

Application of Patient Reported Outcome Measures in Cochlear Implant Patients: Implications for the Design of Specific Rehabilitation Programs

 ,
,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Approval
2.2. Participants
- Patients older than 11 years;
- Last CI surgery at least 12 months before evaluation;
- Regular follow-up controls.
- Not willing to complete the survey;
- Presence of neurological or psychiatric disorders.
2.3. PRO Measures
2.4. Developing of the Rehab Factor
2.5. Audiological Evaluation
2.6. Statistical Analysis
3. Results
3.1. Group Data
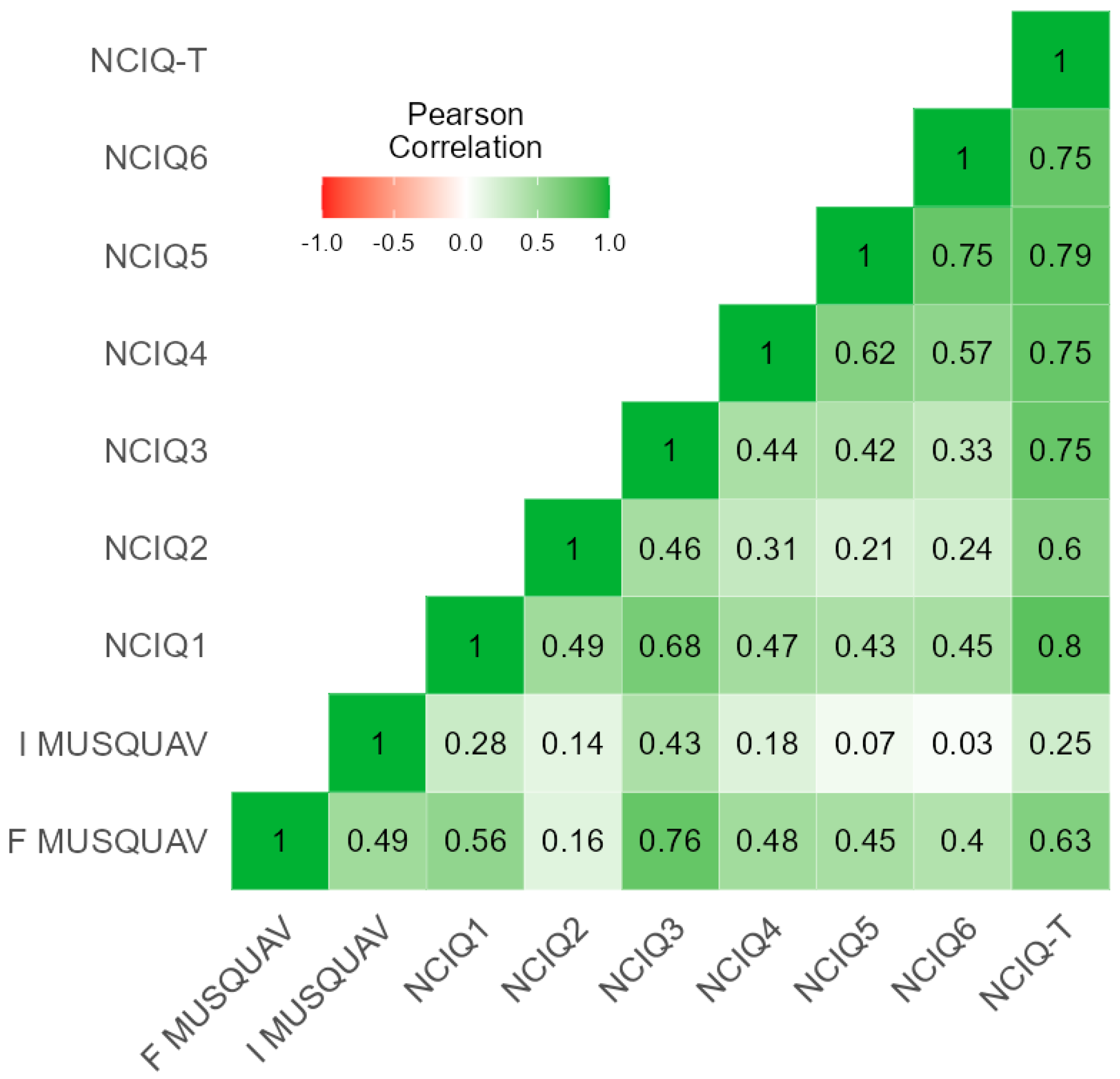
3.2. PRO Measures Correlations
3.3. The REEHAB Factor
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Mandalà, M.; Mazzocchin, L.; Ward, B.K.; Viberti, F.; Bindi, I.; Salerni, L.; Colletti, G.; Colletti, L.; Colletti, V. A retrospective evaluation to assess reliability of electrophysiological methods for diagnosis of hearing loss in infants. Brain Sci. 2022, 12, 950. [Google Scholar] [CrossRef] [PubMed]
- Sorrentino, F.; Gheller, F.; Lunardi, G.; Brotto, D.; Trevisi, P.; Martini, A.; Marioni, G.; Bovo, R. Cochlear implantation in adults with auditory deprivation: What do we know about it? Am. J. Otolaryngol. 2020, 41, 102366. [Google Scholar] [CrossRef] [PubMed]
- Freni, F.; Gazia, F.; Slavutsky, V.; Perello Scherdel, E.; Nicenboim, L.; Posada, R.; Portelli, D.; Galletti, B.; Galletti, F. Cochlear implant surgery: Endomeatal approach versus posterior tympanotomy. Int. J. Environ. Res. Public Health 2020, 17, 4187. [Google Scholar] [CrossRef]
- Forli, F.; Lazzerini, F.; Fortunato, S.; Bruschini, L.; Berrettini, S. Cochlear implant in the elderly: Results in terms of speech perception and quality of life. Audiol. Neurotol. 2019, 24, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Favaretto, N.; Marioni, G.; Brotto, D.; Sorrentino, F.; Gheller, F.; Castiglione, A.; Montino, S.; Giacomelli, L.; Trevisi, P.; Martini, A.; et al. Cochlear implant outcomes in the elderly: A uni- and multivariate analyses of prognostic factors. Eur. Arch. Otorhinolaryngol. 2019, 276, 3089–3094. [Google Scholar] [CrossRef]
- Lehmann, A.; Limb, C.J.; Marozeau, J. Editorial: Music and cochlear implants: Recent developments and continued challenges. Front. Neurosci. 2021, 15, 736772. [Google Scholar] [CrossRef]
- Zimmer, V.; Verhey, J.L.; Ziese, M.; Böckmann-Barthel, M. Harmony perception in prelingually deaf, juvenile cochlear implant users. Front. Neurosci. 2019, 13, 466. [Google Scholar] [CrossRef]
- Hwa, T.P.; Wen, C.Z.; Ruckenstein, M.J. Assessment of music experience after cochlear implantation: A review of current tools and their utilization. World J. Otorhinolaryngol.—Head Neck Surg. 2021, 7, 116–125. [Google Scholar] [CrossRef]
