
Validity and Reliability of the Insole3 Instrumented Shoe Insole for Ground Reaction Force Measurement during Walking and Running


 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Motion Capture: Force Plates and Cameras
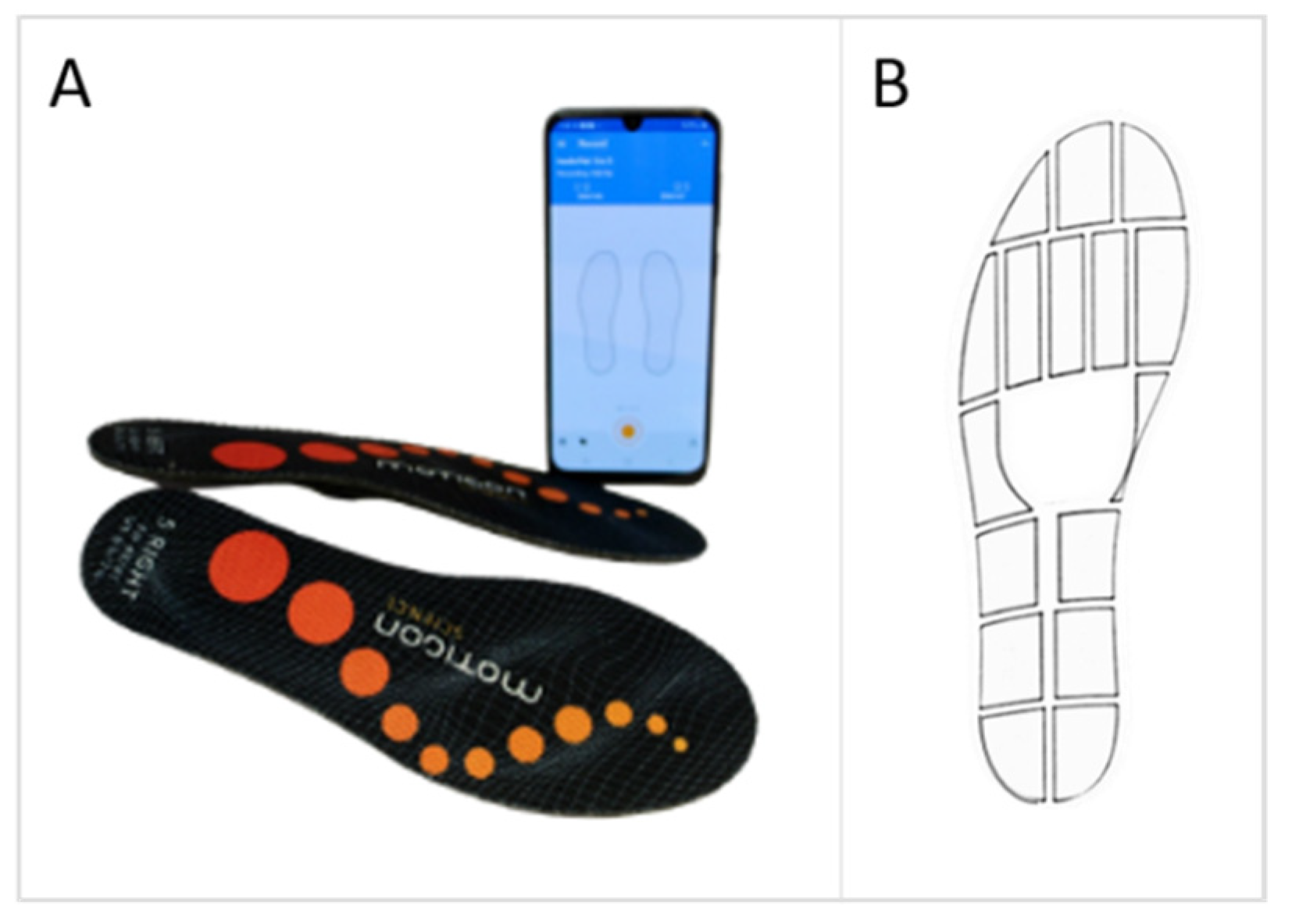
2.3. Insoles
2.4. Gait Conditions
2.5. Data Processing
2.6. Statistical Analyses
3. Results
3.1. Subjects
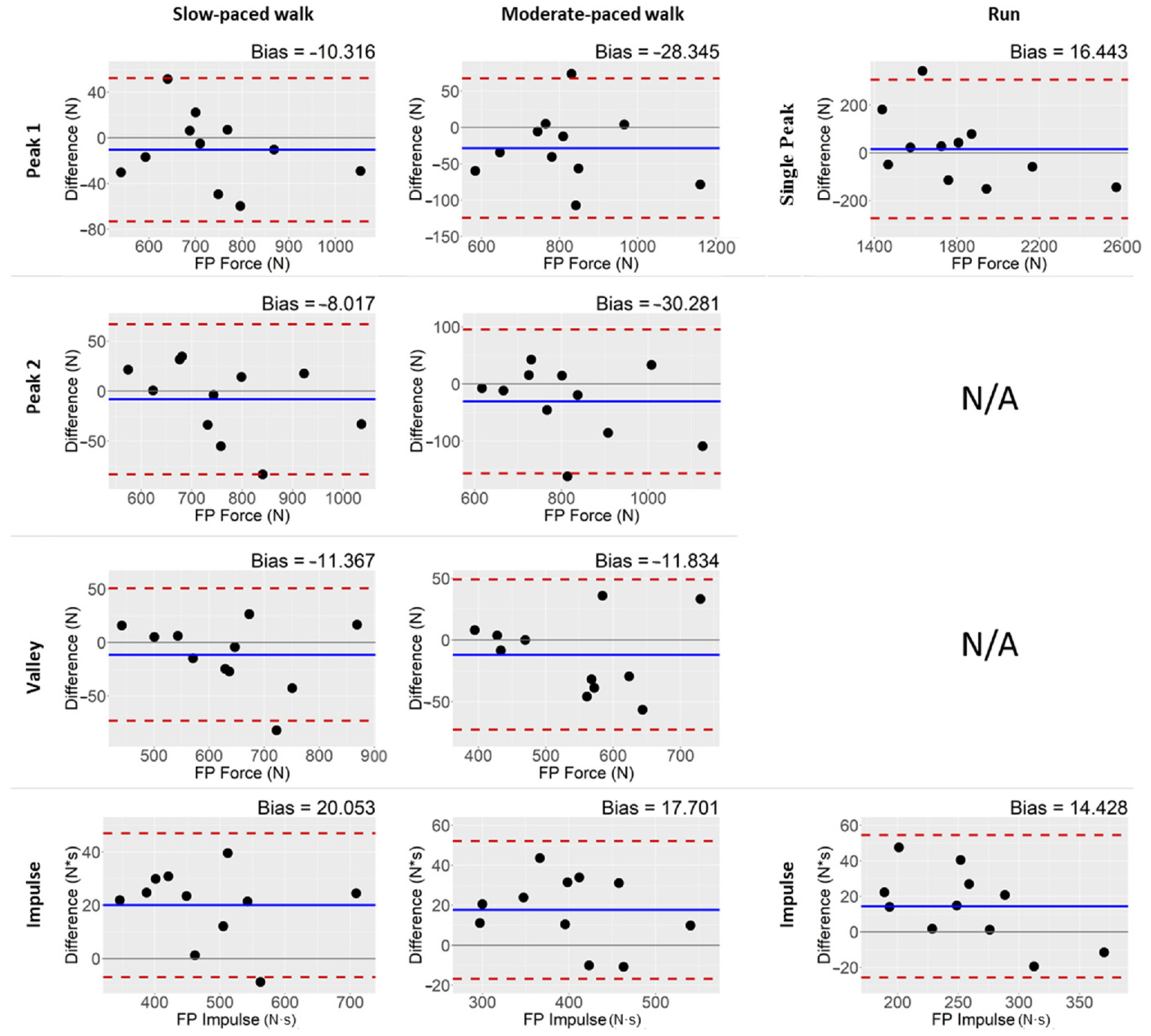
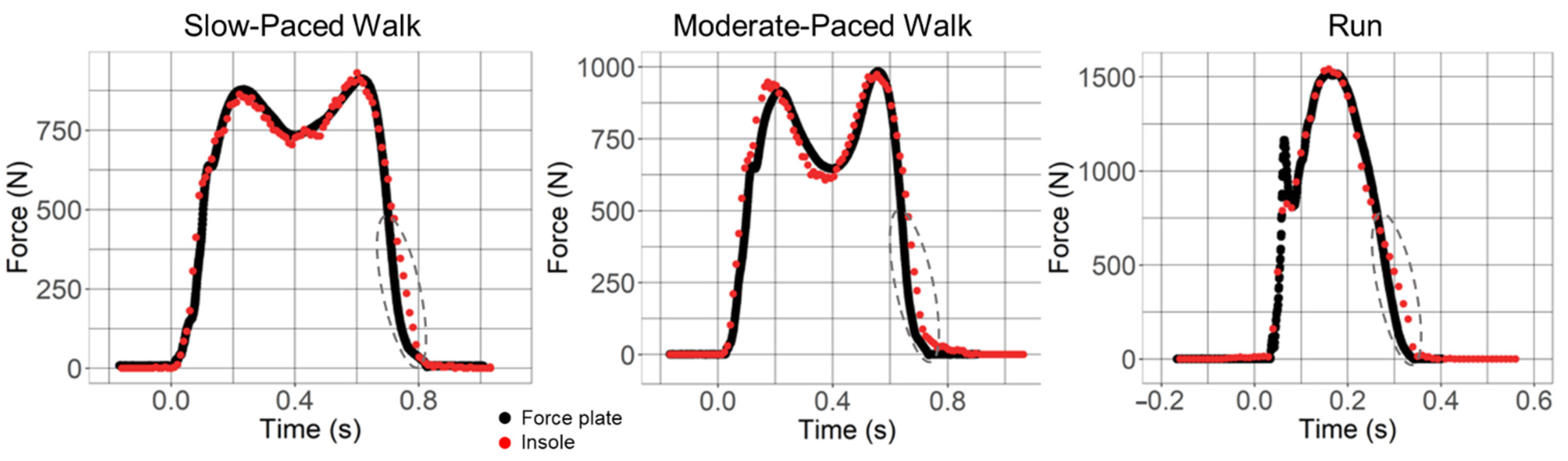
3.2. Absolute Agreement between Insole3 and Force Plate
3.3. Test–Retest Reliability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baker, R.; Esquenazi, A.; Benedetti, M.G.; Desloovere, K. Gait Analysis: Clinical Facts. Eur. J. Phys. Rehabil. Med. 2016, 52, 560–574. [Google Scholar] [PubMed]
- Lu, T.; Chang, C. Biomechanics of Human Movement and its Clinical Applications. Kaohsiung J. Med. Sci. 2012, 28, S13–S25. [Google Scholar] [CrossRef]
- Nagano, H.; Begg, R.K. Shoe-Insole Technology for Injury Prevention in Walking. Sensors 2018, 18, 1468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, S.R. Quantification of Human Motion: Gait Analysis—benefits and Limitations to its Application to Clinical Problems. J. Biomech. 2004, 37, 1869–1880. [Google Scholar] [CrossRef]
