
External Auditory Stimulation as a Non-Pharmacological Sleep Aid


Abstract
1. Introduction
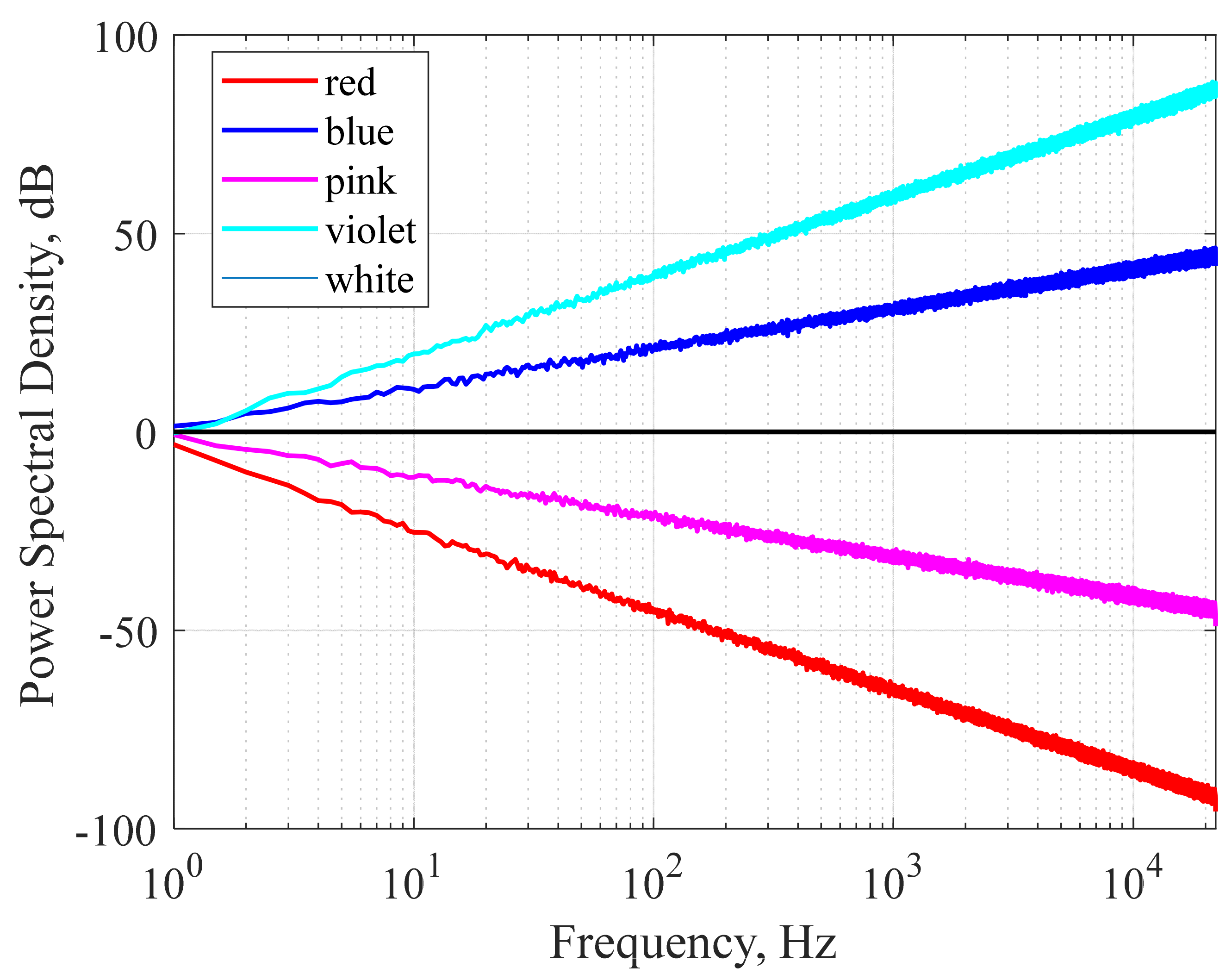
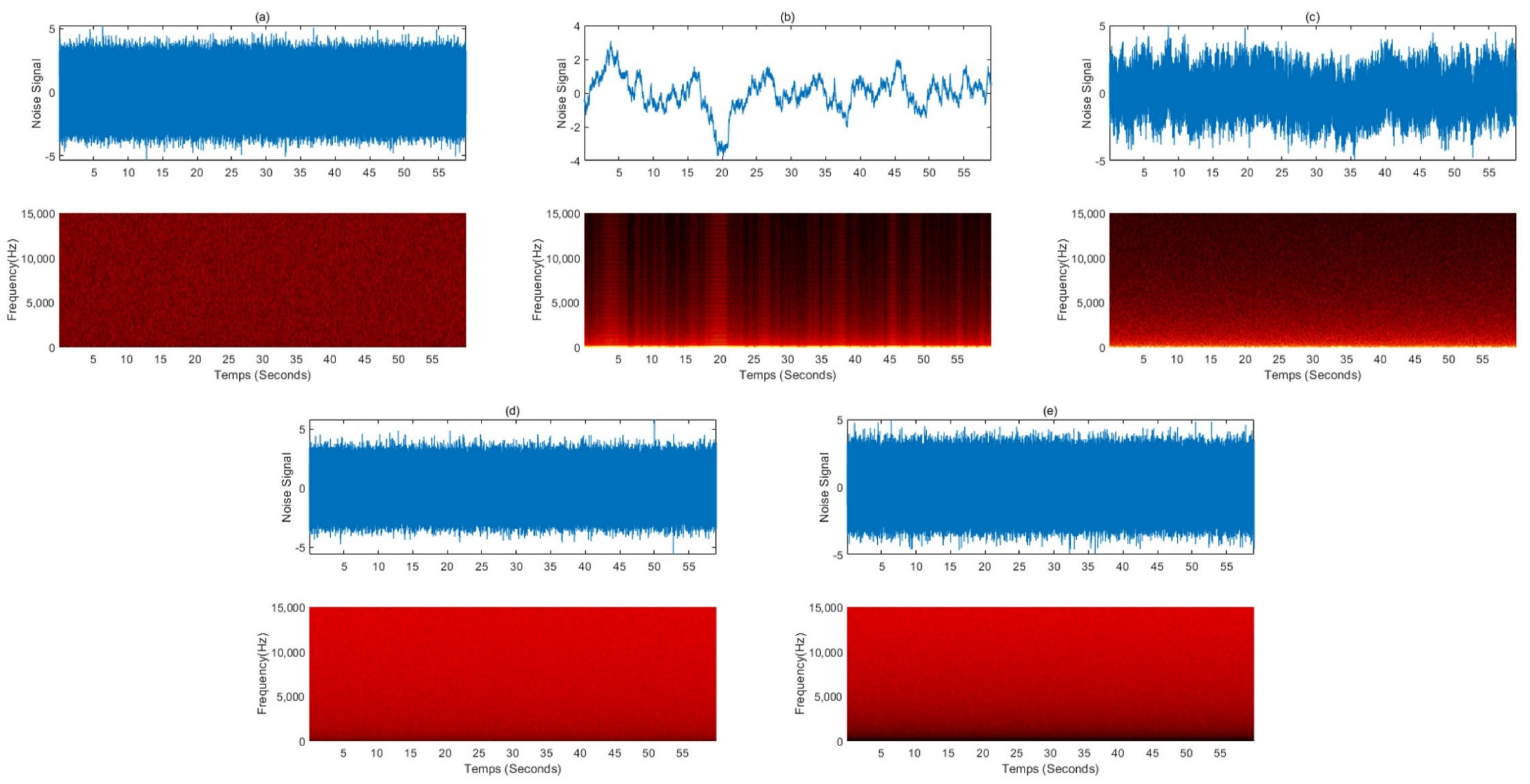
2. Pure Noise
3. Autonomous Sensory Meridian Response (ASMR)
4. Music
5. Discussion
5.1. Limitation
5.2. Treatment Satisfaction Questionaries for Medication
5.3. Effect of Auditory Stimulation on Sleep
5.4. Sleep Improving Evidence
5.5. Potential for Digital Therapeutic Applications
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Naomi, B.; Thomas, R.; Leon, R.; Andreski, P. Sleep Disturbance and Psychiatric Disorders: A Longitudinal Epidemiological Study of Young Adults. Biol. Psychiatry 1996, 39, 411–418. [Google Scholar]
- Lichstein, K.L.; Durrence, H.H.; Taylor, D.J.; Bush, A.J.; Riedel, B.W. Quantitative criteria for insomnia. Behav. Res. Ther. 2003, 41, 427–445. [Google Scholar] [CrossRef]
- Hughes, R.J.; Sack, R.L.; Lewy, A.J. The role of melatonin and circadian phase in age-related sleep-maintenance insomnia: Assessment in a clinical trial of melatonin replacement. Sleep 1998, 21, 52–68. [Google Scholar]
- Roth, T.; Walsh, J.K.; Krystal, A.; Wessel, T.; Roehrs, T.A. An evaluation of the efficacy and safety of eszopiclone over 12 months in patients with chronic primary insomnia. Sleep Med. 2005, 6, 487–495. [Google Scholar] [CrossRef]
- Espie, C.A.; Brooks, D.N.; Lindsay, W.R. An evaluation of tailored psychological treatment of insomnia. J. Behav. Ther. Exp. Psychiatry 1989, 20, 143–153. [Google Scholar] [CrossRef]
- Wu, R.; Bao, J.; Zhang, C.; Deng, J.; Long, C. Comparison of sleep condition and sleep-related psychological activity after cognitive-behavior and pharmacological therapy for chronic insomnia. Psychother. Psychosom. 2006, 75, 220–228. [Google Scholar] [CrossRef]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- American Psychiatry Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychaitry Association: Arlington, VA, USA, 2013. [Google Scholar]
- Walsh, J.K.; Coulouvrat, C.; Hajak, G.; Lakoma, M.D.; Petukhova, M.; Roth, T.; Sampson, N.A.; Shahly, V.; Shillington, A.; Stephenson, J.J.; et al. Nighttime insomnia symptoms and perceived health in the America Insomnia Survey (AIS). Sleep 2011, 34, 997–1011. [Google Scholar] [CrossRef]
- Roth, T.; Coulouvrat, C.; Hajak, G.; Lakoma, M.D.; Sampson, N.A.; Shahly, V.; Shillington, A.C.; Stephenson, J.J.; Walsh, J.K.; Kessler, R.C. Prevalence and perceived health associated with insomnia based on DSM-IV-TR; International Statistical Classification of Diseases and Related Health Problems, Tenth Revision; and Research Diagnostic Criteria/International Classification of Sleep Disorders, Second Edition criteria: Results from the America Insomnia Survey. Biol. Psychiatry 2011, 69, 592–600. [Google Scholar]
- Morin, C.M.; LeBlanc, M.; Daley, M.; Gregoire, J.P.; Merette, C. Epidemiology of insomnia: Prevalence, self-help treatments, consultations, and determinants of help-seeking behaviors. Sleep Med. 2006, 7, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med. Rev. 2002, 6, 97–111. [Google Scholar] [CrossRef]
- Roth, T. Insomnia: Definition, prevalence, etiology, and consequences. J. Clin. Sleep Med. 2007, 3, S7–S10. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Hong, S.C. Prevalence of insomnia and associated factors in South Korea. J. Psychosom. Res. 2002, 53, 593–600. [Google Scholar] [CrossRef]
- Cho, Y.W.; Shin, W.C.; Yun, C.H.; Hong, S.B.; Kim, J.; Earley, C.J. Epidemiology of insomnia in korean adults: Prevalence and associated factors. J. Clin. Neurol. 2009, 5, 20–23. [Google Scholar] [CrossRef]
