
Secure Telemedicine System Design for COVID-19 Patients Treatment Using Service Oriented Architecture



Abstract
1. Introduction
2. Related Work
2.1. SOA in Telemedicine
2.2. SOA Security
3. Security Requirements in Tele-COVID
- Transmission of secure messages and establishment of secure communication between Patient and Physician.
- Transmission of secure messages and establishment of secure communication between Physician and Pharmacy.
- Transmission of secure messages and establishment of secure communication between Physician and Hospital.
- Transmission of secure messages and establishment of secure communication between Pharmacy and Patient.
Security Implementation at Physician and Patient End
4. Research Method
- Identifies the related security aspect of telemedicine systems.
- Examines specific security methods for Tele-COVID applications for all four ends.
- Proposes a security architecture for Tele-COVID that will address the issues of data integration, interoperability and vendor locking.
- Transmits secure encrypted messages from patient to physician and from physician to the hospital.
- a
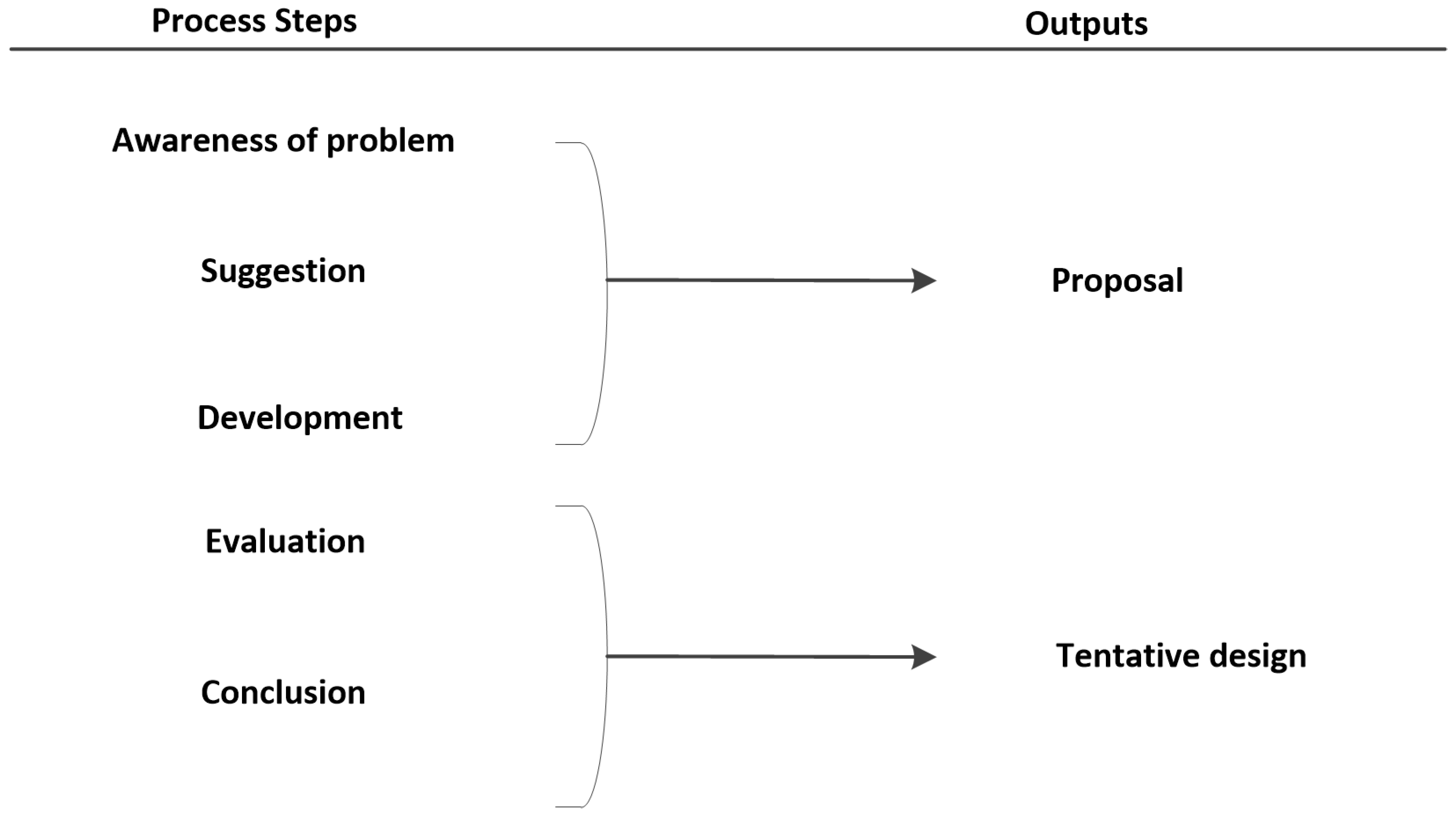
- Process Steps: Techniques that contribute to creating innovation through design research are:
- Awareness of Problems: Security in web-based and mobile applications is currently discussed everywhere, and several methods are being applied for the security methods. However, SOA security is one of the major important elements is being implemented in several telemedicine applications. Thus, we need to make sure that our mobile application and web-based application meet the minimum-security requirements as the awareness step.
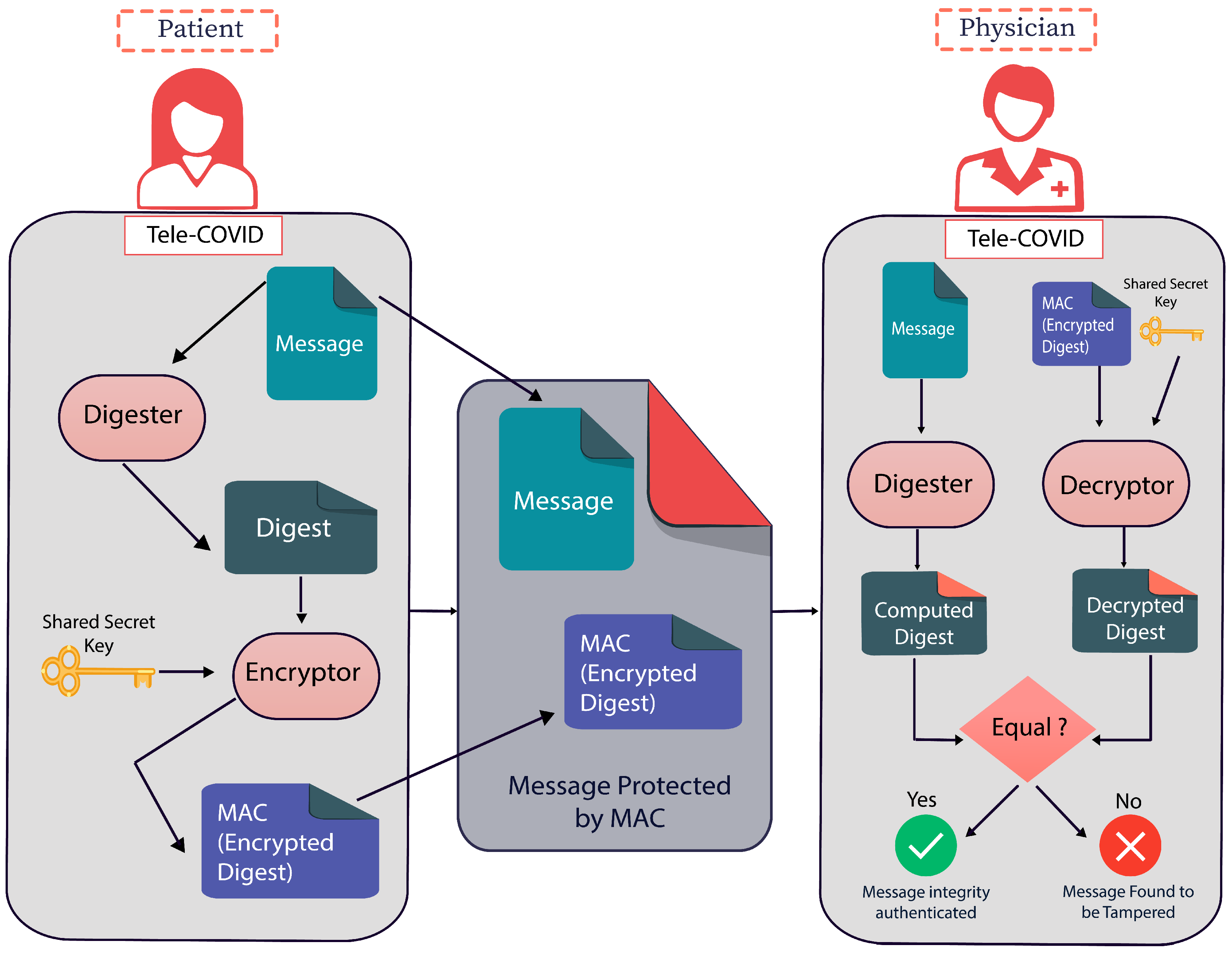
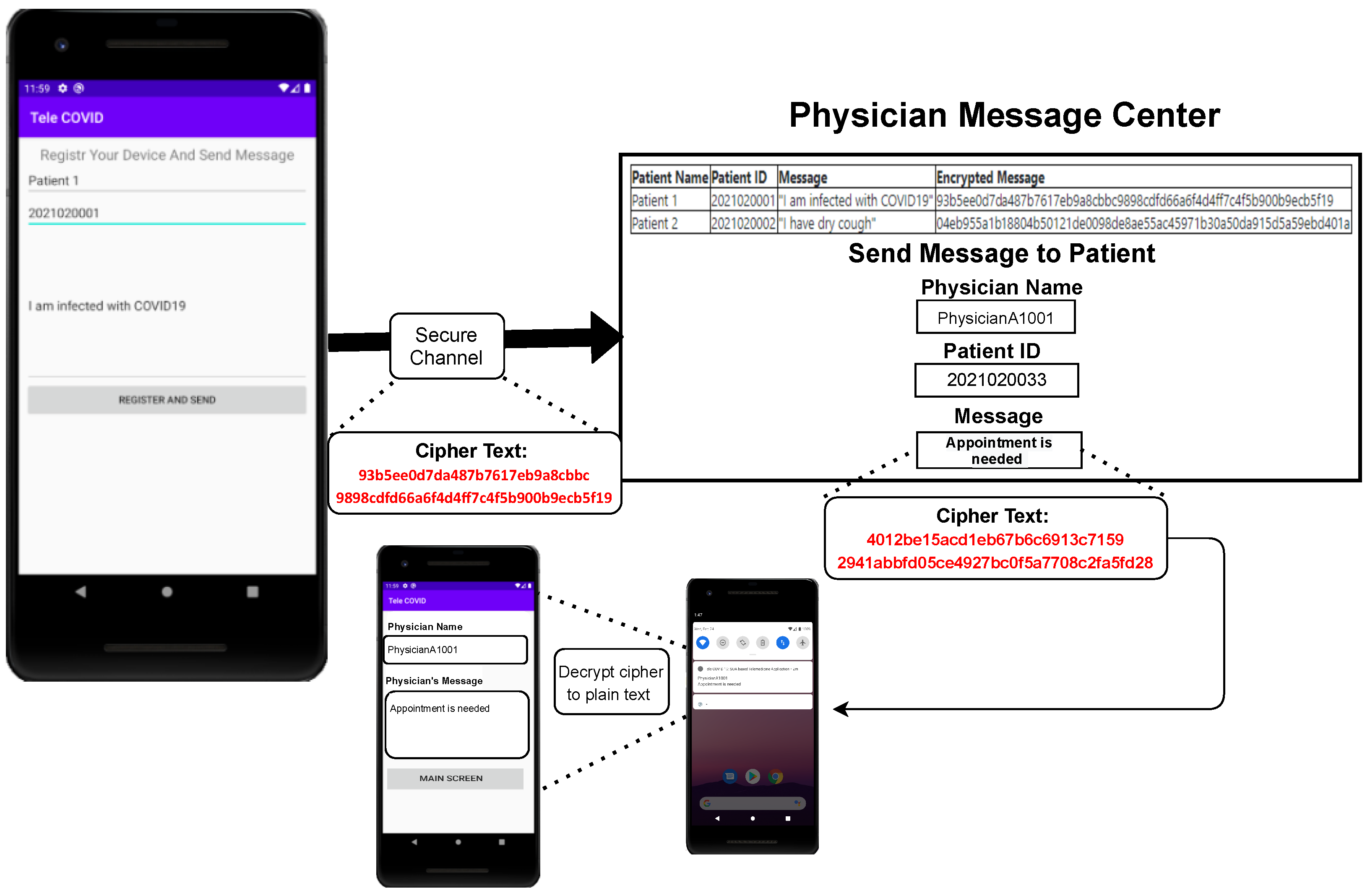
- Suggestion: We provide the solution based on SOA security that is represented in Figure 2, where the patient will send the message that will be digested. After the digestion, the message will be encrypted, and through Tele-COVID, the message will be deployed to the physician end. Consequently, the physician can decrypt the message using the shared secret key.
