrossRef]
- Marquez, G.; Taramasco, C.; Astudillo, H.; Zalc, V.; Istrate, D. Involving Stakeholders in the Implementation of Microservice-Based Systems: A Case Study in an Ambient-Assisted Living System. IEEE Access 2021, 9, 9411–9428. [Google Scholar] [CrossRef]
- Márquez, G.; Veloz, A.; Minonzio, J.G.; Reyes, C.; Calvo, E.; Taramasco, C. Using Low-Resolution Non-Invasive Infrared Sensors to Classify Activities and Falls in Older Adults. Sensors 2022, 22, 2321. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Soto, A.; Gómez-Ramírez, E. Condiciones de salud y factores relacionados con discapacidad en adultos mayores -Una reflexión para la atención-. Univ. Y Salud 2018, 20, 270–282. [Google Scholar] [CrossRef]
- Woznowski, P.; Fafoutis, X.; Song, T.; Hannuna, S.; Camplani, M.; Tao, L.; Craddock, I. A multi-modal sensor infrastructure for healthcare in a residential environment. In Proceedings of the 2015 IEEE International Conference on Communication Workshop (ICCW), London, UK, 8–12 June 2015; pp. 271–277. [Google Scholar]
- Mainetti, L.; Mighali, V.; Patrono, L.; Rametta, P.; Stefanizzi, M.L. An IoT-aware system for elderly monitoring. In Proceedings of the 2017 IEEE 3rd International Forum on Research and Technologies for Society and Industry (RTSI), Modena, Italy, 11–13 September 2017; pp. 1–5. [Google Scholar]
- Al-Adhab, A.; Altmimi, H.; Alhawashi, M.; Alabduljabbar, H.; Harrathi, F.; Almubarek, H. IoT for remote elderly patient care based on Fuzzy logic. In Proceedings of the 2016 International Symposium on Networks, Computers and Communications (ISNCC), Yasmine Hammamet, Tunisia, 11–13 May 2016; pp. 1–5. [Google Scholar]
- Hail, M.A.; Fischer, S. IoT for AAL: An Architecture via Information-Centric Networking. In Proceedings of the 2015 IEEE Globecom Workshops (GC Wkshps), San Diego, CA, USA, 6–10 December 2015; pp. 1–6. [Google Scholar]
- WHO. Demencia. Available online: https://bit.ly/3VlCP2H (accessed on 1 July 2022).
- Botia, J.A.; Villa, A.; Palma, J. Ambient Assisted Living system for in-home monitoring of healthy independent elders. Expert Syst. Appl. 2012, 39, 8136–8148. [Google Scholar] [CrossRef]
- Thakur, N.; Chia, H. Pervasive Activity Logging for Indoor Localization in Smart Homes. In Proceedings of the 2021 4th International Conference on Data Science and Information Technology, Shanghai, China, 23–25 July 2021; pp. 246–255. [Google Scholar] [CrossRef]
- Abtoy, A.; Touhafi, A.; Tahiri, A. Ambient Assisted living system’s models and architectures: A survey of the state of the art. J. King Saud Univ.-Comput. Inf. Sci. 2020, 32, 1–10. [Google Scholar] [CrossRef]
- Rashidi, P.; Mihailidis, A. A survey on ambient-assisted living tools for older adults. IEEE J. Biomed. Health Inform. 2012, 17, 579–590. [Google Scholar] [CrossRef]
- Ghayvat, H.; Awais, M.; Pandya, S.; Ren, H.; Akbarzadeh, S.; Chandra Mukhopadhyay, S.; Chen, W. Smart Aging System: Uncovering the Hidden Wellness Parameter for Well-Being Monitoring and Anomaly Detection. Sensors 2019, 19, 766. [Google Scholar] [CrossRef]
- Susnea, I.; Dumitriu, L.; Talmaciu, M.; Pecheanu, E.; Munteanu, D. Unobtrusive Monitoring the Daily Activity Routine of Elderly People Living Alone, with Low-Cost Binary Sensors. Sensors 2019, 19, 2264. [Google Scholar] [CrossRef]
- Montoliu, R.; Sansano, E.; Gascó, A.; Belmonte, O.; Caballer, A. Indoor Positioning for Monitoring Older Adults at Home: Wi-Fi and BLE Technologies in Real Scenarios. Electronics 2020, 9, 728. [Google Scholar] [CrossRef]
- Ren, L.; Peng, Y. Research of Fall Detection and Fall Prevention Technologies: A Systematic Review. IEEE Access 2019, 7, 77702–77722. [Google Scholar] [CrossRef]
- Seoane, B.; de la Iglesia, F.; Nicolás, R.; Ramos, V.; Pellicer, C.; Diz-Lois, F. Factor analysis of health related quality of life in patients admitted to a short stay medical unit. Rev. Médica De Chile 2009, 137, 1163–1172. Available online: https://bit.ly/3XRoii3 (accessed on 30 June 2022).