- Chung, S.; Cho, S.W.; Jo, M.W.; Youn, S.; Lee, J.; Sim, C.S. The Prevalence and Incidence of Insomnia in Korea during 2005 to 2013. Psychiatry Investig. 2020, 17, 533–540. [Google Scholar] [CrossRef]
- Wang, C.; Song, W.; Hu, X.; Yan, S.; Zhang, X.; Wang, X.; Chen, W. Depressive, anxiety, and insomnia symptoms between population in quarantine and general population during the COVID-19 pandemic: A case-controlled study. BMC Psychiatry 2021, 21, 99. [Google Scholar] [CrossRef]
- Voitsidis, P.; Gliatas, I.; Bairachtari, V.; Papadopoulou, K.; Papageorgiou, G.; Parlapani, E.; Syngelakis, M.; Holeva, V.; Diakogiannis, I. Insomnia during the COVID-19 pandemic in a Greek population. Psychiatry Res. 2020, 289, 113076. [Google Scholar] [CrossRef] [PubMed]
- Şahin, M.K.; Aker, S.; Şahin, G.; Karabekiroğlu, A. Prevalence of Depression, Anxiety, Distress and Insomnia and Related Factors in Healthcare Workers During COVID-19 Pandemic in Turkey. J. Community Health 2020, 45, 1168–1177. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Qin, Q.; Sun, Q.; Sanford, L.D.; Vgontzas, A.N.; Tang, X. Insomnia and psychological reactions during the COVID-19 outbreak in China. J. Clin. Sleep Med. 2020, 16, 1417–1418. [Google Scholar] [CrossRef] [PubMed]
- Danzig, R.; Wang, M.; Shah, A.; Trotti, L.M. The wrist is not the brain: Estimation of sleep by clinical and consumer wearable actigraphy devices is impacted by multiple patient- and device-specific factors. J. Sleep Res. 2020, 29, e12926. [Google Scholar] [CrossRef]
- Edinger, J.D.; Wohlgemuth, W.K.; Radtke, R.A.; Marsh, G.R.; Quillian, R.E. Cognitive behavioral therapy for treatment of chronic primary insomnia: A randomized controlled trial. JAMA 2001, 285, 1856–1864. [Google Scholar] [CrossRef]
- Morin, C.M.; Colecchi, C.; Stone, J.; Sood, R.; Brink, D. Behavioral and pharmacological therapies for late-life insomnia: A randomized controlled trial. JAMA 1999, 281, 991–999. [Google Scholar] [CrossRef] [PubMed]
- Luik, A.I.; Kyle, S.D.; Espie, C.A. Digital cognitive behavioral therapy (dCBT) for insomnia: A state-of-the-science review. Curr. Sleep Med. Rep. 2017, 3, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Seyffert, M.; Lagisetty, P.; Landgraf, J.; Chopra, V.; Pfeiffer, P.N.; Conte, M.L.; Rogers, M.A. Internet-delivered cognitive behavioral therapy to treat insomnia: A systematic review and meta-analysis. PLoS ONE 2016, 11, e0149139. [Google Scholar] [CrossRef]
- Koffel, E.; Bramoweth, A.D.; Ulmer, C.S. Increasing access to and utilization of cognitive behavioral therapy for insomnia (CBT-I): A narrative review. J. Gen. Intern. Med. 2018, 33, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Coulson, N.S.; Smedley, R.; Bostock, S.; Kyle, S.D.; Gollancz, R.; Luik, A.I.; Hames, P.; Espie, C.A. The Pros and Cons of Getting Engaged in an Online Social Community Embedded within Digital Cognitive Behavioral Therapy for Insomnia: Survey among Users. J. Med. Internet Res. 2016, 18, e88. [Google Scholar] [CrossRef]
- Thomas, K.A.; Martin, P.A. NICU sound environment and the potential problems for caregivers. J. Perinatol. 2000, 20, S94–S99. [Google Scholar] [CrossRef]
- Tomei, F.; Papaleo, B.; Baccolo, T.P.; Persechino, B.; Spano, G.; Rosati, M.V. Noise and gastric secretion. Am. J. Ind. Med. 1994, 26, 367–372. [Google Scholar] [CrossRef]
- Falk, S.A.; Woods, N. Hospital noise: Levels and potential health hazards. N. Engl. J. Med. 1973, 289, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Nurminen, T. Female noise exposure, shift work and reproduction. J. Occup. Environ. Med. 1995, 37, 945–950. [Google Scholar] [CrossRef]