- Shahabpoor, E.; Pavic, A. Measurement of Walking Ground Reactions in Real-Life Environments: A Systematic Review of Techniques and Technologies. Sensors 2017, 17, 2085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, B.J.; Veith, N.T.; Hell, R.; Döbele, S.; Roland, M.; Rollmann, M.; Holstein, J.; Pohlemann, T. Validation and Reliability Testing of a New, Fully Integrated Gait Analysis Insole. J. Foot Ankle Res. 2015, 8, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kammerlander, C.; Pfeufer, D.; Lisitano, L.A.; Mehaffey, S.; Bocker, W.; Neuerburg, C. Inability of Older Adult Patients with Hip Fracture to Maintain Postoperative Weight-Bearing Restrictions. J. Bone Jt. Surg. Am. 2018, 100, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Drăgulinescu, A.; Drăgulinescu, A.; Zincă, G.; Bucur, D.; Feieș, V.; Neagu, D. Smart Socks and in-Shoe Systems: State-of-the-Art for Two Popular Technologies for Foot Motion Analysis, Sports, and Medical Applications. Sensors 2020, 20, 4316. [Google Scholar] [CrossRef]
- Renner, K.E.; Williams, D.; Queen, R.M. The Reliability and Validity of the Loadsol® Under various Walking and Running Conditions. Sensors 2019, 19, 265. [Google Scholar] [CrossRef] [Green Version]
- Leal-Junior, A.G.; Domingues, M.F.; Min, R.; Vilarinho, D.; Theodosiou, A.; Tavares, C.; Alberto, N.; Leitão, C.; Kalli, K.; Frizera-Neto, A. Fiber Bragg Based Sensors for Foot Plantar Pressure Analysis. In International Joint Conference on Biomedical Engineering Systems and Technologies; Springer: Cham, Switzerland, 2019; pp. 3–25. [Google Scholar]
- He, J.; Ferrigno, C.; Shakoor, N.; Wimmer, M. Responses to Gait Retraining using Pressure-Based Auditory Feedback for Medial Knee Osteoarthritis. Osteoarthr. Cartil. 2021, 29, S81–S82. [Google Scholar] [CrossRef]
- Ferrigno, C.; Stoller, I.S.; Shakoor, N.; Thorp, L.E.; Wimmer, M.A. The Feasibility of using Augmented Auditory Feedback from a Pressure Detecting Insole to Reduce the Knee Adduction Moment: A Proof of Concept Study. J. Biomech. Eng. 2016, 138, 021014. [Google Scholar] [CrossRef] [PubMed]
