
The Validity of Wireless Earbud-Type Wearable Sensors for Head Angle Estimation and the Relationships of Head with Trunk, Pelvis, Hip, and Knee during Workouts


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
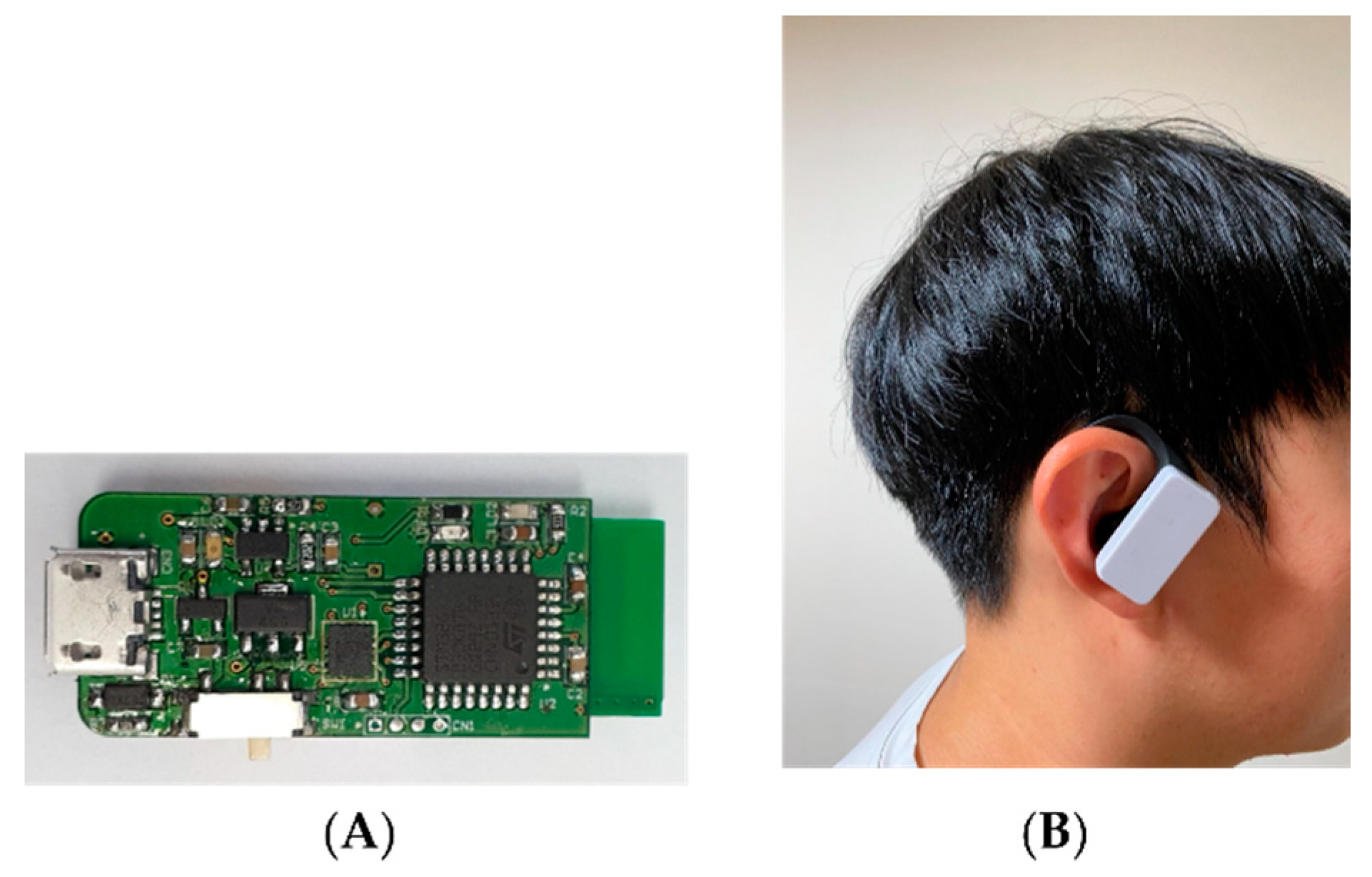
2.2. Instruments
2.3. Procedure
- General preparation stage:
- 2.