- Petersen, B.; Andersen, A.S.F.; Haumann, N.T.; Højlund, A.; Dietz, M.J.; Michel, F.; Riis, S.K.; Brattico, E.; Vuust, P. The CI MuMuFe—A new MMN paradigm for measuring music discrimination in electric hearing. Front. Neurosci. 2020, 14, 2. [Google Scholar] [CrossRef] [Green Version]
- Gfeller, K.; Driscoll, V.; Schwalje, A. Adult cochlear implant recipients’ perspectives on experiences with music in everyday life: A multifaceted and dynamic phenomenon. Front. Neurosci. 2019, 13, 1229. [Google Scholar] [CrossRef]
- Gauer, J.; Nagathil, A.; Martin, R.; Thomas, J.P.; Völter, C. Interactive evaluation of a music preprocessing scheme for cochlear implants based on spectral complexity reduction. Front. Neurosci. 2019, 13, 1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spangmose, S.; Hjortkjær, J.; Marozeau, J. Perception of musical tension in cochlear implant listeners. Front. Neurosci. 2019, 13, 987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galvin, J.J.; Fu, Q.-J.; Nogaki, G. Melodic contour identification by cochlear implant listeners. Ear Hear. 2007, 28, 302–319. [Google Scholar] [CrossRef] [Green Version]
- Phillips-Silver, J.; Toiviainen, P.; Gosselin, N.; Turgeon, C.; Lepore, F.; Peretz, I. Cochlear implant users move in time to the beat of drum music. Hear. Res. 2015, 321, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Fuller, C.; Başkent, D.; Free, R. Early deafened, late implanted cochlear implant users appreciate music more than and identify music as well as postlingual users. Front. Neurosci. 2019, 13, 1050. [Google Scholar] [CrossRef] [Green Version]
- Drennan, W.R. Music perception in cochlear implant users and its relationship with psychophysical capabilities. J. Rehabil. Res. Dev. 2008, 45, 779–790. [Google Scholar] [CrossRef] [PubMed]
- Churruca, K.; Pomare, C.; Ellis, L.A.; Long, J.C.; Henderson, S.B.; Murphy, L.E.D.; Leahy, C.J.; Braithwaite, J. Patient-Reported Outcome Measures (PROMs): A review of generic and condition-specific measures and a discussion of trends and issues. Health Expect. 2021, 24, 1015–1024. [Google Scholar] [CrossRef]
- Vasil, K.J.; Lewis, J.; Tamati, T.; Ray, C.; Moberly, A.C. How does quality of life relate to auditory abilities? A subitem analysis of the Nijmegen cochlear implant questionnaire. J. Am. Acad. Audiol. 2020, 31, 292–301. [Google Scholar] [CrossRef]
- Hinderink, J.B.; Krabbe, P.F.M.; Van Den Broek, P. Development and application of a health-related quality-of-life instrument for adults with cochlear implants: The Nijmegen cochlear implant questionnaire. Otolaryngol. Neck Surg. 2000, 123, 756–765. [Google Scholar] [CrossRef]