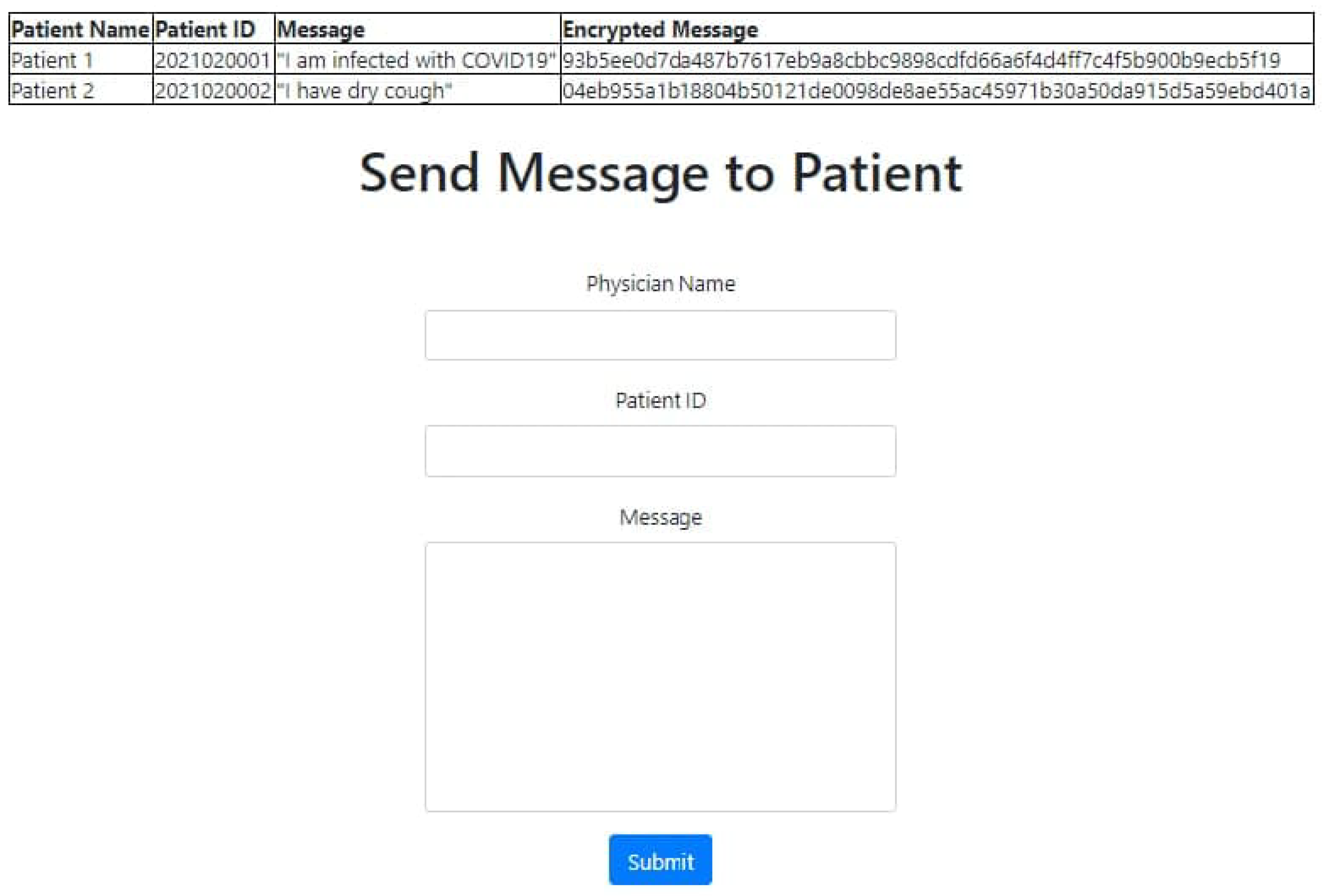
- Development: In this part of the process, we applied the SOA security in our web-based application, the Tele-COVID application which stores the encrypted messages into databases.
- Evaluation: The secure Tele-COVID is currently functional in four ends that are hospital, patient, physician, and pharmacy.
- Conclusion: To check the security whether it is implemented in all four ends.
- b
- Outputs: There will be a unique output in each of the steps. The awareness of the problem and suggestion belongs to the proposal. In case, a researcher finds any errors in the development stage, it can go back to the second step or the third step of the methodology, otherwise in this methodology, we do not have a return mechanism. The targeted output is obtaining a secure Tele-COVID application or system.
Flow Chart of the Proposed Method
- i
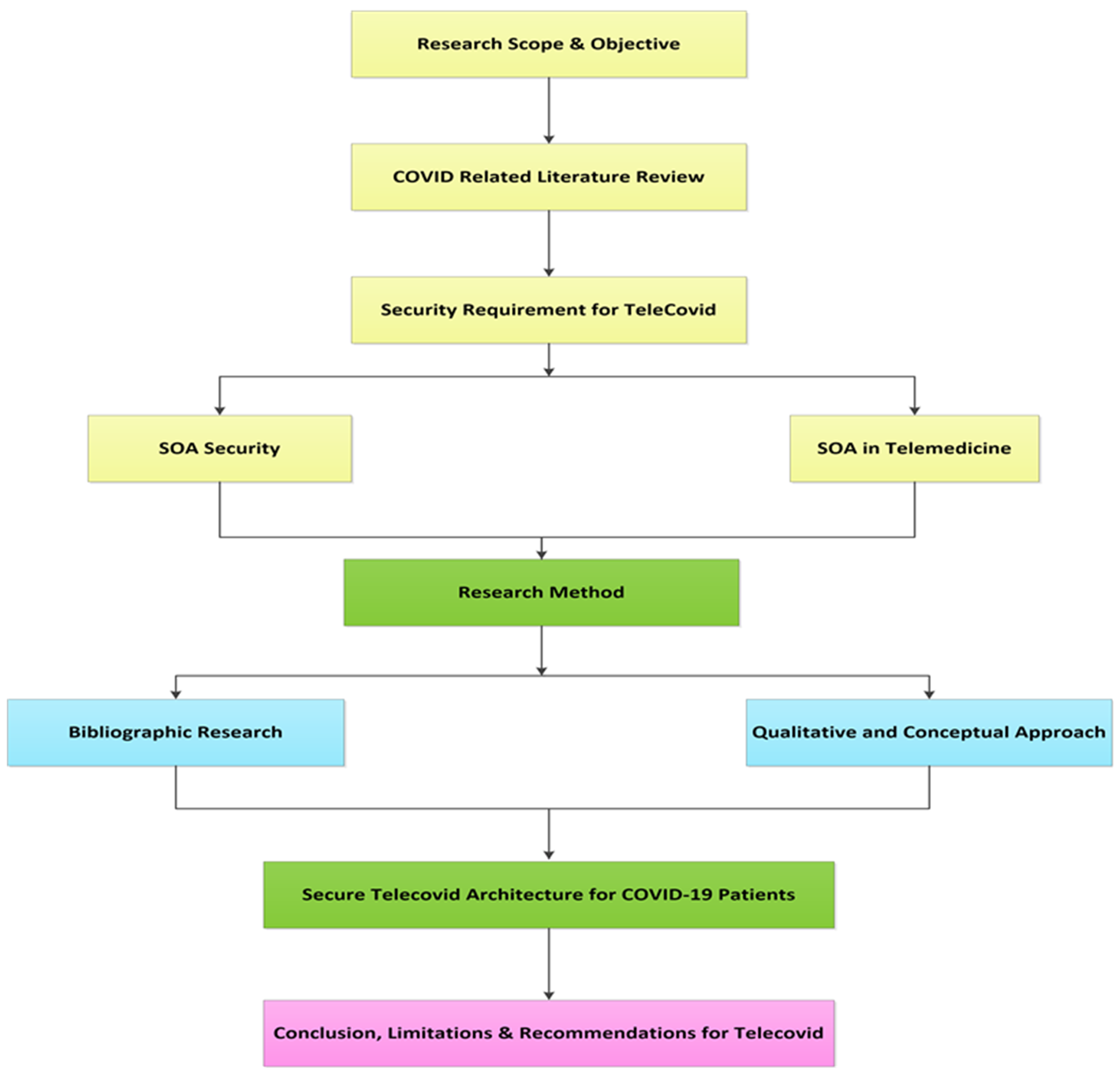
- Research Scope and Objectives: A Tele-COVID secure system architecture that provides treatment for COVID-19 patients remotely while overcoming problems of data interchange problem that occurs when different telemedicine applications are presented.
- ii
- COVID-related Literature Review: An extensive review has been conducted where it is identified that there are a number of SOA security architectures but those are not used in telemedicine. Based on the literature, it is discovered that there a very few architectures in the field of telemedicine with SOA.
- iii
- Security Requirement for Tele-COVID: A broad investigation to discuss major secure compunction requirements while facing COVID-19 pandemic has been discussed that is further divided into two sections: (1) SOA Security, and (2) SOA telemedicine.
- iv
- Research Method: A broad research method has been conducted to investigate existing architecture with comparison to proposed secure architecture which is further divided into two sections: (1) Bibliographic research, and (2) Qualitative and Conceptual research.
- v
- Secure Tele-COVID Architecture for COVID-19 Patients: The presented architecture is designed to integrate service-oriented architecture while utilizing secure communication mode that prevents violation of patient privacy as well as ensuring secure, robust, and flexible characteristics is presented in this design.