- Braun, B.J.; Veith, N.T.; Rollmann, M.; Orth, M.; Fritz, T.; Herath, S.C.; Holstein, J.H.; Pohlemann, T. Weight-Bearing Recommendations After Operative Fracture Treatment—fact Or Fiction? Gait Results with and Feasibility of a Dynamic, Continuous Pedobarography Insole. Int. Orthop. 2017, 41, 1507–1512. [Google Scholar] [CrossRef] [PubMed]
- Braun, B.J.; Bushuven, E.; Hell, R.; Veith, N.T.; Buschbaum, J.; Holstein, J.H.; Pohlemann, T. A Novel Tool for Continuous Fracture Aftercare–clinical Feasibility and First Results of a New Telemetric Gait Analysis Insole. Injury 2016, 47, 490–494. [Google Scholar] [CrossRef]
- Bujang, M.A.; Baharum, N. A Simplified Guide to Determination of Sample Size Requirements for Estimating the Value of Intraclass Correlation Coefficient: A Review. Arch. Orofac. Sci. 2017, 12, 1–11. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MoticonREGO AG. Sensor Insole Specification: Preliminary. 2021. Available online: https://moticon.com/wp-content/uploads/2021/09/OpenGo-Sensor-Insole-Specification-A4SQ-RGB-EN-03.02.pdf (accessed on 22 February 2022).