- Warm-up stage:
- 3.
- Data acquisition stage:
2.4. Data Processing
2.5. Statistical Analysis
3. Results
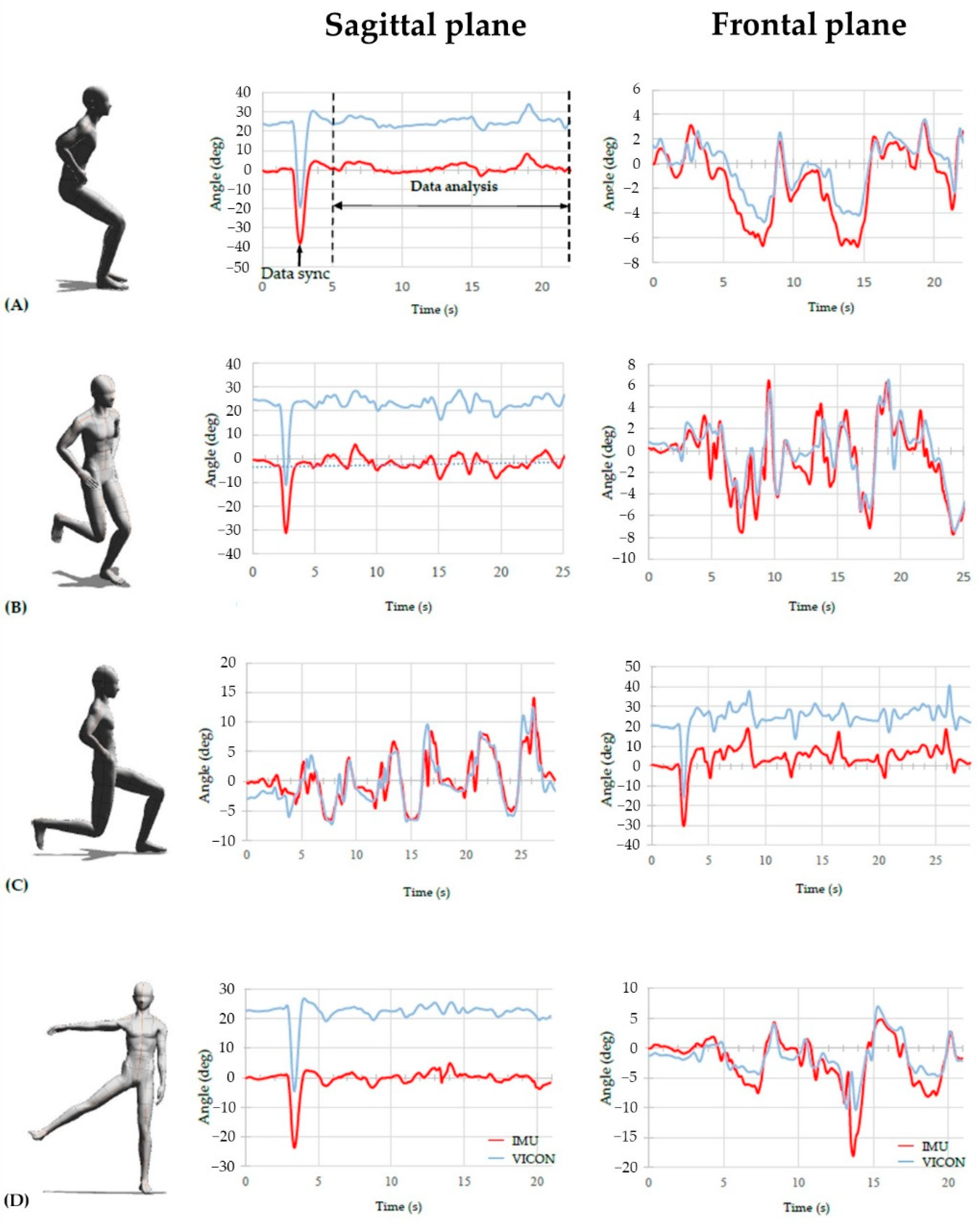
3.1. Concurrent Validity of the Earbud Type IMU Sensor
3.2. Pairwise Correlations between Head Angle Determined with the IMU Sensor and Angles of Other Joints Determined with the 3D Motion Analysis System
3.3. Pairwise Correlations between Head Angle and Angles of Other Joints Determined with the 3D Motion Analysis System

{kind=link}
{kind=link}
| Spearman’s ρ (95% CI) in Sagittal Plane | Spearman’s Ρ (95% CI) in Frontal Plane | ||||
|---|---|---|---|---|---|
| IMU vs. VICON | VICON vs. VICON | IMU vs. VICON | VICON vs. VICON | ||
| Squat | Trunk | −0.028 (−0.22, 0.164) | 0.043 (−0.166, 0.252) | 0.268 * (0.094, 0.442) | 0.222 (0.059, 0.384) |
| Pelvis | −0.005 (−0.173, 0.162) | 0.067 (−0.113, 0.246) | 0.002 (−0.145, 0.198) | −0.035 (−0.153, 0.083) | |
| Hip_Rt | 0.019 (−0.166, 0.203) | 0.076 (−0.121, 0.274) | 0.069 (−0.086, 0.224) | 0.143 (0.01, 0.276) | |
| Hip_Lt | 0.014 (−0.169, 0.198) | 0.07 * (−0.127, 0.267) | 0.071 (−0.079, 0.221) | 0.071 (−0.102, 0.244) | |
| Knee_Rt | −0.063 * (−0.268, 0.141) | −0.006 * (−0.228, 0.216) | −0.024 (−0.195, 0.148) | 0.021 (−0.148, 0.191) | |
| Knee_Lt | −0.023 * (−0.22, 0.173) | 0.048 * (−0.166, 0.262) | 0.003 (−0.153, 0.159) | 0.021 (−0.131, 0.174) | |
| Single-leg squat | Trunk | −0.216 (−0.339, 0.094) | −0.137 (−0.277, 0.003) | 0.536 * (0.405, 0.667) | 0.606 * (0.498, 0.715) |
| Pelvis | −0.122 (−0.25, 0.005) | −0.069 (−0.204, 0.066) | 0.366 * (0.231, 0.501) | 0.33 * (0.182, 0.479) | |
| Hip_Rt | −0.146 (−0.295, 0.003) | −0.115 (−0.273, 0.043) | −0.272 (−0.414, −0.129) | −0.197 (−0.352, −0.041) | |
| Hip_Lt | −0.086 (−0.221, 0.049) | −0.049 (−0.186, 0.089) | 0.267 (0.118, 0.416) | 0.260 (0.114, 0.406) | |
| Knee_Rt | −0.151 (−0.295, −0.007) | −0.145 (−0.298, 0.008) | 0.258 (0.098, 0.417) | 0.276 (0.12, 0.431) | |
| Knee_Lt | −0.121 (−0.23, −0.012) | −0.101 (−0.212, 0.01) | 0.132 (0.017, 0.247) | 0.195 (0.068, 0.322) | |
