1. Introduction
As audiences across the world tuned in to watch the Paralympic Games, they saw athletes using impressive para-sport equipment such as high-technology wheelchairs, prosthetic limbs, and other assistive technology [
1,
2,
3,
4]. For sports played by people with disabilities, research and development of sports equipment according to the events, the sites and degrees of disability, physique, and other conditions are accelerating worldwide [
5,
6,
7,
8,
9,
10,
11]. Although the characteristics of such research and development are rarely disclosed to the public, the results are expected to be developed eventually into commercial products [
12,
13].
The research and development for competitive wheelchairs has also considered lighter and stronger materials such as aluminum, titanium, and carbon [
14]. Differences in frame materials and hand-rim shape alone have led to great differences in mechanical workload and exercise physiology [
15,
16,
17]. Furthermore, competition-specific sports wheelchairs must be configured and adapted in numerous ways to suit an athlete’s physical impairments and to improve performance and comfort. Physical disability types include limb deficiency, impaired muscle power, impaired range of movement, ataxia, and athetosis. Wheelchair hand-rim operation requires arm and hand muscle function. Individuals with disabilities in one arm or hand exhibit markedly lower performance than users of two arms [
18]. Conventionally used manual wheelchairs require long and intensive periods of use and control of two arms until proper hand-rim operation can be achieved. Therefore, some adaptation is necessary for users with asymmetrical arm use. Moreover, propelling a wheelchair with one arm during competition is an even more difficult task when pushing a hand-rim with two hands. Some such individuals with disabilities often require one-arm drive wheelchairs [
19,
20]. Nevertheless, only a few reports of the relevant literature describe studies related to one-arm driven wheelchairs; even these reports have contents related to driving systems or persons with hemiplegic disabilities [
21,
22,
23,
24,
25,
26]. No research report describes such a system for competitive wheelchairs.
This study was conducted to examine a competitive wheelchair for practical application, operable by moving straight ahead with only one arm, which will allow participation in sports. The wheelchair with a dual hand-rim system we developed has two hand-rims attached to the drive wheel on one side [
27,
28]. A user moves in a straight line by gripping both hand-rims simultaneously with one hand. Alternatively, a user can turn using a single hand-rim. The wheelchair presents the added benefit that it can be operated with one arm, even for movements during competition, to execute sudden stops and starts: stop-and-go motion. Such maneuverability enables one-arm movements such as going forwards, backwards, turning, and stopping, which can be done using propulsion with two arms. The results can support many possibilities: for example, if a competitor who still has function of two arms uses this wheelchair, then the wheelchair could be used to drive straight ahead using the same sports motion as that of an athlete holding a racket in one hand while operating the dual hand-rim; also, athletes who can move only one arm can operate the wheelchair just as one might operate a regular dual-arm wheelchair. Sports motions of this kind were not possible with conventional hand-rim operation. The benefits obtained from this study can support and improve athletes’ operations and competitive skills.
Despite the benefits explained above, no report of the relevant literature has described a study of competitive wheelchairs equipped with dual hand-rim systems. Consequently, many unanswered questions remain about loads on the body during hand-rim operation and the loads’ effects on user posture. Once these issues are resolved, it will clarify the conditions of compatibility with the competition and will also allow for training according to the site and degree of disability. Our competitive wheelchair with dual hand-rim system will have a different hand-rim operation than existing competition wheelchairs. Therefore, as a preliminary step in the investigation under subdivided conditions, the first step is necessary to clarify the differences in general muscle activation and movement posture by comparing one-arm with two-arm during the simplest straight-ahead movement. This is because differences in seat height and axle position are known to affect propulsion efficiency, stability, and wheelchair manageability [
29], and estimation of biomechanical parameters during straight-line driving and evaluation of the operability of a competitive wheelchair are important issues for users with disabilities [
30]. An earlier study used findings from surface electromyography (sEMG) of users to characterize and elucidate wheelchair propulsion, because a correlation exists between sEMG data and muscle strength [
31]. The strength of the primary muscles in the user’s upper limb musculature strongly influence the propulsive force transmitted to the wheelchair [
32]. In the case of one-arm operation, there should be a difference in muscle activation between the left and right sides. In other words, this difference in muscle activation is related to changes in the motion of the upper limb. As described herein, we thought that by identifying the site of muscle activation by sEMG it would be possible to estimate approximate movement posture. This knowledge is important for the development of new competitive wheelchairs and their use in sports. Many methods have been proposed for detecting motion posture, including two-dimensional and three-dimensional video analyses based on computer vision and motion capture technology [
33,
34]. However, our methods do not require great resources of equipment, cost, or time, in addition to burdensome preparation for experiments.