- Trahan, T.; Durrant, S.J.; Müllensiefen, D.; Williamson, V.J. The music that helps people sleep and the reasons they believe it works: A mixed methods analysis of online survey reports. PLoS ONE 2018, 13, e0206531. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Chang, E.-T.; Lai, H.-L. Use of integrative medicine approaches for treating adults with sleep disturbances. Appl. Nurs. Res. 2018, 43, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Spencer, J.A.; Moran, D.J.; Lee, A.; Talbert, D. White noise and sleep induction. Arch. Dis. Child. 1990, 65, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Forquer, L.M.; Johnson, C.M. Continuous White Noise to Reduce Sleep Latency and Night Wakings in College Students. Sleep Hypn. 2007, 9, 60–66. [Google Scholar]
- Ebben, M.R.; Yan, P.; Krieger, A.C. The effects of white noise on sleep and duration in individuals living in a high noise environment in New York City. Sleep Med. 2021, 83, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.E.; Hwang, S.K. The Effect of White Noise on Sleep in Hospitalized Patients: A Randomized Controlled Trial. Korean J. Adult Nurs. 2021, 33, 44–55. [Google Scholar] [CrossRef]
- Messineo, L.; Taranto-Montemurro, L.; Sands, S.A.; Oliveira Marques, M.D.; Azabarzin, A.; Wellman, D.A. Broadband Sound Administration Improves Sleep Onset Latency in Healthy Subjects in a Model of Transient Insomnia. Front. Neurol. 2017, 8, 718. [Google Scholar] [CrossRef]
- Papalambros, N.A.; Santostasi, G.; Malkani, R.G.; Braun, R.; Weintraub, S.; Paller, K.A.; Zee, P.C. Acoustic Enhancement of Sleep Slow Oscillations and Concomitant Memory Improvement in Older Adults. Front. Hum. Neurosci. 2017, 11, 109. [Google Scholar] [CrossRef]
- Zhou, J.; Liu, D.; Li, X.; Ma, J.; Zhang, J.; Fang, J. Pink noise: Effect on complexity synchronization of brain activity and sleep consolidation. J. Theor. 2012, 306, 68–72. [Google Scholar] [CrossRef]
- Kawada, T.; Suzuki, S. Sleep induction effects of steady 60 dB (A) pink noise. Ind. Health 1993, 31, 35–38. [Google Scholar] [CrossRef]
- Garcia-Molina, G.; Kalyan, B.; Aquino, A. Closed-Loop Electroencephalogram-Based Modulated Pink Noise to Facilitate Falling Asleep. Sleep 2020, 43, A457. [Google Scholar] [CrossRef]
- Poerio, G.L.; Blakey, E.; Hostler, T.J.; Veltri, T. More than a feeling: Autonomous sensory meridian response (ASMR) is characterized by reliable changes in affect and physiology. PLoS ONE 2018, 13, e0196645. [Google Scholar] [CrossRef] [PubMed]
- Williamson, J.W. The effects of ocean sounds on sleep after coronary artery bypass graft surgery. Am. J. Crit. Care 1992, 1, 91–97. [Google Scholar] [CrossRef]
- Hardian, H.; Febriani, S.S.; Sumekar, T.A.; Muniroh, M.; Indraswari, D.A.; Purwoko, Y.; Ambarwati, E. Improvement of Sleep Quality by Autonomous Sensory Meridian Response (ASMR) Stimulation Among Medical Students. Mal. J. Med. Health Sci. 2020, 16, 81–85. [Google Scholar]
- Umbas, J.C.G.; Bintang, A.K.; Aulina, S.; Bahar, A.; Akbar, M. The effect of white noise on high school students’ sleep quality at Unit B of Rajawali Girls Dormitory Makassar. Med. Clínica Práctica 2021, 4, 1. [Google Scholar] [CrossRef]
- Lee, T.; Moon, S.E.; Baek, J.; Lee, J.S.; Kim, S. Music for Sleep and Wake-Up: An Empirical Study. IEEE Access 2019, 7, 145816–145828. [Google Scholar] [CrossRef]
- Loewy, J. Music Therapy as a Potential Intervention for Sleep Improvement. Nat. Sci. Sleep 2020, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bloch, B.; Reshef, A.; Vadas, L.; Haliba, Y.; Ziv, N.; Kremer, I.; Haimov, I. The effects of music relaxation on sleep quality and emotional measures in people living with schizophrenia. J. Music Ther. 2010, 47, 27–52. [Google Scholar] [CrossRef] [PubMed]