| Reverse lunge | Trunk | −0.129 (−0.239, −0.019) | −0.168 (−0.325, 0.011) | 0.437 * (0.335, 0.54) | 0.459 * (0.329, 0.589) |
| Pelvis | −0.138 (−0.225, −0.051) | −0.193 (−0.327, −0.06) | −0.005 (−0.134, 0.123) | −0.008 (−0.156, 0.141) | |
| Hip_Rt | −0.292 (−0.384, −0.2) | 0.009 (−0.089, 0.107) | −0.148 (−0.242, −0.053) | −0.027 (−0.142, 0.087) | |
| Hip_Lt | 0.076 (−0.064, −0.217) | −0.014 (−0.166, 0.137) | 0.033 (−0.1, 0.166) | −0.008 (−0.157, 0.141) | |
| Knee_Rt | 0.026 (−0.106, −0.158) | 0.099 (−0.05, 0.249) | 0.231 (0.103, 0.36) | 0.191 (0.051, 0.33) | |
| Knee_Lt | 0.094 (−0.036, −0.223) | 0.053 (−0.097, 0.202) | 0.189 (0.072, 0.305) | 0.198 (0.074, 0.323) | |
| Standing hip abduction | Trunk | −0.158 (−0.323, −0.007) | −0.152 (−0.328, 0.025) | 0.384 * (0.185, 0.582) | 0.467 * (0.27, 0.665) |
| Pelvis | −0.183 (−0.349, −0.017) | −0.187 (−0.359, −0.015) | 0.254 * (0.05, 0.458) | 0.234 * (0.022, 0.447) | |
| Hip_Rt | −0.171 (−0.348, −0.006) | −0.201 (−0.382, −0.02) | −0.124 (−0.365, 0.117) | −0.074 (−0.319, 0.171) | |
| Hip_Lt | −0.146 (−0.312, −0.02) | −0.15 (−0.323, 0.024) | −0.155 (−0.354, 0.044) | −0.105 (−0.313, 0.104) | |
| Knee_Rt | −0.239 (−0.357, −0.122) | −0.237 (−0.354, −0.119) | 0.337 * (0.145, 0.529) | 0.296 * (0.112, 0.479) | |
| Knee_Lt | −0.155 (−0.227, −0.038) | −0.132 (−0.272, 0.008) | −0.095 (−0.188, 0.173) | 0.025 (−0.173, 0.223) | |
4. Discussion
4.1. Concurrent Validity of the Earbud-Type IMU Sensor
4.2. Pairwise Correlations between Head Angle and Angles of Other Joints
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Correction Statement
References
- Al Attar, W.S.A.; Husain, M.A. How did athletes train and avoid injuries during the covid-19 quarantine period? Trends Sport Sci. 2021, 28, 109–115. [Google Scholar]