As described herein, we present an estimate of movement posture during one-arm operation of a wheelchair based on changes in integrated electromyography (iEMG) data calculated from sEMG data. The first experiment is designed to elicit insights into differences in muscle activation of a user’s arm and shoulder joint muscles when using one arm and when using two arms with competitive wheelchair equipped with a dual hand-rim system. The experimentally obtained muscle activation results suggest that one arm use can produce equal propulsive force to that produced using two arms. The second experiment was conducted using iEMG data to estimate the movement posture during wheelchair propulsion with one arm. The external oblique abdominis play an important role in producing the movement posture for wheelchair propulsion force with one arm. Finally, using iEMG data, the posture estimation was verified by assessing the amount of change in the user’s body axis and seat pressure distribution. Results demonstrate that one-arm operation uses different muscle activation sites than the body posture used for propulsion by two-arm, indicating the body posture differences estimated from surface EMG.
2. Materials and Methods
This study was conducted to develop competitive wheelchairs that will allow participating in sports by facilitating straight-ahead movement with one arm. For example, our wheelchair is intended for use in situations where the athlete grips a racket in one hand and operates the hand-rim with the other hand, or when the athlete must propel the competitive wheelchair with only one arm. However, the differences in muscle activation and body posture between one-arm and two-arm operations have not been clarified. Once these issues are resolved, it will be possible to determine the muscles needed to strengthen one-arm operation and the approximate range of adaptability to the site and degree of disability. Preliminary test results confirmed great differences in body postures during straight-line motion with one-arm propulsion. In the case of one-arm operation, there should be a difference in muscle activation between the left and right sides. In addition, this difference in muscle activation is related to changes in the motion of the upper limb. We thought that by identifying the site of muscle activation by sEMG, it would be possible to estimate approximate movement posture. The first experiment was conducted to elicit insights into differences in muscle site activity from iEMG results obtained for one-arm and two-arm propulsion of a wheelchair equipped with a dual hand-rim system. Based on results of the first experiment, the second experiment tested whether body posture can be estimated from iEMG data during one-arm wheelchair propulsion based on the results of seat pressure distribution and changes in body axis.
2.1. Competitive Wheelchair with a Dual Hand-Rim System
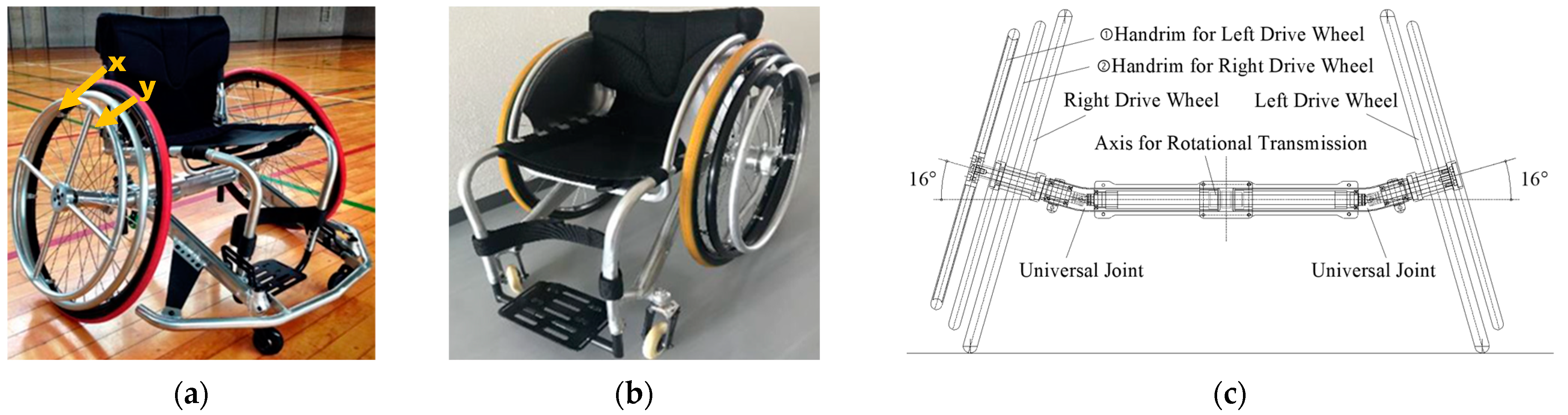
Figure 1 shows a competitive wheelchair with a dual hand-rim system designed for our study. Such wheelchairs are driven by a double-ring drive shaft structure [
27,
28]. Two wheelchairs are used for this research: (a) one with a right-hand drive with a camber angle and (b) one with a left-hand drive without a camber angle. These wheelchairs are de-signed to be interchangeable between the right and left sides by reassembly of parts.