- Dritsakis, G.; van Besouw, R.M.; Kitterick, P.; Verschuur, C.A. A music-related quality of life measure to guide music rehabilitation for adult cochlear implant users. Am. J. Audiol. 2017, 26, 268–282. [Google Scholar] [CrossRef]
- Frosolini, A.; Parrino, D.; Mancuso, A.; Coppola, N.; Genovese, E.; de Filippis, C. The music-related quality of life: Italian validation of MuRQoL into MUSQUAV questionnaire and preliminary data from a cohort of postlingually deafened cochlear implant users. Eur. Arch. Otorhinolaryngol. 2022, 279, 4769–4778. [Google Scholar] [CrossRef] [PubMed]
- Adel, Y.; Nagel, S.; Weissgerber, T.; Baumann, U.; Macherey, O. Pitch matching in cochlear implant users with single-sided deafness: Effects of electrode position and acoustic stimulus type. Front. Neurosci. 2019, 13, 1119. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, K.L.; Caldwell, M.; Limb, C.; Smith, S.; Kessler, D.M.; Gifford, R.H. Musical emotion perception in bimodal patients: Relative weighting of musical mode and tempo cues. Front. Neurosci. 2020, 14, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mo, J.; Jiam, N.T.; Deroche, M.L.D.; Jiradejvong, P.; Limb, C.J. Effect of frequency response manipulations on musical sound quality for cochlear implant users. Trends Hear. 2022, 26, 233121652211200. [Google Scholar] [CrossRef] [PubMed]
- Tahmasebi, S.; Gajȩcki, T.; Nogueira, W. Design and evaluation of a real-time audio source separation algorithm to remix music for cochlear implant users. Front. Neurosci. 2020, 14, 434. [Google Scholar] [CrossRef]
- Di Nardo, W.; Schinaia, L.; Anzivino, R.; De Corso, E.; Ciacciarelli, A.; Paludetti, G. Musical training software for children with cochlear implants. Acta Otorhinolaryngol. Ital. 2015, 35, 249–257. [Google Scholar]
- Boyer, J.; Stohl, J. MELUDIA—Online music training for cochlear implant users. Cochlear Implants Int. 2022, 23, 257–269. [Google Scholar] [CrossRef]
- Paquette, S.; Ahmed, G.D.; Goffi-Gomez, M.V.; Hoshino, A.C.H.; Peretz, I.; Lehmann, A. Musical and vocal emotion perception for cochlear implants users. Hear. Res. 2018, 370, 272–282. [Google Scholar] [CrossRef]
- World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191. [CrossRef] [Green Version]
- Tarabichi, O.; Jensen, M.; Hansen, M.R. Advances in hearing preservation in cochlear implant surgery. Curr. Opin. Otolaryngol. Head Neck Surg. 2021, 29, 385–390. [Google Scholar] [CrossRef]
- Ottaviani, F.; Iacona, E.; Sykopetrites, V.; Schindler, A.; Mozzanica, F. Cross-cultural adaptation and validation of the Nijmegen cochlear implant questionnaire into Italian. Eur. Arch. Otorhinolaryngol. 2016, 273, 2001–2007. [Google Scholar] [CrossRef] [PubMed]
- The Jamovi Project. Jamovi (Version 1.6) [Computer Software]. 2021. Available online: https://www.jamovi.org (accessed on 1 September 2022).