- Berengüí, R.; López-Gullón, J.M.; Angosto, S. Physical sports activities and exercise addiction during lockdown in the Spanish population. Int. J. Environ. Res. Public Health 2021, 18, 3119. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.F.; Agarwal, V.; Zheng, P.; Smuck, M.; Fredericson, M.; Kennedy, D.J.; Krauss, J. Digital care for chronic musculoskeletal pain: 10,000 participant longitudinal cohort study. J. Med. Internet Res. 2020, 22, e18250. [Google Scholar] [CrossRef] [PubMed]
- Shebib, R.; Bailey, J.F.; Smittenaar, P.; Perez, D.A.; Mecklenburg, G.; Hunter, S. Randomized controlled trial of a 12-week digital care program in improving low back pain. NPJ Digit. Med. 2019, 2, 1. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Nava, I.H.; Angelica, M.M. Wearable Inertial Sensors for Human Motion Analysis: A review. IEEE Sens. J. 2016, 16, 7821–7834. [Google Scholar] [CrossRef]
- Aroganam, G.; Manivannan, N.; Harrison, D. Review on Wearable Technology Sensors Used in Consumer Sport Applications. Sensors 2019, 19, 1983. [Google Scholar] [CrossRef] [PubMed]
- Al-Amri, M.; Nicholas, K.; Button, K.; Sparkes, V.; Sheeran, L.; Davies, J.L. Inertial measurement units for clinical movement analysis: Reliability and concurrent validity. Sensors 2018, 18, 719. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.H.; Hong, S.H.; Oh, I.W.; Lee, Y.W.; Kee, I.H.; Lee, S.Y. Measurement of ankle joint movements using imus during running. Sensors 2021, 21, 4240. [Google Scholar] [CrossRef]
- Tak, I.; Wiertz, W.; Barendrecht, M.; Langhout, R. Validity of a New 3-D Motion Analysis Tool for the Assessment of Knee, Hip and Spine Joint Angles during the Single Leg Squat. Sensors 2020, 20, 4539. [Google Scholar] [CrossRef]
- Lee, C.M.; Gorelick, M. Validity of the Smarthealth watch to measure heart rate during rest and exercise. Meas. Phys. Educ. Exerc. Sci. 2011, 15, 18–25. [Google Scholar] [CrossRef]
- Whelan, D.; O’Reilly, M.; Ward, T.E.; Delahunt, E.; Caulfield, B. Evaluating performance of the lunge exercise with multiple and individual inertial measurement units. Pervasive Health Pervasive Comput. Technol. Healthc. 2016, 2016, 101–108. [Google Scholar]