- Iwaki, T.; Tanaka, H.; Hori, T. The Effects of Preferred Familiar Music on Falling Asleep. J. Music Ther. 2003, 40, 15–26. [Google Scholar] [CrossRef]
- Johnson, J.E. The use of music to promote sleep in older women. J. Community Health Nurs. 2003, 20, 27–35. [Google Scholar] [CrossRef]
- Lai, H.L.; Good, M. Music improves sleep quality in older adults. J. Adv. Nurs. 2005, 49, 234–244. [Google Scholar] [CrossRef]
- Shum, A.; Taylor, B.J.; Thayala, J.; Chan, M.F. The effects of sedative music on sleep quality of older community-dwelling adults in Singapore. Complement. Ther. Med. 2013, 22, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Chair, S.Y.; Wong, E.M.L.; Li, X. The Effects of Music Intervention on Sleep Quality in Community-Dwelling Elderly. J. Altern. Complement. Med. 2016, 22, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Dubey, P.; Kumar, Y.; Singh, R.; Jha, K.; Kumar, R. Effect of music of specific frequency upon the sleep architecture and electroencephalographic pattern of individuals with delayed sleep latency: A daytime nap study. J. Fam. Med. Prim. Care 2019, 8, 3915–3919. [Google Scholar]
- Jespersen, K.V.; Otto, M.; Kringelbach, M.; van Someren, E.; Vuust, P. A randomized controlled trial of bedtime music for insomnia disorder. J. Sleep Res. 2019, 28, e12817. [Google Scholar] [CrossRef] [PubMed]
- McCall, C.; McCall, W.V. Comparison of actigraphy with polysomnography and sleep logs in depressed insomniacs. J. Sleep Res. 2012, 21, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, K.A.; Talbot, L.S.; Gruber, J.; Harvey, A.G. Evaluating sleep in bipolar disorder: Comparison between actigraphy, polysomnography, and sleep diary. Bipolar Disord. 2012, 14, 870–879. [Google Scholar] [CrossRef]
- Matthews, K.A.; Patel, S.R.; Pantesco, E.J.; Buysse, D.J.; Kamarck, T.W.; Lee, L.; Hall, M.H. Similarities and differences in estimates of sleep duration by polysomnography, actigraphy, diary, and selfreported habitual sleep in a community sample. Sleep Health 2018, 4, 96–103. [Google Scholar] [CrossRef]
- Brody, D.; Miller, S.; Lerman, C.; Smith, D.; Caputo, G. Patient perception of involvement in medical care: Relationship to illness attitudes and outcomes. J. Gen. Intern. Med. 1989, 4, 506–511. [Google Scholar] [CrossRef]
- Taylor, T.R. Understanding the choices that patients make. J. Am. Board Fam. Pract. 2000, 13, 124–133. [Google Scholar] [CrossRef][Green Version]
- Albrecht, G.; Hoogstraten, J. Satisfaction as a determinant of compliance. Community Dent. Oral Epidemiol. 1998, 26, 139–146. [Google Scholar] [CrossRef]
- McCracken, L.M.; Klock, A.; Mingay, D.J.; Asbury, J.K.; Sinclair, D.M. Assessment of satisfaction with treatment for chronic pain. J. Pain Symptom Manag. 1997, 14, 292–299. [Google Scholar] [CrossRef]
- Weaver, M.; Patrick, D.L.; Markson, L.E.; Martin, D.; Frederic, I.; Berger, M. Issues in the measurement of satisfaction with treatment. Am. J. Manag. Care 1997, 3, 579–594. [Google Scholar]
- Zhang, Z.; Gerstein, D.R.; Friedmann, P.D. Patient satisfaction and sustained outcomes of drug abuse treatment. J. Health Psychol. 2008, 13, 388–400. [Google Scholar] [CrossRef]
- Awad, A.G.; Voruganti, L.N.P. Quality of life and new antipsychotics in schizophrenia. Are patients better off? Int. J. Soc. Psychiatry 1999, 45, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Diamond, R. Drugs and the quality of life: The patient’s point of view. J. Clin. Psychiatry 1985, 46, 29–35. [Google Scholar] [PubMed]