Figure 1c shows a driving force transmission axle (DFTA) and universal joint that were developed to transmit the driving force from the operation of the outer hand-rims to the oppo-site drive wheel in a competitive wheelchair with a camber angle. The material used for the DFTA is standard internal iron with specific gravity of 7.87 g/cm
3 and Young’s modulus of 192.08 GP. A steel universal joint of the same standard is attached to the DFTA on each side. This universal joint has a structure in which the rotational transmission speed is not constant with the rotation angle, but which repeats the speed increase and decrease in a 180-degree rotation cycle. Therefore, by installing two universal joints with rotational phases that are 90 degrees apart, the rotational speed to the opposite drive wheel can be set to a constant speed. The one-arm drive wheelchair developed for bowling competition, as shown in
Figure 1b, has a structure incorporating no camber angle because it must specialize in straight-line driving based on the movement characteristics associated with competition. These two competitive wheelchairs, each of which can be driven with one arm, were manufactured by Ox Engineering Co., Ltd. (Funabashi, Japan).
Following is a description of straight-line operation of the wheelchair using one arm. The x and y shown as markers in
Figure 1a represent the two hand-rims. Regarding the two-handed rims attached to the right-hand drive side, the outer hand-rim shown in “x” operates the opposite left-hand drive wheel. The inner hand-rim shown in “y” operates the right-hand-drive wheel. When the dual hand-rims are operated simultaneously, the driving force is transmitted to both drive wheels. Thereby, the vehicle can move straight ahead. The manual propulsion action necessitates that one arm and hand exert repetitive force to the dual hand-rims accordingly.
2.2. Participants
The research participants in these experiments gave informed consent to serve as a study subject in the experiment. This study and use of the experimentally obtained data were approved by the Ethics Committee of the Nagaoka University of Technology (H30-1, H30-2). Research participants in the first experiment were two healthy men (173.5 ± 1.5 cm height; 70.5 ± 2.5 kg weight). Research