- Siepmann, C.; Kowalczuk, P. Understanding continued smartwatch usage: The role of emotional as well as health and fitness factors. Electron. Mark. 2021, 31, 795–809. [Google Scholar] [CrossRef]
- Farrokhi, S.; Pollard, C.D.; Souza, R.B.; Chen, Y.J.; Reischl, S.; Powers, C.M. Trunk position influences the kinematics, kinetics, and muscle activity of the lead lower extremity during the forward lunge exercise. J. Orthop. Sports Phys. Ther. 2008, 38, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Harriss, J.; Khan, A.; Song, K.; Register-Mihalik, J.K.; Wikstrom, E.A. Clinical movement assessments do not differ between collegiate athletes with and without chronic ankle instability. Phys. Ther. Sport 2019, 36, 22–27. [Google Scholar] [CrossRef]
- Severin, A.C.; Burkett, B.J.; McKean, M.R.; Wiegand, A.N.; Sayers, M.G.L. Limb symmetry during double-leg squats and single-leg squats on land and in water in adults with long-standing unilateral anterior knee pain; a cross sectional study. BMC Sports Sci. Med. Rehabil. 2017, 9, 20. [Google Scholar] [CrossRef] [PubMed]
- Hausamann, P.; Daumer, M.; MacNeilage, P.R.; Glasauer, S. Ecological momentary assessment of head motion: Toward normative data of head stabilization. Front. Hum. Neurosci. 2019, 13, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Anson, E.; Rosenberg, R.; Agada, P.; Kiemel, T.; Jeka, J. Does visual feedback during walking result in similar improvements in trunk control for young and older healthy adults? J. Neuroeng. Rehabil. 2013, 10, 110. [Google Scholar] [CrossRef] [PubMed]
- Psarakis, M.; Greene, D.A.; Cole, M.H.; Lord, S.R.; Hoang, P.; Brodie, M. Wearable technology reveals gait compensations, unstable walking patterns and fatigue in people with multiple sclerosis. Physiol. Meas. 2018, 2, 16–39. [Google Scholar] [CrossRef]
- Hunn, N. The Market for Hearable Devices 2016–2020. Available online: https://www.nickhunn.com/wp-content/uploads/downloads/2016/11/The-Market-for-Hearable-Devices-2016-2020.pdf (accessed on 5 November 2016).