- Mandalà, M.; Baldi, T.L.; Neri, F.; Mencarelli, L.; Romanella, S.; Ulivelli, M.; Prattichizzo, D.; Santarnecchi, E.; Rossi, S. Feasibility of TMS in patients with new generation cochlear implants. Clin. Neurophysiol. 2021, 132, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Hammond-Kenny, A.; Borsetto, D.; Manjaly, J.G.; Panova, T.; Vijendren, A.; Bance, M.; Tysome, J.R.; Axon, P.R.; Donnelly, N.P. Cochlear implantation in elderly patients: Survival duration, hearing outcomes, complication rates, and cost utility. Audiol. Neurotol. 2022, 27, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Gfeller, K.; Mallalieu, R.M.; Mansouri, A.; McCormick, G.; O’Connell, R.B.; Spinowitz, J.; Gellinek Turner, B. Practices and attitudes that enhance music engagement of adult cochlear implant users. Front. Neurosci. 2019, 13, 1368. [Google Scholar] [CrossRef] [PubMed]
- Sparreboom, M. Sequential bilateral cochlear implantation in children quality of life. Arch. Otolaryngol. Neck Surg. 2012, 138, 134. [Google Scholar] [CrossRef] [Green Version]
- Fullerton, A.M.; Vickers, D.A.; Luke, R.; Billing, A.N.; McAlpine, D.; Hernandez-Perez, H.; Peelle, J.E.; Monaghan, J.J.M.; McMahon, C.M. Cross-modal functional connectivity supports speech understanding in cochlear implant users. Cereb. Cortex 2022, bhac277. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, R.A.; Sheffield, S.W.; Butera, I.M.; Gifford, R.H.; Wallace, M.T. Multisensory integration in cochlear implant recipients. Ear Hear. 2017, 38, 521–538. [Google Scholar] [CrossRef]
- Cambridge, G.; Taylor, T.; Arnott, W.; Wilson, W.J. Auditory training for adults with cochlear implants: A systematic review. Int. J. Audiol. 2022, 61, 896–904. [Google Scholar] [CrossRef]
- Lawrence, B.J.; Eikelboom, R.H.; Jayakody, D.M.P. Auditory-cognitive training for adult cochlear implant recipients: A study protocol for a randomised controlled trial. Trials 2021, 22, 793. [Google Scholar] [CrossRef]
- Bernstein, C.M.; Brewer, D.M.; Bakke, M.H.; Olson, A.D.; Machmer, E.J.; Spitzer, J.B.; Schauer, P.C.; Sydlowski, S.A.; Levitt, H. Maximizing cochlear implant outcomes with short-term aural rehabilitation. J. Am. Acad. Audiol. 2021, 32, 144–156. [Google Scholar] [CrossRef]
- Ferreri, L.; Singer, N.; McPhee, M.; Ripollés, P.; Zatorre, R.J.; Mas-Herrero, E. Engagement in music-related activities during the COVID-19 pandemic as a mirror of individual differences in musical reward and coping strategies. Front. Psychol. 2021, 12, 673772. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Descriptives | N | Missing | Mean | Median | SD | IQR | Minimum | Maximum |