participants in the second experiment were seven healthy men (173.1 ± 4.2 cm height; 65.4 ± 5.6 kg weight). All research participants, for whom the right hand was dominant had experienced adequate training in wheelchair manipulation. We want to explain changes and differences in muscle activity in one arm and two arms for a competitive wheelchair with a dual hand-rim system. Accordingly, we recruited healthy athletes as research participants. We understand that the inclusion of able-bodied athletes is a limitation affecting the generalizability of the study results. Research participants with a disability might show clear differences in muscle activity between one-arm and two-arm propulsion. The research participants adjusted the footrest and seat of the wheelchair before starting the experiments. The seating was secured by placing a towel between the gap on either side of the seat surface.
2.3. Experiment Protocol
2.3.1. First Experiment
The purpose of this experiment is to use iEMG results to gain insight into differences in arm and shoulder joint muscle activation of a user during one-arm and two-arm use of our competitive wheelchair equipped with a dual hand-rim system. The driving force provided with the push rims is defined as the delivery of propulsion to the wheelchair. The wheelchair speed is related directly to the magnitude and frequency of the propulsive action. In fact, competitive wheelchair propulsion techniques are divisible into two phases: drive and recovery [
35,
36]. The most important factor affecting this propulsive force is the drive phase. Five measurement points are presented in
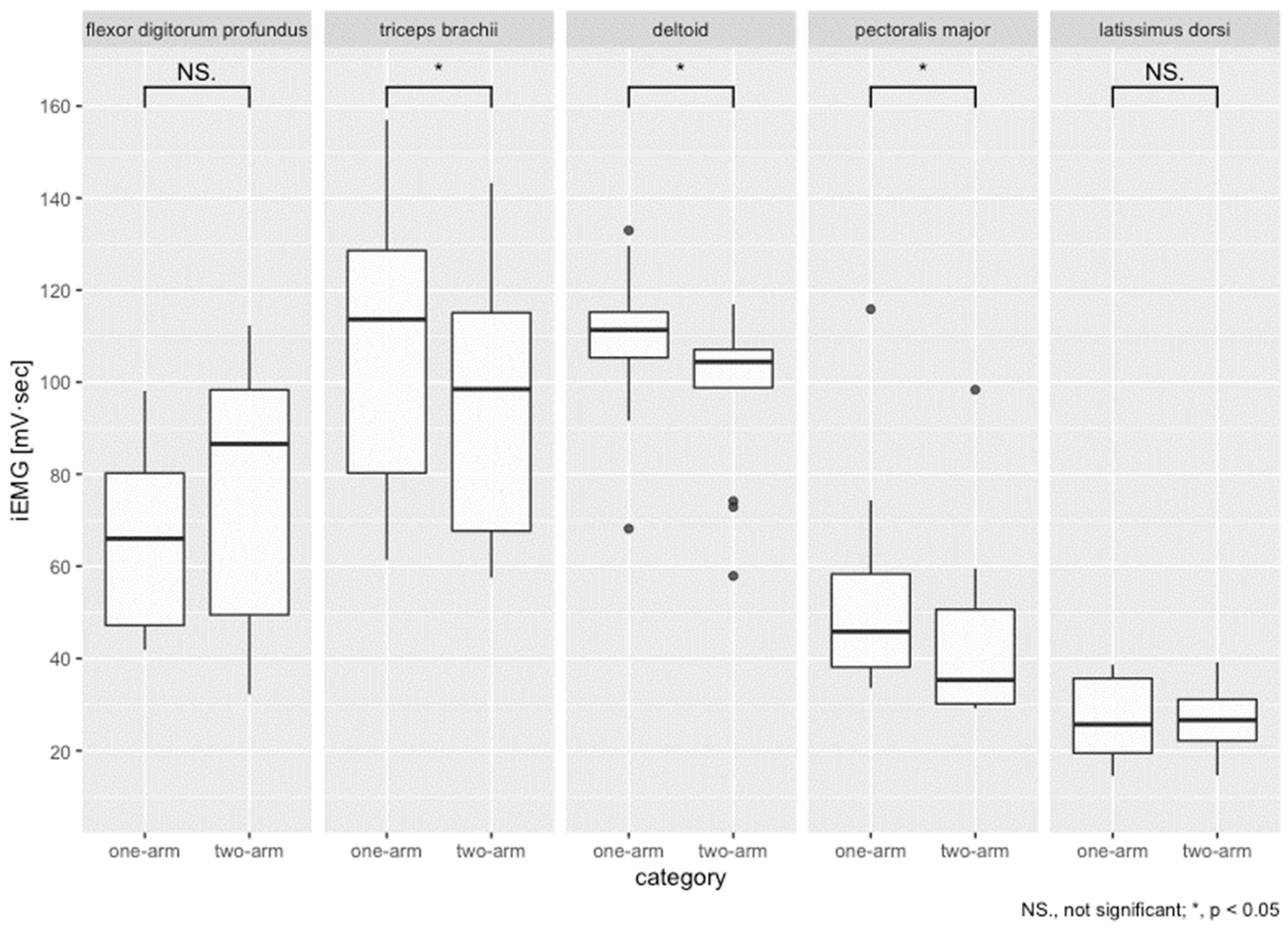
Figure 2a: (1) flexor digitorum profundus (pinky side), (2) triceps brachii, (3) deltoid, (4) pectoralis major, and (5) latissimus dorsi. These muscles were selected for their well-known contribution to the drive and recovery phases.
Figure 2b is a schematic diagram depicting the experiment. The procedure used for this experiment is the following.
As shown in
Figure 3a,b, research participants hold a dumbbell with a load of 5 kg for 30 s before running. All subjects are loaded to produce identical muscle fatigue because it inhibits the possibility of inducing muscle fatigue bias through individual differences.