- Umek, A.; Kos, A. Wearable sensors and smart equipment for feedback in watersports. Procedia Comput. Sci. 2018, 129, 496–502. [Google Scholar] [CrossRef]
- John, M.; Klose, S.; Seewald, B. Innovative Rehabilitation Technologies for Home Environments—An Overview. Handb. Ambient Assist. Living 2012, 11, 805–833. [Google Scholar] [CrossRef]
- Saraceni, N.; Kent, P.; Ng, L.; Campbell, A.; Straker, L.; O’Sullivan, P. To flex or not to flex? Is there a relationship between lumbar spine flexion during lifting and low back pain? A systematic review with meta-analysis. J. Orthop. Sports Phys. Ther. 2020, 50, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Dingenen, B.; Malfait, B.; Nijs, S.; Peers, K.H.E.; Vereecken, S.; Verschueren, S.M.P.; Staes, F.F. Can two-dimensional video analysis during single-leg drop vertical jumps help identify non-contact knee injury risk? A one-year prospective study. Clin. Biomech. 2015, 30, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Hellec, J.; Chorin, F.; Castagnetti, A.; Colson, S.S. Sit-to-stand movement evaluated using an inertial measurement unit embedded in smart glasses—A validation study. Sensors 2020, 20, 5019. [Google Scholar] [CrossRef] [PubMed]
- Butowicz, C.M.; Ebaugh, D.D.; Noehren, B.; Silfies, S.P. Validation of Two Clinical Measures of Core Stability. Int. J. Sports Phys. Ther. 2016, 11, 15–23. [Google Scholar]
- Federolf, P.A. A Novel Approach to Solve the “Missing Marker Problem” in Marker-Based Motion Analysis That Exploits the Segment Coordination Patterns in Multi-Limb Motion Data. PLoS ONE 2013, 8, e78689. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Farewik, E.M.; Bartonek, Å.; Saraste, H. Comparison and evaluation of two common methods to measure center of mass displacement in three dimensions during gait. Hum. Mov. Sci. 2006, 25, 238–256. [Google Scholar] [CrossRef] [PubMed]
- Meldrum, D.; Shouldice, C.; Conroy, R.; Jones, K.; Forward, M. Test-retest reliability of three dimensional gait analysis: Including a novel approach to visualising agreement of gait cycle waveforms with Bland and Altman plots. Gait Posture 2014, 39, 265–271. [Google Scholar] [CrossRef]
- Hughes, T.; Jones, R.K.; Starbuck, C.; Sergeant, J.C.; Callaghan, M.J. The value of tibial mounted inertial measurement units to quantify running kinetics in elite football (soccer) players. A reliability and agreement study using a research orientated and a clinically orientated system. J. Electromyogr. Kinesiol. 2019, 44, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Cristiano, A.; Nazemzadeh, P.; Tettamanti, A.; Sanna, A.; Trojaniello, D. Head acceleration patterns in postural transitions and straight walking: A preliminary study. In Proceedings of the GNB2018, Milan, Italy, 25–27 June 2018. [Google Scholar]
- Bonnet, V.; Mazzà, C.; Fraisse, P.; Cappozzo, A. A least-squares identification algorithm for estimating squat exercise mechanics using a single inertial measurement unit. J. Biomech. 2012, 45, 1472–1477. [Google Scholar] [CrossRef]
- Goulette, D.; Griffith, P.; Schiller, M.; Rutherford, D.; Kernozek, T.W. Patellofemoral joint loading during the forward and backward lunge. Phys. Ther. Sport 2021, 47, 178–184. [Google Scholar] [CrossRef]
- Kim, J.-S.; Kim, Y.-W.; Woo, Y.-K.; Park, K.-N. Validity of an Artificial Intelligence-Assisted Motion-Analysis System Using a Smartphone for Evaluating Weight-Bearing Activities in Individuals with Patellofemoral Pain Syndrome. J. Musculoskelet. Sci. Technol. 2021, 5, 34–40. [Google Scholar] [CrossRef]