- vi
- Conclusion, Limitations, and Recommendations for Tele-COVID: SOA-based architecture has been proposed to provide several web services as assistants for CIOVID-19 patients, on the other hand; limitations and recommendations are presented to be addressed in future work. Figure 4 shows the flow chart of the proposed Tele-COVID Architecture.
5. Proposed Security Architecture
| Algorithm 1 Initiate the token and encrypt the message |
Input Values of the Patient ID, Patient Name, Message Output Device token and encrypt message
|
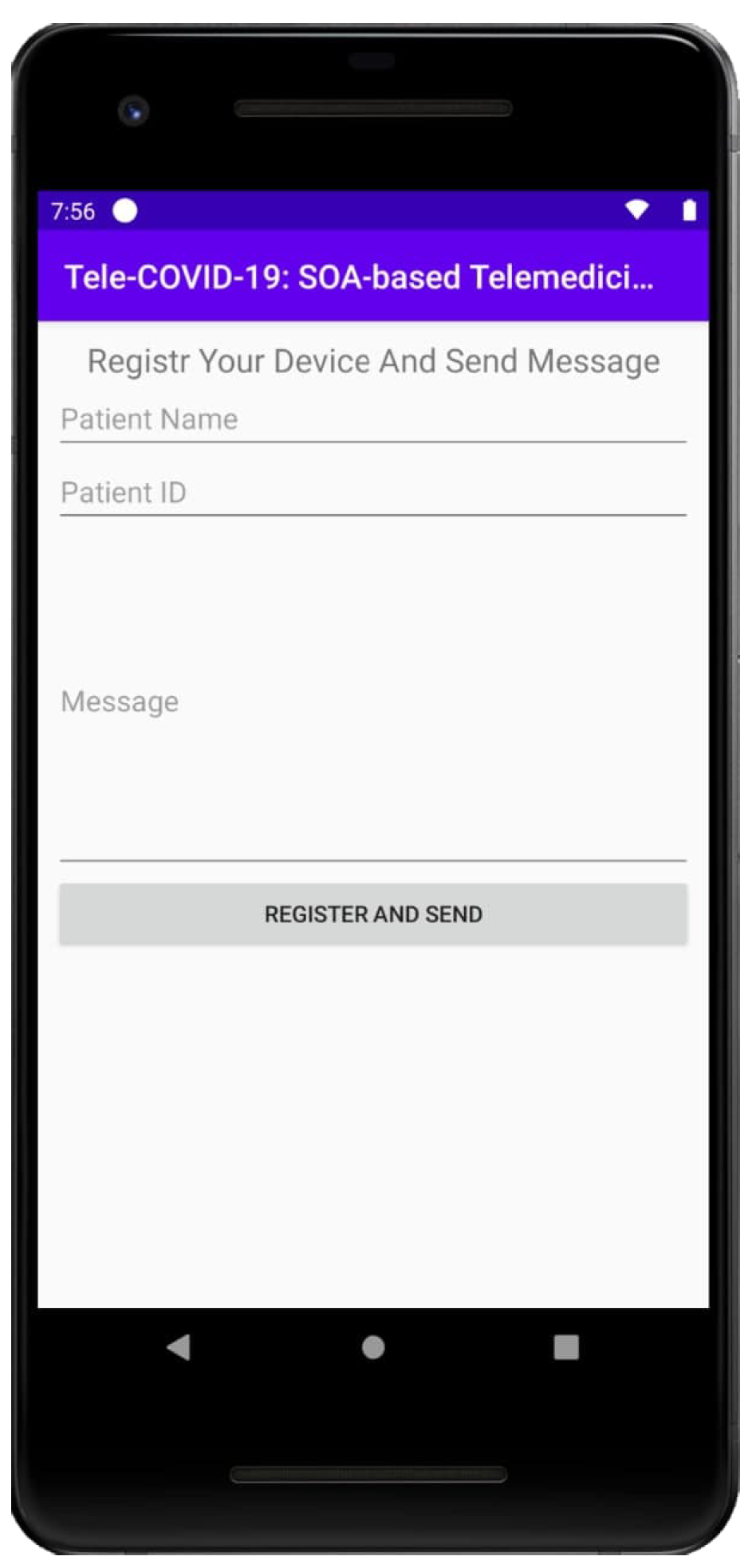
- Patient or care provider download Tele-COVID app.
- If the device has not been registered before a token will be initiated for the device and registration will be completed in the app’s server.
- If the device has initiated a token previously, then the initiated token will be retrieved from the server to establish secure communication.
- The message will be encrypted and sent to the intended receiver.
6. SOA Security Implementation in Tele-COVID
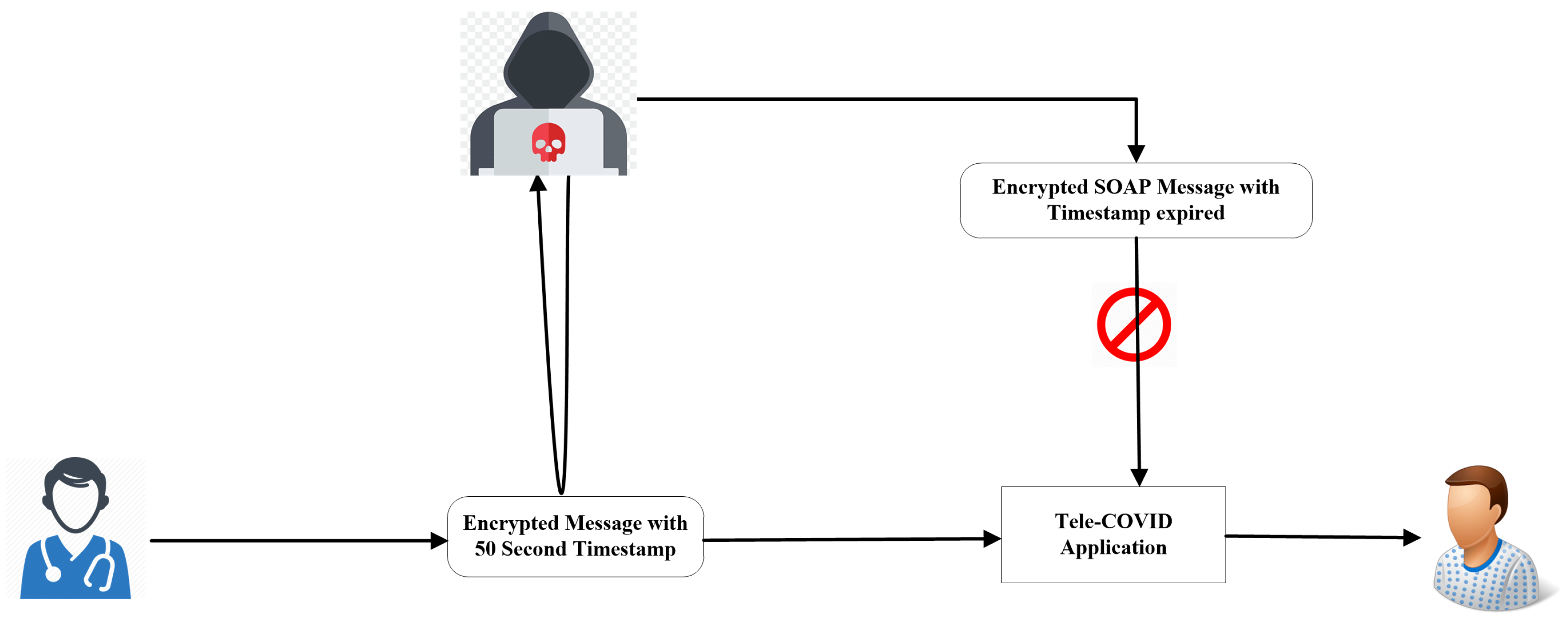
Prevention from Reply Attacks
7. Discussions and Evaluation of Tele-COVID SOA Security Architecture
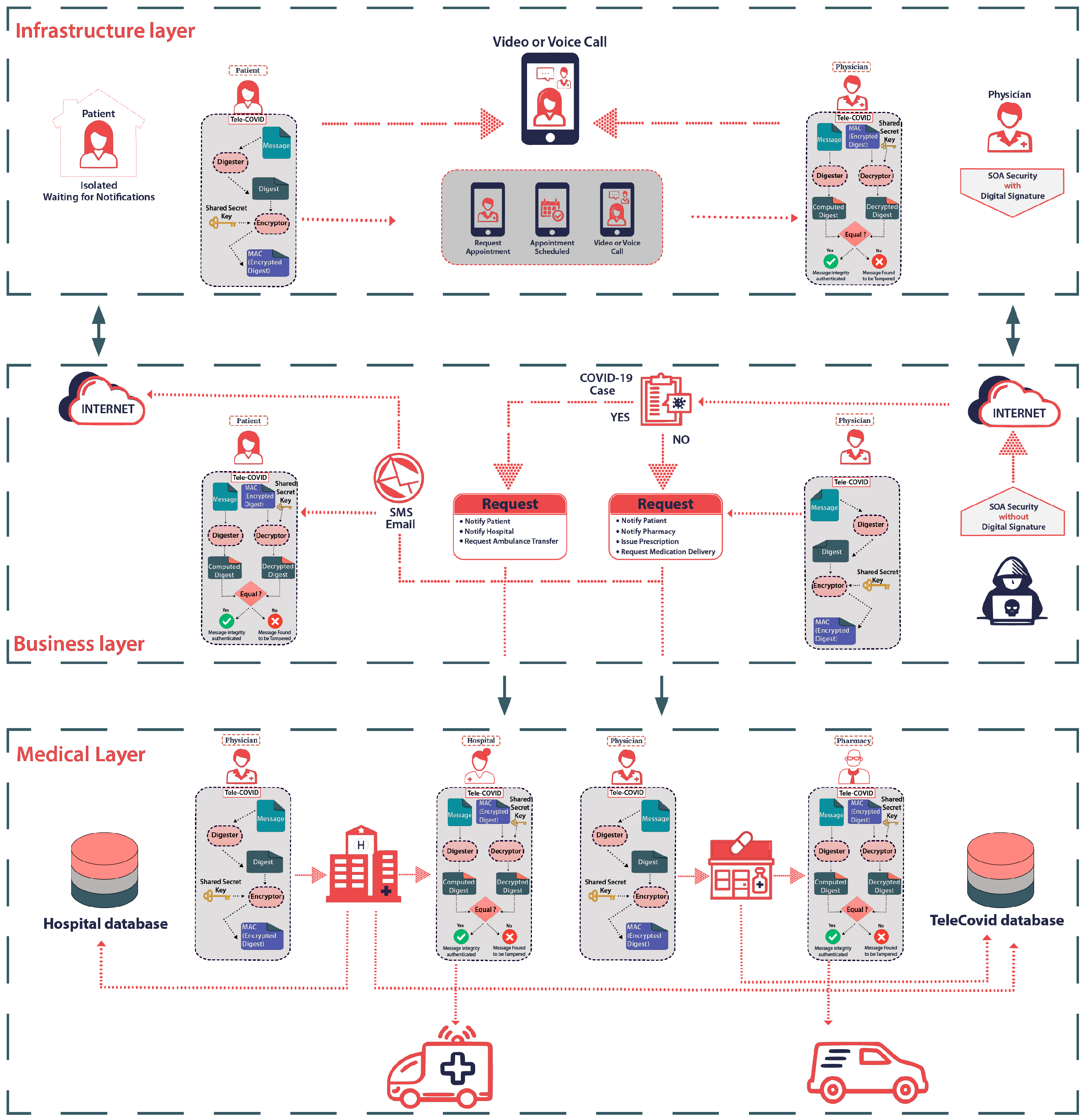
- The first option is a home test which is based on certain questionnaires. Once these questionnaires are filled by the suspected COVID-19 patients, the Tele-COVID telemedicine application will advise the patient to seek immediate medical assistance if required. Alternatively, home quarantine is advised. The home test feature is very useful for those patients who are sensitive and afraid to seek an appointment with a doctor.
- The second option is to reserve an appointment in case Tele-COVID recommends taking the advice of the physician. The second option automatically will be enabled after the questionnaires are filled and the patient requires an appointment. The list of physicians becomes available as per the location of the patient. There is a possibility that the physician can be overbooked in a particular area. In that case, the nearest available physician will be assigned for medical advice. Each physician is capable and obliged of handling a certain number of patients per day.
- The third option is to track medicine; this option is accessible to the patient if the physician has prescribed medication. The physician enters the medical prescription through Tele-COVID and the pharmacy is informed.
- The final option is to order an ambulance in case the patient is serious and has a breathing problem. Ambulance service can also be tracked by the patient through Tele-COVID. This option can only be enabled by the physician and the ambulance will move the patient from home to the COVID-19 special treatment ward.