- Testa, M.A.; Simonson, D.C. Satisfaction and quality of life with premeal inhaled versus injected insulin in adolescents and adults with type 1 diabetes. Diabetes Care 2007, 30, 1399–1405. [Google Scholar] [CrossRef]
- Atkinson, M.J.; Sinha, A.; Hass, S.L.; Colman, S.S.; Kumar, R.N.; Brod, M.; Rowland, C.R. Validation of a general measure of treatment satisfaction, the Treatment Satisfaction Questionnaire for Medication (TSQM), using a national panel study of chronic disease. Health Qual. Life Outcomes 2004, 2, 12. [Google Scholar] [CrossRef] [PubMed]
- Bagel, J.; Levi, E.; Tyring, S.; Knuckles, M.L. Real-life treatment profile of calcipotriene and betamethasone dipropionate topical suspension in patients with psoriasis vulgaris. J. Drugs Dermatol. 2014, 13, 1374–1379. [Google Scholar] [PubMed]
- Whalley, D.; Petigara, T.; Rasouliyan, L.; Tobe, K.; Tunceli, K. Early patient experiences with montelukast orally disintegrating tablets in Japan: A cross-sectional survey of treatment satisfaction in patients with asthma and/or allergic rhinitis. Curr. Med. Res. Opin. 2017, 33, 215–223. [Google Scholar] [CrossRef]
- Dickson, G.T.; Schubert, E. How does music aid sleep? Literature review. Sleep Med. 2019, 63, 142–150. [Google Scholar] [CrossRef]
- Stanchina, M.L.; Abu-Hijleh, M.; Chaudhry, B.K.; Carlisle, C.C.; Millman, R.P. The influence of white noise on sleep in subjects exposed to ICU noise. Sleep Med. 2005, 6, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Talbot, L.S.; Hairston, I.S.; Eidelman, P.; Gruber, J.; Harvey, A.G. The effect of mood on sleep onset latency and REM sleep in interepisode bipolar disorder. J. Abnorm. Psychol. 2009, 118, 448–458. [Google Scholar] [CrossRef]
- Yu, B.; An, P.; Hendriks, S.; Zhang, N.; Feijs, L.; Li, M.; Hu, J. ViBreathe: Heart Rate Variability Enhanced Respiration Training for Workaday Stress Management via an Eyes-Free Tangible Interface. Int. J. Hum. -Comput. Int. 2021, 37, 1551–1570. [Google Scholar] [CrossRef]
- Roth, T.; Soubrane, C.; Titeux, L.; Walsh, J.K. Efficacy and safety of zolpidem-MR: A double-blind, placebo-controlled study in adults with primary insomnia. Sleep Med. 2006, 7, 397–406. [Google Scholar] [CrossRef]
- Scharf, M.B.; Roth, P.B.; Dominguez, R.A.; Ware, J.C. Estazolam and Flurazepam: A Multicenter, Placebo-Controlled Comparative Study in Outpatients with Insomnia. J. Clin. Pharmacol. 1990, 30, 461–467. [Google Scholar] [CrossRef]
- McCall, W.V.; D’Agostino, R.; Dunn, A. A meta-analysis of sleep changes associated with placebo in hypnotic clinical trials. Sleep Med. 2003, 4, 57–62. [Google Scholar] [CrossRef]
- Perlis, M.L.; McCall, W.V.; Jungquist, C.R.; Pigeon, W.R.; Matteson, S.E. Placebo effects in primary insomnia. Sleep Med. Rev. 2005, 9, 381–389. [Google Scholar] [CrossRef]
- Elison, S.; Ward, J.; Williams, C.; Espie, C.; Davies, G.; Dugdale, S.; Ragan, K.; Chisnall, L.; Lidbetter, N.; Smith, K. Feasibility of a UK community-based, eTherapy mental health service in Greater Manchester: Repeated-measures and between-groups study of ‘Living Life to the Full Interactive’, ‘Sleepio’ and ‘Breaking Free Online’ at ‘Self Help Services’. BMJ Open 2017, 7, e016392. [Google Scholar] [CrossRef]
- Cheng, P.; Kalmbach, D.A.; Tallent, G.; Joseph, C.L.; Espie, C.A.; Drake, C.L. Depression prevention via digital cognitive behavioral therapy for insomnia: A randomized controlled trial. Sleep 2019, 42, zsz150. [Google Scholar] [CrossRef] [PubMed]
- Espie, C.A.; Emsley, R.; Kyle, S.D.; Gordon, C.; Drake, C.L.; Siriwardena, A.N.; Cape, J.; Ong, J.C.; Sheaves, B.; Foster, R.; et al. Effect of digital cognitive behavioral therapy for insomnia on health, psychological well-being, and sleep-related quality of life: A randomized clinical Trial. JAMA Psychiatry 2019, 76, 21–30. [Google Scholar] [CrossRef]