- Chan, Y.H. Biostatistics 104. Corrleational analysis. Singapore Med. J. 2005, 46, 153–160. [Google Scholar] [PubMed]
- Mentiplay, B.F.; Hasanki, K.; Perraton, L.G.; Pua, Y.H.; Charlton, P.C.; Clark, R.A. Three-dimensional assessment of squats and drop jumps using the Microsoft Xbox One Kinect: Reliability and validity. J. Sports Sci. 2018, 36, 2202–2209. [Google Scholar] [CrossRef] [PubMed]
- Eltoukhy, M.; Kelly, A.; Kim, C.Y.; Jun, H.P.; Campbell, R.; Kuenze, C. Validation of the Microsoft Kinect® camera system for measurement of lower extremity jump landing and squatting kinematics. Sport. Biomech. 2016, 15, 89–102. [Google Scholar] [CrossRef]
- Duc, C.; Salvia, P.; Lubansu, A.; Feipel, V.; Aminian, K. A wearable inertial system to assess the cervical spine mobility: Comparison with an optoelectronic-based motion capture evaluation. Med. Eng. Phys. 2014, 36, 49–56. [Google Scholar] [CrossRef]
- Jasiewicz, J.M.; Treleaven, J.; Condie, P.; Jull, G. Wireless orientation sensors: Their suitability to measure head movement for neck pain assessment. Man. Ther. 2007, 12, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Parrington, L.; Jehu, D.A.; Fino, P.C.; Pearson, S.; El-Gohary, M.; King, L.A. Validation of an Inertial Sensor algortithm to quantify head and trunk movement in healthy young adults and individuals with mild traumatic brain injury 2018. Sensors 2018, 18, 4501. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Liu, P.; Ou, Y.; Huang, Q.; Song, R.; Dou, Z.; Zheng, Y. Trunk and Head Control during Walking in Patients with Unilateral Vestibular Hypofunction: Effect of Lower Limb Somatosensory Input. Am. J. Phys. Med. Rehabil. 2019, 98, 906–913. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.S.; Walther, R.G.; Beseris, E.A.; Dibble, L.E.; Lester, M.E. Feasibility and validity of discriminating yaw plane head on trunk motion using inertial wearable sensors. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 2347–2354. [Google Scholar] [CrossRef]
- Carroll, L.A.; Kivlan, B.R.; Martin, R.L.; Phelps, A.L.; Carcia, C.R. The Single Leg Squat Test: A “Top-Down” or “Bottom-Up” Functional Performance Test? Int. J. Sports Phys. Ther. 2021, 16, 360–370. [Google Scholar] [CrossRef]
- Basta, D.; Singbartl, F.; Todt, I.; Clarke, A.; Ernst, A. Vestibular rehabilitation by auditory feedback in otolith disorders. Gait Posture 2008, 28, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Dierks, T.A.; Manal, K.T.; Hamill, J.; Davis, I.S. Proximal and distal influences on hip and knee kinematics in runners with patellofemoral pain during a prolonged run. J. Orthop. Sports Phys. Ther. 2008, 38, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Souza, R.B.; Powers, C.M. Differences in hip kinematics, muscle strength, and muscle activation between subjects with and without patellofemoral pain. J. Orthop. Sports Phys. Ther. 2009, 39, 12–19. [Google Scholar] [CrossRef]
- Nakagawa, T.H.; Moriya, E.T.U.; MacIel, C.D.; Serrão, F.V. Trunk, pelvis, hip, and knee kinematics, hip strength, and gluteal muscle activation during a single-leg squat in males and females with and without patellofemoral pain syndrome. J. Orthop. Sports Phys. Ther. 2012, 42, 491–501. [Google Scholar] [CrossRef] [PubMed]