8. Conclusions and Future Work
Author Contributions
Funding
Conflicts of Interest
References
- Elias, B.; Bar-Yam, Y. Could Air Filtration Reduce COVID-19 Severity and Spread; New England Complex Systems Institute: Cambridge, MA, USA, 2020. [Google Scholar]
- Byambasuren, O.; Cardona, M.; Bell, K.; Clark, J.; McLaws, M.L.; Glasziou, P. Estimating the extent of asymptomatic COVID-19 and its potential for community transmission: Systematic review and meta-analysis. Off. J. Assoc. Med Microbiol. Infect. Dis. Can. 2020, 5, 223–234. [Google Scholar]
- Chinese Center for Disease Control and Prevention Epidemiology Working Group for NCIP Epidemic Response. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 41, 145. [Google Scholar]
- Leung, K.; Wu, J.T.; Liu, D.; Leung, G.M. First-wave COVID-19 transmissibility and severity in China outside Hubei after control measures, and second-wave scenario planning: A modelling impact assessment. Lancet 2020, 395, 1382–1393. [Google Scholar] [CrossRef]
- Xu, S.; Li, Y. Beware of the second wave of COVID-19. Lancet 2020, 395, 1321–1322. [Google Scholar] [CrossRef]
- Reznik, A.; Gritsenko, V.; Konstantinov, V.; Yehudai, M.; Bender, S.; Shilina, I.; Isralowitz, R. First and Second Wave COVID-19 Fear Impact: Israeli and Russian Social Work Student Fear, Mental Health and Substance Use. Int. J. Ment. Health Addict. 2021, 1–8. [Google Scholar] [CrossRef]
- Iadecola, C.; Anrather, J.; Kamel, H. Effects of COVID-19 on the nervous system. Cell 2020, 183, 16–27.e1. [Google Scholar] [CrossRef]
- Shaikh, A. The impact of SOA on a system design for a telemedicine healthcare system. Netw. Model. Anal. Health Inform. Bioinform. 2015, 4, 1–16. [Google Scholar] [CrossRef]
- Anton, D.; Kurillo, G.; Yang, A.Y.; Bajcsy, R. Augmented telemedicine platform for real-time remote medical consultation. In Proceedings of the International Conference on Multimedia Modeling, Reykjavik, Iceland, 4–6 January 2017; Springer: Berlin/Heidelberg, Germany, 2017; pp. 77–89. [Google Scholar]
- Smith, W.R.; Atala, A.J.; Terlecki, R.P.; Kelly, E.E.; Matthews, C.A. Implementation guide for rapid integration of an outpatient telemedicine program during the COVID-19 pandemic. J. Am. Coll. Surg. 2020, 231, 216–222. [Google Scholar] [CrossRef]
- Avila, K.; Sanmartin, P.; Jabba, D.; Jimeno, M. Applications based on service-oriented architecture (SOA) in the field of home healthcare. Sensors 2017, 17, 1703. [Google Scholar] [CrossRef]
- Lopes, D.; Abreu, B.; Batista, W. Innovation in telemedicine: An expert medical information system based on SOA, expert systems and mobile computing. In Advances in Computer and Information Sciences and Engineering; Springer: Berlin/Heidelberg, Germany, 2008; pp. 119–124. [Google Scholar]
- Ng, W.S.; Teo, J.C.M.; Ang, W.T.; Viswanathan, S.; Tham, C.K. Experiences on developing SOA based mobile healthcare services. In Proceedings of the 2009 IEEE Asia-Pacific Services Computing Conference (APSCC), Singapore, 7–11 December 2009; pp. 498–501. [Google Scholar]
- Shaikh, A.; AlReshan, M.S.; Asiri, Y.; Sulaiman, A.; Alshahrani, H. Tele-COVID: A Telemedicine SOA-Based Architectural Design for COVID-19 Patients. CMC-Comput. Mater. Contin. 2021, 67, 549–576. [Google Scholar] [CrossRef]
- Shaikh, A.; Memon, M.; Memon, N.; Misbahuddin, M. The role of service oriented architecture in telemedicine healthcare system. In Proceedings of the 2009 International Conference on Complex, Intelligent and Software Intensive Systems, Fukuoka, Japan, 16–19 March 2009; pp. 208–214. [Google Scholar]
- Traore, B.B.; Kamsu-Foguem, B.; Tangara, F. Integrating MDA and SOA for improving telemedicine services. Telemat. Inform. 2016, 33, 733–741. [Google Scholar] [CrossRef][Green Version]
- Satoh, F.; Nakamura, Y.; Mukhi, N.K.; Tatsubori, M.; Ono, K. Methodology and tools for end-to-end soa security configurations. In Proceedings of the 2008 IEEE Congress on Services—Part I, Honolulu, HI, USA, 6–11 July 2008; pp. 307–314. [Google Scholar]
- Yamany, H.F.E.; Capretz, M.A.; Allison, D.S. Quality of security service for web services within SOA. In Proceedings of the 2009 Congress on Services—I, Los Angeles, CA, USA, 6–10 July 2009; pp. 653–660. [Google Scholar]
- Larrucea, X.; Alonso, R. ISOAS: Through an independent SOA Security specification. In Proceedings of the Seventh International Conference on Composition-Based Software Systems (ICCBSS 2008), Madrid, Spain, 25–29 February 2008; pp. 92–100. [Google Scholar]
- Epstein, J.; Matsumoto, S.; McGraw, G. Software security and SOA: Danger, Will Robinson! IEEE Secur. Priv. 2006, 4, 80–83. [Google Scholar] [CrossRef]
- Saleem, M.; Jaafar, J.; Hassan, M. A domain-specific language for modelling security objectives in a business process models of soa applications. AISS 2012, 4, 353–362. [Google Scholar]
- Huang, Z.; Lai, J.; Chen, W.; Li, T.; Xiang, Y. Data security against receiver corruptions: SOA security for receivers from simulatable DEMs. Inf. Sci. 2019, 471, 201–215. [Google Scholar] [CrossRef]
- Tsai, W.T.; Wei, X.; Chen, Y.; Paul, R.; Chung, J.Y.; Zhang, D. Data provenance in SOA: Security, reliability, and integrity. Serv. Oriented Comput. Appl. 2007, 1, 223–247. [Google Scholar] [CrossRef]
- Bustos, N.; Tello, M.; Droppelmann, G.; García, N.; Feijoo, F.; Leiva, V. Machine learning techniques as an efficient alternative diagnostic tool for COVID-19 cases. Signa Vitae 2022, 18, 23–33. [Google Scholar]
- Dash, S.; Aarthy, R.; Mohan, V. Telemedicine during COVID-19 in India—A new policy and its challenges. J. Public Health Policy 2021, 42, 501–509. [Google Scholar] [CrossRef]
- Yamany, H.F.E.; Capretz, M.A. Use of data mining to enhance security for SOA. In Proceedings of the 2008 Third International Conference on Convergence and Hybrid Information Technology, Busan, Korea, 11–13 November 2008; Volume 1, pp. 551–558. [Google Scholar]
- Baker, H.A.; Safavynia, S.A.; Evered, L.A. The ‘third wave’: Impending cognitive and functional decline in COVID-19 survivors. Br. J. Anaesth. 2021, 126, 44–47. [Google Scholar] [CrossRef]
- Graichen, H. What is the difference between the first and the second/third wave of Covid-19?—German perspective. J. Orthop. 2021, 24, A1–A3. [Google Scholar] [CrossRef]
- Nguyen, T.T.; Pathirana, P.N.; Nguyen, T.; Nguyen, Q.V.H.; Bhatti, A.; Nguyen, D.C.; Nguyen, D.T.; Nguyen, N.D.; Creighton, D.; Abdelrazek, M. Genomic mutations and changes in protein secondary structure and solvent accessibility of SARS-CoV-2 (COVID-19 virus). Sci. Rep. 2021, 11, 3487. [Google Scholar] [CrossRef]