- Felder, J.N.; Epel, E.S.; Neuhaus, J.; Krystal, A.D.; Prather, A.A. Efficacy of digital cognitive behavioral therapy for the treatment of insomnia symptoms among pregnant women: A randomized clinical trial. JAMA Psychiatry 2020, 77, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Ritterband, L.M.; Thorndike, F.P.; Ingersoll, K.S.; Lord, H.R.; Gonder-Frederick, L.; Frederick, C.; Quigg, M.S.; Cohn, W.F.; Morin, C.M. Effect of a web-based cognitive behavior therapy for insomnia intervention with 1-year follow-up: A randomized clinical trial. JAMA Psychiatry 2017, 74, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M. Profile of somryst prescription digital therapeutic for chronic insomnia: Overview of safety and efficacy. Expert Rev. Med. Devices 2020, 17, 1239–1248. [Google Scholar] [CrossRef] [PubMed]
- Vedaa, Ø.; Kallestad, H.; Scott, J.; Smith, O.R.; Pallesen, S.; Morken, G.; Langsrud, K.; Gehrman, P.; Thorndike, F.P.; Ritterband, L.M.; et al. Effects of digital cognitive behavioural therapy for insomnia on insomnia severity: A large-scale randomised controlled trial. Lancet Digit. Health 2020, 2, e397–e406. [Google Scholar] [CrossRef]
- Lee, H.A.; Lee, H.J.; Moon, J.H.; Lee, T.; Kim, M.G.; In, H.; Cho, C.H.; Kim, L. Comparison of wearable activity tracker with actigraphy for sleep evaluation and circadian rest-activity rhythm measurement in healthy young adults. Psychiatry Investig. 2017, 14, 179. [Google Scholar] [CrossRef]
- Baek, H.J.; Cho, J. Novel heart rate variability index for wrist-worn wearable devices subject to motion artifacts that complicate measurement of the continuous pulse interval. Physiol. Meas. 2019, 40, 105010. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Product Category | Product Name | Sound Material | Additional Functions | Photo |
|---|---|---|---|---|
| Sound machine | Sound + Sleep Mini | 12 audio programs, each with multiple options for environment and complexity, for a total of 48 unique audio settings (rainfall, flowing water, ocean, city, white/pink/brown noise, etc.) | Built-in microphone to listen to your environment and dynamically adjust the volume based on ambient noise levels |  |
| Sound machine | Lectrofan | 12 unique digital sounds to mask noises and a choice from 10 electric fan sounds and 10 variations of pure white noise (including pink and brown noise variations) | Soft-glow reading light without eye-straining blue hues |  |
| Sound machine | Hatch Restore | Library of soothing sounds (white noise, ocean, rain, water, wind, birds, dryer, heartbeat, etc) | Sunrise alarm, smart light, meditation app, and an alarm clock |  |
| Sound machine | WAVE™ | 6 soothing sounds (white noise, fan, ocean, rain, stream, and summer night) | USB port with 2A output to charge USB-powered device |  |
| Sound machine | Letsfit T126L | 14 natural sounds (white noise, ocean wave, crickets, fan noise, clothes dryer, birds, thunderstorm, water stream, nursery rhyme) | Warm night-light |  |
| Wearable | Sleepphones | 17 audio tracks featuring binaural beat technology (colored noise, waterfall, stream, waves, etc.) | For listening to music and TV in bed at night while your partner sleeps |  |
| App | Sleepmaker Rain1 | 21 rain sounds (rainfall in forests, rain against window with wind, rain onto porch roof, torrential downpour, etc.) | Programmable Sleep Timer |  |
| App | Sleepa | Sleepa Sound Library (rain, forest, creek, wind, fire, city sound, colored noise, binaural beats that replicate brainwaves) | Mix, match, and save over 120 M combinations of soundsProgrammable Sleep Timer |  |