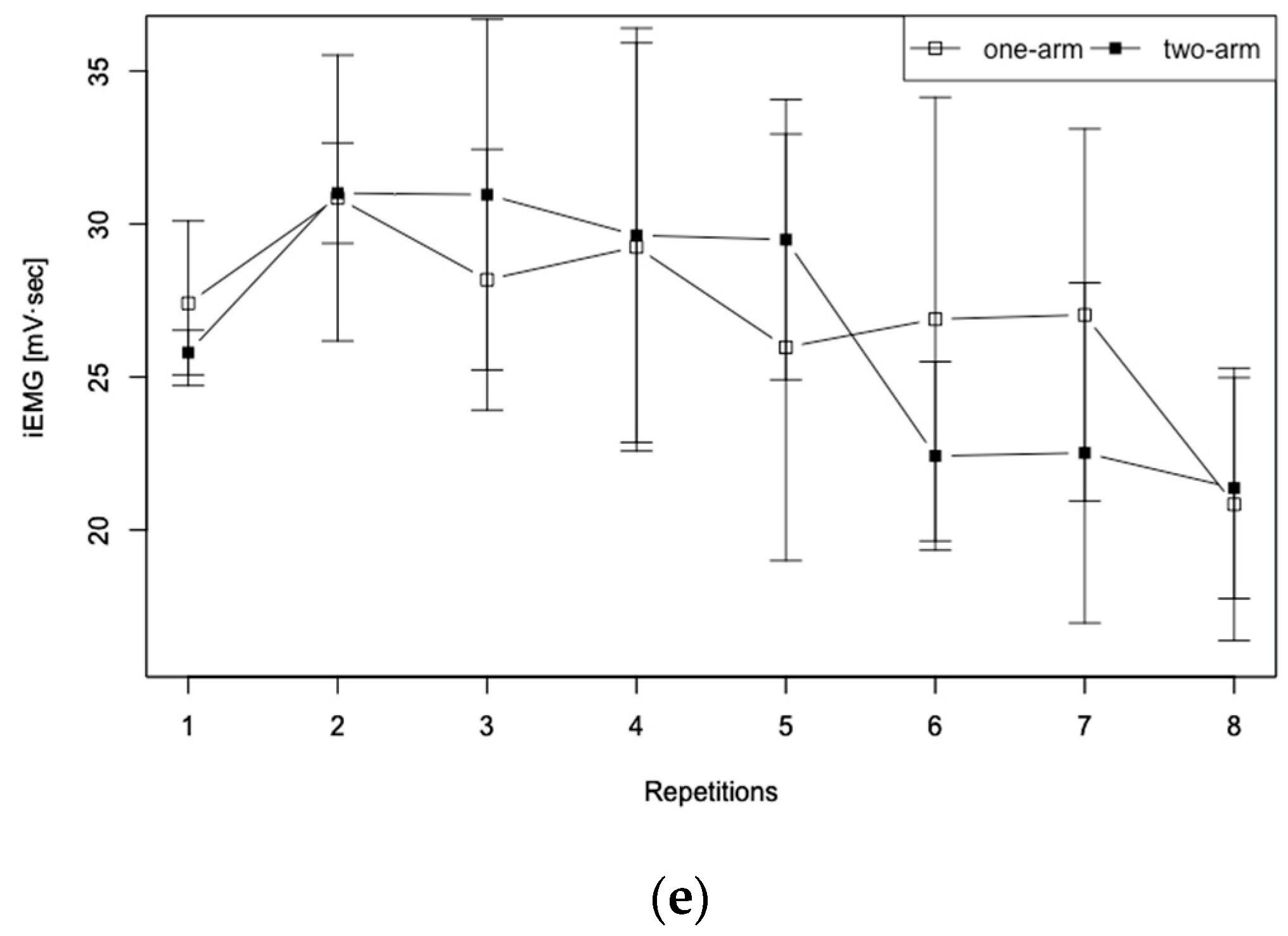
The start is made from a stationary position. During running, the hand-rim operation is performed once per second (for one rotation) for eight repetitions (for eight rotations) at full speed. The minimum number of cycles required for the wheelchair pro-pulsion to reach its maximum value from the stationary position is assumed because many competitions necessitate rapid acceleration in fewer cycles.
After completing running, the research participants take sufficient rest to recover from fatigue.
Steps 1–3 are performed alternately: three times in the case of one-handed running and three times in the case of two-handed running.
2.3.2. Second Experiment
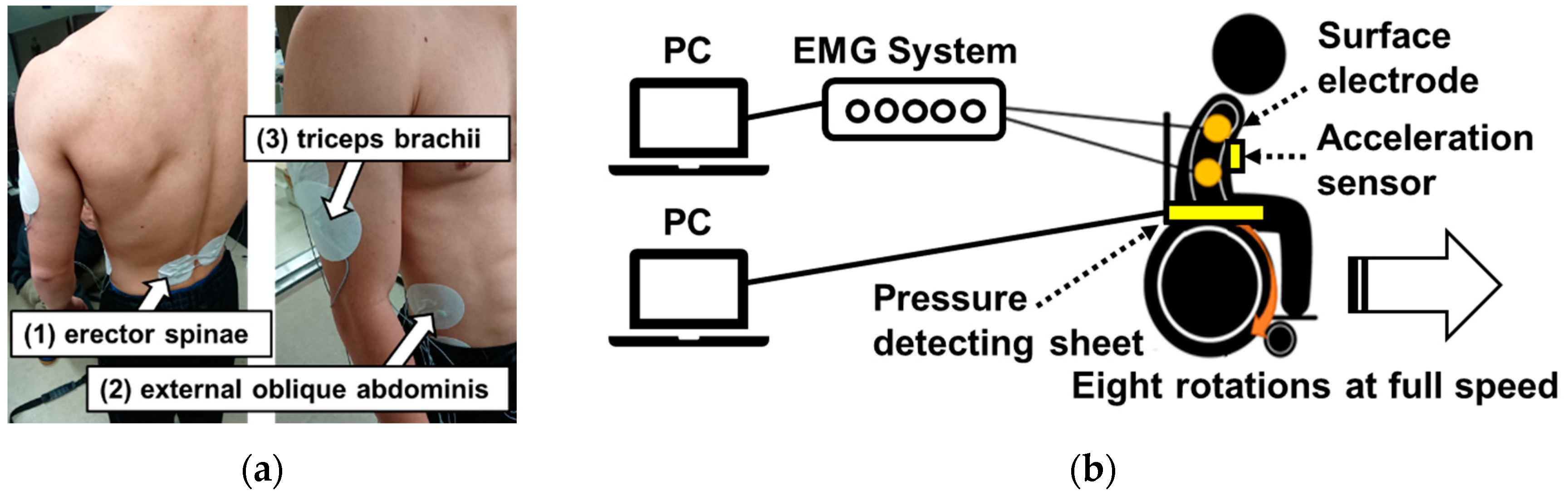
The purpose of this experiment was to use iEMG data to estimate the movement posture during wheelchair propulsion with one-arm operation. Based on the hypothesis produced in light of the first experiment results, this experiment also measured the seat pressure distribution and three-dimensional movement of the upper limb synchronized with the sEMG findings. These results corroborate evidence obtained for body posture effects during one-arm propulsion of the wheelchair. The wheelchair used for this experiment had no camber angle, as shown in
Figure 1b because the experiment specifically examines the operating posture during straight-line operation. Three measurement points are shown in
Figure 4a: (1) erector-spinae, (2) external oblique abdominis, and (3) triceps brachii. Not all measurement points are shown in
Figure 4a, but six measurement points were used for these surface EMGs because they were prepared for the left and right sides of the body. These muscles were selected for their well-known contributions to the drive phase [
37]. A schematic diagram of the experiment is presented in
Figure 4b. The procedures used for this experiment were the same as those described in 1–4 of
Section 2.4.1.
2.4. Data Recording and Analysis
2.4.1. Measuring Instruments
The following is a description of the measuring instruments used for data collection, which included a surface electromyogram (PolymatePro MP6000 biological signal system; Miyuki Giken Co., Ltd., Bunkyo, Japan), a pressure-detecting sheet (SR Soft Vision; Sumitomo Riko Co., Ltd., Nagoya, Japan), and a three-axis acceleration sensor (MyBeat; Union Tool Co., Tokyo, Japan). The sampling frequencies used for sEMG were 20–2000 Hz, with impedance of 250 GΩ and 24 input channels. For EMG data, surface electrodes were attached to the measurement position of the agonist muscle necessary for hand-rim operation. Details of its position are presented in the experiment protocol. The electrical signals obtained from the electrodes were recorded using a biological signal