|---|---|---|---|---|---|---|---|---|
| Age (years) | 73 | 0 | 47.1 | 49.0 | 23.1 | 46.0 | 11.0 | 89.0 |
| CI use (years) | 73 | 0 | 9.75 | 10.0 | 6.32 | 10.00 | 1.00 | 27.00 |
| Auditory deprivation (years) | 73 | 0 | 7.32 | 0.00 | 11.8 | 13.00 | 0.00 | 65.00 |
| PTA (dB) | 73 | 0 | 104 | 115 | 22.6 | 23.8 | 35.0 | 120 |
| CI-PTA (dB) | 73 | 0 | 29.8 | 30.0 | 5.84 | 8.75 | 20.0 | 50.0 |
| SRT (dB) | 69 | 4 | 40.6 | 40.0 | 9.27 | 10.0 | 22.0 | 63.0 |
| SIT (dB) | 42 | 31 | 51.9 | 50.0 | 9.94 | 17.5 | 40.0 | 70.0 |
| F MUSQUAV | 73 | 0 | 3.00 | 3.11 | 0.864 | 1.46 | 1.50 | 4.65 |
| I MUSQUAV | 73 | 0 | 3.34 | 3.44 | 0.798 | 0.83 | 1.50 | 5.00 |
| REHAB | 46 | 27 | 0.791 | 0.514 | 0.675 | 0.903 | 0.033 | 2.44 |
| NCIQ1 | 73 | 0 | 3.59 | 3.60 | 0.770 | 1.20 | 1.60 | 5.00 |
| NCIQ2 | 73 | 0 | 4.04 | 4.10 | 0.675 | 1.00 | 2.29 | 5.00 |
| NCIQ3 | 73 | 0 | 3.44 | 3.50 | 0.664 | 1.10 | 1.70 | 4.60 |
| NCIQ4 | 73 | 0 | 3.35 | 3.30 | 0.563 | 0.700 | 2.20 | 4.60 |
| NCIQ5 | 73 | 0 | 3.66 | 3.70 | 0.861 | 1.30 | 1.30 | 5.00 |
| NCIQ6 | 73 | 0 | 3.47 | 3.57 | 0.658 | 1.00 | 1.78 | 4.71 |
| NCIQ-T | 73 | 0 | 3.59 | 3.60 | 0.524 | 0.733 | 2.05 | 4.66 |
| F MUSQUAV | I MUSQUAV | NCIQ-T | Gender | Age | Onset | Rehabil. | CI Use | Aud. Depr. | PTA | CI-PTA | SRT | SIT | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F MUSQUAV | ρ | - | ||||||||||||
| adj. p-v. | - | |||||||||||||
| I MUSQUAV | ρ | 0.488 | - | |||||||||||
| adj. p-v. | 0.008 * | - | ||||||||||||
| NCIQ-T | ρ | 0.609 | 0.209 | - | ||||||||||
| adj. p-v. | 0.039 * | 0.132 | - | |||||||||||
| Gender | ρ | 0.197 | 0.049 | 0.083 | - | |||||||||
| adj. p-v. | 0.143 | 0.717 | 0.557 | - | ||||||||||
| Age | ρ | −0.399 | −0.300 | −0.223 | −0.131 | - | ||||||||
| adj. p-v. | 0.020 * | 0.029 * | 0.103 | 0.334 | - | |||||||||
| Onset | ρ | −0.367 | −0.204 | −0.133 | −0.045 | 0.601 | - | |||||||
| adj. p-v. | 0.016 * | 0.137 | 0.328 | 0.732 | 0.005 * | - | ||||||||
| Rehabil. | ρ | −0.128 | −0.204 | 0.001 | −0.201 | 0.293 | 0.270 | - | ||||||
| adj. p-v. | 0.342 | 0.138 | 0.990 | 0.142 | 0.032 * | 0.051 | - | |||||||
| CI use | ρ | 0.261 | 0.112 | 0.127 | 0.151 | −0.247 | −0.421 | −0.598 | - | |||||
| adj. p-v. | 0.058 | 0.403 | 0.342 | 0.274 | 0.072 | 0.007 * | 0.006 * | - | ||||||
| Aud. depr. | ρ | 0.178 | 0.148 | 0.050 | 0.242 | −0.160 | −0.249 | −0.845 | 0.630 | - | ||||