- Hunt, M.A.; Wrigley, T.V.; Hinman, R.S.; Bennell, K.L. Individuals with severe knee osteoarthritis (OA) exhibit altered proximal walking mechanics compared with individuals with less severe OA and those without knee pain. Arthritis Care Res. 2010, 62, 1426–1432. [Google Scholar] [CrossRef] [PubMed]
- Hunt, M.A.; Birmingham, T.B.; Bryant, D.; Jones, I.; Giffin, J.R.; Jenkyn, T.R.; Vandervoort, A.A. Lateral trunk lean explains variation in dynamic knee joint load in patients with medial compartment knee osteoarthritis. Osteoarthr. Cartil. 2008, 16, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Poitras, I.; Dupuis, F.; Bielmann, M.; Campeau-Lecours, A.; Mercier, C.; Bouyer, L.J.; Roy, J.S. Validity and reliability ofwearable sensors for joint angle estimation: A systematic review. Sensors 2019, 19, 1555. [Google Scholar] [CrossRef]
- Al-Eisa, E.; Egan, D.; Deluzio, K.; Wassersug, R. Effects of pelvic asymmetry and low back pain on trunk kinematics during sitting: A comparison with standing. Spine 2006, 31, E135–E143. [Google Scholar] [CrossRef]
- Kim, H.; Son, S.J.; Seeley, M.K.; Hopkins, J.T. Altered movement strategies during jump landing/cutting in patients with chronic ankle instability. Scand. J. Med. Sci. Sports. 2019, 29, 1130–1140. [Google Scholar] [CrossRef]
- Garrick, L.; Alexander, B.; Schache, A.; Pandy, M.; Crossley, K.; Collins, N. Validation of visual rating criteria for single leg squat performance in asymptomatic runners. J. Sci. Med. Sport 2014, 18, e75–e76. [Google Scholar] [CrossRef]
- Sabatini, A.M. Estimating three-dimensional orientation of human body parts by inertial/magnetic sensing. Sensors 2011, 11, 1489–1525. [Google Scholar] [CrossRef] [PubMed]
| Variables | Mean ± Standard Deviation |
|---|---|
| Male/female, n | 9/11 |
| Age, years | 21.1 ± 3.1 |
| Weight, kg | 63.7 ± 11.3 |
| Height, cm | 169.3 ± 7.8 |
| Body mass index, kg/m2 | 22.1 ± 2.6 |
| Exercise frequency per week, times/week | 3.6 ± 1.7 |
| Daily exercise duration, min | 69.5 ± 33.3 |
| Sagittal Plane | Frontal Plane | |||
|---|---|---|---|---|
| Spearman’s ρ | 95% CI | Spearman’s ρ | 95% CI | |
| Squat | 0.906 * | 0.861, 0.951 | 0.760 * | 0.695, 0.825 |
| Single-leg squat | 0.897 * | 0.879, 0.915 | 0.753 * | 0.706, 0.799 |
| Reverse lunge | 0.624 * | 0.56, 0.689 | 0.784 * | 0.74, 0.828 |
| Standing hip abduction | 0.912 * | 0.887, 0.938 | 0.766 * | 0.691, 0.841 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, A.-R.; Park, J.-H.; Kim, S.-H.; Kim, K.B.; Park, K.-N. The Validity of Wireless Earbud-Type Wearable Sensors for Head Angle Estimation and the Relationships of Head with Trunk, Pelvis, Hip, and Knee during Workouts. Sensors 2022, 22, 597. https://doi.org/10.3390/s22020597
Kim A-R, Park J-H, Kim S-H, Kim KB, Park K-N. The Validity of Wireless Earbud-Type Wearable Sensors for Head Angle Estimation and the Relationships of Head with Trunk, Pelvis, Hip, and Knee during Workouts. Sensors. 2022; 22(2):597. https://doi.org/10.3390/s22020597
Chicago/Turabian StyleKim, Ae-Ryeong, Ju-Hyun Park, Si-Hyun Kim, Kwang Bok Kim, and Kyue-Nam Park. 2022. "The Validity of Wireless Earbud-Type Wearable Sensors for Head Angle Estimation and the Relationships of Head with Trunk, Pelvis, Hip, and Knee during Workouts" Sensors 22, no. 2: 597. https://doi.org/10.3390/s22020597
APA StyleKim, A.-R., Park, J.-H., Kim, S.-H., Kim, K. B., & Park, K.-N. (2022). The Validity of Wireless Earbud-Type Wearable Sensors for Head Angle Estimation and the Relationships of Head with Trunk, Pelvis, Hip, and Knee during Workouts. Sensors, 22(2), 597. https://doi.org/10.3390/s22020597