| First Author, Year, Country | Study Design | Participants | N, Mean Age ± SD (or Range) | Noise (Method) | Intervention Duration | Control Group | Sleep Measure(s) | Sleep Outcomes |
|---|---|---|---|---|---|---|---|---|
| Spencer (1990) England | Randomized controlled trial | Healthy neonates | 40, (2–7 days old) | White noise (speaker) | Four and a half minutes | Not exposed to white noise | Observed by a single investigator | 80% of babies fell asleep when they were exposed to the white noise compared with 25% who fell asleep in the control group. |
| Forquer&Johnson (2007) USA | Crossover | Healthy college students | 4, 19 | White noise (speaker) | Continuously from bedtime to waking for 7 nights | None | Sleep diary, PSQI, sleep hygiene test | Decrease in both sleep latency and night wakings during treatment |
| Rosalez (2020) | Crossover | ADHD Children | 3 (9–11) | White noise (speaker) | Continuous at night | Not exposed to white noise | Sleep diary | Decreased bedtime sleep latency and spontaneous night wakings at home |
| Ebben (2021) USA | Crossover | Adults with insomnia | 10, 58 (39–74) | White noise (speaker) | 2nd week of 3 weeks, | None | Daily sleep diary and actigraphy | Reduced WASO and sleep latency, reduced the number of awakenings during the night, improved sleep efficiency |
| Cho (2021) Korea | Randomized controlled trial | Adult inpatient | 61 | White noise (earphone) | 1 h per night for 3 days | Wear earplugs | VSH, actigraphy | Positive effects on subjective sleep quality, improved sleep time and sleep efficiency |
| Messineo (2017) USA | Crossover | Healthy adults | 18 (20–65) | Broadband (speaker) | 1 of 2 weeks | None | PSG, PSQI, VAS, SSS | Reduced sleep onset latency, improved subjective sleep quality |
| Kawada (1993) Japan | Crossover | Healthy young subjects | 4, 19.8 (19–21) | Pink noise (speaker) | 1 of 2 days | None | PSG | Reduced sleep latency |
| Garcia-Molina (2020) USA | Crossover | Healthy subjects | 7, 33.6 ± 8.7 | Pink noise (headband) | 4 of 5 sleep sessions | None | PSG | Reduced slap latency |
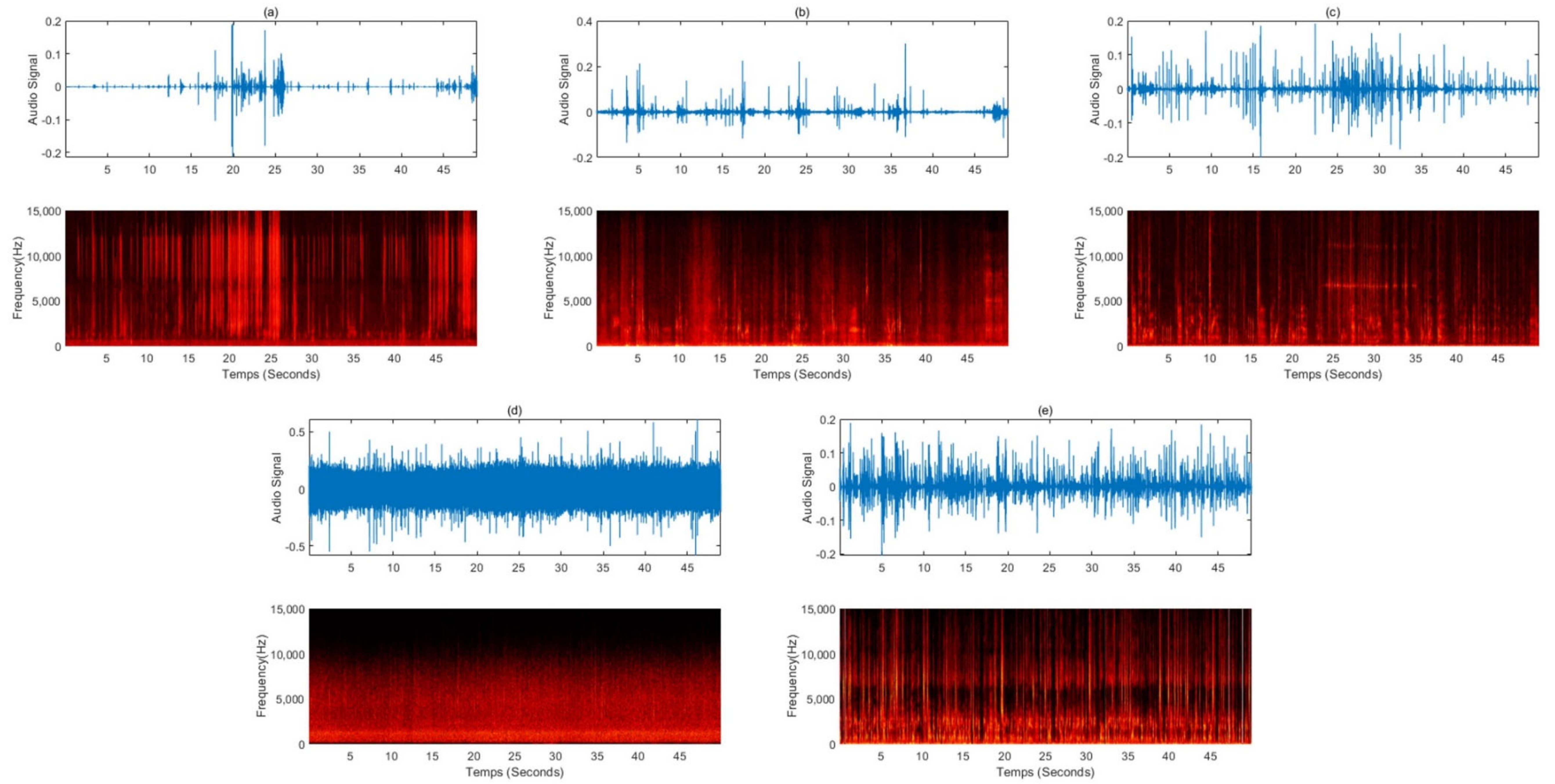
| Num | Sound | URL | Total Views |
|---|---|---|---|
| (a) | The sound of making glossy slime with a piping bag | https://youtu.be/NaHEoL1Zs-E | 3,113,664 |
| (b) | A voice whispering softly during a hair shop role play | https://youtu.be/yWIXozR85c0 | 1,694,665 |
| (c) | The sound of an oil massage and the whispering sound overlapped | https://youtu.be/j71CE1dpwmw | 681,237 |
| (d) | The sound of raindrops falling from the eaves and raindrops pouring | https://youtu.be/Ol5CxwbC5ag | 746,214 |
| (e) | Steel wool sponges, the sound of rubbing various brushes, dolls, paper packaging materials, toys, etc. | https://youtu.be/We02eW1950M | 500,158 |
| First Author, Year, Country | Study Design | Participant | N, Mean Age ± SD (or Range) | Noise (Method) | Intervention Duration | Control Group | Sleep Measure(s) | Sleep Outcomes |
|---|---|---|---|---|---|---|---|---|
| Williamson (1992) USA | Randomized controlled trial | First-time CABG patients | 60 | Soothing nature sounds such as rain, waves, or waterfalls (speaker) | Three consecutive nights posttransfer from the ICU | Not exposed to ocean sound | Richards–Campbell Sleep Questionnaire, a visual analog scale | Falling asleep faster and maintaining sleep |
| Hardian (2020) Indonesia | Randomized controlled trial | Students at medical college | 30, 18.4 ± 0.72, 17~20 | Haircut, cooking, whispering, rubbing, delicate hand movements (earphone) | 14 days, 20 min from 9:00 pm | Not exposed to ASMR | PSQI | Improved subjective sleep quality |