- Peral, J.; Ferrandez, A.; Gil, D.; Munoz-Terol, R.; Mora, H. An ontology-oriented architecture for dealing with heterogeneous data applied to telemedicine systems. IEEE Access 2018, 6, 41118–41138. [Google Scholar] [CrossRef]
- Weider, D.Y.; Bhagwat, R. Modeling emergency and telemedicine heath support system: A service oriented architecture approach using cloud computing. Int. J. E-Health Med. Commun. (IJEHMC) 2011, 2, 63–88. [Google Scholar]
- Guillén, E.; Ubaque, J.; Ramirez, L.; Cardenas, Y. Telemedicine network implementation with SOA architecture: A case study. In Proceedings of the World Congress on Engineering and Computer Science, San Francisco, CA, USA, 24–26 October 2012; Volume 2012, pp. 24–27. [Google Scholar]
- Tai, Y.; Gao, B.; Li, Q.; Yu, Z.; Zhu, C.; Chang, V. Trustworthy and intelligent COVID-19 diagnostic iomt through xr and deep learning-based clinic data access. IEEE Internet Things J. 2021, 8, 15965–15976. [Google Scholar] [CrossRef]
- Habib, M.; Faris, M.; Qaddoura, R.; Alomari, A.; Faris, H. A Predictive Text System for Medical Recommendations in Telemedicine: A Deep Learning Approach in the Arabic Context. IEEE Access 2021, 9, 85690–85708. [Google Scholar] [CrossRef]
- Ahmed, S.T.; Sankar, S.; Sandhya, M. Multi-objective optimal medical data informatics standardization and processing technique for telemedicine via machine learning approach. J. Ambient Intell. Humaniz. Comput. 2021, 12, 5349–5358. [Google Scholar] [CrossRef]
- Apache Axis, Web Service Security. Available online: http://axis.apache.org/axis/java/security.html (accessed on 5 May 2021).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | Patient ID | Patient Name | Physician ID | Physician Name | Patient Request Date, Time and Symptoms | Connection Established Time | Patient’s Encrypted Message |
|---|---|---|---|---|---|---|---|
| 1 | Patient0101 | Patient 1 | PhysicianA1001 | Physician A | Mon 4 Jan. 2021 7:24 a.m. I am infected with COVID-19 | Mon 4 Jan. 2021 11:51 a.m. | Encrypted Message Here |
| 2 | Patient0102 | Patient 2 | PhysicianA1001 | Physician A | Mon 4 Jan. 2021 9:06 a.m. I have notice that my cough is too dry | Mon 4 Jan. 2021 13:33 p.m. | Encrypted Message Here |
| 3 | Patient0103 | Patient 3 | PhysicianA1001 | Physician A | Mon 4 Jan. 2021 10:17 a.m. Recently, I just loss of taste and barely smell | Mon 4 Jan. 2021 13:51 p.m. | Encrypted Message Here |
| 4 | Patient0104 | Patient 4 | PhysicianA1001 | Physician A | Mon 4 Jan. 2021 11:35 a.m. My symptoms for COVID are that difficulty breathing and shortness of breath | Mon 4 Jan. 2021 14:08 p.m. | Encrypted Message Here |
| 5 | Patient0105 | Patient 5 | PhysicianA1001 | Physician A | Mon 4 Jan. 2021 14:45 a.m. I have a loss of speech and movement | Mon 4 Jan. 2021 15:12 p.m. | Encrypted Message Here |
| 6 | Patient0106 | Patient 6 | PhysicianB1002 | Physician B | Tues 5 Jan. 2021 8:16 a.m. I have a chest pain and pressure | Tues 5 Jan. 2021 09:17 a.m. | Encrypted Message Here |
| 7 | Patient0107 | Patient 7 | PhysicianB1002 | Physician B | Tues 5 Jan. 2021 9:04 a.m. I have a strange headache | Tues 5 Jan. 2021 09:21 a.m. | Encrypted Message Here |
| 8 | Patient0108 | Patient 8 | PhysicianB1002 | Physician B | Tues 5 Jan. 2021 9:16 a.m. I have a conjunctivitis | Tues 5 Jan. 2021 10:26 a.m. | Encrypted Message Here |
| 9 | Patient0109 | Patient 9 | PhysicianB1002 | Physician B | Tues 5 Jan. 2021 11:36 a.m. I have a saver corona Symptoms | Tues 5 Jan. 2021 11:53 a.m. | Encrypted Message Here |
| 10 | Patient0110 | Patient 10 | PhysicianB1002 | Physician B | Tues 5 Jan. 2021 11:52 a.m. I have a fever, chest pain and loss of taste | Tues 5 Jan. 2021 14:16 p.m. | Encrypted Message Here |
| 11 | Patient0111 | Patient 11 | PhysicianC1003 | Physician C | Wend 6 Jan. 2021 11:24 a.m. I feel aches and pains this morning | Wend 6 Jan. 2021 15:05 p.m. | Encrypted Message Here |
| 12 | Patient0112 | Patient 12 | PhysicianC1003 | Physician C | Wend 6 Jan. 2021 11:32 a.m. Nasal congestion and runny nose. I need to see a doctor | Wend 6 Jan. 2021 15:25 p.m. | Encrypted Message Here |
| 13 | Patient0113 | Patient 13 | PhysicianC1003 | Physician C | Wend 6 Jan. 2021 12:13 p.m. I am not sure if I am infected with COVID. Any consultation appointment? | Wend 6 Jan. 2021 15:45 p.m. | Encrypted Message Here |
| 14 | Patient0114 | Patient 14 | PhysicianC1003 | Physician C | Wend 6 Jan. 2021 13:41 p.m. I am unable to speech and move | Wend 6 Jan. 2021 16:07 p.m. | Encrypted Message Here |
| 15 | Patient0115 | Patient 15 | PhysicianC1003 | Physician C | Wend 6 Jan. 2021 14:14 p.m. I am experiencing lately some tiredness and fatigueness | Wend 6 Jan. 2021 16:19 p.m. | Encrypted Message Here |
| 16 | Patient0116 | Patient 16 | PhysicianD1004 | Physician D | Thurs 7 Jan. 2021 10:05 a.m. Serious signs of covid19 which affect my living during the day | Thurs 7 Jan. 2021 11:03 a.m. | Encrypted Message Here |
| 17 | Patient0117 | Patient 17 | PhysicianD1004 | Physician D | Thurs 7 Jan. 2021 10:43 a.m. I was in a room with coronavirus infected person | Thurs 7 Jan. 2021 11:17 a.m. | Encrypted Message Here |
| 18 | Patient0118 | Patient 18 | PhysicianD1004 | Physician D | Thurs 7 Jan. 2021 10:54 a.m. I started to feel some fever | Thurs 7 Jan. 2021 11:33 a.m. | Encrypted Message Here |
| 19 | Patient0119 | Patient 19 | PhysicianD1004 | Physician D | Thurs 7 Jan. 2021 11:36 a.m. My partner has body pains for a week | Thurs 7 Jan. 2021 11:59 a.m. | Encrypted Message Here |
| 20 | Patient0120 | Patient 20 | PhysicianD1004 | Physician D | Thurs 7 Jan. 2021 15:58 a.m. I am a 73-year person, and I was diagnosed with COVID 2 month ago | Thurs 7 Jan. 2021 16:14 p.m. | Encrypted Message Here |
| 21 | Patient0121 | Patient 21 | PhysicianE1005 | Physician E | Sun 7 Feb. 2021 9:16 a.m. I have a shortness of breath when I talk or walk | Sun 7 Feb. 2021 11:25 a.m. | Encrypted Message Here |
| 22 | Patient0122 | Patient 22 | PhysicianE1005 | Physician E | Tues 9 Feb. 2021 12:42 p.m. I feel strong headache for a quite long period of time | Tues 9 Feb. 2021 1:18 p.m. | Encrypted Message Here |
| 23 | Patient0123 | Patient 23 | PhysicianE1005 | Physician E | Wend 10 Feb. 2021 11:27 a.m. Unable to breath and I have side effects of some drugs for covid | Wend 10 Feb. 2021 11:57 a.m. | Encrypted Message Here |