- Martini, E.; Fiumalbi, T.; Dell’Agnello, F.; Ivanić, Z.; Munih, M.; Vitiello, N.; Crea, S. Pressure-Sensitive Insoles for Real-Time Gait-Related Applications. Sensors 2020, 20, 1448. [Google Scholar] [CrossRef] [Green Version]
- Soangra, R.; Lockhart, T.E. Agreement in Gait Speed from Smartphone and Stopwatch for Five Meter Walk in Laboratory and Clinical Environments. Biomed. Sci. Instrum. 2014, 50, 254–264. [Google Scholar] [PubMed]
- Makowski, D.; Ben-Shachar, M.S.; Lüdecke, D. bayestestR: Describing Effects and their Uncertainty, Existence and Significance within the Bayesian Framework. J. Open Source Softw. 2019, 4, 1541. [Google Scholar] [CrossRef]
- Kottner, J.; Audigé, L.; Brorson, S.; Donner, A.; Gajewski, B.J.; Hróbjartsson, A.; Roberts, C.; Shoukri, M.; Streiner, D.L. Guidelines for Reporting Reliability and Agreement Studies (GRRAS) were Proposed. Int. J. Nurs. Stud. 2011, 48, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Zaki, R.; Bulgiba, A.; Ismail, R.; Ismail, N.A. Statistical Methods used to Test for Agreement of Medical Instruments Measuring Continuous Variables in Method Comparison Studies: A Systematic Review. PLoS ONE 2012, 7, e37908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasegawa, H.; Yamauchi, T.; Kraemer, W.J. Foot Strike Patterns of Runners at the 15-km Point during an Elite-Level Half Marathon. J. Strength Cond. Res. 2007, 21, 888. [Google Scholar]
- Gruber, A.H.; Edwards, W.B.; Hamill, J.; Derrick, T.R.; Boyer, K.A. A Comparison of the Ground Reaction Force Frequency Content during Rearfoot and Non-Rearfoot Running Patterns. Gait Posture 2017, 56, 54–59. [Google Scholar] [CrossRef]
- Stöggl, T.; Martiner, A. Validation of Moticon’s OpenGo Sensor Insoles during Gait, Jumps, Balance and Cross-Country Skiing Specific Imitation Movements. J. Sports Sci. 2017, 35, 196–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Low, D.; Dixon, S. Footscan Pressure Insoles: Accuracy and Reliability of Force and Pressure Measurements in Running. Gait Posture 2010, 32, 664–666. [Google Scholar] [CrossRef]
- Hori, N.; Newton, R.U.; Kawamori, N.; McGuigan, M.R.; Kraemer, W.J.; Nosaka, K. Reliability of Performance Measurements Derived from Ground Reaction Force Data during Countermovement Jump and the Influence of Sampling Frequency. J. Strength Cond. Res. 2009, 23, 874–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Queen, R.M.; Abbey, A.N.; Wiegerinck, J.I.; Yoder, J.C.; Nunley, J.A. Effect of Shoe Type on Plantar Pressure: A Gender Comparison. Gait Posture 2010, 31, 18–22. [Google Scholar] [CrossRef]
- Murphy, D.F.; Beynnon, B.D.; Michelson, J.D.; Vacek, P.M. Efficacy of Plantar Loading Parameters during Gait in Terms of Reliability, Variability, Effect of Gender and Relationship between Contact Area and Plantar Pressure. Foot Ankle Int. 2005, 26, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Salbach, N.M.; O’Brien, K.K.; Brooks, D.; Irvin, E.; Martino, R.; Takhar, P.; Chan, S.; Howe, J. Reference Values for Standardized Tests of Walking Speed and Distance: A Systematic Review. Gait Posture 2015, 41, 341–360. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Andrews, A.W. Normal Walking Speed: A Descriptive Meta-Analysis. Physiotherapy 2011, 97, 182–189. [Google Scholar] [CrossRef]