| adj. p-v. | 0.198 | 0.273 | 0.718 | 0.076 | 0.239 | 0.074 | 0.009 * | 0.010 * | - | |||||
| PTA | ρ | −0.162 | 0.040 | −0.065 | −0.077 | −0.178 | −0.043 | −0.417 | 0.277 | 0.074 | - | |||
| adj. p-v. | 0.243 | 0.750 | 0.633 | 0.579 | 0.192 | 0.740 | 0.004 * | 0.045 * | 0.586 | - | ||||
| CI-PTA | ρ | −0.292 | −0.178 | −0.352 | −0.370 | 0.428 | 0.137 | 0.270 | −0.233 | −0.197 | −0.117 | - | ||
| adj. p-v. | 0.033 * | 0.194 | 0.009 * | 0.078 | 0.005 * | 0.315 | 0.049 * | 0.089 | 0.147 | 0.385 | - | |||
| SRT | ρ | −0.365 | −0.166 | −0.270 | −0.255 | 0.659 | 0.384 | 0.372 | −0.314 | −0.233 | −0.250 | 0.682 | - | |
| adj. p-v. | 0.007 * | 0.240 | 0.057 | 0.072 | 0.006 * | 0.013 * | 0.007 * | 0.027 * | 0.098 | 0.076 | 0.004 * | - | ||
| SIT | ρ | −0.427 | −0.106 | −0.199 | −0.377 | 0.731 | 0.476 | 0.447 | −0.448 | −0.306 | −0.276 | 0.728 | 0.844 | - |
| adj. p-v. | 0.016 * | 0.572 | 0.272 | 0.036 * | 0.007 * | 0.016 * | 0.010 * | 0.010 * | 0.091 | 0.131 | 0.010 * | 0.005 * | - |
| F MUSQUAV | I MUSQUAV | NCIQ-T | CI-PTA | SRT | SIT | ||
|---|---|---|---|---|---|---|---|
| F MUSQUAV | ρ | - | |||||
| adj. p-v. | - | ||||||
| I MUSQUAV | ρ | 0.447 | - | ||||
| adj. p-v. | 0.015 * | - | |||||
| NCIQ-T | ρ | 0.582 | 0.171 | - | |||
| adj. p-v. | 0.008 * | 0.364 | - | ||||
| CI-PTA | ρ | −0.124 | −0.051 | −0.304 | - | ||
| adj. p-v. | 0.401 | 0.687 | 0.039 * | - | |||
| SRT | ρ | −0.084 | 0.125 | −0.146 | 0.520 | - | |
| adj. p-v. | 0.555 | 0.385 | 0.387 | 0.005 * | - | ||
| SIT | ρ | −0.180 | 0.225 | −0.224 | 0.403 | 0.540 | - |
| adj. p-v. | 0.412 | 0.362 | 0.327 | 0.040 * | 0.004 * | - |
| Descriptives | N | Missing | Mean | Median | SD | IQR | Minimum | Maximum |
|---|---|---|---|---|---|---|---|---|
| Age (years) | 46 | 0 | 46.9 | 47.0 | 21.3 | 34.3 | 11.0 | 79.0 |
| CI use (years) | 46 | 0 | 9.57 | 9.00 | 6.59 | 10.0 | 1.00 | 27.0 |
| Auditory depr. (years) | 46 | 0 | 6.96 | 0.00 | 10.7 | 13.0 | 0.00 | 48.0 |
| PTA (dB) | 46 | 0 | 107 | 116 | 19.2 | 19.1 | 48.8 | 120 |
| CI-PTA (dB) | 46 | 0 | 30.3 | 30.0 | 5.79 | 9.69 | 21.3 | 50.0 |
| SRT (dB) | 44 | 2 | 41.0 | 40.0 | 6.77 | 7.50 | 25.0 | 57.0 |
| SIT (dB) | 23 | 23 | 54.3 | 50.0 | 8.96 | 10.0 | 40.0 | 70.0 |
| F MUSQUAV | 46 | 0 | 2.85 | 2.79 | 0.75 | 1.15 | 1.61 | 4.39 |
| I MUSQUAV | 46 | 0 | 3.64 | 3.56 | 0.59 | 0.74 | 2.50 | 5.00 |
| REHAB | 46 | 0 | 0.791 | 0.514 | 0.675 | 0.903 | 0.033 | 2.44 |
| NCIQ1 | 46 | 0 | 3.50 | 3.60 | 0.703 | 0.975 | 1.60 | 4.56 |
| NCIQ2 | 46 | 0 | 4.05 | 4.01 | 0.700 | 1.09 | 2.29 | 5.00 |