system (PolymatePro MP6000; Miyuki Giken Co., Ltd.) to a PC connected to the system at a sampling frequency of 1 kHz. The 450 × 450 mm pressure-detecting sheet included 256 pressure sensor elements. The sampling frequency was 5 Hz. The measurement range of pressure values was 0–200 mmHg. The right side of the lateral direction of the wheelchair was the X-axis positive direction. The front direction was the Y-axis positive direction. The three-axis acceleration sensor measured body axis movement. The right side of the lateral direction of the wheelchair was the X-axis positive direction. The vertically upward direction was the Y-axis positive direction. The front direction was the Z-axis positive direction. The sampling frequency was 128 Hz. The acceleration range was ±4 G.
2.4.2. Data Analysis
Muscle activation, which is described as the linear envelope of the EMG signal [
38], has been studied quantitatively using iEMG [
39]. In an earlier study, sEMG findings of wheelchair users were used as indicators of wheelchair propulsion because a correlation exists between sEMG data and muscle strength [
31]. For this study, sEMG measurements were taken at the arm, shoulder, and trunk muscles related to hand-rim operations. Re-search participants were prepared for placement of EMG electrodes at the measurement position by wiping the skin with alcohol and by lightly abrading it. Next, sufficient electrode paste (Ten20 Conductive; Weaver and Co., Aurora, CO, USA) was applied inside the surface Ag/AgCl EMG electrodes (MA-C001-15; Fukuda M-E Kogyo Co., Ltd., Nagareyama, Japan) to slightly overfit it. Then the electrode was placed onto the measurement position and pressed firmly. The electrodes were secured with surgical tape to minimize displacement during movement. A ground electrode was placed on a bony site over the iliac bone. For this study, sEMG data from each muscle were collected at a sampling frequency of 1 kHz during eight cycles for each research participant. One cycle defined here is one stroke of the hand-rim operation (to recovery phase from drive phase). The raw sEMG data were exported (BIMUTAS II; Kissei Comtec Co., Ltd., Matsumoto, Japan) for signal analysis and post-acquisition processing. A high-pass filter was used to remove noise. The integrated EMG (iEMG) was calculated using full-wave rectification smooth of sEMG data for each muscle for each research participant. In this study, the integrated value per second of iEMG measured at rest was normalized by the average value per stroke of iEMG measured during eight strokes of driving. These iEMG data quantitatively represent the total work-load of electrical activity of the muscles, meaning that the data quantify the amount of muscle activity for one drive during wheelchair operation.