- Andriacchi, T.; Ogle, J.; Galante, J. Walking Speed as a Basis for Normal and Abnormal Gait Measurements. J. Biomech. 1977, 10, 261–268. [Google Scholar] [CrossRef]
- Jordan, K.; Challis, J.H.; Newell, K.M. Walking Speed Influences on Gait Cycle Variability. Gait Posture 2007, 26, 128–134. [Google Scholar] [CrossRef]
- Müßig, J.A.; Brand, A.; Kröger, I.; Klöpfer-Krämer, I.; Augat, P. Effects of Assistive Insole Feedback Training on Immediate and Multi-Day Partial Weight Bearing Retention during Walking: A Pilot Study. Gait Posture 2022, 93, 78–82. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic | Mean ± Standard Deviation |
| Number of Females (%) | 3/11 (27%) |
| Height (inches) | 68.5 ± 3.5 |
| Age (years) | 33.1 ± 16.7 |
| Weight (kilograms) | 74.2 ± 14.6 |
| BMI (kilograms/m2) | 24.6 ± 4.4 |
| Insoles | Median (range) |
| Insole Size (European size) | 42/43 (36/37–44/45) |
| Insole Size (Manufacturer Size) | Size 6 (3–7) |
| Gait Condition | vGRF Variable | Force Plate | Insole | Absolute Agreement | ||||
|---|---|---|---|---|---|---|---|---|
| Mean ± Standard Deviation | Mean ± Standard Deviation | ICC (3,k) | 95% CI | F(10,10) | p-Value | Mean Bias (%) | ||
| Slow Walk | Peak 1 (N) | 737.01 ± 139.91 | 726.69 ± 134.87 | 0.986 | (0.960, 0.995) | 72.766 | 0.0000 | −1.4 |
| Peak 2 (N) | 762.43 ± 133.45 | 754.42 ± 123.15 | 0.978 | (0.938, 0.993) | 46.067 | 0.0000 | −1.1 | |
| Valley (N) | 634.95 ± 120.53 | 623.58 ± 115.80 | 0.981 | (0.946, 0.994) | 54.837 | 0.0000 | −1.8 | |
| Impulse (N·s) | 481.71 ± 101.11 | 501.76 ± 99.36 | 0.986 | (0.771, 0.996) | 210.582 | 0.0000 | 4.2 | |
| Moderate-Paced Walk | Peak 1 (N) | 815.70 ± 153.14 | 787.35 ± 155.32 | 0.968 | (0.895, 0.990) | 38.63 | 0.0000 | −3.5 |
| Peak 2 (N) | 818.13 ± 148.97 | 787.85 ± 139.37 | 0.941 | (0.827, 0.980) | 19.166 | 0.0000 | −3.7 | |
| Valley (N) | 545.99 ± 103.76 | 534.16 ± 105.13 | 0.976 | (0.931, 0.992) | 44.094 | 0.0000 | −2.2 | |
| Impulse (N·s) | 400.15 ± 72.23 | 417.85 ± 69.66 | 0.970 | (0.803, 0.992) | 64.278 | 0.0000 | 4.4 | |
| Run | Peak Max (N) | 1814.98 ± 329.14 | 1831.42 ± 279.74 | 0.942 | (0.836, 0.980) | 17.383 | 0.0000 | 0.9 |
| Impulse (N·s) | 256.29 ± 54.75 | 270.71 ± 44.96 | 0.940 | (0.777, 0.981) | 23.001 | 0.0000 | 5.6 | |
| Insole3 | Test–Retest Consistency | |||||||
|---|---|---|---|---|---|---|---|---|
| Condition | vGRF Variable | Visit 1 Mean ± SD | Visit 2 Mean ± SD | ICC(3,k) | 95% CI | F(10,10) | p-Value | % Bias |
| Slow-paced walk | Peak 1 (N) | 726.69 ± 134.87 | 727.24 ± 140.06 | 0.996 | (0.987, 0.999) | 224.49 | 0 | 0.1 |
| Peak 2 (N) | 754.42 ± 123.15 | 745.05 ± 134.40 | 0.988 | (0.963, 0.996) | 81.05 | 0 | −1.2 | |
| Valley (N) | 623.58 ± 115.80 | 631.70 ± 119.66 | 0.995 | (0.985, 0.998) | 193.61 | 0 | 1.3 | |