| NCIQ3 | 46 | 0 | 3.39 | 3.40 | 0.625 | 1.00 | 1.70 | 4.60 |
| NCIQ4 | 46 | 0 | 3.31 | 3.20 | 0.564 | 0.667 | 2.30 | 4.60 |
| NCIQ5 | 46 | 0 | 3.50 | 3.58 | 0.870 | 1.28 | 1.30 | 4.80 |
| NCIQ6 | 46 | 0 | 3.33 | 3.40 | 0.687 | 1.04 | 1.78 | 4.44 |
| NCIQ-T | 46 | 0 | 3.51 | 3.55 | 0.526 | 0.763 | 2.05 | 4.59 |
| Variables | N | % of Total |
|---|---|---|
| Gender | ||
| Female | 33 | 71.7% |
| Male | 13 | 28.3% |
| Onset | ||
| Pre-verbal | 19 | 41.3% |
| Post-verbal | 27 | 58.7% |
| Rehabilitation | ||
| Unilateral CI | 18 | 39.1% |
| Bilateral CI | 15 | 32.6% |
| Bimodal | 13 | 28.3% |
| CI-PTA | SRT | SIT | NCIQ-T | NCIQ1 | NCIQ2 | NCIQ3 | NCIQ4 | NCIQ5 | NCIQ6 | |
|---|---|---|---|---|---|---|---|---|---|---|
| REHAB | ||||||||||
| Spearman’s rho | 0.221 | 0.417 | 0.067 | −0.356 | −0.185 | −0.092 | −0.570 | −0.344 | −0.203 | −0.230 |
| adj. p-value | 0.293 | 0.050 * | 0.806 | 0.087 | 0.325 | 0.642 | 0.010 * | 0.080 | 0.307 | 0.318 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frosolini, A.; Badin, G.; Sorrentino, F.; Brotto, D.; Pessot, N.; Fantin, F.; Ceschin, F.; Lovato, A.; Coppola, N.; Mancuso, A.; et al. Application of Patient Reported Outcome Measures in Cochlear Implant Patients: Implications for the Design of Specific Rehabilitation Programs. Sensors 2022, 22, 8770. https://doi.org/10.3390/s22228770
Frosolini A, Badin G, Sorrentino F, Brotto D, Pessot N, Fantin F, Ceschin F, Lovato A, Coppola N, Mancuso A, et al. Application of Patient Reported Outcome Measures in Cochlear Implant Patients: Implications for the Design of Specific Rehabilitation Programs. Sensors. 2022; 22(22):8770. https://doi.org/10.3390/s22228770
Chicago/Turabian StyleFrosolini, Andrea, Giulio Badin, Flavia Sorrentino, Davide Brotto, Nicholas Pessot, Francesco Fantin, Federica Ceschin, Andrea Lovato, Nicola Coppola, Antonio Mancuso, and et al. 2022. "Application of Patient Reported Outcome Measures in Cochlear Implant Patients: Implications for the Design of Specific Rehabilitation Programs" Sensors 22, no. 22: 8770. https://doi.org/10.3390/s22228770
APA StyleFrosolini, A., Badin, G., Sorrentino, F., Brotto, D., Pessot, N., Fantin, F., Ceschin, F., Lovato, A., Coppola, N., Mancuso, A., Vedovelli, L., Marioni, G., & de Filippis, C. (2022). Application of Patient Reported Outcome Measures in Cochlear Implant Patients: Implications for the Design of Specific Rehabilitation Programs. Sensors, 22(22), 8770. https://doi.org/10.3390/s22228770