The inclination of the body axis during wheelchair propulsion was measured using a three-axis acceleration sensor mounted in the center of the chest. The sampling frequency was 128 Hz. First, the sensor values in the three-axis (X-axis, Y-axis, Z-axis) were recorded when the research participants were held stationary in a competitive wheelchair for 10 s. We adopted the average of these values as our reference value at rest. Next, the difference between the results of all eight cycles and the reference value was then determined. Finally, we integrated the difference values for each cycle interval. The cycling interval is one second. However, individual differences occur. The samplings per cycle were adjusted by individually checking the peak values of the measured data. The result is presented as the inclination of the body axis during the wheelchair propulsion cycle. The reason for grouping them into eight cycles is to synchronize them with the iEMG results.
The seat pressure distribution during wheelchair propulsion was measured using a pressure-detecting sheet. The sampling frequency was 5 Hz. The sensor elements in a pressure-detecting sheet are arranged longitudinally and horizontally (16 × 16). The sheet was divided into nine grids because we wanted to classify the direction of the pressure distribution horizontally, vertically, and diagonally. The total sensor elements inherent in one grid were set to 32 (6 × 6). First, the sensor values in the seat pressure were recorded when the research participants were held stationary in a competitive wheelchair for 10 s. We adopted the average in the one grid as each reference value of static seat pressure. Next, the difference between the results of eight cycles in each grid and the reference values was then determined. Finally, we add the difference values for eight cycles. The result was recorded as the seat pressure distribution during the wheelchair propulsion cycle. These values are used as validation data for the body posture estimation.
2.4.3. Statistical Analysis
Data were analyzed using software (RStudio, ver. 1.4.1106: GNU Affero General Public License). For the first experiment, iEMG data from five muscles were analyzed: flex-or digitorum profundus (pinky side), triceps brachii, deltoid, pectoralis major, and latissimus dorsi. For the second experiment, iEMG data from six muscles were analyzed: erector spinae (right and left side), external oblique abdominis (right and left side), and triceps brachii (right and left side). Shapiro–Wilk’s test revealed normality of the iEMG data in each experiment [
40]. To assess significance of differences, a Wilcoxon signed-rank test by non-parametric data was selected for the corresponding two groups (one arm and two arms) [
41]. The Friedman test was selected for the four groups of the corresponding non-parametric data. Furthermore, differences in means between the two groups in the four groups of data were selected with the Tukey honestly significant difference test. All thresholds for significance were set at the
p < 0.05 level of confidence. The effect size was based on Cohen’s report [
42].
5. Conclusions
This study was conducted to develop competitive wheelchairs that will allow participating in sports by facilitating straight-ahead movement with one arm. This wheelchair has the potential to be a new assistive technology for people participating in sports. However, the differences in muscle activation and body posture between one-arm and two-arm operations have not been clarified. Once these issues are resolved, it will be possible to determine the muscles needed to strengthen one-arm operation and the approximate range of adaptability to the site and degree of disability.
The first experiment, using iEMG results, was conducted to elucidate differences in muscle activation of a user’s arm and shoulder joint muscles during propulsion using only one arm using two arms with a competitive wheelchair equipped with our dual hand-rim system. One-arm operation showed significant differences in activation of the triceps brachii and deltoid and pectoralis major, with a 10–20% increase in muscle activation compared to that when using two arms. Nevertheless, the amounts of muscle activation during one-handed driving were less than expected. The experimentally obtained results suggest that only one arm and other factors can provide the same propulsive force as that supplied by two-arm driving.