| Impulse (N·s) | 501.76 ± 99.36 | 510.66 ± 103.87 | 0.995 | (0.984, 0.998) | 182.40 | 0 | 1.8 | |
| Moderate-paced walk | Peak 1 (N) | 787.35 ± 155.32 | 775.92 ± 161.95 | 0.983 | (0.951, 0.994) | 60.40 | 0 | −1.5 |
| Peak 2 (N) | 787.85 ± 139.37 | 779.08 ± 147.02 | 0.981 | (0.943, 0.994) | 52.55 | 0 | −1.1 | |
| Valley (N) | 534.16 ± 105.13 | 540.71 ± 102.65 | 0.986 | (0.959, 0.995) | 72.17 | 0 | 1.2 | |
| Impulse | 417.85 ± 69.66 | 420.33 ± 79.53 | 0.983 | (0.950, 0.994) | 59.83 | 0 | 0.6 | |
| Run | Max vGRF (N) | 1831.42 ± 279.74 | 1812.07 ± 282.82 | 0.970 | (0.912, 0.990) | 33.83 | 0 | −1.1 |
| Impulse (N·s) | 270.71 ± 44.96 | 266.02 ± 48.00 | 0.983 | (0.950, 0.994) | 59.39 | 0 | −1.7 | |
| Force Plate | ||||||||
| Slow-paced walk | Peak 1 (N) | 737.01 ± 139.91 | 735.55 ± 138.90 | 0.998 | (0.994, 0.999) | 491.40 | 0 | −0.2 |
| Peak 2 (N) | 762.43 ± 133.45 | 763.14 ± 135.32 | 0.999 | (0.996, 0.999) | 671.18 | 0 | 0.1 | |
| Valley (N) | 634.95 ± 120.53 | 642.20 ± 123.53 | 0.998 | (0.993, 0.999) | 403.99 | 0 | 1.1 | |
| Impulse (N·s) | 481.71 ± 101.11 | 492.60 ± 101.56 | 0.994 | (0.984, 0.998) | 180.85 | 0 | 2.2 | |
| Moderate-paced walk | Peak 1 (N) | 815.70 ± 153.14 | 813.80 ± 160.77 | 0.990 | (0.970, 0.997) | 99.85 | 0 | −0.2 |
| Peak 2 (N) | 818.13 ± 148.97 | 817.67 ± 146.97 | 0.999 | (0.996, 1.000) | 765.10 | 0 | −0.1 | |
| Valley (N) | 545.99 ± 103.76 | 550.67 ± 103.22 | 0.988 | (0.965, 0.996) | 84.69 | 0 | 0.9 | |
| Impulse (N·s) | 400.15 ± 72.23 | 405.25 ± 77.49 | 0.992 | (0.975, 0.997) | 119.70 | 0 | 1.3 | |
| Run | Peak vGRF (N) | 1814.98 ± 329.14 | 1832.57 ± 336.15 | 0.992 | (0.976, 0.997) | 123.65 | 0 | 1 |
| Impulse (N·s) | 256.29 ± 54.75 | 256.39 ± 52.55 | 0.991 | (0.975, 0.997) | 117.21 | 0 | 0.04 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cramer, L.A.; Wimmer, M.A.; Malloy, P.; O’Keefe, J.A.; Knowlton, C.B.; Ferrigno, C. Validity and Reliability of the Insole3 Instrumented Shoe Insole for Ground Reaction Force Measurement during Walking and Running. Sensors 2022, 22, 2203. https://doi.org/10.3390/s22062203
Cramer LA, Wimmer MA, Malloy P, O’Keefe JA, Knowlton CB, Ferrigno C. Validity and Reliability of the Insole3 Instrumented Shoe Insole for Ground Reaction Force Measurement during Walking and Running. Sensors. 2022; 22(6):2203. https://doi.org/10.3390/s22062203
Chicago/Turabian StyleCramer, Leora A., Markus A. Wimmer, Philip Malloy, Joan A. O’Keefe, Christopher B. Knowlton, and Christopher Ferrigno. 2022. "Validity and Reliability of the Insole3 Instrumented Shoe Insole for Ground Reaction Force Measurement during Walking and Running" Sensors 22, no. 6: 2203. https://doi.org/10.3390/s22062203
APA StyleCramer, L. A., Wimmer, M. A., Malloy, P., O’Keefe, J. A., Knowlton, C. B., & Ferrigno, C. (2022). Validity and Reliability of the Insole3 Instrumented Shoe Insole for Ground Reaction Force Measurement during Walking and Running. Sensors, 22(6), 2203. https://doi.org/10.3390/s22062203