- Selva-Sevilla, C.; Ferrara, P.; Gerónimo-Pardo, M. Interchangeability of the EQ-5D and the SF-6D, and comparison of their psychometric properties in a spinal postoperative Spanish population. Eur. J. Health Econ. 2020, 21, 649–662. [Google Scholar] [CrossRef] [PubMed]
- Tsang, H.H.L.; Cheung, J.P.Y.; Wong, C.K.H.; Cheung, P.W.H.; Lau, C.S.; Chung, H.Y. Psychometric validation of the EuroQoL 5-dimension (EQ-5D) questionnaire in patients with spondyloarthritis. Arthritis Res. Ther. 2019, 30, 41. [Google Scholar] [CrossRef] [PubMed]
- Młyńczak, K.; Golicki, D. Validity of the EQ-5D-5L questionnaire among the general population of Poland. Qual. Life Res. 2021, 30, 817–829. [Google Scholar] [CrossRef]
- Zarate, V.; Kind, P.; Valenzuela, P.; Vignau, A.; Olivares-Tirado, P.; Munoz, A. Social valuation of EQ-5D health states: The Chilean case. Value Health 2011, 14, 1135–1141. [Google Scholar] [CrossRef]
- Grant, L.A.; Rockwood, T.; Stennes, L. Client Satisfaction with Telehealth in Assisted Living and Homecare. Telemed. J. E-Health 2015, 21, 987–991. [Google Scholar] [CrossRef]
- Torkamani, M.; McDonald, L.; Saez Aguayo, I.; Kanios, C.; Katsanou, M.N.; Madeley, L.; Limousin, P.D.; Lees, A.J.; Haritou, M.; ALADDIN Collaborative Group; et al. A randomized controlled pilot study to evaluate a technology platform for the assisted living of people with dementia and their carers. J. Alzheimer’s Dis. 2014, 41, 515–523. [Google Scholar] [CrossRef]
- Fahad, L.; Tahir, S. Activity recognition and anomaly detection in smart homes. Neurocomputing 2021, 423, 362–372. [Google Scholar] [CrossRef]
- Alarifi, A.; Alwadain, A. Killer heuristic optimized convolution neural network-based fall detection with wearable IoT sensor devices. Measurement 2021, 167, 108258. [Google Scholar] [CrossRef]
- Al-Okby, M.; Al-Barrak, S. New approach for fall detection system using embedded technology. In Proceedings of the IEEE 24th International Conference on Intelligent Engineering Systems (INES), Reykjavík, Iceland, 8–10 July 2020; pp. 209–214. Available online: https://bit.ly/3bQhhL3 (accessed on 1 July 2022).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Control Group (n = 32) | Intervention Group (n = 37) | Total (n = 69) | p-Value |
|---|---|---|---|---|
| Clinical Characteristics | ||||
| Mean age (years) (SD) | 67.8 ± 8.5 | 70.8 ± 6.5 | 69.4 ± 7.6 | 0.11 1 |
| Female sex (n, %) | 26 (81.3%) | 29 (78.4%) | 55 (79.7%) | >0.99 2 |
| Asthma (n, %) | 2 (6.3%) | 4 (10.8%) | 6 (8.7%) | 0.68 2 |
| Chronic obstructive pulmonary disease (n, %) | 1 (3.1%) | 1 (2.7%) | 2 (2.9%) | >0.99 2 |
| Arterial hypertension (n, %) | 20 (62.5%) | 30 (81.1%) | 50 (72.5%) | 0.11 2 |
| Diabetes mellitus (n, %) | 10 (31.3%) | 14 (37.8%) | 24 (34.8%) | 0.62 2 |
| Depression (n, %) | 3 (9.4%) | 4 (10.8%) | 7 (10.1%) | >0.99 2 |
| Hypothyroidism (n, %) | 3 (9.4%) | 6 (16.2%) | 9 (13.0%) | 0.49 2 |
| Heart failure (n, %) | 3 (9.4%) | 5 (13.5%) | 8 (11.6%) | 0.72 2 |
| Ischemic Stroke (n, %) | 2 (6.3%) | 1 (2.7%) | 3 (4.4%) | 0.59 2 |
| Osteoarthritis (n, %) | 11 (34.4%) | 16 (43.2%) | 27 (39.1%) | 0.47 2 |
| Clinical Evaluation Scales | ||||
| Median Minimental State Evaluation Score (IQR) | 30 (27–30) | 29 (27–30) | 29 (27–30) | 0.27 3 |
| Median Barthel Index Score (IQR) | 100 (100) | 100 (100) | 100 (100) | 0.98 3 |
| Median Lawton Index Score (IQR)) | 8 (8) | 8 (8) | 8 (8) | 0.85 3 |
| Median EQ5D Baseline Score (IQR) | 0.798 (0.694–1.0) | 0.590 (0.456–0.798) | 0.698 (0.590–0.800) | <0.01 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taramasco, C.; Rimassa, C.; Martinez, F. Improvement in Quality of Life with Use of Ambient-Assisted Living: Clinical Trial with Older Persons in the Chilean Population. Sensors 2023, 23, 268. https://doi.org/10.3390/s23010268
Taramasco C, Rimassa C, Martinez F. Improvement in Quality of Life with Use of Ambient-Assisted Living: Clinical Trial with Older Persons in the Chilean Population. Sensors. 2023; 23(1):268. https://doi.org/10.3390/s23010268
Chicago/Turabian StyleTaramasco, Carla, Carla Rimassa, and Felipe Martinez. 2023. "Improvement in Quality of Life with Use of Ambient-Assisted Living: Clinical Trial with Older Persons in the Chilean Population" Sensors 23, no. 1: 268. https://doi.org/10.3390/s23010268
APA StyleTaramasco, C., Rimassa, C., & Martinez, F. (2023). Improvement in Quality of Life with Use of Ambient-Assisted Living: Clinical Trial with Older Persons in the Chilean Population. Sensors, 23(1), 268. https://doi.org/10.3390/s23010268