| 24 | Patient0124 | Patient 24 | PhysicianE1005 | Physician E | Thurs 11 Feb. 2021 9:48 a.m. I think I am infected with COVID because I have a diarrhoea | Thurs 11 Feb. 2021 10:21 a.m. | Encrypted Message Here |
| 25 | Patient0125 | Patient 25 | PhysicianE1005 | Physician E | Thurs 11 Feb. 2021 11:59 a.m. I have a sore throat | Thurs 11 Feb. 2021 15:37 p.m. | Encrypted Message Here |
| Tele-COVID Response Time, and Diagnosis | Physician’s Encrypted Message | Hospital Response Time and Message | Hospital’s Encrypted Message | Ambulance Dispatched | Pharmacy Response Time and Message | Pharmacy’s Encrypted Message |
|---|---|---|---|---|---|---|
| Tues 5 Jan. 2021 9:07 a.m. Appointement is needed | Encrypted Message Here | Tues 5 Jan. 2021 09:26 a.m. | Not Applicable | Not Applicable | Not Applicable | Not Applicable |
| Tues 5 Jan. 2021 10:04 a.m. Medicine is prescribed | Not Applicable | Tues 5 Jan. 2021 10:16 a.m. | Not Applicable | Not Applicable | Thurs 7 Jan. 2021 14:41 p.m. | Encrypted Message Here |
| Tues 5 Jan. 2021 10:28 a.m. Appointment is needed | Encrypted Message Here | Tues 5 Jan. 2021 10:55 a.m. | Not Applicable | Not Applicable | Not Applicable | Not Applicable |
| Tues 5 Jan. 2021 11:13 a.m. An a.m.bulance is sent | Not Applicable | Tues 5 Jan. 2021 11:24 a.m. | Encrypted Message Here | Tues 5 Jan. 2021 12:01 p.m. | Not Applicable | Not Applicable |
| Tues 5 Jan. 2021 13:02 p.m. Appointment is needed | Encrypted Message Here | Tues 5 Jan. 2021 13:43 p.m. | Not Applicable | Not Applicable | Not Applicable | Not Applicable |
| Wend 6 Jan. 2021 09:57 a.m. An a.m.bulance is sent | Not Applicable | Wend 6 Jan. 2021 10:03 a.m. | Encrypted Message Here | Wend 6 Jan. 2021 10:43 a.m. | Not Applicable | Not Applicable |
| Wend 6 Jan. 2021 10:33 a.m. Medicine is prescribed | Not Applicable | Wend 6 Jan. 2021 10:48 a.m. | Not Applicable | Not Applicable | Thurs 7 Jan. 2021 13:14 p.m. | Encrypted Message Here |
| Wend 6 Jan. 2021 11:07 a.m. Appointment is needed | Encrypted Message Here | Wend 6 Jan. 2021 11:34 a.m. | Not Applicable | Not Applicable | Not Applicable | Not Applicable |
| Wend 6 Jan. 2021 13:04 p.m. An a.m.bulance is sent | Not Applicable | Wend 6 Jan. 2021 13:19 p.m. | Encrypted Message Here | Wend 6 Jan. 2021 13:56 p.m. | Not Applicable | Not Applicable |
| Wend 6 Jan. 2021 13:43 p.m. An a.m.bulance is sent | Not Applicable | Wend 6 Jan. 2021 13:59 p.m. | Encrypted Message Here | Wend 6 Jan. 2021 15:16 p.m. | Not Applicable | Not Applicable |
| Thurs 7 Jan. 20219:33 a.m. Medicine is prescribed | Not Applicable | Thurs 7 Jan. 2021 10:07 a.m. | Not Applicable | Not Applicable | Fri 8 Jan. 2021 10:43 p.m. | Encrypted Message Here |
| Thurs 7 Jan. 2021 11:20 a.m. Appointment is needed | Encrypted Message Here | Thurs 7 Jan. 2021 11:37 a.m. | Not Applicable | Not Applicable | Not Applicable | Not Applicable |
| Thurs 7 Jan. 2021 14:10 p.m. Appointment is needed | Encrypted Message Here | Thurs 7 Jan. 2021 14:16 p.m. | Not Applicable | Not Applicable | Not Applicable | Not Applicable |
| Thurs 7 Jan. 2021 15:13 a.m. An a.m.bulance is sent | Not Applicable | Thurs 7 Jan. 2021 15:36 p.m. | Encrypted Message Here | Thurs 7 Jan. 2021 15:47 p.m. | Not Applicable | Not Applicable |
| Thurs 7 Jan. 2021 15:50 p.m. Medicine is prescribed | Not Applicable | Thurs 7 Jan. 2021 16:24 p.m. | Not Applicable | Not Applicable | Fri 8 Jan. 2021 14:42 p.m. | Encrypted Message Here |
| Fri 8 Jan. 2021 9:37 a.m. An a.m.bulance is sent | Not Applicable | Fri 8 Jan. 2021 10:11 a.m. | Encrypted Message Here | Fri 8 Jan. 2021 10:52 a.m. | Not Applicable | Not Applicable |
| Fri 8 Jan. 2021 10:17 a.m. Appointment is needed | Encrypted Message Here | Fri 8 Jan. 2021 10:39 a.m. | Not Applicable | Not Applicable | Not Applicable | Not Applicable |
| Fri 8 Jan. 2021 10:53 a.m. Medicine is prescribed | Not Applicable | Fri 8 Jan. 2021 11:18 a.m. | Not Applicable | Not Applicable | Sat 9 Jan. 2021 14:49 p.m. | Encrypted Message Here |
| Fri 8 Jan. 2021 11:25 a.m. Medicine is prescribed | Not Applicable | Fri 8 Jan. 2021 11:47 a.m. | Not Applicable | Not Applicable | Sat 9 Jan. 2021 14:49 p.m. | Encrypted Message Here |
| Fri 8 Jan. 2021 14:10 p.m. Appointment is needed | Encrypted Message Here | Fri 8 Jan. 2021 14:34 p.m. | Not Applicable | Not Applicable | Not Applicable | Not Applicable |
| Mon 8 Feb. 2021 19:07 a.m. An a.m.bulance is sent | Not Applicable | Mon 8 Feb. 2021 14:39 a.m. | Encrypted Message Here | Mon 8 Feb. 2021 20:32 a.m. | Not Applicable | Not Applicable |
| Tues 9 Feb. 2021 15:22 p.m. Appointment is needed | Encrypted Message Here | Wend 10 Feb. 2021 10:09 p.m. | Not Applicable | Not Applicable | Not Applicable | Not Applicable |
| Wend 10 Feb. 2021 13:17 p.m. An ambulance is sent | Not Applicable | Wend 10 Feb. 2021 13:48 p.m. | Encrypted Message Here | Wend 10 Feb. 2021 21:19 p.m. | Not Applicable | Not Applicable |
| Thurs 11 Feb. 2021 12:40 p.m. Appointment is needed | Encrypted Message Here | Thurs 11 Feb. 2021 14:11 p.m. | Not Applicable | Not Applicable | Not Applicable | Not Applicable |
| Fri 12 Feb. 2021 09:19 a.m. Medicine is prescribed | Not Applicable | Fri 12 Feb. 2021 10:48 a.m. | Not Applicable | Not Applicable | Fri 12 Feb. 2021 11:15 a.m. | Encrypted Message Here |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shaikh, A.; Al Reshan, M.S.; Sulaiman, A.; Alshahrani, H.; Asiri, Y. Secure Telemedicine System Design for COVID-19 Patients Treatment Using Service Oriented Architecture. Sensors 2022, 22, 952. https://doi.org/10.3390/s22030952
Shaikh A, Al Reshan MS, Sulaiman A, Alshahrani H, Asiri Y. Secure Telemedicine System Design for COVID-19 Patients Treatment Using Service Oriented Architecture. Sensors. 2022; 22(3):952. https://doi.org/10.3390/s22030952
Chicago/Turabian StyleShaikh, Asadullah, Mana Saleh Al Reshan, Adel Sulaiman, Hani Alshahrani, and Yousef Asiri. 2022. "Secure Telemedicine System Design for COVID-19 Patients Treatment Using Service Oriented Architecture" Sensors 22, no. 3: 952. https://doi.org/10.3390/s22030952
APA StyleShaikh, A., Al Reshan, M. S., Sulaiman, A., Alshahrani, H., & Asiri, Y. (2022). Secure Telemedicine System Design for COVID-19 Patients Treatment Using Service Oriented Architecture. Sensors, 22(3), 952. https://doi.org/10.3390/s22030952