| Umbas (2021) Indonesia | Crossover | High school students | 12 (16–18) | Rain sound (speaker) | Whole night for 30 days | None | PSQI | Reducing sleep onset latency Triggering deeper sleep |
| First Author, Year, Country | Study Design | Participant | N, Mean Age ± SD (or Range) | Noise (Method) | Intervention Duration | Control Group | Sleep Measure(s) | Sleep Outcomes |
|---|---|---|---|---|---|---|---|---|
| Iwaki (2003) Japan | Crossover | Healthy university students | 20 (20–28) | Preferred familiar music (speaker) | 1 week before nap | No music played | PSG, KSS | Reduced sleep latency in natural sleep |
| Johnson (2003) USA | Crossover | Older subjects with insomnia | 52 (80.5, 71–87) | Participant selected music (NA) | turn the music on as soon as they got into bed for 10 nights | No music played | Stanford Sleepiness Scale Sleep log | Significant increase in level of sleepiness at bedtime Significant decrease in time to sleep onset and number of nighttime awakenings |
| Lai (2006) USA | Randomized controlled trial | Subjects with difficulty in sleeping | 60 (60~83) | five types of Western and one of Chinese music (NA) | 45 min at bedtime for 3 weeks | No music played | PSQI, ESC | Better sleep quality, better perceived sleep quality, longer sleep duration, greater sleep efficiency, shorter sleep latency, less sleep disturbance, and less daytime dysfunction |
| Bloch (2010) Israel | Crossover | Subjects with schizophrenia | 24, 45.67 ± 9.6 (18~70) | Relaxation music composed specifically for the study (speaker) | 40 min at bedtime, 7 of 14 days | No intervention | Actigraphy, Subjective sleep questionnaires | Reduced sleep latency, improved sleep efficiency, reduction in the number of reported complaints of subjective insomnia |
| Shum (2014) Singapore | Randomized controlled trial | Community-dwelling older adults | 60, 55 years or above | Soft, instrumental slow sedative music without lyrics (earphone) | 40 min per night for 6 weeks | Not listen to sedative music, but they were not restricted from listening to radio or TV | PSQI | Improving sleep quality |
| Wang (2016) China | Randomized controlled trial | Older with poor sleep quality | 64, 69.38 ± 5.46 | Preferred music (earphone) | 30–45 min per night for 3 months | No intervention | PSQI, QoS | Improving sleep latency, sleep efficiency, and daytime dysfunction |
| Dubey (2019) India | Crossover | Healthy male volunteer with a history of delayed sleep latency | 15 (18~40) | 432 Hz music (NA) | 15 to 20 min before nap | No intervention | PSG | Decrease in the mean sleep latency, increase in the energy of alpha waves at the sleep onset. |
| Jespersen (2019) Denmark | Randomized controlled trial | Subjects with insomnia | 57 (18 and 65) | Classical, jazz, new age, and ambient music (NA) | Minimum 30-min at bedtime for 3 weeks | No intervention | PSG, PSQI, pQoL | Positive impact on sleep perception and quality of life, reduced sleep onset latency |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, H.; Baek, H.J. External Auditory Stimulation as a Non-Pharmacological Sleep Aid. Sensors 2022, 22, 1264. https://doi.org/10.3390/s22031264
Yoon H, Baek HJ. External Auditory Stimulation as a Non-Pharmacological Sleep Aid. Sensors. 2022; 22(3):1264. https://doi.org/10.3390/s22031264
Chicago/Turabian StyleYoon, Heenam, and Hyun Jae Baek. 2022. "External Auditory Stimulation as a Non-Pharmacological Sleep Aid" Sensors 22, no. 3: 1264. https://doi.org/10.3390/s22031264
APA StyleYoon, H., & Baek, H. J. (2022). External Auditory Stimulation as a Non-Pharmacological Sleep Aid. Sensors, 22(3), 1264. https://doi.org/10.3390/s22031264