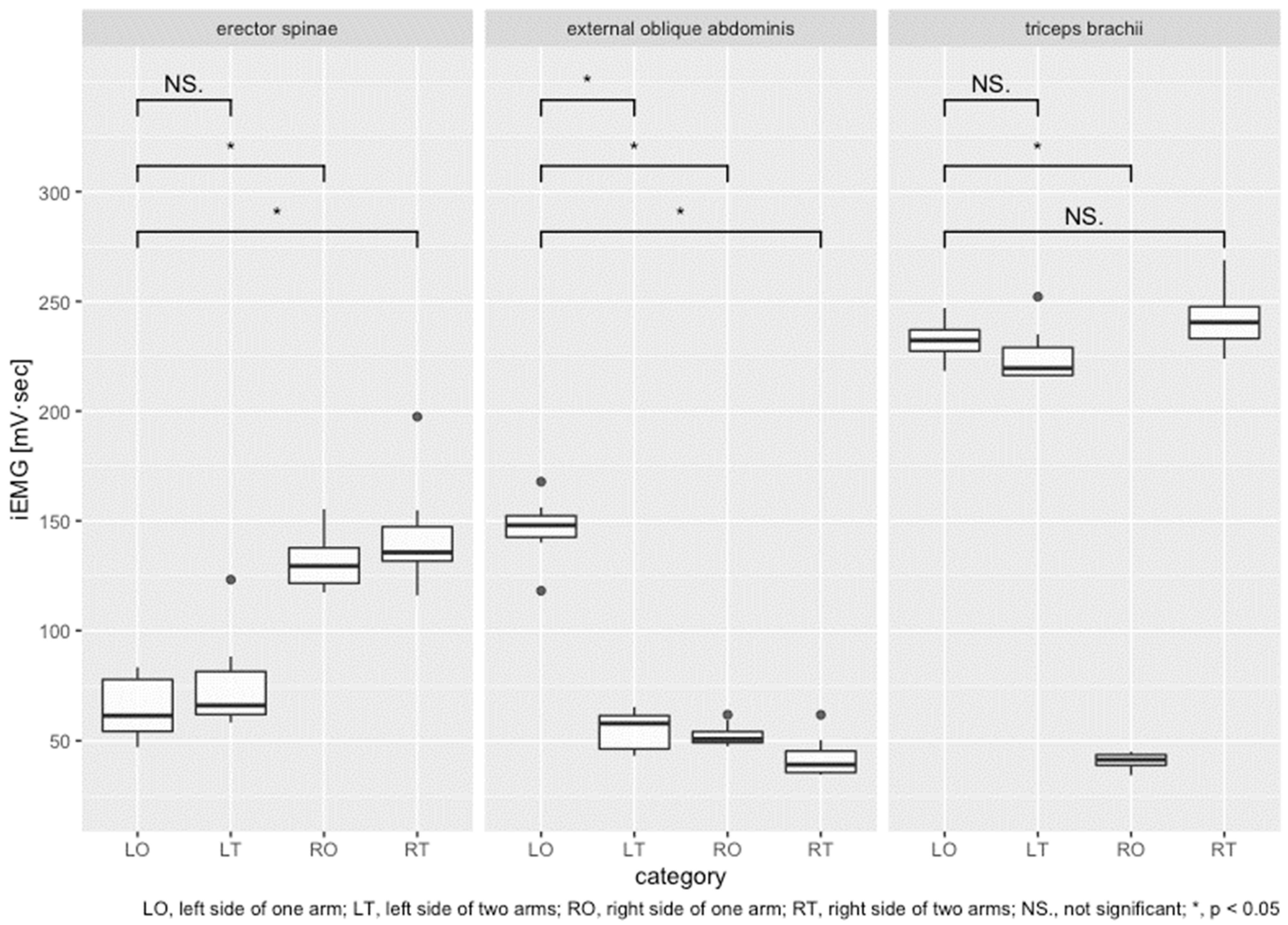
The second experiment was undertaken to use iEMG data to estimate the movement posture during wheelchair propulsion with one-arm operation. For the erector spinae, muscle activation was approximately half on the hand-rim manipulation side (left) com-pared to the right side. For the external oblique abdominis, the left-side muscle activation was about 2.7 times greater than at other times. For the triceps brachii, comparisons be-tween the left side of one arm and the left side of two arms during hand-rim manipulation revealed no significant difference in muscle activation. The external oblique abdominis muscles played an important role in producing wheelchair propulsion during one-arm operation. Finally, the validity of using iEMG for posture estimation was verified by the amount of change found in the user’s body axis and seat pressure distribution. In conclusion, results indicate that one-arm wheelchair operation activates different muscle sites and produces different body posture than wheelchair manipulation by two arms, thereby allowing movement and posture estimation using surface EMG.
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}